Back to Journals » Clinical Interventions in Aging » Volume 21
Construction of Outcome Quality Evaluation Indicators for Home Hospice Care in Older Patients with Terminal Cancer in China: A Delphi Study
Authors Wang L, Zhang Y, Chi Y
Received 26 January 2026
Accepted for publication 6 May 2026
Published 18 May 2026 Volume 2026:21 599036
DOI https://doi.org/10.2147/CIA.S599036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Lei Wang,1 Yiming Zhang,2 Yuan Chi3
1Department of Nursing, Jinzhou Medical University, Jinzhou, Liaoning Province, People’s Republic of China; 2School of Nursing, Soochow University, Suzhou, Jiang Su Province, People’s Republic of China; 3Department of Graduate, Jinzhou Medical University, Jinzhou, Liaoning Province, People’s Republic of China
Correspondence: Yuan Chi, Jinzhou Medical University, No. 40, Section 3, Songpo Road, Linghe District, Jinzhou City, Liaoning Province, 121000, People’s Republic of China, Tel +8615124020001, Email [email protected]
Purpose: With the rapid aging of the population and the increasing prevalence of terminal cancer among older adults worldwide, the demand for high-quality home hospice care is growing. However, there is a lack of culturally appropriate and systematic outcome quality evaluation indicators. This study aimed to construct a set of outcome quality evaluation indicators for home hospice care in older patients with terminal cancer in China, guided by the Harmony Nursing Theory.
Methods: A three-phase methodological design was employed. First, a 12-member multidisciplinary research team was established. Second, preliminary indicators were developed through a literature review of 18 relevant studies and qualitative interviews with 12 healthcare professionals. Third, two rounds of Delphi expert consultation were conducted to refine and validate the indicators. A pilot test was subsequently performed to assess feasibility. We calculated the expert positive coefficient (response rate), expert authority coefficient, and expert opinion coordination coefficient (Kendall’s W).
Results: In the first round of Delphi consultation, 24 questionnaires were distributed and 22 were returned, yielding a response rate of 91.7% In the second round, 22 questionnaires were distributed and all were returned (100% response rate). The expert authority coefficient was 0.96 in both rounds. Kendall’s W was 0.247 and 0.296 in the first and second rounds, respectively. After the first round, three indicators were deleted, fifteen indicators were revised, and four indicators were added. Following the second round, two indicators were modified. The outcome quality evaluation indicator for home hospice care consisted of 4 first-level indicators, 12 second-level indicators, and 45 third-level indicators.
Conclusion: This study developed a culturally relevant and methodologically sound outcome quality evaluation indicator for home hospice care in older patients with terminal cancer in China. The indicators provide a tool for evaluating care quality, guiding clinical practice, and improving patient-centered outcomes in home hospice settings.
Keywords: hospice care, older adult, harmony nursing theory, cancer, Delphi method
Introduction
Population aging has become a global trend, the global proportion of people aged 65 and above increased from 5% in 1950 to 10% in 2023, and is projected to reach 16% by 2050.1 From 1950 to 2050, the proportion of older adults in countries such as France, Sweden, and the United States is projected to increase by 13–15 percentage points.2 According to the Chinese Seventh National Population Census (2020), individuals aged 60 and above reached 264 million (18.7%), with those aged 65 and above at 191 million (13.5%).3 Against this backdrop, influenced by lifestyle and environmental factors, malignant tumor incidence among older adults continues to rise, emerging as a leading cause of death.4 By 2030, the United States is expected to have 22.1 million cancer patients, 64% of whom will be aged 65 or older;5 data from the Chinese National Cancer Center indicate peak incidence at age 80, with a cumulative risk of 36% by age 85.6 Thus, the number of older cancer patients is rising markedly across multiple countries amid population aging. Older cancer patients often have an insidious onset and atypical early symptoms, with approximately 80% diagnosed at advanced stages and a metastasis rate as high as 74.8%, frequently missing the optimal treatment window.7,8 Studies show that terminal older cancer patients commonly suffer from symptoms such as fatigue, pain, and malnutrition, accompanied by psychological issues like anxiety and low self-esteem,9 forming a vicious cycle of physical-psychological exacerbation that severely impairs quality of life. Currently, quality of life and death in the terminal stage are receiving increasing attention, with the Economist Intelligence Unit’s Quality of Death Index ranking China 53rd out of 80 countries and indicating a relatively low overall level.10 The “14th Five-Year Plan” issued by the State Council of China in 2021 explicitly proposes to develop hospice care services,11 and China has officially unified the terms “hospice care”, “palliative care”, and “end-of-life care” under the single designation of “hospice care”.12 Hospice care is patient- and family-centered, providing symptom control, comfort care, and psychosocial support through multidisciplinary collaboration to improve end-of-life quality of life and achieve dignified, pain-free death.13,14 Hospice care service modes include inpatient hospice care (in hospitals, nursing homes, etc), community hospice care, and home hospice care.15 At present, community and home hospice services have become important components of hospice care systems in the UK and US, with a common direction of shifting from “institution-centered” to “community- and family-centered”.16,17 The WHO also advocates integrating hospice care into family and community levels.18 Influenced by the cultural concept of “returning to one’s roots”, most Chinese terminal older cancer patients prefer dying at home.19 Therefore, home hospice care is a service mode worth promoting in China. Quality evaluation in hospice care is the primary step for accurately assessing, controlling, and improving the quality of home hospice care services.20 Among these, outcome quality refers to events accompanying the structure and process of care, mainly describing the impact of care on patient and population health status, serving as the gold standard in quality evaluation.21 Western countries initiated hospice care earlier, with more in-depth research on outcome quality indicators for home hospice care. Masaki et al developed a outcome quality indicator system for end-of-life older adult care from a nursing perspective, encompassing symptom management, pain relief, daily care in the dying phase, and family/social support.22 Additionally, outcome quality indicators vary by service type and are categorized into physical, psychological, social support, and spiritual care domains. Harman et al focused on physiological and psychological aspects, proposing indicators such as fall rates, severe pain incidence, and caregiver grief rates for home end-of-life older adult hospice care.23 Furthermore, the eight domains of palliative care proposed by the U.S. National Quality Forum (NQF) have become core requirements for high-quality services.24 Hospice care research in mainland China started relatively late, with existing indicator systems primarily targeting inpatient settings, such as Hongju Yang et al’s framework for cancer patient hospice care quality evaluation, including 6 first-level indicators like environment management, symptom care, and nutritional support.25 In older adult care, studies mainly address needs assessment, adverse event rates, and satisfaction. Currently, there is no dedicated tools exist for evaluating outcome quality in home hospice care for terminal older cancer in China.
International approaches to indicator construction predominantly employ modified Delphi techniques, integrating best-practice evidence from literature reviews with principles of feasibility and applicability, followed by expert panel discussions or consultations to finalize outcome indicators.26 Chinese scholars constructing hospice care service quality indicators often adopt foreign methods and theoretical frameworks (eg., Maslow’s hierarchy of needs and the Compassionate Collaborative Care Model).27,28 However, the frequent absence of localized theoretical support results in mechanistic application and compromised practical effectiveness, as these foreign frameworks were developed in Western cultural contexts and fail to capture the culturally specific end-of-life needs of Chinese patients. Consequently, developing culturally adapted outcome quality indicators grounded in indigenous Chinese theories has become a priority in the advancement of home hospice care. To address this gap rigorously, an ideal indigenous theoretical framework for hospice care indicator construction must meet three non-negotiable core criteria: (1) deep integration of Chinese core cultural values to capture culturally specific patient experiences and needs; (2) alignment with the holistic core principles of hospice care (encompassing physical, psychological, social, and spiritual dimensions); and (3) demonstrated empirical applicability and validity in Chinese clinical hospice settings. However, the widely adopted foreign frameworks referenced above fail to fully satisfy these criteria. While they provide valuable universal care principles, they lack explicit consideration of Chinese foundational values such as filial piety, family-centered decision-making, and collective harmony—factors that fundamentally shape how Chinese patients experience end-of-life care and evaluate its quality. This inherent cultural disconnect directly explains the mechanistic translation and limited real-world utility of existing indicator systems developed using foreign theories.
Against this backdrop, the Harmony Nursing Theory, proposed by Li Zheng (2016) based on Rogers’ Science of Unitary Human Beings, incorporates traditional Chinese concepts of “harmony”, “family culture”, and “filial piety ethics”, forming a framework with both universality and cultural appropriateness.29 The theory comprises three phases: early identification of harmony needs, construction of “harmony” and “coordination” mechanisms, and fulfillment of harmony demand. It has already been successfully applied in Chinese hospice care contexts for situational analysis, nursing decision-making, care pathway development, and intervention effect evaluation.30 Moreover, it aligns perfectly with the core tenets of hospice care by emphasizing holistic coordination across physical, psychological, social, and spiritual dimensions to achieve patient inner peace and tranquility. Thus, it serves as the most theoretically sound and practically suitable foundation for investigating culturally appropriate outcome quality indicators in home hospice care services.
This study, grounded in Harmony Nursing Theory and integrating literature review, qualitative research, and the Delphi method, constructs culturally appropriate outcome quality indicators for home hospice care in older patients with terminal cancer in China. These indicators have the potential to provide a preliminary basis for adjusting clinical nursing behaviors and optimizing care processes, potentially facilitating timely service improvements and ultimately contributing to the enhancement of quality of life for older cancer patients.
Materials and Methods
Phase I: Establishment of the Research Team
The research team consists of 12 members in total, including 1 team leader (director of the nursing department), 1 secretary (hospice care specialist nurse), 2 geriatric nurses (senior nurses), 2 community doctors (chief physicians), 2 community nurses (senior nurses), 2 nursing teachers (professors), and 2 research assistants (doctoral nursing graduate). The work contents of the research team are as follows: determining the research topic, searching the literature and collecting data, formulating the consultation questionnaire, identifying experts for consultation, discussing research results, etc.
Phase II: Initial Construction of Outcome Quality Evaluation Indicators for Home Hospice Care
First, systematic literature searches were conducted across five English databases (PubMed, Web of Science, CINAHL, Scopus, and EMBASE) using the English search terms: (“terminal care” OR “end-of-life care” OR “home hospice care” OR “home palliative care”) AND (“quality assessment” OR “quality evaluation” OR “quality indicators”). Simultaneously, searches were performed in three Chinese databases (CNKI, Wanfang, and VIP) using the Chinese search terms: “居家 (home-based)”, “安宁疗护 / 缓和医疗 / 善终服务 / 终末期护理 (palliative care/hospice care/end-of-life care)”, “护理质量 / 质量评价 / 评价指标 (nursing quality/quality evaluation/evaluation indicators)”, “癌症 (cancer)”, “终末期 (terminal stage)”, and “老年人 (older adult)”. The search period covered from the establishment of each database to February 28, 2025. Languages are limited to English and Chinese. Inclusion criteria for literature: (1) Study type: cross-sectional studies, Delphi studies, and randomized controlled trials; (2) Study subjects: older adults aged 60 years and above with terminal cancer; (3) Care setting: home-based hospice or palliative care; (4) Study content: focusing on quality evaluation or outcome indicator construction of home hospice care. Exclusion criteria for literature: (1) Reviews, commentaries, conference abstracts, and case reports; (2) Studies with unavailable full text or incomplete data.
A total of 6772 English and Chinese articles were initially retrieved. After automatic deduplication using EndNote 20 software, 4,318 articles remained and entered the title/abstract screening stage. Two independent researchers (Author Lei and Author Yiming) who had received standardized training conducted screening according to the pre-specified inclusion and exclusion criteria. Discrepancies were resolved through discussion with a third senior researcher (Author Yuan) until consensus was reached. During title/abstract screening, 2,432 articles were excluded for not meeting the study scope, leaving 22 articles for full-text assessment. After full-text review, 4 additional articles were excluded (2 for non-outcome indicators, 2 for unavailable full text), resulting in a final inclusion of 18 eligible studies. Methodological quality assessment was performed using the JBI Critical Appraisal Checklist, and all 18 included studies had a quality score of >60%, indicating moderate to high overall methodological quality.
Based on the 18 included studies, we extracted all reported outcome quality indicators for home hospice care. Guided by the four core dimensions of the Harmony Nursing Theory (physical harmony, psychological harmony, social harmony, and spiritual harmony), we categorized and merged the extracted indicators to construct a preliminary draft of the outcome quality evaluation indicator system. The preliminary draft consisted of 4 first-level indicators, 8 second-level indicators (including symptom control, activities of daily living, emotional support, and family burden relief), and 27 third-level indicators mapped to the corresponding second-level indicators.
Second, semi-structured qualitative interviews were conducted from April 1 to June 30, 2025. Maximum variation purposive sampling was employed to select healthcare professionals engaged in home hospice care services from three community health service centers in Jinzhou City, Liaoning Province, China. This sampling strategy ensured representation across different professional roles, genders, and years of clinical experience. Inclusion criteria for participants were: (1) Healthcare staff who had obtained a valid practicing physician or practicing nurse license; (2) Healthcare staff with at least two years of work experience in home hospice care. Exclusion criteria: (1) Those on leave, sick leave, or away for further study during the survey period; (2) Those who withdrew from the study midway. All participants signed written informed consent forms prior to the interview and voluntarily participated in face-to-face interviews. Interviews were conducted in a quiet, private meeting room at each community health service center, lasted 35–50 minutes per participant, and were audio-recorded with explicit verbal permission. All recordings were transcribed with verbatim within 24 hours of the interview, and all personally identifiable information was anonymized to ensure confidentiality. Respondents were asked to consider the Chinese national context and cultural practices to elicit their understanding of outcome quality evaluation indicators for home hospice care among terminally ill older cancer patients. The semi-structured interview guide focused on the following core questions: (1) What aspects do you prioritize when treating (or caring for) patients receiving home hospice care? (2) What difficulties do you encounter in the process of managing (or caring for) patients receiving home hospice care? What is the greatest difficulty, and how do you address it? (3) How is the outcome quality of home hospice care currently evaluated in your setting? Are there any relevant evaluation tools? From which aspects are the evaluation conducted? (4) In your opinion, what additional content should be included in (or removed from) the outcome quality evaluation of home hospice care, and why? (5) Do you have any other thoughts or suggestions regarding this home hospice care outcome quality evaluation? The interview data were analyzed using the standardized Colaizzi seven-step method, implemented independently by two trained qualitative researchers: (1) Read all verbatim transcripts repeatedly to gain a holistic understanding of participants’ perspectives; (2) Extract significant statements directly related to home hospice care outcome quality evaluation; (3) Code the extracted statements and formulate corresponding meaning units; (4) Cluster similar meaning units into preliminary themes and sub-themes; (5) Describe the essential structure of the research phenomenon based on clustered themes; (6) Construct a comprehensive descriptive text integrating all themes; (7) Return preliminary themes to 2 participants for member checking to validate authenticity. Inter-coder reliability was assessed using Cohen’s Kappa coefficient, which reached 0.89, indicating excellent coding consistency. Discrepancies in coding and theme extraction were resolved through consensus discussion with a third senior qualitative researcher. Data collection was terminated when thematic saturation was achieved, defined as no new themes emerging in 2 consecutive interviews after the 10th participant.
This study ultimately interviewed 12 healthcare professionals (6 nurses, 6 physicians). Among them, 4 were male (33.33%) and 8 were female (66.67%), with an average age of (34.56 ± 4.87) years. Their average years of experience in home hospice care were (9.35 ± 5.14) years. Through data analysis, four themes related to outcome quality evaluation of home hospice care for older patients with terminal cancer were identified: symptoms and functional outcomes (effectiveness of physical symptom control and maintenance of activities of daily living), psychological and spiritual peace (improvement in negative emotions, acceptance of illness, and fear of death), family caregiving capacity and support systems (healthcare professionals’ support and education for families, accessibility of home care, and linkage with external resources), and dignity and compassionate care at the end of life (spiritual and humanistic support, and respect for end-of-life wishes). Based on the interview findings, “daily living skills” was added to the “physical harmony” dimension, “acceptance of death” to the “psychological harmony” dimension, “family support” to the “social harmony” dimension, and “spiritual solace and faith support” to the “spiritual harmony” dimension.
Finally, referencing the “Practice Guidelines for Hospice Care” issued by the National Health Commission of China,9 the research team integrated the main indicators derived from the literature review and qualitative interviews through group meetings and eliminated duplicate indicators. Meanwhile, the items were classified into four dimensions (first-level indicators) based on the theoretical framework of harmony nursing theory, which includes physical, psychological, social and spiritual harmony. A preliminary outcome quality evaluation indicator for home hospice care for older patients with terminal cancer was thus constructed, comprising 4 first-level indicators, 12 second-level indicators, and 44 third-level indicators.
Phase III: Refinement of Outcome Quality Evaluation Indicators for Home Hospice Care
The outcome quality evaluation indicators for home hospice care were refined through Delphi expert consultation and a pilot study. The Delphi method is a structured approach that achieves consensus on a specific topic through a series of questionnaires and expert evaluations.31 The key to the Delphi method lies in the judicious selection of experts, who should be representative and authoritative.32 Additionally, consideration must be given to the experts’ professional fields and geographic regions. The number of experts typically ranges from 15 to 30.33 Based on practical circumstances and available resources, 22 experts were selected for consultation between July and September 2025. Experts participating in this study must meet the following criteria: (1) Hold a bachelor’s degree or higher; (2) Possess an associate senior professional title or higher; (3) Have 10 or more years of experience in home hospice care, oncology clinical nursing and medical care, nursing administration, nursing education, or related fields; (4) Be willing to participate in the study and able to complete two rounds of correspondence questionnaires promptly.
This study employed Email and WeChat to distribute electronic Delphi expert questionnaires. Questionnaires were collected within two weeks of distribution, with Email or WeChat reminders sent to experts who did not respond by the deadline. The questionnaire comprised three sections: (1) Introduction: Briefly outlined the study’s purpose, content, consultation timeline, and contact information; (2) Consultation Content: Included indicator names, importance rating, and an “Expert Comments” section. A five-point Likert scale (5 = Extremely Important, 1 = Not Important) was used to rate the importance of each indicator. Experts were also required to modify, add, or delete content in the “Expert Comments” section and provide personal suggestions and opinions; (3) Expert Background Information: Included basic information, self‑assessment of familiarity with the content, and the basis for their judgments. After collecting the questionnaires, the research team analyzed and discussed the experts’ feedback. If any content in the returned questionnaires was unclear, the experts were contacted promptly. After each round of consultation, indicators were selected based on the following criteria: simultaneously meeting an importance mean > 3.50, a coefficient of variation (CV) < 0.25, and a perfect-score ratio > 0.20.34,35 The research team then added, deleted, or modified evaluation items to prepare the next round of questionnaires. The consultation process concluded when expert opinions reached substantial consensus. This study conducted two rounds of expert consultations.
Next, a small‑scale pilot test was conducted at the Linghe District Community Service Center in Jinzhou City, Liaoning Province, among older patients with terminal cancer receiving home hospice care (5 with gastric cancer, 5 with leukemia, 5 with pancreatic cancer, and 5 with colorectal cancer). This aimed to evaluate the linguistic expression of the outcome quality indicators. Throughout this process, all indicator statements were found to be clearly articulated and semantically complete, requiring no revisions. Thus, the outcome quality evaluation indicator for home hospice care in older patients with terminal cancer was established. The flow chart of this study is shown in Figure 1.
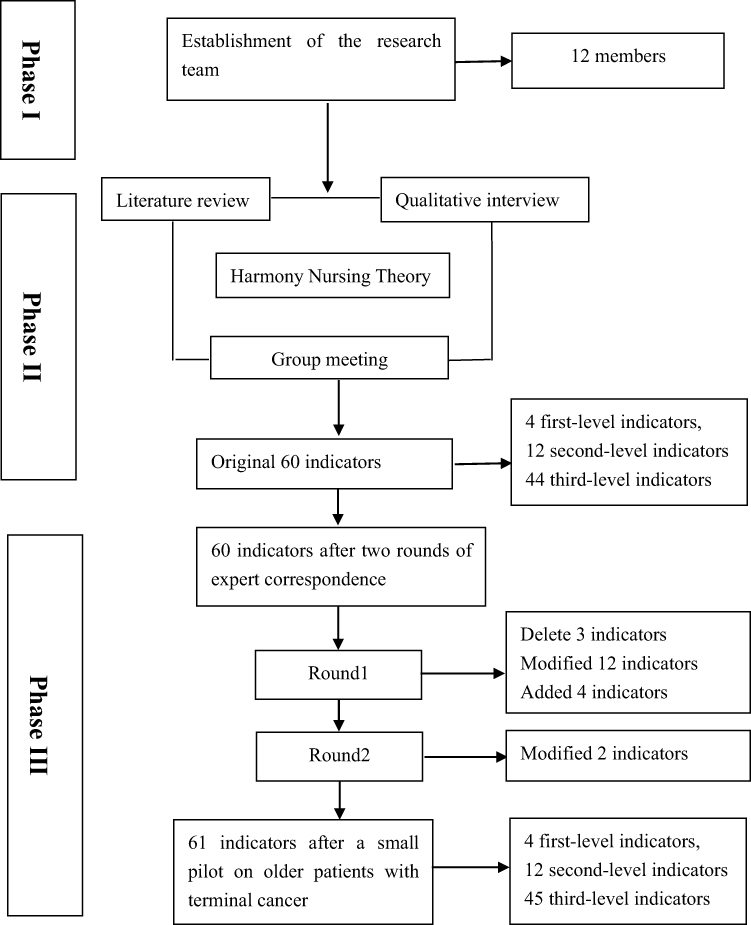 |
Figure 1 Flowchart of program construction for the outcome quality evaluation indicator in home hospice care. |
Data Statistics and Analysis
The collected data were double-checked and entered into Excel software, and SPSS 25.0 software was used for data analysis. In addition to the descriptive statistical analysis of experts’ general information, the results of the expert consultation evaluation were reflected by three indicators: expert positive coefficient, expert authority coefficient, and expert opinion coordination coefficient. (1) Experts’ general information: Including age, educational background, professional title, years of experience, whether they are a supervisor, and professional field, all expressed by frequency and percentage; (2) Expert positive degree: Reflected by the recovery rate of consultation questionnaires. Expert positive coefficient = Percentage of questionnaires returned to the total distributed questionnaires. A positive coefficient higher than 85% indicates that experts have good feedback on this consultation;36 (3) Expert authority degree: Expressed by the expert authority coefficient (Cr), calculated as Cr = (Ca + Cs)/2. A larger Cr value indicates a higher authority degree of experts. An expert authority degree of Cr ≥ 0.7 is acceptable.37 Among them, Ca is the experts’ judgment basis, which mainly includes four parts: theoretical analysis, practical experience, reference to domestic and foreign literature, and subjective judgment, and is quantitatively assigned according to the degree of their influence; Cs is the experts’ familiarity with the content of the consultation, which is specifically divided into 5 levels (very familiar, familiar, general, unfamiliar, and very unfamiliar); (4) Expert opinion coordination: Measured using the coefficient of variation (CV) and Kendall’s W.36 The coefficient of variation is calculated as the ratio of the standard deviation to the mean. Generally, a CV < 0.25 indicates minimal disagreement among experts regarding the item’s evaluation, signifying acceptable consistency in expert opinions. Kendal’s W ranges from 0 to 1, with higher values indicating greater expert agreement on the indicator content. Additionally, P < 0.05 must be satisfied for the results to be considered reliable.
Ethical Consideration
This study was provided by the School of Nursing, Jinzhou Medical University (NO: JZMULL2025348) and was conducted according to the tenets of the Declaration of Helsinki. Confirms that all experiments were performed in accordance with relevant named guidelines and regulations. Each recruited participant signed a written informed consent before participation.
Results
Expert Demographic Characteristics
In the first and second rounds of this study, a total of 22 experts were consulted, from Fujian (n=4), Harbin (n=5), Zhejiang (n=4), Beijing (n=5), and Anhui (n=4) provinces. The participants included chief physicians and head nurses from 8 hospitals, as well as professors and associate professors from 6 universities. In terms of age distribution, 13 experts (59.09%) were aged 45–55 years, 6 experts (27.27%) were aged 56–65 years, and 3 experts (13.64%) were 65 years or older. Regarding their professional fields, 4 experts (18.18%) specialized in home hospice care, 3 experts (13.64%) in geriatric nursing education, 6 experts (27.27%) in community oncology nursing, 4 experts (18.18%) in nursing administration, and 5 experts (22.73%) in community oncology medicine. Table 1 presents the detailed demographic characteristics of the experts.
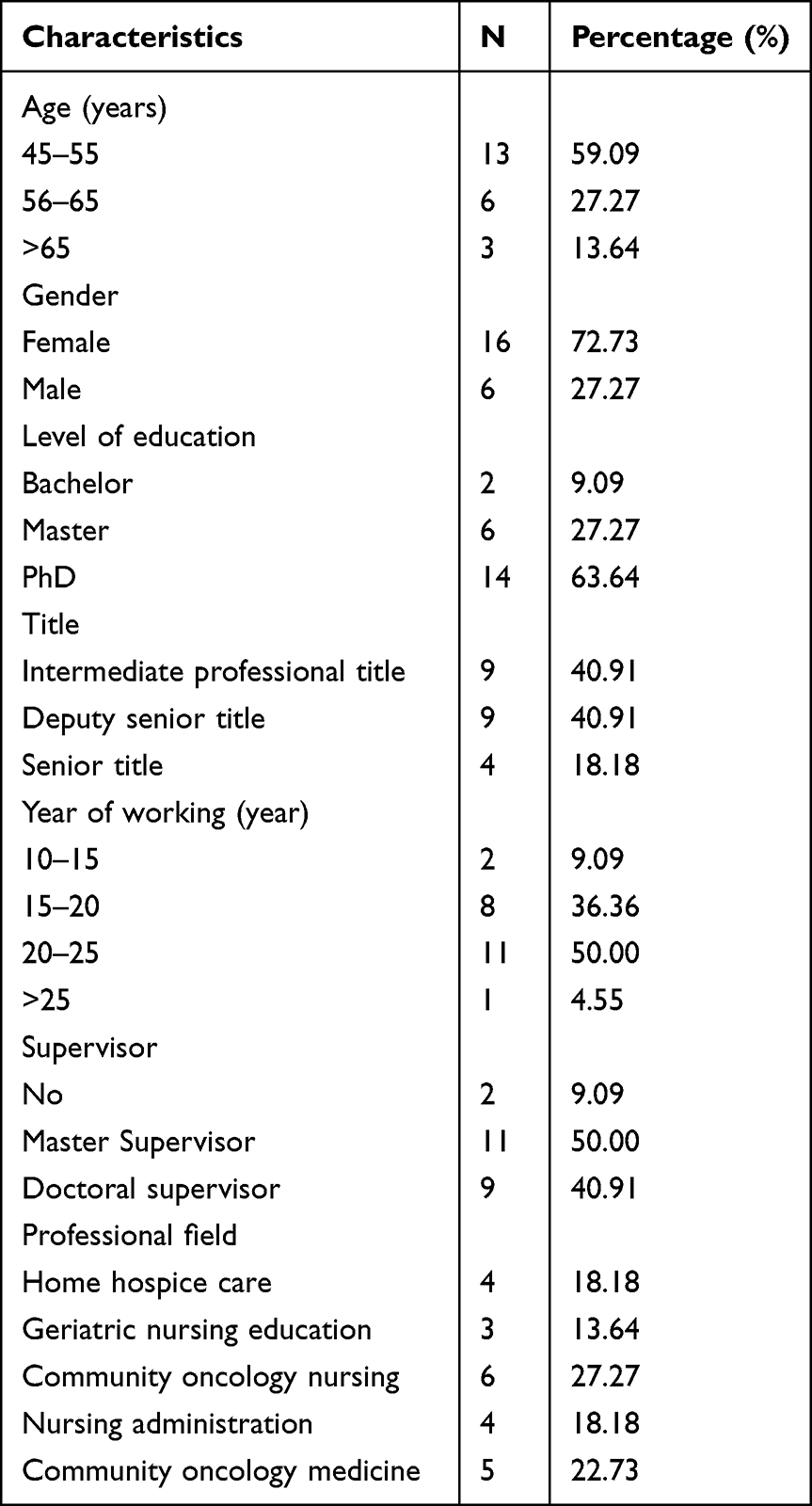 |
Table 1 Demographic Characteristics of Experts (n = 22) |
Modified Outcome Quality Evaluation Indicators for Home Hospice Care in Older Patients with Terminal Cance
Round 1
After the first round of the Delphi expert consultation, the mean importance score of the first-level indicators was 5, with a coefficient of variation (CV) of 0 and a perfect-score ratio of 1. The mean importance scores of the second-level indicators ranged from 4.59 to 5.00, with CVs ranging from 0.00 to 0.13 and perfect-score ratios ranging from 0.64 to 1. Among the third-level indicators, three indicators (1.2.3, 2.3.2, and 3.2.4) did not meet the retention criteria in terms of mean importance score, CV, and perfect-score ratio. The remaining third-level indicators had mean important scores ranging from 4.23 to 4.91, with CVs ranging from 0.06 to 0.18 and perfect-score ratios ranging from 0.401to 0.91. Subsequently, based on the experts’ suggestions, the wording of some second-level indicators was revised. First, experts considered that indicator 2.1 “Emotional state” was inadequately phrased, as it needed to cover both emotional outcomes and regulatory abilities; thus, it was revised to “Emotional state and adjustment”. Second, experts pointed out that the content under indicator 3.1 “Family support” included care collaboration outcomes among family members as well as between family members and healthcare providers, and suggested revising the item to “Family relationships and care coordination”. Finally, experts believed that the wording of indicator 4.3 “Interpersonal relationships” needed to be clearer, explicitly referring to relationship repair and the degree of completion of saying goodbye; therefore, the research team revised this item to “Repair of interpersonal relationships and emotional farewell”. Among the third-level indicators, experts also provided corresponding revision suggestions. For example, in indicator 1.1.7 “Family members can correctly administer medication and master non-drug intervention methods”, the phrase “under the guidance of healthcare staff” was added; in indicator 2.2.1 “Older patients can view their end-of-life conditions rationally”, it was revised to “Older patients can view the end of life within the scope of their cultural and personal beliefs”; in indicator 3.2.2 “Older patients can receive companionship and life assistance from volunteers or neighbors”, the phrase “when conditions permit” was added. Additionally, experts recommend adding four new indicators. Following the first round of consultation, three indicators were deleted, fifteen indicators were modified, and four indicators were added. A total of 4 first-level indicators, 12 second-level indicators, and 45 third-level indicators were identified. Table 2 lists the scores and modification details for each indicator during the first consultation round.
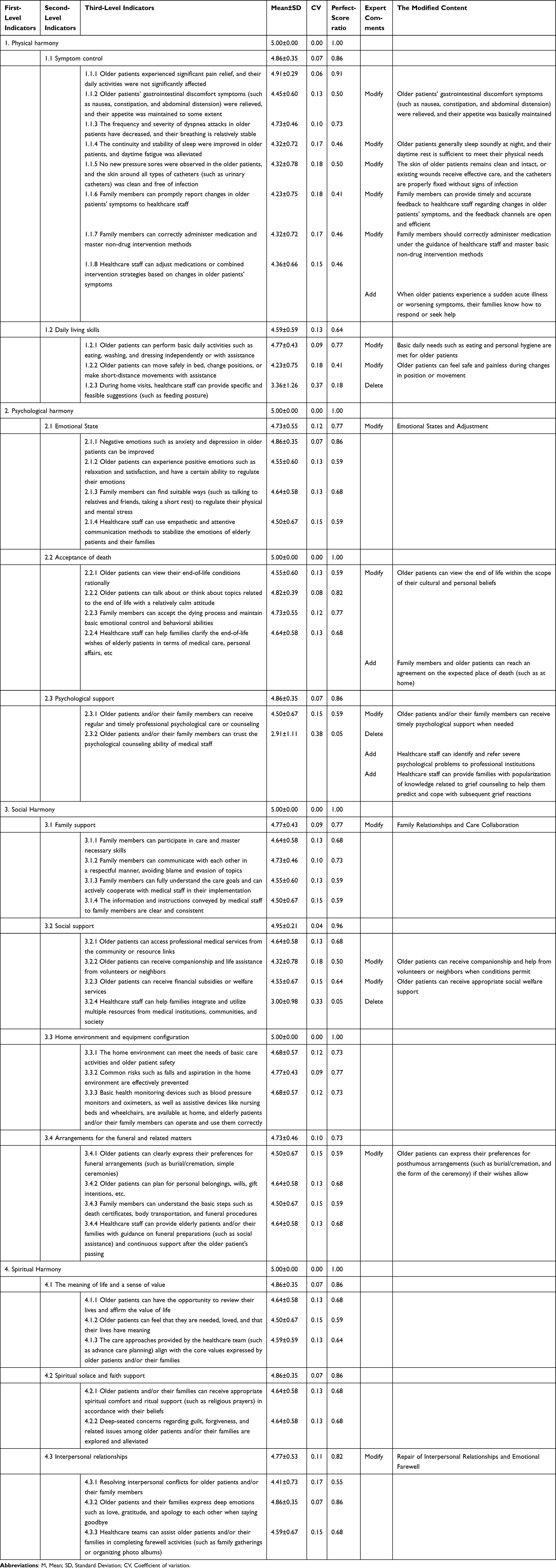 |
Table 2 The Outcome Quality Evaluation Indicator for Home Hospice Care in Older Patients with Terminal Cancer After Expert Consultation (First Round) |
Round 2
Experts did not mention the addition or deletion of indicators in the second round of expert consultation. They reached a consensus on the content, and the scores met the consensus standards. The mean importance score of first-level indicators ranged from 4.72 to 5.00, the coefficient of variation was between 0.06 and 0.18, and the perfect-score ratio was between 63.6% and 100%; the mean importance score of second-level indicators was 4.32 to 4.91, the coefficient of variation was between 0.05 and 0.20, and the perfect-score ratio was between 50.0% and 90.9%; the mean importance score of third-level indicators was 4.00 to 5.00, the coefficient of variation was between 0.00 and 0.20, and the perfect-score ratio was between 63.6% and 100%.
Six experts put forward suggestions for revising the specific contents under the third-level indicators. In indicator 2.2.4 “Healthcare staff can help families clarify the end-of-life wishes of elderly patients in terms of medical care, personal affairs, etc”, four experts believed that the scope of “personal affairs” was vague. In addition, two experts opined that indicator 4.2.1 “Older patients and/or their families can receive appropriate spiritual comfort and ritual support (such as religious prayers) in accordance with their beliefs” did not cover non-religious spiritual sustenance, resulting in a narrow scope of application. After the second round of consultation, the research team revised the above two indicators and finally formulated the outcome quality evaluation indicators for home hospice care in older Chinese patients with terminal cancer, which included 4 first-level indicators, 12 second-level indicators, and 45 third-level indicators (see Table 3).
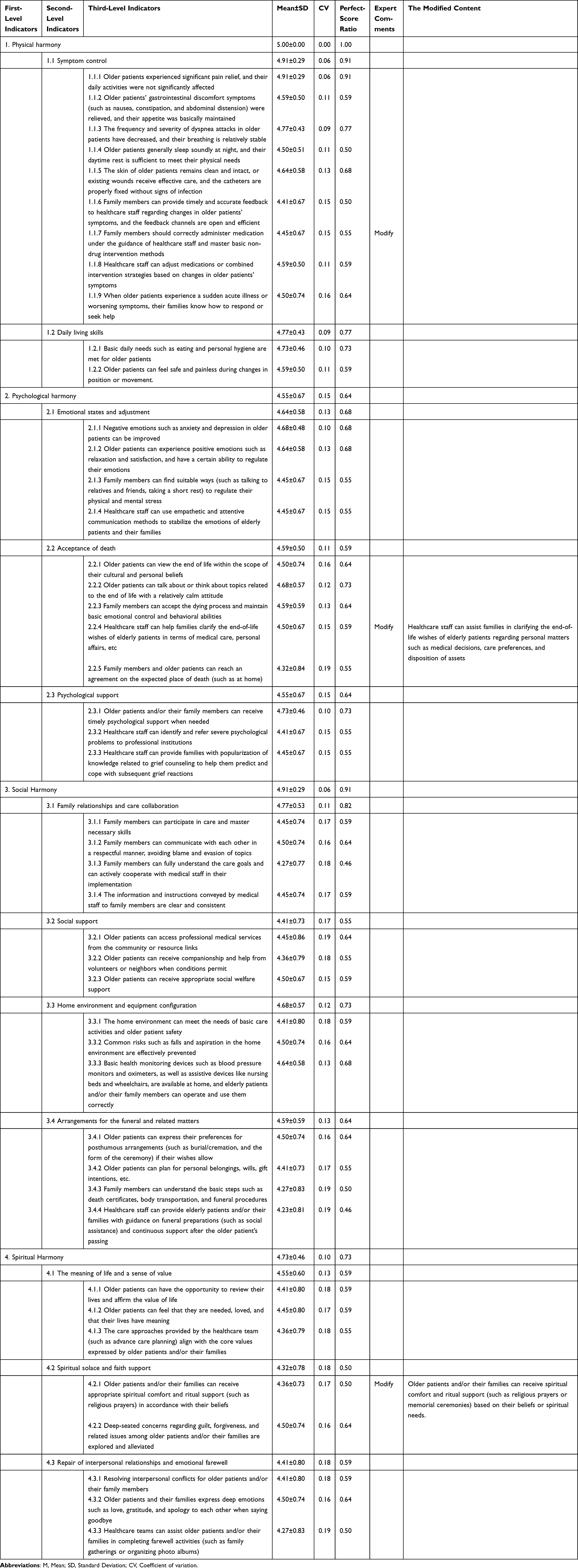 |
Table 3 The Outcome Quality Evaluation Indicator for Home Hospice Care in Older Patients with Terminal Cancer After Expert Consultation (Second Round) |
Authority of Experts and Coordination of Expert Opinions
In the first round of expert consultation in this study, a total of 24 questionnaires were distributed, and 22 valid questionnaires were recovered, with an effective recovery rate of 91.67%. 18 experts put forward suggestions, accounting for 81.82%. In the second round of expert consultation, a total of 22 questionnaires were distributed, and 22 valid questionnaires were recovered, with an effective recovery rate of 100%. 6 experts put forward suggestions, accounting for 27.27%. Overall, the effective response rate of experts was more than 85%, and the authority coefficient was 0.96 (≥0.7), indicating the authority of experts and the credibility of the Delphi method results. In addition, Kendall’s W values for the two rounds were 0.247 and 0.296, respectively, with both reaching statistical significance (P < 0.001). These values suggest a low-to-moderate level of agreement among experts, although the degree of consensus improved in the second round. Despite this, the Delphi process was terminated after two rounds because most indicators demonstrated stability between rounds, with only minor revisions required, and all items met the predefined retention criteria (eg., coefficient of variation < 0.25 and mean importance scores above the threshold). Therefore, further rounds were considered unlikely to produce substantial changes, and the current results were deemed sufficient to establish a consensus-based indicator set (see Table 4).
 |
Table 4 Expert Opinion Coordination Degree in Two Rounds of Delphi Consultation |
Discussion
This study developed a culturally adapted outcome quality evaluation indicator system for home hospice care in older patients with terminal cancer in China, grounded in the Harmony Nursing Theory. The final indicator system consists of 4 first-level indicators, 12 second-level indicators, and 45 third-level indicators, covering four core dimensions: physical harmony, psychological harmony, social harmony, and spiritual harmony. The system adopts a patient- and family-centered approach and uses a multi-source, multi-timepoint comprehensive assessment method, providing a practical tool for standardized quality evaluation of home hospice care services in the Chinese context.
The Harmony Nursing Theory adopted in this study aligns with the Chinese traditional cultural context and clinical practice, with its “harmony” and “coordination” mechanisms highly consistent with hospice care principles,29 essentially achieving normative-practice unity based on patient needs to attain the goal of “a comfortable and dignified death”.38 This study focuses on constructing patient- and family-centered outcome quality indicators, defined as measurable changes in patients’ or family caregivers’ health status, experience, or well-being resulting from home hospice care interventions. A small number of retained indicators phrased as healthcare provider capabilities are explicitly framed as valid proxy outcomes rather than process indicators. This approach is justified because: (1) many subjective end-of-life outcomes (eg., spiritual comfort) cannot be directly measured objectively; (2) healthcare providers’ standardized behaviors and competencies are the most reliable predictors of patient outcomes in home care settings; and (3) proxy indicators enable consistent evaluation across different care teams and settings.
To address the limitation of incomplete indicators from the literature review, this study conducted semi-structured interviews with community healthcare providers for qualitative exploration, extracting quality-influencing indicators from the supply-side perspective to effectively supplement prior literature findings. Furthermore, the Delphi method was employed to construct the indicator system, where expert selection is critical to results. Experts were selected from tertiary hospitals, community institutions, and medical universities across five provinces in China, covering clinical practice, nursing management, nursing education and hospice care, ensuring good representativeness. High authority coefficients in both rounds enhanced result reliability and persuasiveness. Questionnaire recovery rates were 91.7% and 100% respectively, indicating strong engagement and interest. Indicators met the inclusion criteria in both rounds, with Kendall’s coefficients passing significance tests, demonstrating good coordination and credible results. The research team rigorously double-checked data and analyzed opinions, resolving queries promptly to ensure integrity and accuracy, yielding 4 first-level indicators, 12 second-level indicators, and 45 third-level indicators. With the continuous development and advancement of hospice care, this indicator system can evaluate quality in home hospice care for terminal cancer older adults, and provide a reference for optimizing care plans, improving service processes, and enhancing quality management.39
In home hospice care, physical harmony extends beyond mere physiological health to a balanced state rooted in the Chinese cultural concept of “moderation”. Keratichewanun et al demonstrate that effective symptom management is essential for achieving a “good death”,40 aligning with this study’s prioritization of symptom management as the primary task in home hospice care, which received strong expert endorsement. Terminal older cancer patients often experience multiple symptoms due to disease progression and metastasis, including pain, dyspnea, and fatigue.41 Symptom management outcomes, measured by significant pain relief and minimal impact on daily activities, constitute the core component of outcome quality evaluation in home hospice care and are the most direct and critical indicators in numerous domestic and international tools.42,43 Thus, enhancing healthcare providers’ symptom management skills is a necessary process to achieve the patient outcome of reduced suffering and improved comfort. In this study, the highest-rated third-level indicator under “Symptom management” was “Older adult patients experienced significant pain relief, with daily activities minimally affected”. Pain, as one of the most prevalent terminal symptoms,44 is vital for ensuring quality in home hospice care for terminal older cancer patients. Given its high incidence, community providers should prioritize evidence-based personalized pain interventions to achieve this core patient outcome. Additionally, this study demonstrates that “Daily living skills maintenance” forms the core of home hospice care outcomes. Provision of fundamental care such as bathing, hair care, oral hygiene, and feeding assistance results in improved comfort and preserved dignity for terminal older adult cancer patients,45 with consistent recognition across cultural backgrounds among healthcare professionals.46
In the psychological harmony dimension, the second-level indicator “Emotional states and adjustment” serves as a key outcome quality indicator, directly reflecting the level of psychological relief and service effectiveness in terminal older cancer patients. This is consistent with Wittenberg-Lyles et al, who found that emotional adjustment in home hospice care—particularly through verbal support and positive expression from providers—effectively improves patient and family emotions, reducing anxiety and depression, and constitutes a core element for enhancing home care quality.47 A scoping review by Wu et al further indicated that psychological interventions targeting caregivers, such as training in emotional regulation skills, significantly reduce negative emotions and improve psychological adaptation, thereby supporting emotional adjustment as a standard outcome indicator48 This aligns with the highest-rated third-level indicator under “Psychological support” in this study, which is that “Older adult patients and/or their family members can receive timely psychological support when needed”. At the same time, the importance of “Acceptance of death” was unanimously affirmed by the experts. Assessing death acceptance allows for an understanding of how well patients’ needs are met in the final stage of life and their state at the time of death, thereby enabling an evaluation of hospice care quality. A systematic review on “good death” definitions emphasizes that acceptance of death is a core theme recognized by all stakeholders (patients, families, and providers), essential for outcome indicators.49 Multiple international hospice care quality evaluation tools, such as the Palliative Care Outcome Scale (POS) and Good Death Inventory (GDI),50,51 also incorporate death acceptance as a key component. Therefore, this study positions “Acceptance of death” as a second-level indicator for measuring hospice care outcome quality, refining its content into specific issues for older cancer patients before, during, and after death to enable quantitative evaluation of home hospice care quality and ongoing optimization of death outcomes.
The social harmony dimension comprises four second-level indicators, namely “Family relationships and care collaboration”, “Social support”, “Home environment and equipment configuration”, and “Arrangements for the funeral and related matters”. Among these, “Family relationships and care collaboration” and “Social support” received higher expert importance scores, indicating their significant influence on home hospice care quality evaluation. Rooted in Confucian culture emphasizing family and kinship, studies show that robust family and social support alleviate stress, grief, and depression when facing death.52 Hughes et al’s systematic review, which synthesized data from 34 included studies, confirms that family care collaboration and emotional support in hospice care directly improve symptom control and quality of life.53 Furthermore, Wang et al’s study in the integrated health and social care model further indicates that the quality of social relationships in terminal patients positively influences their perceived quality of hospice care services.54 Accordingly, community healthcare providers should comprehensively assess family and social support systems, encourage family involvement, and provide resource information, leveraging medical social workers and volunteers to build support networks. Grov et al’s qualitative study reveals that a safe and adaptable home environment (eg., quietness, cleanliness, ventilation, assistive devices) directly impacts cancer patients’ psychological stability and care quality outcomes,55 consistent with the high-rated third-level indicator in this study, which is that “Common risks such as falls and aspiration in the home environment are effectively prevented”. Literature also supports “Arrangements for the funeral and related matters” as a core “good death” factor, influencing terminal patient quality and family-perceived care outcomes.56 Thus, community healthcare providers are encouraged to proactively guide discussions on posthumous matters (eg., funeral preferences) and assist with body care and planning to ensure the patient outcome of a dignified death.
The spiritual dimension refers to an individual’s inner conscious experience of the meaning and value of existence,57 primarily manifested in the meaning of life, religious faith, harmony with nature, interpersonal relationships, and self-integration. It aligns closely with the three second-level indicators in this study (“The meaning of life and a sense of value”, “Spiritual solace and faith support”, and “Repair of interpersonal relationships and emotional farewell”). Steinhauser et al identified critical factors in end-of-life care from the perspectives of patients, families, and healthcare providers, emphasizing that life meaning and preparation are central to a “good death” and directly impact the overall quality of care for home cancer patients58 Additionally, Balboni et al further demonstrated that providing spiritual solace and faith support in the home setting significantly enhances patients’ inner peace and end-of-life satisfaction outcomes,59 thereby supporting its inclusion as an indicator of spiritual quality Similarly, Vuksanovic et al showed that facilitating the expression of final wishes and relationship repair (eg., emotional farewells) improves interpersonal reconciliation and sense of fulfillment among home patients, thereby elevating end-of-life quality.60 These three dimensions collectively reflect patients’ spiritual tranquility and integration, serving as critical components for evaluating the effectiveness of home hospice care services. Therefore, healthcare providers must understand patients’ wishes while respecting their religious beliefs and values during hospice care practice, fostering emotional connections and providing comprehensive spiritual care to achieve improved patient spiritual outcomes.
To ensure the practical usability of the indicator system, this study adopts a multi-source and multi-timepoint comprehensive assessment approach. In terms of assessment subjects, indicators of the physical harmony dimension are evaluated by primary care nurses; indicators of the psychological harmony dimension are mainly self-reported by patients, with caregiver proxy assessment for patients with impaired cognition; indicators of the social harmony dimension are jointly assessed by medical social workers and nurses; indicators of the spiritual harmony dimension are comprehensively determined by patient self-report and nurses. Three key assessment time points are set: baseline assessment is completed within 72 hours of patient enrollment in home hospice care, regular follow-up assessments are conducted every 2 weeks during the care period, final assessment is performed within 72 hours of patient death, and an additional bereavement follow-up assessment is conducted for family caregivers at 4 weeks post-death. All indicators are scored on a 5-point Likert scale, with 1 point representing a poor outcome and 5 points representing an excellent outcome. Regarding the length of the assessment tool and completion burden, the 45-item third-level indicator questionnaire has an average completion time of 3–5 minutes per dimension and a total completion time of 15–20 minutes. Considering that terminal older patients generally have reduced physical strength and attention span, we have adopted a flexible strategy of dimension-by-dimension assessment and phased completion, allowing patients to pause the assessment when feeling fatigued. For patients with severely impaired cognitive function or extremely poor physical status, proxy assessment by primary caregivers is implemented to minimize the impact of completion burden on response accuracy.
This study has several limitations. First, constrained by the current developmental stage of hospice care as a specialty, some experts participating in the Delphi consultation held only intermediate professional titles. Future research should broaden the expert selection pool to include more senior specialists, thereby enabling further revision and optimization of the evaluation indicator system. Second, the study constructed the content for evaluating outcome quality in home hospice care solely through interviews with community healthcare providers, adopting a supply-side perspective and omitting the needs and experiences of patients and their families. Subsequent studies are recommended to incorporate the perspectives of terminal older cancer patients and their families to further enrich and refine the indicator system, particularly by validating the proxy outcome indicators against direct patient-reported outcomes. Finally, due to time constraints, the indicator system developed in this study has not yet undergone empirical validation, and its reliability and validity remain to be confirmed. Future investigations should conduct multi-center, large-sample clinical application studies to verify its effectiveness and maximize its practical utility.
Conclusion
This study, grounded in Harmony Nursing Theory, developed a consensus-based and culturally adapted set of outcome quality evaluation indicators for home hospice care in older Chinese patients with terminal cancer. By integrating evidence from a literature review, qualitative interviews with community healthcare providers, and two rounds of Delphi expert consultation, the resulting indicator system comprises four first-level indicators (physical harmony, psychological harmony, social harmony, and spiritual harmony), 12 second-level indicators, and 45 third-level indicators. The framework incorporates key Chinese cultural elements, such as “family relationships and care collaboration”, and provides a preliminary reference framework for assessing and improving the quality of home hospice care. It may support the optimization of nursing practices, promote end-of-life dignity, and contribute to addressing challenges related to population aging and the increasing cancer burden. Further empirical validation is warranted to assess its reliability and applicability in diverse clinical settings.
Acknowledgment
We are very grateful to the community healthcare workers who participated in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang X, Huang Z, Xu T, Li Y, Qin X. Exploring the future design approach to ageing based on the double diamond model. Systems. 2023;11(8):404. doi:10.3390/systems11080404
2. Kiniorska I, Brambert P, Kamińska W, Kopacz-Wyrwał I. Aging of the society: the European perspective. Bull Geograph Socio-Econ Series. 2023;81–24. doi:10.12775/bgss-2023-0017
3. Chen C, Lai X, Xu A, Yang S, Jin J, Yang H. The decision for hospice care in patients with terminal illness in Shanghai: a mixed-method study. Int J Nurs Sci. 2022;9(1):71–78. doi:10.1016/j.ijnss.2021.12.002
4. Kalita M, D M, Saha I, Chakrabarti A. Global burden of cancer pattern in 2020 & prediction to 2040 among older adults. Indian J Med Res. 2024;160:397–406. doi:10.25259/ijmr_1729_23
5. Miller K, Nogueira L, Mariotto A, et al. Cancer treatment and survivorship statistics, 2019. Ca a Cancer J Clin. 2019;69.
6. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Center. 2024;4:47–53. doi:10.1016/j.jncc.2024.01.006
7. Demb J, Kolb J, Dounel J, et al. Red flag signs and symptoms for patients with early-onset colorectal cancer. JAMA Network Open. 2024;7:e2413157. doi:10.1001/jamanetworkopen.2024.13157
8. Zimolzak A, Kapadia P, Upadhyay D, et al. Frequent missed opportunities for earlier diagnosis of advanced-stage colorectal or lung cancer. JAMA Intern Med. 2025;185:1102. doi:10.1001/jamainternmed.2025.2875
9. Podbury B, Gurgenci T, Huggett G, Greer R, Hardy J, Good P. Psychological distress and physical symptoms in advanced cancer: cross-sectional study. BMJ Support Palliat Care. 2024;15:827–830. doi:10.1136/spcare-2024-004940
10. Yan Y, Zhang H, Gao W, et al. Current awareness of palliative care in China. Lancet Glob Health. 2020;8:3. doi:10.1016/S2214-109X(20)30006-1
11. Lu Y, Yu W, Zhang J, Li R. Advancements in hospice and palliative care in China: a five-year review. Asia Pac J Oncol Nurs. 2024;11.
12. Lu Y, Gu Y, Yu W. Hospice and palliative care in China: development and challenges. Asia Pac J Oncol Nurs. 2018;5:26–32. doi:10.4103/apjon.apjon_72_17
13. Dong Y, Chen M, Yu Y, et al. Construction of a palliative care services framework for end‐of‐life adult patients at medical institutions: a Delphi study. Eur J Cancer Care. 2025;2025. doi:10.1155/ecc/9034166
14. De Lima Costa VG, Rizzo AFR, De Oliveira Souza É, et al. The role of the multidisciplinary team in decision-making at the end of life: an analysis of integrated palliative care management. CONTRIBUCIONES A LAS CIENCIAS SOCIALES. 2024.
15. Lekhan V. Retrospective analysis of the construction of the national system of hospice and palliative care in Great Britain. Inter Collegas. 2024;11:52–56. doi:10.35339/ic.11.1.lvm
16. Sugar K, McCabe C, Llewellyn A, et al. Implementation of a hospice community service redesign: qualitative research identifying lessons learned. Palliat Care Social Pract. 2025;19. doi:10.1177/26323524251349839
17. Freeman S, Flood D, Banner D, et al. A holistic approach to supporting death in the home: implementation of a home hospice program in a northern community–A study protocol. PLoS One. 2024;19.
18. Sakitani M. Substantial shift in palliative care from hospice to community and its integration into community-based primary health care. J Med Clin Res Rev. 2023;7. doi:10.33425/2639-944X.1344
19. Cheng Q, Duan Y, Zheng H, et al. Knowledge, attitudes and preferences of palliative and end-of-life care among patients with cancer in mainland China: a cross-sectional study. BMJ open. 2021;11.
20. Zhang H, Diao H-X, Wang -Q-Q. Enhancing the quality of hospice shared care for end-stage malignant tumor patients: a structure-process-outcome three-dimensional quality evaluation model. Am J Hospice Palliat Care. 2025;10499091251343216.
21. Kan Y, Xiao Y, Li Z, Chen Z, Yue P. Quality indicators for home-based palliative care: a systematic review. J Pain Sympt Manage. 2025;70:e213–e227. doi:10.1016/j.jpainsymman.2025.06.011
22. Masaki H, Kawai N, Matsumoto K, et al. Consensus development of quality indicators for end-of-life care for elders in Japan. Int J Nurs Pract. 2017;23(Suppl 1). doi:10.1111/ijn.12562
23. Harman L, Guthrie D, Cohen J, et al. Potential quality indicators for seriously ill home care clients: a cross-sectional analysis using Resident Assessment Instrument for Home Care (RAI-HC) data for Ontario. BMC Palliat Care. 2019;18:18. doi:10.1186/s12904-019-0401-1
24. Dahlin C. National consensus project for quality palliative care. Oxford Textbook Palliat Nurs. 2019.
25. Hongju Y, Xiaowen Y, Zhaoxia Y, Chunying Z. Developing the nursing services quality indicator system of hospice care for cancer patients. Chin J Nurs. 2018;53(12):1487–1491.
26. Zeng A, Gu Y, Ma L, et al. Development of quality indicators for the ultrasound department through a modified Delphi method. Diagnostics. 2023;13.
27. Poirier T, Devraj R. Pharmacy in an improved health care delivery model using Maslow’s hierarchy of needs. Am J Pharm Educ. 2019;83.
28. Smith B. Psychology for Nursing and healthcare professionals: developing compassionate care. Journal of Perioperative Practice. 2018;28:138. doi:10.1177/1750458918755969
29. Li Z, Liu HP, Kang XF, Li Y, Li XH. Development of harmony nursing theory based on Confucianism and Daoism beliefs. Chin J Nurs. 2016;51(9):1034–1038.
30. Zuo T, Yeap SY, Lu G. Navigating the delicate balance of autonomy and harmony: a case study on the cultural adaptation of palliative care interventions in China. BMC Palliat Care. 2025;24.
31. Devaney L, Henchion M. Who is a Delphi ‘expert’? Reflections on a bioeconomy expert selection procedure from Ireland. Futures. 2018;99:45–55. doi:10.1016/j.futures.2018.03.017
32. Okoli C, Pawlowski S. The Delphi method as a research tool: an example, design considerations and applications. Inf Manag. 2004;42:15–29. doi:10.1016/j.im.2003.11.002
33. McPherson S, Reese C, Wendler M, Wendler M. Methodology update: Delphi studies. Nurs Res. 2018;67:404. doi:10.1097/NNR.0000000000000297
34. Czúcz B, Keith H, Maes J, et al. Selection criteria for ecosystem condition indicators. Ecol Indic. 2021;133:108376. doi:10.1016/j.ecolind.2021.108376
35. Yan W, Limei S, Yanbo J, Yujie X, Shengxia L, Ruirui Z. Construction of comprehensive quality of evaluation index system about palliative care in general hospitals based on the structure-process-outcome quality model. Chin J Practl Nurs. 2022;38(5):360–364.
36. Xin T, Ding X, Gao H, Li C, Jiang Y, Chen X. Using Delphi method to develop Chinese women’s cervical cancer screening intention scale based on planned behavior theory. BMC Women’s Health. 2022;22(1):512. doi:10.1186/s12905-022-02113-1
37. De Schreye R, Houttekier D, Deliens L, Cohen J. Developing indicators of appropriate and inappropriate end-of-life care in people with Alzheimer’s disease, cancer or chronic obstructive pulmonary disease for population-level administrative databases: a RAND/UCLA appropriateness study. Palliat Med. 2017;31(10):932–945. doi:10.1177/0269216317705099
38. Mousazadeh N, Rakhshan M. Dignified death: a concept analysis and implications for nursing. Fam Med Primary Care Rev. 2022;24:146–150. doi:10.5114/fmpcr.2021.110362
39. Patel D, Patel P, Ramani M, Makadia K. Exploring perception of terminally ill cancer patients about the quality of life in hospice based and home based palliative care: a mixed method study. Indian J Palliat Care. 2023;29:57–63. doi:10.25259/IJPC_92_2021
40. Keratichewanun P, Dejkriengkraikul N, Angkurawaranon C, et al. Stakeholders’ perspectives of a good death: a qualitative study from Thailand. Heliyon. 2023;9:e15775. doi:10.1016/j.heliyon.2023.e15775
41. Henson L, Maddocks M, Evans C, Davidson M, Hicks S, Higginson I. Palliative care and the management of common distressing symptoms in advanced cancer: pain, breathlessness, nausea and vomiting, and fatigue. J clin oncol. 2020;38:905–914. doi:10.1200/JCO.19.00470
42. Valero-Cantero I, Casals C, Espinar-Toledo M, Barón-López FJ, Martínez-Valero FJ, Vázquez-Sánchez MÁ. Cancer patients’ satisfaction with in-home palliative care and its impact on disease symptoms. Healthcare. 2023;11(9):1272. doi:10.3390/healthcare11091272
43. Victora CG, Matijasevich A, Silveira M, Santos I, Barros AJ, Barros FC. Socio-economic and ethnic group inequities in antenatal care quality in the public and private sector in Brazil. Health Policy Plan. 2010;25(4):253–261. doi:10.1093/heapol/czp065
44. Khojayeva K, Aubakirova M, Viderman D. Advanced pain management in patients with terminal cancer. Curr Med Chem. 2025;32. doi:10.2174/0109298673333227250106085952
45. Tamdin T, Bhandari S, Bhandari S, Barbery M, Bajwa R. Barriers to timely transitions to comfort care in cancer patients: a review. Ann Med Surg. 2025;87:5770–5774. doi:10.1097/MS9.0000000000003618
46. Castelo-Loureiro A, Perez-De-Acha A, Torres-Pérez A, et al. Delivering palliative and supportive care for older adults with cancer: interactions between palliative medicine and geriatrics. Cancers. 2023;16:15. doi:10.3390/cancers16010015
47. Wittenberg-Lyles E, Goldsmith J, Oliver DP, Demiris G, Kruse RL, Van Stee S. Exploring oral literacy in communication with hospice caregivers. J Pain Sympt Manage. 2013;46(5):731–736. doi:10.1016/j.jpainsymman.2012.11.006
48. Wu H, Dong P, Chai Y, Huang P, Huang H. Psychological distress interventions for family members in palliative care: a scoping review. BMC Palliat Care. 2025;24(1):230. doi:10.1186/s12904-025-01873-5
49. Esmaeili-Abdar M. Analyzing the concepts of “good death” from the perspective of nursing: a systematic review and concept analysis. Elect Phys. 2022;14:7898–7910. doi:10.26415/2008-5842-vol14iss2p7898-7910
50. Ostan R, Gambino G, Franchini L, et al. Assessment and monitoring by integrated palliative care outcome scale: an observational study on cancer patients at home. Support Care Cancer. 2025;34:33. doi:10.1007/s00520-025-10215-3
51. Miyashita M, Morita T, Sato K, Hirai K, Shima Y, Uchitomi Y. Good death inventory: a measure for evaluating good death from the bereaved family member’s perspective. J Pain Sympt Manage. 2008;35(5):486–498. doi:10.1016/j.jpainsymman.2007.07.009
52. Chen R. Social support as a protective factor against the effect of grief reactions on depression for bereaved single older adults. Death Studies. 2020;46:756–763. doi:10.1080/07481187.2020.1774943
53. Hughes NM, Noyes J, Eckley L, Pritchard T. What do patients and family-caregivers value from hospice care? A systematic mixed studies review. BMC Palliat Care. 2019;18(1):18.
54. Zhang W, He X, Liu Z. Factors and mechanism influencing client experience of residential integrated health and social care for older people: a qualitative model in Chinese institutional settings. Int J Environ Res Public Health. 2023;20(5):4638. doi:10.3390/ijerph20054638
55. Grov EK, Ytrehus S. Do You Feel Safe at Home? A Qualitative Study among Home-Dwelling Older Adults with Advanced Incurable Cancer. Healthcare. 2022;10(12):2384. doi:10.3390/healthcare10122384
56. Liang H-J, Xiong Q, Lin P-C, Tsai J-H, Preston N. ‘A good ending but not the end’: exploring family preparations surrounding a relative’s death and the Afterlife – a qualitative study. Palliat Med. 2024;38:1184–1193. doi:10.1177/02692163241280016
57. Ko I, Choi S, Kim JS. Evolutionary Concept Analysis of Spirituality. J Korean Acad Nurs. 2017;47(2):242–256. doi:10.4040/jkan.2017.47.2.242
58. Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284(19):2476–2482. doi:10.1001/jama.284.19.2476
59. Balboni TA, Paulk ME, Balboni MJ, et al. Provision of spiritual care to patients with advanced cancer: associations with medical care and quality of life near death. J Clin Oncol. 2010;28(3):445–452. doi:10.1200/JCO.2009.24.8005
60. Vuksanovic D, Green H, Morrissey S, Smith S. Dignity therapy and life review for palliative care patients: a qualitative study. J Pain Sympt Manage. 2017;54(4):530–537.e531. doi:10.1016/j.jpainsymman.2017.07.016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.