Back to Journals » International Journal of Women's Health » Volume 18
Construction and Validation of a Prediction Model for Conversion to Cesarean Section in Primiparous Women Receiving Epidural Labor Analgesia: A Retrospective Cohort Study
Received 5 March 2026
Accepted for publication 19 May 2026
Published 3 June 2026 Volume 2026:18 607220
DOI https://doi.org/10.2147/IJWH.S607220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Xingyu Huang,1 Jiao Hua2
1Department of Obstetrics, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi People’s Hospital, Wuxi Medical Center, Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China; 2Department of Nursing, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
Correspondence: Jiao Hua, Department of Nursing, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: To develop and validate a clinical prediction model for intrapartum conversion to cesarean section in primiparous women receiving epidural labor analgesia.
Patients and Methods: This retrospective cohort study included 1020 primiparous women who received epidural labor analgesia at a tertiary hospital in Wuxi, China. The model was developed to estimate cesarean conversion risk within this specific clinical cohort. Participants who delivered between March and December 2023 comprised the training cohort, whereas those who delivered between January and March 2024 comprised the validation cohort. Maternal, fetal, and intrapartum variables were extracted from electronic medical records, anesthesia records, and intrapartum fetal monitoring systems. A multivariable logistic regression model was developed to predict conversion to cesarean section, and a nomogram was constructed based on the final model. Model discrimination and calibration were assessed using the area under the receiver operating characteristic curve (AUC), the Hosmer–Lemeshow test, and calibration plots. Clinical utility was evaluated using decision curve analysis.
Results: The rate of conversion to cesarean section was 15.9% in the training cohort and 15.3% in the validation cohort. Six variables were identified as independent predictors of cesarean conversion: maternal age, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor. The prediction model showed good discrimination, with an AUC of 0.810 (sensitivity 0.822, specificity 0.606) in the training cohort. In the validation cohort, the AUC was 0.763 (sensitivity 0.786, specificity 0.592), indicating consistent predictive performance.
Conclusion: This prediction model provides reliable risk estimation for conversion to cesarean section within a specific cohort of primiparous women receiving epidural labor analgesia. It may support early intrapartum risk stratification and individualized clinical decision-making. Further multicenter studies are warranted to assess its generalizability.
Keywords: prediction model, cesarean section, epidural labor analgesia, primiparous women, intrapartum risk
Introduction
Labor pain is widely recognized as one of the most intense forms of physical discomfort experienced by women.1 Effective pain management is therefore a critical component of obstetric care during childbirth. With advancements in medical technology and a growing emphasis on comfort-oriented maternity services, the use of labor analgesia has become increasingly common.2 Among all analgesic techniques, epidural analgesia is considered the most effective for relieving labor pain and is regarded as the gold standard for comparison with other methods.3
Despite its advantages in labor pain relief, some women receiving epidural labor analgesia may still require cesarean delivery during labor, and timely risk assessment remains important for intrapartum management.4,5 Primiparous women are particularly vulnerable because they often have a longer first stage of labor due to an undilated birth canal and the absence of prior delivery experience. As a result, they have a higher likelihood of cesarean section compared with multiparous women.6–8 Managing labor progression in primiparous women therefore remains a significant clinical challenge.
Developing reliable prediction models is essential to help clinicians identify primiparous women at increased risk of intrapartum cesarean conversion at an early stage.9 However, most previous studies have focused on the effects and complications of epidural analgesia.10,11 Although several factors associated with intrapartum cesarean delivery have been reported, clinically applicable prediction models for primiparous women receiving epidural labor analgesia remain limited.12,13 Primiparous women receiving epidural labor analgesia constitute a specific intrapartum population in whom early risk stratification is clinically important. Because labor progression and fetal status may change dynamically after analgesia initiation, a prediction model incorporating routinely collected intrapartum variables may support timely monitoring, multidisciplinary communication, and individualized intrapartum management.
In this study, we developed and validated a prediction model using routinely collected maternal, fetal, and intrapartum variables to estimate the risk of cesarean conversion among primiparous women receiving epidural labor analgesia. This model was developed to support risk assessment in this specific population and to facilitate early warning, multidisciplinary communication, and individualized intrapartum management.
Materials and Methods
Study Design and Participants
This retrospective cohort study was conducted in the delivery room of a tertiary hospital in Wuxi, Jiangsu Province, China. Clinical data were obtained from electronic medical records, anesthesia records, and intrapartum fetal monitoring systems. Eligible primiparous women who received epidural labor analgesia between March 2023 and March 2024 were retrospectively identified, and relevant clinical data were extracted in 2025 for analysis. Participants who delivered between March 2023 and December 2023 were included in the training cohort, whereas those who delivered between January 2024 and March 2024 were included in the validation cohort. The study protocol was reviewed and approved by the Research Ethics Committee of Wuxi People’s Hospital (approval No. KY25157). Given the retrospective nature of the study and the use of routinely collected clinical data, the requirement for informed consent was waived by the ethics committee. All data were anonymized/de-identified before analysis. The study was conducted in accordance with the Declaration of Helsinki.
Inclusion criteria: (1) Gestational age ≥ 37 weeks with a full-term, singleton pregnancy in cephalic presentation; (2) Maternal age ≥ 20 years; (3) Eligibility for a vaginal trial of labor; (4) Willingness to undergo a trial of labor, either with spontaneous onset or following labor induction; (5) Category I fetal heart rate tracing before analgesia, defined according to the National Institute of Child Health and Human Development (NICHD) guidelines as a baseline of 110 to 160 bpm with moderate variability and no late or variable decelerations;14 (6) Baseline maternal body temperature < 37.5°C.
Exclusion criteria: (1) Preterm birth; (2) Multiple pregnancies; (3) Severe maternal comorbidities that contraindicate vaginal delivery; (4) Previous cesarean section or uterine scarring; (5) Psychiatric disorders or inability to cooperate with the research procedures.
Outcome Definition
The primary outcome was first-stage intrapartum obstetric conversion to cesarean section after initiation of epidural labor analgesia. This outcome referred to cesarean delivery performed during the first stage of labor after a planned trial of vaginal delivery. The timing and clinical indications of cesarean delivery were confirmed by reviewing delivery records and operative records. In the original dataset, all cesarean conversions occurred during the first stage of labor, and no second-stage cesarean conversion was identified. The cesarean indications were obstetric in nature and mainly included relative cephalopelvic disproportion, persistent occiput posterior position, non-reassuring fetal heart rate status or suspected acute fetal compromise, and other obstetric indications.
Anesthesia records were also reviewed to identify serious anesthesia-related adverse events, including high or total neuraxial block, local anesthetic systemic toxicity, and severe hypotension. According to the available anesthesia, delivery, and operative records, no cesarean delivery was documented as being directly caused by these serious anesthesia-related complications. Therefore, the outcome in this study primarily represented obstetric cesarean conversion during the first stage of labor rather than cesarean delivery directly attributed to anesthesia-related complications.
Variables and Definitions
Based on a comprehensive literature review, expert consultation, and clinical considerations, we identified a set of maternal, fetal, and intrapartum variables with potential relevance to intrapartum cesarean conversion among primiparous women receiving epidural labor analgesia.15,16 Thirteen candidate predictors were included in this study: maternal age, height, BMI, gestational age, estimated fetal weight, cervical dilation at epidural placement, duration of epidural labor analgesia, intrapartum temperature, pregnancy complications (hypertension, diabetes, or hypothyroidism), amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor. All variables were extracted from electronic medical records, anesthesia documentation, and intrapartum fetal monitoring records. Fetal heart rate status referred to intrapartum fetal heart rate status after initiation of epidural labor analgesia and was classified according to NICHD criteria.14 Category I fetal heart rate tracings were defined as normal, whereas Category II or III tracings during labor were grouped as non-normal fetal heart rate status for analysis. Amniotic fluid characteristics were categorized as clear or meconium-stained based on delivery records and intrapartum clinical documentation. A detailed description of each variable and its coding is provided in Table 1.
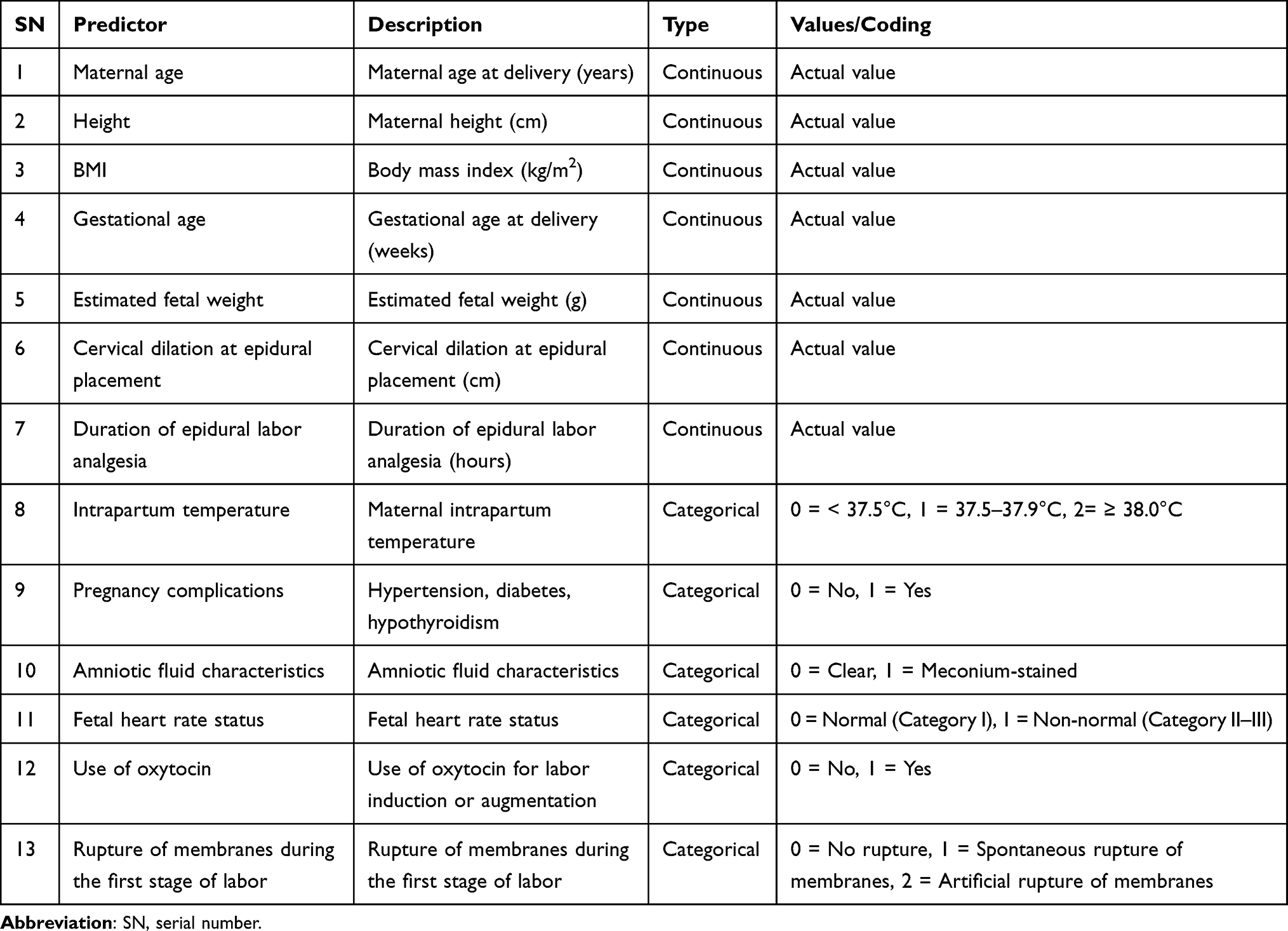 |
Table 1 Description of the Study Variables |
Epidural Analgesia Method
All parturients received epidural labor analgesia using programmed intermittent epidural bolus (PIEB) technology combined with a patient-controlled epidural analgesia (PCEA) mode. The analgesic solution consisted of 150 mg of ropivacaine and 50 µg of sufentanil. The PIEB pump was programmed to deliver an 8–12 mL bolus every 45 minutes, while the PCEA mode allowed an additional 8–10 mL per self-administered dose with a lockout interval of 15–30 minutes.
Sample Size Calculation
The prediction model included 13 independent variables. For logistic regression models, the required sample size is commonly estimated as five to ten times the number of predictors. Given that the model included 13 variables and the incidence of intrapartum cesarean conversion among women receiving epidural labor analgesia is approximately 18%,17 the minimum required sample size was estimated to be at least 803 participants after accounting for an expected 10–20% sample loss. According to the recommended 4 to 1 sample size ratio between the training and validation cohorts,18 the validation cohort required at least 161 participants. Ultimately, 850 primiparous women receiving epidural labor analgesia were enrolled in the training cohort from March 2023 to December 2023, and 170 women were enrolled in the validation cohort from January 2024 to March 2024 (Figure 1).
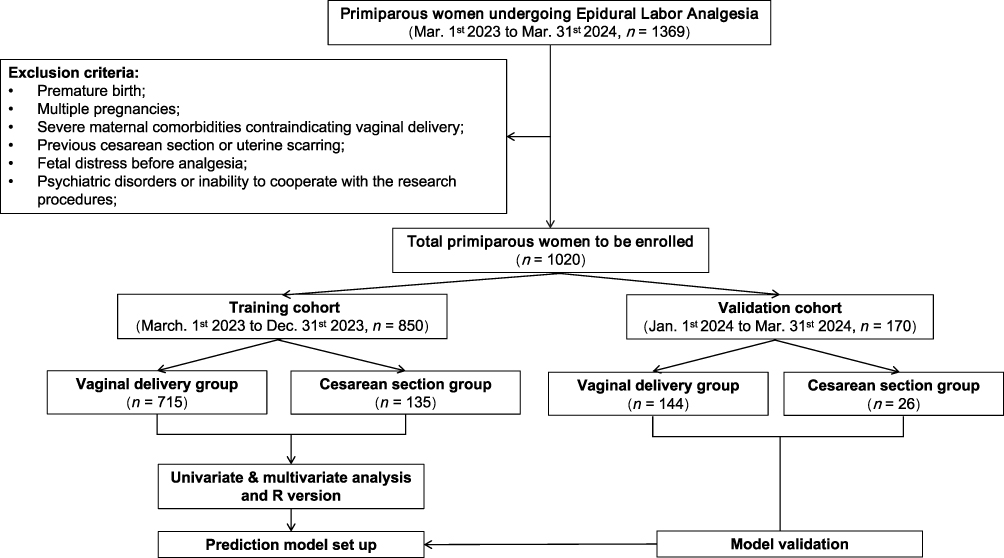 |
Figure 1 Study flow diagram. |
Statistical Analysis
Data were processed and analyzed using SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA) and R software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were summarized as frequencies and percentages (%), and group comparisons were performed using the χ2 test. Continuous variables with a normal distribution were expressed as mean ± standard deviation (SD), and differences between groups were assessed using the independent samples t-test.
All 13 candidate predictors were first evaluated using univariate analysis. Variables with P < 0.05 in the univariate analysis were then assessed for multicollinearity using variance inflation factors (VIFs). Variables without evidence of multicollinearity were included in the multivariable logistic regression model to identify independent predictors and construct the final prediction model. Based on the final multivariable logistic regression model, a nomogram was constructed to provide an intuitive graphical representation of the prediction model for individualized risk estimation. Model discrimination was evaluated using the receiver operating characteristic (ROC) curve, and calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test.
Validation was subsequently performed. A calibration curve was generated to assess the agreement between predicted and observed probabilities. Decision curve analysis (DCA) was used to quantify the net clinical benefit of the prediction model across a range of threshold probabilities. All statistical tests were two-sided, and a P < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Training and Validation Cohorts
Baseline characteristics of the training and validation cohorts are presented in Table 2. The two cohorts were comparable in maternal age, height, body mass index, gestational age, estimated fetal weight, fetal heart rate status, use of oxytocin, and amniotic fluid characteristics (P > 0.05). Differences were observed in intrapartum temperature distribution and pregnancy complications (P < 0.05). The duration of epidural labor analgesia also differed between the cohorts (P = 0.013), whereas the distribution of rupture of membranes during the first stage of labor did not differ significantly (P = 0.095).
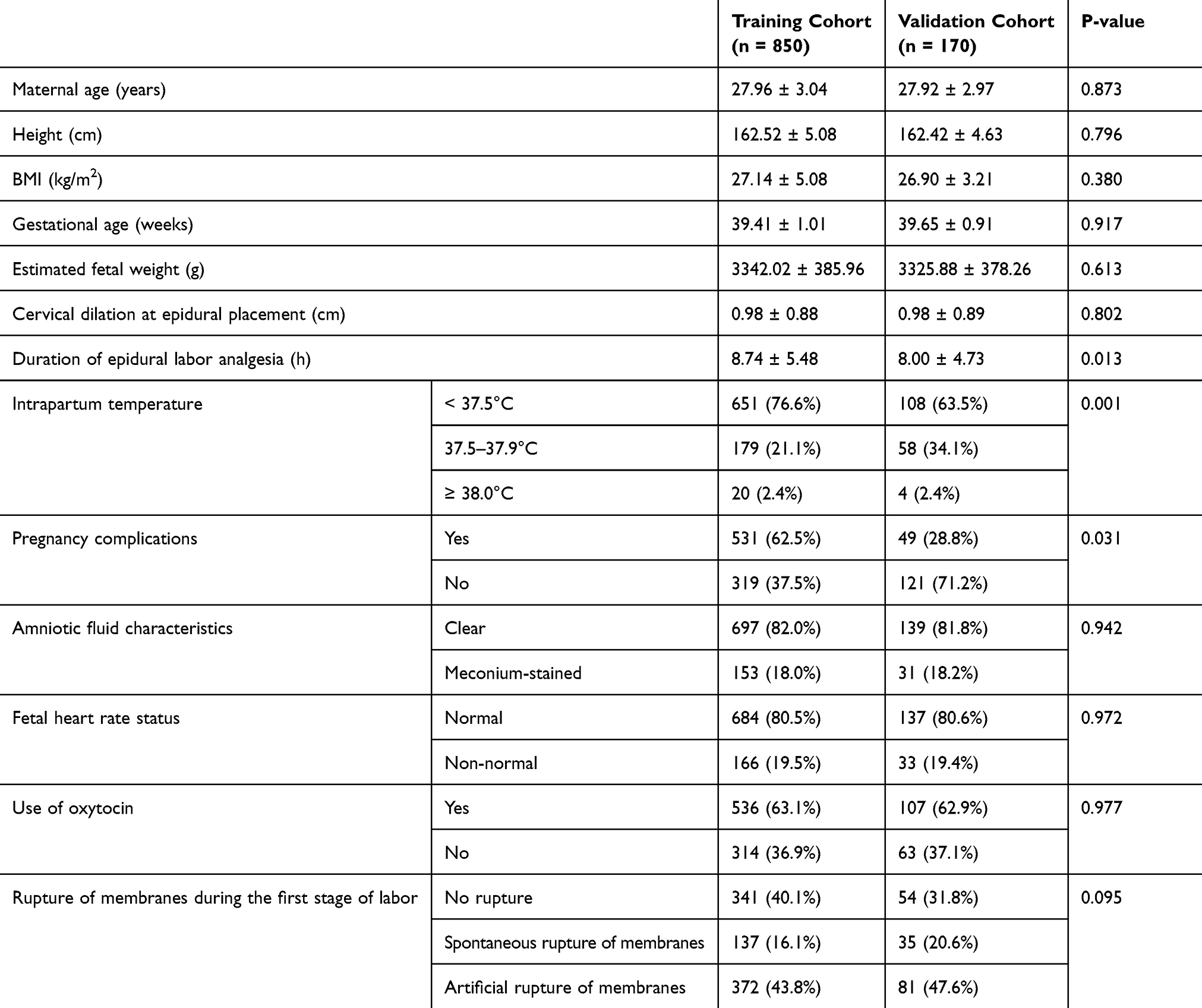 |
Table 2 Baseline Characteristics of the Training and Validation Cohorts |
Univariate Analysis
Among the 850 primiparous women who received epidural labor analgesia in the training cohort, 135 (15.9%) converted to cesarean section and 715 (84.1%) delivered vaginally. All cesarean conversions occurred during the first stage of labor. Participants were therefore categorized into the vaginal delivery group (n = 715) and the cesarean section group (n = 135). Univariate analysis showed that maternal age, cervical dilation at epidural placement, duration of epidural labor analgesia, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor were significantly associated with conversion to cesarean section (P < 0.05). The detailed clinical characteristics of the two groups are summarized in Table 3.
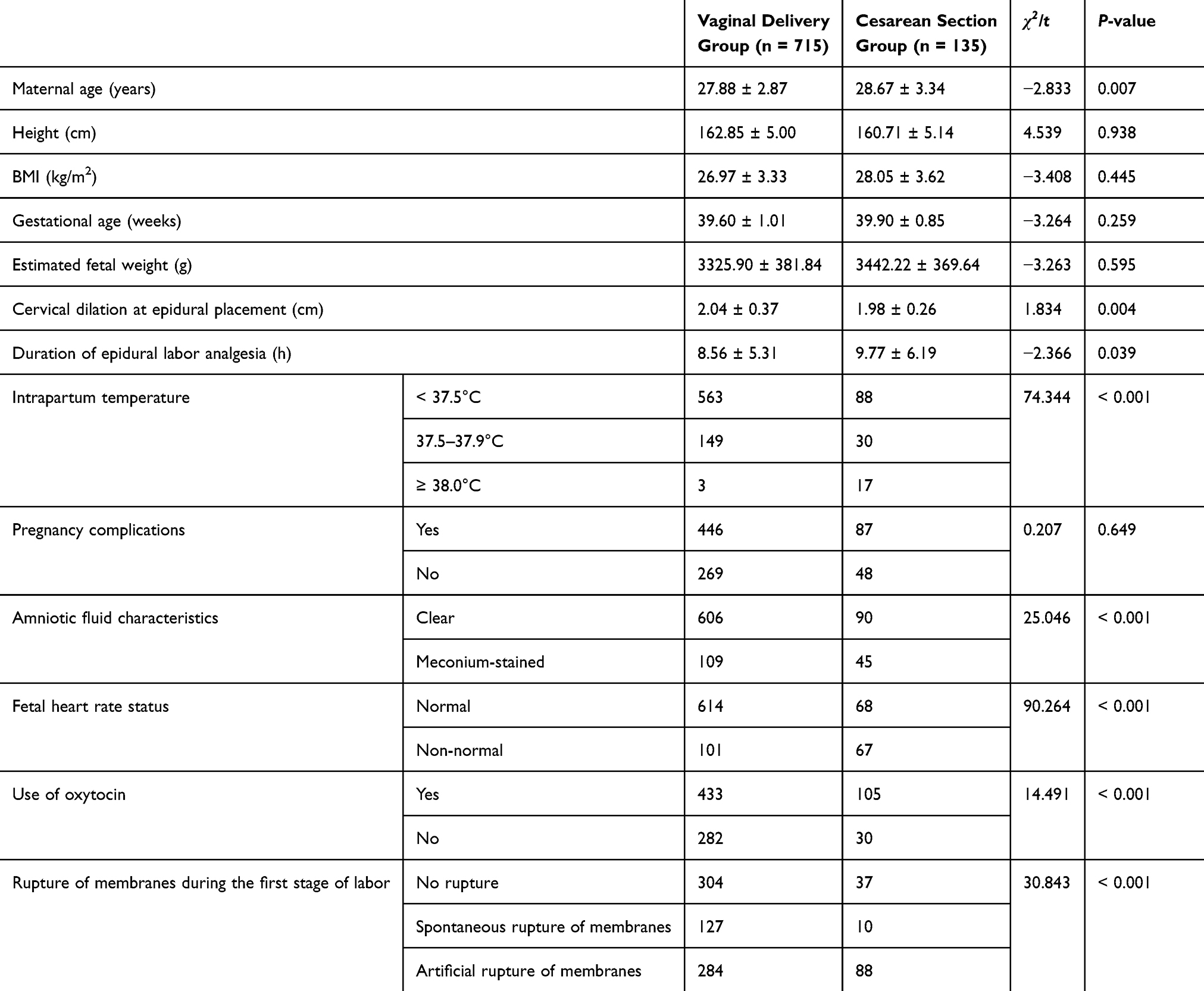 |
Table 3 Comparison of Clinical Characteristics Between the Vaginal Delivery and Cesarean Section Groups in the Training Cohort |
The eight variables identified as significant in the univariate analysis were subsequently assessed for multicollinearity. The VIF values for all variables were less than 5, indicating no evidence of multicollinearity among the predictors.
Multivariable Logistic Regression Analyses
Based on the univariate analysis, eight variables were initially included in the multivariable logistic regression model. After the multivariable analysis, cervical dilation at epidural placement and the duration of epidural labor analgesia were excluded (P > 0.05). As shown in Table 4, the final model retained six significant predictors of conversion to cesarean section: maternal age, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor (P < 0.05). Among these predictors, maternal age and fetal heart rate status were identified as independent risk factors (OR >1, P < 0.05). The final multivariable logistic regression model was further visualized as a nomogram to facilitate individualized risk estimation.
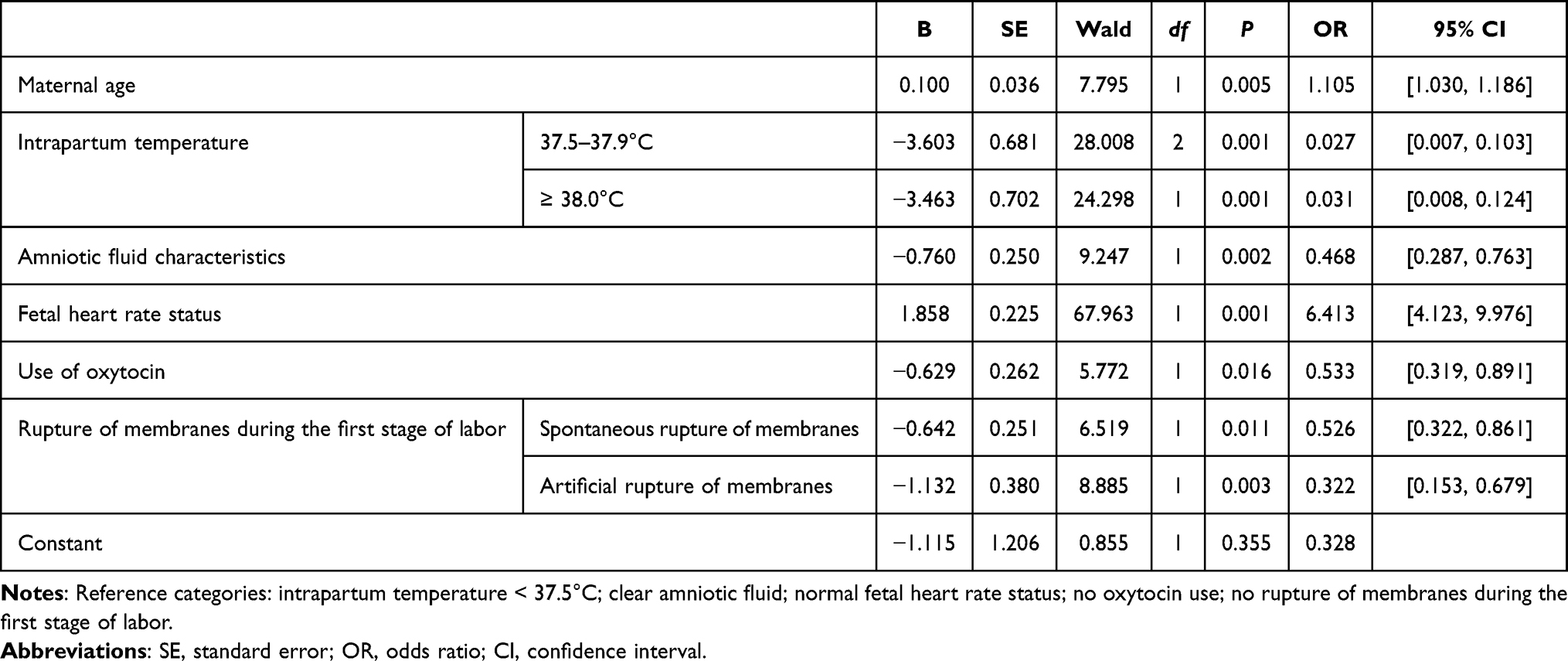 |
Table 4 Multivariable Logistic Regression Analyses |
Development of the Risk Prediction Nomogram
Based on the final multivariable logistic regression model, a risk prediction nomogram was developed to estimate the probability of conversion to cesarean section among primiparous women receiving epidural labor analgesia. The nomogram incorporated the independent predictors identified in the multivariable analysis, including maternal age, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor (Figure 2).
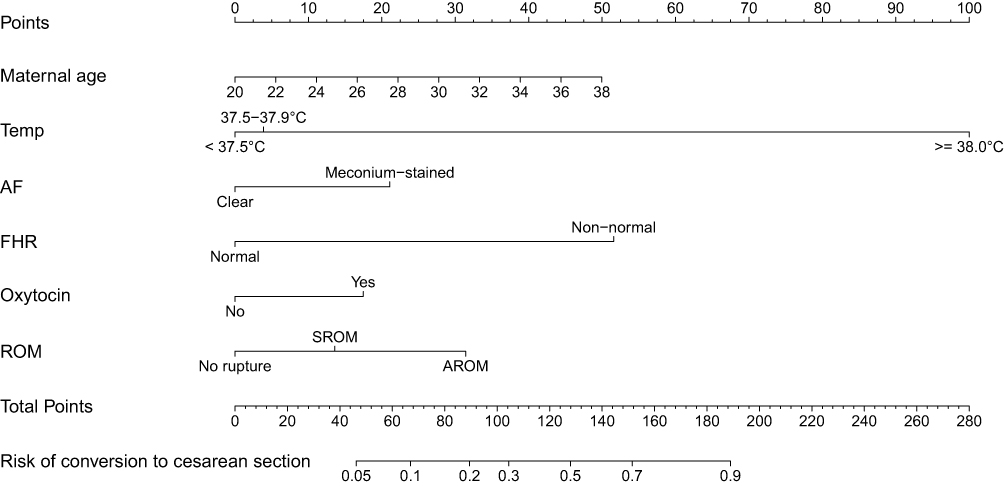 |
Figure 2 Nomogram for predicting conversion to cesarean section in primiparous women receiving epidural labor analgesia. Abbreviations: Temp, intrapartum temperature; AF, amniotic fluid characteristics; FHR, fetal heart rate status; Oxytocin, use of oxytocin; ROM, rupture of membranes during the first stage of labor; SROM, spontaneous rupture of membranes; AROM, artificial rupture of membranes. |
In the nomogram, each predictor corresponds to a specific point value according to its relative contribution to the model. The total score is obtained by summing the points for all predictors, and the corresponding probability of conversion to cesarean section can be determined by projecting the total score onto the probability scale. Higher total points indicate a higher predicted risk of conversion to cesarean section.
Model Construction and Predictive Performance
Based on the results of the logistic regression analysis, the Hosmer-Lemeshow goodness-of-fit test was performed to assess the model calibration. The test yielded a P-value of 0.916 (P > 0.05), indicating good agreement between the predicted and observed outcomes and suggesting that the model was well calibrated.
The model’s discriminatory performance was evaluated using the receiver operating characteristic (ROC) curve. The area under the ROC curve (AUC) was 0.810 (95% CI: 0.768–0.851, P < 0.001), demonstrating good predictive accuracy in distinguishing primiparous women who converted to cesarean section from those who delivered vaginally. The Youden index was 0.428, with a sensitivity of 0.822, and a specificity of 0.606, indicating good overall discriminatory ability (Figure 3).
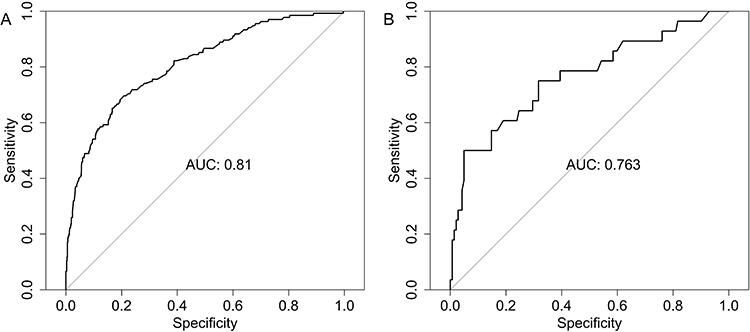 |
Figure 3 Receiver operating characteristic curves of the prediction model for conversion to cesarean section. (A) training cohort; (B) validation cohort. |
Validation of the Clinical Application Effect
For validation of the prediction model, 170 primiparous women were included in the validation cohort, among whom 26 (15.3%) converted to cesarean section. The model achieved a sensitivity of 0.786 and a specificity of 0.592 (Figure 3). The AUC for the validation cohort was 0.763 (95% CI: 0.655–0.871, P < 0.001), demonstrating good discriminatory ability.
The calibration curves showed that the predicted probabilities were reasonably well aligned with the observed outcomes. In both the training and validation cohorts, the calibration plots approached the ideal 45° reference line (Figure 4), suggesting good agreement between predicted and actual risks and indicating satisfactory model calibration.
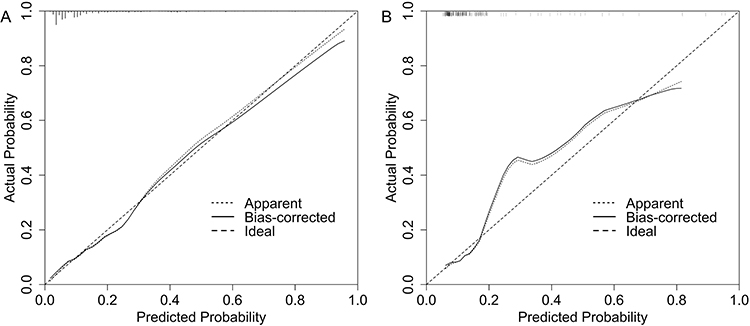 |
Figure 4 Calibration curves of the prediction model for conversion to cesarean section. (A) training cohort; (B) validation cohort. |
Decision curve analysis demonstrated that the prediction model provided a positive net benefit across a range of clinically relevant threshold probabilities in both the training and validation cohorts (Figure 5). Compared with the “treat all” and “treat none” strategies, the model yielded higher net benefit within this range, indicating potential clinical usefulness for decision-making regarding conversion to cesarean section.
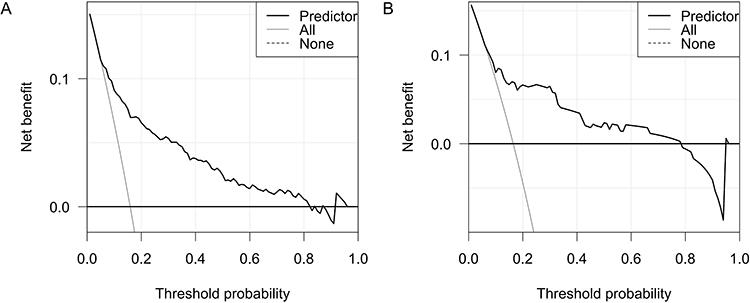 |
Figure 5 Decision curve analysis of the prediction model for conversion to cesarean section. (A) training cohort; (B) validation cohort. |
Discussion
This study examined factors associated with intrapartum cesarean conversion among primiparous women receiving epidural labor analgesia and developed a prediction model to estimate this risk. Epidural labor analgesia defined the study cohort and was not evaluated as an independent exposure variable. Therefore, the findings should be interpreted as predictors of cesarean conversion within this cohort, rather than as evidence of the effect of epidural analgesia on cesarean delivery. The results showed that maternal age, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor were significant predictors of cesarean conversion. The prediction model demonstrated good discriminatory performance, with an area under the curve (AUC) of 0.810, a sensitivity of 0.822, and a specificity of 0.606, indicating satisfactory validity and accuracy. These findings suggest that the model may serve as an early warning tool in clinical practice to help clinicians identify women at increased risk of cesarean conversion and support timely monitoring and appropriate intrapartum management.
Maternal age emerged as an important predictor in our model. This finding is consistent with previous prediction model studies that have reported a higher likelihood of cesarean delivery following labor induction as maternal age increases.19,20 In China, the proportion of older primiparous women has continued to rise in recent years,21 highlighting the clinical relevance of maternal age in obstetric practice. In addition, several large epidemiologic studies have shown that advanced maternal age is associated with increased obstetric and neonatal risks as well as greater psychological stress.22–24 By incorporating maternal age into a multivariable prediction framework tailored to primiparous women receiving epidural labor analgesia, our study provides quantitative evidence that maternal age contributes meaningfully to individualized intrapartum risk assessment. This information may help clinicians identify women who would benefit from closer monitoring or earlier intervention during labor.
Fetal heart rate status was classified as normal (Category I) or non-normal (Category II–III). Non-normal FHR status emerged as one of the strongest predictors in our model, with women in this group having more than a sixfold increased likelihood of conversion to cesarean section. This finding is consistent with previous studies showing that non-reassuring fetal heart rate patterns or suspected intrapartum fetal compromise are associated with an increased likelihood of operative or cesarean delivery.25,26 According to current international guidelines, FHR status is interpreted using a three-tier classification system (Category I–III).27 Non-normal FHR status may arise from multiple mechanisms. On the one hand, epidural labor analgesia can induce sympathetic blockade and maternal hypotension, potentially reducing uteroplacental perfusion and contributing to transient FHR changes.28,29 On the other hand, persistent non-normal FHR patterns may indicate possible fetal compromise, representing early signs of impaired oxygenation or altered autonomic regulation.30,31 In such cases, timely clinical assessment and intervention may be required to prevent further deterioration. Integrating FHR status into a multivariable prediction model provides an effective approach to identifying women at high risk of cesarean conversion during epidural labor analgesia, supporting closer intrapartum surveillance and timely intrapartum management.
In our model, intrapartum temperature was analyzed as a three-level categorical variable. Both moderate temperature elevation (37.5–37.9°C) and fever (≥ 38.0°C) were associated with odds ratios below 1 compared with the reference group (< 37.5°C). This unexpected inverse association should be interpreted cautiously and should not be considered evidence that elevated intrapartum temperature has a true protective effect against cesarean conversion. Instead, it may be partly explained by institution-specific intrapartum management patterns, early interventions after temperature elevation, differences in labor progression, and residual confounding. At our institution, clinical management is initiated once maternal temperature reaches 37.5°C, including intravenous fluid administration, antipyretic treatment, and enhanced electronic fetal monitoring. These interventions may help stabilize maternal-fetal status and prevent further deterioration in some cases. In addition, non-infectious epidural-related maternal fever is thought to involve sterile inflammatory activation and altered thermoregulatory control during epidural analgesia, leading to transient temperature elevation without necessarily compromising fetal oxygenation.32,33 In contrast, women with temperatures <37.5°C may have included those with prolonged labor or poor progress but without fever, who were more likely to require cesarean delivery for labor arrest despite normothermia. Nevertheless, maternal fever remains clinically important. Febrile parturients receiving epidural labor analgesia have been reported to show higher cesarean rates,34 and chorioamnionitis is strongly associated with maternal fever and adverse outcomes.35 Furthermore, intrapartum fever may trigger inflammatory pathways and alter placental microcirculation, potentially impairing fetal oxygenation.36,37 Therefore, the observed ORs below 1 for higher temperature categories should be interpreted as model-specific associations influenced by clinical management patterns and residual confounding rather than as evidence of a protective effect. These findings highlight the importance of careful assessment for possible infection and close maternal-fetal monitoring during labor.
Oxytocin promotes prostaglandin synthesis in the decidua and amnion, which facilitates cervical ripening and strengthens myometrial contractions.38 In clinical practice, oxytocin is often used together with artificial rupture of membranes to enhance uterine activity and support labor progress. Recent studies indicate that timely oxytocin augmentation can shorten labor duration, improve contraction efficiency, and reduce the risk of intrapartum cesarean delivery in women with delayed labor progress.39,40 Combined oxytocin and artificial rupture of membranes strategies have also been shown to be more effective than artificial rupture of membranes alone.41 Although earlier studies have suggested that rupture of membranes increases the risk of intrapartum fever,42,43 our collinearity assessment showed variance inflation factor values below five for all predictors, indicating that their correlation did not introduce instability into the model. Both variables contributed independently to the prediction of cesarean conversion. In addition, use of oxytocin was associated with an adjusted odds ratio below one, consistent with evidence that timely oxytocin augmentation can improve uterine contraction efficiency, support labor progress, and lower the likelihood of cesarean conversion.
In summary, this prediction model provides a practical and evidence-based tool for early identification of primiparous women at increased risk of intrapartum cesarean conversion within an epidural labor analgesia cohort. The model uses routinely collected maternal, fetal, and intrapartum variables and could be integrated into electronic medical record systems or simple clinical tools to support risk assessment during labor and individualized care. Its use may help clinicians recognize concerning labor patterns earlier, strengthen intrapartum monitoring, and adjust management in a timely manner. Future studies should validate this model in different populations and develop accessible digital tools to support its use in everyday practice.
Limitations
This study has several limitations. First, the retrospective design may introduce potential selection bias and unmeasured confounding. Second, although all cesarean conversions occurred during the first stage of labor and no cesarean delivery was documented as being directly caused by serious anesthesia-related complications, the retrospective design limited our ability to fully assess the potential indirect effects of physiological changes related to epidural labor analgesia on labor progression and fetal status. Finally, this was a single-center study, which may limit the generalizability of the prediction model to other institutions or populations. Although the model demonstrated good performance in the validation cohort, external validation in multicenter cohorts is warranted to confirm its broader applicability. Future studies incorporating additional clinical variables and advanced modeling approaches, including machine learning techniques, may further improve predictive performance and clinical utility.
Conclusion
Maternal age, intrapartum temperature, amniotic fluid characteristics, fetal heart rate status, use of oxytocin, and rupture of membranes during the first stage of labor were identified as key predictors of intrapartum cesarean conversion among primiparous women receiving epidural labor analgesia. This study developed and validated a logistic regression prediction model for risk assessment within this specific intrapartum cohort. The model demonstrated good discrimination, calibration, and clinical utility, indicating its potential value for early warning and individualized intrapartum management. Future studies should include multicenter external validation and integration of the model into practical clinical tools to enhance its applicability.
Funding
This study was supported by the Science and Technology Development Fund of Nanjing Medical University (Grant number: NMUB20240256).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zuarez-Easton S, Erez O, Zafran N, Carmeli J, Garmi G, Salim R. Pharmacologic and nonpharmacologic options for pain relief during labor: an expert review. Am J Obstet Gynecol. 2023;228(5S):S1246–13. doi:10.1016/j.ajog.2023.03.003
2. Halliday L, Nelson SM, Kearns RJ. Epidural analgesia in labor: a narrative review. Int J Gynaecol Obstet. 2022;159(2):356–364. doi:10.1002/ijgo.14175
3. Nanji JA, Carvalho B. Pain management during labor and vaginal birth. Best Pract Res Clin Obstet Gynaecol. 2020;67:100–112. doi:10.1016/j.bpobgyn.2020.03.002
4. Li P, Ma X, Han S, et al. Risk factors for failure of conversion from epidural labor analgesia to cesarean section anesthesia and general anesthesia incidence: an updated meta-analysis. J Matern Fetal Neonatal Med. 2023;36(2):2278020. doi:10.1080/14767058.2023.2278020
5. Deepak D, Kumari A, Mohanty R, Prakash J, Kumar T, Priye S. Effects of epidural analgesia on labor pain and course of labor in primigravid parturients: a prospective non-randomized comparative study. Cureus. 2022;14(6):e26090. doi:10.7759/cureus.26090
6. Šklebar I, Vrljičak M, Habek D, Šklebar T, Šakić L. Conversion rate of epidural analgesia to caesarean section regional or general anesthesia. Acta Clin Croat. 2022;61(Suppl 2):15–21. doi:10.20471/acc.2022.61.s2.02
7. Ghanbari-Homaie S, Meedya S, Mohammad-Alizadeh-Charandabi S, Jafarabadi MA, Mohammadi E, Mirghafourvand M. Recommendations for improving primiparous women’s childbirth experience: results from a multiphase study in Iran. Reprod Health. 2021;18(1):146. doi:10.1186/s12978-021-01196-7
8. Lindblad V, Melgaard D, Jensen KL, et al. Primiparous women differ from multiparous women after early discharge regarding breastfeeding, anxiety, and insecurity: a prospective cohort study. Eur J Midwifery. 2022;6:12. doi:10.18332/ejm/146897
9. Khamehchian M, Adib-Hajbaghery M, HeydariKhayat N, Rezaei M, Sabery M. Primiparous women’s experiences of normal vaginal delivery in Iran: a qualitative study. BMC Pregnancy Childbirth. 2020;20(1):259. doi:10.1186/s12884-020-02954-4
10. Patel S, Ciechanowicz S, Blumenfeld YJ, Sultan P. Epidural-related maternal fever: incidence, pathophysiology, outcomes, and management. Am J Obstet Gynecol. 2023;228(5S):S1283–S1304.e1. doi:10.1016/j.ajog.2022.06.026
11. Layera S, Bravo D, Aliste J, Tran DQ. A systematic review of DURAL puncture epidural analgesia for labor. J Clin Anesth. 2019;53:5–10. doi:10.1016/j.jclinane.2018.09.030
12. Danilack VA, Hutcheon JA, Triche EW, et al. Development and validation of a risk prediction model for cesarean delivery after labor induction. J Womens Health. 2020;29(5):656–669. doi:10.1089/jwh.2019.7822
13. Pfützenreuter GR, Cavalieri JC, Fragoso APO, Da Corregio KS, Freitas PF, Trapani A Jr. Fatores associados à cesárea intraparto em mulheres submetidas a indução do parto [Factors Associated with Intrapartum Cesarean Section in Women Submitted to Labor Induction]. Rev Bras Ginecol Obstet. 2019;41(6):363–370. Portuguese. doi:10.1055/s-0039-1688966
14. Macones GA, Hankins GD, Spong CY, Hauth J, Moore T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Obstet Gynecol. 2008;112(3):661–666. doi:10.1097/AOG.0b013e3181841395
15. Saritha MS, Suneetha A. Epidural analgesia during labour: its influences on pain relief, progress of labour, mode of delivery, maternal and foetal outcomes. Int J Reprod Contracept Obstet Gynecol. 2020;9(2):555–562. doi:10.18203/2320-1770.ijrcog20200100
16. Van Smeden M, Reitsma JB, Riley RD, Collins GS, Moons KG. Clinical prediction models: diagnosis versus prognosis. J Clin Epidemiol. 2021;132:142–145. doi:10.1016/j.jclinepi.2021.01.009
17. Zhu S, Wei D, Zhang D, Jia F, Liu B, Zhang J. Prolonged epidural labor analgesia increases risks of epidural analgesia failure for conversion to cesarean section. Nan Fang Yi Ke Da Xue Xue Bao. 2022;42(8):1244–1249. doi:10.12122/j.issn.1673-4254.2022.08.18
18. Pham B, Delage M, Girault A, Lepercq J, Bonnet MP. Risk factors for conversion to general anesthesia for urgent cesarean among women with labor epidural analgesia: a retrospective case-control study. J Gynecol Obstet Hum Reprod. 2022;51(9):102468. doi:10.1016/j.jogoh.2022.102468
19. Correa-de-Araujo R, Yoon SSS. Clinical outcomes in high-risk pregnancies due to advanced maternal age. J Womens Health. 2021;30(2):160–167. doi:10.1089/jwh.2020.8860
20. Attali E, Doleeb Z, Hiersch L, et al. The risk of intrapartum cesarean delivery in advanced maternal age. J Matern Fetal Neonatal Med. 2022;35(25):8019–8026. doi:10.1080/14767058.2021.1940936
21. Zhang S, Qian Z, Zhao Y, Yu X, Cheng C, Li Q. Effects of Group Prenatal Health Care combined with happiness training on delivery mode and maternal role adaptation in elderly primiparous women: a study for improvements in patients health behavior. Am J Health Behav. 2023;47(2):369–377. doi:10.5993/AJHB.47.2.16W
22. Frick AP. Advanced maternal age and adverse pregnancy outcomes. Best Pract Res Clin Obstet Gynaecol. 2021;70:92–100. doi:10.1016/j.bpobgyn.2020.07.005
23. Glick I, Kadish E, Rottenstreich M. Management of pregnancy in women of advanced maternal age: improving outcomes for mother and baby. Int J Womens Health. 2021;13:751–759. doi:10.2147/IJWH.S283216
24. Guarga Montori M, Álvarez Martínez A, Luna Álvarez C, Abadía Cuchí N, Mateo Alcalá P, Ruiz-Martínez S. Advanced maternal age and adverse pregnancy outcomes: a cohort study. Taiwan J Obstet Gynecol. 2021;60(1):119–124. doi:10.1016/j.tjog.2020.11.018
25. Kalafat E, Morales-Rosello J, Thilaganathan B, Tahera F, Khalil A. Risk of operative delivery for intrapartum fetal compromise in small-for-gestational-age fetuses at term: an internally validated prediction model. Am J Obstet Gynecol. 2018;218(1):134.e1–134.e8. doi:10.1016/j.ajog.2017.10.022
26. Novillo-Del Álamo B, Martínez-Varea A, Nieto-Tous M, et al. Prediction of cesarean section for intrapartum fetal compromise: a multivariable model from a prospective observational approach. J Pers Med. 2024;14(6):658. doi:10.3390/jpm14060658
27. Mohan M, Ramawat J, La Monica G, et al. Electronic intrapartum fetal monitoring: a systematic review of international clinical practice guidelines. AJOG Glob Rep. 2021;1(2):100008. doi:10.1016/j.xagr.2021.100008
28. Ghidini A, Vanasche K, Cacace A, Cacace M, Fumagalli S, Locatelli A. Side effects from epidural analgesia in laboring women and risk of cesarean delivery. AJOG Glob Rep. 2023;4(1):100297. doi:10.1016/j.xagr.2023.100297
29. Hyuga S, Parry R, Dan W, Onishi Y, Gallos G, Okutomi T. Maternal heart rate variability patterns associated with maternal hypotension and non-reassuring fetal heart rate patterns following initiation of combined spinal-epidural labor analgesia: a prospective observational trial. Int J Obstet Anesth. 2023;54:103645. doi:10.1016/j.ijoa.2023.103645
30. Jia YJ, Chen X, Cui HY, Whelehan V, Archer A, Chandraharan E. Physiological CTG interpretation: the significance of baseline fetal heart rate changes after the onset of decelerations and associated perinatal outcomes. J Matern Fetal Neonatal Med. 2021;34(14):2349–2354. doi:10.1080/14767058.2019.1666819
31. Tournier A, Beacom M, Westgate JA, et al. Physiological control of fetal heart rate variability during labour: implications and controversies. J Physiol. 2022;600(3):431–450. doi:10.1113/JP282276
32. Lin R, Shi P, Li H, Liu Z, Xu Z. Association between epidural analgesia and indications for intrapartum caesarean delivery in group 1 of the 10-group classification system at a tertiary maternity hospital, Shanghai, China: a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21(1):464. doi:10.1186/s12884-021-03925-z
33. Seiler FA, Scavone BM, Shahul S, Arnolds DE. Maternal fever associated with continuous spinal versus epidural labor analgesia: a single-center retrospective study. Anesth Analg. 2022;135(6):1153–1158. doi:10.1213/ANE.0000000000005905
34. Callahan EC, Lee W, Aleshi P, George RB. Modern labor epidural analgesia: implications for labor outcomes and maternal-fetal health. Am J Obstet Gynecol. 2023;228(5S):S1260–S1269. doi:10.1016/j.ajog.2022.06.017
35. Lipschuetz M, Guedalia J, Daud-Sabag L, Shimonovitz ZA, Yagel S, Karavani G. Chorioamnionitis and its association with neonatal and maternal adverse outcomes in women with and without epidural analgesia administration. Eur J Obstet Gynecol Reprod Biol. 2022;273:33–37. doi:10.1016/j.ejogrb.2022.04.011
36. Sultan P, Blumenfeld Y. Elucidating the effects of labor analgesia on fetal immune function and in utero temperature: a novel approach to understanding epidural-related maternal fever. Am J Obstet Gynecol. 2023;229(4):476–477. doi:10.1016/j.ajog.2023.04.035
37. Jansen S, Lopriore E, Naaktgeboren C, et al. Epidural-related fever and maternal and neonatal morbidity: a systematic review and meta-analysis. Neonatology. 2020;117(3):259–270. doi:10.1159/000504805
38. Uvnäs-Moberg K. The physiology and pharmacology of oxytocin in labor and in the peripartum period. Am J Obstet Gynecol. 2024;230(3S):S740–S758. doi:10.1016/j.ajog.2023.04.011
39. Brüggemann C, Carlhäll S, Grundström H, Blomberg M. Labor dystocia and oxytocin augmentation before or after six centimeters cervical dilatation, in nulliparous women with spontaneous labor, in relation to mode of birth. BMC Pregnancy Childbirth. 2022;22(1):408. doi:10.1186/s12884-022-04710-2
40. Nabhan A, Boulvain M. Augmentation of labour. Best Pract Res Clin Obstet Gynaecol. 2020;67:80–89. doi:10.1016/j.bpobgyn.2020.03.011
41. Dick A, Gutman-Ido E, Chill HH, et al. Artificial rupture of membranes as a mode for induction of labor in women with a previous cesarean section- a retrospective cohort study. BMC Pregnancy Childbirth. 2022;22(1):886. doi:10.1186/s12884-022-05237-2
42. Abu Shqara R, Nakhleh Francis Y, Lowenstein L, Frank Wolf M. The relation between low-grade fever during prolonged rupture of membranes (>12 hours) at term and infectious outcomes: a retrospective cohort study. Am J Obstet Gynecol. 2024;231(3):361.e1–361.e10. doi:10.1016/j.ajog.2024.05.054
43. An H, Zheng W, Zhu Q, Chai Y. A retrospective study of risk factors for early-onset neonatal sepsis with intrapartum maternal fever. PeerJ. 2022;10:e13834. doi:10.7717/peerj.13834
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of a Model to Predict Cesarean Delivery as the Outcome of a Failed Labor Induction in Singleton Obese Pregnant Women at Term
Feng Y, Luan Y, Zhou L, Yin C
International Journal of Women's Health 2025, 17:5277-5286
Published Date: 9 December 2025