Back to Journals » International Journal of Women's Health » Volume 10
Construct validity and factor structure of a Spanish-language Social Support Questionnaire during early pregnancy
Authors Friedman LE, Manriquez Prado AK, Santos Malavé GF, Vélez JC, Gillibrand Esquinazi RW, Sanchez SE, Zhong QY, Gelaye B, Williams MA
Received 22 December 2017
Accepted for publication 24 April 2018
Published 19 July 2018 Volume 2018:10 Pages 379—385
DOI https://doi.org/10.2147/IJWH.S160619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Lauren E Friedman,1 Ana Karen Manriquez Prado,2,* Gabriel Fidel Santos Malavé,2,* Juan Carlos Vélez,3 Rodrigo Winston Gillibrand Esquinazi,4 Sixto E Sanchez,5,6 Qiu-Yue Zhong,1 Bizu Gelaye,1 Michelle A Williams1
1Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA, USA; 2Multidisciplinary International Research Training Program, Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA, USA; 3Department of Rehabilitation, Hospital del Trabajador, Santiago, Chile; 4Department of Mental Health, Hospital del Trabajador, Santiago, Chile; 5Universidad Peruana de Ciencias Aplicadas, Lima, Peru; 6Asociación Civil PROESA, Lima, Peru
*These authors contributed equally to this work
Background: The Social Support Questionnaire – Short Form (SSQ-6) is a widely used instrument that assesses availability and satisfaction of a person’s social support. The present study aimed to evaluate the construct validity and factor structure of the Spanish language version of the SSQ-6 during early pregnancy.
Participants and methods: A total of 4,236 pregnant Peruvian women were interviewed at 10.3 ± 3.8 weeks of gestation. In-person interviewers were used to collect lifestyle, demographic, and social support characteristics. The construct validity and factorial structure of the SSQ-6 were assessed through exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The internal consistency was evaluated using Cronbach’s alpha.
Results: The mean SSQ-6 score was 39.6 ± 6.8 and Cronbach’s alpha was 0.83. EFA resulted in a three-factor solution that accounted for 60.6% of the variance. CFA results confirmed the three-factor structure and yielded measures indicating goodness of fit (comparative fit index of 0.9401) and accuracy (root mean square error of approximation of 0.0394).
Conclusion: Although the SSQ-6 was originally developed as a two-factor model, and previous studies have supported this, in our study a three-factor model was found to be more appropriate. The SSQ-6 was found to have good construct validity and reliability for assessing social support.
Keywords: social support, SSQ-6, pregnancy, validation
Introduction
Social support is broadly defined as social resources that are available or provided to individuals by non-professionals in formal support groups and informal helping relationships.1 Social support has been associated with a higher quality of life and well-being, and has even been found to have a buffering effect on life stressors.2 Individuals with higher levels of support have good overall mental and physical health.3 Additionally, social support is associated with better outcomes from chronic diseases including diabetes,4 cardiovascular disease,5 and overall mortality.6 During pregnancy, lower social support is associated with maternal mental health problems including anxiety;7 antepartum8 and postpartum depression;9 and pregnancy complications including lower Apgar scores,10 impaired fetal growth,11 and preterm delivery.12 Maternal social support during pregnancy has long-lasting impacts on both mothers and children.
Characterizing maternal social support is needed for further research and interventions of maternal mental health to improve maternal and perinatal outcomes. The Social Support Questionnaire – Short Form (SSQ-6) was developed as a way to assess the availability and satisfaction of a person’s social support.13 However, to our knowledge, 1) there has been only one study assessing the SSQ-6 in a Spanish-speaking population14 and 2) one previous study has used the SSQ-6 in a population of Japanese pregnant women.15 The objective of our study was to evaluate the construct validity and factor structure of a Spanish-language version of the SSQ-6 among pregnant women in Lima, Peru.
Participants and methods
Study population
Our study is a part of the Pregnancy Outcomes, Maternal and Infant Study (PrOMIS), a longitudinal study carried out between February 2012 and March 2014. This study was designed to examine social and behavioral maternal risk factors of pregnancy outcomes among Peruvian women attending the Instituto Nacional Materno Perinatal (INMP) in Lima, Peru. The PrOMIS cohort has been described previously.16–18 Eligible participants were between 18 and 49 years old, fluent in Spanish, and had a gestational age of at least 16 weeks. Our study consisted of 4,361 pregnant women; however, 125 were excluded due to missing responses on the SSQ-6. The remaining analyzed sample consisted of 4,236 women. Excluded participants did not differ from the rest of the sample in regard to sociodemographic and lifestyle characteristics. Study procedures were approved by the institutional review boards of the Human Research Administration Office at Harvard T.H. Chan School of Public Health in Boston, MA, USA and INMP in Lima, Peru. All study participants provided written informed consent.
Social Support Questionnaire-6 (SSQ-6)
Social support was measured using a Spanish-language version of the SSQ-6, a 12-item questionnaire that assesses the availability and satisfaction of a person’s social support.13 The original 27-item Sarason’s Social Support Questionnaire was developed in 1983.19 The SSQ-6 is a brief 6-question version of the original 27-item questionnaire that was developed in 1987. Since its development, the SSQ-6 has been adapted in other languages including Russian,20 French,21 Japanese,15 and Spanish.14 The responses to the SSQ-6 are used to calculate 1) a Social Support Questionnaire-6 Number Score (SSQN) and 2) a Social Support Questionnaire-6 Satisfaction Score (SSQS). Study participants were asked about social support that they received since becoming pregnant. The SSQN measures the number of available individuals that participants can turn to in different situations. The SSQN score was calculated using 6 items, which are referred to as items 1–6. For each item, participants listed zero to nine people they felt could provide them with support in a specific scenario. The SSQN total score can range from 0 to 54. The SSQS was calculated by asking participants to rate their levels of satisfaction with the support they received in each of the six scenarios. Participants rated their satisfaction on a Likert scale from 1 (very unsatisfied) to 6 (very satisfied). The SSQS questions will be referred to as items 1–6. The total SSQS score a participant could receive ranges from 6 to 36.
Other covariates
Structured questionnaires were used to determine participants’ sociodemographic and reproductive characteristics. Participants’ age was categorized as 18–19, 20–29, 30–34, and ≥35 years. Other covariates examined were education (≤6, 7–12, >12 years of education), ethnicity (Mestizos of mixed Amerindian and European descent vs others), married or living with a partner (yes vs no), employed (yes vs no), difficulty paying for basics (very hard to somewhat hard vs not very hard), difficulty paying for medical care (very hard to somewhat hard vs not very hard), nulliparous (yes vs no), planned pregnancy (yes vs no), early pregnancy measured body mass index (<18.5, 18.5–24.9, 25–29.9, >30 kg/m2), and gestational age at interview (weeks).
Statistical analysis
The frequency distributions of sociodemographic, physical, and lifestyle characteristics were assessed using mean ± SD for continuous variables and numbers and percentages for categorical variables. Reliability was assessed using Cronbach’s alpha for all 12 items, and for the SSQN and the SSQS separately. We further analyzed each item’s reliability by assessing its item-total correlation and the overall reliability when a specific item was deleted. Construct validity was assessed using an exploratory factor analysis (EFA). We first examined the data to ensure suitability for EFA. This analysis demonstrated that it was appropriate to proceed with factor analysis (Bartlett’s test of sphericity, p-value = <0.0001, and Kaiser’s measure of sampling adequacy = 0.779). We conducted an EFA using principal component analysis with varimax rotation. Factors with eigenvalues >1 were assumed to be meaningful and retained for rotation. Rotation factor loadings of ≥0.4 were considered sufficient, while items with factor loadings of ≥0.4 on more than one factor were considered cross-loading. A confirmatory factor analysis (CFA) was conducted to evaluate the fit of our model. CFA was done using weighted least-squares estimation. As recommended by Brown, the following criteria were used to ensure an adequate fit: 1) standardized root mean residual (SRMR) values ≤0.08; 2) root mean square error of approximation (RMSEA) values ≤0.06 or below; and 3) comparative fit index ≥0.95.22 To further analyze the correlation between the 12 items, we conducted a bivariate correlation using Pearson’s coefficients. Statistical analyses were performed using SPSS Statistics, version 23.0 (IBM, Armonk, NY, USA), and Statistical Analysis System software (SAS Institute, Cary, NC, USA).
Results
Table 1 shows the demographic and lifestyle characteristics of study participants. The majority of women were between the ages of 20–29 years (55.6%). Most were married or living with a partner (81.7%) and identified as Mestizo (78.1%). About half of the women were employed (47.6%) and found that it was not very hard to pay for their basic needs (53.4%) or medical care (52.3%). The mean SSQ-6 score was 39.6 ± 6.8, with a mean SSQN score of 8.2 ± 3.2 and mean SSQS score of 31.4 ± 4.7 (Table 1).
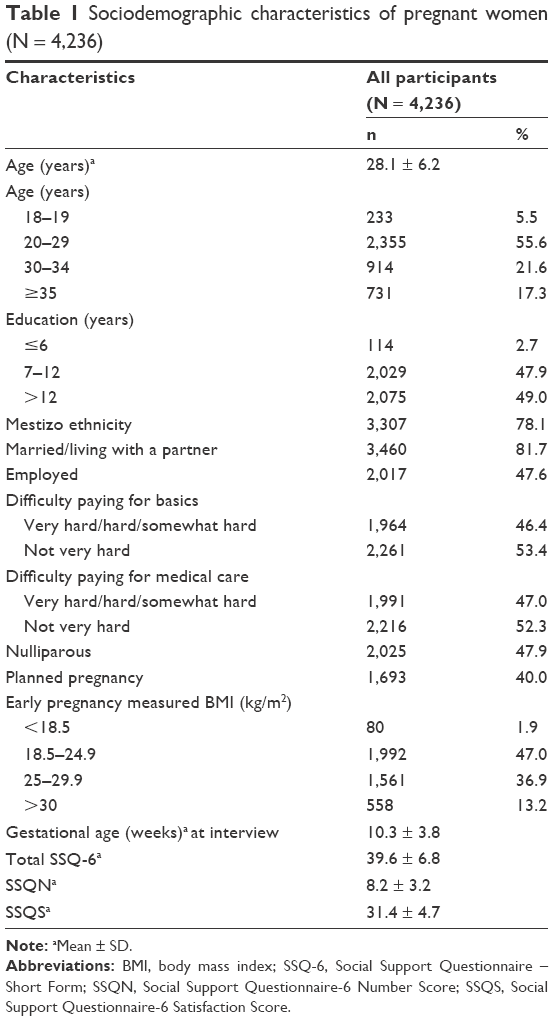 | Table 1 Sociodemographic characteristics of pregnant women (N = 4,236) |
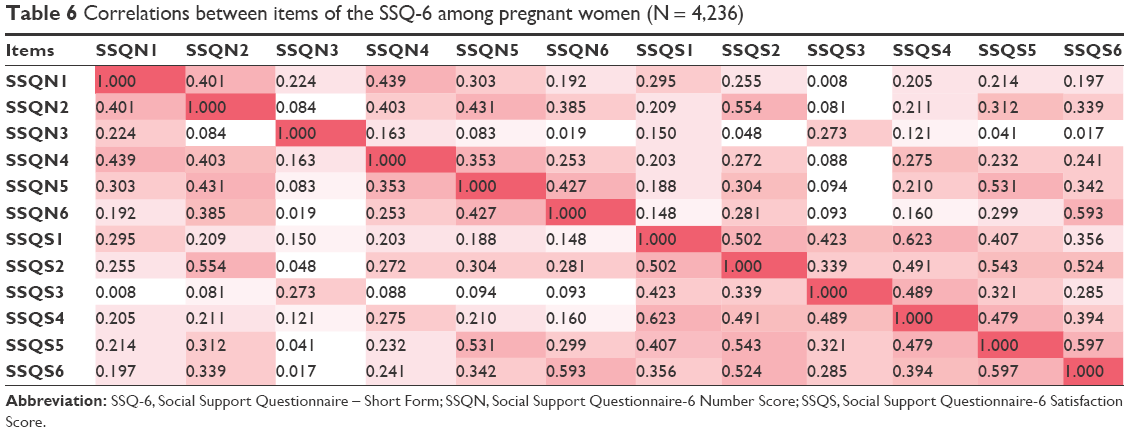
The Cronbach’s alpha reliability coefficient for the SSQ-6 total score was 0.83 (Table 2). The SSQN and SSQS subscales had a Cronbach’s alpha of 0.70 and 0.83, respectively (Table 2). The correlations between the 12 items of the SSQ-6 are listed in Table 3. The highest item-total correlation coefficient was for item 2 of the SSQS (0.64) and the lowest was for item 3 of the SSQN (0.18) (Table 3).
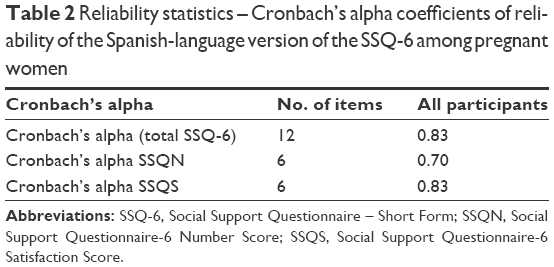 | Table 2 Reliability statistics – Cronbach’s alpha coefficients of reliability of the Spanish-language version of the SSQ-6 among pregnant women |
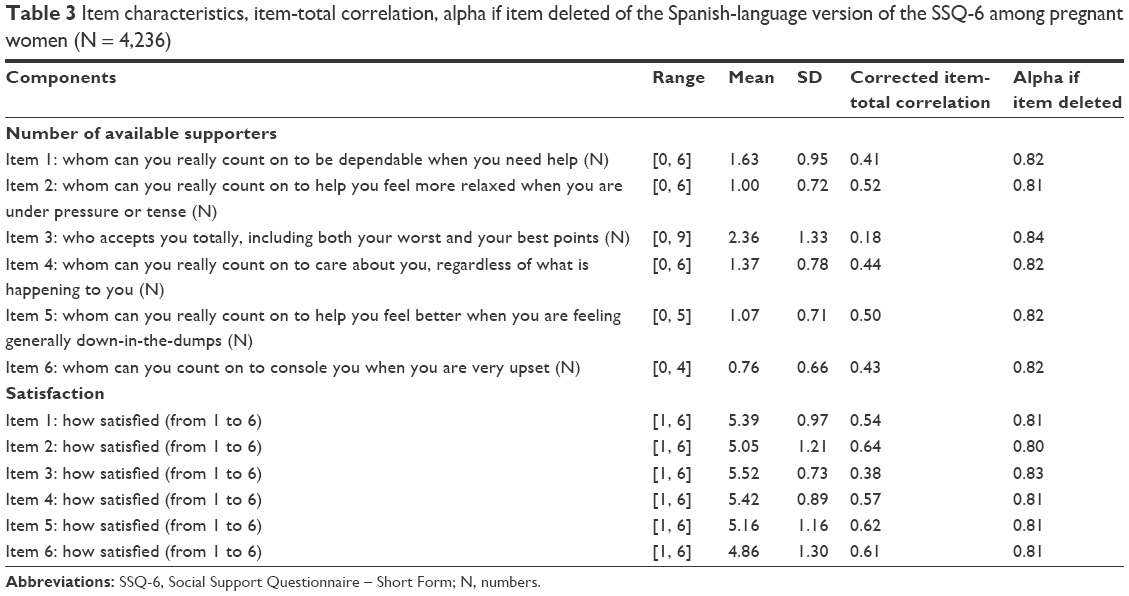 | Table 3 Item characteristics, item-total correlation, alpha if item deleted of the Spanish-language version of the SSQ-6 among pregnant women (N = 4,236) |
The EFA showed a three-factor solution in our population, which accounted for 60.6% of the total variance (Table 4). The SSQS items loaded to Factor 2 (satisfaction), except for questions 5 and 6 of SSQS that loaded to Factor 1 (circumstantial). The SSQN items were distributed between Factor 1 (circumstantial) and Factor 3 (unconditional). Items 2, 5, and 6 of SSQN loaded to Factor 1 (circumstantial), while items 1, 3, and 4 loaded to Factor 3 (unconditional). Factors 1, 2, and 3 explained 36.4%, 13.4%, and 10.8% of the variance, respectively (Table 4). The results of the CFA confirmed the findings of the EFA indicating a three-factor model (Table 5; Figure 1). The first three-factor model we examined resulted in a comparative fit index (CFI) value of 0.9401, a SRMR of 0.0362, and RMSEA of 0.0394 (Table 5). Estimates of the loadings of the measures on each of the factors are presented in Figure 1. Table 6 shows the results of the bivariate correlations between SSQ-6 items.
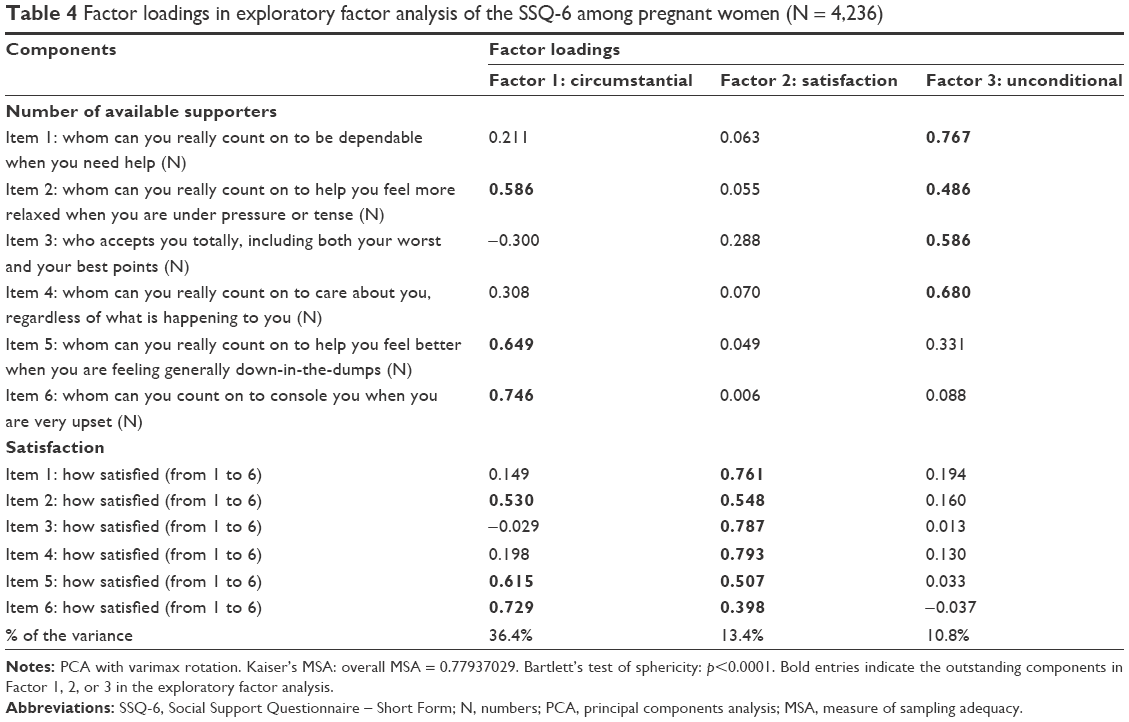 | Table 4 Factor loadings in exploratory factor analysis of the SSQ-6 among pregnant women (N = 4,236) |
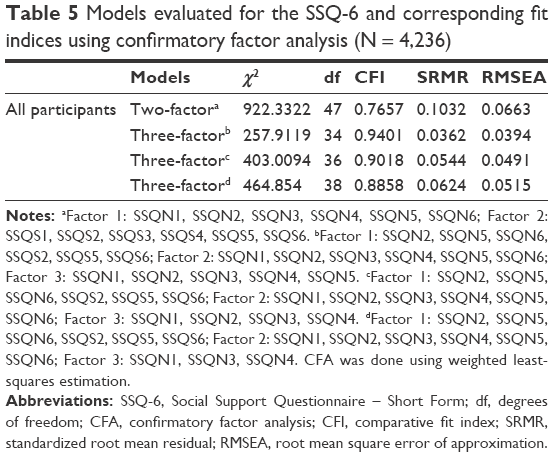 | Table 5 Models evaluated for the SSQ-6 and corresponding fit indices using confirmatory factor analysis (N = 4,236) |
 | Figure 1 Standardized regression weights for paths associated with the best fit model for the SSQ-6 (N = 4,236). |
 | Table 6 Correlations between items of the SSQ-6 among pregnant women (N = 4,236) |
Discussion
In our cohort, the SSQ-6 has good construct validity and reliability for assessing social support. We found that the Spanish-language version of the SSQ-6 had an overall Cronbach’s alpha of 0.83. The mean total SSQ-6 score was 39.6 ± 6.8, with a mean SSQN score of 8.2 ± 3.2 and mean SSQS score of 31.4 ± 4.7. Previous studies had higher SSQN and SSQS scores compared to our population. For example, in a French cohort of university undergraduates and unemployed men, the mean total SSQN was 20.1 and SSQS was 28.1.21 In a study of university students in Spain, the mean was 4.96 per item for SSQN and 5.24 per item for SSQS.14
The SSQ-6 questionnaire was originally designed as a two-factor model. However, the EFA and CFA indicate that in our cohort the most appropriate model is a three-factor solution. In contrast to our results, previous studies assessing the psychometric properties of the SSQ-6 reported a two-factor model with all SSQS items loaded to one factor, and all SSQN items to another.20,21 An adaptation in a cohort of Russian-speaking immigrants in Portugal (N = 555) did not account for mean satisfaction and availability responses, but did find a two-factor structure to be the best fit and tested high for reliability.20 In the population of Russian-speaking immigrants, the two factors extracted using a factor analysis were number of supporters and satisfaction with social support received.20 Similarly, in a French population of university students (N = 348) and unemployed men (N = 304), the SSQ-6 yielded the two factors of availability and satisfaction.21 A cohort of Japanese pregnant women (N = 888) also showed a two-factor model with number and satisfaction subscales.15
In our study, however, a three-factor model was more appropriate. We found the SSQ-6 number and satisfaction subscales were divided among the following three factors: Factor 1 (circumstantial), Factor 2 (satisfaction), and Factor 3 (unconditional). The 6 items of SSQS all loaded to Factor 1 (circumstantial) or Factor 2 (satisfaction), and the 6 items of SSQN loaded to Factor 1 (circumstantial) or Factor 3 (unconditional). Significant portions of items 2, 5, and 6 of SSQS (How satisfied are you?) loaded to both Factor 1 (circumstantial) and Factor 2 (satisfaction) (Table 4). Corresponding items 2, 5, and 6 of the SSQN also loaded to Factor 1 (circumstantial). SSQN items 2, 5, and 6 each ask about social support during stressful or negative experiences (“Whom can you really count on to help you feel more relaxed when you are under pressure or tense?”, “Whom can you really count on to help you feel better when you are feeling generally down-in-the-dumps?”, and “Whom can you count on to console you when you are very upset?”). By contrast, SSQN items 1, 3, and 4 loaded to Factor 3 (unconditional) and ask about dependability and support in both positive and negative circumstances (“Whom can you really count on to be dependable when you need help?”, “Who accepts you totally, including both your worst and your best points?” “Whom can you really count on to care about you, regardless of what is happening to you?”). Social support during stressful experiences may be especially important during pregnancy. Since our results are unique when compared to studies assessing the psychometric properties of the SSQ-6; additional studies should be done to analyze the factor structure in diverse obstetric populations.
Strengths and limitations
Our study has notable strengths, including a well-characterized study cohort and a large sample size, which allowed us to conduct a robust factor analysis. Our study also has some limitations. Given that all participants were pregnant women attending prenatal care at INMP, there is a strong possibility that our sample is not representative of other communities of pregnant women in Peru, specifically women identified as members of indigenous or rural communities. As a result, our study may not be generalizable to all Peruvians or other South American populations. Another limitation is that we were unable to evaluate criterion validity, as there is no diagnostic gold standard for measuring social support. Moreover, there is inherent difficulty in measuring temporal mental health, including social support. Stigma concerning the reporting mental health concerns may lead to disclosure and recall bias.
Conclusion
Our study is the first to assess the reliability and construct validity of the SSQ-6 among Peruvian pregnant women. Given the influence of social support in maternal and prenatal health, it is important to implement valid and reliable tools to measure social support. The SSQ-6 in our specific cohort resulted in a three-factor model with good construct validity and reliability. Additionally, the SSQ-6 may continue to serve as a research tool to measure social support among other cohorts of pregnant women, a population whose mental health is often at risk.
Acknowledgments
The authors wish to thank Ms Elena Sanchez and the dedicated staff members of Asociación Civil Proyectos en Salud (PROESA), Peru, and INMP, Peru, for their expert technical assistance with this research. This research was supported by awards from the National Institutes of Health (NIH), National Institute of Minority Health and Health Disparities (T37-MD-001449), and Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01-HD-059835). The NIH had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Author contributions
LEF, BG, and MAW conceived and designed the study. QYZ, AKMP, GFSM, and LEF analyzed data. AKMP, GFSM, and LEF drafted the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Cohen S, Gottlieb BH, Underwood LG. Social relationships and health. In: Cohen S, Underwood LG, Gottlieb BH, editors. Social Support Measurement and Intervention: A Guide for Health and Social Scientists. New York, NY: Oxford University Press; 2000:1–2. | ||
Orr ST. Social support and pregnancy outcome: a review of the literature. Clin Obstet Gynecol. 2004;47(4):842–855. | ||
Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav. 2011;52(2):145–161. | ||
Strom JL, Egede LE. The impact of social support on outcomes in adult patients with type 2 diabetes: a systematic review. Curr Diab Rep. 2012;12(6):769–781. | ||
Hernandez DC, Reitzel LR, Wetter DW, McNeill LH. Social support and cardiovascular risk factors among black adults. Ethn Dis. 2014;24(4):444–450. | ||
Mazzella F, Cacciatore F, Galizia G, et al. Social support and long-term mortality in the elderly: role of comorbidity. Arch Gerontol Geriatr. 2010;51(3):323–328. | ||
Aktan NM. Social support and anxiety in pregnant and postpartum women: a secondary analysis. Clin Nurs Res. 2012;21(2):183–194. | ||
Agostini F, Neri E, Salvatori P, Dellabartola S, Bozicevic L, Monti F. Antenatal depressive symptoms associated with specific life events and sources of social support among Italian women. Matern Child Health J. 2015;19(5):1131–1141. | ||
Heh SS. Relationship between social support and postnatal depression. Kaohsiung J Med Sci. 2003;19(10):491–496. | ||
Pagel MD, Smilkstein G, Regen H, Montano D. Psychosocial influences on new born outcomes: a controlled prospective study. Soc Sci Med. 1990;30(5):597–604. | ||
Feldman PJ, Dunkel-Schetter C, Sandman CA, Wadhwa PD. Maternal social support predicts birth weight and fetal growth in human pregnancy. Psychosom Med. 2000;63(5):715–725. | ||
Hetherington E, Doktorchik C, Premji SS, McDonald SW, Tough SC, Sauve RS. Preterm birth and social support during pregnancy: a systematic review and meta-analysis. Paediatr Perinat Epidemiol. 2015;29(6):523–535. | ||
Sarason IG, Sarason BR, Shearin EN, Pierce GR. A brief measure of social support: practical and theoretical implications. J Soc Pers Relat. 1987;4(4):497–510. | ||
Martínez-López Z, Páramo Fernández MF, Guisande Couñago MA, et al. Apoyo social en universitarios españoles de primer año: propiedades psicométricas del Social Support Questionnaire-Short Form y el Social Provisions Scale. [Social support in Spanish first year university students: Psychometrics properties of the Social Support Questionnaire-Short Form and the Social Provisions Scale]. Rev Lat Psic. 2014;46(2):102–110. Spanish. | ||
Morikawa M, Okada T, Ando M, et al. Relationship between social support during pregnancy and postpartum depressive state: a prospective cohort study. Sci Rep. 2015;5:10520. | ||
Friedman LE, Gelaye B, Rondon MB, Sanchez SE, Peterlin BL, Williams MA. Association of migraine headaches with suicidal ideation among pregnant women in Lima, Peru. Headache. 2016;56(4):741–749. | ||
Barrios YV, Gelaye B, Zhong Q, et al. Association of childhood physical and sexual abuse with intimate partner violence, poor general health and depressive symptoms among pregnant women. PLoS One. 2015;10(1):e0116609. | ||
Gelaye B, Barrios YV, Zhong QY, et al. Association of poor subjective sleep quality with suicidal ideation among pregnant Peruvian women. Gen Hosp Psychiatry. 2015;37(5):441–447. | ||
Sarason I, Levine H, Basham R, Sarason B. Assessing social support: The Social Support Questionnaire. J Personal Soc Psychol. 1983;44(1):127–139. | ||
Monteiro AP. Psychometric properties of a Russian version of the Social Support Questionnaire (SSQ6) in eastern European immigrants. Contemp Nurse. 2011;39(2):157–162. | ||
Rascle N, Bruchon-Schweitzer M, Sarason IG. Short form of Sarason’s Social Support Questionnaire: French adaptation and validation. Psychol Rep. 2005;97(1):195–202. | ||
Brown TA. Confirmatory Factor Analysis for Applied Research. New York, NY: Guilford Press; 2006. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.