Back to Journals » International Journal of Women's Health » Volume 17
Conservative Treatment of Third Trimester Appendicitis Misdiagnosed as Round Ligament Pain. A Case Report and Review of the Literature in a Resource-Limited Setting
Authors Hassan RA ![]() , Ali IA, Elmi AH
, Ali IA, Elmi AH ![]() , Omar AA
, Omar AA ![]()
Received 24 April 2025
Accepted for publication 31 July 2025
Published 4 August 2025 Volume 2025:17 Pages 2413—2420
DOI https://doi.org/10.2147/IJWH.S536394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Rayaan Abdirahman Hassan,1 Ismail A Ali,2 Abdullahi Hassan Elmi,3 Abdullahi Abdirahman Omar1
1Dr.Sumait Hospitals, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Surgery, Dr. Sumait Hospitals, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 3Department of Nursing and Midwifery, Dr. Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia
Correspondence: Rayaan Abdirahman Hassan, Email [email protected]
Introduction: Identifying acute appendicitis during pregnancy is particularly challenging, especially in the third trimester, as its symptoms may resemble typical gestational discomfort. While surgery remains the standard treatment, conservative treatment is being considered more often, especially when surgical intervention can pose risks to either the mother or the fetus.
Case Presentation: We report the case of a 30-year-old woman at 33 weeks of gestation who presented with right lower quadrant pain initially misattributed to round ligament strain. Her condition deteriorated over several days with worsening abdominal pain, fever, and leukocytosis. Imaging confirmed an acute uncomplicated appendicitis. After multidisciplinary evaluation and counseling, the patient declined surgery due to concerns over fetal safety. A conservative approach with intravenous antibiotics was initiated, resulting in complete clinical resolution. The patient delivered a healthy infant at term, without complications or recurrence.
Conclusion: This case demonstrates that conservative management of appendicitis during the third trimester can be a safe and effective alternative for highly selected patients. This underscores the importance of individualized care, shared decision-making, and close clinical monitoring, particularly when standard surgical treatment has declined. As the conversation around non-operative strategies evolves, this case adds meaningful support for expanding tailored management options during pregnancy in resource-limited settings.
Keywords: appendicitis in pregnancy, conservative management, third trimester, round ligament pain, non-operative treatment, maternal-fetal safety
Introduction
Acute appendicitis is the most frequently encountered non-obstetric surgical emergency during pregnancy and represents a key cause of acute abdominal pain in this population. It is defined as the inflammation of the vermiform appendix. It is reported to occur at a rate comparable to that in the general population, with an estimated incidence of 1 in 1,250–1 in 2,000 pregnancies.1,2 Diagnosing appendicitis in pregnancy is challenging because common symptoms like nausea, vomiting, and increased white blood cells often overlap with normal pregnancy changes.3,4
As the uterus grows, it pushes the appendix upward, changing where pain appears and making physical exams less reliable.5,6 Ultrasound is safe and commonly used, though it becomes less accurate later in pregnancy.7 MRI offers better accuracy, but access and cost can be limiting.8,9
Delays in diagnosis increase the risk of complications like perforation, which occurs in up to 43% of pregnant patients.10,11 Although maternal death is rare, it may still occur, especially with perforation or sepsis.8 Recently, non-surgical treatment with antibiotics has been considered in selected cases, particularly in late pregnancy to avoid surgical risks.12 On a global scale, appendicitis during pregnancy affects approximately 0.05% to 0.07% of women, with the second trimester showing the highest reported incidence.10,13 In the United States, it remains a leading indication for emergency surgical intervention among pregnant individuals.8
In recent years, there has been a growing interest in the non-operative management of acute appendicitis during pregnancy, particularly in the third trimester when surgical intervention may pose greater risks to both the mother and fetus. Emerging evidence, including studies by Nakashima et al14 and Ceresoli et al15 has demonstrated favorable outcomes in carefully selected patients managed conservatively with antibiotics alone. While current international guidelines do not universally recommend this approach, the accumulating data suggest it may represent a viable alternative in specific clinical contexts, especially where surgical access is limited or patient preference is a key consideration.
Data from middle-income countries such as Turkey report similar rates, with an incidence close to 1 in 1000.16 However, in resource-limited settings, diagnostic delays, limited imaging availability, and reduced access to multidisciplinary care are associated with increased maternal and fetal morbidity.17 In this case report, we describe a patient diagnosed with acute appendicitis at 33 weeks of gestation who was successfully treated with a conservative approach.
Case Presentation
A 30-year-old gravida 4, para 2+1 woman at 33 weeks and 2 days of gestation presented with a 3-day history of right lower quadrant abdominal pain accompanied by nausea and vomiting. On initial evaluation, her vital signs were stable, with a blood pressure of 105/67 mmHg, heart rate of 78 bpm, and a blood glucose level of 102 mg/dL. Obstetric ultrasound confirmed a viable singleton pregnancy in cephalic presentation, appropriate for the gestational age (Figure 1). Given the absence of alarming features and musculoskeletal distribution of pain, round ligament discomfort was considered the most likely cause, and the patient was discharged with paracetamol for symptomatic relief.
 |
Figure 1 Ultrasound showing a viable singleton fetus at 33 weeks’ gestation in cephalic presentation. |
Three days later, the pain worsened and was accompanied by persistent fever and constipation. Nausea persisted despite the administration of analgesia. There were no urinary symptoms, gastrointestinal bleeding, or signs of labor. The fetal movements remained reassuring. Notably, her medical history included a previous postpartum hemorrhage and second-trimester pregnancy loss.
Upon re-evaluation, the clinical picture changed. The temperature was elevated at 39.2°C, heart rate was 113 bpm, respiratory rate 28/min, and blood pressure dropped to 90/50 mmHg. Blood glucose remained stable at 95 mg/dL, and the neurological status was intact with a GCS score of 15/15. Abdominal examination revealed tenderness in the right lower quadrant and suprapubic region with a positive Rovsing’s sign. There was no rebound, guarding, costovertebral angle tenderness, or uterine fundal tenderness observed. The fetal heart tones were reactive, and no uterine contractions or cervical changes were noted. Laboratory tests showed leukocytosis (14.1 × 10[9]/L) and moderate anemia. Urinalysis and liver function test results were within normal limits. Viral screening results were negative (Table 1).
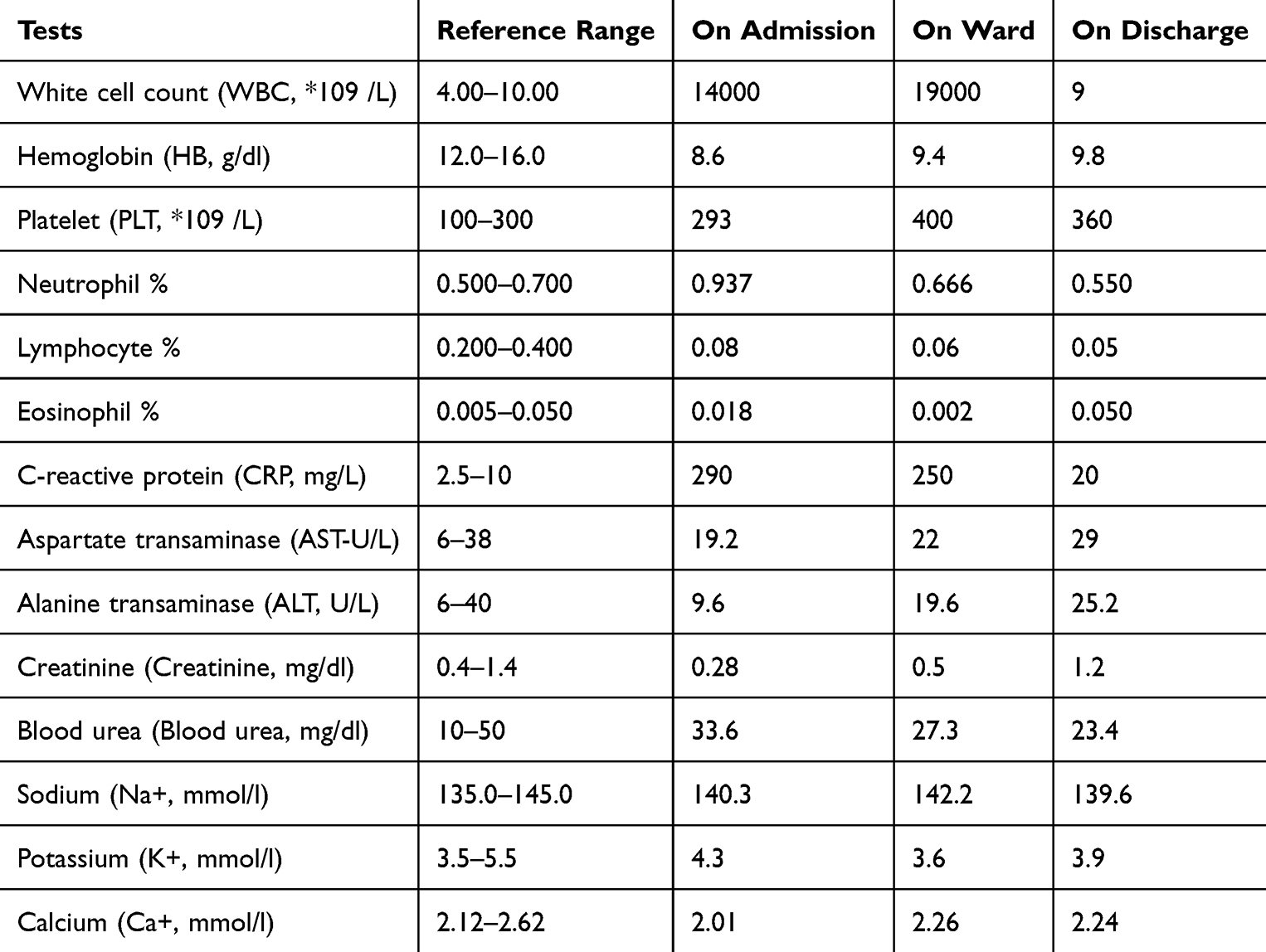 |
Table 1 The Laboratory Investigations Results |
A repeat abdominal ultrasound revealed a non-compressible, blind-ended tubular structure in the right iliac fossa measuring 16.2 mm in diameter, with surrounding free fluid findings consistent with acute appendicitis (Figure 2). Obstetric ultrasonography confirmed an appropriately grown fetus in the right occiput anterior position (Figure 3). The initial treatment was started at the emergency department include ceftriaxone 2 g intravenously for once then 1 g for twice daily at the ward and metronidazole 500 mg intravenously for once then 500 mg for three times a day at the ward, 1 liter for Ringer lactate intravenous fluid, paracetamol solution 1009 mg/100mL and super-hema oral Solution 5 mL at night. On hospital day 2 (33 + 4 weeks’ gestation) her white-blood-cell count rose slightly and right-lower-quadrant pain persisted. A bedside multidisciplinary review, involving the consultant obstetrician (chair), consultant general surgeon, anaesthesiologist, senior radiologist and ward general practitioner, recommended early appendectomy. The patient declined surgery because she feared losing her baby. As she remained haemodynamically stable and ultrasound showed a non-perforated appendix without abscess, the team continued conservative management, switching intravenous therapy from ceftriaxone to amoxicillin–clavulanate and maintaining close monitoring; the discussion and written consent were filed in the paper case notes.
 |
Figure 2 Abdominal ultrasound revealing a dilated, non-compressible appendix (16.2 mm) with surrounding free fluid, consistent with acute appendicitis. |
 |
Figure 3 Obstetric ultrasound confirming appropriate fetal growth and right occiput anterior position. |
At follow-up one-week post-discharge, she reported complete resolution of symptoms, except for mild residual cramping. Her pregnancy progressed uneventfully, and at 40 weeks, she had a spontaneous vaginal delivery of a healthy baby. Postpartum ultrasonography confirmed complete resolution (Figure 4), and surgical consultation concluded that no further intervention was necessary.
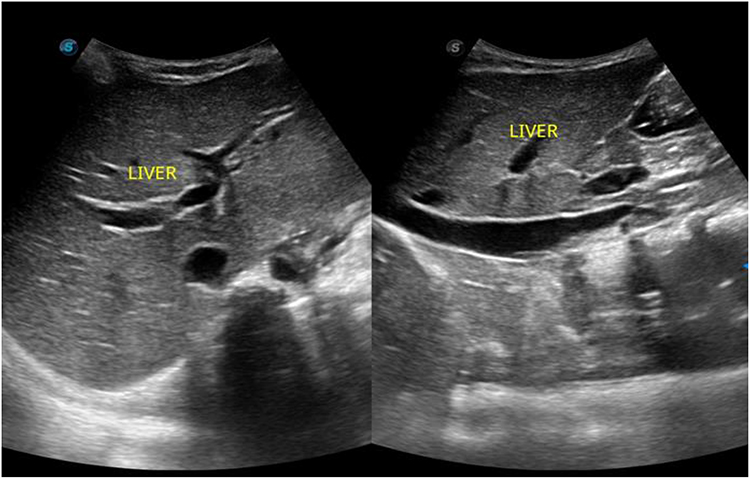 |
Figure 4 Postpartum ultrasound showing complete resolution of appendiceal inflammation. |
Discussion
This case highlights the potential of conservative management as a safe and effective alternative to surgery for treating acute appendicitis during the third trimester of pregnancy. At 33 weeks and 2 days of gestation, the patient presented with symptoms that closely mimicked common pregnancy-related discomfort, nausea, vomiting, and lower abdominal pain. These symptoms, often associated with benign causes, such as round ligament pain, make early diagnosis particularly difficult. As described in previous studies, the clinical presentation of appendicitis in pregnancy is frequently obscured by physiological changes during gestation, including leukocytosis and altered pain perception due to the anatomical displacement of the appendix by the enlarging uterus.10,18,19 In this case, the initial misdiagnosis and delayed diagnosis underscore the real-world challenges that clinicians face when evaluating abdominal pain in pregnant patients.
The choice to manage this patient conservatively was made following multidisciplinary discussions between the obstetrics and general surgery teams. Her stable condition, late gestational age, and clear ultrasound findings supported a non-operative approach. Additionally, the patient’s active involvement in the decision-making process, including her refusal of surgery due to concerns about fetal risk, was central. This case underscores the importance of collaborative care and shared decision-making in managing complex surgical conditions during pregnancy.
Non-operative treatment is best suited for hemodynamically stable patients with imaging-confirmed, uncomplicated appendicitis and no signs of peritonitis or systemic infection. Reliable access to follow-up care is also essential. In pregnancy, decisions should also consider gestational age, fetal status, and the risks of anesthesia and preterm labor. This case illustrates that when these criteria are met, conservative management can be safely pursued under close inpatient observation.
According to the 2020 guidelines by the World Society of Emergency Surgery (WSES), conservative management is not routinely recommended for appendicitis during pregnancy due to limited supporting evidence and concern for adverse outcomes.20 However, this case adds to a growing body of literature suggesting that in highly selected patients, especially those in late pregnancy who decline surgery or lack access to timely operative care, non-surgical management may still be considered under close clinical supervision.
What makes our case especially noteworthy is the combination of factors rarely reported: a third-trimester diagnosis of appendicitis initially mistaken for round ligament pain, refusal of surgery due to maternal preference, and complete clinical resolution through conservative treatment alone. While similar cases exist, few have documented successful outcomes with advanced gestational age (33+ weeks), and most include surgical backup plans or eventual appendectomy.13,21 Our case shows that full-term resolution without recurrence is achievable in highly selected patients, even when surgery is discontinued.
In this patient, ultrasonography confirmed a non-compressible, dilated appendix with peri-appendiceal fluid, consistent with acute appendicitis. Although MRI was not used in this case, it showed high diagnostic accuracy during pregnancy, with a sensitivity of 90–100% and specificity of 94–98%, making it a valuable second-line imaging modality when the ultrasound findings are inconclusive. However, access to MRI may be limited in resource-constrained settings, which can affect timely diagnosis and treatment decisions.22 CT scans, while highly sensitive, are generally avoided during pregnancy due to fetal radiation exposure concerns.19,22
In our setting, MRI was not pursued because of a combination of clinical certainty based on ultrasound findings, the patient’s stable condition, and local resource limitations, highlighting a common barrier in many low-income and middle-income countries.9,22 This underscores the importance of strong clinical judgment and the need for accessible diagnostic tools.
Surgical removal of the appendix has long been considered the standard approach for appendicitis during pregnancy, as it prevents progression to perforation, peritonitis, or sepsis, all of which pose serious risks to both the mother and the fetus.8,16 However, a growing body of evidence now supports the use of conservative (non-surgical) antibiotic treatment in selected cases, particularly in late pregnancy, when surgical intervention may increase the risk of preterm labor and fetal compromise.13–15,17 Recent studies reinforce the feasibility of this approach. Nakashima et al reported that among pregnant patients with appendicitis in Japan, those managed non-operatively had outcomes comparable to those of those who underwent appendectomy, with similar low rates of fetal loss and no maternal deaths. Similarly, a 2025 population-based analysis by Ceresoli et al concluded that nonoperative management can be a viable option in appropriately selected patients, potentially avoiding surgical complications and allowing for faster recovery.15
In our case, after a thorough multidisciplinary consultation and discussion of the risks and benefits, conservative management was pursued in light of the patient’s stable clinical status and preference to avoid surgery. The patient responded well to intravenous antibiotics, with gradual resolution of fever and pain. This outcome aligns with other reports demonstrating favorable maternal and fetal outcomes following conservative management during late gestation.17,22 For example, a similar case documented full resolution of appendicitis at 31 weeks of gestation with antibiotic therapy alone, supporting the feasibility of this approach in carefully monitored scenarios.13 Ajjarapu and Moreira recently described successful non-surgical management of a third-trimester appendicitis, resulting in symptom resolution and a term delivery without recurrence, further bolstering evidence for conservative management in well-selected patients.21
While conservative treatment during pregnancy has been described, most cases involve earlier gestational stages or include contingency plans for surgery. For instance, Edwardes and Sud reported conservative treatment at 31 weeks but maintained surgical readiness.13 Ajjarapu et al similarly documented symptom resolution without surgery, though they raised concerns about recurrence risk.21 In contrast, our patient was successfully managed medically through term without recurrence or complications, offering a unique insight into the feasibility of strictly non-surgical care in advanced pregnancy.
However, conservative management is not without risks. Delayed or failed antibiotic treatment can lead to disease progression, including perforation and sepsis, which dramatically increase morbidity.8,9 This caution is underscored by a recent national study of Cheng et al analyzed over 33,000 pregnancy admissions and found that non-operative management was associated with significantly higher odds of preterm labor and pregnancy loss compared to immediate appendectomy.23 For this reason, strict inpatient observation, availability of emergency surgical intervention, and close fetal monitoring are essential components of nonoperative management protocols. Moreover, patients must be carefully selected those with signs of complicated appendicitis, systemic instability, or equivocal imaging findings may not be suitable candidates for conservative treatment.8,9,16
Long-term considerations also include the potential for recurrence and the need for interval appendectomy. Although our patient remained stable throughout the remainder of her pregnancy and postpartum period, we maintained a close follow-up to confirm full resolution, as recommended in similar reports of conservative management.9,17 The absence of recurrence and successful term delivery in this case further supports the role of conservative therapy as a viable option in appropriately selected patients.
This case underscores the diagnostic challenges of acute appendicitis in late pregnancy, where symptoms may closely resemble benign conditions like round ligament pain, contributing to delayed recognition. In select cases during the third trimester, when surgical intervention is declined and imaging confirms an uncomplicated presentation, conservative management may offer a safe and effective alternative. A multidisciplinary approach, vigilant clinical monitoring, and shared decision-making centered around the patient’s values and clinical stability are critical to achieving favorable non-operative outcomes especially in low resources setting.
This single-patient case limits generalizability and lacks long-term follow-up to assess recurrence risk. Conservative management was guided by patient preference and clinical stability in a resource-limited setting, which may not be applicable universally. The absence of MRI also restricted diagnostic precision.
Future studies should include larger cohorts with extended follow-up to assess outcomes and recurrence. In low-resource settings, we recommend the development of context-specific protocols and multicenter registries to guide safe, selective use of conservative management in pregnancy-related appendicitis.
The patient remained clinically stable throughout the remainder of her pregnancy and achieved a full-term vaginal delivery without complications. Postpartum ultrasonography confirmed complete resolution of the appendiceal inflammation. Although the potential for recurrence exists with conservative treatment, particularly in the absence of interval appendectomy, this case demonstrated that with appropriate monitoring, favorable long-term outcomes are achievable.
Conclusion
While appendectomy remains the standard treatment for appendicitis during pregnancy, this case illustrates that conservative, non-operative management may be a safe and effective alternative in highly selected third trimester patients. Our experience emphasizes the value of multidisciplinary teamwork, shared decision-making, and personalized care tailored to maternal preferences and clinical context. With growing global interest in non-surgical strategies, this case supports the need for prospective studies, multicenter registries, and structured guidelines to better define criteria and optimize outcomes for conservative management of appendicitis during pregnancy, not as an exception but as a valid treatment pathway.
Abbreviations
Mg/dL, milligrams per deciliter; MRI, Magnetic Resonance Imaging; CT, computed tomography.
Ethics and Consent
Written informed consent was obtained from the patient, who specifically requested the publication of this case report along with related images. Ethical approval was not required for case reports according to the guidelines of our institution.
Acknowledgments
We are deeply grateful to the Center for Research and Development at SIMAD University for their invaluable support and constructive recommendations throughout this work. We also extend our sincere thanks to Dr. Ismail Ahmed Ali for his expert guidance and thoughtful contributions, which have greatly enriched the development of this case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. Upadhyay A, Stanten S, Kazantsev G, Horoupian R, Stanten A. Laparoscopic management of a nonobstetric emergency in the third trimester of pregnancy. Surg Endosc. 2007;21:1344–1348. doi:10.1007/s00464-007-9280-1
2. Brown JJ, Wilson C, Coleman S, Joypaul BV. Appendicitis in pregnancy: an ongoing diagnostic dilemma. Colorectal Dis. 2009;11:116–122. doi:10.1111/j.1463-1318.2008.01599.x
3. Kammere WS. Non-obstetric surgery in pregnancy. Med Clin North Am. 1987;71:551–560. doi:10.1016/S0025-7125(16)30639-9
4. Weingold AB. Appendicitis in pregnancy. Clin Obstetr Gynecol. 1983;26:801–809. doi:10.1097/00003081-198312000-00006
5. Babaknia A, Parsa H, Woodruff JD. Appendicitis during pregnancy. Obstetr Gynecol. 1977;50:40–44.
6. Tamir IL, Bongard FS, Klein SR. Acute appendicitis in the pregnant patient. Am J Surg. 1990;160(6):571–575. doi:10.1016/S0002-9610(05)80546-6
7. Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in pregnant women: value of sonography. AJR. 1992;159:539–542. doi:10.2214/ajr.159.3.1503032
8. Dongarwar D, Taylor J, Ajewole V, et al. Trends in appendicitis among pregnant women, the risk for cardiac arrest, and maternal–fetal mortality. World J Surg. 2020;44(11):3999–4005. doi:10.1007/s00268-020-05663-7
9. Burcu B, Ekinci O, Atak T, et al. Acute appendicitis in pregnancy: case series and review. Northern Clin Istanbul. 2016;3(1):60–63. doi:10.14744/nci.2016.55943
10. Andersen B, Nielsen TF. Appendicitis in pregnancy: diagnosis, management and complications. Acta Obstetricia et Gynecologica Scandinavica. 1999;78:758–762. doi:10.1034/j.1600-0412.1999.780907.x
11. Yilmaz HG, Akgun Y, Bac B, Celik Y. Acute appendicitis in pregnancy: risk factors associated with principal outcomes. Int J Surg. 2007;5(3):192–197. doi:10.1016/j.ijsu.2006.03.005
12. Ball E, Waters N, Cooper N, et al. Evidence-based guideline on laparoscopy in pregnancy. Facts Views Vision ObGyn. 2019;11(1):5–25.
13. Edwardes C, Sud V. Conservative versus surgical management of appendicitis during pregnancy. J Nuffield Dept Surg Sci. 2020.
14. Tanrıdan Okcu N, Banlı Cesur İ, Irkörücü O. Acute appendicitis in pregnancy: 50 case series, maternal and neonatal outcomes. Ulusal Travma ve Acil Cerrahi Dergisi. 2021;27(2):255–259. doi:10.14744/tjtes.2020.47583
15. Davoodabadi A, Davoodabadi H, Akbari H, et al. Appendicitis in pregnancy: presentation, management and complications. Zahedan J Res Med Sci. 2016;18(7):e7557. doi:10.17795/zjrms-7557
16. Yavuz Y, Şentürk M, Gümüş T, Patmano M. Acute appendicitis in pregnancy. Ulusal Travma ve Acil Cerrahi Dergisi. 2021;27(1):85–88. doi:10.14744/tjtes.2020.03842
17. Murariu D, Tatsuno B, Hirai CM, Takamori R. Case report and management of suspected acute appendicitis in pregnancy. Hawaii Med J. 2011;70:30–32.
18. Konrad J, Grand D, Lourenco A. MRI: first-line imaging modality for pregnant patients with suspected appendicitis. Abdominal Imaging. 2015;40(8):3359–3364. doi:10.1007/s00261-015-0514-4
19. Nakashima M, Takeuchi M, Kawakami K. Clinical outcomes of acute appendicitis during pregnancy: conservative management and appendectomy. World J Surg. 2021;45(6):1717–1724. doi:10.1007/s00268-020-05949-w
20. Di Saverio S, Podda M, De Simone B. et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(27). doi:10.1186/s13017-020-00306-3
21. Ajjarapu A, Moreira NN. Successful non-surgical management of acute, uncomplicated appendicitis in pregnancy: a case report. Proc Obstetr Gynecol. 2020;9(3):Article8. doi:10.17077/2154-4751.1460
22. Ceresoli M, Rigamonti V, Fama I, et al. Operative and non-operative management of acute appendicitis during pregnancy: a population-based study. Arch Gynecol Obstetrics. 2025;311(1):33–42. doi:10.1007/s00404-024-07238-6
23. Cheng V, Ashbrook M, Youssefzadeh AC, et al. Management for acute uncomplicated appendicitis during pregnancy: national trends and patient outcomes. Ann Surg. 2023;278(6):932–936. doi:10.1097/SLA.0000000000005678
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.