Back to Journals » Open Access Emergency Medicine » Volume 17
Conservative Management of Perforated Duodenal Diverticulum: A Case Report and Narrative Review
Authors Mazahreh TS ![]() , Afaneh MW
, Afaneh MW ![]() , Husein A
, Husein A ![]()
Received 25 June 2025
Accepted for publication 5 November 2025
Published 14 November 2025 Volume 2025:17 Pages 345—352
DOI https://doi.org/10.2147/OAEM.S547882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Amit Agrawal
Tagleb S Mazahreh, Mohammed W Afaneh, Anas Husein
Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science and Technology, King Abdullah University Hospital (KAUH), Irbid, 22110, Jordan
Correspondence: Tagleb S Mazahreh, Email [email protected]
Abstract: Duodenal diverticular disease is a common finding in the general population and most individuals, in fact, remain asymptomatic. However, duodenal diverticular perforation is an occasional unfortunate endpoint that carries significant morbidity, and mortality rates and requires a particular attention and a wise judgement whether to liberally interfere surgically or to stay more conservative.In this writing, we describe a case of a 45-year-old male with a perforated duodenal diverticulum that presented in a stable general condition and was successfully managed conservatively, sparing the patient a particularly morbid surgical intervention. Perforated duodenal diverticula, though rare, can be managed conservatively in stable patients without signs of sepsis or generalized peritonitis. Conservative treatment, including intravenous antibiotics, bowel rest, and nasogastric suction, can be effective and avoid the morbidity associated with surgery. In our case, conservative management led to significant improvement, underscoring the importance of individualized treatment plans and close monitoring to decide on the necessity of surgical intervention.Conservative management of perforated duodenal diverticula should be considered in selected patients who fulfill the general settled criteria. Nevertheless, an individualized approach is recommended and escalating up the invasiveness of interventions may seem vital at any time during treatment.
Keywords: duodenal diverticulum, perforation, conservative management, case report
Introduction
The duodenum is the second most common site for intestinal diverticula, typically discovered incidentally as most patients are asymptomatic. However, complications occur in about 1–5% of cases and may include obstruction of the pancreas, duodenum or biliary tract as well as perforation or bleeding.1 This clinical heterogenicity presents a fundamental management challenge, regarding the appropriate timing for surgical intervention versus when conservative care can prevent harm.
Duodenal diverticula appear as saccular outpouchings and may contain gas, fluid, contrast material, or food debris.2
Perforation of duodenal diverticula is associated with a high mortality rate reported in 3–30% of cases. Although duodenal diverticula are rare, their incidence may reach to 22% based on findings from autopsy and endoscopic retrograde cholangiopancreatography (ERCP) studies. The prevalence increases with age, affecting 10–27% of individuals over the age of 50.3 Duodenal diverticula are either congenital (true) or acquired with acquired forms being more common. True diverticula involve all layers of the duodenal wall, mucosa, submucosa, muscaris and serosa. While acquired diverticula result from the mucosa and submucosa pushing through weak points in the muscular layer, where mesenteric vessels pass.4 Perforation of duodenum diverticula results from their thin walls, with most cases occurring along the medial wall of the second portion of the duodenum typically within 2 cm of the ampulla of Vater.5 It can be challenging to differentiate between perforated duodenal ulcer and perforated duodenal diverticulum in the diagnosis and can be differentiated mainly through the location of perforation.6
The mainstay approach in managing perforated duodenal diverticula once establishing the diagnosis is surgical treatment using the Stapled or hand-sewn diverticulectomy.7 Other studies have used laparoscopic diverticulectomy, or patch reinforcement using the omentum, or retroperitoneum drainage.8 Conservative management for perforated duodenal diverticulum is mainly a choice in patients at high surgical risk such as older adults and those with significant comorbidities.9 Conservative management includes hydration, intravenous antibiotics, bowel rest, and nasogastric suction.10
Case Presentation
A 45-year-old male, who was previously healthy with no reported chronic medical or surgical history, presented to the emergency department with one-day duration of periumbilical abdominal pain that started suddenly and progressed since. It was sharp, continuous and gradually became diffused all over the abdomen. There was no associated nausea, vomiting, diarrhea or fever. However, he reported constipation for a few days. By that time, both upper and lower respiratory symptoms had disappeared.
On arrival at our tertiary hospital, he was conscious, alert and oriented. He had stable vital signs with a low-grade fever of 37.5-degrees Celsius and a heart rate of 115 beats-per-minute. He was normotensive, not tachypneic with normal O2-saturation. The abdomen was soft, non-distended with localized tenderness in the epigastric region, showing no peritoneal signs.
Laboratory tests showed elevated inflammatory markers with leukocytosis of 12,000 per milliliter, neutrophilia and a C-reactive protein (CRP) of 84 milligrams-per-liter. Amylase and lipase levels were within normal as were the kidney and liver function tests.
Abdominal and chest X-rays were unremarkable. Computed tomography (CT) scan with intravenous and oral contrast revealed complete midgut non-rotation with an outpouching seen bulging from the mesenteric side of the second part of duodenum containing gas and bowel content, associated with thickened enhancing edematous wall and surrounding fat stranding. A duodenal wall defect at the same site was noted, connected to an extraluminal peri-duodenal fluid collection of about 5×3 centimeters. There was no evidence of free intraperitoneal air or lymphadenopathy, and a diagnosis of duodenal diverticulitis complicated by a contained retroperitoneal perforation was concluded (Figure 1).
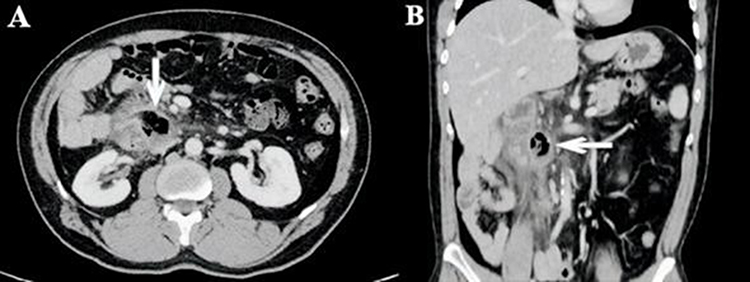 |
Figure 1 Outpouching at the mesenteric side of the second portion of the duodenum, with associated wall enhancement and a defect in continuity with retroperitoneal collection containing gas and fluid, along with surrounding fat stranding. Arrows point to collection in continuation with the diverticulum. (A): Axial view; (B): Coronal view. |
Contrast fluoroscopic follow-through study was attempted to ensure containment and self-drainage of the collection but could not be completed due to patient’s non-cooperation.
After resuscitation, a decompressive nasogastric tube (NG) was inserted, and the patient was admitted, assigned nothing-by-mouth and closely observed on the floor. Intravenous (IV) broad-spectrum antibiotic coverage with imipenem was chosen and maximum-dose IV omeprazole was given.
Over a period of five days of observation, the patient remained stable and improved significantly. Fever and tachycardia are both resolved by day two of admission. Abdominal tenderness ceased gradually and disappeared on day two. NG tube was removed on day two. The white blood cells (WBC) normalized, and the neutrophilia diminished on day one and remained so throughout the observation period. The CRP initially increased to 239 during the first two days and then gradually returned to normal levels over one week.
On the third day of admission, a follow-up CT scan was done to assess the adequacy of our approach. It showed a remarkable improvement in the inflammatory changes. The fluid collection decreased in size down to about 2cm X 1.5cm, suggesting a self-draining contained collection (Figure 2).
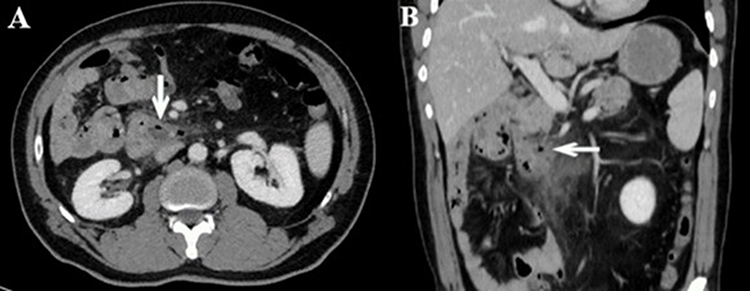 |
Figure 2 Marked improvement with a decreased collection size and surrounding inflammatory changes. Arrows point to collection in continuation with the diverticulum.(A): Axial view; (B): Coronal view. |
Oral fluid intake was resumed on day five of admission and slowly advanced to regular diet thereafter. We felt that parenteral nutrition was not needed due to the good nutritional status of the patient, his young age and the expected short period of fasting. He was discharged in good shape after a total of seven days of hospitalization and completed a ten-days course of oral antibiotics.
On follow-up visit at the outpatient clinic one week after discharge, the patient was doing very well. An additional CT scan, approximately 5 weeks from the event, documented a well-sealed diverticulum with no oral contrast leak. He had a near total resolution of collection, with minimal remaining inflammation (Figure 3).
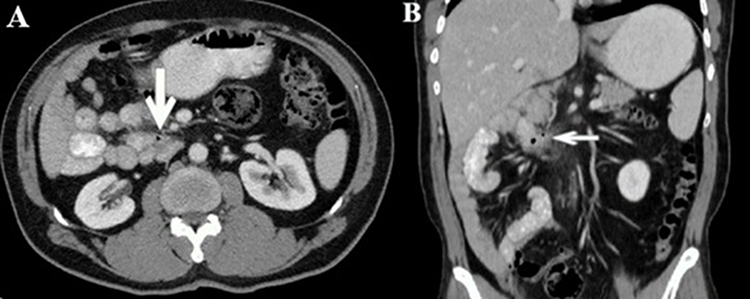 |
Figure 3 A well-sealed duodenal diverticulum with resolved inflammation and absence of oral contrast leak. Arrows point to the diverticulum.(A): Axial view; (B): Coronal view. |
A contrast fluoroscopic study (small bowel follow through) was done, which confirmed a lack of contrast leak from the duodenum (Figure 4). On endoscopy, deformed duodenal first and second parts were noticed and a scar of a previous ulcer within the second part was observed. The diverticulum could not be seen on the forward-viewing endoscope.
 |
Figure 4 Contrast fluoroscopic study confirming absence of contrast leak from the duodenum on lateral view. |
In the next section, we detailed principal information obtained from the literature about duodenal diverticular disease and its possible complications, namely, perforation. We then outline the management options, delineating precisely when and how each option can be implemented judiciously in treating these patients.
Discussion
In this case, the decision to pursue conservative management was based on a structured clinical assessment and multidisciplinary discussion. The patient presented hemodynamically stable, without signs of sepsis, generalized peritonitis, or free intraperitoneal air, all key factors that reduce the urgency for surgical intervention. Laboratory markers showed inflammation but no evidence of organ dysfunction, and imaging confirmed a contained retroperitoneal perforation rather than free leakage. Additionally, the patient’s relatively young age, absence of significant comorbidities, and favorable clinical trajectory after initial resuscitation supported a trial of non-operative management. Consideration of resource availability and the potential morbidity associated with duodenal surgery further supported the choice of a conservative approach. This reasoning highlights the importance of individualized assessment rather than defaulting to surgical exploration in all cases.
Epidemiology and Anatomy
Duodenal diverticular disease is a relatively common condition, especially in older adults with no difference in occurrence between males and females.11 It was first described by a pathologist in the eighteenth century and later reported by a radiologist nearly 200 years afterward.12 It is considered the most common intestinal diverticular disease after colonic diverticula, with an estimated prevalence of 5–22% based on findings from endoscopy, contrast imaging and autopsy studies.13 Among its types, intraluminal congenital diverticula are rare and occur because of abnormal embryologic development such as duodenal webs or strictures.3 Diverticula are most commonly found on the concave surface of the second part of duodenum (D2), near the major duodenal papilla, and may be single or multiple. Less frequently, they are seen in the third (D3), first (D1), and fourth (D4) parts of the duodenum, with convex surface of D2 being the least common site.14 It can be classified as either congenital or acquired based on etiology. Congenital diverticula are true diverticula, containing all the layers of the duodenal wall. They are further subdivided into intraluminal or extraluminal types based on their structure.3 Acquired extraluminal diverticula, which represents most duodenal diverticula, and like those in the colon, are the result from prolapse of mucosa and submucosa through a focal weakness in the muscular layer at the points where the feeding vessels enter. Acquired diverticula can also develop as a consequence of gallstones, cholecystitis and peptic ulcer disease.15
Clinical Presentation and Diagnosis
Although duodenal diverticula are common, most patients are diagnosed incidentally and remain asymptomatic throughout their lives. These typically require no intervention.11 However, a minority of 5–10% manifest clinical symptoms.13 Most symptomatic diverticula are within the D2 boundaries.3 Symptoms may arise due to inflammation, ulceration, erosion leading to upper gastrointestinal bleeding, small intestinal bacterial overgrowth, obstruction of biliopancreatic ducts, enterolith formation causing duodenal obstruction, or even perforation (6). Symptoms are typically nonspecific and may include abdominal or back pain, vomiting and fever which can mimic a variety of other abdominal pathologies.13 Perforation is exceptionally rare and most commonly occurs due to duodenal diverticulitis. Duodenal diverticulitis is less common when compared to its colonic counterpart. This is thought to be due to the higher luminal flow rate of duodenal contents, a lower bacterial load, and the typically larger size of duodenal diverticula.3 Perforation can also result from iatrogenic trauma, including endoscopy and retroperitoneal surgeries, external abdominal trauma, ulcer formation, ingestion of foreign material and back-pressure from distal intestinal obstruction.16 Another cause could be the presence of ectopic pancreatic tissue within diverticulum.17 Diagnosing duodenal diverticulitis and perforation can be difficult because the retroperitoneal position of most of the duodenum often masks peritoneal signs.18 However, diagnosis can be achieved using various imaging modalities. Computed tomography (CT) with intravenous and oral contrast is considered the gold standard due to its high accuracy. On CT, diverticula typically appear as contrast-filled outpouchings of the duodenum and may contain air, fluid, air-fluid level or food debris.2 They can mimic pancreatic or biliary cysts but are best distinguished using magnetic resonance cholangiopancreatography (MRCP). On CT, Diverticulitis typically appears as duodenal wall thickening of more than or equal to 4mm, along with mesenteric or retroperitoneal fat stranding.19 On endoscopy, the presence of mucosal edema and erythema along with purulent discharge from the diverticulum is virtually diagnostic of diverticulitis.20 Perforation is indicated by the presence of extraluminal air in the retroperitoneum or less commonly, within the peritoneal cavity, often accompanied by free fluid collection.3 Micro perforation refers to a well contained perforation demonstrated by the presence of air bubbles outside the bowel lumen without any associated fluid collection.13
Management Options and Selection Criteria
Management options include conservative, endoscopic and surgical approaches, and to date, there is still no strong evidence to support one option over the other.10 Factors that support an initial trial of conservative management include older age, significant comorbidities, hemodynamic stability, presence of micro perforations, and absence of peritonitis, sepsis or free intraperitoneal air. A step-up approach can be considered at any stage if the patient’s condition worsens or fails to improve.12 Conservative management includes bowel rest, intravenous broad-spectrum antibiotics, proton pump inhibitors, nasogastric decompression and total parenteral nutrition as needed.21 Regular physical examinations and monitoring of inflammatory markers through laboratory tests are essential. Follow-up imaging should be considered if there is any clinical deterioration.22 Additionally, interventional radiology and endoscopy services should be readily available for drainage, as abscess formation is a potential complication with this approach.10 In fact, this more conservative approach has gained attention in recent years to avoid invasive intervention that could increase the risk of morbidity and mortality.1 Since many years, over 200 cases have been reported with more than 30 successfully treated patients without surgery.23 The first case managed non-operatively was documented in 1963 by Shackleton.5 These cases provide valuable insights that support initially adopting a conservative approach in clinically appropriate sittings, like the management of perforated duodenal ulcers and colonic diverticula.24 Nevertheless, surgical exploration, whether open or laparoscopic, should be considered whenever the diagnosis is uncertain or the clinical status worsens while the patient is on conservative management.10 The type of surgical intervention depends on the clinical status of the patient and the intraoperative findings including the site of perforation, the size of the defect relative to the diameter of the involved duodenal segment, and the severity of contamination.10 A variety of surgical techniques have been described in the literature including drainage procedures, diverticulectomy, duodenectomy, pancreaticoduodenectomy and several types of diversion procedures.25 It is worth mentioning that diverticulectomy with primary repair or drainage has been the most used approach in various studies.23 Endoscopic drainage and transluminal irrigation have been shown to be effective in a few reported cases.18 Endoscopically placed naso-biliary and naso-pancreatic drains have previously been used as complementarily alongside surgery.26 In addition, the novel Endoscopic Negative Pressure Vacuum Therapy has been successfully implemented in several cases.21
While this case does not introduce a novel strategy, it highlights the practicality of clinical decision-making in resource-limited settings and supports the principle that management must be individualized rather than protocol-driven. It demonstrates how conservative treatment can remain a viable and effective option when surgical risk is high, when resources are constrained, or when the disease process is contained and closely monitored. By reflecting on the reasoning process, this report adds value beyond the clinical outcome itself, showing how thoughtful patient selection and regular reassessment can achieve favorable results while minimizing unnecessary interventions.
Clinical Implications and Practical Framework
This case underlines the importance of individualized care in managing perforated duodenal diverticulum, particularly in patients who are hemodynamically stable and show no signs of generalized peritonitis. It reinforces the need for careful patient selection, structured monitoring, and timely escalation when necessary. A stepwise approach not only minimizes the risks associated with surgical intervention but also tailors treatment to the patient’s condition and available resources. Importantly, this strategy is highly relevant in older adults or in settings where surgical capacity is limited, where conservative management can be both safe and effective.
Complications and Outcomes
Complications of duodenal diverticulitis with or without perforation, and regardless of whether managed conservatively surgically, may include gastrointestinal bleeding, infection with intrabdominal abscess formation, fistula formation, portal vein thrombosis, pyelophlebitis, sepsis, or even death.20 The overall mortality rate following duodenal diverticular perforation is estimated to range between 6% and 20%.21
Perforated duodenal diverticulum can be successfully managed in stable patients through conservative measures through continuous clinical and laboratory monitoring. This case underscores the importance of selection criteria, serial assessment and imaging review to prevent unnecessary surgical interventions while maintaining patient safety.
Conclusion
Perforated duodenal diverticulum, though rare and potentially life threatening, can be effectively managed conservatively in carefully selected patients. In the absence of sepsis, generalized peritonitis, or hemodynamic instability, conservative treatment including bowel rest, nasogastric decompression, intravenous antibiotics, and proton pump inhibitors combined with close clinical, laboratory, and imaging monitoring can lead to full recovery while avoiding the risks associated with surgery. Continuous reassessment is essential, and escalation to surgical intervention should remain an option if the patient’s condition worsens.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the patient. Following the HIPPA guidelines, IRB approval was not necessary due to the nature of the study being a case report.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editorial office upon request.
Funding
No funding was received for this manuscript.
Disclosure
The authors confirm that there is no conflict of interest to declare regarding this work.
References
1. Kim KH, Park SH. Conservative treatment of duodenal diverticulitis perforation: a case report and literature review. Oaem. 2018;10:101–104. doi:10.2147/OAEM.S168487
2. Radiopaedia EM. Duodenal diverticula | radiology Case | radiopaedia.org. Available from: https://radiopaedia.org/cases/duodenal-diverticula-6?lang=us.
3. A systematic review of the perforated duodenal diverticula: lessons learned from the last decade. Langenbecks Arch Surg. 2022;407(1)
4. Lamb R, Kahlon A, Sukumar S, Layton B. Small bowel diverticulosis: imaging appearances, complications, and pitfalls. Clin. Radiol. 2022;77(4):264–273. doi:10.1016/j.crad.2021.12.003
5. Degheili JA, Abdallah MH, Haydar AA, Moukalled A, Hallal AH. Perforated duodenal diverticulum treated conservatively: another two successful cases. “Case Report. Surg. 2017;2017:4045970. doi:10.1155/2017/4045970
6. Farné G, Lauro A, Vaccari S, et al. Spontaneous perforated duodenal diverticulum: wait or cut first? Dig Dis Sci. 2021;66:2876–2880. doi:10.1007/s10620-021-07092-1
7. Boot M, Chew K, Archer J, Sowter S, Bergamin P. Iatrogenic duodenal diverticulum perforation: a systematic review. ANZ J Surg 2023 https://consensus.app/papers/iatrogenic-duodenal-diverticulum-perforation-a-boot-chew/4d51c8e8167753858ea8a1a0e3798d09/..
8. Laparoscopic duodenal segmental resection and duodenojejunostomy for symptomatic duodenal diverticula in three cases treated at a community hospital. J Minim Invasive Surg. 24. 1. https://pubmed.ncbi.nlm.nih.gov/35601280/.
9. Sasaki Y, Nakahodo J, Onishi T, et al. Duodenal diverticular perforation treated conservatively: reassessing indications for treatment. Internal Medicine. 2023;62(22):3327. doi:10.2169/internalmedicine.1211-22
10. Franken R, Möllers M, Otterloo A, Puylaert J. Nonoperative management of perforated diverticulitis of the duodenum: report of three cases and review of literature. “Case Report. Surg. 2021;2021:6647470. doi:10.1155/2021/6647470
11. Ren J, Ding J, Su T, et al. Evaluation and management of symptomatic duodenal diverticula: a single-center retrospective analysis of 647 patients. Front Surg. 2023;10:1267436. doi:10.3389/fsurg.2023.1267436
12. K A, EH E, Ar A, et al. Surgical approach for duodenal diverticulum perforation: a case report. Int. J. Surg. Case Rep. 2020. https://pubmed.ncbi.nlm.nih.gov/33049647/.
13. Aljabri WA, Hasosah M, AlMehdar A, Bakhsh D, Alturkistany FO. Duodenal diverticulosis as an unusual cause of severe abdominal pain. Cureus. 2020;12(9):e10586. doi:10.7759/cureus.10586
14. Presence of duodenal diverticula in cadaveric study – European Journal of Anatomy. Available from: https://eurjanat.com/articles/presence-of-duodenal-diverticula-in-cadaveric-study/.
15. K E, G S, C D, F I, R M. Perforated duodenal diverticulitis: a case report of a rare surgical entity treated by roux-en-y deriving intestinal patch. Cureus. 2022;14(3). doi:10.7759/cureus.29717
16. Khan K, Saeed S, Maria H, et al. Duodenal diverticular perforation after small bowel obstruction: a case report. “Case Report. Surg. 2018;2018:6197828. doi:10.1155/2018/6197828
17. Tsukihara S, Onda S, Son K, et al. Laparoscopic surgery for duodenal perforation due to a diverticulum with heterotopic pancreas: a case report. Surgical Case Reports. 2022;8:106. doi:10.1186/s40792-022-01460-3
18. Vasin D, Mijovic K, Pavlovic A, Stanic D, Tomic T. Retroperitoneal duodenal diverticulum microperforation: the role of computed tomography. Cureus. 2024;16(7):e65494. doi:10.7759/cureus.65494
19. Salgado D, Kang J, Costa AF. Mimics of pancreatic neoplasms at cross-sectional imaging: pearls for characterization and diagnostic work-up. Curr. Probl. Diagn. Radiol. 2025;54(3):382–391. doi:10.1067/j.cpradiol.2024.12.002
20. Ryou S, Nam K, Kim J. Duodenal diverticulitis accompanied by portal vein thrombosis treated with endoscopic therapy. Korean J Gastroenterol. 2021;78(2):129–133. doi:10.4166/kjg.2021.054
21. Endoscopic negative pressure therapy as stand-alone treatment for perforated duodenal diverticulum: presentation of two cases. BMC Gastroenterol. 21. 1. https://pubmed.ncbi.nlm.nih.gov/34802417/.
22. The challenging diagnosis and treatment of duodenal diverticulum perforation: a report of two cases. BMC Gastroenterol. 20. 1. https://pubmed.ncbi.nlm.nih.gov/31914931/.
23. Perforated duodenal diverticulum successfully treated with a combination of surgical drainage and endoscopic nasobiliary and nasopancreatic drainage: a case report. Surgical case reports.6;1
24. Philip J, Cocieru A. Pancreatoduodenectomy in patient with perforated duodenal diverticulum and peritonitis: case report. Int. J. Surg. Case Rep. 2019;58:48. doi:10.1016/j.ijscr.2019.04.011
25. Perforated duodenal diverticulum with postoperative diverticulum bleeding successfully treated using transcatheter arterial embolization. Cureus. 13. 9. https://pubmed.ncbi.nlm.nih.gov/34722030/.
26. Duodenal diverticulitis accompanied by abscess formation treated successfully using an endoscopic nasobiliary drainage catheter: a case report. Clin J Gastroenterol. 10. 3. https://pubmed.ncbi.nlm.nih.gov/28321821/
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gallbladder Perforation with Choledochogastric Fistula Due to Ascaris Infestation, a Case Report

Amsalu A, Molla Y
International Medical Case Reports Journal 2023, 16:443-447
Published Date: 2 August 2023