Back to Journals » International Medical Case Reports Journal » Volume 19
Conservative Management of Intrastromal Corneal Ring Segment Extrusion Using Suture-Assisted Repositioning: A Case Series
Authors Warrak J, Tlaiss Y ![]() , Tarchichi A, Warrak E
, Tarchichi A, Warrak E
Received 4 March 2026
Accepted for publication 10 April 2026
Published 10 July 2026 Volume 2026:19 604746
DOI https://doi.org/10.2147/IMCRJ.S604746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
John Warrak, Yehya Tlaiss, Alaa Tarchichi, Elias Warrak
Department of Ophthalmology, University of Balamand, Beirut, Lebanon
Correspondence: Yehya Tlaiss, Email [email protected]
Purpose: To describe a conservative surgical technique for managing Intrastromal Corneal Ring Segment (ICRS) extrusion using suture-assisted repositioning and to report clinical outcomes in a small case series.
Methods: This retrospective case series of two eyes (two patients) included eyes with keratoconus that developed recurrent ICRS extrusion despite exhaustive conservative management, including bandage contact lens use, topical antibiotic and corticosteroid therapy, and manual repositioning. Suture-assisted repositioning was performed after exclusion of active infection, corneal melting, or stromal perforation. Following manual repositioning of the segment into its original stromal tunnel, interrupted 10– 0 nylon sutures (Sharpoint™, Ref A9003N, Ultraglide Spatula needle, 3/8c 6.15mm; Surgical Specialties Corporation) were placed anterior to mid-stromally to mechanically stabilize the overlying corneal tissue. Postoperative management included topical antibiotics, corticosteroids, and prolonged bandage contact lens use. Clinical outcomes, epithelial healing, complications, and ICRS retention were assessed during follow-up. Given the descriptive nature of this case series and the small sample size (n=2), no formal statistical analysis was performed. Follow-up visits were conducted at 1 month, 2– 3 months, and then at 5– 6 months post-procedure, with additional visits as clinically indicated.
Results: Two eyes of two patients were treated using suture-assisted repositioning. Complete and sustained epithelial healing was achieved in both cases, with no recurrence of segment exposure during follow-up. One eye required a single suture, while the other required two sutures due to greater biomechanical instability. Sutures were retained for approximately 5– 6 months and removed after long-term epithelial stability was confirmed. Visual acuity and corneal topography remained stable, and the corneal reshaping effect of the ICRS was preserved. No intraoperative or postoperative complications, including infection, stromal melting, or endothelial compromise, were observed.
Conclusion: Suture-assisted repositioning of extruding ICRS represents a minimally invasive, tissue-sparing alternative to explantation in carefully selected cases. This technique may allow durable epithelial healing and preservation of corneal biomechanics while avoiding immediate segment removal. Larger studies with longer follow-up are warranted to further evaluate its role in the management of ICRS extrusion.
Keywords: intracorneal ring segments, ICRS extrusion, keratoconus, suture-assisted repositioning, conservative surgical management, Intrastromal Corneal Ring Segment
Introduction
Intrastromal Corneal Ring Segment (ICRS) are an established surgical option for the management of corneal ectatic disorders, particularly keratoconus, where they improve corneal regularity, reduce refractive error, and delay or obviate the need for keratoplasty.1 Despite their overall safety profile, ICRS implantation is associated with a spectrum of postoperative complications, among which segment extrusion remains one of the most visually and structurally significant.2–4
ICRS extrusion typically results from a combination of biomechanical instability, progressive stromal thinning, superficial tunnel placement, and chronic epithelial breakdown overlying the segment.5,6 Once exposure occurs, the compromised epithelial barrier increases the risk of infection, stromal melting, and irreversible corneal damage.7 Consequently, ICRS explantation is frequently recommended as the definitive management strategy, particularly in cases of recurrent exposure or failed conservative therapy.
However, removal of an ICRS may lead to loss of the corneal reshaping effect, progression of ectasia, and deterioration in visual function, especially in eyes that have limited remaining therapeutic options.6 In such cases, the decision to explant the segment represents a trade-off between preventing sight-threatening complications and preserving corneal biomechanics. While conservative measures such as bandage contact lens use, topical antibiotics and corticosteroids, and manual repositioning are commonly attempted, these strategies often provide only temporary epithelial healing, with a high risk of recurrent re-exposure.
Despite the clinical relevance of this dilemma, there is a paucity of literature describing structured, reproducible conservative surgical approaches aimed at salvaging extruding ICRS without resorting to explantation. Previous reports have largely focused on segment removal, tunnel revision, or subsequent keratoplasty, with limited emphasis on techniques that mechanically stabilize the overlying corneal tissue to promote durable epithelial healing while maintaining the segment in situ.8–11
In this context, suture-assisted repositioning of extruding ICRS represents a logical yet underreported strategy. By providing localized mechanical support to the area of epithelial breakdown and stabilizing the repositioned segment within its original stromal tunnel, suturing may facilitate sustained epithelial closure and prevent recurrent extrusion, thereby preserving the intended biomechanical and refractive benefits of the ICRS.
The purpose of this study is to describe a conservative surgical technique of suture-assisted ICRS repositioning and to report clinical outcomes in a small case series. Unlike previously described approaches — which have largely focused on segment removal, tunnel revision, or keratoplasty — the technique presented here offers a structured, reproducible method of mechanically stabilizing the extruding segment in situ using anterior stromal suturing. This approach aims to offer an alternative to explantation in carefully selected patients, expanding the therapeutic armamentarium for the management of ICRS extrusion and addressing a gap in the current literature regarding conservative surgical salvage options.
The mechanism of focal ICRS exposure and the key steps of the suture-assisted repositioning technique are summarized in Figure 1.
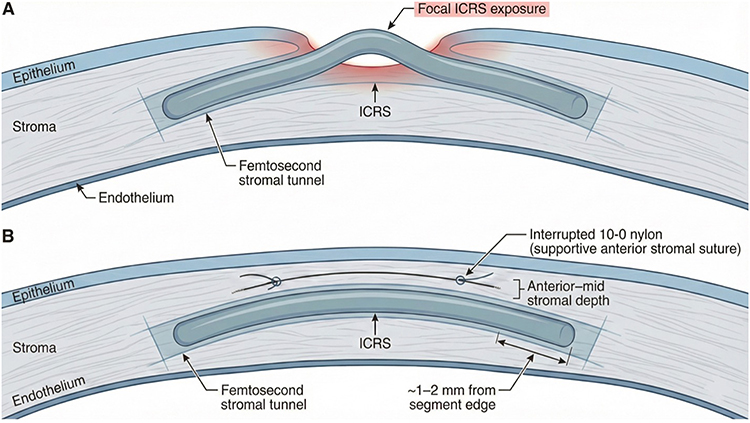 |
Figure 1 Schematic illustration of focal Intrastromal Corneal Ring Segment (ICRS) exposure and the suture-assisted repositioning technique. (A) Focal ICRS exposure overlying the femtosecond-created stromal tunnel. (B) Interrupted 10–0 nylon supportive anterior stromal suture placed at anterior–mid stromal depth approximately 1–2 mm from the segment edge to re-bury the ICRS and support epithelial closure. |
Results
Patient Characteristics
Two eyes of two patients with keratoconus who developed recurrent ICRS extrusion despite conservative management were included. In both cases, extrusion occurred in the absence of active infection or corneal melting. Prior to suture-assisted repositioning, multiple conservative measures—including bandage contact lens use, topical antibiotic and corticosteroid therapy, and manual repositioning of the ICRS—had failed to prevent recurrent exposure.
Baseline patient and segment characteristics are summarized in Table 1.
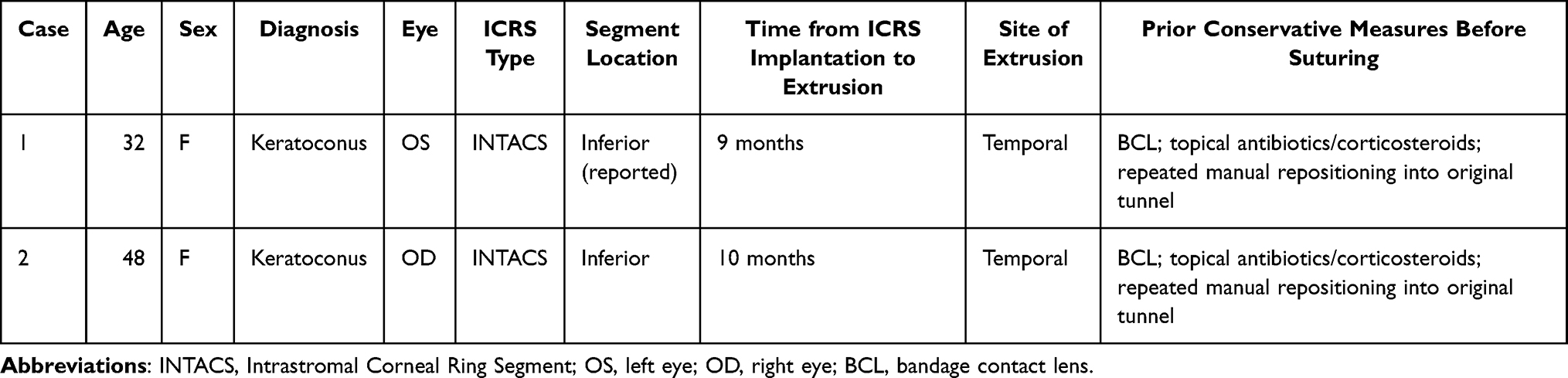 |
Table 1 Baseline Patient and Intrastromal Corneal Ring Segment Characteristics |
Clinical Course and Epithelial Healing
Following suture-assisted repositioning, complete epithelial closure was achieved in both cases. No further episodes of segment re-exposure were observed during the follow-up period. Bandage contact lenses were maintained until stable epithelial healing was confirmed and exchanged at regular intervals.
In Case 1, epithelial stability was achieved and maintained with a single interrupted suture. The suture was retained for approximately 5–6 months and removed after sustained epithelial integrity was documented.
In Case 2, due to greater biomechanical instability and recurrent prior exposure, two vertically stacked interrupted 10–0 nylon sutures (Sharpoint™, Ref A9003N; Surgical Specialties Corporation) were required. The immediate postoperative slit-lamp appearance in Case 2, with the supportive sutures in situ and the ICRS re-buried, is shown in Figure 2. One suture was removed earlier, while the final suture was removed at approximately 5 months following placement. After suture removal, slit-lamp examination in Case 2 confirmed stable epithelial closure with the segment retained in situ (Figure 3). Clinical course, epithelial healing, postoperative management, and complications are summarized in Table 2.
 |
Table 2 Clinical Outcomes Following Suture-Assisted ICRS Repositioning |
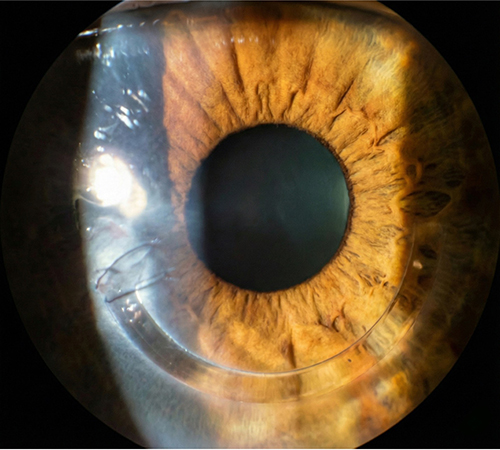 |
Figure 2 Postoperative slit-lamp photograph immediately after suture-assisted (ICRS = Intrastromal Corneal Ring Segment) repositioning, showing the interrupted 10–0 nylon supportive anterior stromal suture with the segment re-buried within the stromal tunnel. |
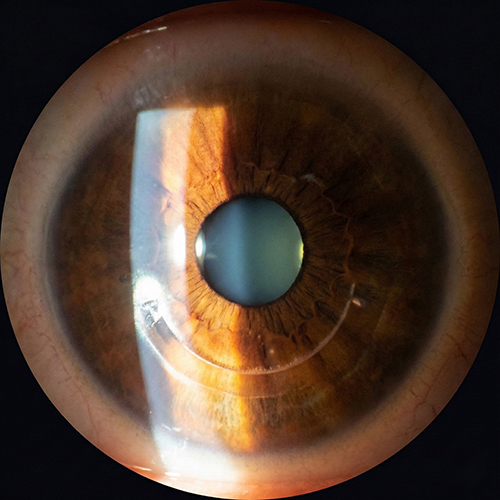 |
Figure 3 Slit-lamp photograph after suture removal, demonstrating stable epithelial closure with the intracorneal ring segment retained in situ and no recurrent exposure. |
Visual and Topographic Outcomes
Throughout follow-up, visual acuity and corneal topography remained stable in both cases, with preservation of the corneal reshaping effect achieved by the ICRS. No clinically significant deterioration in uncorrected or corrected distance visual acuity was observed following suturing or after suture removal.
Corneal topographic parameters, where available, demonstrated no progression of ectasia following the procedure. The ICRS remained well positioned within the original stromal tunnel, without migration or re-extrusion. Visual acuity and corneal tomographic parameters before and after intervention are summarized in Table 3.
 |
Table 3 Visual and Corneal Parameters Before and After Suture-Assisted Repositioning |
Complications
No intraoperative complications occurred. During the postoperative period, no cases of infectious keratitis, stromal melting, endothelial compromise, or significant inflammatory reaction were observed. Both eyes tolerated prolonged suture retention without adverse events.
A summary of clinical outcomes and follow-up duration is provided in Table 2.
Discussion
ICRS extrusion remains one of the most challenging complications following implantation, often forcing clinicians to choose between repeated conservative measures with limited durability and definitive explantation with potential loss of biomechanical and refractive benefit.7 In this case series, suture-assisted repositioning provided sustained epithelial stability and successful retention of the ICRS without progression to infection, stromal melting, or keratoplasty, suggesting that this approach may represent a viable conservative surgical alternative in carefully selected cases.
Clinical Rationale and Mechanism
The pathogenesis of ICRS extrusion is multifactorial, involving progressive stromal thinning, localized biomechanical stress, superficial tunnel positioning, and chronic epithelial breakdown. Once exposure occurs, epithelial instability perpetuates a cycle of inflammation and mechanical trauma, predisposing to recurrent re-extrusion despite temporary healing with bandage contact lenses or topical therapy. While manual repositioning of the segment can restore its position transiently, lack of mechanical stabilization of the overlying corneal tissue often results in recurrence.
Suture-assisted repositioning addresses this limitation by providing localized mechanical support over the area of maximal vulnerability, effectively redistributing stress away from the segment edge and allowing sustained epithelial closure. By anchoring the corneal tissue anterior to the repositioned ICRS, suturing promotes epithelial healing while preserving the segment within its original stromal tunnel, thereby maintaining the intended corneal reshaping effect.
Comparison with Existing Management Strategies
Traditional management of ICRS extrusion has favored explantation, particularly in cases of recurrent exposure or failed conservative therapy.1,6 Although explantation reliably eliminates the risk of infection, it may precipitate loss of refractive benefit, ectatic progression, and the need for subsequent keratoplasty, especially in advanced keratoconus.9 Alternative strategies described in the literature—including tunnel revision, segment exchange, or lamellar grafting—are more invasive and not universally applicable.7,12
In contrast, the technique described in this series represents a minimally invasive, reversible, and tissue-sparing approach. Importantly, suturing does not preclude future explantation or keratoplasty if required, but rather serves as an intermediary step aimed at salvaging the segment in the absence of infection or melt.
Clinical Decision-Making Framework
Based on our experience, suture-assisted repositioning may be most appropriate in eyes with recurrent ICRS exposure despite conservative management, where the stromal tunnel remains intact and no active infection or corneal melting is present. Conversely, eyes with active keratitis, progressive stromal thinning, or impending perforation should proceed directly to explantation.2 The number of sutures required should be individualized, with greater biomechanical instability or recurrent exposure favoring multiple anchoring points to improve load distribution.
Safety Considerations
A potential concern with this approach is prolonged suture retention in a compromised cornea. However, in both cases presented, sutures were well tolerated over several months without evidence of infection, inflammation, or endothelial compromise. Careful placement of anterior to mid-stromal sutures, avoidance of deep stromal penetration, and meticulous postoperative management are essential to minimizing risk. In both cases, strict sterile surgical technique was observed throughout the procedure. Postoperatively, patients received topical fluoroquinolone antibiotics for a minimum of four weeks and were monitored closely for early signs of infectious keratitis or stromal melt. Bandage contact lenses were exchanged at regular intervals under aseptic conditions to reduce the risk of microbial colonization. Patients were educated regarding the signs of infection — including increased redness, pain, or discharge — and instructed to present immediately for evaluation if any such symptoms developed. These combined measures likely contributed to the absence of infectious or inflammatory complications in this series.
Limitations
The primary limitations of this study include its small sample size and retrospective nature. Quantitative topographic and biomechanical data were limited, and longer-term follow-up is necessary to determine the durability of this technique over years rather than months. Anterior segment optical coherence tomography (AS-OCT) imaging before and after the procedure was not performed in these cases; future reports should include AS-OCT documentation to provide additional objective evidence of stromal tunnel integrity and suture positioning. Additionally, this approach may not be applicable to all cases of ICRS extrusion, particularly those associated with advanced ectasia or active inflammatory disease.
Conclusions and Clinical Implications
Suture-assisted repositioning of extruding ICRS offers a conservative surgical option that may preserve corneal integrity and refractive benefit while avoiding immediate explantation. In carefully selected patients, this technique can expand the management spectrum of ICRS extrusion and may delay or obviate the need for more invasive interventions.
Ethics Statement
Institutional Review Board approval to publish this case series was per institutional policy at the University of Balamand was not required. Written informed consent was obtained from both patients for publication of their clinical details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. D’Oria F, Abdelghany AA, Ledo N, Barraquer RI, Alio JL. Incidence and reasons for intrastromal corneal ring segment explantation. Am J Ophthalmol. 2021;222:351–8. doi:10.1016/j.ajo.2020.09.041
2. Ibáñez-Alperte J, Pérez-García D, Cristóbal JA, Mateo AJ, Río BJ, Mínguez E. Keratitis after implantation of intrastromal corneal rings with spontaneous extrusion of the segment. Case Rep Ophthalmol. 2010;1(2):42–46. doi:10.1159/000320585
3. Ambrósio R, Salomão MQ, Barros L, et al. Multimodal diagnostics for keratoconus and ectatic corneal diseases: a paradigm shift. Eye Vis. 2023;10(1):45. doi:10.1186/s40662-023-00363-0
4. D’Oria F, Bagaglia SA, Alio Del Barrio JL, Alessio G, Alio JL, Mazzotta C. Refractive surgical correction and treatment of keratoconus. Surv Ophthalmol. 2024;69(1):122–139. doi:10.1016/j.survophthal.2023.09.005
5. D’Oria F, Alio JL, Martinez-Abad A, Izquierdo L, Larco P, Abdelghany AA. Astigmatic change as a predictor of intrastromal corneal ring segment late extrusion. J Cataract Refract Surg. 2022;48(4):401–407. doi:10.1097/j.jcrs.0000000000000774
6. Bautista-Llamas MJ, Sánchez-González MC, López-Izquierdo I, et al. Complications and explantation reasons in intracorneal ring segments (ICRS) implantation: a systematic review. J Refract Surg. 2019;35(11):740–747. doi:10.3928/1081597X-20191010-02
7. Mounir A, Farouk MM, Abdellah MM, Mohamed Mostafa E. Extrusion of femtosecond laser-implanted intrastromal corneal ring segments in keratoconic eyes: prevalence, risk factors, and clinical outcomes. J Ophthalmol. 2020;2020:8704219. doi:10.1155/2020/8704219
8. Struckmeier AK, Hamon L, Flockerzi E, Munteanu C, Seitz B, Daas L. Femtosecond laser and mechanical dissection for ICRS and MyoRing implantation: a meta-analysis. Cornea. 2022;41(4):518–537. doi:10.1097/ICO.0000000000002937
9. Nguyen N, Gelles JD, Greenstein SA, Hersh PS. Incidence and associations of intracorneal ring segment explantation. J Cataract Refract Surg. 2019;45(2):153–158. doi:10.1016/j.jcrs.2018.09.021
10. Nuzzi R, Tripoli F, Rossi A, Ghilardi A. A combined procedure of intrastromal corneal rings explantation and penetrating keratoplasty in a patient with keratoconus: a case report. Front Med Lausanne. 2022;9:853702. doi:10.3389/fmed.2022.853702
11. Sheludchenko VM, Osipyan GA, Khraystin K, Dzhalili RA, Abukerimova AK. Glubokaya perednyaya posloinaya keratoplastika pri ekstruzii nepolnogo intrastromal’nogo kol’tsa (klinicheskoe nablyudenie) [Deep anterior lamellar keratoplasty in extrusion of an incomplete intrastromal corneal ring segment (clinical observation)]. Vestn Oftalmol. 2023;139(1):75–79. doi:10.17116/oftalma202313901175
12. Daoud RC, Sammouh FK, Baban TA, Warrak JE, Warrak EL. Allogenic corneal tissue transplantation in substitution for extruded intracorneal rings: a case series. J Fr Ophtalmol. 2019;42(10):1090–1093. doi:10.1016/j.jfo.2019.05.028
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.