Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Consequences of Canada’s Drug Agency Reimbursement Recommendations for New Medicines and Pan-Canadian Pharmaceutical Alliance Price Negotiations on Patient Access
Authors Rawson NSB ![]()
Received 16 September 2025
Accepted for publication 4 December 2025
Published 23 December 2025 Volume 2025:17 Pages 975—989
DOI https://doi.org/10.2147/CEOR.S567932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xing Lin Feng
Nigel SB Rawson1– 4
1Independent Researcher, Saskatoon, SK, Canada; 2Macdonald-Laurier Institute, Ottawa, ON, Canada; 3Canadian Health Policy Institute, Toronto, ON, Canada; 4Fraser Institute, Vancouver, BC, Canada
Correspondence: Nigel SB Rawson, Email [email protected]
Introduction: Prescription drugs are excluded from Canada’s federal legislation covering health care. Each provincial government has developed its own drug plan. To get new prescription medicines listed in these plans, developers must pass regulatory review, health technology assessment and price negotiation, and convince individual government plans to list their drugs. The objective of this research is to assess how many reimbursement recommendations issued by Canada’s Drug Agency (CDA) have clinical and/or price conditions and what the consequences are.
Methods: Data were obtained on drugs with CDA recommendations issued between January 2020 and December 2024, together with dates of price negotiations between the pan-Canadian Pharmaceutical Alliance (pCPA) and manufacturers by the end of July 2025 and listings in government plans relating to the same drugs by early November 2025.
Results: Of 344 CDA recommendations, only three (0.9%) were unconditional reimbursement, 291 (84.6%) reimbursement with clinical criteria and/or a price condition, and 50 (14.5%) no reimbursement. Median time for CDA reviews was 221 days (interquartile range (IQR): 199– 282 days). Where recommended to achieve cost-effectiveness of $50,000/quality-adjusted life-year, median reduction was 74.5% (IQR: 50.0%-90.0%). Median time for the pCPA to decide whether to negotiate was 128 days (IQR: 73– 191 days) and median negotiation time was 131 days (IQR: 82– 219 days). The median time between submission to CDA and pCPA outcome was 518 days (IQR: 394– 633 days). Government drug plan listing rates for drugs successfully negotiated with the pCPA ranged from 58.6% to 91.6%. Five patients had prior-authorization requests to a private insurer for costly drugs denied because the drugs had conditional CDA recommendations.
Conclusion: CDA and pCPA processes take considerable time and listing decisions by government drug plans add extra time before potential access by patients. Nearly all CDA reimbursement recommendations, which are intended for government drug plans (not private payers), are conditional.
Plain Language Summary: The purpose of this work is to evaluate how many recommendations for coverage of new medicines were issued between 2020 and 2024 by Canada’s Drug Agency (CDA), which assesses the cost-effectiveness of drugs for coverage by government drug plans (except Quebec’s), and examine the time taken by CDA to do its work. The time taken by the pan-Canadian Pharmaceutical Alliance (pCPA), which negotiates drug prices with manufacturers for all government drug plans, to perform its activities is also evaluated, as is how many drugs were actually listed by these drug plans. Almost all CDA recommendations to cover drugs are conditional on clinical criteria for how the drugs should be used and/or a price reduction condition. Price reduction recommendations are substantial (half are more than 74%). CDA took longer than its target time of up to 180 days in 98% of its reviews. The pCPA took much longer than its performance target to decide whether to negotiate with drug developers for almost 80% of the drugs and exceeded its target time to negotiate for 51%. Government drug plans are not required to cover drugs that have successfully passed CDA and pCPA processes and, consequently, listing rates in the plans ranged from 58.6% to 91.6% by early November 2025. CDA and pCPA processes take considerable time and listing decisions by government drug plans add extra time before potential access by patients. Although not designed to do so, CDA recommendations can influence access decisions by adjudicators for private drug plans.
Keywords: health technology assessment, drug price negotiation, government drug plan coverage, private insurance, Canada
Introduction
Canada is not a unitary country but a federation of 10 provinces and three territories. Its federal government claims the country has a “universal”, publicly-funded health care system.1 However, the federal legislation that tries to ensure a comparable standard of care for all residents without financial barrier only covers access to medically necessary hospital and physician services, and the actual delivery of these services is the responsibility of provincial and territorial governments.
Drugs prescribed in the ambulatory setting are excluded from the legislation. Consequently, each provincial and territorial government has established its own public drug plan and the federal government has created the Non-Insured Health Benefits (NIHB) plan for First Nations and Inuit.2,3 Provincial and territorial plans vary widely in structure and funding, leading to differences in which residents are eligible, methods for cost-sharing between patients and government, and the number and types of drugs included in their benefit lists.4–6 All have programs for seniors, low-income individuals and patients with chronic conditions, while some offer broader coverage; all require residents to share the cost of medicines via copayments and/or a deductible amount that must be paid by the patient before drug costs are covered partially or fully. Some provinces also have an annual premium. The result is a patchwork of drug coverage and payment methods that has been described as a postal code lottery, meaning access depends on where a patient lives. For years, calls have been made for national pharmacare and the federal government has taken a small step with bilateral agreements with three provinces and one territory covering contraceptives and older diabetic medications.7 With no additional money allocated in the 2025 federal budget for agreements with other jurisdictions8 and the current uncertain state of the Canadian economy,9 a comprehensive national pharmacare program is unlikely in the foreseeable future.
To get new prescription medicines to Canadians through government drug plans, developers must pass several gatekeeping organizations. These comprise Health Canada, which provides regulatory review and approval of new drugs;10 the Institut national d’excellence en santé et services sociaux (INESSS) and Canada’s Drug Agency (CDA) that, respectively, perform health technology assessments for government drug plans in Quebec and the rest of Canada;11,12 the pan-Canadian Pharmaceutical Alliance (pCPA), which negotiates prices with drug developers on behalf of all government plans;13 the Patented Medicine Prices Review Board, which assesses whether patented medicine prices are excessive;14 and individual government drug plans that decide whether to add new medicines to their benefit lists. Most countries with public health care systems have health technology assessment agencies, but usually only one.15,16 None have an organization comparable with the Patented Medicine Prices Review Board, which is almost obsolete.17
CDA makes non-binding reimbursement recommendations to government drug plans and cancer agencies based on reviews and re-analyses of submissions from biopharmaceutical developers to reimburse medicines without conditions, reimburse with clinical criteria and/or conditions, or no reimbursement. Clinical recommendations may include criteria for treatment initiation, renewal and discontinuation and the specialty of physicians that should prescribe the medication, while price reduction conditions are almost always intended to achieve a quality-adjusted life-year (QALY) cost of CAN$50,000.18–21 After CDA issues a recommendation, the developer may be invited by the pCPA into a collective price negotiation with some or all government drug plans; it is thought that all plans participate in negotiations for new medicines, especially costly ones. If an agreement is successfully negotiated, a letter of intent is signed implying the drug will be listed in any subsequent agreement with participating government plans with an established price and listing criteria. However, government plans are not mandated to reimburse medicines successfully negotiated with the pCPA but can negotiate further with manufacturers before deciding whether or not to list new drugs.
Private health insurance is popular among Canadians. Before the 1970s, the need was because government plans did not exist.22 Over time, private health benefits were negotiated as part of employment agreements, instead of salary increases, or to provide recruitment incentives. There is also a tax incentive because the cost of private health benefits is not taxable federally or provincially, except in Quebec. Today, about two-thirds of Canadians have access to private insurance through their own or a family member’s plan paid entirely by the insured person or cost-shared with an employer or union to which they belong.23 Private drug insurance remains popular, particularly among working-age Canadians24 because some government plans do not cover them, and because government plans commonly have more restrictive benefit lists than private plans.25 There are now more than 145 health benefit providers in Canada and thousands of private plans with varying levels of drug coverage depending on how much individuals, employers and unions are willing to pay.23 Little is publicly available about the structure of private plans or their cost-control mechanisms.26
CDA recommendations and pCPA negotiations are intended for the drug plans of the governments that own, fund and manage these agencies. Some private payers may refer to CDA recommendations to guide their assessments of drugs, define prior-authorization criteria, or make coverage decisions. However, government plans serve different population segments and aim to provide economic prescription drug coverage within health care budgets. Private insurance should assess and cover drugs based on their impact on payers’ mainly working-age members to promote a healthy and productive workforce.
Nevertheless, one adjudicator, Cubic Health’s Facet program,27 which manages prior-authorization requests for expensive medications for the health and benefit plans of over one million Canadians in a variety of trade and professional unions across the country, uses CDA recommendations to approve or deny these requests. For example, one trade union’s benefit plan states “specialized or new drugs may require pre-approval by Facet” and that a specific prior-authorization medication may not be covered if it “has not received an unconditional recommendation for listing by the Canadian Agency for Drugs and Technologies in Health [now CDA] or a similar independent health technology assessment agency based on concerns around safety and/or clinical effectiveness and/or cost-effectiveness”.28 Health benefit plans for the faculty associations of two major universities (Universities of British Columbia and Alberta), the Ontario school education sector, and CUPE Ontario Education Workers have the same adjudicator for prior-authorization requests.29–32
The objective of this analysis is to assess how many CDA reimbursement recommendations issued between 2020 and 2024 have clinical criteria regarding treatment initiation and who should prescribe the medicine and/or price reduction conditions and what their consequences are with regard to price negotiations, listing in government drug plans, and how long processes take. An additional objective was to attempt to examine the consequences of Cubic Health’s Facet program on prior-authorization requests.
Materials and Methods
Data on reimbursement recommendations – submission and final report dates, the recommendation, any criteria regarding treatment initiation and who should prescribe the medicine, and any price reduction condition – issued between January 2020 and December 2024 were downloaded from CDA’s reimbursement review reports webpage, together with the date on which Health Canada approved the drug for use.33 Information available at the end of July 2025 on price negotiations between the pCPA and developers, including dates when negotiations began and ended or a decision was made not to pursue a negotiation, relating to the CDA recommendations were transcribed by the author from the pCPA’s brand name drug negotiations status list.34
Benefit lists of all provincial plans and the NIHB federal plan were reviewed by the author to identify whether the drugs were listed by the early November 2025.35–45 Oncology drugs are listed in the formularies of New Brunswick, Newfoundland and Labrador, Nova Scotia, Prince Edward Island and the NIHB, while Alberta, British Columbia, Ontario and Saskatchewan have separate cancer drug formularies.46–49 Manitoba’s cancer drug formulary is not publicly available, but additional information on oncology and non-oncology drugs can be obtained from the province’s bulletin archive.50 Relevant orphan medicines in current bilateral agreements between provinces and the federal government as part of the National Strategy for Drugs for Rare Diseases were included.51
To evaluate listing in government drug plans, CDA recommendations with no pCPA record and those with an active pCPA negotiation or under consideration for negotiation were excluded. COVID-19 medicines tend to be dealt with differently and were also excluded. In addition, where there was more than one recommendation with the same diagnosis (eg when a drug initially received a negative recommendation but a later submission received a positive one) or when successive submissions led to a widening of the drug’s indication, only the latest recommendation was included. Lastly, drugs with a concluded pCPA negotiation (successful or not) or a decision by the pCPA not to negotiate dated after March 31, 2025 were also excluded to allow a minimum time of seven months for listing decisions to be made.
Specific aims with regard to government drug plans were to evaluate:
- Rate of CDA recommendations issued between 2020 and 2024 with treatment initiation or prescribing criteria and/or price reduction conditions.
- Percentage price reductions recommended by CDA to achieve a cost-effectiveness threshold of $50,000 per QALY gained.
- Time taken by CDA to perform evaluations.
- Any association between recommended price reductions and pursuing price negotiations.
- Time taken by the pCPA to decide whether to invite drug developers to negotiate and time for negotiations.
- Outcomes of any price negotiations between the pCPA and drug developers.
- Listing of drugs in government benefit lists and any association with price recommendations.
Comparisons of these factors were performed between positive and negative reimbursement recommendations and between three mutually exclusive drug groups: oncology, orphan, and other drugs. Orphan drugs were those for non-oncology disorders with a prevalence of less than one per 2000 individuals using information from the Orphanet database52 or, if necessary, relevant publications. Statistical comparisons were performed using Mann–Whitney and Kruskal–Wallis tests.53
An additional objective was to see whether patients with prior-authorization requests for expensive medicines denied by the Cubic Health Facet program could be identified. The 32 patient support groups that are members of the Best Medicines Coalition (BMC)54 were asked by BMC’s executive director whether any of the groups’ members had reported receiving a denial letter for a prior-authorization request for an expensive drug from a private insurer or an adjudicator acting on their behalf due to a policy that limits reimbursement to drugs with an unconditional CDA recommendation.
Results
CDA Assessments
Between January 2020 and December 2024, CDA issued 344 recommendations for submissions from drug developers for 242 unique medicines or combinations of drugs (Supplementary Table 1). More than 75% of the medicines had one recommendation, 16.9% had two, and the rest had between three and 15. Fourteen applications (4.1%) were categorized as resubmissions or reassessments by CDA, while another 12 (3.5%) appeared to be resubmissions but were not classified as such. Submissions to CDA can be made up to 180 days before regulatory approval from Health Canada is anticipated; 189 (54.9%) were submitted in this way (median time before Health Canada approval: 127 days; interquartile range (IQR): 164 to 73 days before approval), while 155 (45.1%) were submitted after regulatory approval (median time after approval: 153 days; IQR: 61 to 494 days).
The CDA recommendation was “reimburse” without any specified clinical criteria or price reduction condition for three (0.9%) of the 344 recommendations. In the other 341 recommendations, 291 (84.6%) were to reimburse with clinical criteria and/or price reduction conditions and 50 (14.5%) were to not reimburse. Thus, 291 of the 294 (99.0%) CDA recommendations to reimburse the drug were conditional on clinical and/or cost reduction criteria.
Of the 294 positive recommendations, 13 (4.4%) had clinical criteria, 18 (6.1%) had price reduction conditions, 260 (88.4%) had both, and three (1.0%) had neither (Table 1). Sixteen (5.4%) of the 294 recommendations had no mention of a price reduction condition, while 44 (15.0%) had a non-specific price reduction condition. In the remaining 234 recommendations (79.6%), a percentage reduction to achieve $50,000 per QALY gained was specified, with a median reduction of 74.5% (IQR: 50.0% to 90.0%).
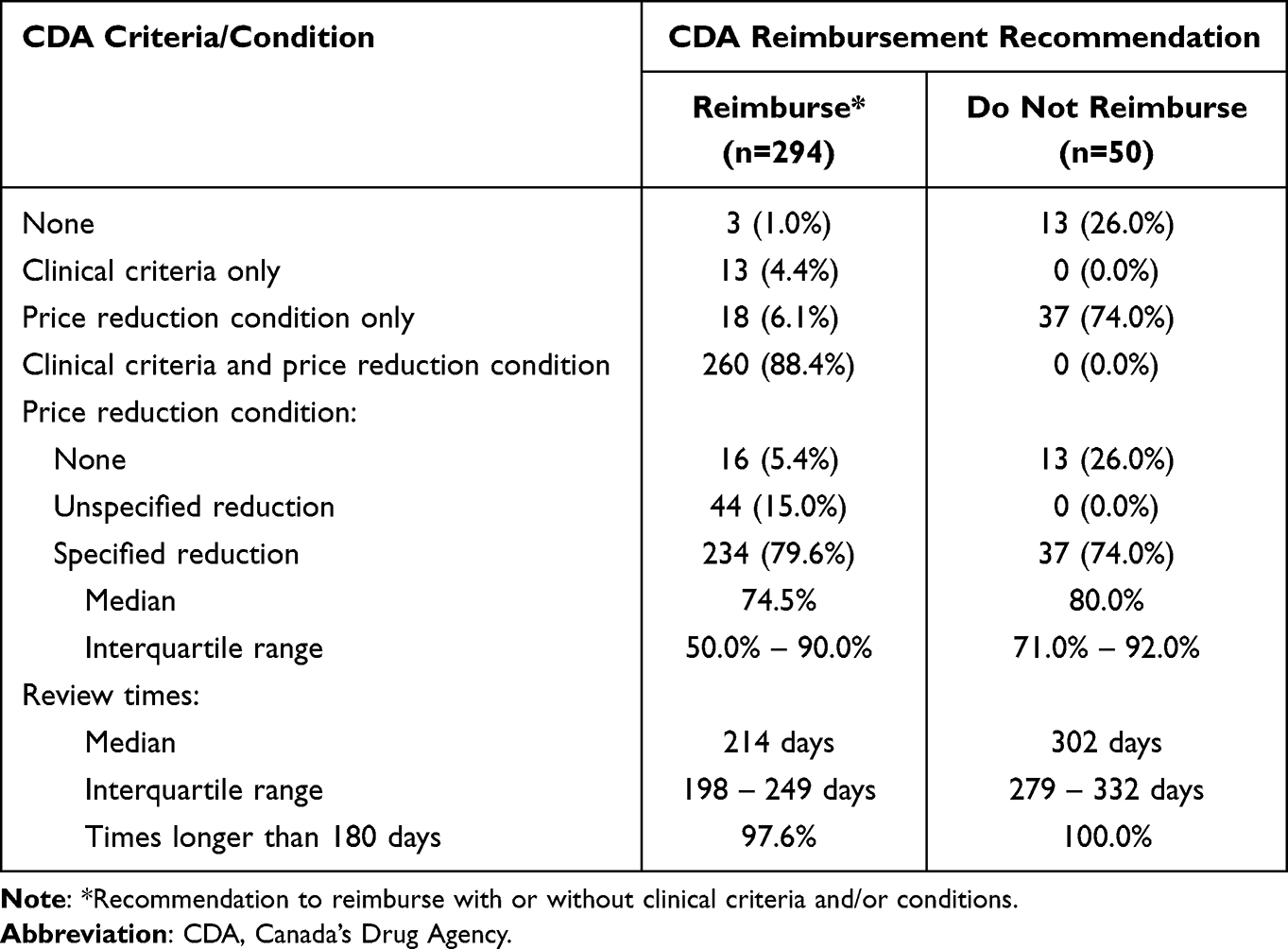 |
Table 1 Clinical and Price Reduction Criteria in 344 CDA Reimbursement Recommendations |
Concerns about the medication’s efficacy were expressed in the reviews of all 50 assessments receiving a negative recommendation. None of these reviews included clinical criteria, but 37 (74.0%) had a price reduction recommendation to achieve $50,000 per QALY (median reduction 80.0%; IQR: 71.0% to 92.0%). Recommended price reductions in the positive and negative CDA recommendations were not statistically different (p=0.11).
The median time required by CDA to complete assessments was 221 days (IQR: 199 to 282 days). Review times for medicines receiving a recommendation to reimburse were significantly shorter (median: 214 days; IQR: 198 to 249 days) than those for drugs with a negative recommendation (median: 302 days; IQR: 279 to 332 days) (p<0.00001).
Table 2 compares oncology, orphan, and other drugs. No differences were found between the time taken by CDA to complete assessments of oncology, orphan, and other drugs (p=0.37). Recommended price reductions for orphan drugs (median: 90.0%; IQR: 65.0% to 96.0%) and oncology medicines (median: 77.0%; IQR: 55.0% to 90.0%) were marginally different (p=0.036), but both were significantly greater (p=0.000072 and p=0.014, respectively) than reductions recommended for other drugs (median: 65.0%; IQR: 43.0% to 82.5%).
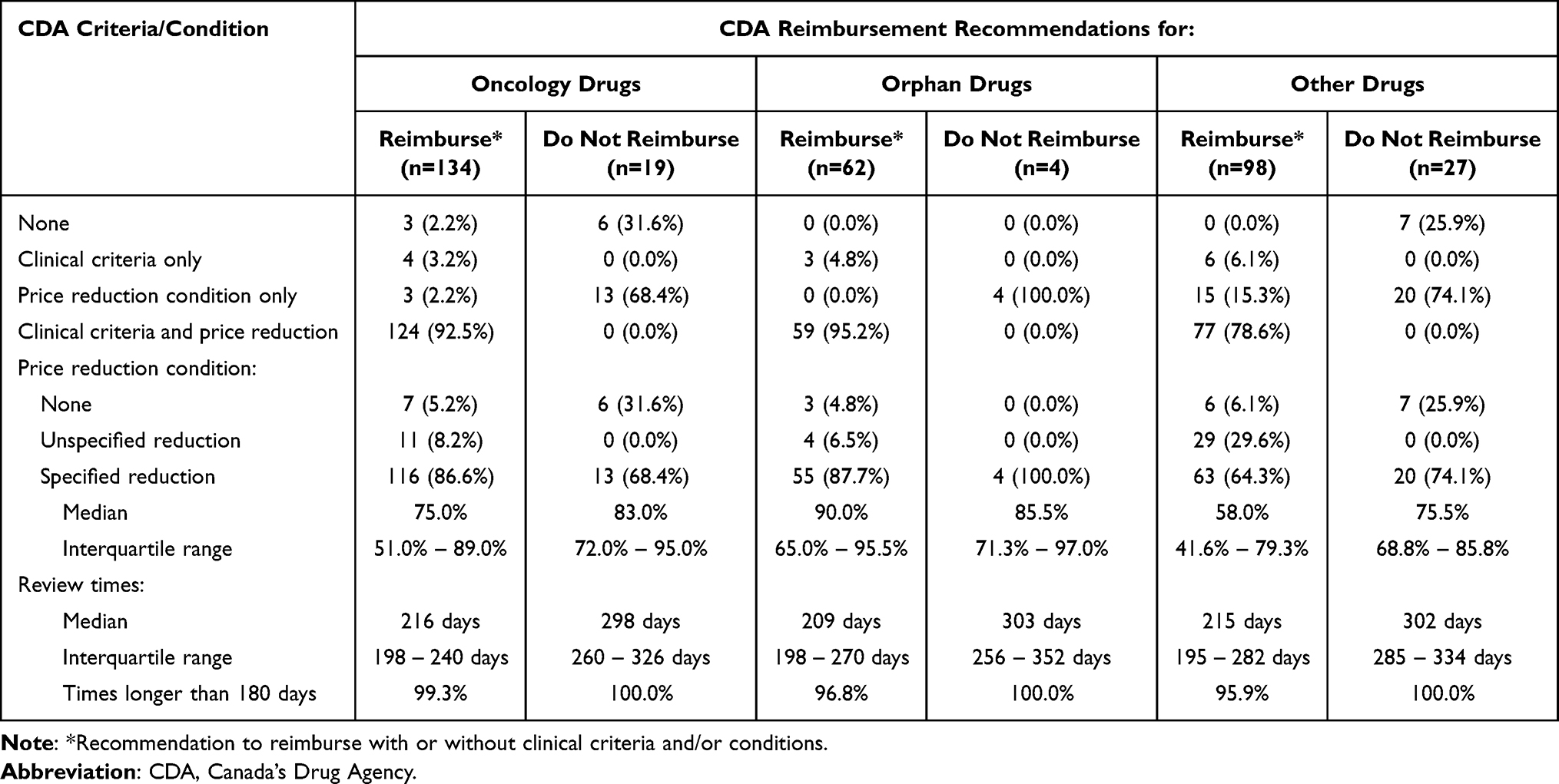 |
Table 2 Clinical and Price Reduction Criteria in 344 CDA Reimbursement Recommendations by Drug Types |
pCPA Negotiations
At the end of July 2025, no record was found in pCPA data corresponding with seven CDA recommendations; five were blood products negotiated by Canadian Blood Services for its national formulary,55 not by the pCPA. In the other 337, negotiations were active for 17 (5.0%) and under consideration for one (0.3%), while price negotiations reached a successful outcome for 248 (73.6%) or ended without agreement for 39 (11.6%); no negotiation was pursued for 32 (9.5%) (Table 3). Recommendations not to reimburse resulted in only about a third of the drug developers being invited to negotiate.
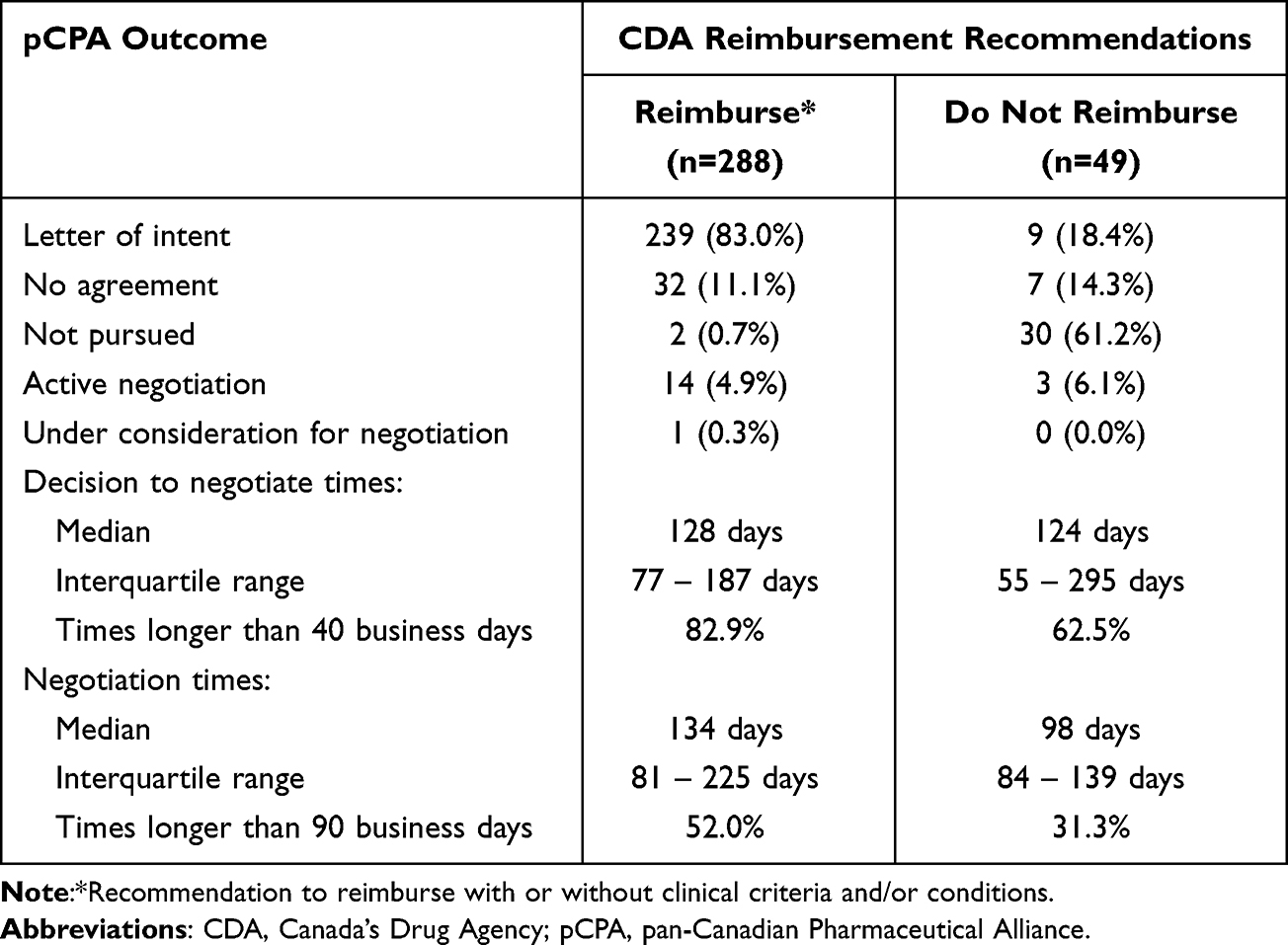 |
Table 3 Outcomes of 337 pCPA Negotiations by CDA Reimbursement Recommendation |
For drugs with a specific price decrease recommended by CDA, percentage reductions were similar among drugs with a successful negotiation (median: 74.0%; IQR: 51.0% to 90.0%), those with an unsuccessful negotiation (median: 75.0%; IQR: 43.8% to 91.5%) and those for which negotiation was not pursued (median: 77.0%; IQR: 66.5% to 92.0%) (p=0.62).
Following CDA recommendations, the median time taken by the pCPA to decide whether to invite developers to negotiate was 128 days (IQR: 73 to 191 days) and the median negotiation time was 131 days (IQR: 82 to 219 days).
The time taken by CDA and the pCPA to complete their work led to the median time between submission to CDA and a concluded pCPA negotiation (successful or not) or a decision not to negotiate being 518 days (IQR: 394 to 633 days). Times were over 18 months for 41.1% of the drugs and longer than two years for 14.7%.
Table 4 shows pCPA outcomes for the 337 drugs divided into oncology, orphan, and other drugs. The percentage of oncology drugs with a positive CDA recommendation and a successful pCPA negotiation (91.7%) was much higher than the rates for orphan (75.9%) and other drugs (75.3%). In all three categories, drugs with a negative CDA recommendation had a higher than 57% rate of the pCPA deciding not to pursue negotiation.
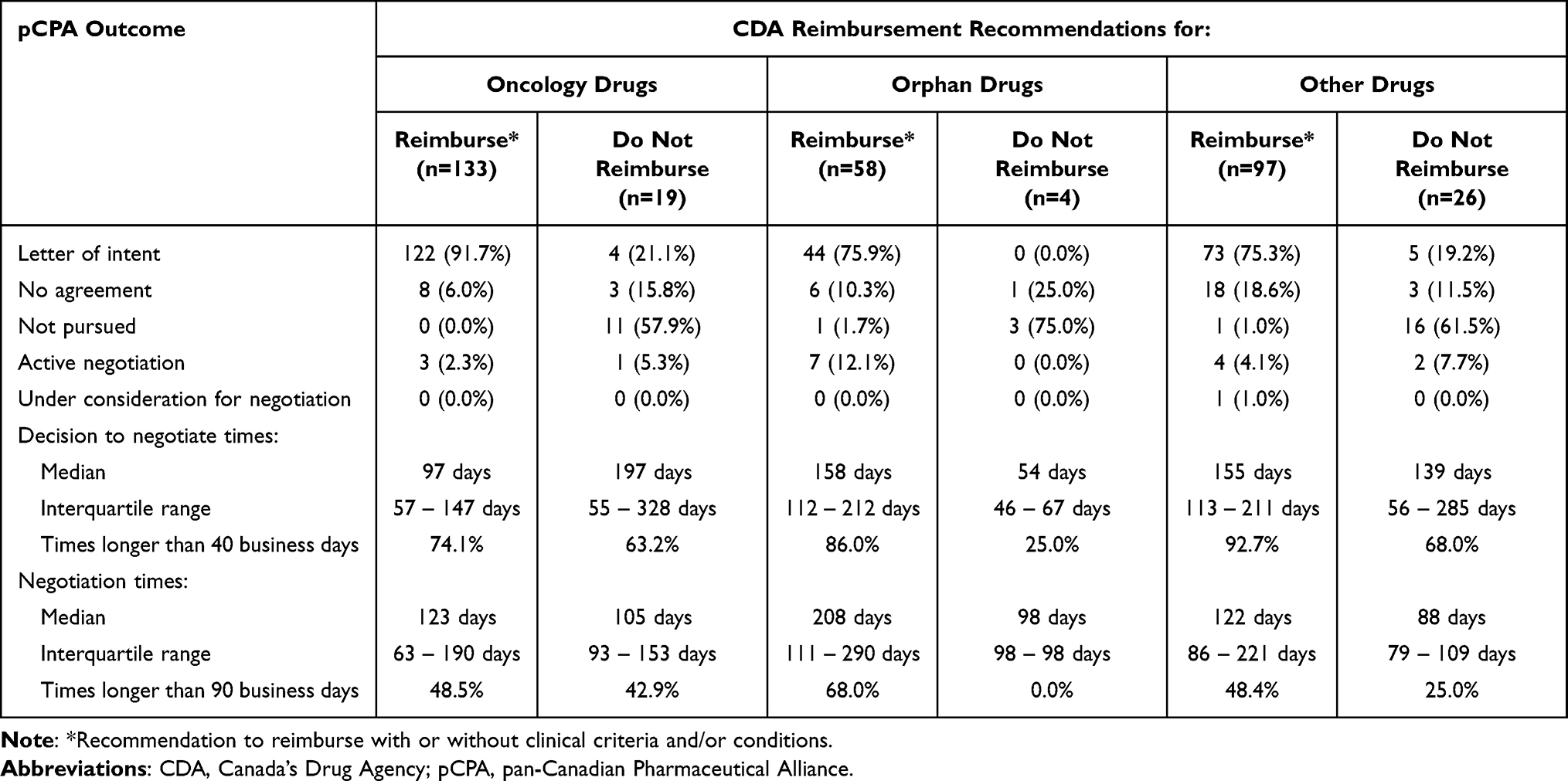 |
Table 4 Outcomes of 337 pCPA Negotiations by Drug Types and CDA Reimbursement Recommendation |
The times to decide whether to invite developers to negotiate prices for oncology drugs (median: 97 days; IQR: 56 to 161 days) were significantly shorter than those for orphan drugs (median: 149 days; IQR: 82 to 206 days) and other drugs (median: 149 days; IQR: 95 to 207 days) (p=0.0037 and p<0.00001, respectively). Decision times for orphan and other drugs were not significantly different. Negotiation times for orphan drugs were significantly longer (median: 208 days; IQR: 106 to 285 days) than those for oncology medicines (median: 119 days; IQR: 65 to 185 days) and other drugs (median: 120 days; IQR: 84 to 215 days) (p=0.00048 and p=0.021, respectively).
Government Drug Plan Listings
Seven CDA recommendations with no pCPA record, 18 with an active pCPA negotiation or under consideration for negotiation, and two COVID-19 medicines were excluded from the analysis of government drug plan listings. A further 33 CDA recommendations were excluded because there was more than one with the same diagnosis or an extended indication for the same drug. In addition, 23 drugs were excluded because the pCPA completion date was after March 31, 2025. Thus, 261 recommendations were included in the analysis of government drug plan listings. Drugs with unrestricted coverage, coverage limited to patients satisfying specified clinical criteria, or case-by-case coverage with undefined criteria were considered to be listed. Although drugs are evaluated for reimbursement recommendation in Quebec by INESSS, the province is a member of the pCPA and was included in the listings analysis.
In the 203 drugs with a successful pCPA negotiation, listing rates in early November 2025 were 77.8% to 91.6% in Ontario and the western provinces of British Columbia, Alberta, Saskatchewan and Manitoba compared with 58.6% to 72.4% in Quebec, the Atlantic provinces of New Brunswick, Nova Scotia, Prince Edward Island and Newfoundland and Labrador, and the NIHB (Figure 1). Much higher percentages of oncology drugs are listed in Ontario and the western provinces than in the other plans. Listing rates of orphan drugs were over 80% in Alberta, Saskatchewan, Ontario, Quebec, Nova Scotia, Newfoundland and Labrador, and the NIHB, while listing rates of other drugs were over 70% in all plans.
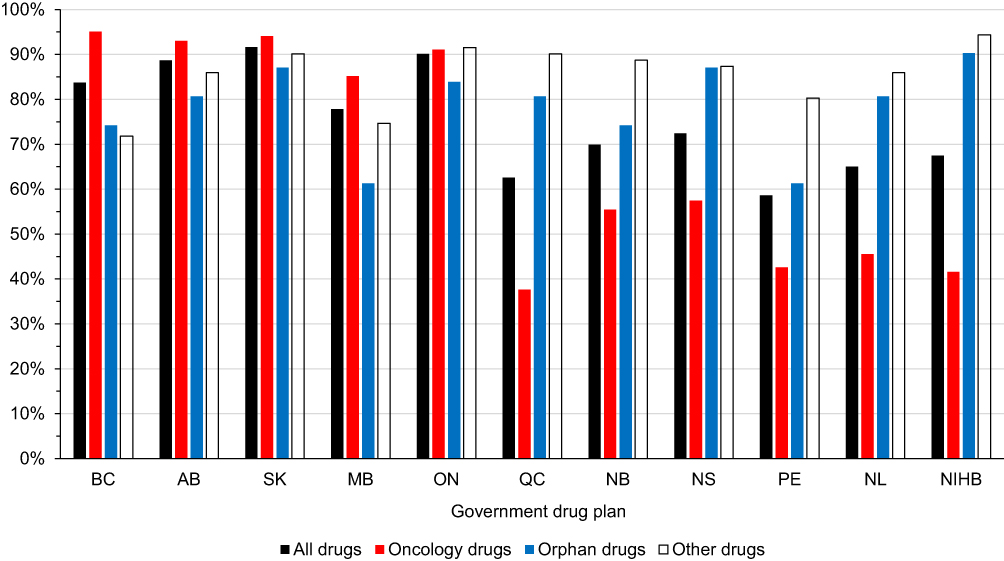 |
Figure 1 Government drug plan listing rates for 203 drugs with successful pan-Canadian Pharmaceutical Alliance outcomes. Abbreviations: AB, Alberta; BC, British Columbia; MB, Manitoba; NB, New Brunswick; NIHB, Non-Insured Health Benefits; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PE, Prince Edward Island; QC, Quebec; SK, Saskatchewan. |
The 58 drugs with either an unsuccessful pCPA negotiation or no negotiation had listing rates of 19.0% or lower, although rates for oncology drugs were generally higher in British Columbia, Saskatchewan, Manitoba and Ontario. Nine of the 58 drugs were orphan drugs; none were listed in any plan.
An explicit percentage price reduction was recommended in 205 CDA reports of the 261 drugs. The listing rates for drugs with a price reduction recommendation of under 70% were higher than the rates for those with a larger recommended reduction in all drug plans, but the difference was most marked in Alberta, Saskatchewan, Manitoba and Ontario (Figure 2).
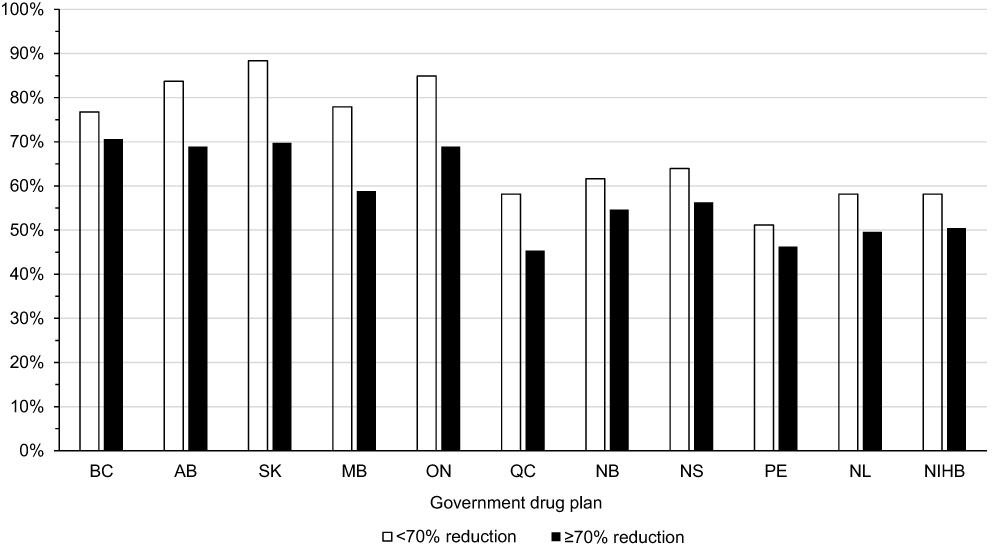 |
Figure 2 Government drug plan listing rates for 205 drugs with a specific recommended price reduction from Canada’s Drug Agency. Abbreviations: AB, Alberta; BC, British Columbia; MB, Manitoba; NB, New Brunswick; NIHB, Non-Insured Health Benefits; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PE, Prince Edward Island; QC, Quebec; SK, Saskatchewan. |
With one exception, government drug plans do not specify when drugs were first listed. The exception is the province of Alberta, whose non-cancer formulary36 records “date listed/coverage updated” and its cancer drug benefit list47 records “approval date” (month and year only). Multiple dates are recorded for some cancer drugs, likely because listings were revised in some way. Of the 261 drugs, 189 were listed in Alberta. When the time between CDA recommendation date and the date in the relevant Alberta benefit list was calculated, seven drugs had a negative value; all seven had CDA recommendations for the same or a similar indication prior to 2020. These drugs were excluded from further analysis. The median time between CDA recommendation dates and Alberta listing dates for the other 182 drugs was 402 days (IQR: 301 to 605 days).
Prior-Authorization Requests to a Private Plan Sponsor
After two requests to BMC members, confidential information was received about four patients whose prior-authorization requests for expensive orphan drugs were denied by the Cubic Health Facet program27 acting on behalf of a plan sponsor (plan sponsors choose and fund group health benefit plans and can be employers, unions, boards of trustees or multi-employer benefit trusts). The names of the medicines being denied were supplied to the author without any patient identification details. Confidential information about another patient’s prior-authorization request being denied by the same adjudicator was received from an industry source. In all five cases, Facet acknowledged that the requested orphan drugs, all of which are for genetic conditions that untreated can have serious outcomes, had been approved by Health Canada and that CDA had made recommendations to reimburse them, but said CDA’s recommendations were not “unconditional” and drugs with conditional recommendations or a “requirement by CDA for a lower price before they can be considered for … listing” are ineligible for coverage.
Three of the five patients wanted access to orphan drugs that, so far, no government plan has listed. Without private insurance covering the costs, they can only obtain these drugs if they pay out-of-pocket which, with list prices in Canada for both drugs beginning at more than $130,000 per year, places them beyond their means. The other two individuals wanted access to a drug listed by most government plans, but they live in a province that does not cover drugs for working-age adults.
Discussion
This analysis shows that, unless CDA reviewers doubt the efficacy of a medicine, recommendations are to reimburse, but virtually all have clinical criteria and/or a price reduction condition. The overall median price reduction recommended between 2020 and 2024 was higher than 74%; for orphan drugs, it was 90%. Behind these recommendations is CDA’s emphasis on using a $50,000 per QALY threshold to determine “cost-effectiveness”, regardless of medicine type, seriousness of the disease the drug is designed to treat, or the unmet need for the drug. Use of this threshold emerged in the United States in the early 1990s.56 By the mid-1990s, it had become widely used in several countries (adapted for difference currencies),15,16,57 including in Canada.21 The threshold has never been adjusted for inflation, economic growth, severity or rarity of the disease being treated, or the considerable increase in research, development, production and regulatory costs of innovative medicines in the last thirty years. In the past, reimbursement recommendations in Canada were more flexible, using higher thresholds for some drugs, especially cancer therapies,58 and took a more compassionate approach when the use of QALYs was inappropriate. The $50,000 per QALY threshold has only been used consistently in the last decade or so.
The time taken for CDA reviews between 2020 and 2024 exceeded CDA’s “target timeline” of up to 180 calendar days59 in 98% of the reviews. This high rate of failure to meet the “target timeline” was consistent regardless of drug type. CDA maintains it regularly achieves its time target, but its publicly available records do not support this claim and are insufficiently detailed to assess why reviews exceed the target time. When a review record mentions a delay due to causes such as later than expected regulatory approval from Health Canada or a request for reconsideration of a recommendation from the drug developer, the length of the delay is not publicly recorded. Even when review times were limited to those with no mention of a delay, 96.6% exceeded 180 days.
Developers of drugs receiving CDA recommendations to reimburse frequently achieved successful price negotiations with the pCPA, whereas negotiations for two-thirds of drugs with negative CDA recommendations were not pursued. The success rate was considerably higher for oncology drugs than non-oncology drugs.
The time taken by the pCPA to make a decision about whether to negotiate surpassed its performance standard of 40 business days for 79.9% of the medicines and 50.9% of the negotiations took longer than the pCPA’s standard of 90 business days.60 The decision whether to negotiate is entirely the responsibility of the pCPA because drug developers have to wait to be invited into negotiation, whereas the length of negotiations is dependent on both the developer and the pCPA. The pCPA’s website provides no insight into reasons for lengthy times to make decisions or to negotiate.
Medicines not recommended for reimbursement by CDA and not pursued for negotiation by the pCPA are generally not listed in government drug plans. Drugs for which the pCPA and the developer were unable to achieve a successful negotiation are also usually not listed, especially in plans in the Atlantic provinces. In addition, some drugs that successfully pass through CDA and the pCPA are never listed. Even when they are, the decision process takes months, sometimes years. The Conference Board of Canada found that, in 2022, the average time between pCPA negotiation outcome and “time to patient”, which should be longer than time to listing, varied between 44 days in Quebec to 662 days in Prince Edward Island; in Alberta, it was 273 days.61 The average time between pCPA outcome and listing in Alberta for drugs with CDA recommendations between 2020 and 2024 was much longer at 478 days (nearly 16 months), while the median was 402 days. Delays resulting from government processes add to wait times caused by new medicines regularly being submitted for regulatory review by Health Canada a year after submission in the United States and Europe10 and mean that drugs, particularly orphan drugs,19,20 are listed in government plans in Canada three or more years after Americans and western Europeans have access to them.10
Being included in government drug benefit lists does not guarantee that medicines are easily accessible.19 New drugs are nearly always listed with clinical criteria that must be met to obtain access. These typically match criteria recommended by CDA19,62 which, in turn, are usually based on the often highly selective criteria used to enrol patients in clinical trials submitted as evidence of the drug’s efficacy and safety in developers’ applications to Health Canada and CDA. Access to tests or measures required by these criteria may not be available in everyday medical practice in Canada, or the tests are only available in specialized centres, which requires patients to travel long distances and pay for accommodation that they may not be able to afford. Some clinical criteria placed on drug access through government drug plans seem poorly thought out.63
The processes of CDA, pCPA and drug plan managers have been established for government health care systems, not private payers. Canadian governments’ focus is the impact of new medicines on their health system budgets,64 whereas private payers should have a wider productivity viewpoint that includes the contribution of new medicines to patients’ ability to continue to attend work or school or return to these activities as soon as possible, which is of high importance to plan sponsors and Canadians.65
Five patients were identified as having prior-authorization requests for orphan drugs denied by the Facet adjudicator.27 Whether these individuals represent the tip of an iceberg is unknown, but the number could be much higher because Facet manages prior-authorization requests for medications for the health and benefit plans of over a million Canadians. Almost all CDA recommendations are to reimburse conditional on clinical criteria and/or a price reduction. CDA recommendations are never updated when the drugs are successfully negotiated with the pCPA and listed in government drug plans. Consequently, the requirement that drugs must have unconditional CDA recommendations before prior-authorization requests can be approved by Facet means requests for virtually all new drugs will always be denied.
CDA recommendations are intended for “health system leaders”,12 who are focused on the impact of new drugs on their budgets and not their broader benefits to society or patients’ ability to return to work or school. Plan sponsors, employers and unions should want to ensure their employees and members are using appropriate medications and be concerned when they are denied access to new drugs that have potential productivity benefits in reducing absenteeism or long-term disability compensation.66 When patients’ coverage is refused based on outcomes of government processes, private plan sponsors are failing to take this broader perspective. They may be using the requirement for drugs to have unconditional CDA reimbursement recommendations before approving prior-authorization requests as a way to cope with the costs of new medicines, but other methods exist to mitigate these costs that do not result in wholesale denials of patient access to virtually all new drugs.
Canada is a relatively small pharmaceutical market within the global environment in which multinational manufacturers work and, as such, there is a need to incentivize developers to launch new medicines in Canada, not multiple adversarial gatekeeping processes that deter them.67,68 Specific recommendations based on this analysis are:
- Canada should align its patent and data protection standards with international norms and introduce similar processes to fast-track the review and approval of new medicines to those in other jurisdictions like the United States and the European Union.69 Canada should also mutually recognize new medicines, particularly those for life-threatening or severely disabling diseases, soon after approval by regulatory agencies in the United States or the European Union as being safe and beneficial for Canadians and approve them.70 Delays while Health Canada reviews medicines already evaluated and approved by other larger and more well-funded agencies are unacceptable.
- CDA should achieve its performance target time in at least 90% of its reviews and transparently explain the reasons when it is not achieved. CDA should significantly raise its cost-effectiveness threshold from $50,000 per QALY to account for inflation, economic growth, type of the disease being treated, and the increase in research, development, production and regulatory costs of innovative medicines in the last thirty years. The agency should use more flexible thresholds for medicines for cancers, rare diseases and other life-threatening or disabling conditions for which an unmet health need exists. CDA should also remove or downgrade any conditions attached to recommendations for drugs that are successfully negotiated with the pCPA and are listed by 90% of government drugs.
- The pCPA is developing a process to begin negotiations with drug developers more quickly for some oncology drugs71 and one to accelerate non-complex negotiations.72 However, the pCPA should immediately begin negotiations for all medicines with positive CDA reimbursement recommendations and not take months to decide whether to negotiate.
- Government drug plans should list medicines with positive CDA recommendations and successful negotiations with the pCPA as soon as possible, unless they can provide transparent reasons for not doing so. While governments may have different health priorities, population distributions and budgets, they should make every effort to achieve consistency of coverage because the existing diversity between plans will always mean some Canadians can obtain coverage, while others cannot.4–6,73
- Private plan sponsors should not base reimbursement decisions based solely on whether medicines have an unconditional CDA reimbursement recommendation.
Limitations
Transcribing of pCPA and listing data was done by one person, although with considerable experience in extracting and using these data.19,20,74 There is no universal definition of the prevalence that distinguishes a rare disease. The classification as an orphan drug was based on diseases with a prevalence of less than one per 2000 individuals, which is commonly used in Canada, but these are only estimates based on global data. The currency of provincial listing data is variable. Provinces with searchable formularies update listings almost daily, while others that have pdf-format listings only update monthly. Some provincial cancer drug formularies are updated less frequently. Governments may have other lists of drugs that are reimbursed on a case-by-case review, which are not publicly accessible. Consequently, the listing data only represent publicly available information in early November 2025. Drugs with completed pCPA negotiations earlier in the observation period might be expected to have a higher chance of being listed in more government drug plans than those with completed pCPA negotiations late in the period and lead to bias. However, the rate of medicines with pCPA negotiations completed in 2020 to 2022 listed in at least nine drug plans was 47.3%, which was only marginally higher than the corresponding rate of 42.9% for medicines with completed negotiations in 2023 to 2024.
Conclusions
The consequences of delays and denials of access to medicines resulting from CDA recommendations, pCPA negotiations and government listing processes for patients reliant on government drug plans have been of concern for years. All Canadians are impacted when government processes lead to drug developers giving Canada lower priority when considering where to launch innovative medicines or, in many cases, deciding not bring their products to Canada.10
Patients and their families have pleaded for access to reduce suffering and extend lives75–82 and others have drawn attention to process delays and lack of access.18–21,83–86 Patients have actively tried to make politicians aware of their concerns,75,87–89 but politicians have only recently begun to voice their awareness.90 So far, they have done little to improve the situation by requiring their organizations (Health Canada, CDA and the pCPA) prioritize patients over process or break down their siloed budgetary systems91 that result in the addition of new medicines to benefit lists being regarded solely as an increase in drug budgets, instead of taking a wider view of potential benefits to their health care systems.
Private health benefit plans are vital for many Canadians without access to government plans or those who find government plans lacking. Private plan sponsors perform their own evaluations that include productivity and societal benefits of new medicines. When prior-authorization requests are only approved for drugs with unconditional CDA recommendations, patients with private insurance not only have to wait while CDA completes its lengthy procedures but then may find their prior-authorization requests for new costly drugs denied because almost all CDA recommendations are conditional. Further research into reasons for delays in CDA, pCPA and government drug plan listing processes and the impact of denial of access to medicines by private plan sponsors is warranted.
Data Sharing Statement
Apart from information about patients with denied prior-authorization requests, data used in this analysis are available from publicly accessible resources.33–52
Acknowledgments
I thank Best Medicines Coalition for asking members whether patients had been denied prior-authorization requests due to a policy limiting approval to drugs with unconditional CDA recommendations and their members that responded.
Funding
The author gratefully acknowledges open access funding from RAREi, an informal network of Canadian research-based biopharmaceutical organizations developing therapeutics for rare diseases. RAREi had no input into the concept, content or writing of the manuscript. No other funding for this work was received from any source.
Disclosure
During the past three years, Dr. Rawson received research and consultation fees from Abbvie Canada, Macdonald-Laurier Institute and 3Sixty Public Affairs Inc., and article processing expenses from CanCertainty Coalition and RAREi. No conflict of interest exists between these activities and the present work. The author reports no other conflicts of interest in this work.
References
1. About Canada’s health care system. Ottawa, ON: Government of Canada; 2025. Available from: https://www.canada.ca/en/health-canada/services/canada-health-care-system.html.
2. Provincial and territorial public drug benefit programs. Ottawa, ON: Government of Canada; 2025. Available from: https://www.canada.ca/en/health-canada/services/health-care-system/pharmaceuticals/access-insurance-coverage-prescription-medicines/provincial-territorial-public-drug-benefit-programs.html.
3. Drugs and pharmacy benefits for first nations and inuit. Ottawa, ON: Government of Canada; 2024. Available from: https://www.sac-isc.gc.ca/eng/1574784515492/1574784549876.
4. Demers V, Melo M, Jackevicius C, et al. Comparison of provincial prescription drug plans and the impact on patients’ annual drug expenditures. CMAJ. 2008;178(4):405–409. doi:10.1503/cmaj.070587
5. Campbell DJT, Manns BJ, Soril LJJ, Clement F. Comparison of Canadian public medication insurance plans and the impact on out-of-pocket costs. CMAJ Open. 2017;5(4):E808–E813. doi:10.9778/cmajo.20170065
6. Casey B. Pharmacare now: prescription medicine coverage for all Canadians. Ottawa, ON: House of Commons; 2018. Available from: https://www.ourcommons.ca/Content/Committee/421/HESA/Reports/RP9762464/hesarp14/hesarp14-e.pdf.
7. National pharmacare bilateral agreements. Ottawa, ON: Government of Canada; 2025. Available from: https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/national-pharmacare-bilateral-agreements.html.
8. Federal budget doesn’t include new money for pharmacare expansion. CBC News. 2025. Available from: https://www.cbc.ca/player/play/video/9.6972112.
9. Gellatly G, McCormack C. Recent developments in the Canadian economy: fall 2025. Ottawa, ON: Statistics Canada; 2025. Available from: https://www150.statcan.gc.ca/n1/pub/36-28-0001/2025010/article/00004-eng.htm.
10. Skinner B. Waiting for new medicines in Canada, Europe and the United States 2018-2023. Can Health Policy. 2024;2024(APR). doi:10.54194/QQVC3893
11. About the institut. Quebec, QC: Government of Quebec; 2025. Available from: https://www.inesss.qc.ca/en/about-us/about-the-institut.html.
12. About us. Ottawa, ON: Canada’s Drug Agency; 2025. Available from: https://www.cda-amc.ca/about-us.
13. About pCPA. Pan-Canadian pharmaceutical alliance. 2025. Available from: https://www.pcpacanada.ca/index.php/about.
14. Patented medicine prices review board. Ottawa, ON: Government of Canada; 2020. Available from: https://pmprb-cepmb.gc.ca/home.
15. Fernandez J, de Boissieu P, Galbraith M. Health technology assessment in Europe: a comparison of organizations and introduction to the European regulation. Presse Med. 2025;54(2):104282. doi:10.1016/j.lpm.2025.104282
16. Kim H, Byrnes J, Goodall S; for Australia ISPOR Chapter executive committee. Health technology assessment in Australia: the pharmaceutical benefits advisory committee and medical services advisory committee. Value Health Reg Issues. 2021;24:6–11. doi:10.1016/j.vhri.2020.09.001
17. Rawson N, Adams J. One federal agency we could axe? The drug prices review board. Financial Post. 2025. Available from: https://financialpost.com/opinion/federal-agency-axe-drug-prices-review-board.
18. Balijepalli C, Gullapalli L, Joshy J, Rawson NSB. The impact of willingness-to-pay threshold on price reduction recommendations for oncology drugs: a review of reimbursement assessments by the Canadian agency for drugs and technologies in health. J Comp Eff Res. 2024;13(5):e230178. doi:10.57264/cer-2023-0178
19. Rawson NSB, Adams J. Orphan drugs approved in Canada: health technology assessment, price negotiation, and government formulary listing. Expert Opin Orphan Drugs. 2024;12(1):1–11. doi:10.1080/21678707.2024.2313766
20. Rawson NSB. Health technology assessment and price negotiation alignment for rare disorder drugs in Canada: who benefits? Orphanet J Rare Dis. 2022;17(1):218. doi:10.1186/s13023-022-02390-x
21. Binder L, Ghadban M, Sit C, Barnard K. Health technology assessment process for oncology drugs: impact of CADTH changes on public payer reimbursement recommendations. Curr Oncol. 2022;29(3):1514–1526. doi:10.3390/curroncol29030127
22. MacPhail E, Shea B. An inside look at the early history of the CADTH common drug review in Canada. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health; 2017. Available from: https://www.cda-amc.ca/sites/default/files/pdf/early_history_of_CDR.pdf.
23. Canadian life and health insurance facts, 2025 edition. Toronto, ON: Canadian Life and Health Insurance Association; 2025. Available from: http://clhia.uberflip.com/i/1539498-canadian-life-and-health-insurance-facts-2025-edition/0.
24. Fleming H. Policy brief: high demand for private health insurance in Canada. Regina, SK: Second Street; 2025. Available from: https://secondstreet.org/wp-content/uploads/2025/03/Policy-Brief-High-Demand-for-Private-Health-Insurance-in-Canada-V3-March-3.pdf.
25. Skinner BJ. Public v private insurance coverage for new drugs in Canada, 2018-2023, 7th edition. Can Health Policy. 2024. doi:10.54194/DKPO5320
26. Kratzer J, McGrail K, Strumpf E, Law MR. Cost-control mechanisms in Canadian private drug plans. Healthc Policy. 2013;9(1):35–43.
27. Clinical experts, responsible care. Toronto, ON: Facet; n.d.. Available from: https://www.facetprogram.ca/en/.
28. IBEW Local 353 benefit plan. Toronto, ON: Toronto Electrical Industry Benefit Administration Services; 2024. Available from: https://teibas.com/wp-content/uploads/2024/12/IBEW-Local-353-Benefit-Plan-Booklet-FINAL.pdf.
29. Facet prior authorization drug program. Vancouver, BC: University of British Columbia; 2025. Available from: https://hr.ubc.ca/benefits/benefit-plan-details/extended-health-benefits/facet-prior-authorization-drug-program.
30. Sun Life Financial. Your group benefits. Edmonton, AB: University of Alberta; 2024. Available from: https://www.ualberta.ca/en/human-resources-health-safety-environment/media-library/employee-benefits/25379-booklet-academic-2024-10-15.pdf.
31. What is drug prior authorization and why is it important? Waterloo, ON: Ontario Teachers Insurance Plan; 2025. Available from: https://www.otip.com/why-otip/news/what-is-drug-prior-authorization-and-why-is-it-important.
32. Welcome to your benefits. Uxbridge, ON: CUPE Ontario Education Workers; 2025. Available from: https://www.cupe-ewbt.ca/.
33. Reimbursement review reports. Ottawa, ON: Canada’s Drug Agency; 2025. Available from: https://www.cda-amc.ca/reimbursement-review-reports.
34. Brand name drug negotiations status. Pan-Canadian pharmaceutical alliance. 2025. Available from: https://www.pcpacanada.ca/negotiations.
35. BC PharmaCare formulary search. Victoria, BC: Government of British Columbia; 2025. Available from: https://pharmacareformularysearch.gov.bc.ca/Search.xhtml.
36. Welcome to the iDBL. Edmonton, AB: Government of Alberta; 2025. Available from: https://idbl.ab.bluecross.ca/idbl/load.do.
37. Home – search formulary. Regina, SK: Government of Saskatchewan; 2025. Available from: https://formulary.drugplan.ehealthsask.ca/SearchFormulary.
38. Drug formulary lookup. Winnipeg, MB: Manitoba Health; 2025. Available from: https://web22.gov.mb.ca/eFormulary/.
39. Formulary search. Toronto, ON: Government of Ontario; 2025. Available from: https://www.formulary.health.gov.on.ca/formulary/.
40. Find out whether a drug is covered: prescription drug search. Quebec, QC: Régie de l’assurance maladie; 2025. Available from: https://www.ramq.gouv.qc.ca/en/citizens/prescription-drug-insurance/find-out-whether-a-drug-covered.
41. New Brunswick drug plan formulary. Fredericton, NB: Government of New Brunswick; 2025. Available from: https://www2.gnb.ca/content/dam/gnb/Departments/h-s/pdf/en/NBDrugPlan/NewBrunswickDrugPlansFormulary.pdf.
42. Formulary. Halifax, NS: Government of Nova Scotia; 2025. Available from: https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf.
43. PEI Pharmacare formulary search. Charlottetown, PE: Health PEI; 2025. Available from: https://www.princeedwardisland.ca/en/feature/pei-pharmacare-formulary-search/#/service/DrugFormulary/DrugFormularySearch.
44. Search the NLPDP drug product database. St. John’s, NL: Government of Newfoundland and Labrador; 2025. Available from: https://www.health.gov.nl.ca/health/prescription/newformulary.asp.
45. Drug benefit list. Toronto, ON: Express Scripts Canada; 2025. Available from: https://nihb-ssna.express-scripts.ca/en/0205140506092019/16/160407.
46. BC Cancer benefit drug list. Vancouver, BC: BC Cancer Agency; 2025. Available from: http://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf.
47. Outpatient cancer drug benefit program. Edmonton, AB: Alberta Health Services; 2025. Available from: https://www.albertahealthservices.ca/assets/programs/ps-1025651-drug-benefit-list.pdf.
48. Saskatchewan Cancer Agency drug formulary. Regina, SK: Saskatchewan Cancer Agency; 2025. Available from: https://saskcancer.ca/sites/default/files/2025-03/SCA%20Drug%20Formulary%20-%202025-04-01.pdf.
49. Drug formulary. Toronto, ON: Cancer Care Ontario; 2025. Available from: https://www.cancercareontario.ca/en/drugformulary/drugs.
50. Bulletin archive. Winnipeg, MB: Manitoba Health; 2025. Available from: https://www.gov.mb.ca/health/mdbif/bulletins.html.
51. Drugs for rare diseases: common list of drugs. Ottawa, ON: Government of Canada; 2025. Available from: https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/shared-health-priorities/drugs-for-rare-diseases-bilateral-agreements/common-list-drugs.html.
52. Search for a rare disease. Paris: Orphanet; 2025. Available from: https://www.orpha.net/en/disease.
53. Statistics online. Melbourne, Australia: Statistics Kingdom; 2017. Available from: https://www.statskingdom.com/index.html.
54. About the best medicines coalition. Toronto, ON: Best Medicines Coalition; 2025. Available from: https://bestmedicinescoalition.org/about/.
55. Plasma protein and related products national formulary. Ottawa, ON: Canadian Blood Services; 2025. Available from: https://formulary.blood.ca/en.
56. Grosse SD. Assessing cost-effectiveness in healthcare: history of the $50,000 per QALY threshold. Expert Rev Pharmacoecon Outcomes Res. 2008;8(2):165–178. doi:10.1586/14737167.8.2.165
57. Drummond M, Banta D. Health technology assessment in the United Kingdom. Int J Technol Assess Health Care. 2009;25(suppl 1):178–181. doi:10.1017/s0266462309090618
58. Rocchi A, Menon D, Verma S, Miller E. The role of economic evidence in Canadian oncology reimbursement decision-making: to lambda and beyond. Value Health. 2008;11(4):771–783. doi:10.1111/j.1524-4733.2007.00298.x
59. Procedures for reimbursement review. Ottawa, ON: Canada’s Drug Agency; 2025. Available from: https://www.cda-amc.ca/sites/default/files/Drug_Review_Process/Drug_Reimbursement_Review_Procedures.pdf.
60. pCPA brand process guidelines. Pan-Canadian pharmaceutical alliance. 2025. Available from: https://www.pcpacanada.ca/sites/default/files/eng/pCPA_Brand_Process_Guidelines.pdf.
61. Access and time to patient: prescription drugs in Canada. Ottawa, ON: Conference Board of Canada; 2024. Available from: https://www.conferenceboard.ca/wp-content/uploads/2022/10/access-and-time-to-patient_jan2024.pdf.
62. Pant S. Overview of formulary management practices of publicly funded provincial and territorial drug plans. Can J Health Technol. 2021;1(5).
63. Begovic M. Getting sick to get better: cystic fibrosis patients worry about access to ‘breakthrough’ drug. Toronto, ON: Healthing.ca; 2022. Available from: https://www.healthing.ca/cystic-fibrosis/trikafta-cystic-fibrosis-drug-access.
64. Laupacis A. Inclusion of drugs in provincial drug benefit programs: who is making these decisions, and are they the right ones? CMAJ. 2002;166(1):44–47.
65. Rizzardo S, Bansback N, Dragojlovic N, et al. Evaluating Canadians’ values for drug coverage decision making. Value Health. 2019;22(3):362–369. doi:10.1016/j.jval.2018.08.008
66. Shafrin J, Kim J, Cohen JT, et al. Valuing the societal impact of medicines and other health technologies: a user guide to current best practices. Forum Health Econ Policy. 2024;27(1):29–116. doi:10.1515/fhep-2024-0014
67. Rawson NSB, Adams J. More than a dose of collaboration: what Ottawa should do if it wants drugs and vaccines to be made in Canada and benefit patients. Ottawa, ON: Macdonald-Laurier Institute; 2021. Available from: https://macdonaldlaurier.ca/mli-files/pdf/20210525_More_than_a_dose_of_collaboration_Rawson_Adams_PAPER_FWeb.pdf?mc_cid=44923e3a19&mc_eid=UNIQID.
68. Rawson NSB, Adams J. Life on hold: how Canada’s drug approval delays endanger patients. Ottawa, ON: Macdonald-Laurier Institute; 2025. Available from: https://macdonaldlaurier.ca/life-on-hold-how-canadas-drug-approval-delays-endanger-patients-nigel-s-b-rawson-and-john-adams/.
69. Lybecker KM. Intellectual property rights protection and the biopharmaceutical industry: how Canada measures up. Vancouver, BC: Fraser Institute; 2017. Available from: https://www.fraserinstitute.org/sites/default/files/intellectual-property-rights-protection-and-the%20biopharmaceutical-industry.pdf.
70. Barua B, Westcott W, Vo VN. Timely access to new pharmaceuticals in Canada, the United States, and the European Union. Vancouver, BC: Fraser Institute; 2021. Available from: https://www.fraserinstitute.org/sites/default/files/timely-access-to-new-pharmaceuticals-in-canada-US-and-EU.pdf.
71. Early negotiation process (ENP). Pan-Canadian pharmaceutical alliance. 2025. Available from: https://www.pcpacanada.ca/enp-pathway.
72. Targeted negotiation process (TNP). Pan-Canadian pharmaceutical alliance. 2025. Available from: https://www.pcpacanada.ca/tnp-pathway.
73. MacPhail C, Snow S. Not all Canadian cancer patients are equal – disparities in public cancer drug funding across Canada. Curr Oncol. 2022;29(3):2064–2072. doi:10.3390/curroncol29030166
74. Rawson NSB, Stewart DJ. Timeliness of health technology assessments and price negotiations for oncology drugs in Canada. Clinicoecon Outcomes Res. 2024;16:437–445. doi:10.2147/ceor.s462872
75. Armstrong J, Shum D. Madi Vanstone pleads with Wynne to cover cystic fibrosis drugs. Global News. 2014. Available from: https://globalnews.ca/news/1183376/madi-vanstone-to-meet-with-premier-wynne-on-drug-fight-report/.
76. Ghoussoub M. UBC student fights for her life after being diagnosed with rare disease not covered in BC. CBC News. 2017. Available from: https://www.cbc.ca/news/canada/british-columbia/ubc-student-fights-for-her-life-after-being-diagnosed-with-rare-disease-not-covered-in-b-c-1.4398260.
77. Pfeffer A. Patient with rare disease pleads for life-saving drug funding. CBC News. 2019. Available from: https://www.cbc.ca/news/canada/ottawa/rare-disease-rituximab-payment-pharmacare-1.5172457.
78. Cooke A. ‘Heartbreaking’ death of cystic fibrosis patient shines light on drug access issues. CBC News. 2020. Available from: https://www.cbc.ca/news/canada/nova-scotia/chantelle-lindsay-cystic-fibrosis-death-canada-drug-access-1.5471605.
79. Payne E. Cornwall woman fighting for cystic fibrosis drug turned down for exceptional access. Ottawa Citizen. 2023. Available from: https://ottawacitizen.com/news/local-news/cornwall-woman-fighting-for-cystic-fibrosis-drug-turned-down-for-exceptional-access.
80. Dobson C. Fighting for her life. Sarnia Journal. 2023. Available from: https://www.thesarniajournal.ca/news/fighting-for-her-life-7973384.
81. Patient Voice. Stories from the frontlines of the fight for access to innovative therapies. Maclean’s. 2023. Available from: https://macleans.ca/sponsored/the-fight-for-access-to-innovative-therapies/.
82. Darke AC. Can I be honest with my neurologist? A problem of health technology in Canada. Can J Neurol Sci. 2023;51(5):603–605. doi:10.1017/cjn.2023.307
83. Gotfrit J, Shin JJW, Mallick R, Stewart DJ, Wheatley-Price P. Potential life-years lost: the impact of the cancer drug regulatory and funding process in Canada. Oncologist. 2020;25(1):e130–137. doi:10.1634/theoncologist.2019-0314
84. Stewart DJ. A Short Primer on Why Cancer Still Sucks. Victoria, BC: Tellwell; 2022.
85. Stewart DJ, Bradford J-P, Batist G. Treatment access, health economics, and the wave of the magic wand. Curr Oncol. 2022;29(2):1176–1189. doi:10.3390/curroncol29020100
86. Sehdev SR, Rawson NSB, Aseyev OI, et al. Access to oncology medicines in Canada: consensus forum for recommendations for improvement. Curr Oncol. 2024;31(4):1803–1816. doi:10.3390/curroncol31040136
87. System broken: how public drug coverage is failing Canadians with mental illness. Ottawa, ON: Mood Disorders Society of Canada; 2023. Available from: https://mdsc.ca/wp-content/uploads/2023/11/Report-on-Access-to-Medications-for-Mental-Illness-English.pdf.
88. British Columbia medication coverage report. Vancouver, BC: Gastrointestinal Society; 2025. https://badgut.org/wp-content/uploads/BC-Medication-Coverage-Report-2025-v2.pdf.
89. Osman H, Lintern S, Campo McLeod D. Approved but denied: canadians with neuromuscular diseases face unequal access to treatment. Toronto, ON: Healthy Debate; 2025. Available from: https://healthydebate.ca/2025/07/topic/approved-but-denied-canadians-with-neuromuscular-diseases-face-unequal-access-to-treatment/.
90. Rushowy K. Doug Ford wants Canada to approve drugs faster. Is that possible? Toronto Star. 2024. Available from: https://www.thestar.com/politics/provincial/doug-ford-wants-canada-to-approve-drugs-faster-is-that-possible/article_b3fdf7f8-3ef1-11ef-a405-db669ffaca4d.html.
91. Lau RS, Boesen ME, Richer L, Hill MD. Siloed mentality, health system suboptimization and the healthcare symphony: a Canadian perspective. Health Res Policy Syst. 2024;22(1):87. doi:10.1186/s12961-024-01168-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.