Back to Journals » Clinical Ophthalmology » Volume 19
Conscious Monitored Anesthesia Care versus General Anesthesia for Vitreoretinal Surgeries
Authors Namvar E, Attar A, Salari M, Alamdari M, Hadipour M
Received 10 June 2025
Accepted for publication 16 September 2025
Published 2 October 2025 Volume 2025:19 Pages 3595—3601
DOI https://doi.org/10.2147/OPTH.S546027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ehsan Namvar,1 Alireza Attar,1 Mehrdad Salari,2 Mohammad Alamdari,1 Maryam Hadipour3
1Poostchi Ophthalmology Research Center, Department of Ophthalmology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; 2Anesthesiology and Critical Care Research Center, Department of Anesthesiology and Critical Care, School of Medicine, Shiraz University of Medical Science, Shiraz, Iran; 3Health Policy Research Center, Institute of Health, School of Medicine, Shiraz University of Medical Science, Shiraz, Iran
Correspondence: Mehrdad Salari, Anesthesiology and Critical Care Research Center, Department of Anesthesiology and Critical Care, School of Medicine, Shiraz University of Medical Science, Shiraz, Iran, Email [email protected]
Purpose: This study compares monitored anesthesia care (MAC) with general anesthesia (GA) for vitreoretinal surgery, aiming to assess safety, efficacy, and patient outcomes.
Patients and Methods: This was a prospective non-randomized clinical trial. This trial was conducted during vitreoretinal surgery. Forty Patients were included in this study and divided into MAC and GA groups. The patients were divided in to two groups. In one group, patients who were operated under general anesthesia and in the other group those who were operated with conscious sedation were included. Anesthesia quality, surgical outcomes, anesthesia time, surgery time and recovery time were compared between two groups using standardized criteria and statistical analysis.
Results: MAC provided comparable analgesia, immobilization, and hemodynamic stability to GA, with no reported complications. All patients in both groups had successful surgery. Anesthesiologist favored MAC for its hemodynamic control, while surgeons showed no preference. MAC exhibited shorter anesthesia time than GA with lower anesthetics. These findings support the use of MAC in vitreoretinal surgery, especially for patients at risk of complications from GA.
Conclusion: Moderate sedation with MAC offers a safe and effective alternative to GA for vitreoretinal surgery, with similar outcomes, reduced anesthesia time, and lower drug doses. Further research with larger cohorts is warranted to validate these results and refine anesthesia protocols.
Keywords: moderate sedation, conscious sedation, monitored anesthesia care, general anesthesia, vitreoretinal surgeries
Introduction
In modern ophthalmic surgery, various anesthesia options, including topical anesthesia (TA), sub tenons anesthesia (STs), peribulbar anesthesia (PB), retrobulbar anesthesia (RB), and general anesthesia (GA), offer distinct advantages and disadvantages. Surgeon, anesthetist, and patient factors dictate anesthesia selection, emphasizing the need for tailored approaches to ensure optimal outcomes.1 During eye surgeries under general anesthesia, challenges like visual axis divergence and patient movements, though infrequent, pose risks to ocular health. Adjusting anesthesia and muscle relaxation can manage these issues but may not entirely eliminate them.2 Monitored anesthesia care (MAC) combines local anesthesia with sedation and analgesia for diagnostic or therapeutic procedures, providing safe conscious sedation, anxiety alleviation, and effective pain control.3,4 Vitrectomy, a common ophthalmic surgery, involves replacing the vitreous body with solutions like balanced salt solution or silicon oil. Indications include retinal issues such as vitreous hemorrhage, retinal detachment, or membrane peeling.5,6 Achieving optimal sedation levels in pars planar vitrectomy (PPV) is crucial to mitigate risks, yet surgeons lack reliable tools to assess anesthesia quality, creating uncertainty about potential complications.7 Developing objective evaluation methods is essential to enhance anesthesia practices and ensure patient safety. Research and development efforts are needed to advance eye anesthesia, improving surgical outcomes and overall patient care in ophthalmology.8 The aim of a prospective observational study is to compare sedation/MAC versus GA in patients undergoing pars plana vitrectomy, contributing to refining anesthesia protocols and optimizing surgical outcomes.
Materials and Methods
This was a prospective non-randomized clinical trial that 40 patients who were candidate for 23 gauge-pars plana vitrectomy (PPV) due to vitreoretinal disorders were included. Informed written consent was obtained from all participants. In accordance with the Declaration of Helsinki, this study was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1402.455). The patients were divided in to two groups. In one group, patients who were operated under general anesthesia and in the other group those who were operated with conscious sedation were included. Patients of two groups were matched together according to age, gender, diagnosis and type of surgery. If the patients could not tolerate conscious-sedation it could be converted to general anesthesia.
Anesthesia and Surgery
We employ four anesthesia models: minimal anesthesia, moderate anesthesia or conscious sedation, deep anesthesia, and general anesthesia.
In general anesthesia, four drugs are utilized: Midazolam at 0.03 mg/kg for anti-anxiety, Fentanyl at 1–2 ug/kg for a short-acting narcotic, Propofol at 2 ug/kg for sedation and Atracurium at 0.6 mg/kg for muscle relaxation.
For conscious sedation or moderate anesthesia, a combination of 6 cc Propofol 1%, 2 cc Lidocaine 2%, and 2 cc Fentanyl 50 ug/cc is administered using a 5–10 cc/hour pump syringe. Patient monitoring included heart monitoring, blood pressure, and oxygen saturation. Remifentanil at 10 ug/cc serves as a rescue drug in the presence of pain or 1 minute before any painful procedure like trocar insertion or scleral depression.
In MAC method, tetracaine drop was utilized. In this method, the patients were conscious and can obey and answer our questions. During surgery, we regularly asked patients about any pain and their comfort. Additionally, patients’ consciousness was checked regularly. In addition, O2 saturation decrease more than 5 were reported by anesthetics and then we asked the patient to breathe. If the patient did not respond and O2 saturation decrease continued, anesthesiologist would reduce medications, although painful stimulation of patients by surgeon like scleral depression may be useful. Finally, we evaluated anesthesia quality, surgical outcomes, anesthesia time, surgery time and recovery time and compared these parameters between two groups.
Measuring Quality of Immobilization
Parameters were graded depending on the type of anesthesia: central eye position, anesthesia, akinesia of the eye and or body, soft tissue or orbital hemorrhage, and absence of vitreous bulge.
Postoperatively, quality of immobilization was investigated by interviewing surgeon using a standardized questionnaire. Spiteri et al published and evaluated such a questionnaire in 2015.8 For the purpose of this study, the questionnaire was slightly modified while leaving the core score system unchanged (Figure 1). Patients and persons who analyzed information were blinded.
 |
Figure 1 Data collection questionnaire. Information gathered by the operating surgeon. Different parameters, including analgesia, eye position, akinesia of the eye and body, and eye softness, were assessed and graded as either present (yes) or absent (no). In addition, documentation of complications, duration of anesthesia and surgery and preference of anesthesiologist and surgeon was possible. |
Inclusion Criteria
- Patients who are cooperative for conscious sedation and candidate for vitreoretinal surgery
Exclusion Criteria
- Patients who are uncooperative for conscious sedation
- Difficult vitreoretinal surgeries
- Patients who are at risk for vitreoretinal surgeries and general anesthesia
- Patients who are addict
Statistical Analysis
Authors performed all statistical analyses using SPSS 25 (Chicago IL, USA). We compared the intervention group and control group using t-test and chi-square test. P-values less than 0.05 were considered statistically significant.
Results
Among the 20 participants receiving MAC anesthesia, 65% are male and 35% are female, demonstrating the gender distribution in the study, mirroring similar proportions observed in the GA group. There was no significant difference observed between the average ages of men and women participating in the study (P-value=0.599), with men averaging 61.69 years and women averaging 64.00 years (Table 1).
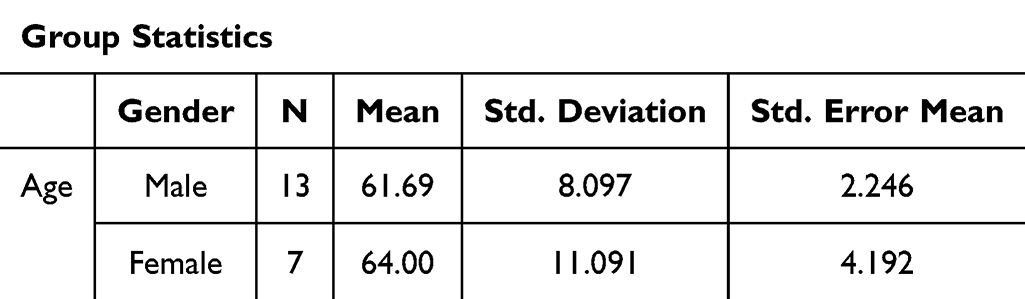 |
Table 1 Gender-Based Age Distribution of Patients |
The statistical analysis conducted for the variables of Analgesia, Eye position, Akinesia of body, and Hemodynamic stability revealed that the obtained p-values exceeded the critical value of 0.05. This suggests that there were no significant differences observed between patients who underwent surgery with MAC and those who received GA in terms of pain experience, eye and body movements, and hemodynamic stability. Therefore, it can be inferred that the outcomes of MAC anesthesia were comparable to those of GA.
Regarding the occurrences of soft tissue bleeding and vitreous protrusion, it is noteworthy that no adverse events were reported among patients in the MAC group. Notably, 100% of patients in this group exhibited the absence of these symptoms, mirroring the outcomes observed in patients receiving GA. This indicates a high level of consistency between the two anesthesia approaches in terms of mitigating potential complications during ophthalmic surgery (Table 2).
 |
Table 2 Analyzing Anesthesia Quality Distribution by Type |
The significance level for the comparison of anesthesia methods among anesthesiologists is notably lower than 0.05 (P-value=0.001). This indicates a profound disparity in preferences between the two methods. Specifically, in all 40 surgeries, the prevailing inclination among anesthesiologists leaned towards the MAC method. Conversely, the significance level concerning surgeon preferences exceeds 0.05 (P-value=0.231), suggesting no substantial difference in preference between the two anesthesia methods. Notably, all 20 patients underwent GA according to the surgeon’s preference. Additionally, in the subset of 20 patients subjected to the MAC method, the surgeon opted for this approach in 17 cases (85%) based on individual patient conditions and cooperation levels. These findings underscore a clear preference for the MAC method among anesthesiologists, while surgeons demonstrate no distinct preference between the two methods) (Table 3).
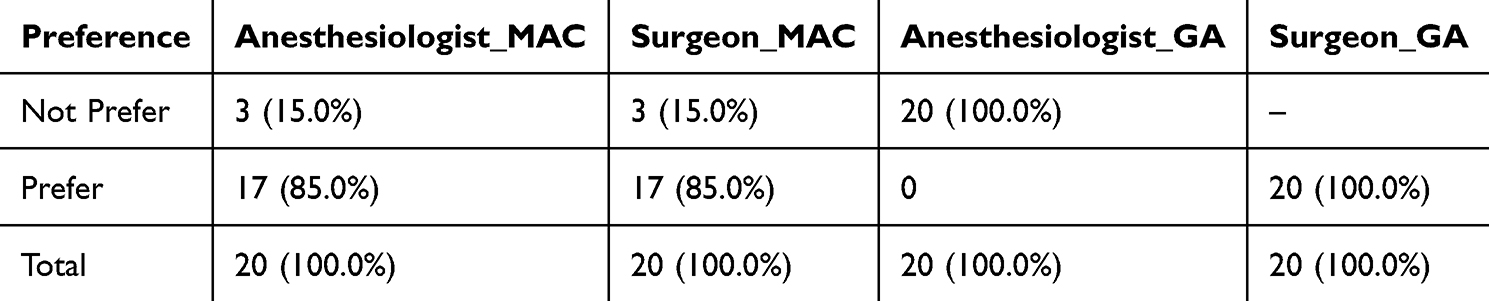 |
Table 3 Surgeon and Anesthesiologist Preference in GA and MAC Surgery |
Anesthesia induction time emerged as a pivotal factor, with MAC patients experiencing a notably shorter mean induction to surgery interval of 5.5 minutes compared to GA patients whose, induction time averaged at 17.5 minutes. This significant discrepancy underscores the efficiency of MAC in swiftly preparing patients for surgery, a difference confirmed by Mann–Whitney’s non-parametric test (P-value < 0.001). However, when examining surgery duration, no statistically significant difference was observed between the MAC and GA groups, with means of 43.25 and 44.75 minutes, respectively (P-value = 0.678). This suggests that once the surgical procedure commenced, the choice of anesthesia method did not substantially impact the duration of the operation.
Remarkably, post-surgery recovery time exhibited a substantial difference, with MAC patients spending an average of 6.75 minutes in recovery, significantly shorter than the 14.00 minutes for GA patients (P-value < 0.001). This disparity underscores the efficiency of MAC in facilitating quicker recovery and potentially reducing postoperative complications. When considering total procedural time, MAC again emerged as the more time-efficient option, with an average duration of 55.50 minutes compared to GA’s 76.25 minutes (P-value < 0.001). Effect size analysis using Cohen’s d further elucidated the impact of anesthesia methods on procedural outcomes. The effect size for anesthesia induction to surgery time was notably high at 5.77, indicating a significant difference favoring MAC. Conversely, the effect size for surgery duration was small at 0.134, suggesting no substantial difference between the two methods. However, recovery time (2.25) and total procedural time (1.74) exhibited relatively high effect sizes, highlighting significant efficiency gains with MAC (Table 4).
 |
Table 4 Comparison of Anesthetic Techniques: Anesthesia and Surgery Time Analysis |
These findings underscore the multifaceted impact of anesthesia methods on procedural timelines and patient recovery, emphasizing the importance of tailored approaches in surgical care. The preoperative diagnosis distribution varying from 5% to 35% of the total population (Table 5).
 |
Table 5 Diagnosis Distribution of Diseases |
Additionally, among 40 patients, 22 had cataract requiring simultaneous cataract surgery. Furthermore, 18 patients were pseudophakic.
Discussion
We found that pars plana vitrectomy with moderate sedation can be successfully performed without conversion to GA in all (100%) patients. It represented that pars plana vitrectomy with moderate sedation could be tolerated easily. Different studies represented that conscious sedation can be safely applied for transcatheter aortic valve replacement.9,10 Similarly in our study that six parameters including pain, eye and body movements, soft tissue hemorrhage, vitreous bulge and hemodynamic stability were considered, there was no statistically significant difference between two methods and the outcomes of MAC were not inferior to outcomes of GA. Since dosage of systemic anesthetic medications in GA is more than MAC, systemic side effects in MAC are probably less and hemodynamic controllability seems to be more in MAC. In our study, no ocular complication or surgery failure was reported in both groups and all surgeries were successful in MAC and GA group, therefore MAC does not affect the safety of patients and the success of the surgery. These results are consistent with a meta-analysis that compared conscious sedation with GA in transcatheter aortic valve replacement.11 Comparing the time of surgery between two groups demonstrated no statistically significant difference, however the total duration of anesthesia was greater in GA than MAC. As a result, MAC saves more time and reduces costs. Although in 3 patients; pain, eye and body movement were reported, but it was not significant and surgery was continued. However, it may be due to non-prescribing Remifentanil in the first few patients as a rescue drug 1 minute before painful procedures like trocar insertion or scleral depression. In many studies, conscious sedation was used together with local/regional anesthesia,12 whereas in this study just topical anesthesia was used without other local/regional anesthesia, which are more aggressive and probably has more complications. Morley et al study demonstrated that the trend of patients who experienced both midazolam and propofol during vitreoretinal surgeries were in favor of propofol for intraoperative sedation.13 Accordingly, we used propofol instead of midazolam in our study. During surgery, patients’ consciousness should be evaluated by surgeon along with anesthetists regularly to control the level of anesthesia and any change in level of consciousness should be reported to anesthetist to reduce medication and vice versa, any significant O2 saturation decrease should be reported to surgeon by anesthetist in order to ask the patient to breathe. Therefore, in conscious sedation method, cooperation between surgeon, anesthetist and patient is critical. Overall, the anesthesiologist preferred MAC to GA due to more hemodynamic stability and controllability in MAC method. It indicates that MAC seems to be hemodynamically more safe than GA. However, there was no statistically significant difference in preference of surgeon between two groups. It indicates that MAC is not inferior to GA. limitations of this study included small number of patients and non-randomized selection of patients. These findings suggest that MAC can be safely applied for vitreoretinal surgeries with phacoemulsification and seems to be an appropriate substitution for GA especially for patients who are at risk for GA. However, patient and surgeon preference, as well as anesthesiologist and surgeon experience, have important roles in choosing the type of anesthesia. Nevertheless, further studies with larger sample sizes are required in the future to more accurately evaluate the safety of this method.
Conclusion
In this study, MAC compared with GA resulted in similar outcomes and success rate, without any complication, less anesthesia time, lower dose of anesthetics. These findings suggest that moderate sedation can be safely applied for vitreoretinal surgeries.
Abbreviations
MAC, monitored anesthesia care; GA, general anesthesia; TA, topical anesthesia; STs, sub-Tenons anesthesia; PB, peribulbar anesthesia; RB, retrobulbar anesthesia; GA, general anesthesia; PPV, pars planar vitrectomy.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent for Participation
This study protocol was reviewed and approved by the ethics committee at Shiraz university of Medical Sciences (IR.SUMS.MED.REC.1402.455). The trial was registered in Iranian Registry of Clinical Trials (registration number: IRCT20201120049450N3) on December 10, 2023, adhered to the CONSORT statement and was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all participants, who were informed of their rights, including the option to withdraw from the study at any stage.
Acknowledgments
The authors would like to thank the Vice-Chancellor of Shiraz University of Medical Sciences for supporting this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kumar C, Eke T, Dodds C, et al. Local anaesthesia for ophthalmic surgery—new guidelines from the Royal College of Anaesthetists and the Royal College of Ophthalmologists. Eye. 2012;26(6):897–898. doi:10.1038/eye.2012.82
2. Rossiter J, Wood M, Lockwood A, Lewis K. Operating conditions for ocular surgery under general anaesthesia: an eccentric problem. Eye. 2006;20(1):55–58. doi:10.1038/sj.eye.6701789
3. Das S, Ghosh S. Monitored anesthesia care: an overview. J Anaesthesiol Clin Pharmacol. 2015;31(1):27–29. doi:10.4103/0970-9185.150525
4. Ghisi D, Fanelli A, Tosi M, et al. Monitored anesthesia care. Minerva Anestesiol. 2005;71(9):533–538.
5. Wong SC, Lee TC, Heier JS, Ho AC. Endoscopic vitrectomy. Curr Opin Ophthalmol. 2014;25(3):195–206. doi:10.1097/ICU.0000000000000052
6. Aylward G. Sutureless vitrectomy. Ophthalmologica. 2011;225(2):67–75. doi:10.1159/000317910
7. McCusker S, Chaudhary V, Blew P, et al. Sedation during vitreoretinal surgery: practice patterns in Canada. Can J Anaesth. 2020;67:1439–1441. doi:10.1007/s12630-020-01689-2
8. Spiteri N, Sidaras G, Czanner G, et al. Assessing the quality of ophthalmic anesthesia. J Clin Anesth. 2015;27(4):285–289. doi:10.1016/j.jclinane.2015.01.008
9. Thiele H, Kurz T, Feistritzer HJ, et al. General versus local anesthesia with conscious sedation in transcatheter aortic valve implantation: the randomized SOLVE-TAVI trial. Circulation. 2020;142(15):1437–1447. doi:10.1161/CIRCULATIONAHA.120.046451
10. Harjai KJ, Bules T, Berger A, et al. Efficiency, safety, and quality of life after transcatheter aortic valve implantation performed with moderate sedation versus general anesthesia. Am J Cardiol. 2020;125(7):1088–1095. doi:10.1016/j.amjcard.2020.01.002
11. Hung KC, Chen JY, Hsing CH, et al. Conscious sedation/monitored anesthesia care versus general anesthesia in patients undergoing transcatheter aortic valve replacement: a meta-analysis. Front Cardiovasc Med. 2022;9:1099959. doi:10.3389/fcvm.2022.1099959
12. Vann MA, Ogunnaike BO, Joshi GP. Sedation and anesthesia care for ophthalmologic surgery during local/regional anesthesia. Anesthesiology. 2007;107(3):502–508. doi:10.1097/01.anes.0000278996.01831.8d
13. Morley HR, Karagiannis A, Schultz DJ, et al. Sedation for vitreoretinal surgery: a comparison of anaesthetist-administered midazolam and patient-controlled sedation with propofol. Anaesth Intensive Care. 2000;28(1):37–42. doi:10.1177/0310057X0002800106
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.