Back to Archived Journals » Open Access Surgery » Volume 13
Congenital Isolated Penile Torsion: A Case Report in 2 Brothers
Authors Ahmed F ![]() , Al-wageeh S
, Al-wageeh S ![]() , Al-shami E
, Al-shami E ![]() , Al-naggar K
, Al-naggar K ![]() , Askarpour MR
, Askarpour MR ![]() , Naji M
, Naji M
Received 21 August 2020
Accepted for publication 24 September 2020
Published 12 October 2020 Volume 2020:13 Pages 75—78
DOI https://doi.org/10.2147/OAS.S275810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Faisal Ahmed,1 Saleh Al-wageeh,2 Ebrahim Al-shami,1 Khalil Al-naggar,1 Mohammad Reza Askarpour,3 Mohammed Naji4
1Urology Research Center, Al-Thora General Hospital, Department of Urology, Ibb University of Medical Science, Ibb, Yemen; 2Department of General Surgery, Ibb University of Medical Science, Ibb, Yemen; 3Department of Urology, Shiraz University of Medical Sciences, Shiraz, Iran; 4Department of Urology, Dar Al-Shifa Hospital, Ibb, Yemen
Correspondence: Faisal Ahmed
Al-Thora General Hospital, Alodine Street, Ibb 71234-44251, Yemen
Tel/Fax +9674407128
Email [email protected]
Abstract: Penile torsion is a congenital anomaly rarely detected in isolation and mostly accompanied by hypospadias and chordee. It could also happen iatrogenically after penile circumcision. In previous literature, the incidence rate of isolated penile torsion has been reported between 1.7 and 27%. The diagnosis and treatment of penile torsion have been illustrated in the previous published articles. However, there are few published studies on the familial predominance of penile torsion. Additionally, the clinical characteristics and potential hereditary components of penile torsion are not well known. Therefore, we studied a 12-year-old boy with a severe 180-degree penile torsion, which surgically corrected and his one-year-old brother, who had mild penile torsion and surgically corrected during circumcision.
Keywords: congenital anomaly, familial, penile torsion, surgery
Plain Language Summary
Penile torsion is a congenital anomaly which is rarely detected in isolation, and mostly accompanying with hypospadias and chordee. The incidence rate of isolated penile torsion has been reported between 1.7 and 27%. based on the degree of glanular angulation, the severity of penile torsion is classhfied into mild; less than 45 degree, moderate; between 45-90 degree, or sever; more than 90 degrees. There are few published studies focused on the familial predominance of penile torsion. Additionally, the clinical characteristics and potential hereditary components are not well known. We present a severe penile torsion 180 degrees in a 12 years old boy, which surgically corrected and mild penile torsion in one-year old his brother. The surgical procedure includes degloving the penis, Bucks fascia resection, some incision in the base of the penis, plication of tunica, and dorsal dartos flap. Three months after the operation, the pateint had a successful correction of penile rotation with no residual rotation.
Introduction
Penile rotation firstly was defined by Horton and Devine in 1973. It is a 3D rotation of corporal bodies of the penis in an abnormal way.1 Due to limited data on this subject, the actual incidence of this anomaly is unknown; therefore, it may remain undetected until either circumcision or the foreskin retractility. The overall rate of penile torsion was reported between 1.7% to 27% in previous literature when the rotation of corporal bodies is more than 90 degrees; this prevalence rate could decrease to 0.7% of cases.2,3 It could occur in isolation or in accompany with hypospadias, chordee, or even after penile circumcision.3 Based on the degree of glanular angulation, the severity of penile torsion is classified into mild; less than <45 degrees, moderate; between 45–90 degrees, or severe; more than 90 degrees. However, penile torsion degrees in the majority of cases (87%) are between 10 and 20 degrees.2 Cosmetic, functional, and sexual activity are the main reasons for surgical penile corrections.1 Treatment of penile torsion is a surgical exploration including the development of the penis, Buck’s fascia resection, some incision in the base of the penis, and cutting angular ellipses of corporeal tissue followed by plication of tunica, dorsal dartos flap, and suturing the lateral aspect of the corpus cavernosum to the pubic periosteum.4 In middle age, the functional outcomes of isolated penile torsion are not completely demarcated. However, in a study, about 12% of men visiting infertility/sexual dysfunction clinics in Egypt had penile torsion.5 Considering the small number of studies on potential hereditary component of congenital penile torsion, we presented our case series.
Case Report
Two brothers, aged 1 and 12 years old, were examined by a urologist. Patients’ parents were involved with cosmetic and sexual problems of the older child while younger brother needed circumcision. The patients were evaluated physically and in terms of history. Associated anomalies of penile layers such as hypospadias were absent in both cases. However, the older boy had a history of penile torsion at birth.
The first brother was diagnosed with an isolated 180-degree clockwise penile rotation (Figure 1). As previously described, the problem had been surgically corrected (Figure 2). The surgical procedure includes degloving the penis, Buck’s fascia resection, some incision in the base of the penis, plication of tunica, and dorsal dartos flap. Three months after the operation, the patient had a successful correction of penile rotation with no residual rotation. The second brother (younger) was visited and during a physical examination, an isolated 20-degree torsion was detected, which was surgically corrected during circumcision.
 |
Figure 1 Showing penile torsion (showing the meatus on dorsal side). |
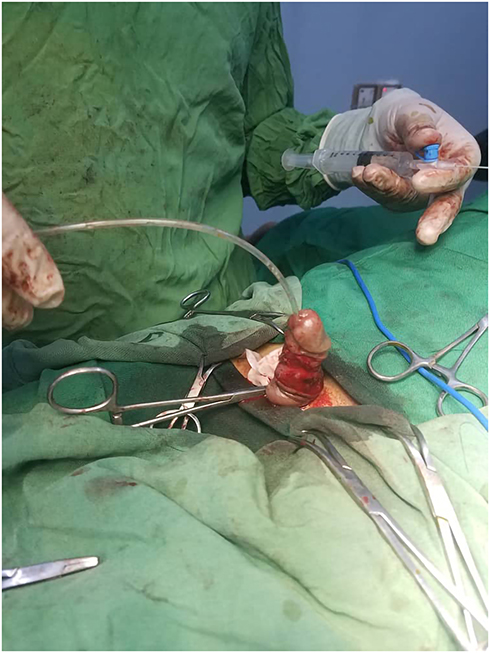 |
Figure 2 Showing correction of penile torsion. |
Discussion
The difference between penile curvature and penile torsion in the published articles has not clarified so that both terms have been frequently used for both bending of the penis and rotation of the penis. Many authors have referred to the bending of the penis as curvature, while rotation has been often used when there was a torsion on the penile axis.5 Moreover, few published reports have recognized a potential hereditary trace in penile rotation etiology, such as Paxson and associations. They have observed congenital torsion of the penis in three neonates with a previous history of penile torsion in their fathers.6
Isolated congenital penile torsion might be familial, father to son. There are a few studies reporting this malformation in brothers, such as Gunduz et al as well as the present case report.3 Also, a strong association has been found between maternal age and parity number and the incidence of penile torsion.7 On the other side, the etiology of isolated penile rotation is not known yet.8
Several studies have suggested the unequal growth of the corpora cavernosa, eccentric fusion of the ectodermal/endodermal folds, and false attachment of the ectoderm (skin and dartos fascia), as possible etiologies.1,8 For example, Bauer et al assumed that the groin area’s fetal heel is the mechanism leading to the deformed Buck’s fascia. However, this theory could not explain the counter-clockwise torsion.8
Rotation more than 60 degrees is rare. The shaft of the penis is usually rotated to the left, in a counter-clockwise; however, despite having a severe torsion, the rotation in our cases was in the clockwise direction.2 Although radiologic imaging, such as cavernosography and magnetic resonance imaging (MRI) is highly beneficial to show how the corporal bodies are wrapped around each other,9 unfortunately, due to regional conflict, MRI was out of our reach. The reasons for surgery in the penile rotation could be cosmetic, parents’ psychological concerns, and functional sexual activity.9 However, surgical correction has been clinically indicated only in 4% of patients.10
The latest available surgical procedures include the release of skin adhesions and realignment of the skin after evaluating torsion severity and resection of Buck’s fascia and the tunica albuginea based on the severity.3 However, multiple studies have shown that in the short term, the dorsal dartos flap rotation technique could provide excellent outcomes.8,10 For instance, Gunduz and associations performed the degloving and realignment procedure, which is a minimal and noninvasive method compared to other techniques. However, in moderate or severe penile torsion such as our case, this technique could not be strong enough to hold the expanding and rotating force of an erection and may lead to under correction or recurrence.3
Modified Nesbit procedure is another procedure used in severe penile torsion and includes the excision of angled ellipses from the corporal tissue and plication. It is also accompanied by complications, such as neurovascular injury, loss of penile sensitivity, lymphedema, ugly scarring at the base of the penis, penile shortening, and hemorrhage.1,10,11
Bhat et al performed surgery on 116 patients with hypospadias and penile torsion. Penile degloving was performed on 11%, mobilization of the urethral plate and the corpus spongiosum were performed in 28%, mobilization of the proximal urethra was performed in 40%, and mobilization of the urethral plate into the glans was performed in 21% of the cases.4
Conclusion
Penile torsion remains a debatable condition since there is no consensus on its complete definition and genetic inheritance. Therefore, we suggest that if one sibling is diagnosed with penile torsion, the other male siblings should be thoroughly examined in this regard.
Consent for Publication
Written informed consent for publication of this case was obtained from the patient parents.
Ethical Consideration
The parental written informed consent was obtained for publication of the case details including the publication of the images.
Institutional Approval
The operation is done following standard protocols and is reported in a way to hide patients’ identities completely. Thus, no institutional approval was required.
Disclosure
The authors declare that they have no competing interests.
References
1. Taghavi K, Upadhyay V, Mirjalili SA. Familial isolated congenital penile torsion. J Pediatr Surg Case Rep. 2013;1(8):239. doi:10.1016/j.epsc.2013.04.009
2. Sarkis PE, Sadasivam M. Incidence and predictive factors of isolated neonatal penile glanular torsion. J Pediatr Urol. 2007;3(6):495. doi:10.1016/j.jpurol.2007.03.002
3. Gunduz M, Ciftci I. Isolated penile torsion in brothers: a case report. Arch Clin Exp Surg. 2012;1:122. doi:10.5455/aces.20120409014645
4. Bhat A, Bhat MP, Saxena G. Correction of penile torsion by mobilization of urethral plate and urethra. J Pediatr Urol. 2009;5(6):451. doi:10.1016/j.jpurol.2009.05.013
5. Shaeer O. Torsion of the penis in adults: prevalence and surgical correction. J Sex Med. 2008;5(3):735. doi:10.1111/j.1743-6109.2007.00709.x
6. Paxson CL, Corriere LJN
7. Bhat A, Bhat M, Kumar V, et al. The incidence of isolated penile torsion in North India: a study of 5018 male neonates. J Pediatr Urol. 2017;13(5):
8. Bauer R, Kogan BA. Modern technique for penile torsion repair. J Urol. 2009;182:286.
9. Hsieh J-T, Wong W-Y, Chen J, et al. Congenital isolated penile torsion in adults: untwist with plication. Urology. 2002;59(3):438. doi:10.1016/S0090-4295(01)01596-5
10. Zvizdic Z, Milisic E, Vranic S. Penile degloving and dorsal dartos flap rotation surgery in the management of severe isolated penile torsion in a 6-year-old boy. Acta Medica (Hradec Kralove). 2020;63(1):52. doi:10.14712/18059694.2020.16
11. Waterloos M, Hoebeke P, Spinoit A-F. Penile rotation. In:Fahmy M, editor. Congenital Anomalies of the Penis. Cham,Switzerland: Springer; 2017:79–84. doi:10.1007/978-3-319-43310-3_12.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.