Back to Journals » International Medical Case Reports Journal » Volume 18
Congenital Acute Myeloid Leukemia (AML): A Case Report
Authors Alsharidah S, Almatar E
Received 30 November 2024
Accepted for publication 11 May 2025
Published 20 May 2025 Volume 2025:18 Pages 585—590
DOI https://doi.org/10.2147/IMCRJ.S499579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Sondus Alsharidah,* Eman Almatar*
Department of Pediatrics, NBK Children Specialized Hospital, Sabah, Kuwait
*These authors contributed equally to this work
Correspondence: Eman Almatar, Department of Pediatrics, NBK Children Specialized Hospital, Sabah, Kuwait, Email [email protected]
Background: Congenital acute myeloid leukemia (AML) is a rare but critical hematologic malignancy diagnosed in neonates and associated with a high mortality rate.
Case Presentation: This report describes a 3-month-old female diagnosed with congenital AML, characterized by mixed lineage leukemia (MLL) gene rearrangement. The patient presented with severe complications, including typhlitis, abscess, seizures, and pericardial effusion.
Management and Outcomes: Despite the challenges posed by the patient’s age and the severity of her condition, she responded well to initial treatment. However, her long-term prognosis remains uncertain. Hematopoietic stem cell transplantation (HSCT) is being considered as part of her ongoing management.
Conclusion: Early diagnosis and tailored treatment strategies for congenital AML are crucial. This case underscores the need for continued research to refine treatment protocols aimed at improving survival rates in this vulnerable population.
Keywords: neonatal leukemia, MLL gene rearrangement, chemotherapy, hematopoietic stem cell transplantation, cytogenetics in AML
Introduction
Acute myeloid leukemia (AML) is a highly heterogeneous group of hematopoietic malignancies characterized by abnormal clonal proliferation of myeloid hematopoietic stem cells, impaired differentiation, and resistance to apoptosis. The most common mutations found in AML include Fms-Like Tyrosine Kinase 3 (FLT3), Nucleophosmin 1 (NPM1), Isocitrate Dehydrogenase 2 (IDH2), DNA Methyltransferase 3 Alpha (DNMT3A), Neuroblastoma RAS Viral Oncogene Homolog (NRAS), and compound mutations.1 Pediatric AML accounts for 3–10% of primary childhood leukemias and presents with a broad range of symptoms, including low-grade fever, diarrhea, easy bruising, failure to thrive, and life-threatening conditions.2 Congenital leukemia, a rare subset occurring in neonates, has an estimated incidence of 1 in 5 million live births, with AML being the predominant subtype. This case report presents a case of a 3-month-old female diagnosed with congenital AML highlighting diagnostic challenges and management considerations.
Case Presentation
A 3-month-old female presented to the outpatient department with a one-day history of fever. A complete blood count revealed leukocytosis, and blood film examination showed 87% blast cells. Further investigations, including immunophenotyping, minimal residual disease (MRD) analysis, and molecular studies from a peripheral blood work up led to the diagnosis of AML with cytogenetics of mixed lineage leukemia (MLL) gene rearrangement, confirmed by fluorescence in situ hybridization (FISH) technique. Due to her elevated white blood cell (WBC) count, cerebrospinal fluid (CSF) and bone marrow examinations were postponed.
During admission, the patient developed dyspnea and irritability, crying, respiratory distress, and worsening in the left leg cellulitis. A chest X-ray was taken, which showed marked cardiomegaly (Figure 1), prompting an echocardiogram that reported moderate pericardial effusion. The patient received a platelet transfusion. The condition was reassessed by repeating a chest X-ray (Figure 2), and echocardiography showed improvement. The patient was advised to start colchicine for three months and methylprednisolone for three days, followed by a tapering regimen over two weeks.
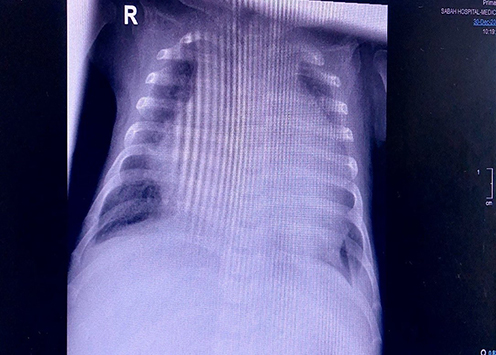 |
Figure 1 Chest X-ray findings revealing cardiomegaly. |
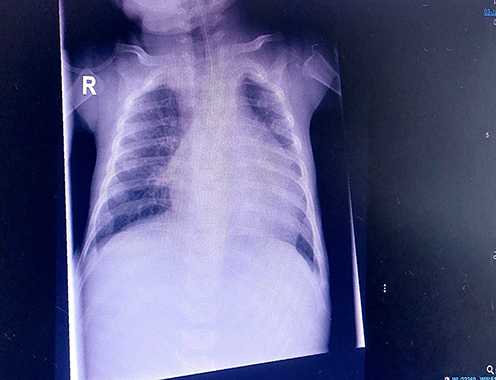 |
Figure 2 Chest X-ray findings revealing resolved cardiomegaly. |
Echocardiography Findings Revealing Pericardial Effusion
- Moderate pericardial effusion: 10 mm at the lateral wall of the left ventricle, 6 mm at the apex, 7 mm behind the left atrium, no diastolic collapse, 8 mm anteriorly.
- Good left ventricular function.
Echocardiography Findings After Platelet Transfusion
- Good ventricular function.
- Pericardial effusion around the right atrium: 4 mm.
- Pericardial effusion around the right ventricle: 4 mm.
- Improved resolution of other previously observed effusions.
Laboratory Investigations at Diagnosis
- Complete Blood Count with Peripheral Smear.
- Hemoglobin (Hb): 105 g/L (Normal range: 140–220 g/L).
- WBC Count: 171×109/L (Normal range: 9–30×109/L).
- Immature Cells: 84% (Normal range: 0–5%).
- Platelet Count: 135×109/L (Normal range: 150–450×109/L).
- Biochemical Profile.
- Normal except for high LDH: 764 U/L (Normal range: 2.09–3.67 U/L).
- Coagulation Profile.
- APTT: 34.8 sec (Normal range: 31–55 sec).
- PT: 11.5 sec (Normal range: 10–16 sec).
- INR: 1.17 (Normal range: 0.8–1.2).
- Ratio: 1.17 (Normal range: 1.0–1.3).
- Hemoglobin Electrophoresis.
- Hb A: 19.7% (Normal range: 10–40%).
- Hb F: 80.3% (Normal range: 60–90%).
- G6PD & Immunoglobulin: Normal
- Virology & Hepatitis Screening: Negative
- Immunophenotyping.
- CD11b: 95% (Normal range: 70–90%).
- HLA-DR: 99% (Normal range: 90–100%).
- CD33: 100% (Normal range: 80–100%).
- CD14: 64% (Normal range: 50–80%).
- CD15: 56% (Normal range: 50–90%).
- CD64: 99% (Normal range: >90%).
- CD56: 95% (Normal range: <20%).
- 75% of cells gated at the myeloid region.
- Cytogenetic Study by FISH Technique.
- 70% of MLL gene rearrangement detected (Chromosome 11, 19)
- Molecular Study.
- KMT2A (8) -ELL (3): Ch. 11: 118353210, Ch. 19: 18576728.
Imaging Procedures at Diagnosis
- Chest X-ray: Normal lung fields and cardiac size. No mediastinal mass.
- Echocardiography: Left ventricular ejection fraction (LVEF) 70%, small patent foramen ovale, good ventricular function.
- Ultrasound Abdomen: Normal
There was no family history of malignancies or blood disorders, though her sister had died at 10 days old from a condition suggestive of Edward syndrome, though this remains unconfirmed.
She was started on induction chemotherapy as per the UK AML 17 protocol with cytarabine and mitoxantrone. Due to her high WBC count, she initially received a low-dose cytarabine (1.5 mg/kg) for 4 days before receiving full-dose chemotherapy. After treatment, she developed severe neutropenia and thrombocytopenia. Additionally, she experienced diarrhea, with stool tests returning negative for infectious causes. Imaging revealed thickened bowel loop walls, leading to a diagnosis of typhlitis, which was managed accordingly.
The next day, while on systemic antibiotics, she developed redness and swelling of her left leg, which progressed to an abscess. Two days later, she experienced abnormal jerking movements of her right upper limb, accompanied by stiffness lasting less than a minute. Buccal midazolam was administered as an emergency measure, and after a pediatric neurology consultation, levetiracetam (Keppra) 60 mg twice daily was started.
Over the next few days, the patient became dyspneic and irritable, with worsening respiratory distress and left leg cellulitis. A chest X-ray revealed cardiomegaly, and an echocardiogram showed pericardial effusion. This condition improved following platelet transfusion, and colchicine was started for three months along with a three-day course of methylprednisolone which was gradually tapered over two weeks. Her left leg cellulitis improved, and she remained afebrile.
The patient continued well and stable for a while until she began experiencing episodes of eye-rolling and breath-holding, lasting about a minute and causing facial cyanosis, were observed. Buccal midazolam was administered again as an emergency and after neurologist evaluation, her levetiracetam dose was increased. No further convulsions were seen ever since.
The current plan is to continue chemotherapy and supportive care until the HSCT team evaluates the patient for a possible bone marrow transplant after achieving remission.
Discussion
Congenital leukemia refers to leukemia diagnosed at birth or within the first few months of life.3 Despite its rarity, congenital leukemia is a significant cause of neonatal mortality, and one of the leading causes of death from malignancy during the first month of life.4,5 Our case aligns with the diagnostic criteria for congenital leukemia, which includes proliferation of immature white blood cells.6
Cytogenetic abnormalities play a prominent role in risk stratification of AML, with translocation-associated AML presenting a unique phenotype.7 Infants diagnosed with AML within the first few months of life often present with non-specific symptoms such as low-grade fever, diarrhea, hepatomegaly, failure to thrive, lethargy, and, in some cases, seizures.8 Immunophenotyping by flow cytometry, along with morphology and cytogenetic studies, is critical for the precise diagnosis of congenital leukemia.9
Choosing the optimal treatment strategy for infants diagnosed with congenital AML is very challenging due to the vulnerability of the neonatal population and the need for age-appropriate dose adjustments. Increasing treatment intensity is associated with a higher risk of toxicity, including both early and late cardiotoxicity. Some studies suggest that infants with congenital AML may have improved outcomes with HSCT. However, determining the optimal timing for transplantation remains challenging due to the high toxicity and mortality risks associated with the procedure.4
Recent advances in HSCT protocols have focused on reducing transplant-related mortality while maintaining long-term remission rates. Novel conditioning regimens, such as reduced-intensity conditioning (RIC) and targeted therapies integrated with HSCT, have shown promise in improving outcomes in high-risk pediatric AML cases, including congenital AML. Advances in graft manipulation, such as T-cell depletion and umbilical cord blood transplantation, have expanded donor options while reducing graft-versus-host disease (GVHD). Additionally, post-transplant maintenance strategies using targeted agents, such as FLT3 inhibitors or hypomethylating agents, are being explored to minimize relapse risk. These evolving strategies highlight the potential of HSCT as a curative approach while addressing its historically high treatment-related risks.
Further studies and clinical trials are necessary to identify the most effective and least harmful treatment protocols for congenital AML. HSCT remains a viable option for improving survival outcomes in selected patients, and ongoing research into optimizing transplant regimens may enhance the feasibility and safety of this approach.
Conclusion
This case highlights the complexity and challenges in diagnosing and treating AML in neonates. Despite advancements in chemotherapy protocols and supportive care, managing the disease in neonates remains challenging due to their heightened vulnerability to treatment-related toxicities. HSCT offers a potential pathway to improve survival, but its timing and associated risks necessitate careful consideration. This case underscores the need for continued research to refine treatment protocols for congenital AML, aiming to enhance survival rates and reduce complications in this vulnerable population.
Ethical Approval
Ethical approval was not required for this case report, as the patient was referred to the hospital for normal treatment. Patient was treated and discharged according to standard hospital procedures. However, since such cases are rare at the medical literature, we decided to publish this case and obtained a written consent from the guardians of the pediatric patient.
Human and Animal Guidelines
“Not applicable” as this case involved routine clinical care.
Informed Consent
Written informed consent was obtained from legal guardians for the publication of any potentially identifiable images or data included in this article.
Medical Writing Support
Medical Writing support was provided by Al Essa Medical and Scientific Group.
Funding
The publication of this article was supported by NBK Children Specialized Hospital, Kuwait.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374:2209–2221. doi:10.1056/NEJMoa1516192
2. Masoumi Dehshiri R, Hashemi AS, Neamatzadeh H, et al. A case report: acute myeloid leukemia (FAB M7). Iran J Ped Hematol Oncol. 2014;4(4):188–190.
3. Perkins SL. Hematopoietic system. In: Gilbert-Barness E, editor. Potter’s Pathology of the Fetus, Infant, and Child. Philadelphia: Mosby Inc; 2007.
4. Green K, Tandon S, Ahmed M, et al. Congenital Acute Myeloid Leukemia: Challenges and Lessons. Leukemia and Lymphoma. London: Taylor and Francis Group; 2020.
5. Orbach D, Samacki S, Brisse HJ, et al. Neonatal cancer. Lancet Oncol. 2003;25(5).
6. Iqbal W, Khan F, Muzaffar M, et al. Congenital leukemia in Down Syndrome. Intern J Pathol. 2005;3(2).
7. Haferlach T, Kohlmann A, Klein H, et al. AML with translocation t(8;16) (p11;p13) demonstrates unique cytomorphological, cytogenetic,molecular and prognostic features. Leukemia. 2009;23(5):934–943. doi:10.1038/leu.2008.388
8. Prakash KP, Rau A, Bhat S, et al. Congenital Leukemia: a diagnostic dilemma. Indian J Med Paediatr Oncol. 2008;4:41–43.
9. McCoy JP, Overton WR. Immunophenotyping of congenital leukemia. Division of pediatric hematology oncology. Cooper Hospital, New Jersey. Commun Cytometry. 1995;22.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.