Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Comprehensive physical domain care needs of burn patients: a qualitative study
Authors Mohammadhossini S ![]() , Ahmadi F, Gheibizadeh M
, Ahmadi F, Gheibizadeh M ![]() , Saki Malehi A, Zarea K
, Saki Malehi A, Zarea K ![]()
Received 14 May 2019
Accepted for publication 29 July 2019
Published 21 August 2019 Volume 2019:12 Pages 573—581
DOI https://doi.org/10.2147/CCID.S215517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sima Mohammadhossini,1 Fazlollah Ahmadi,2 Mahin Gheibizadeh,3 Amal Saki Malehi,4 Kourosh Zarea3
1Nursing & Midwifery School, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 2Department of Nursing, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran; 3Nursing Care Research Center in Chronic Diseases, Nursing & Midwifery School, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 4Biostatistics and Epidemiology Department, Public Health Faculty, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Correspondence: Kourosh Zarea
Nursing Care Research Center in Chronic Diseases, Nursing & Midwifery School, Ahvaz Jundishapur University of Medical Sciences, Postal Box 159, Ahvaz City, Khuzestan Province 61357-15794, Iran
Tel +98 916 615 4943
Email [email protected]
Introduction: Burn patients have various physical needs. To provide full care for such patients, we need a broad range of services. The current study aims at showing the physical needs of burn patients.
Methods: The current qualitative study has been done through content analysis. The data were collected from 20 in-depth, unstructured individual interviews with hospitalized patients with burns on more than 25% of their body, nurses, physiotherapists, and psychologists. The participants were selected by purposive sampling. The data were analyzed with a conventional content analysis approach using the Elo and Kyngas method.
Results: By analyzing the data, 7 main categories were obtained from 932 primary codes: the necessity to provide optimal physiotherapy, the necessity of the patient’s overall physical assessment, the necessity of monitoring and coordination in care, healthy nutrition for burn patients, the need for pharmacotherapy, the need for pain reliefs, and finally the theme for comprehensive physical care needs in burn patients.
Conclusion: According to the findings, by applying the extracted categories, it is possible to provide quality care based on the patient’s individual needs. This can help speed up the treatment and shorten the length of hospitalization significantly.
Keywords: care needs, burn, physical domain, qualitative study
Introduction
The need is defined as the gap between the current situation and the desired situation.1 The physiological need is a concept basically derived to explain motivation. This concept is the main foundation for Maslow’s hierarchy of needs. In addition, the physiological needs are the bases for man’s survival. This means that physiological needs are universal human needs.2 Peplau’s theory emphasizes on helping the patients to understand their needs and on practicing the humane principles to solve the patients’ problems.3 Understanding the needs is the main factor in providing different services and performing various tasks aimed at improving the comfort and ease in target populations, including the patients.1
Burns are one of the major health problems all around the world, especially in the developing countries.4 Burn injury is one of the most destructive injuries around the world. An estimated 265,000 deaths every year are caused by burns globally. Fire-related burns alone caused over 300,000 deaths per year, with more deaths from scalds, electricity, chemical burns and other forms of burns.5 About 95% of the injured are in countries with low or average incomes. Burns impose huge expenses on health care systems throughout the world. This is one of the greatest concerns for the health care system in Iran: the annual rate of burns is 129.85 in 1000 people.6 The burn penetrates in the surface tissue (epithelial, connective, muscular, and nervous tissue), thoroughly damages the skin, and reaches the deeper layers below the subcutaneous tissue, muscles, tendons and bones.7 The degree of the injury depends on the Abbreviated Burn Severity Index (ABSI), based on 5 criteria: age, gender, respiratory tract damages, depth of burn (based on the burn degree) and percentage. Burns cause physiological changes such as cardiovascular issues, water and electrolyte disturbances, respiratory, renal, gastrointestinal, immune disorders, and abnormality in body’s temperature-regulating system.8
The main priorities in burn emergency care are as follows: blood circulation, respiration and airway management. After a primary stabilization in respiration and blood circulation, it is important to examine and classify the injuries in terms of the burn percentage. Burns are classified according to the size, depth, and etiological factors, which determine the patient’s need for hospitalization.9
Sheridan (2002) divides care for burn patients into 4 phases: initial evaluation and resuscitation; initial wound excision and its physiological closure; complete wound closure; and rehabilitation and reconstruction.10
Most nurses and nursing researchers agree that care, meaning nursing measures, is the key part of nursing.11–13 Being complicated and a completely abstract concept, care forms structural foundation for many nursing theories.14 Modern care theories and models emerged since Florence Nightingale: theory, philosophy, ethics, and ethnography of nursing care in various environments were studied. Common ideologies assert that care is a basic central concept which distinguishes nursing from other areas of health. A nurse is able to discover the patients’ needs and limitations, while providing care.15
It is difficult to define care; however, every definition must include two key parts to clarify care. The first part relates to the physical and technical aspects of care.13 Care giving varies depending on the patient’s conditions and needs: it may be mechanical or holistic.16 Accordingly, Gaut has mentioned three necessary conditions for a care measurement: a) related knowledge about the clients and their care needs, b) application of necessary measures and c) evaluation of measures to be beneficial for the patients and achieve his comfort.17 Care for a burn patient needs the collaboration of a multidisciplinary team. The nurse plays a strategic role in such a situation, as the nurses are in constant contact with the patients and their families.7 Thus, care, as one of the complicated theoretical aspects of nursing, is a multidimensional phenomenon.18 According to Sheini-Jaberi et al, there are three aspects in meeting the needs of burn patients and providing them with multidimensional care by the nurses: physical care for the burn patients, psychological care for them, and social protection of patients with burn injuries.19
The final purpose of nursing is to provide care. This care plays a crucial role in preventing patients’ deaths, necessitating the nurses to constantly look for opportunities to improve the quality of care. Various factors influence nursing in burn injuries. Moreover, both patients and the nurses have their own viewpoints about care in burn injuries, thus affecting the nurses’ function.
There are differences in understanding the care needs among different cultures and researchers. As a result, it is important to understand and analyze the past experience and the patients’ perception about physical care. This can help enhance the quality of care.
Considering the variety of physical care needs in patients with burns more than 25%, the current qualitative study has been done to explore the comprehensive care needs of burn injuries Physical domain. The results can provide a better understanding of patients, their expectations and needs.
Methods
Study design
The current qualitative study applies the conventional content analysis method. Since the researcher aims at this study explaining the needs of patients with burns more than 25%, and their basic aspects, she has chosen the qualitative approach using the content analysis method Elo and Kyngas.20 In this method, the goal is to provide deeper knowledge and perception about the subject of the study. Content analysis allows the researcher to methodically study a huge amount of data.
A qualitative research environment is a physical location where the subjects under study live and their experiences take place. Therefore, Ahvaz’s Taleghani Burn Hospital was selected as the research environment. Data collection happened from January to October 2018. This study was approved by Ahvaz Jundishapur University of Medical Sciences ethics committee with code IR.AJUMS.REC.1396.877, that all participants provided written informed consent, and that it was conducted in accordance with the Declaration of Helsinki.
Data collection and analysis
Both the care giver and the care taker were focused on as they are key factors in care. The selection of participants was determined using a purposeful sampling method. Participants include the hospitalized patients with burns more than 25%, nurses of the burn center, physicians and physiotherapists. Through purposive sampling, 14 patients with burns more than 25%, 3 nurses of the burn center, a physiotherapist, a psychologist, and a physician were interviewed. At the beginning, the interview, the purpose of the research, the interview method and the privacy and confidentiality of data were explained to the participant. After obtaining informed consent from the participants, in-depth, unstructured interviews with open questions were carried out in a calm environment. The interviews lasted between 30 and 90 mins. The main criteria for the length of the interview were tolerance, information, willingness, and the agreement of the participants. All interviews were recorded with audiotape and transcribed verbatim. Each transcript underwent several intuitively and precise readings. Codes derived from the data were systematically applied to words and passages in the text. Two researchers independently coded the first 2 transcripts. Independent coding results were compared and a coding structure was developed that was applied to all transcripts. Similarities in the codes were sorted into categories; the underlying meaning of the categories was then formulated into a theme; themes from all interviews were compared and then reviewed before final themes were established and agreed upon. The researcher also allowed the participants to leave the interview if they wished.
Credibility of the study
To certify the credibility and integrity of the data, Guba and Lincoln’s criterion was applied.21 The analysis and data collection were done concurrently. After analyzing the data, participants were asked to check the accuracy of the results (Member check). To ensure the accuracy of the codes, the interviews were presented to two of the faculty members for their opinion (External check). In case of ambiguity or need for deeper investigations, the interview was repeated. The researcher devoted sufficient time to collect the data, entangling with them over a long time, thereby increasing the depth and breadth of the information.
Results
Fourteen hospitalized patients with burns more than 25%, 3 nurses of the burn center, a physiotherapist, a psychologist, and a physician of the center participated in this study. Details of the participants were as follows:
- Age: 22–86 years old,
- Gender: 11 men, 9 women;
- Marital status: 16 married and 4 single;
- Education: doctoral degree 1 person, bachelor’s degree 9 persons, associate degree 3 persons, high school diploma 2 persons, below high school diploma 3 persons, uneducated 2 persons;
- Occupation: physician 1 person, psychologist 1 person, physiotherapist 1 person, nurses 3 persons, housewives 3 persons, retired 2 persons, staffers 8 persons, self-employed 1 person (Table 1)
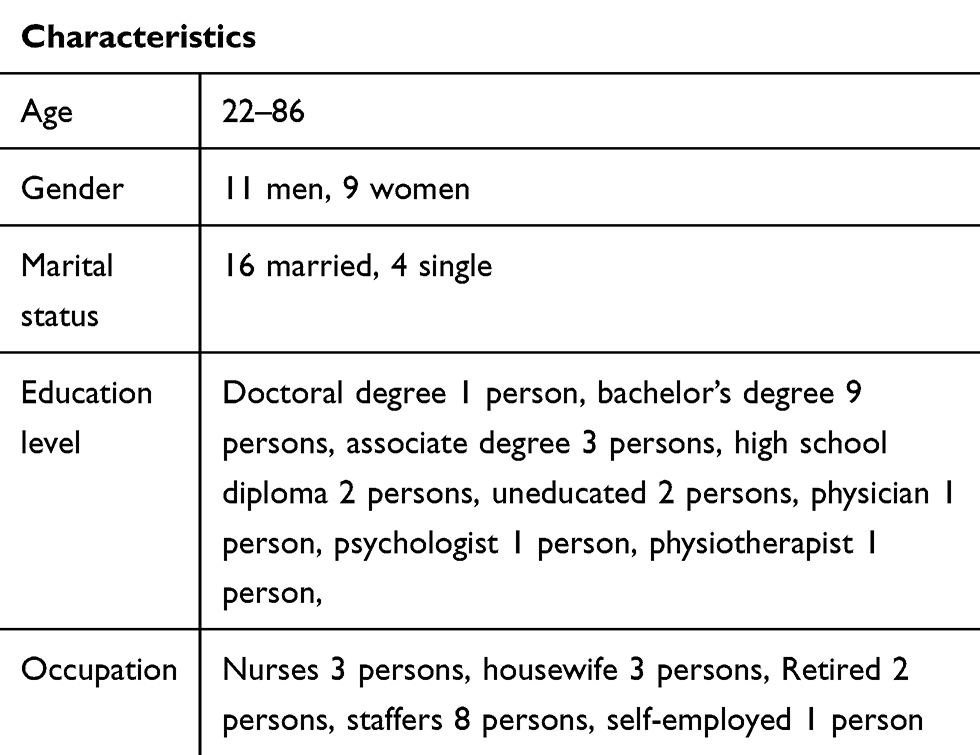 |
Table 1 Demographic characteristics of the participants |
932 primary codes were obtained from the interviews. These codes were classified into 7 main categories and one theme through the data analysis.
Theme
Comprehensive care needs from a physical domain
This theme clarifies the need for establishing the optimal physiotherapy conditions, the necessity of comprehensive physical evaluation of the patient, the necessity of monitoring and coordination in care giving, suitable diet for burn injuries, the need for pharmacotherapy, and the need for pain and infection control.
1-1) The need for establishing optimal physiotherapy conditions means prevention of joint problems, coordination of the physiotherapy with physical conditions of the patient, the need for mental preparation of the patient and his cooperation in physiotherapy, the need for teaching the patient and the persons accompanying him/her about joint movements, the need for on-time physiotherapy services, the need for proper physiotherapy equipment in the center. In this regard, participant No. 3 said:
The physiotherapist here will be blessed; he insists the patient should walk. I had a car accident and my hand burnt severely. It was badly swollen. He forces me to move my wrist. Even he forces my roommate to walk. He couldn’t walk first, but he had him walk for 10 minutes. He really spreads positive energy.
We have expectations; for example, we need at least 10–20 pieces of hand, foot and body stretch exercise equipment in the yard for us; but there is not. We are burn patients with burnt and buckled bodies that now look like a piece of plastic. (Participant No. 2)
The key factor in preventing the deformity, joint contracture, and lumpy skin is physiotherapy. The doctor prescribes this for the patients and the physiotherapist does the job for them. Also, the nurses move the joints while washing the area and … They teach this to the patients too. The physiotherapist does her job but the facilities and tools are not adequate. (Nurse participant No. 1)
2-1) The necessity of comprehensive evaluation of the patient means considering the underlying diseases, the necessity of examining the wound, the primary evaluation of the patient’s physical conditions, and the necessity of caring for the injury in accordance with the nature of the injury. In this regard, nurse participant No. 1 said:
Usually, these patients are first admitted to the emergency department. The first thing to do is to insert a foley catheter and nasogastric tube for them. Then, fluid therapy starts. They enter our ward after necessary arrangements. We weigh them and precisely measure the size of the surface of the injury and continue with the fluid therapy, he sometimes complains of thirst … we should make sure that he receives enough fluid.
When I was hospitalized in the burn center, I was worried what would happen. Thanks God, there were nice doctors and nurses in the center. From the start, they told me not to worry, and said they would do whatever they could. They immediately gave me an IV solution, cleaned the burnt areas, dressed the wound, injected painkiller medication. (Participant No. 7)
When I told the nurses that I had diabetes, they constantly checked my wound to avoid infection. (Participant No. 11)
3-1) The necessity of monitoring and coordination in care means the necessity of control over the nursing care and the coordination of the team in care. In this regard, participant No. 4 said:
I may not be in a position to spread my words and transfer my feelings to the authorities, but today is the digital age; you can control everything with the cameras. Check and see if what I say has happened in the burn department or the surgery room or not…?
It’s a good idea for the supervisor, who comes every morning, to the check if everything was OK the night before, and to ask the patients if they were well taken care of, didn’t have any problem, and … (Participant No. 8)
4-1) Nutrition consistent with burn means consultation and control based on the dietary needs of the patient and the necessity of proper nutrition both qualitatively and quantitatively. In this regard nurse, participant No. 3 said:
The nurses also said to me, maybe her teeth had problems, you could grind the pistachios. Prepare ground pistachio and give it to her, because we want the potassium level to remain high. Give her figs, raisins, bananas, because a burn patient suffers from low potassium.
5-1) The need for pharmacotherapy means the necessity of administering the medication at particular times and the necessity of considering the side effects. In this regard, nurse participant No. 4 said
If the patient’s fever increases and is not controllable, they will schedule consultation with an infectious disease specialist. Usually, patients with fever receive antibiotics. So, the impacts of antibiotics and their side effects are also checked.
The nurses should watch carefully when to give us the antibiotics so we don’t get miserable. (Participant No. 6)
6-1) The need to control pain means the necessity of relieving pain and applying music therapy to soothe the pain in burn patients. In this regard, participant No. 8 said
Because burn is painful and terrifying in nature, most of the sufferers are scared. A patient with burns needs pain killers and pain relief medicines over and over to soothe his pain.
I like that they play music while changing my wound dressing; it calms me down. (Participant No. 10)
7-1) Infection control means preventing the burn patient from developing infection and also means overseeing the infection control methods. In this, participant No. 9 said:
Everyone says “be careful, so-and-so died of infection in the center, because infection spreads all over the body.”
After the nurse assistant changed the wet blanket of this patient, she washed her hands before going to the other patient in order not to spread the infection to other patients and get them wretched. I liked these practices. (Participant No. 12)
Examples of extracting subcategories, main categories and theme are shown in Table 2.
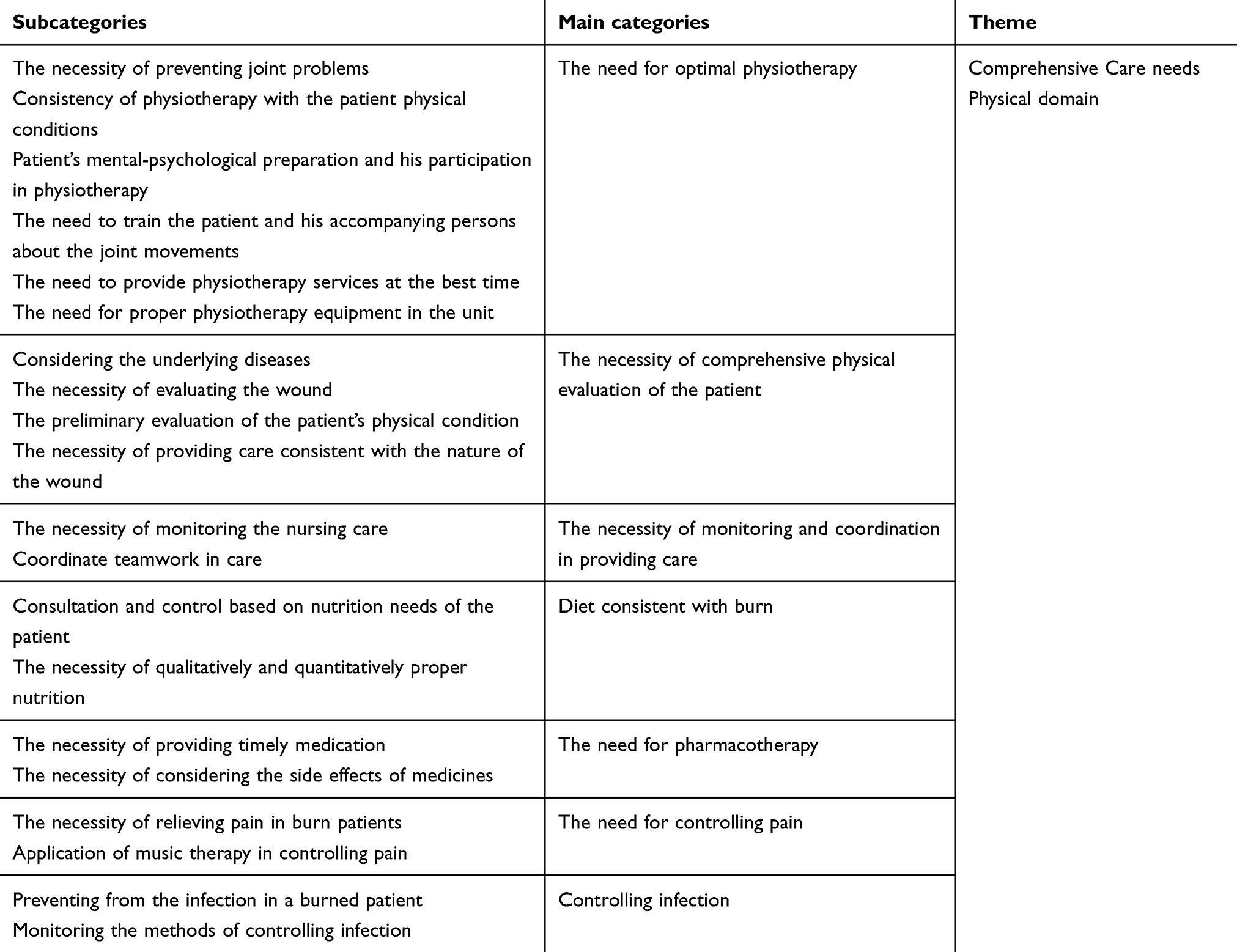 |
Table 2 Subcategories, categories, and theme |
Discussion
The purpose of this study was to investigate all physical care needs of burn patients. The data were obtained from the qualitative analysis of in-depth interviews with hospitalized burn patients, nurses, physiotherapists, and doctors in Ahvaz’s Taleghani Burn Hospital. The extracted data contained a comprehensive set of physical care needs.
According to the interviews, the need for establishing high-quality physiotherapy services has been one of the main categories, which includes a number of subcategories as follows: the necessity of prevention of joint problems, making physiotherapy consistent with the patient’s physical conditions, the need for mental-psychological preparation, and patient’s cooperation for performing the physiotherapy, instructing the patient and his accompanying person(s) about joint movements, the need for timely physiotherapy services and proper physiotherapy equipment in the ward. In their study, Grisbrook et al showed that instructing burn patients in body exercises had a positive impact on their physical well-being and quality of life.22 The findings of that study indicated that burn patients face deformations in parts of the body after passing the acute phase of the burn. These deformations could adversely impact the normal function of different body parts such as arms and legs. Therefore, Physiotherapy and exercise are of particular importance for the rehabilitation of burn patients.
The main theme contained another category called the necessity of comprehensive evaluation of the patient’s physical needs. It includes subcategories of attention to underlying diseases, necessity of examining the injury, and preliminary evaluation of the patient’s physical conditions. Preliminary actions for burn patients are similar to those for trauma patients. These are, respectively, 1) checking the patient from head to toe and precise determination of injuries, 2) acquiring information on past deceases, use of medication, allergy, and how the incident took place, 3) taking the IV line, in which case the Ringer’s lactate solution should be connected, 4) covering the burn area with a clean piece of cloth, 5) prescribing pain relief medications, and 6) covering the burn patient with a clean blanket to avoid losing body heat.17 According to the study conducted by Sheini Jaberi et al, some of the main responsibilities of the burn nurses are as follows: the need for the participants’ holistic approach to the patients, comprehensive evaluation and assessment, and providing care consistent with the results of the evaluation and the patients’ requests.19 Based on the results, a preliminary comprehensive evaluation and constant check-ups of the burn patients are their main needs.
Another subcategory is the necessity of appropriate care suitable for the nature of the burn injuries. According to standards, the treatment team including burn surgeons, nurses, and physiotherapists make a collaborative effort in order to speed up healing of the burn injuries. This is also reflected in the results of the qualitative study on the injuries and types of care conducted by Fagerdahl.23 In this study, covering the burn wounds is one of the problems that acute burn patients are faced with; after assessing the depth and breadth of the burns, the wound should be properly cleaned and debrided. Then, it should be dressed with proper covers. Participants expressed a great deal of concern for their wounds.
The necessity of control and coordination in care was another main category extracted. The subcategories included the necessity of overseeing nursing care and the team coordination in care. One of the responsibilities of a nurse is to provide lawful care, i.e., to observe the law in care so that care is provided with minimal harm to the patient. Here, the question is whether these responsibilities are fulfilled properly with standard methods. This is a legal responsibility of nurses. By accepting this responsibility, it must be ensured that the job meets the standards and is done appropriately in order to provide quality care. Considering the fact that most of the care is provided by nurses, they play a crucial role in improving the quality of services.24 In the line with this study Rafiee’s study, entitled “the theory of nursing care for burn patients,” the patients and the personnel stated that the care at the evening and night times had a lower quality. According to the participants, the causes included shortage of the personnel, heavy workload, and supervisory problems resulting from the absence of the head nurse and wasting of the supervisor’s time due to involvement in care affairs (because such issues reduced supervisor’s availability for a good supervision). In addition, nurses believe that the managers do not care about the quality of the job; their only goal is to finish the job and gain revenue.25 Moreover, Zagheri Tafreshi et al conducted another qualitative study to identify the factors related to applying nursing care models. One of the extracted themes was effective to control over the nurses’ performance and, on a larger scale, over the strategic policies of the health care system.26 Hauser also showed in his study that organizing nursing care, leadership skills, and the ability to balance various needs is of great importance; in addition, there is a meaningful relation between effective leadership and patients’ experience.27 Karimollahi et al conducted a qualitative study on patients with open-heart surgery in Qaem Shahr’s Social Security Hospital and Sari’s Fatemah Zahra (PBUH) Hospital. The participants in that study mentioned the mastery of nurses in providing care and teamwork as a verification of their professionalism, and love in nursing care as an art.28 Also, Greenfield states in his study that complexities and interactions of different body systems in the burn patient require a nurse with strong background knowledge in different disorders, different body parts, special care techniques, diagnostic studies, and psychological-social and rehabilitation skills. This is because a nurse working in a burn center oversees patient’s overall care and coordinates with other disciplines such as occupational therapy, physiotherapy, social services, nutritional services, and pharmaceutics. A nurse is also an expert in caring for the wounds, infection prevention, and pain control.29
Based on the findings another main category was nutrition suitable for the burn conditions. It includes subcategories of counseling and overseeing based on the patient’s nutritional needs and the necessity of good nutrition both qualitatively and quantitatively. Estimating the nutritional needs of burn patients is one of the most essential treatment processes.
In the intensive care unit, patients with different illnesses in varying degrees are hospitalized. The burn unit is also considered as an intensive care unit. Shayesteh quotes from Farahani that the rate of malnutrition in these units are higher than other units. The metabolism in the burn patients is therefore increased. If sufficient calories and proteins are not received in a timely manner, catabolism will increase and fat resources and muscle mass will decrease.30 Thus, the patient’s nutrition is immensely important, urging the presence of nutrition counselors in burn units. Accordingly, Endevelt also mentioned in his study that continuity of the nutritional counseling depends on many aspects of the patient’s experience with the nutrition specialist in the first session. Psychological, physical, cultural, and normative obstacles may prevent the patient from behavioral changes, especially nutritional ones.31 In addition, the current qualitative study shows that another common problem a burn patient suffers from is nutritional and metabolic disorders. Burn is a multidimensional disorder that involves various body systems. In order to change patients’ eating patterns, dietitians must adopt a more therapeutic approach and relate to patients’ cultural needs and desires to achieve sustainable results. Thus, from metabolic and nutritional perspectives, consultation with a nutrition specialist seems necessary.
In this qualitative study, the need for pharmacotherapy includes the following subcategories: the necessity of giving the medication to the patient on time and the necessity of the paying attention to the side effects. In their study, Rojas et al state that severe burn damages, stress, and trauma cause an unnatural response that prevents recovery if left untreated. In the last two decades, anabolic, beta-adrenergic receptor antagonists, and anti-hyperglycemia agents have been used successfully against after-burn diseases including catabolism, metabolic reaction of catecholamine and insulin resistance.32 Hamblin et al noted that pharmacotherapy has been used for treating various pathophysiological effects of burn damages. In addition, advances in stem cells and tissue reconstruction will enhance recovery and prevent disability during life. Moreover, pharmaceutical research aimed at preventing various effects of burn is continuously advancing.33 Participants in this qualitative study also called for proper treatment at the right time.
The need for pain control was one of the main categories. It included the need for pain relief in burn patients and music therapy for pain control. It is worth noting that burn comes with severe pain, and pain control is now considered an important part of care. The American Pain Society uses the term “Pain, the fifth vital sign” to emphasize its importance. Also, Maslow believes that treating pain is the first priority in satisfying physiological needs of human. International Council of Nurses also mentions relief of patients’ pain and discomfort as one of the five important responsibilities of nursing.34 Boluda et al stated in their studies that burn patients experience pain in different situations, especially when replacing the bandage.35 The studies of Park et al on burn patients showed that the use of breathing techniques can serve as a simple, cheap method for reducing the pain resulting from the dressing replacement.36 The study of Li et al also shows the impact of music on the control of burn pains.37 Pain disrupts physical function of the burn patient. It is also an important threat to the process of healing the burn injuries. The reason is that pain can potentially impact the healing process through psychological and physiological factors. In the present study, according to the burn patients, pain control should be an important objective of care. Therefore, nurses should focus on relieving and preventing pain and the stress resulting from it.
Control of infections is the last main category that includes preventing infection in the burn patient and monitoring infection control methods. Due to the lack of the defensive barrier of the skin, weakness of the immune systems as a result of the burn, long hospital stay, and a series of invasive treatments, burn patients are at the risk of developing hospital-acquired infections. For this reason, most burn-related deaths are due to infection that causes sepsis,38 Dries et al acknowledge the importance of infection control in the burn section of hospitals.39 Therefore, isolation and maintaining sterile conditions are necessary in the hospital, especially the burn sections, where the patients have lost their first line of defense (skin). In this study, the participating patients also emphasized very much control of their burn infections.
Conclusion
This study showed that after the acute phase, the burn patients need physiotherapy, rehabilitation, a comprehensive preliminary assessment and monitoring of the wounds bandages and dressing, dietitian counseling for nutrition and metabolic needs, pain relief and control of wound infections. According to the findings, hospitalized burn patients have various physical needs, each requiring a particular type of care. In the present study, the care needs have been determined based on interviews with patients and the treatment team in order to understand their actual needs. This can help speed up the treatment and shorten the length of hospitalization significantly. Therefore, using these findings, the patients can receive quality care based on their needs. Also, in addition to the study of care needs, it is necessary to study the factors related to these needs in our hospital environments. This would help nurses with providing care to the patients and the nursing management teams with organizing resources and providing supportive solutions with an open view. It should be noted that physical care is not separate from overall care; according to the patients, a satisfactory care is the one that considers also mental and physiological aspects in addition to the physical aspect.
Acknowledgments
The present study is part of a PhD dissertation in nursing by Sima Mohammadhossini S; Designing and Psychometrics of a Care Needs Assessment Tool in Hospitalized Patient With second - degree Burn; Ahvas: Ahvaz Jondishapour University; 2019. The dissertation was passed and funded by Ahvaz Jondishapour University. The authors are grateful to the burn patients, nurses, and others who helped in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Watson J. Caring theory as an ethical guide to administrative and clinical practices. JONA’S Healthcare Law Ethics Regul. 2006;8(3):87–93.
2. McCance TV, McKenna HP, Boore JR. Caring: dealing with a difficult concept. Int J Nurs Stud. 1997;34(4):241–248.
3. Husted JH, Husted GL. Ethical Decision Making in Nursing and Health Care: The Symphonological Approach. New York: Springer Publishing Company; 2008.
4. Pajnkihar M. Is caring a lost art in nursing? Int J Nurs Stud. 2008;45(5):807. doi:10.1016/j.ijnurstu.2007.09.013
5. Cheng W, Wang S, Shen C, Zhao D, Li D, Shang Y. Epidemiology of hospitalized burn patients in China: a systematic review. Burns Open. 2018;2(1):8–16. doi:10.1016/j.burnso.2017.10.003
6. Abouie A, Salamati P, Hafezi-Nejad N, et al. Incidence and cost of non-fatal burns in Iran: a nationwide population-based study. Int J Inj Contr Saf Promot. 2018;25(1):23–30. doi:10.1080/17457300.2017.1310739
7. Silva IFX, Moulin LL, de Oliveira SP, et al. Challenges faced by the nursing team in the care of burned victim: literature review. Int Arch Med. 2016;9.
8. Hinkle JL, Cheever KH. Study Guide for Brunner & Suddarth’s Textbook of Medical-surgical Nursing. Lippincott Williams & Wilkins; 2013.
9. McLatchie G, Borley N, Chikwe J. Oxford Handbook of Clinical Surgery. OUP Oxford; 2013.
10. Sheridan RL. Burns. Crit Care Med. 2002;30:500–514. doi:10.1097/00003246-200211001-00015
11. Soltani M, Hejazi SM, Noorian A, Zendedel A, Ashkanifar F. The Effect of Aerobic Training on the Improvement of Expanded Disability Status Scale (EDSS) in Multiple Sclerosis Patients. JMS. 2009;1(5):15–20.
12. Armstrong LE, Winant DM, Swasey PR, Seidle ME, Carter AL, Gehlsen G. Using isokinetic dynamometry to test ambulatory patients with multiple sclerosis. Phys Ther. 1983;63(8):1274–1279. doi:10.1093/ptj/63.8.1274
13. Soltani M, Hejazi S, Nornematolahi S. The Effect of Aquatic Aerobic Training on the Quality of Life on Multiple Sclerosis Patients. Journal of Medical Sciences of Islamic Azad University of Mashhad. 2010; 5(4):267–274.
14. Tomey AM, Alligood M. Nursing Theory: Utilization & Application. St Louis: Mosby Co.; 2006.
15. Bolderston A, Lewis D, Chai MJ. The concept of caring: perceptions of radiation therapists. Radiography. 2010;16(3):198–208. doi:10.1016/j.radi.2010.03.006
16. Finch LP. Development of a substantive theory of nurse caring. Int J Human Caring. 2008;12(1):25–32. doi:10.20467/1091-5710.12.1.25
17. Finfgeld‐Connett D. Meta‐synthesis of caring in nursing. J Clin Nurs. 2008;17(2):196–204. doi:10.1111/j.1365-2702.2006.01824.x
18. Lee-Hsieh J, Kuo C-L, Tseng H-F, Turton MA. Development of an instrument to measure caring behaviors in nursing students in Taiwan. Int J Nurs Stud. 2005;42(5):579–588. doi:10.1016/j.ijnurstu.2004.09.018
19. Sheini-Jaberi P, Zarea K, Moradi M. Holistic care as a response to the needs of burn patients: a qualitative content analysis. J Clin Nurs Midwifery. 2014;4(3):17–27.
20. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
21. Guba EG, Lincoln YS. Competing paradigms in qualitative research. Handbook Qual Res. 1994;2(163–194):105.
22. Grisbrook T, Reid S, Edgar D, Wallman K, Wood F, Elliott C. Exercise training to improve health related quality of life in long term survivors of major burn injury: a matched controlled study. Burns. 2012;38(8):1165–1173. doi:10.1016/j.burns.2012.03.007
23. Fagerdahl A-M, Boström L, Ottosson C, Ulfvarson J. Patients’ experience of advanced wound treatment-a qualitative study. Wounds. 2013;25(8):205–211.
24. Sharifi H. The workload of nursing: a concept analysis using walker and avant approach. J Clin Nurs Midwifery. 2017;6(2):37–47.
25. Rafiee F, Haghdoost Oskouie S, Nikravesh M. Developing Theory for Nursing Care of Burn Patients. Tehran, Iran: Iran University of Medical Sciences; 2005.
26. Zagheri Tafreshi M, Rassouli M, Pazargadi M, Yaghmaie F, Barbaz A. Exploring relevant components to apply nursing care models. J Hosp. 2012;11(3):9–16.
27. Houser J. A model for evaluating the context of nursing care delivery. J Nurs Administration. 2003;33(1):39–47.
28. Karimollahi M, Mousavi A, Jouybari L, Sanagoo A, Tazakori Z. The concept of nursing art in the experiences of patients with open heart surgery: a phenomenological study. J Health Care. 2018;20(1):82–95. doi:10.29252/jhc.20.1.82
29. Greenfield E. The pivotal role of nursing personnel in burn care. Indian J Plast Surg. 2010;43(Suppl):S94. doi:10.4103/0970-0358.70728
30. Shayesteh F, Poudineh S, Pouryazdanpanah-Kermani M, Sadat Ayoudi S, Norouzy A. Assessment of nutritional intake in intensive care unit patients of Ghaem hospital. Med J Mashhad Univ Med Sci. 2015;58(4):217–224.
31. Endevelt R, Gesser-Edelsburg A. A qualitative study of adherence to nutritional treatment: perspectives of patients and dietitians. Patient Prefer Adherence. 2014;8:147. doi:10.2147/PPA
32. Rojas YFC, Radhakrishnan RS, Herndon DN. Burns: an update on current pharmacotherapy. Expert Opin Pharmacother. 2012;13(17):2485–2494. doi:10.1517/14656566.2012.738195
33. Hamblin MR. Novel pharmacotherapy for burn wounds: what are the advancements. Expert Opin Pharmacother. 2019;20(3):305–321. doi:10.1080/14656566.2018.1551880
34. Esfahlan AJ, Lotfi M, Zamanzadeh V, Babapuor J. Burn pain and patients’ responses. Burns. 2010;36(7):1129–1133. doi:10.1016/j.burns.2010.02.007
35. Boluda MP, Asencio JM, Vela AC, et al. The dynamic experience of pain in burn patients: a phenomenological study. Burns. 2016;42(5):1097–1104. doi:10.1016/j.burns.2016.03.008
36. Park E, Oh H, Kim T. The effects of relaxation breathing on procedural pain and anxiety during burn care. Burns. 2013;39(6):1101–1106. doi:10.1016/j.burns.2013.01.006
37. Li J, Zhou L, Wang Y. The effects of music intervention on burn patients during treatment procedures: a systematic review and meta-analysis of randomized controlled trials. BMC Complement Altern Med. 2017;17(1):158. doi:10.1186/s12906-017-1669-4
38. Saaiq M, Ahmad S, Zaib MS. Burn wound infections and antibiotic susceptibility patterns at Pakistan Institute of Medical Sciences, Islamabad, Pakistan. World J Plastic Surg. 2015;4(1):9.
39. Dries DJ, Marini JJ. Management of critical burn injuries: recent developments. Korean J Crit Care Med. 2017;32(1):9–21. doi:10.4266/kjccm.2016.00969
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.