Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Comprehensive Multimodal Prehabilitation for Lung Cancer: A Systematic Review of Randomized Controlled Trials
Authors Mania K, Pieczynska A, Hojan K
Received 26 August 2025
Accepted for publication 17 November 2025
Published 16 December 2025 Volume 2025:21 Pages 1735—1745
DOI https://doi.org/10.2147/TCRM.S563218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Krystian Mania,1 Anna Pieczynska,2 Katarzyna Hojan2– 4
1Greater Poland Provincial Hospital in Poznan, Department of Otorhinolaryngology, Poznan, Poland; 2Poznan University of Medical Sciences, Department of Occupational Therapy, Poznan, Poland; 3Greater Poland Cancer Centre, Department of Rehabilitation, Poznan, Poland; 4Greater Poland Provincial Hospital in Poznan, Neurorehabilitation Ward, Poznan, Poland
Correspondence: Anna Pieczynska, Department of Occupational Therapy, Poznan University of Medical Sciences, Poznan, 60-781, Poland, Email [email protected]
Introduction: Surgical resection is a cornerstone of curative treatment for early-stage lung cancer. Multimodal prehabilitation, a comprehensive, patient-centered program integrating physical exercise, nutritional status, and psychological support, has emerged as a promising approach to enhance patients’ physiological and psychological resilience prior to surgery. While multimodal prehabilitation is valuable for optimizing patients’ tolerance of oncological treatment, there is a scarcity of studies incorporating multimodal interventions, likely due to the absence of clear guidelines for lung cancer patients. This systematic review aimed to assess the comprehensiveness and effectiveness of prehabilitation activities for lung cancer patients undergoing thoracic surgery.
Evidence Acquisition: A systematic literature search was conducted according to PRISMA guidelines. The search was performed in PubMed, Google Scholar, PEDro, and Cochrane Library, with additional publications identified from reference lists. The search was completed on February 27, 2024. Studies published between 2019 and 2024 were included to capture the most recent evidence. The study was registered in PROSPERO (registration number CRD42024499622).
Evidence Synthesis: Out of 1233 identified studies, 10 randomized controlled trials were included. Prehabilitation programs varied in duration and setting. Only three studies (Liu et al, 2020; Yao et al, 2022; Ferreira et al, 2021) employed a comprehensive multimodal approach integrating physical exercise, psychological care, and nutrition interventions. Prehabilitation was associated with improved exercise capacity (eg, increased 6MWT distance), reduced postoperative complications, and potential benefits for quality of life and psychological well-being. However, the impact on length of stay and cognitive function remains unclear.
Conclusion: This review highlights a significant gap in the implementation of comprehensive multimodal prehabilitation for lung cancer patients. While physical exercise is widely adopted, psychological and nutritional components are often overlooked. Further research is needed to establish clear guidelines and elucidate the full benefits of a comprehensive multimodal prehabilitation approach, particularly regarding its impact on mental health, quality of life, and long-term outcomes in lung cancer patients.
Keywords: oncology, prehabilitation, multimodal rehabilitation, cancer care, psycho-oncology, physical exercise, nutrition, surgical outcomes
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide, with the highest mortality rates observed in both men and women.1 Surgical resection remains a cornerstone of curative treatment for early-stage lung cancer.2 Optimizing patient resilience to manage the challenges of oncological treatment, including surgery, is crucial for improving outcomes and reducing healthcare costs. 3
Multimodal prehabilitation has emerged as an intervention aimed at enhancing patients’ physiological and psychological resilience prior to surgery. We define comprehensive prehabilitation as a short-term, patient-centred program focuses on optimizing physical function, nutritional status, and psychological well-being. 4 By addressing modifiable behavioural and lifestyle risk factors in the preoperative period, prehabilitation bolsters patients’ physiological reserve, thereby augmenting their resilience to the stressors associated with surgery. Prehabilitation equips individuals to better tolerate the physiological stress of surgery and to minimize or overcome potential complications. 5,6
Preoperative exercise training is known to increase physical capacity and significantly reduce the risk of postoperative pulmonary complications in individuals with lung cancer compared to no exercise group. 7,9 Cancer prehabilitation, a comprehensive process spanning from diagnosis to the start of acute treatment, should equally address both physical and psychological well-being. This involves assessments and targeted interventions to improve overall health and reduce impairments. Preparing patients both physically and psychologically is crucial for optimal outcomes in cancer treatment. 10
Patients with cancer encounter a multitude of physical, social, psychological, and emotional challenges, including anxiety and depression, following diagnosis and throughout the course of treatment. 11 A wide array of psychological interventions has been proposed to alleviate distress in cancer patients. Traditionally, these interventions have been administered post-treatment. However, recognizing the significant distress experienced by cancer patients during the perioperative period, accumulating evidence suggests that pre-surgical interventions may positively influence postoperative recovery. 12,14
Malnutrition is strongly associated with adverse outcomes in surgical patients. Major surgical stress induces catabolism, the extent of which correlates with both the magnitude of surgical stress and patient outcomes. Perioperative nutritional supplementation has been shown to mitigate postoperative complications, both infectious and non-infectious, and reduce length of stay in patients undergoing surgery. 15,16
Despite the compelling rationale for comprehensive care, there are currently no established guidelines for the optimal preoperative intervention in lung cancer patients, unlike in lung transplantation.17 Furthermore, there is a scarcity of studies incorporating truly multimodal interventions. This gap may stem from factors such as the clinical methodological difficulty in implementing complex interventions, research methodology limitations in designing and funding such trials, or a lack of widespread awareness or adherence to existing oncology or perioperative guidelines, which typically advocate for nutritional screening and intervention. This highlights a key challenge in translational research for this patient population.
The aim of the review was to assess the comprehensiveness of activities undertaken as part of prehabilitation for lung cancer patients and evaluate their effectiveness in recent Randomized Controlled Trials (RCTs).
Evidence Acquisition
We performed a systematic literature search according to the Preferred Reporting Items for Systematic Reviews and MetaAnalysis (PRISMA) recommendations.18 This study did not require the approval of the bioethics committee. The study was registered in health and social care, welfare, public health, education, crime, justice, and international development, where there is a health-related outcome PROSPERO. The registration number of presented study is: CRD42024499622.
Search Strategy
To find relevant publications, the algorithm of keywords (“lung cancer”) AND (“surgery” OR “operation”) AND (“prehabilitation” OR “preoperative”) was used. The search was conducted in PubMed, Google Scholar, PEDro and Cochrane Library. Reference lists were also searched for additional publications. The search was performed simultaneously and independently by the two authors KM and AP. The searches were completed on February 27, 2024. The search terms were formulated using the PICO structure. Subjects (P) were adults (> 18years of age) with lung cancer. Intervention (I) included prehabilitation before oncological treatment. Comparisons (C) standard care (rehabilitation after surgery). Outcomes (O) included functional measure or evaluation.
Inclusion Criteria
- Randomized controlled trials published in English.
- Participants with confirmed lung cancer.
- Participants qualified for radical treatment.
- Studies incorporating a prehabilitation program.
- Studies published between 2019 and 2024. This timeframe was chosen to focus on the most recent advancements and practices in prehabilitation for lung cancer, reflecting contemporary clinical approaches and research methodologies.
- Participants aged 18–75 years.
Exclusion Criteria
- Studies involving different types of cancer.
Quality Assessment
The Quality Assessment Tool for Quantitative Studies (QATQS) was used to assess the methodological quality of the included studies. The evaluation was carried out by two authors, KM and AP, and any conflicts were resolved by the third author, KH. This tool evaluates eight areas: selection bias, study design, confounders, blinding, data collection methods, withdrawals and dropouts, intervention integrity, and analysis. In the case of one-time surveys, the withdrawals and dropouts section was rated as 1. Individual sections were rated as weak, moderate, or strong according to dictionary. 19 A study was classified as strong if no section was rated as weak; moderate if one section was weak; and weak if two or more sections were rated as weak. The results of the quality assessment are shown in Figure 1.
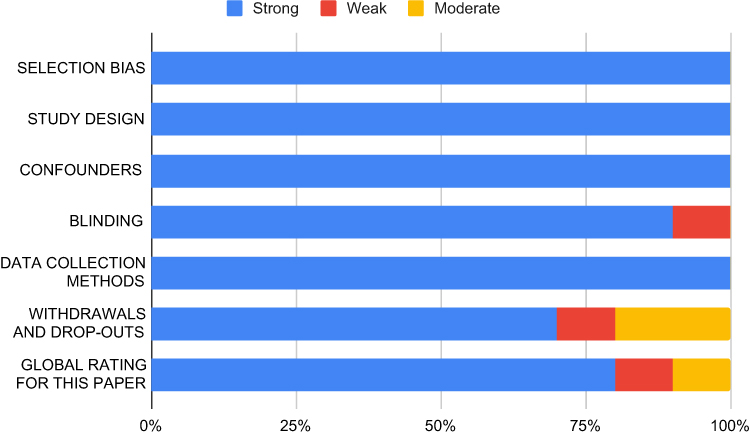 |
Figure 1 Risk of Bias Assessment. This figure presents the summary of the quality assessment for the studies included in the systematic review. The risk of bias was evaluated across several key domains, including Selection Bias, Study Design, Confounders, Blinding, Data Collection Methods, and Withdrawals and Drop-Outs. The bar graph format displays the percentage of studies rated as Strong, Moderate, or Weak for each domain, with a final overall quality rating provided for the included papers (Global Rating). This assessment helps to determine the reliability and internal validity of the evidence base. |
Results
Study Selection and Characteristics
After searching the databases and considering additional records, 1233 studies were identified. Ultimately, 10 studies were included in this review. 20,29 The flow diagram according to PRISMA guidelines is presented in Figure 2.
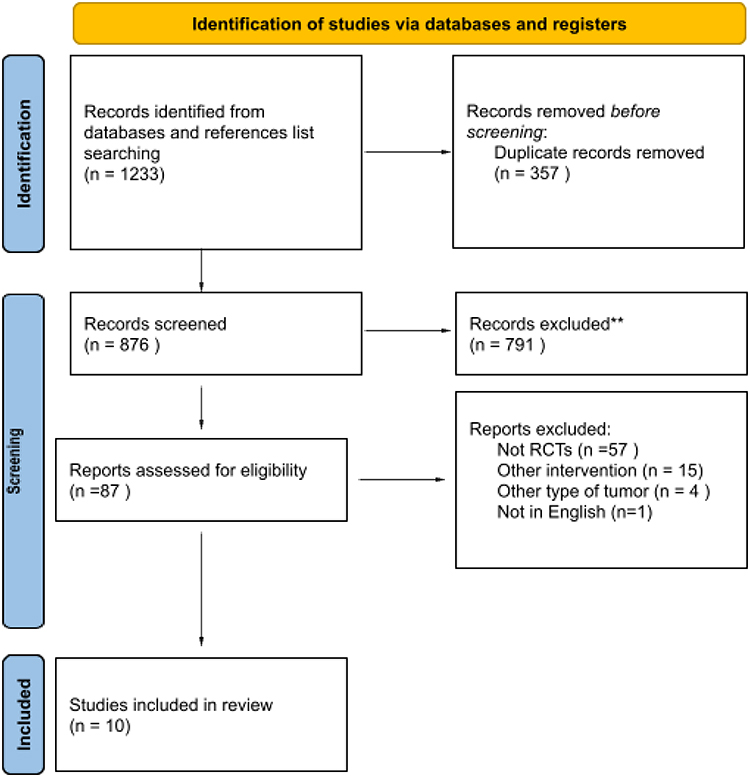 |
Figure 2 PRISMA 2020 Flow Diagram for the Study Selection Process. This flowchart illustrates the systematic identification, screening, and inclusion process for studies in the review, based on the PRISMA 2020 statement guidelines. The process began with Identification, yielding 1233 records from databases and reference list searching. Following the removal of 357 duplicate records, 876 records were screened. Of these, 791 were excluded, leaving 87 reports for full-text eligibility assessment. The Reports Excluded stage details the reasons for exclusion of the final 77 reports: not Randomized Controlled Trials (RCTs) (n = 57), other intervention types (n = 15), other tumor types (n = 4), and not in English (n = 1). This systematic process concluded with 10 studies included in the final review. |
Time and Frequency and Sitting of Prehabilitation
A variety of training regimens and durations of prehabilitation were implemented in the reviewed studies. The length of prehabilitation period was determined by the specific program in place. Among the studies, six reported a prehabilitation duration of 2–3 weeks, two studies prescribed 1 week, one study aligned prehabilitation with the waiting time (approximately 3–4 weeks), while one study did not specify a timeframe (Table 1). Notably, despite the varying durations of prehabilitation, there was no observed delay in the execution of surgical procedures.
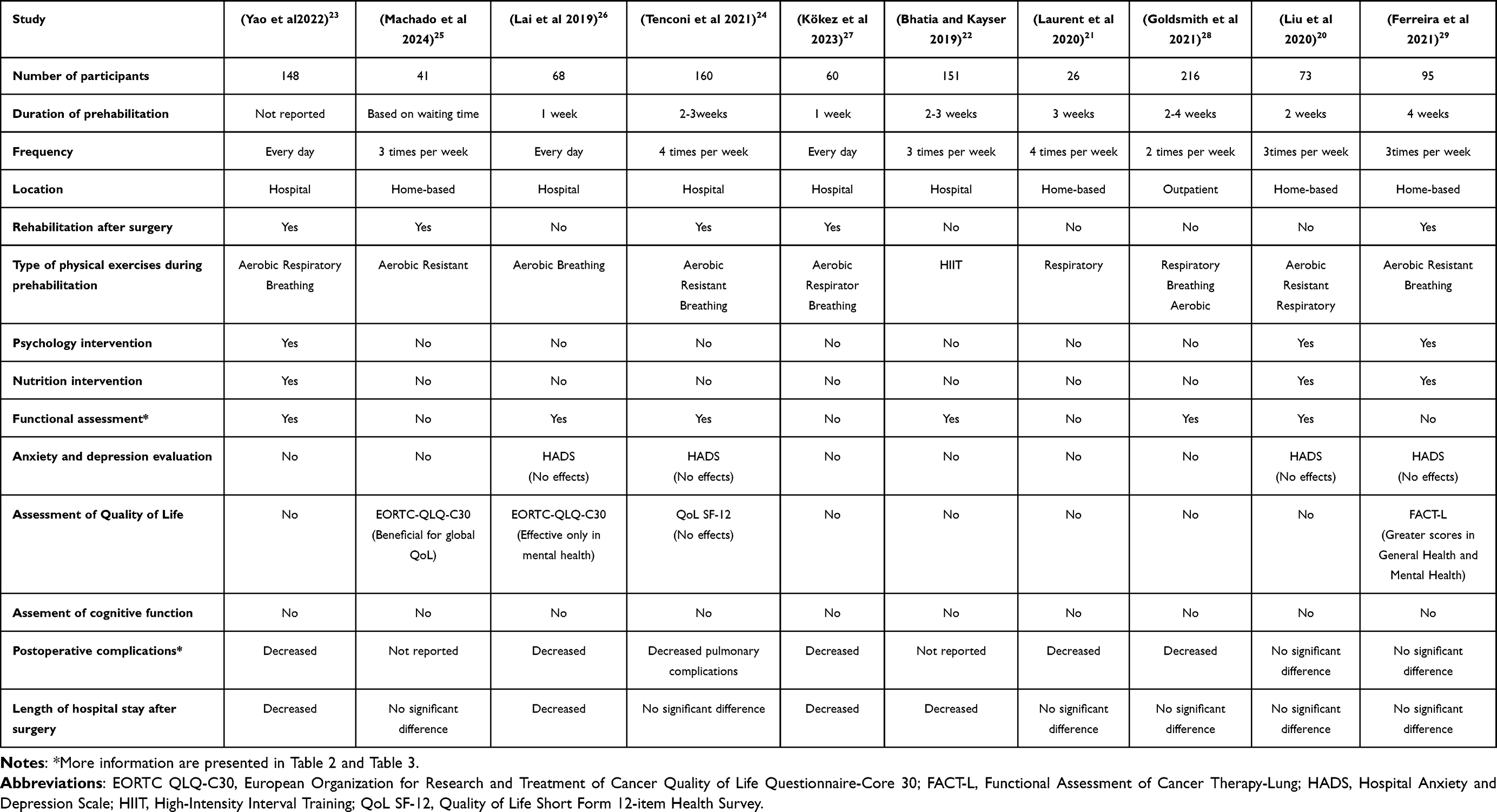 |
Table 1 Characteristics of Included Studies |
Studies employed various settings for prehabilitation programs, including hospital wards, home-based training, or combined home and outpatient rehabilitation (Table 1).
Multimodal Preoperative Care
A critical finding is the limited adoption of a truly comprehensive approach. Only three of the ten included studies (Liu et al, 2020; Yao et al, 2022; Ferreira et al, 2021) utilized a comprehensive multimodal prehabilitation approach, integrating psychological care and nutrition interventions with physical exercise. The remaining studies primarily focused on enhancing physical capacity. This highlights a significant implementation gap (Table 1).
Type of Physical Exercise Training
The most common form of physical prehabilitation involved breathing exercises combined with other physical activities. Breathing training often included diaphragmatic breathing, segmental breathing, and effective airway clearance techniques, typically recommended for thrice-daily practice. Aerobic training, such as ergometric cycling, walking, or stair climbing, was also frequently used to elevate and maintain target heart rate. Some studies also incorporated resistance training. Bhatia and Kayser (2019) notably used a high-intensity interval training (HIIT) program on an electromagnetic cycle ergometer during supervised sessions three times per week. Four articles (Yao et al, 2022; Machado et al, 2024; Tenconi et al, 2021; Kökez et al, 2023; Ferreira et al, 2021) reported additional rehabilitation programs post-surgery. While these post-surgical interventions could potentially influence overall outcomes, the focus of this review remains on the preoperative prehabilitation period. The design of these studies, as randomized controlled trials, aims to control for such biases by comparing prehabilitation groups to standard care groups.
Psychological Interventions
Three of the ten studies in this review included psychological interventions as part of a multimodal prehabilitation program. The study by Liu et al (2020) included psychological guidance, although the specific details of the intervention were not provided. The study by Yao et al (2022) included relaxation training, which involved deep breathing exercises and listening to relaxing music. The study by Ferreira et al (2021) included relaxation strategies, such as imagery, visualization, and deep breathing exercises.
Nutrition Interventions
Similar to psychological interventions, only three studies (Liu et al, 2020; Yao et al, 2022; Ferreira et al, 2021) integrated nutrition interventions into their multimodal prehabilitation programs. Liu et al (2020) included nutrition counselling with whey protein supplementation. Yao et al (2022) mentioned nutrition as part of a trimodal model but did not provide specific details. Ferreira et al (2021) also included nutritional counselling with whey protein supplementation.
Functional Assessment
The 6-minute walk test (6MWT), a measure of exercise capacity, has a recognized association with surgical outcomes and the incidence of postoperative complications. 30 The 6MWT is a crucial factor in assessing eligibility for lung resection. Several studies incorporated the 6MWT into preoperative evaluations, consistently demonstrating significant differences between intervention and control groups (Table 2).
 |
Table 2 Differences in Walking Distance (in 6-Minute Walk Test) in Patients with Lung Cancer After Prehabilitation |
Quality of Life
Three studies assessed the impact of radical lung cancer treatment on quality of life (QoL) and daily functioning. Two studies used the EORTC QLQ-C30, and one used the QoL Short Form Health Survey (SF-12), and another used the Functional Assessment of Cancer Therapy-Lung (FACT-L). Machado et al (2024) found beneficial effects for global QoL. Lai et al (2019) noted effectiveness only in mental health. Tenconi et al (2021) showed no significant effects on QoL. Ferreira et al (2021) reported greater scores in General Health and Mental Health using FACT-L. Quantitative data for these QoL assessments were not consistently provided across studies, limiting further meta-analysis.
Depression and Anxiety
Four studies examined the impact of prehabilitation on anxiety and depression levels in lung cancer patients using the Hospital Anxiety and Depression Scale (HADS). Three of these studies (Liu et al, 2020; Lai et al, 2019; Tenconi et al, 2021; Ferreira et al, 2021) reported a reduction in anxiety and depression levels after prehabilitation, but these changes were not statistically significant, implying no statistically demonstrable change despite potential clinical trends. One study (Yao et al, 2022) demonstrated a statistically significant reduction in anxiety and stress (p<0.05), and these effects persisted postoperatively. Numerical data for these scores were not consistently reported.
Cognitive Function
A major limitation observed is the complete absence of cognitive function assessment in any of the included studies. The impact of prehabilitation on cognitive function in this population therefore remains entirely unclear.
Postoperative Complications
All but one study emphasized the positive impact of prehabilitation on reducing the frequency and severity of postoperative complications, as classified by the Clavien-Dindo Classification. 31 The prehabilitation groups exhibited a significantly lower risk of complications, and those that did occur were less severe. The most frequent complications observed were postoperative pulmonary complications (PPCs), including pneumonia, atelectasis, and prolonged air leak. Prehabilitation groups experienced reduced incidence of pneumonia, likely due to breathing exercises and coughing techniques. Atelectasis incidence was also significantly reduced in prehabilitated patients. The prehabilitation group also experienced a lower incidence of prolonged air leak (PAL). Table 3 provides details on postoperative complication rates.
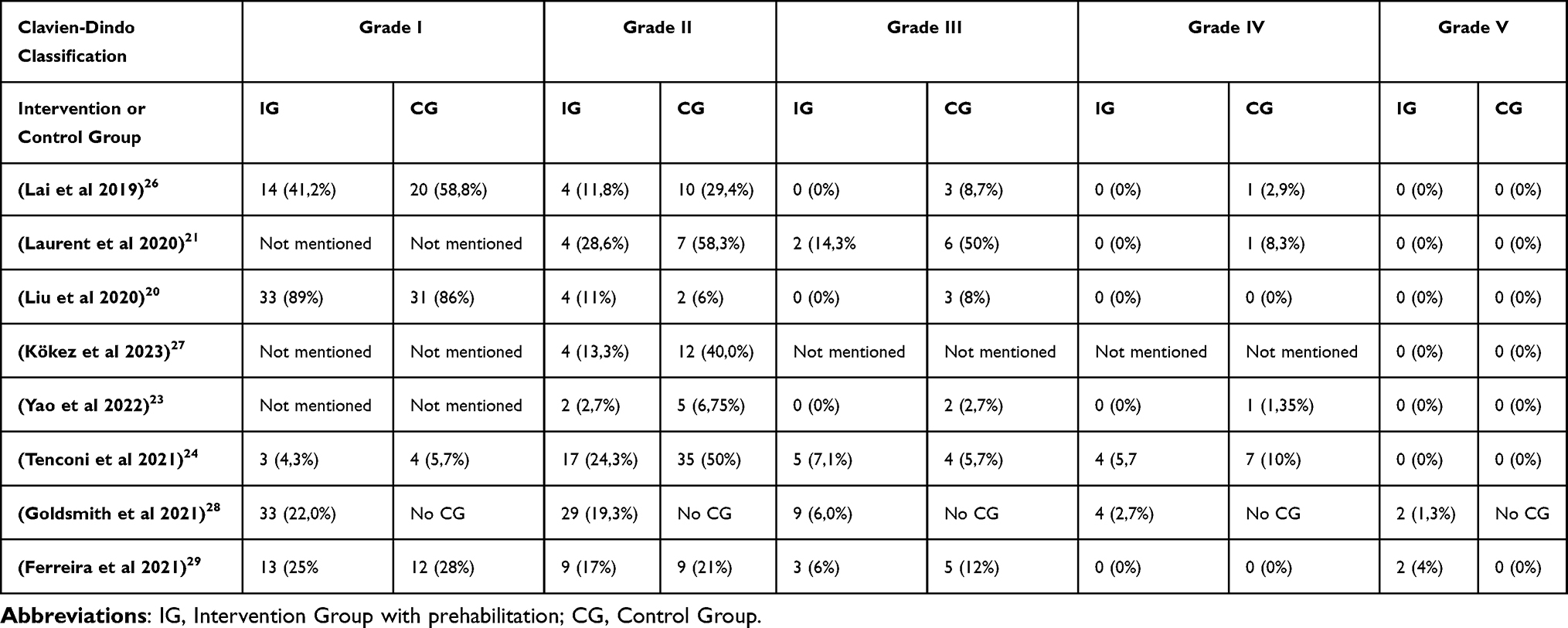 |
Table 3 Postoperative Complications Rate by Clavien-Dindo Classification |
Length of Stay
There was no consensus regarding length of stay (LOS) among the studies. While four studies demonstrated a significantly shorter LOS in the prehabilitation group, five studies found no significant difference in LOS between the prehabilitation and control groups. (Table 1) The majority of studies reported a LOS averaging approximately 7 days. Notably, some studies reported shorter ICU stays after surgery for the prehabilitation group.
Discussion
The objective of this systematic review was to thoroughly analyse the comprehensiveness of prehabilitation programs in adult lung cancer patients undergoing oncological – surgical treatment. A comprehensive approach to preoperative care should address the physical, psychological, and nutritional needs of patients in preparation for surgery. 32 To address this gap in knowledge, we reviewed recent literature (within the past five years) to assess the implementation and effectiveness of contemporary preoperative interventions.
Our findings reveal a critical insight: despite the recognized benefits of multimodal prehabilitation, only three out of ten included studies truly adopted a comprehensive approach, integrating physical exercise, psychological care, and nutritional interventions. This scarcity of comprehensive programs is a significant finding that warrants deeper discussion. Why are there so few? This could be attributed to several factors, including clinical methodological difficulty in implementing complex interventions, research methodology limitations in designing and funding such trials, or a lack of widespread awareness or adherence to existing guidelines for comprehensive patient care. For instance, while the European Society for Clinical Nutrition and Metabolism (ESPEN) emphasizes early nutritional assessment and intervention 33,35 only three studies in our review incorporated nutrition. This suggests a potential disconnect between established recommendations and their practical application in prehabilitation research and practice for lung cancer. The challenges in integrating these components might stem from a lack of interdisciplinary collaboration, insufficient training for healthcare professionals in areas outside their primary expertise, or the perceived complexity and resource intensity of delivering truly holistic care within existing healthcare systems. Future research could explore these barriers in more detail through qualitative studies or surveys of healthcare providers.
The value of comprehensive prehabilitation lies in its potential to yield additional or more holistic benefits beyond single-modality interventions. Physical exercise, particularly breathing exercises, aerobic training, and resistance training, consistently demonstrated effectiveness in improving functional capacity and reducing postoperative complications. This aligns with existing literature emphasizing the importance of physical optimization.4,5,10,36,37 However, the limited inclusion of psychological and nutritional components in most studies means we are likely missing crucial opportunities to further enhance patient resilience and outcomes. A truly multimodal approach is designed to address the interconnectedness of physical, mental, and nutritional health. For example, improved nutritional status can enhance physical performance, while reduced anxiety can improve adherence to exercise programs. The synergistic effects of these combined interventions are hypothesized to lead to superior overall outcomes compared to isolated interventions.
The studies that did incorporate psychological interventions (Liu et al, 2020; Yao et al, 2022; Ferreira et al, 2021) used approaches like psychological guidance, relaxation training, imagery, and visualization. While some showed clinically meaningful reductions in anxiety and depression, only one reported statistically significant improvements, highlighting the need for more robust research in this area. The lack of statistically significant changes in some studies might be due to variations in intervention intensity or duration, as lower intensity programs may not elicit significant psychological shifts. 38 It is also possible that the assessment tools used (eg, HADS) may not fully capture the nuanced psychological benefits or that the sample sizes were insufficient to detect statistically significant differences. Addressing psychological distress is paramount in cancer care 11,14 and its limited integration into prehabilitation programs for lung cancer patients represents a missed opportunity to improve patient well-being and potentially influence physiological recovery. Future research should consider more tailored psychological interventions and more sensitive outcome measures.
Similarly, the infrequent inclusion of nutritional interventions is concerning given the high prevalence of malnutrition in cancer patients, particularly those with lung cancer 33 Malnutrition is strongly associated with adverse surgical outcomes.15,16 The absence of comprehensive nutritional support in most prehabilitation programs could lead to suboptimal patient preparation, potentially impacting recovery and increasing complications. This oversight might be due to a lack of routine nutritional screening, limited access to dietitians, or a prevailing focus on surgical aspects over holistic patient preparation. Future research should explore the optimal timing, type, and intensity of nutritional interventions within multimodal prehabilitation to maximize benefits, potentially including personalized dietary plans and targeted supplementation.
The consistent improvement in functional outcomes, particularly the 6-minute walk test, across several studies underscores the effectiveness of prehabilitation in enhancing physical capacity. This functional improvement is critical for patients undergoing lung resection, as it directly correlates with surgical eligibility and postoperative recovery 30 The ability of prehabilitation to maintain enhanced physical capacity post-resection, unlike standard care, is a significant benefit, promoting greater independence in daily activities. While a meta-analysis on functional outcomes was considered, the heterogeneity in intervention types, durations, and reported metrics across the included studies limited its feasibility for this review. This highlights a need for greater standardization in prehabilitation protocols and outcome reporting to facilitate future meta-analyses and stronger evidence synthesis.
Regarding postoperative complications, prehabilitation consistently demonstrated a positive impact, reducing both the frequency and severity of complications, especially pulmonary complications like pneumonia and atelectasis. This is a crucial finding given the significant impact of PPCs on patient morbidity, mortality, and healthcare costs 39,40 The benefits observed are likely due to the emphasis on breathing exercises and improved airway clearance techniques within prehabilitation programs, which directly target respiratory function. The reduction in more severe complications (Clavien-Dindo Grade III or higher) further underscores the clinical significance of prehabilitation in improving patient safety and reducing the burden on healthcare systems.
The inconsistent findings regarding the length of hospital stay suggest that while prehabilitation may offer benefits in some cases, it does not universally lead to a shorter hospital stay. This could be influenced by various factors not fully captured in the reviewed studies, such as patient comorbidities, surgical complexity, hospital protocols, and variations in discharge criteria. However, the reported shorter ICU stays for prehabilitated patients are a positive indicator, suggesting that even if overall LOS is not consistently reduced, prehabilitation may contribute to a less complicated and more efficient immediate postoperative recovery. Further research is needed to identify specific patient subgroups or prehabilitation characteristics that are most likely to benefit from reduced LOS.
Future Perspectives and Challenges
The findings of this review underscore the need for a paradigm shift towards truly comprehensive multimodal prehabilitation in lung cancer care. A significant challenge lies in the implementation of such programs within diverse healthcare settings, requiring interdisciplinary collaboration among surgeons, oncologists, physiotherapists, dietitians, psychologists, and nurses. Developing standardized, yet individualized, protocols that are adaptable to different patient needs and resource availability is crucial. The role of digital health technologies, as highlighted by recent studies on digital multimodal cancer prehabilitation,3 offers a promising avenue for delivering scalable and accessible interventions, particularly for home-based programs.
Another key perspective is the need for more rigorous research designs. Future randomized controlled trials should explicitly compare comprehensive multimodal prehabilitation against single-modality interventions and standard care, with sufficient power to detect statistically significant differences across a broad range of outcomes, including long-term survival, quality of life, and cognitive function. Standardized reporting of intervention details and outcome measures would greatly enhance the ability to synthesize evidence and conduct meta-analyses. Furthermore, qualitative research could provide valuable insights into patient and provider perspectives on the feasibility, acceptability, and perceived benefits of comprehensive prehabilitation.
Finally, the economic implications of comprehensive prehabilitation warrant further investigation. While initial investment in multimodal programs may seem high, the potential for reduced postoperative complications, shorter ICU stays, and improved long-term outcomes could lead to significant cost savings for healthcare systems. Robust cost-effectiveness analyses are essential to advocate for the widespread adoption of these programs. By addressing these challenges and pursuing these research avenues, the field can move closer to establishing clear, evidence-based guidelines for comprehensive prehabilitation in lung cancer, ultimately optimizing patient outcomes and enhancing their overall well-being throughout their treatment journey.
Limitation of Study
This systematic review has several limitations that should be acknowledged. Firstly, the number of studies included was relatively small (10 studies), and their limited sample sizes may affect the generalizability of the findings. Secondly, significant heterogeneity existed in the prehabilitation interventions, including variations in duration, setting, and specific components, which makes it challenging to draw definitive conclusions about the optimal approach. Thirdly, the majority of included studies focused primarily on physical prehabilitation, with limited attention to psychological and nutritional interventions. This limits the ability to draw comprehensive conclusions about the effectiveness of truly multimodal prehabilitation programs. Finally, the review was limited to studies published in English within the past five years, which may have excluded relevant research published in other languages or earlier timeframes.
Conclusions
In summary, prehabilitation demonstrates a positive impact on surgical outcomes by reducing postoperative complications, particularly pulmonary complications, and enhancing patients’ physical capacity, which can be maintained postoperatively, promoting greater independence. However, our findings indicate a significant underutilization of comprehensive multimodal prehabilitation, with only three of the ten included studies incorporating the crucial psychological and nutrition components. The impact of prehabilitation on length of stay, quality of life, and emotional and mental health requires further investigation, and its effect on cognitive function in lung cancer patients remains largely unexplored. This review highlights the urgent need for paradigm shift toward truly comprehensive multimodal care and the establishment of clear, evidence-basedid guidelines for this patient population. Future high-quality Randomized Controlled Trials (RCTs) must be designed to rigorously evaluate comprehensive multimodal prehabilitation against single-modality interventions and standard care, with a strong focus on standardized outcome reporting and detailed assessments of psychological, nutritional, and cognitive outcomes to fully elucidate its benefits. By addressing these knowledge gaps and promoting a comprehensive approach to prehabilitation, we can optimize patient outcomes and enhance their overall well-being throughout the lung cancer treatment journey. New studies published since the completion of this review, such as those exploring digital multimodal cancer prehabilitation 3 and the impact of psychological interventions on molecular biomarkers,41 further emphasize the evolving landscape and the need for continued research in this area.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Cancer Society. Key Statistics for Lung Cancer. Available from: https://www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html.
2. Lackey A, Donington JS. Surgical management of lung cancer. Semin Intervent Radiol. 2013;30(2):133–140. doi:10.1055/s-0033-1342954
3. Gkaintatzi E, Nikolaou CK, Rampal T, Laza-Cagigas R, Zand N, McCrone P. Cost analysis of a digital multimodal cancer prehabilitation. Curr Oncol. 2022;29(12):9305–9313. doi:10.3390/curroncol29120729
4. López-Baamonde M, Arguis MJ, Navarro-Ripoll R, et al. Multimodal prehabilitation in heart transplant recipients improves short-term post-transplant outcomes without increasing costs. J Clin Med. 2023;12(11):3724. doi:10.3390/jcm12113724
5. Santa Mina D, Scheede-Bergdahl C, Gillis C, Carli F. Optimization of surgical outcomes with prehabilitation. Appl Physiol Nutr Metab. 2015;40(9):966–969. doi:10.1139/apnm-2015-0084
6. Durrand J, Singh SJ, Danjoux G. Prehabilitation. Clin Med. 2019;19(6):458–464. doi:10.7861/clinmed.2019-0257
7. Edbrooke L, Bowman A, Granger CL, et al. Exercise across the lung cancer care continuum: an overview of systematic reviews. J Clin Med. 2023;12(5):1871. doi:10.3390/jcm12051871
8. Granger C, Cavalheri V. Preoperative exercise training for people with non-small cell lung cancer. Cochrane Database Syst Rev. 2022;9(9):CD012020. doi:10.1002/14651858.CD012020.pub3
9. Michael CM, Lehrer EJ, Schmitz KH, Zaorsky NG. Prehabilitation exercise therapy for cancer: a systematic review and meta-analysis. Cancer Med. 2021;10(13):4195–4205. doi:10.1002/cam4.4021
10. Silver JK, Baima J. Cancer prehabilitation: an opportunity to decrease treatment-related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. Am J Phys Med Rehabil. 2013;92(8):715–727. doi:10.1097/PHM.0b013e31829b4afe
11. Shalata W, Gothelf I, Bernstine T, et al. Mental health challenges in cancer patients: a cross-sectional analysis of depression and anxiety. Cancers. 2024;16(16):2827. doi:10.3390/cancers16162827
12. Civilotti C, Lucchini D, Fogazzi G, et al. The role of integrated psychological support in breast cancer patients: a randomized monocentric prospective study evaluating the Fil-Rouge Integrated Psycho-Oncological Support (FRIPOS) program. Support Care Cancer. 2023;31(5):266. doi:10.1007/s00520-023-07732-4
13. Nosarti C, Roberts JV, Crayford T, McKenzie K, David AS. Early psychological adjustment in breast cancer patients: a prospective study. J Psychosom Res. 2002;53(6):1123–1130. doi:10.1016/s0022-3999(02)00350-1
14. Mavros MN, Athanasiou S, Gkegkes ID, Polyzos KA, Peppas G, Falagas ME. Do psychological variables affect early surgical recovery? PLoS One. 2011;6(5):e20306. doi:10.1371/journal.pone.0020306
15. Zhang B, Najarali Z, Ruo L, et al. Effect of perioperative nutritional supplementation on postoperative complications-systematic review and meta-analysis. J Gastrointest Surg. 2019;23(8):1682–1693. doi:10.1007/s11605-019-04173-5
16. Weimann A, Braga M, Carli F, et al. ESPEN practical guideline: clinical nutrition in surgery. Clin nutr. 2021;40(7):4745–4761. doi:10.1016/j.clnu.2021.03.031
17. Wickerson L, Rozenberg D, Janaudis-Ferreira T, et al. Physical rehabilitation for lung transplant candidates and recipients: an evidence-informed clinical approach. World J Transplant. 2016;6(3):517–531. doi:10.5500/wjt.v6.i3.517
18. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
19. Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176–184. doi:10.1111/j.1524-475X.2004.04006.x
20. Liu Z, Qiu T, Pei L, et al. Two-week multimodal prehabilitation program improves perioperative functional capability in patients undergoing thoracoscopic lobectomy for lung cancer: a randomized controlled trial. Anesth Analg. 2020;131(3):840–849. doi:10.1213/ANE.0000000000004342
21. Laurent H, Aubreton S, Galvaing G, et al. Preoperative respiratory muscle endurance training improves ventilatory capacity and prevents pulmonary postoperative complications after lung surgery. Eur J Phys Rehabil Med. 2020;56(1):73–81. doi:10.23736/S1973-9087.19.05781-2
22. Bhatia C, Kayser B. Preoperative high-intensity interval training is effective and safe in deconditioned patients with lung cancer: a randomized clinical trial. J Rehabil Med. 2019;51(9):712–718. doi:10.2340/16501977-2592
23. Yao L, Chen H, Xue B. Application and practice of trimodal prehabilitation model in preoperative management of patients with lung cancer undergoing video-assisted thoracoscopic surgery. Front Surg. 2022;9:1047977. doi:10.3389/fsurg.2022.1047977
24. Tenconi S, Mainini C, Rapicetta C, et al. Rehabilitation for lung cancer patients undergoing surgery: results of the PUREAIR randomized trial. Eur J Phys Rehabil Med. 2021;57(6):1002–1011. doi:10.23736/S1973-9087.21.06789-7
25. Machado P, Pimenta S, Garcia AL, et al. Effect of preoperative home-based exercise training on quality of life after lung cancer surgery: a multicenter randomized controlled trial. Ann Surg Oncol. 2024;31(2):847–859. doi:10.1245/s10434-023-14503-2
26. Lai Y, Wang X, Zhou K, Su J, Che G. Impact of one-week preoperative physical training on clinical outcomes of surgical lung cancer patients with limited lung function: a randomized trial. Ann Transl Med. 2019;7(20):544. doi:10.21037/atm.2019.09.151
27. Kökez H, Keskin H, Ergin M, Erdoğan A. Is preoperative pulmonary rehabilitation effective in the postoperative period after lung resection? Afr Health Sci. 2023;23(1):646–655. doi:10.4314/ahs.v23i1.69
28. Goldsmith I, Chesterfield-Thomas G, Toghill H. Pre-treatment optimization with pulmonary rehabilitation in lung cancer: making the inoperable patients operable. EClinicalMedicine. 2021;31:100663. doi:10.1016/j.eclinm.2020.100663
29. Ferreira V, Minnella EM, Awasthi R, et al. Multimodal prehabilitation for lung cancer surgery: a randomized controlled trial. Ann Thorac Surg. 2021;112(5):1600–1608. doi:10.1016/j.athoracsur.2020.11.022
30. Lee H, Kim HK, Kang D, et al. Prognostic value of 6-min walk test to predict postoperative cardiopulmonary complications in patients with non-small cell lung cancer. Chest. 2020;157(6):1665–1673. doi:10.1016/j.chest.2019.12.039
31. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
32. Hijazi Y, Gondal U, Aziz O. A systematic review of prehabilitation programs in abdominal cancer surgery. Int J Surg. 2017;39:156–162. doi:10.1016/j.ijsu.2017.01.111
33. Arends J, Baracos V, Bertz H, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187–1196. doi:10.1016/j.clnu.2017.06.017
34. Lobo DN, Gianotti L, Adiamah A, et al. Perioperative nutrition: recommendations from the ESPEN expert group. Clin Nutr. 2020;39(11):3211–3227. doi:10.1016/j.clnu.2020.03.038
35. Arends J. Malnutrition in cancer patients: causes, consequences and treatment options. Eur J Surg Oncol. 2024;50(5):107074. doi:10.1016/j.ejso.2023.107074
36. Bausys A, Luksta M, Kuliavas J, et al. Personalized trimodal prehabilitation for gastrectomy. Medicine. 2020;99(27):e20687. doi:10.1097/MD.0000000000020687
37. Toohey K, Hunter M, McKinnon K, et al. A systematic review of multimodal prehabilitation in breast cancer. Breast Cancer Res Treat. 2023;197(1):1–37. doi:10.1007/s10549-022-06759-1
38. Paolucci EM, Loukov D, Bowdish DME, Heisz JJ. Exercise reduces depression and inflammation but intensity matters. Biol Psychol. 2018;133:79–84. doi:10.1016/j.biopsycho.2018.01.015
39. Agostini P, Cieslik H, Rathinam S, et al. Postoperative pulmonary complications following thoracic surgery: are there any modifiable risk factors? Thorax. 2010;65(9):815–818. doi:10.1136/thx.2009.123083
40. Aprile V, Bacchin D, Calabrò F, et al. Intraoperative prevention and conservative management of postoperative prolonged air leak after lung resection: a systematic review. J Thorac Dis. 2023;15(2):878–892. doi:10.21037/jtd-22-736
41. Hanalis-Miller T, Ricon-Becker I, Sakis N, et al. Peri-operative individually tailored psychological intervention in breast cancer patients improves psychological indices and molecular biomarkers of metastasis in excised tumors. Brain Behav Immun. 2024;117:529–540. doi:10.1016/j.bbi.2024.02.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.