Back to Journals » Clinical Interventions in Aging » Volume 20
Complications, Blood Transfusion Prediction, and Long-Term Survival in Elderly Patients with Pubic Rami Fractures
Authors Beloosesky Y ![]() , Naser MS
, Naser MS ![]() , Levy Y, Cooper L, Kagansky N, Weiss A
, Levy Y, Cooper L, Kagansky N, Weiss A
Received 8 August 2025
Accepted for publication 2 December 2025
Published 12 December 2025 Volume 2025:20 Pages 2535—2542
DOI https://doi.org/10.2147/CIA.S553024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yichayaou Beloosesky,1,2 Muhammad Saeed Naser,2 Yochai Levy,3 Lisa Cooper,2 Nadya Kagansky,3 Avraham Weiss2
1Adelson School of Medicine, Ariel University, Ariel, Israel; 2Department of Geriatrics, Rabin Medical Center, Beilinson Hospital, Gray Faculty of Medical and Health Sciences, Tel Aviv University, Petach Tikvah, Israel; 3Shmuel Harofeh Geriatric Hospital, Gray Faculty of Medical and Health Sciences, Tel Aviv University, Be’er Ya’akov, Israel
Correspondence: Yichayaou Beloosesky, Adelson School of Medicine, Ariel University, Ariel, Israel, Email [email protected]
Introduction: The elderly population is steadily increasing, concurrently with the incidence of pubic rami fractures (PRFs), impacting function, morbidity and mortality. We aimed to assess functional background, clinical course, hemoglobin decline, transfusion needs, complications, and long-term survival.
Methods: A retrospective cohort study. Data was collected from patients hospitalized in a geriatric internal medicine ward, due to PRFs between 2012 and 2022. Demographic, clinical, and outcome data were recorded and analyzed.
Results: The study comprised 165 patients, mean age 85.9± 6.4 years; 138 (83.6%) were women, 133 (80%) had experienced at least one PRF, an additional 32 cases had experienced another pelvic fracture. Functionally, 76 (46%) were independent, 49 (29.7%) partially dependent, and 40 (24.2%) fully dependent. Cognitively, 106 (64.2%) were preserved, 29 (17.6%) experienced a cognitive decline, and 30 (18.2%) suffered from dementia. The complication rate was 15.1%, half from infectious diseases. One-year mortality was 20%. The average maximum decrease in hemoglobin occurred 4.4 days post-fracture, with a difference in average admission hemoglobin between those who required blood transfusions and those who did not (9.81 g/dL and 12.06 g/dL) (p=0.0001). Almost 10% of the elderly needed blood transfusions. Logistic regression analysis identified two independent predictors for blood transfusions: an admission hemoglobin level < 10 g/dL and the presence of cognitive decline or dementia. The model showed high accuracy, with a ROC AUC of 0.885, sensitivity of 0.875, and specificity of 0.792. Over half of the patients returned home; 35% were transferred to rehabilitation facilities.
Conclusion: This study provides new and important information on PRFs in the elderly. We recommend closely monitoring these patients because of complications, functional decline, need for rehabilitation, and the high risk of significant blood loss peaking several days post-fracture, thereby, requiring transfusions, particularly, in elderly individuals suffering from cognitive decline or dementia and low initial hemoglobin.
Plain Language Summary: We found a complication rate of 15.1% after pubic rami fractures, half from infectious diseases and a one-year mortality of 20%.The average maximum decrease in hemoglobin occurred 4.4 days post pubic rami fractures, with 9.7% of the elderly needing blood transfusions.We developed a simple and highly accurate model (AUC 0.885, sensitivity 0.875, specificity 0.792), predicting which patients > 65 with pubic rami fractures will need transfusions, based on hemoglobin levels < 10 g/dL and cognitive decline or dementia at admission.Over half of the patients with pubis rami fractures returned home; 35% were transferred to rehabilitation facilities.
Keywords: blood loss, mortality, pelvic fracture, transfusion risk, rehabilitation
Introduction
The global elderly population is projected to reach 15.9% by 2050, with higher rates in industrialized countries.1 The occurrence of pelvic fragility fractures is increasing due to aging of populations, osteoporosis and falls.2 The annual incidence of fragility pubic rami fractures (PRFs) is at least 13% after age 65, and has steadily risen in many countries during the last few decades, ie, the USA,3 Germany,4 the UK5,6 and Switzerland.7 These fractures are significantly more common in women, increasing with age, thus, leading to severe consequences. Elderly patients with PRFs experience elevated rates of complications, prolonged hospital stays, increased in-hospital and long-term mortality, as well as higher incidences of ambulation deterioration, loss of independence, and institutionalization.8–11
Pubic ramus fractures have been less extensively studied than hip fractures,12 mainly because they are usually stable, treated conservatively,13 occasionally, under-recognized14 and are associated with lower mortality. In contrast, hip fractures require surgical management, carry a high morbidity and mortality, and are systematically recorded in major databases.15 Consequently, research efforts and funding have traditionally focused on hip fractures, whereas, pubic ramus fractures have received limited attention despite their impact, especially in old age on pain, complications, mobility, and very often functional decline.
The aim of this retrospective study was to assess functional background, clinical course, hemoglobin decline, transfusion requirements, complications, and long-term survival in a cohort of elderly patients hospitalized with PRFs.
Methods
Study Design and Subjects
The study was conducted in the Acute Geriatric Ward at Rabin Medical Center, Beilinson Hospital, Petach Tikvah Israel, and approved by the Hospital’s Institutional Review Board. Participants’ consent was exempted by the Hospital’s Institutional Review Board because it was a retrospective study. Patient data was kept strictly confidential.
Inclusion criteria: patients ≥65 years admitted from January 2012 to December 2022 for conservative treatment of fragility PRFs. Exclusion criteria: terminal illnesses, end-stage heart and lung failure, other limb fractures, and candidates for surgical treatment.
Data Collection
Data including socio-demographic characteristics, cognitive and functional status, laboratory data, comorbidities, number of packed cells (PCs) given and medications were collected from the electronic medical records of the Rabin Medical Center. Cognitive level was assessed by the Mini-Mental State Examination,16 categorizing patients into three groups: severely impaired (scores <14), moderately impaired (scores 15–24), and normal (scores ≥25).17 Functional status was evaluated by the Katz Index of Activities of Daily Living so as to classify patients as fully dependent, partially dependent, and independent.18 Survival was recorded for all patients; the last one recruited was followed-up for at least one year.
Statistical Analysis
This study was primary hypothesis-generating, therefore, subgroups were not predefined, but, based on the analysis of the data. The pelvic fracture cohort consisted of patients with varying fracture types, some with only PRF and others with additional pelvic fractures, as well as differing levels of function and cognition. Therefore, we compared several variables between these subgroups, such as the need for blood transfusions. Non-normally distributed continuous variables were compared by the Wilcoxon Rank-Sum test; normally distributed continuous variables were analyzed by T tests and ANOVA. The Fisher’s exact test compared variables between patient groups. A logistic regression analysis was conducted to identify independent variables affecting blood transfusion. The variables were hemoglobin levels (<10 g/dL vs ≥10 g/dL), functional levels (independent, partially dependent, fully dependent), cognitive levels (normal, cognitively impaired, demented), use of anti-aggregant and anticoagulant drugs, and background diseases. Sensitivity and specificity for predicting blood transfusions among patients with PRFs were assessed via a ROC analysis and AUC. A p value of <0.05 was considered significant for all analyses. Analyses were performed using the SAS 9.4 software.
Results
The study included 165 patients aged 65 to 100 years, with an average age of 85.9±6.4 years. Of these, 138 (83.6%) were women and 27 (16.4%) were men. Among the patients, 133 (80%) had experienced at least one PRF; 32 (20%) had experienced other pelvic fractures including sacrum, acetabulum, and ileum. Table 1 shows the demographic and clinical parameters for each group, with no significant differences between them.
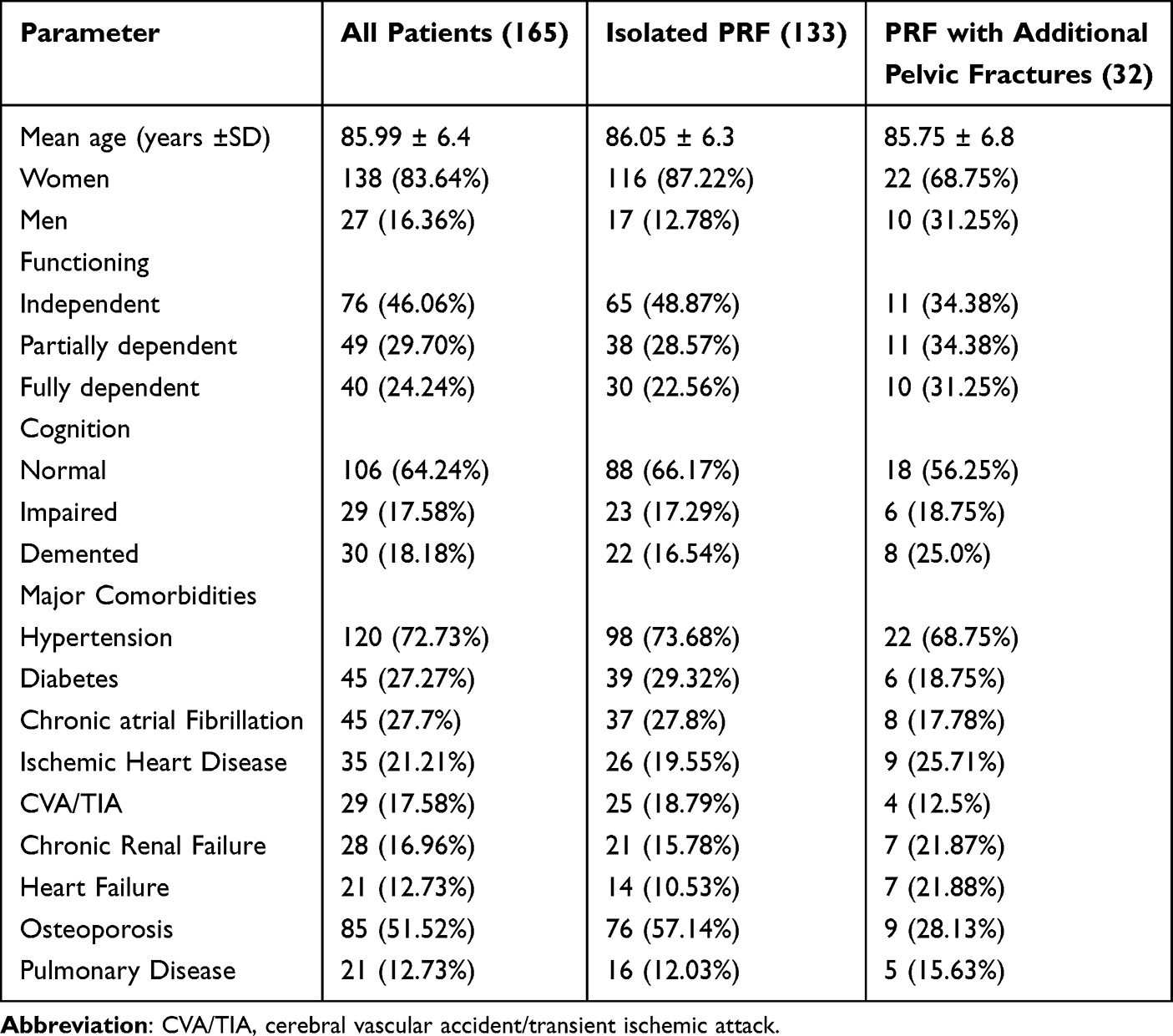 |
Table 1 Demographic and Clinical Parameters of Patients’ Groups |
Overall, 25 (15.1%) patients experienced complications: urinary tract infections −8, respiratory infections −3, other infections −3, severe delirium −6, cerebral vascular accident/transient ischemic accident −2, pressure sores −1, pulmonary embolus −1 and acute coronary syndrome −1. Fifty-four (32.7%) patients received anti-aggregating drugs; 49 (29.7%) - anticoagulation drugs, and 62 did not receive any medications. Patients lost an average of 0.91 g/dL hemoglobin from admission to discharge, with the lowest point averaging a 1.5 g/dL loss on an average of 4.4 days after admission. There were no significant differences in the lowest hemoglobin levels among the groups taking anti-aggregating drugs, anticoagulation drugs, or no drugs at all (p = 0.26). Sixteen patients (9.7%) needed PCs transfusions, with an average blood loss of 2.4 g/dL. Among them, six received anti-aggregating drugs, four - anticoagulating drugs, and six - no medication at all. The need for PCs transfusions did not significantly differ between patients receiving anti-aggregating or anticoagulating drugs to those not receiving these medications (p=0.19). Among the sixteen patients who received blood transfusions, eleven presented with PRF only, whereas, five had additional pelvic fractures; this difference was not statistically significant (p=0.2). There was also no significant difference between the functional groups and the PCs transfusions (p=0.7). Of the cognitively normal, cognitively impaired, and demented groups, 5.71%, 24.14%, and 10.0%, respectively, required a PC transfusion (p=0.012).
Patients with cognitive impairment had a significantly higher risk of needing a PC transfusion compared to cognitively normal patients (OR 5.2, CI: 1.6–17.2, p=0.017). However, the difference between demented and cognitively normal groups was not statistically significant, possibly due to sample size limitations (OR 1.8, CI: 0.4–7.8). Patients with chronic renal failure required more PCs transfusions than those without (p=0.033). The mean hemoglobin level at admission was 9.81 g/dL for patients who received PCs and 12.06 g/dL for those who did not (p=0.0001).
Logistic regression analysis showed that only hemoglobin <10 g/dL (p<0.0001) and cognitive impairment/dementia (p=0.005) independently affect blood transfusion. Receiver operating characteristic (ROC) curve analysis yielded an AUC of 0.885, with a sensitivity of 0.875 and specificity of 0.792 for predicting blood transfusion in patients with PRF (Figure 1). The average length of hospitalization was 9 days, (range 1–32 days) with a longer duration for patients with PRF and additional pelvic fractures compared to those with PRF-only, 10.5 and 8.7 days, respectively, (p=0.38). Eighty-nine patients (54%) returned home, 59 (35.15%) were transferred to rehabilitation facilities, 12 (7.27%) were sent to nursing homes, and 5 (3.21%) died during hospitalization.
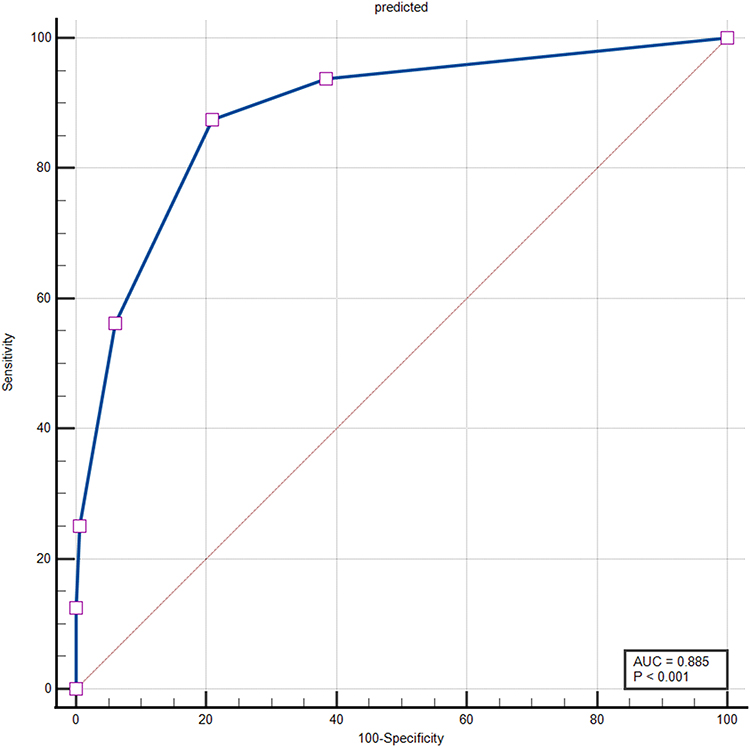 |
Figure 1 ROC curve and AUC value predicting blood loss, sensitivity 0.875, specificity 0.792. |
One-year mortality was 20% (33 patients). Over the 11-year follow-up, 99 patients (60%) died: 86 in the PRF-only group (64.7%) and 13 in the PRF additional pelvic fracture group (40.6%). The Kaplan-Meier curves showed worse survival for the PRF-only group (p = 0.03), and worse long-term survival for the 16 patients who needed PCs compared to those who did not (p=0.049) (Figure 2).
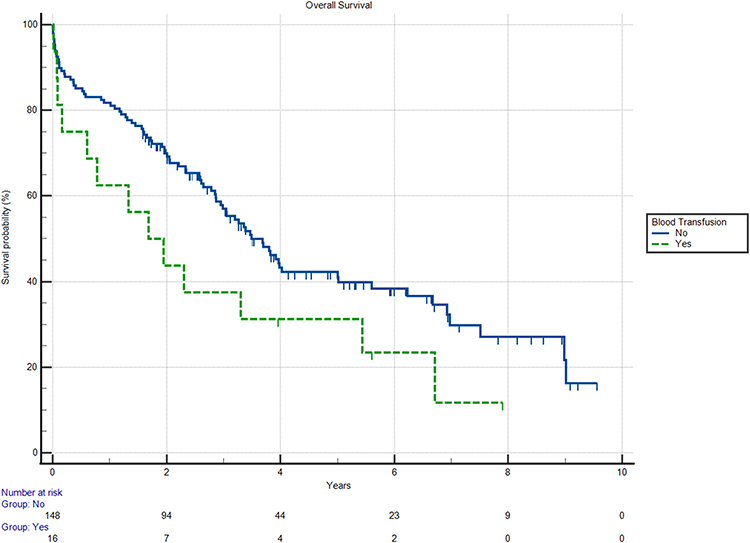 |
Figure 2 Kaplan Meier survival analysis graphs of 16 patients who needed packed cells compared to 148 who did not (p=0.049) (Data for one patient is missing). |
Discussion
We describe the clinical, functional and cognitive background of elderly patients with fragility PRFs, their hospital stays, complications, and 10-year survival. We ascertained three key findings: 1. ~10% of the elderly patients needed blood transfusions; 2. hemoglobin levels dropped most significantly after the fourth day post-fracture; 3. in patients >65 with cognitive impairment or dementia, and hemoglobin <10 g/dL, the need for a blood transfusion can be predicted with high sensitivity and specificity.
The average age of the patients was 85.9 ± 6.4 years, with ages ranging from 65 to 100 years, similar to previous studies.7,9,11,19 Most patients were women (83.6%), consistent with prior findings.7–9,19,20 A few studies mention the functional and cognitive status of patients pre-fracture, though, Mears et al19 lacks detailed information. Approximately 38% of the patients were demented, comparable to our study of 35.2%. In the present study, 46% were independent, 29.7% partially dependent, and 24.2% fully dependent prior to their fracture.
No significant differences were observed in demographic, functional, clinical data, and background diseases between patients with isolated PRFs and those with additional pelvic fractures. Similar findings were reported by others who compared pelvic fractures with or without displacement with additional fractures.19 The lack of differences between the groups may be attributed to the fact that many patients in the present study were frail and had experienced multiple PRFs, rather than a single branch. Moreover, some studies indicated that most cases involved other fractures in different parts of the pelvis, which were discovered only after a further evaluation with a CT or MRI, thus, suggesting that these injuries were more complex than initially identified as just a PRF.21,22
The in-hospital complication rate was 15.1%, with ~50% urinary and respiratory tract infections, and the rest primarily significant delirium and cardiovascular events. The low delirium rate observed may be due to the retrospective study design and lack of awareness. Delirium was not recorded as a complication in previous studies, most probably, overlooked rather than absent. Other studies reported complication rates of 25.4%,19 20.2%,23 40%11 (including urinary retention), and 16.5%.8 The average length of stay was ~9 days, ranging from 1 to 32 days due to patient variability. Other studies have reported varying lengths: Switzerland averaged 39 days,7 France, 45 days,11 the USA, 7 days,19 and Germany, 8 days.8 Differences were most probably due to healthcare systems, hospital practices, and transfer protocols.
Sixteen patients (9.7%) received PCs. The average blood loss among these patients was 2.4 g/dL. Apart from one study that reported a 2 g/dL drop in hemoglobin,23 we found no quantitative data on hemoglobin reduction or the lowest hemoglobin levels in patients with PRFs in the reviewed literature. Furthermore, the proportion of patients who received the PCs was not documented. Several case reports and brief reviews describe massive hemorrhages resulting from these fractures; some hemorrhages were life-threatening, and some resulted in fatalities, despite treatment with PCs, other blood products, and embolization of bleeding pelvic arteries.23–28 These hemorrhages are often caused by tears in the corona mortis and obturator arteries which are in close proximity and in contact with the pubis. These tears are more common in the elderly due to changes in their connective tissue, muscles and atherosclerosis of the arteries, causing high fragility and inability to adequately vasoconstrict, as well as the use of anti-coagulants and antiplatelet medications. Indeed,10 out of 16 patients who received PCs were on such medications. Significant drops in hemoglobin can occur with a delay, so close monitoring is essential for up to several days post-fracture.23–26
Logistic regression analysis identified two independent predictors for blood transfusions in patients with PRFs: admission hemoglobin levels <10 g/dL and cognitive impairment/dementia. The model’s AUC was 0.885, indicating excellent predictive ability with high sensitivity (0.875) and good specificity (0.792). Most patients (54%) returned home; 36% needed continued treatment in rehabilitation facilities, indicating the severity of this injury. Some studies showed that 49% had lost independence and 34% required rehabilitation.9 Other studies have reported that half did not regain pre-fracture function and ~25% moved to nursing homes.11 Other authors reported that 33% moved to nursing homes and 36% needed mobility assistance.20
The overall mortality rate after one year among our patients was 20%. Previous studies reported similar mortality rates, ranging from 14.3% to 27%.7–11,20 This variation in mortality rates may be attributed to different patient demographics, fracture types, hospital settings, and backgrounds. Only a limited amount of studies have tracked long-term mortality following PRFs. Hill et al’s study of 286 patients, with an average age of 74.7 years, (36 of whom were involved in traffic accidents), found a 5-year mortality rate of 54.4%.6 Hamilton et al’s study of 43 patients, with an average age of 79.4 years, reported a mortality rate of 58.1% after 5 years.20
In the only study with a 10-year follow-up, involving 99 patients with an average age of 80.1 years (fractures occurred between 1994–2007), the mortality rate was 93.8%. The authors compared the PRF group to age and sex-matched controls and found a higher mortality among patients with fractures.28 In the current study, only 40% survived after 11 years of follow-up (but, patients were recruited over a 10-year period). Those who received PCs experienced a higher long-term mortality. This is most probably due to overall poorer health and a higher vulnerability at baseline, since they had a higher rate of cognitive impairment, renal failure and initially lower hemoglobin levels.
Our study has several limitations. As a retrospective study based on data from databases, the study inherently lacks the advantages of a prospective study. It was challenging to ensure that all the information was accurately received and recorded. Some complications might not have been documented or may have been incorrectly recorded. This is a single center rather than multi-center study, thus, introducing potential biases due to differing approaches, including diagnoses and treatments between centers, thereby, may not represent a comprehensive, multi-regional sample of patients with PRF.
There is also a selection bias at multiple levels. Some patients with PRFs may have been discharged home or returned to nursing homes after a diagnosis in the emergency room, potentially leading to an underrepresentation of seemingly milder cases in our sample. Additionally, patients with more complex medical conditions could have been hospitalized in geriatric or internal medicine departments for ongoing medical issues, while those with less severe medical issues were admitted to the orthopedic department.
On the other hand, the current study has notable strengths. A relatively large number of patients were examined compared to other studies in the field. Patients were hospitalized in a geriatric internal medicine department where they were evaluated and classified according to function and cognition, parameters that are seldom referenced in medical literature. The follow-up period was extensive and unique. Accurate hemoglobin level recordings were made upon admission to the emergency department and at the point when it reached its lowest level, allowing for the determination of hemoglobin drop for all patients. Additionally, a precise record was kept of the number of patients who received blood transfusions, both, rarely addressed in the medical literature.
Conclusions
PRFs are common in the elderly, leading to a high morbidity, mortality, rehabilitation need and dependency on care. Maximal blood loss typically occurred after 4 days post-fracture, with ~10% of patients needing transfusions. We developed a simple and highly accurate model, predicting which patients >65 with PRFs will need transfusions, based on hemoglobin levels <10 g/dL and cognitive impairment/dementia at admission. In clinical practice, we highly recommend close monitoring of these patients due to possible complications, functional deterioration, rehabilitation needs, and most significantly, even life-threatening blood loss that may require transfusions, especially, in those with cognitive impairment/dementia and low initial hemoglobin level.
Abbreviations
AUC, area under the curve; CVA/TIA, cerebral vascular accident/transient ischemic attack, PCs, packed cells; PRFs, pubic rami fractures.
Data Sharing Statement
Data supporting the findings of this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Rabin Medical Center, Beilinson Hospital, Institutional Review Board.
No informed consent was required in this retrospective study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; they took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Gu D, Andreev K, Dupre ME. Major trends in population growth around the world. China CDC Wkly. 2021;3(28):604–613. doi:10.46234/ccdcw2021.160
2. Rommens PM, Hofmann A. Focus on fragility fractures of the pelvis. Eur J Trauma Emerg Surg. 2021;47:1–2. doi:10.1007/s00068-020-01550-7
3. Suneja N, Kong RM, Tracey OC, Mallon Z, Tischler EH. Epidemiology of fragility pubic ramus fractures in the United States. Geriatr Orthop Surg Rehabil. 2022;13:21514593221097274. doi:10.1177/21514593221097274
4. Andrich S, Haastert B, Neuhaus E, et al. Epidemiology of pelvic fractures in Germany: considerably high incidence rates among older people. PLoS One. 2015;10(9):e0139078. doi:10.1371/journal.pone.0139078
5. Clement ND, Court-Brown CM. Elderly pelvic fractures: the incidence is increasing and patient demographics can be used to predict the outcome. Eur J Orthop Surg Traumatol. 2014;24(8):1431–1437. doi:10.1007/s00590-014-1439-7
6. Hill RM, Robinson CM, Keating JF. Fractures of the pubic rami: epidemiology and five-year survival. J Bone Joint Surg Br. 2001;83(8):1141–1144. doi:10.1302/0301-620x.83b8.11709
7. Studer P, Suhm N, Zappe B, Bless N, Jakob M. Pubic rami fractures in the elderly - a neglected injury? Swiss Med Wkly. 2013;143:w13859. doi:10.4414/smw.2013.13859
8. Rommens PM, Hopf JC, Herteleer M, Devlieger B, Hofmann A, Wagner DJ. Isolated pubic ramus fractures are serious adverse events for elderly persons: an observational study on 138 patients with fragility fractures of the pelvis type I (FFP Type I). Clin Med. 2020;9(8):2498. doi:10.3390/jcm9082498
9. Loggers SAI, Joosse P, Jan Ponsen K. Outcome of pubic rami fractures with or without concomitant involvement of the posterior ring in elderly patients. Eur J Trauma Emerg Surg. 2019;45(6):1021–1029. doi:10.1007/s00068-018-0971-2
10. Morris RO, Sonibare A, Green DJ, Masud T. Closed pelvic fractures: characteristics and outcomes in older patients admitted to medical and geriatric wards. Postgrad Med J. 2000;76(900):646–650. doi:10.1136/pmj.76.900.646
11. Taillandier J, Langue F, Alemanni M, Taillandier-Heriche E. Mortality and functional outcomes of pelvic insufficiency fractures in older patients. Joint Bone Spine. 2003;70(4):287–289. doi:10.1016/s1297-319x(03)00015-0
12. Lundin N, Huttunen TT, Enocson A, Marcano AI, Felländer-Tsai L, Berg HE. Epidemiology and mortality of pelvic and femur fractures - a nationwide register study of 417,840 fractures in Sweden across 16 years: diverging trends for potentially lethal fractures. Acta Orthop. 2021;92(3):323–328. doi:10.1080/17453674.2021.1878329
13. Osche DB, Liodakis E, Huber S, et al. Fragility Fractures of the pelvic ring: analysis of epidemiology, treatment concepts, and surgical strategies from the Registry of the German Pelvic Multicenter Study Group. J Clin Med. 2025;14(9):2935. doi:10.3390/jcm14092935
14. Abdalmaqsoud H, Sehmisch S, Giannoudis V, Liodakis E. Standard imaging in the ED in geriatric patients with immobilizing pelvic pain after low-energy trauma or without trauma: x-ray vs CT. Injury. 2024;55(3):111294. doi:10.1016/j.injury.2023.111294
15. Royal College of Physicians. National Hip Fracture Database (NHFD) Annual Report 2025: Hip Fracture in 2024 - the Report at a Glance. London: RCP; 2025.
16. Folstein MF, Folstein SE, McHugh PR. “Mini-Mental State” A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198. doi:10.1016/0022-3956(75)90026-6
17. Beloosesky Y, Grinblat J, Epelboym B, Weiss A, Grosman B, Hendel D. Functional gain of Hip fracture patients in different cognitive and functional groups. Clin Rehabil. 2002;16(3):321–328. doi:10.1191/0269215502cr497oa
18. Katz S. Assessing self-maintenance: activities of daily living, mobility and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–727. doi:10.1111/j.1532-5415.1983.tb03391.x
19. Mears SC, Berry DJ. Outcomes of displaced and nondisplaced pelvic and sacral fractures in elderly adults. J Am Geriatr Soc. 2011;59(7):1309–1312. doi:10.1111/j.1532-5415.2011.03455.x
20. Hamilton CB, Harnett JD, Stone NC, Furey AJ. Morbidity and mortality following pelvic ramus fractures in an older Atlantic Canadian cohort. Can J Surg. 2019;62(4):270–274. doi:10.1503/cjs.011518
21. Scheyerer MJ, Osterhoff G, Wehrle S, Wanner GA, Simmen HP, Werner CM. Detection of posterior pelvic injuries in fractures of the pubic rami. Injury. 2012;43(8):1326–1329. doi:10.1016/j.injury.2012.05.016
22. Cosker TD, Ghandour A, Gupta SK, Tayton KJ. Pelvic ramus fractures in the elderly: 50 patients studied with MRI. Acta Orthop. 2005;76(4):513–516. doi:10.1080/17453670510044634
23. Kastanis G, Pantouaki A, Siligardou M-R, et al. Can non displacement osteoporotic pubic rami fracture be life-threatening injuries? A case report, overview, and algorithm protocol for management. J Investig Med High Impact Case Rep. 2024;12:23247096241231648. doi:10.1177/23247096241231648
24. Solarz MK, Kistler JM, Rehman S. Obturator artery injury resulting in massive hemorrhage from a low-energy pubic ramus fracture. Orthopedics. 2017;40(3):E546–548. doi:10.3928/01477447-20161229-03
25. Ten Broek RP, Bezemer J, Timmer FA, Mollen RM, Boekhoudt FD. Massive haemorrhage following minimally displaced pubic ramus fractures. Eur J Trauma Emerg Surg. 2014;40(3):323–330. doi:10.1007/s00068-013-0361-8
26. Rich C, Rayner J, Raukar N. Nondisplaced pubic ramus fracture associated with exsanguination and death. Am J Emerg Med. 2018;36(2):342.e1–342.e2. doi:10.1016/j.ajem.2017.10.062
27. Garrido-Gómez J, Pena-Rodríguez C, Martín-Noguerol T, Hernández-Cortes P. Corona mortis artery avulsion due to a stable pubic ramus fracture. Orthopedics. 2012;35(1):e80–82. doi:10.3928/01477447-20111122-25
28. van Dijk WA, Poeze M, van Helden SH, Brink PR, Verbruggen JP. Ten-year mortality among hospitalised patients with fractures of the pubic rami. Injury. 2010;41(4):411–414. doi:10.1016/j.injury.2009.12.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.