Back to Journals » Patient Preference and Adherence » Volume 17
Comparison of Postoperative Pain After the Utilization of Different File Systems in Single Visit Endodontics
Authors Bhardwaj A, Gupta RK, Ates AA, Wahjuningrum DA ![]() , Arıcan B
, Arıcan B ![]() , AlOmari T
, AlOmari T ![]() , Luke AM
, Luke AM ![]() , Pawar AM
, Pawar AM ![]()
Received 23 January 2023
Accepted for publication 30 March 2023
Published 15 April 2023 Volume 2023:17 Pages 1025—1034
DOI https://doi.org/10.2147/PPA.S405723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Anuj Bhardwaj,1,2 Rudra Kumar Gupta,1 Ayfer Atav Ates,3 Dian Agustin Wahjuningrum,2 Burçin Arıcan,4 Taher AlOmari,5 Alexander Maniangat Luke,6,7 Ajinkya M Pawar2,8
1Department of Conservative Dentistry and Endodontics, College of Dental Science and Hospital, Indore, India; 2Department of Conservative Dentistry, Universitas Airlangga, Surabaya, Indonesia; 3Department of Endodontics, Istinye University, Faculty of Dentistry, Istanbul, Turkey; 4Department of Endodontics, Bahçeşehir University, School of Dental Medicine, Istanbul, Turkey; 5Department of Conservative Dentistry, Jordan University of Science and Technology, Al-Ramtha, Jordan; 6Department of Clinical Science, College of Dentistry, Ajman University, Ajman, United Arab Emirates; 7Center of Medical and Bio-allied Health Sciences Research, Ajman University, Ajman, United Arab Emirates; 8Department of Conservative Dentistry and Endodontics, Nair Hospital Dental College, Mumbai, 400008, India
Correspondence: Dian Agustin Wahjuningrum, Department of Conservative Dentistry, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, 60132, Indonesia, Email [email protected] Alexander Maniangat Luke, Department of Clinical Science, College of Dentistry, Ajman University, J1 Building C Block, Al-Jurf 346, Ajman, United Arab Emirates, Email [email protected]
Purpose: This prospective single-blind, parallel-group, randomized clinical trial was aimed to compare the effect of three different rotary instrumentation systems ProTaper Next (PTN), Self-Adjusting File (SAF) and XP-endo Shaper (XPS) on postoperative pain and analgesic intakes.
Patients and Methods: A total of 159 molars diagnosed with symptomatic irreversible pulpitis were randomly divided into three study groups according to the instrumentation techniques: PTN (n = 54), SAF (n = 52), and XPS (n = 53). The preoperative pain scores were taken before the onset of treatment in the groups. After a single appointment for root canal treatment, the patients were asked to rate the level of their pain according to the Visual Analog Scale (VAS) of 100 mm at 6, 24, 48, and 72-hour post-treatment intervals. Ibuprofen was prescribed to be taken while experiencing pain; patients were requested to note the number of pills consumed at intervals after treatment.
Results: The patients in SAF and XPS groups had lower mean VAS scores than the PTN group at 24-, 48-, and 72-hour intervals (p < 0.05). The most common analgesic intake was optimally seen in the PTN group at a 6-hour interval. All shaping procedures caused postoperative pain, whose intensity decreased with time.
Conclusion: The SAF and XPS groups had a lesser intensity of pain as well as minimum analgesic intakes as compared to the PTN group. All instrumentation systems moderately caused pain, and the PTN group experienced the highest pain among others.
Keywords: postoperative pain, ProTaper next, randomized clinical trial, root canal treatment, XP-endo shaper, patient satisfaction
Introduction
Postoperative pain following root canal treatment has been defined as pain of any degree that occurs after the commencement of root canal therapy.1 The causative factors of postoperative pain include the utilization of different motion kinematics, apical preparation sizes, number of visits and obturation techniques, extrusion of debris and irrigants, trauma to periapical tissue, tissue inflammation, and pre-operative conditions.2–6 Instrumentation of root canals with rotary file systems also plays a key role in root canal treatment by reducing the number of microorganisms and by cleaning canal walls mechanically, thereby resulting in the formation of debris.2 During this therapy, the periradicular tissues may get irritated and cause postoperative pain. Although modern root-canal treatment utilizes many different file systems according to availability in the market and clinician preference, postoperative pain may still occur.
The ProTaper Next (PTN) is a sequenced system introduced by Dentsply (Dentsply Maillefer, Ballaigues, Switzerland) with rectangular cross-section, offset design, and continuous rotation as well as snake-like swaggering movement, which helps auger out of debris coronally.7
The Self-Adjusting file (SAF) (ReDent Nova, Ra’anana, Israel) is a root canal preparation system that has the advantage of in-built irrigation with anatomic instrumentation. The nickel-titanium (Ni-Ti) hollow cylindrical meshwork of the SAF helps adapt to the root canal anatomy8 in three dimensions and causes low micro-cracks and extrusion of debris.9,10
XP-endo Shaper (XPS) (FKG Dentaire, La Chaux-de-Fonds, Switzerland) is another anatomical file developed to maximize the efficacy of cleaning the root canal system. Previous studies claim that the XPS file addresses more surface area of root canal walls than the PTN one.11 It is said to cause higher intracanal bacterial reduction than Reciproc,12 which impacts postoperative pain.13
In the literature search, there is a dearth of clinical evidence comparing postoperative pain after root canal preparation between using single file systems such as XPS and SAF and multiple file systems such as PTN. The null hypothesis stated that there was no difference in postoperative pain and analgesic intakes after root canal preparation in the three studied groups. With the background of root canal treatment concerns, this study aimed to compare postoperative pain after the use of different file systems in the single-visit endodontic treatment of maxillary and mandibular molars with symptomatic irreversible pulpitis. The null hypothesis anticipated was that there would be no variation in postoperative pain and analgesic intakes across groups.
Materials and Methods
Participant Selection and Allocation
This study completely complied with ethical principles, including the World Medical Association Declaration of Helsinki and the revised Consolidated Standards of Reporting Trials statement. This study was designed as a prospective, parallel, single-blind, single-center, and randomized clinical trial. It was independently reviewed and approved by Institutional Ethical Committee of College of Dental Science & Hospital (CDSH/IEC/2019-2020/006) and registered in CLINICAL TRIALS REGISTRY-INDIA (CTRI/2020/02/023339).
Sample size calculation revealed that 40 patients per group14 were selected at a significance level of 0.05 with a power of 80%. To ensure representative sampling and compensation of the participant loss for follow-ups, 159 patients, with more than 50 cases per instrumentation system, were enrolled in the study (Figure 1).
 |
Figure 1 The PRIRATE 2020 flowchart. |
Patients with percussion pain and spontaneous pain scores less than 56 mm on VAS were included. Both permanent maxillary and mandibular first molars were examined. Patients diagnosed with symptomatic irreversible pulpitis and matured roots were included. The pulp sensibility was confirmed using a cold test with Endo-Ice (1,1,1,2 tetrafluoroethane; Hygenic Corp, Akron, OH).
This study excluded patients with non-vital teeth and cases of endodontic retreatment, third molars, teeth with the periapical radiolucent lesion, root resorption, immature/open apex, root caries, and gross decay which could not be restorable with composite filling (need indirect restoration like inlay, onlay or crown), mobile, and having complex anatomy.
The exclusion criteria were also applied to patients using some type of medication preoperatively such as analgesics or nonsteroidal or steroidal anti-inflammatory drugs in the last 12 hours, pregnant and breastfeeding patients, patients with any uncontrolled systemic disease, and patients aged < 18 and > 65 years. Computer-assisted blocks of ten prepared by the statisticians were used for randomization.
Participant Selection and Allocation
Patients were first asked to give verbal consent and then written informed consent. All the procedures were performed by a single skilled operator (a specialist in endodontics with more than ten years of experience and training in using the tested files). Before the commencement of this trial, a standardization protocol was carried out by the operators. Only one local anesthesia (2% lidocaine 1:80,000 epinephrine) (Lidayn) (Dr. DENTAIDS, Kolkata, India) was administered. For mandibular molars, inferior alveolar nerve block technique and a buccal infiltration anaesthesia were performed and for maxillary molars, buccal local infiltration and palatal injection were performed. Patients who needed a second anesthesia or supplemental anesthesia like pulpal, intraosseous and intraligamenter were not selected for further examination. Following the rubber dam application, a traditional access cavity was prepared. To standardize the samples for maxillary and mandibular molars, exploration was attempted to locate the mesio-buccal-2 (MB2), mid-mesial under magnification, illumination, and tactile perception techniques. If any were discovered or even an orifical catch was felt, they were excluded from the research as Pain may linger if this canal is not fully located and instrumented till the apex. The entire procedure was performed under a dental operating microscope (OPMI PICO; Carl Zeiss, Göttingen, Germany). Following the opening of the pulp chamber, the occurrence of bleeding, which is an indicator of pulp vitality, was observed, and only cases with bleeding were included in the study. The patency was checked with # 10 C-pilot files. The working length (WL) was determined using an apex locator (Root ZX II; J.Morita, Tokyo, Japan) and was then confirmed radiographically. The glide path was created with ProGlider® (DentsplyMaillefer, Ballaigues, Switzerland), ProFile® (Dentsply Tulsa Dental Specialties, USA) and ScoutRace (FKG Dentaire, La Chaux-de-Fonds, Switzerland) files according to the manufacturer recommendations for PTN, SAF, and XPS, respectively.
For the preparation of root canals, the tip size of a master apical file for PTN was standardized as follows: (1) #25-#30 (X3) for mesiobuccal and distobuccal root canals on maxillary molars and mesiobuccal and mesiolingual root canals on mandibular molars; (2) #40 (X4) for distal root canals on mandibular molars and palatal root canals on maxillary molars. For SAF, a 1.5 mm apical file was used for narrow and curved canals, and 2 mm was used for larger canals. For XPS, a single file #30/04 was used for all root canals, ascribed to its wide-ranging anatomic adaptability. The root canals were irrigated with 2 mL 2.5% sodium hypochlorite (NaOCl) (Rankem, Avantor Performance Materials India Limited, Gurugram, India) after each file change in the PTN group and after every 15 strokes all along the root canals in the XPS group. The PTN and XPS groups were driven by an electric endo motor DentaPort ZX OTR (Morita, Osaka, Japan). The SAF group was driven by X-SMARTTM (Dentsply Maillefer, Ballaigues, Switzerland) using an RDT3 handpiece. Torque limits and rotation speed for these file systems were strictly set individually as per the manufacturer’s instructions.
For final irrigation, some protocols ie, administration of 5mL 2.5% NaOCl, 5mL 17% ethylene-diamine-tetra-acetic acid (EDTA) (Kerr Corporation, Orange, CA) were given to each group for one minute. The root canals were flushed with saline between these irrigants. A final flush was done with 0.9% saline solution.
The master cone was confirmed radiographically. Obturation was completed using the lateral compaction method with AH-plus sealer (Dentsply Maillefer, Ballaigues, Switzerland) at the same visit. Post-endodontic composite (3M ESPE FiltekTM Z350 XT) restoration was done, and the occlusal contacts were checked in this appointment.
The primary outcome was the intensity of postoperative pain that was measured using a visual analog scale (VAS) at 6-, 24-, 48-, and 72-hour intervals. A VAS sheet (ranging from 0–100 mm) was given to all the patients to answer the outcome assessor during the postoperative questionnaire. The intensity of the pain (primary outcome) was classified into four categories: no pain (level A, 0–24 mm), mild pain (level B, 25–49 mm), moderate pain (level C, 50–74 mm), and severe pain (level D, 75–100 mm). The visual scale was explained by the operator verbally and numerically to facilitate its substantial use by the patients. The patients were called via phone during the intervals and then asked to fill the postoperative pain section with the assistance of a blinded outcome assessor. After 72 hours of observing the postoperative pain, a control appointment was created for them. The patients were instructed to fill in the VAS score section by choosing a level of pain out of the four categories.
The secondary outcome was the number of analgesic tablets taken by the patients at each interval. All patients were instructed to take Ibuprofen (400 mg) when experiencing pain and to record the number of tablets taken at each interval.
Statistical Analysis
R Studio (Open-source analytical tool V 1.2.335) was used to carry out the statistical analysis. A one-way ANOVA test was applied to find a significant difference between the mean VAS scores followed by a post hoc Tukey’s test to compare the individual group. The association between the frequency of analgesic intake and the types of systems was determined using the Chi-square test. The pre- and post-comparisons of mean VAS scores at different intervals were calculated by using a paired t-test.
The Student’s t-test was applied to analyze the comparison of mean VAS scores between mandibular molars and maxillary molars of all the systems taken together at all intervals. The one-way ANOVA followed by the post hoc Tukey’s test was applied to compare the mean VAS scores of mandibular molars as well as maxillary molars separately among the groups with a p-value of <0.05 being considered significant.
Results
A total of 200 patients aged between 18 and 65 years and attending the Dentistry Faculty on February 14, 2020, to March 17, 2020, were screened to select research participants (Figure 1). Out of these patients, 159 patients were enrolled in the study. Nine patients did not report when followed up. A total of 150 were available for the final analysis divided into three groups with 50 patients each (Figure 1). The operators documented case history sheets, covering baseline parameters such as age, gender, medical history, pulp sensibility status of the tooth, and pre-instrumentation pain scores [using a visual analog scale (VAS) of 0–100 mm] (Table 1).
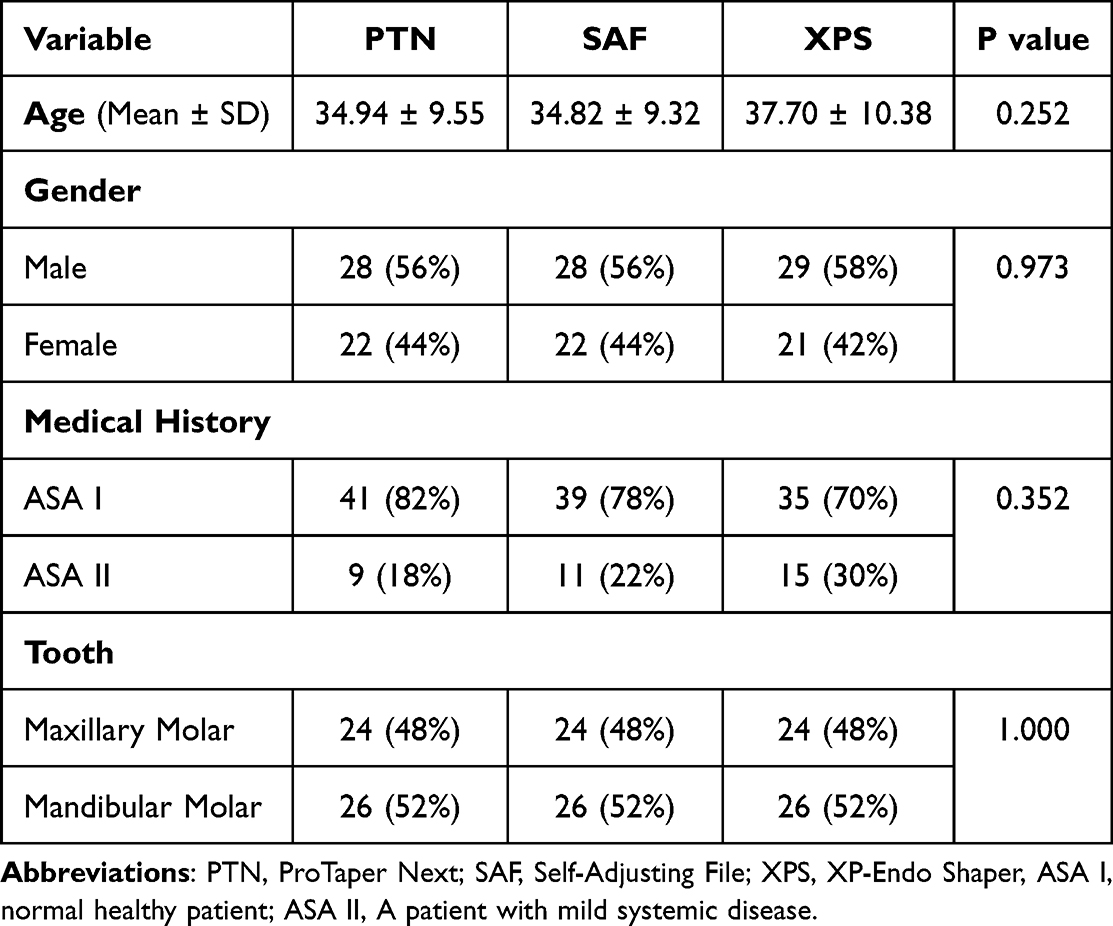 |
Table 1 Baseline Demographic and Clinical Features of Patients in the Study Groups |
The demographic and clinical baselines of patients are shown in Table 1. There was no statistical difference between mean age, gender distribution, medical history, and tooth type (p > 0.05). This study found that 47.4% of mandibular molars were given analgesics, and so were 38.9% of all maxillary molars. Of all male patients, 42.4% consumed analgesic doses, and so did 44.6% of female patients.
The overall mean VAS scores between the study groups at different intervals are shown in Table 2.
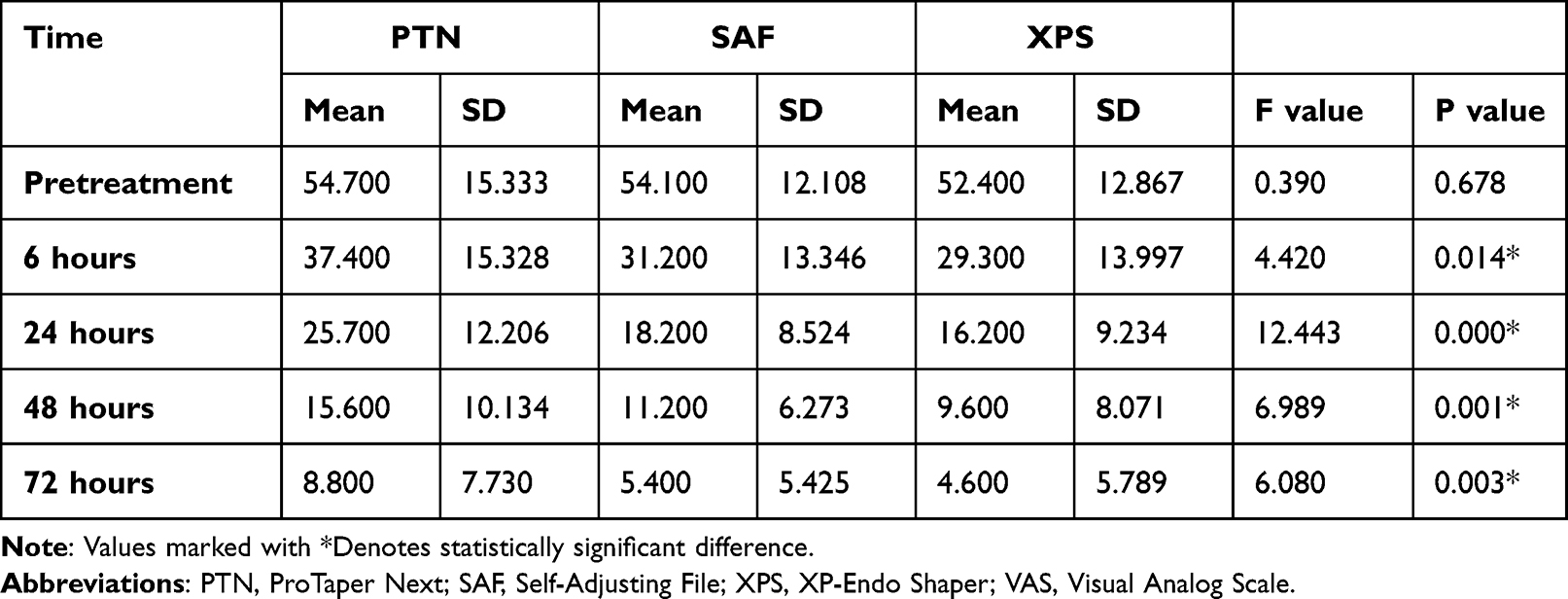 |
Table 2 Comparison of Mean VAS Scores (Primary Outcome) of the Study Groups at Different Time Points |
Primary Outcome
The Intensity of Pain by Mean VAS Scores
The mean VAS scores of all examined groups reduced significantly (p < 0.05), and a continuous declining trend was observed (Figure 2).
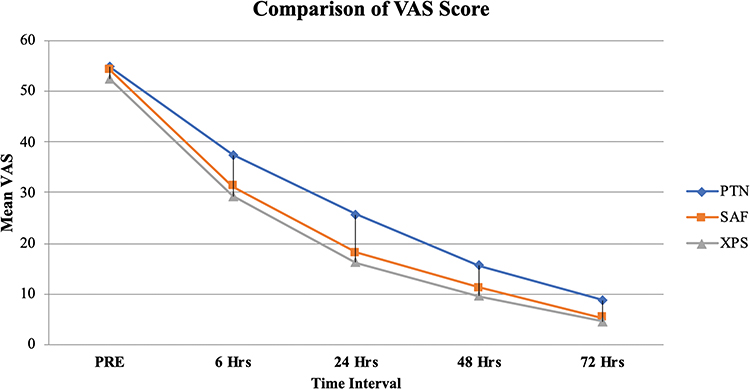 |
Figure 2 Means plot of pain over different time points. Abbreviations: PRE, Pretreatment; PTN, ProTaper Next; SAF, Self-Adjusting File; XPS, XP-Endo Shaper; Hrs, Hours; VAS, Visual Analog Scale. |
Six hours after the treatment, the mean VAS score of the PTN group was found to be significantly higher than that of the XPS group. However, there was no significant difference in mean VAS scores between the SAF group and both PTN and XPS groups.
At 24-, 48-, and 72-hour intervals, the mean VAS score of the PTN group was higher than those of the SAF and XPS groups (p < 0.05). Whereas there was no significant difference in mean VAS scores between SAF and XPS groups (p > 0.05).
Regarding the mean VAS scores by tooth type, a significant difference was only observed in maxillary molars at a 48-hour interval (p < 0.05).
The Intensity of the Pain (Mild, Moderate, and Severe Levels)
Levels of pain experienced by the patients are depicted in Figure 3. At all intervals, the highest percentage of patients who experienced no pain (level A) was observed in the XPS group followed by SAF and then PTN.
 |
Figure 3 The percentage of patients of the study groups with various levels of postoperative pain. Abbreviations: PTN, ProTaper Next; SAF, Self-Adjusting File; XPS, XP-Endo Shaper. |
Secondary Outcome
Intake of Analgesics
The analgesic consumption by patients in each group is presented in Table 3. Ninety-nine analgesics were used by 60 patients within 72 hours after treatment (within 6 hours = 43.3%; 24 hours = 15.3%; within 48 hours = 6.7%; and within 72 hours = 0.7%). Ninety patients did not take analgesics.
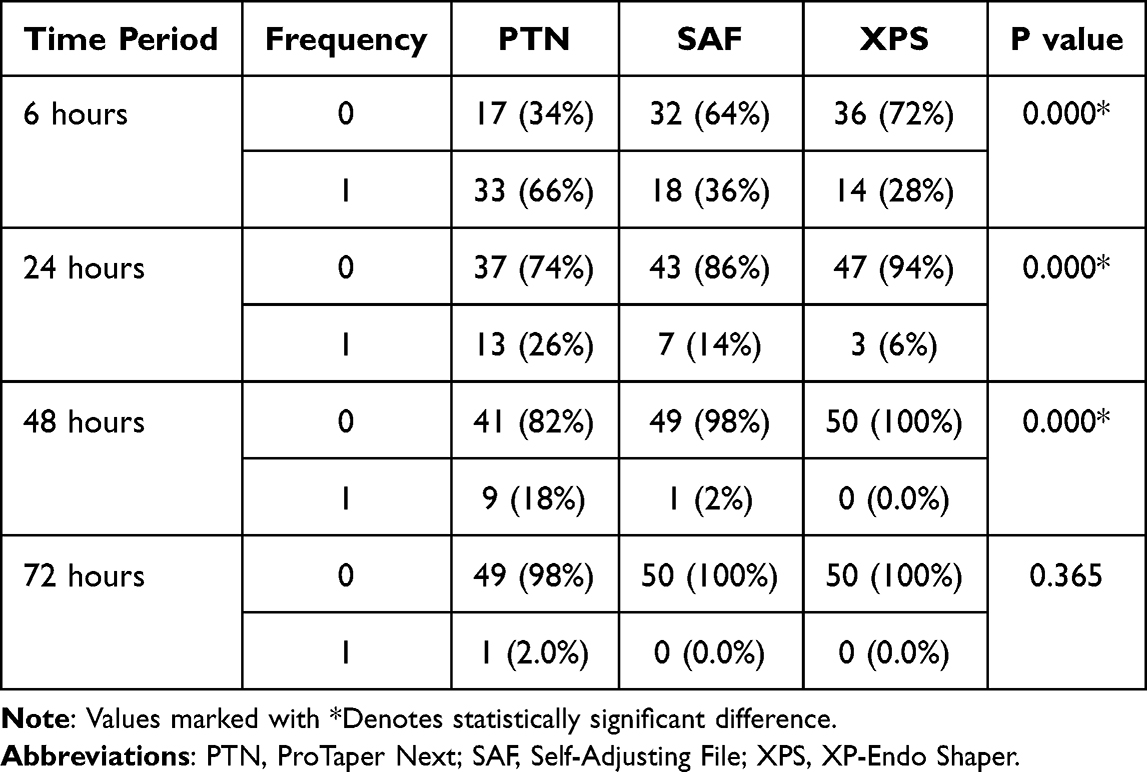 |
Table 3 Analgesic Intake (Secondary Outcome) After Completion of Treatment at Various Time Points |
In the XPS group, the number of patients who took analgesics was significantly lower than in the PTN group (p <0.05).
Discussion
Studies on endodontic postoperative pain are important because they offer important information on how to manage and avoid postoperative pain during endodontic therapy. Interestingly, studies on endodontic postoperative pain might assist clinicians in creating efficient plans for the avoidance and treatment of postoperative pain. Clinicians can create treatment regimens that reduce patient suffering and enhance treatment results by studying the variables that contribute to postoperative pain. Preoperative pharmaceutical usage, improved anaesthetic methods, and postoperative pain control procedures might all fall under this category.
This study aimed to compare the intensity of postoperative pain after a single-visit root canal treatment of molar teeth using PTN, SAF, and XPS for patients with symptomatic irreversible pulpitis. Pain is a personal and subjective experience, and the etiology of postoperative pain is very complex. Technical problems (extrusion of debris, irrigants or obturation materials, and over-preparation) as well as host-dependent factors can cause postoperative pain.15 Demographic characteristics such as age, gender, and geographical regions are important factors that affect pain.16–18 In this study, there was no statistical difference in demographic characteristics between the groups. According to the current results, there was a significant difference in mean VAS scores and the consumption of ibuprofen in the instrumentation systems. Compared to XPS and SAF, patients treated with PTN had more pain at each interval. Different consumption of analgesic intake made a significant difference between the three groups at the intervals, except at a 72-hour interval. At this maximum interval, XPS significantly caused less postoperative pain, and PTN caused the highest pain. In light of these results, the null hypothesis was rejected.
The quantity of extruded debris after the use of PTN was compared with that after the SAF was given. Such procedures were also done by Pawar et al.13 Kfir et al19 and Ozsu et al.20 These studies concluded that SAF had statistically less debris extrusion than PTN. Boijink et al21 also show that the reduced number of files was related to less extrusion of debris. Adiguzel et al22 report that XPS caused less postoperative pain than iRace (FKG Dentaire SA) and Reciproc Blue (REC Blue; VDW, Munich, Germany) at 24-hour and 48-hour intervals. When taking the current results and previous research into consideration, single file systems (XPS and SAF) cause less post-operative pain than PTN. These two file systems are single anatomical files that can adapt to root canal walls tri-dimensionally. This could be a possible reason for the results.
In the present study, the patients were advised to use Ibuprofen when experiencing postoperative pain. Ibuprofen is the first-choice nonsteroidal anti-inflammatory drug to control postoperative pain after root canal treatments. Previous studies also suggest a similar treatment to release postoperative pain.2,5
All the cases were followed up during the first 72 hours. The greatest pain and Ibuprofen intake in all groups occurred in the first six hours (58%). The mean VAS scores in all the study groups reduced significantly (p < 0.05), and a continuous declining trend was observed (Figure 2). The current findings accord with previous research conducted by Ng et al.23 They investigated the prevalence of postoperative pain after the obturation of the root canal with different variables. Their study demonstrates that 58.2% of the patients who had single-visit root canal treatment had postoperative pain within 48 hours. In the present study, only 64.67% of all tested groups experienced postoperative pain within 48 hours. The possible reason for this discrepancy could be due to different patient populations, operators’ skills, and the spectrum of VAS. In the present study, all root canal treatments were done by two endodontists. In addition, VAS of 0–100 mm was used because of its confirmed reliability.24 The main reason for choosing this large scale was to provide the patients with a scale that would score even the slightest discomfort.25
Glennon et al26 indicated that postoperative pain level was higher in molar teeth than in anterior and premolar teeth. It might be attributed to the increased number of canals and the complexities of canal anatomy.27 Most of the studies reported that the presence of periapical lesions acts as a buffer against the exudate created as an inflammatory response to mechanical and chemical injuries.23,28,29 Ng et al23 showed that patients with a periapical lesion, which had a size of more than 3 mm, had less postoperative pain compared to those who had a smaller lesion size or without lesions. Thus, in this study, only vital molar teeth without periapical lesions were included.
Concerning postoperative pain, the mandibular molar group had higher postoperative pain scores and analgesic intake than the maxillary molars. These results are similar to a previous study, which explains the difference between spongy bone structure and better blood supply of the maxilla to help in healing.26 In this study, as in previous other studies,30,31 postoperative pain was observed more in women than men at 24-hour and 72-hour intervals. It may be related to women’s low tolerance to pain and different hormone levels such as serotonin, nor-adrenaline, and estrogen between genders.30–32
The focus of the present study was to evaluate and compare both single and sequenced file systems whether to cause postoperative pain. To reduce clinical conditions, both mandibular and maxillary molars were included. Also, the gender of participants was harmonized among the groups. Participation of the patients in the study was also quantitatively adequate. Only nine participants did not attend the follow-up sessions. None of the patients reported flare-ups. When compared to the PTN group, the pain was less observed with SAF and XPS groups. The possible reason may be attributed to (1) continuous replacement of fresh and activated irrigants; (2) absence of positive pressure as the irrigant easily escaped through openings in the lattice of the file; (3) anatomical shaping of the root canals in SAF group eg, small core size which allows a place for debris to move to the coronal areas of XPS group.
This current study used a randomized allocation of instrumentation systems, calibration of operators to the instrumentation systems, blinded outcome assessor, the time of follow‐up, and the follow-up questionnaire. Furthermore, single-visit treatment was appropriately chosen to eliminate all the potential affecting factors on the appointments and the influence of intracanal medicament.
Performing standardization in clinical studies is challenging due to some limitations that exist in the present study. Considering that pain is subjective, individuals have different pain thresholds. Therefore, various pain experiences may not be used to standardize the VAS scores. Moreover, the difference in the anatomy of teeth alters chairside time, which also affects postoperative pain.32,33 Also, operators performing the treatment were not blindly assigned. Blinding was only applied to patients and outcome assessors. Hence, the present study is not triple-blind. Although all instrumentation systems in this study were able to reduce the intensity of postoperative pain at progressive intervals, XPS and SAF systems significantly caused less postoperative pain and fewer analgesic intakes as compared to PTN. The significance of this study is the clinical acceptability of anatomical shaping by patients with symptomatic irreversible pulpitis in single-visit endodontics. Within the limitations of this study, this result indicates a good way to decrease postoperative pain. To understand, new clinical studies should be done with anatomical shaping files on symptomatic irreversible pulpitis patients with high pain intensity. Moreover, further clinical trials should involve various clinical conditions (eg, non-vital teeth, retreatment cases), and multiple-visit root canal treatment should be carried out to enlighten the potential effects of the instrumentation systems in non-surgical root canal treatment.
Conclusion
The SAF and XPS groups had a lesser intensity of pain as well as minimum analgesic intakes as compared to the PTN group. All instrumentation systems moderately caused pain, and the PTN group experienced the highest pain among others.
Acknowledgments
The authors would like to thank Mrs. Sukla Adhikari, a staff nurse for recording the VAS scores of the research participants via telephone.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sathorn C, Parashos P, Messer H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic review. Int Endod J. 2008;41:91–99. doi:10.1111/j.1365-2591.2007.01316.x
2. Kherlakian D, Cunha RS, Ehrhardt IC, Zuolo ML, Kishen A, da Silveira Bueno CE. Comparison of the incidence of postoperative pain after using 2 reciprocating systems and a continuous rotary system: a prospective randomized clinical trial. J Endod. 2016;42:171–176. doi:10.1016/j.joen.2015.10.011
3. Silva EJ, Menaged K, Ajuz N, Monteiro MR, de Souza Coutinho-Filho T. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis: a prospective and randomized clinical trial. J Endod. 2013;39:173–176. doi:10.1016/j.joen.2012.11.013
4. Singh S, Garg A. Incidence of post-operative pain after single visit and multiple visit root canal treatment: a randomized controlled trial. J Conserv Dent. 2012;15:323–327. doi:10.4103/0972-0707.101888
5. Ates AA, Dumani A, Yoldas O, Unal I. Post-obturation pain following the use of carrier-based system with AH Plus or iRoot SP sealers: a randomized controlled clinical trial. Clin Oral Invest. 2019;23:3053–3061. doi:10.1007/s00784-018-2721-6
6. Bıçakcı H, Çapar İD, Genç S, Ihtiyar A, Sütçü R. Influence of rotary instrumentation with continuous irrigation on pain and neuropeptide release levels: a randomized clinical trial. J Endod. 2016;42:1613–1619. doi:10.1016/j.joen.2016.08.010
7. Burklein S, Mathey D, Schafer E. Shaping ability of ProTaper NEXT and BT-RaCe nickel-titanium instruments in severely curved root canals. Int Endod J. 2015;48(8):774–781. doi:10.1111/iej.12375
8. Metzger Z, Teperovich E, Zary R, Cohen R, Hof R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy-a new concept of endodontic files and its implementation. J Endod. 2010;36:679–690. doi:10.1016/j.joen.2009.12.036
9. Yoldas O, Yilmaz S, Atakan G, Kuden C, Kasan Z. Dentinal microcrack formation during root canal preparations by different NiTi rotary instruments and the self-adjusting file. J Endod. 2012;38:232–235. doi:10.1016/j.joen.2011.10.011
10. De-Deus G, Souza EM, Barino B, et al. The self-adjusting file optimizes debridement quality in oval-shaped root canals. J Endod. 2011;37:701–705. doi:10.1016/j.joen.2011.02.001
11. Öztürk BA, Ateş AA, Fişekçioğlu E. Cone-beam computed tomographic analysis of shaping ability of XP-endo shaper and ProTaper next in large root canals. J Endod. 2020;46:437–443. doi:10.1016/j.joen.2019.11.014
12. Alves FR, Paiva PL, Marceliano-Alves MF, et al. Bacteria and hard tissue debris extrusion and intracanal bacterial reduction promoted by XP-endo Shaper and Reciproc instruments. J Endod. 2018;44:1173–1178. doi:10.1016/j.joen.2018.04.007
13. Pawar AM, Pawar MG, Metzger Z, Kokate SR. The self-adjusting file instrumentation results in less debris extrusion apically when compared to WaveOne and ProTaper NEXT. J Conserv Dent. 2015;18:89–93. doi:10.4103/0972-0707.153057
14. Zand V, Milani AS, HassaniDehkharghani A, Rahbar M, Tehranchi P. Treatment of necrotic teeth using two engine-driven systems and patient’s postoperative pain: a double-blind clinical trial. Iran Endod J. 2016;11:267–272. doi:10.22037/iej.2016.3
15. Siqueira JF. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics. 2005;10:123–147. doi:10.1111/j.1601-1546.2005.00134.x
16. Ali SG, Mulay S, Palekar A, Sejpal D, Joshi A, Gufran H. Prevalence of and factors affecting post-obturation pain following single visit root canal treatment in Indian population: a prospective, randomized clinical trial. Contemp Clin Dent. 2012;3:459–463. doi:10.4103/0976-237X.107440
17. Alí A, Olivieri JG, Duran-Sindreu F, Abella F, Roig M, García-Font M. Influence of preoperative pain intensity on postoperative pain after root canal treatment: a prospective clinical study. J Dent. 2016;45:39–42. doi:10.1016/j.jdent.2015.12.002
18. Sadaf D, Ahmad MZ. Factors associated with postoperative pain in endodontic therapy. International journal of biomedical science. IJBS. 2014;10:243–247.
19. Kfir A, Moza-Levi R, Herteanu M, Weissman A, Wigler R. Apical extrusion of debris during the preparation of oval root canals: a comparative study between a full-sequence SAF system and a rotary file system supplemented by XP-endo finisher file. Clin Oral Invest. 2018;22:707–713. doi:10.1007/s00784-017-2144-9
20. Ozsu D, Karatas E, Arslan H, Topcu MC. Quantitative evaluation of apically extruded debris during root canal instrumentation with ProTaper universal, protaper next, WaveOne, and self-adjusting file systems. Eur J Dent. 2014;8:504–508. doi:10.4103/1305-7456.143633
21. Boijink D, Costa DD, Hoppe CB, Kopper PMP, Grecca FS. Apically extruded debris in curved root canals using the WaveOne Gold reciprocating and Twisted File Adaptive systems. J Endod. 2018;44:1289–1292. doi:10.1016/j.joen.2018.04.011
22. Adiguzel M, Tufenkci P, Pamukcu II. Comparison of postoperative pain intensity following the use of three different instrumentation techniques: a randomized clinical trial. J Dent Res Dent Clin Dent Prospects. 2019;13(2):133. doi:10.15171/joddd.2019.021
23. Ng YL, Glennon J, Setchell D, Gulabivala K. Prevalence of and factors affecting post‐obturation pain in patients undergoing root canal treatment. Int Endod J. 2004;37:381–391. doi:10.1111/j.1365-2591.2004.00820.x
24. Holdgate A, Asha S, Craig J, Thompson J. Comparison of a verbal numeric rating scale with the visual analogue scale for the measurement of acute pain. EmergMed. 2003;15:441–446. doi:10.1046/j.1442-2026.2003.00499.x
25. Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod. 2011;37:429–438. doi:10.1016/j.joen.2010.12.016
26. Glennon JP, Ng Y-L, Setchell DJ, Gulabivala K. Prevalence of and factors affecting postpreparation pain in patients undergoing two-visit root canal treatment. Int Endod J. 2004;37:29–37. doi:10.1111/j.1365-2591.2004.00748.x
27. Shibu TM. Post operative pain in endodontics: a systemic review. J Dent Oral Hyg. 2015;7:130–137. doi:10.5897/JDOH2015.0168
28. Arias A, la Macorra J, Hidalgo J, Azabal M. Predictive models of pain following root canal treatment: a prospective clinical study. Int Endod J. 2013;46:784–793. doi:10.1111/iej.12059
29. Marshall JG, Liesinger AW. Factors associated with endodontic posttreatment pain. J Endod. 1993;19:573–575. doi:10.1016/S0099-2399(06)81290-2
30. Albashaireh Z, Alnegrish A. Postobturation pain after single-and multiple-visit endodontic therapy. A prospective study. J Dent. 1998;26(227–232). doi:10.1016/S0300-5712(97)00006-7
31. Watkins CA, Logan HL, Kirchner HL. Anticipated and experienced pain associated with endodontic therapy. J Am Dent Assoc. 2002;133:45–54. doi:10.14219/jada.archive.2002.0020
32. Segura‐Egea JJ, Cisneros‐Cabello R, Llamas‐Carreras JM, Velasco‐Ortega E. Pain associated with root canal treatment. Int Endod j. 2009;42:614–620. doi:10.1111/j.1365-2591.2009.01562.x
33. Pawar AM, Bhardwaj A, Zanza A, et al. Severity of post-operative pain after instrumentation of root canals by XP-Endo and SAF full sequences compared to manual instrumentation: a randomized clinical trial. J Clin Med. 2022;11:7251. doi:10.3390/jcm11237251
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.