Back to Journals » Clinical Ophthalmology » Volume 15
Comparison of Pain Scores Among Patients Undergoing Conventional and Novel Panretinal Photocoagulation for Diabetic Retinopathy: A Systematic Review
Authors Azarcon CP ![]() , Artiaga JCM
, Artiaga JCM ![]()
Received 30 November 2020
Accepted for publication 11 January 2021
Published 2 March 2021 Volume 2021:15 Pages 953—971
DOI https://doi.org/10.2147/OPTH.S294227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Corrina P Azarcon,1 Jose Carlo M Artiaga2,3
1Department of Ophthalmology and Visual Sciences, Philippine General Hospital, University of the Philippines – Manila, Manila, Philippines; 2International Eye Institute, St. Luke’s Medical Center Global City, Taguig City, Philippines; 3Department of Ophthalmology, Ospital ng Muntinlupa, Muntinlupa City, Philippines
Correspondence: Corrina P Azarcon
Department of Ophthalmology and Visual Sciences, Philippine General Hospital, University of the Philippines – Manila, Manila, Philippines
Email [email protected]
Purpose: To summarize key findings from a systematic review focusing on pain as an adverse outcome of panretinal photocoagulation (PRP) among patients with diabetic retinopathy.
Design: Systematic review.
Methods: We systematically searched articles in major databases from July to September 2020. Studies that compared pain outcomes of PRP among diabetic patients who underwent conventional single-spot laser (SSL), conventional multi-spot laser (MSL), and/or novel navigated laser (NNL) were included. The Cochrane RoB 2 tool and ROBINS-I tool were used to evaluate the risk of bias of the included randomized controlled trials (RCTs) and controlled clinical trials (CCTs), respectively.
Results: We included 13 RCTs and 4 CCTs. Thirteen studies were included for Comparison 1 (Conventional SSL versus Conventional MSL), 3 studies were included for Comparison 2 (NNL versus Conventional MSL), and 3 studies were included for Comparison 3 (NNL versus Conventional SSL). A total of 783 patients and 1961 eyes were included in this review. The review showed that NNL yielded the lowest pain scores, followed by conventional MSL, then by conventional SSL.
Conclusion: This review summarizes findings of multiple studies that reported pain as an adverse outcome of PRP among patients with advanced diabetic retinopathy. Data from RCTs with mostly some concerns for bias (RoB 2 tool) and CCTs with mostly moderate risk of bias (ROBINS-I tool) show benefit of using MSL over SSL, and NNL over conventional systems for PRP in diabetic retinopathy, considering pain as the primary outcome.
Keywords: pain, panretinal photocoagulation, diabetic retinopathy, PASCAL®, NAVILAS®
Introduction
Diabetes mellitus is a global epidemic that affects nearly half a billion people worldwide.1 This disease is a significant health and economic burden, as patients with diabetes are at risk for multiple disabling and life-threatening complications.2,3 Among the most common complications of diabetes is diabetic retinopathy.2 Global estimates in 2010 indicated that around 4.5 million people were visually impaired or blind as a consequence of this condition.4
Diabetic retinopathy is characterized by microvascular damage leading to retinal ischemia, neovascularization, and edema.2,5 The earlier stage, non-proliferative diabetic retinopathy (NPDR), is classified based on the presence and the number of microaneurysms, retinal hemorrhages, intraretinal microvascular abnormalities, and venous beading. The advanced stage, proliferative diabetic retinopathy (PDR), is characterized by preretinal neovascularization.2,6
Panretinal photocoagulation (PRP) has been considered as the standard of care in the management of advanced diabetic retinopathy since its introduction in the late 1970s.7,8 In PRP, laser burns are applied at the retinal periphery using slit lamp or indirect ophthalmoscope-based systems.9 Laser energy is primarily absorbed by melanocytes located at the retinal pigment epithelium layer. The energy, which is converted to heat, causes a localized increase in temperature.10 Local destruction of retinal tissue brought about by the heat decreases oxygen demand and improves oxygenation of the surrounding retina.11 In conventional laser therapy, a total of 1200 to 1600 moderate-intensity burns measuring 200 μm to 500 μm are delivered in 100 to 200 millisecond pulses. The treatment is traditionally administered using single-spot laser (SSL) systems and completed over 2 to 3 sessions.9 The effectiveness of this protocol in prevention of vision loss has been demonstrated in large multicenter trials - the Diabetic Retinopathy Study (DRS) and the Early Treatment Diabetic Retinopathy Study (ETDRS).12,13
Multi-spot lasers (MSL) are semi-automated, fully integrated, slit lamp-based laser systems that can deliver multiple laser spots in a single depression of the foot pedal. Using these machines, ophthalmologists can select and deliver various patterns, shapes, and sizes of laser burns.14 The Pattern Scanning Laser (PASCAL®) photocoagulator (OptiMedica, Inc., Santa Clara, CA, USA) was introduced in 2006. It makes use of a frequency-doubled Neodymium:Yttrium Aluminum Gallium (Nd:YAG) laser to deliver single or multiple shots in arrays, circles, arcs, or lines. The Valon Multispot Laser (Valon Lasers Oy, Vantaa, Finland) is similar with PASCAL® but adds an important function that allows display of the settings over the retinal image. The VISULAS 532s VITE (Carl Zeiss Meditec AG, Jena, Germany) is a 532-nm solid-state photocoagulator that also delivers pre-programmed short-pulse multi-spot patterns on the retina. The NAVILAS® (OD-OS GmbH, Teltow, Germany) is a novel retinal navigation system and laser device that incorporates a digital fundus imaging system to a 532-nm and 577-nm diode pumped solid-state laser (DPSS). The fundus camera generates a large, glare-free image that allows live red-free, infrared, and fluorescein angiography imaging useful for treatment planning.15 Pulse durations of these MSL’s are usually in the 10 to 20 millisecond range, compared to the 100 to 200 millisecond duration used in conventional SSL systems.14 Total treatment times with MSL’s are approximately one-fifth of the time required to complete PRP using conventional SSL.15
One of the undesirable side effects of PRP is pain. With the conventional procedure, Visual Analog Scale (VAS) scores have been reported to range from 37.3 to 53.1 using a 100-millimeter scale.16 Word descriptors included the following: sharp, flashing, pricking, tiring, blinding, intense, annoying, piercing, and nagging.17 Previous reports show that pain may be controlled by adjusting laser parameters, which include wavelength, duration, and fluence.10,14,17 Other factors that may influence pain perception are sex, culture, previous experiences, and anxiety levels.17
Pain is an important undesirable side-effect of any medical intervention. Up to 64.1% of patients are unable to tolerate pain associated with laser therapy.18 Experience of pain may affect compliance to therapy and result to deterioration of vision.15,19–21 In addition, pain may increase the patient’s risk for complications during the procedure if it stimulates sudden movement of the eye.22 Ophthalmologists should employ methods to minimize the amount of pain experienced by their patients during ocular procedures. The use of retrobulbar, peribulbar, and sub-Tenon’s block have been suggested, but these methods pose the patient toadditional risk for complications.10,23 Several drugs, which include oral non-steroidal anti-inflammatory drugs, topical diclofenac, inhalational nitrous oxide, oral diazepam, intramuscular ketorolac tromethamine, have been also described in different studies.10,16,17,23–25 To date, there are no systematic reviews on PRP for diabetic retinopathy that have focused on pain as a primary adverse outcome. This systematic review shall compare pain scores obtained from patients undergoing conventional SSL, conventional MSL (PASCAL®), and novel navigated laser (NNL, NAVILAS®).
Methods
Guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses were followed.26 Randomized clinical trials (RCTs) and controlled clinical trials (CCTs) were included in the study, regardless of the setting and sample size. Trials wherein randomization was not explicitly stated in the text but compared outcomes of the two eyes of one patient using different types of laser on each eye were considered as CCTs. Retrospective studies, observational studies, and reviews were excluded. We intended to include studies comparing pain scores of patients undergoing PRP by conventional SSL, conventional MSL (PASCAL®) and NNL (NAVILAS®). We only included studies involving patients diagnosed with diabetic retinopathy whose condition warranted PRP. Studies focusing on other retinal pathologies were excluded. Reports about focal laser therapy for diabetic macular edema were also excluded, except for studies which separately analyzed and reported data for patients who underwent PRP.
Search Methods
Two authors (CA and JA) independently conducted an electronic search from July to September 2020 using a pre-defined search strategy. No language restrictions were imposed. Search terms included “multi-spot”, “pattern”, “navigated,” “panretinal photocoagulation,” and “pain.” Synonyms, alternate spellings, prefixes, and suffixes were also used. The following databases were searched: MEDLINE, CENTRAL, EMBASE, ClinicalTrials.gov, LILACS, and Herdin.ph. We sought for grey literature in OpenGrey and Google Scholar using similar search terms. Hand-searching was also performed through reference lists of retrieved studies.
Trial Selection
Two authors (CA and JA) independently screened titles and abstracts of the search yield. Differences in assessment were resolved through discussion between the first two authors. A third ophthalmologist served as the arbiter for disagreements. Two authors (CA and JA) selected studies based on the defined inclusion and exclusion criteria.
Outcomes of Interest
Primary outcomes were measured using pain scales which include the visual analog scale (VAS), numerical rating scale (NRS), verbal rating scale (VRS) and other ordinal and continuous arbitrary pain scales for pain. Secondary outcomes included laser parameters (average laser power, average laser fluence, number of laser shots administered) and number of treatment sessions.
Data Collection and Assessment of Trials for Risk of Bias
Data was extracted into a pre-formatted electronic data collection sheet (Microsoft Excel) by the two investigators. All authors of the selected studies were e-mailed for clarifications regarding their protocols and reports. Studies of authors who were not able to respond were evaluated based on published data. The Cochrane RoB 2 tool and the ROBINS-I tool were used to assess the risk of bias of the RCTs and CCTs, respectively.27,28 The robvis tool29 was used to generate the risk of bias plots. Data from the RCTs were encoded into the Review Manager 5.4 software of the Cochrane Collaboration.
Data Synthesis and Analysis
Mean pain scores and standard deviations were extracted for each study. We used Microsoft Excel to calculate for means and standard deviations for studies that provided raw data. For articles that did not provide the standard deviation (SD) but provided the range of the scores, the estimate of the SD was computed using the method described by Walter.30 Results of the RCTs and CCTs were included in the qualitative analysis, with consideration of its risk of bias. Pain scores from RCTs were encoded into the Review Manager 5.4 software for quantitative analysis. Pain scores were treated as continuous outcomes; standardized mean differences (SMD’s) were obtained to account for differences in the pain scales used. Confidence intervals were set at 95%. A random effects model (Mantel-Haenszel) was applied. The p-value cut-off for significance was set at 0.05. Heterogeneity was assessed by individual evaluation of the methodologies and by using the I2 statistic. Sensitivity analysis was done by checking if results and conclusions would change if studies with high or serious risk of bias were removed. Standardized mean differences and ranges were back-transformed to mean differences in the 10-point visual analog scale (VAS) following the method described in the Cochrane Handbook.31 The protocol of this study was registered in PROSPERO (ID: CRD42020203047).
Results
The search process is detailed in Figure 1. Nineteen (19) full-text articles were retrieved for review. Of the 19 papers, a paper by Röckl et al32 was excluded since the population included patients with retinal pathologies other than diabetic retinopathy, and a breakdown of the data was not available. Two reports written by Chhablani et al published in 2014 and 2015 consisted of the same set participants; only the updated article was included in our analysis.33,34 Of the 17 articles remaining, 13 articles were included for Comparison 1 (conventional MSL versus conventional SSL), 3 articles were included for Comparison 2 (NNL and conventional MSL), and 3 articles were included for Comparison 3 (NNL versus conventional SSL). The search did not yield any studies that investigated the use of NNL systems other than NAVILAS®. Table 1 lists the characteristics of included studies. The inclusion and exclusion criteria used in the review are presented in Table 2.
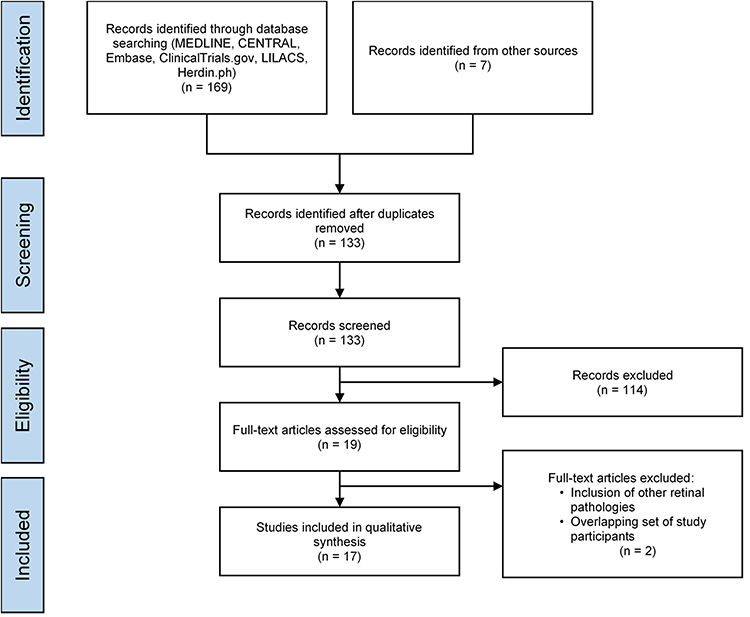 |
Figure 1 Search yield. |
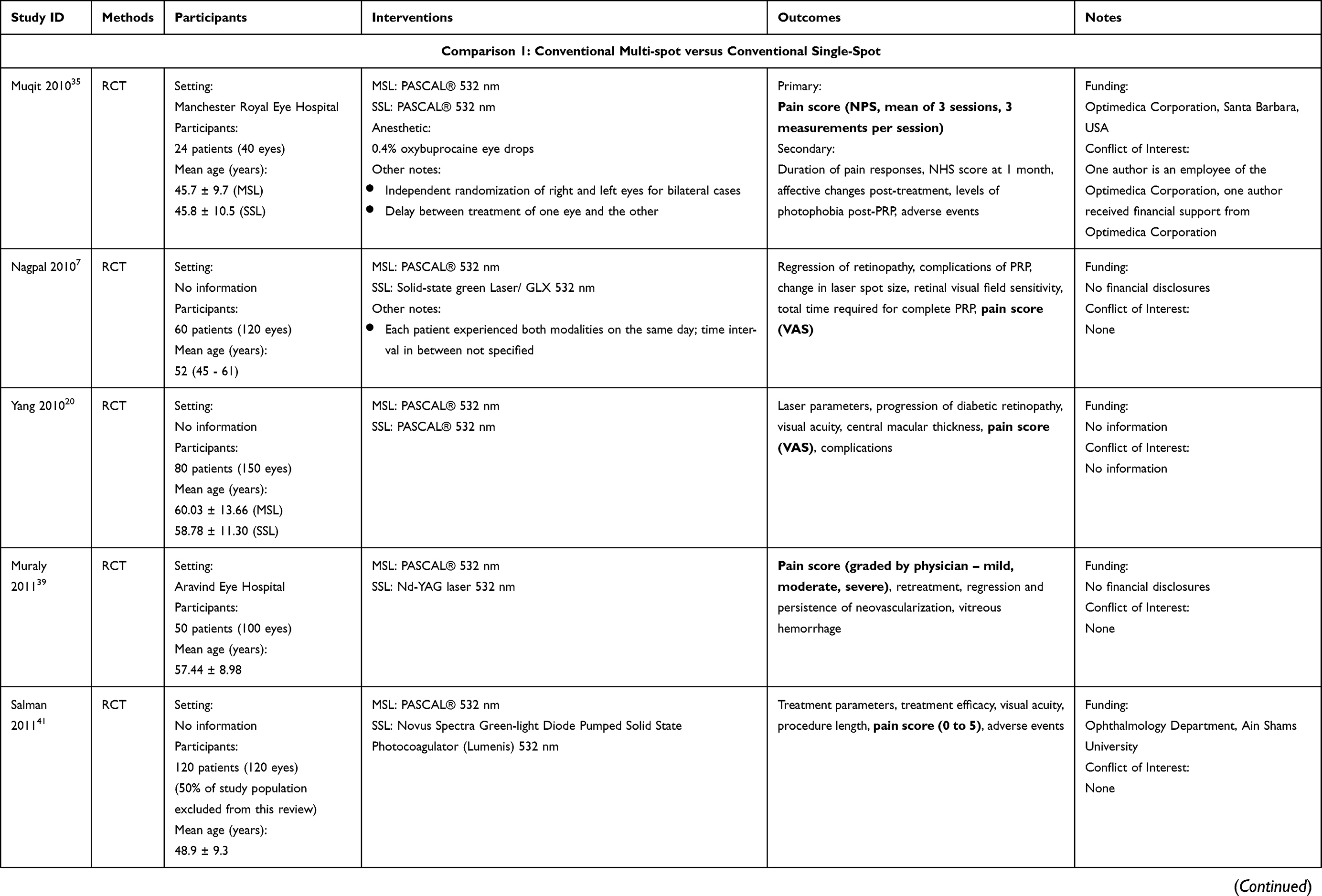 | 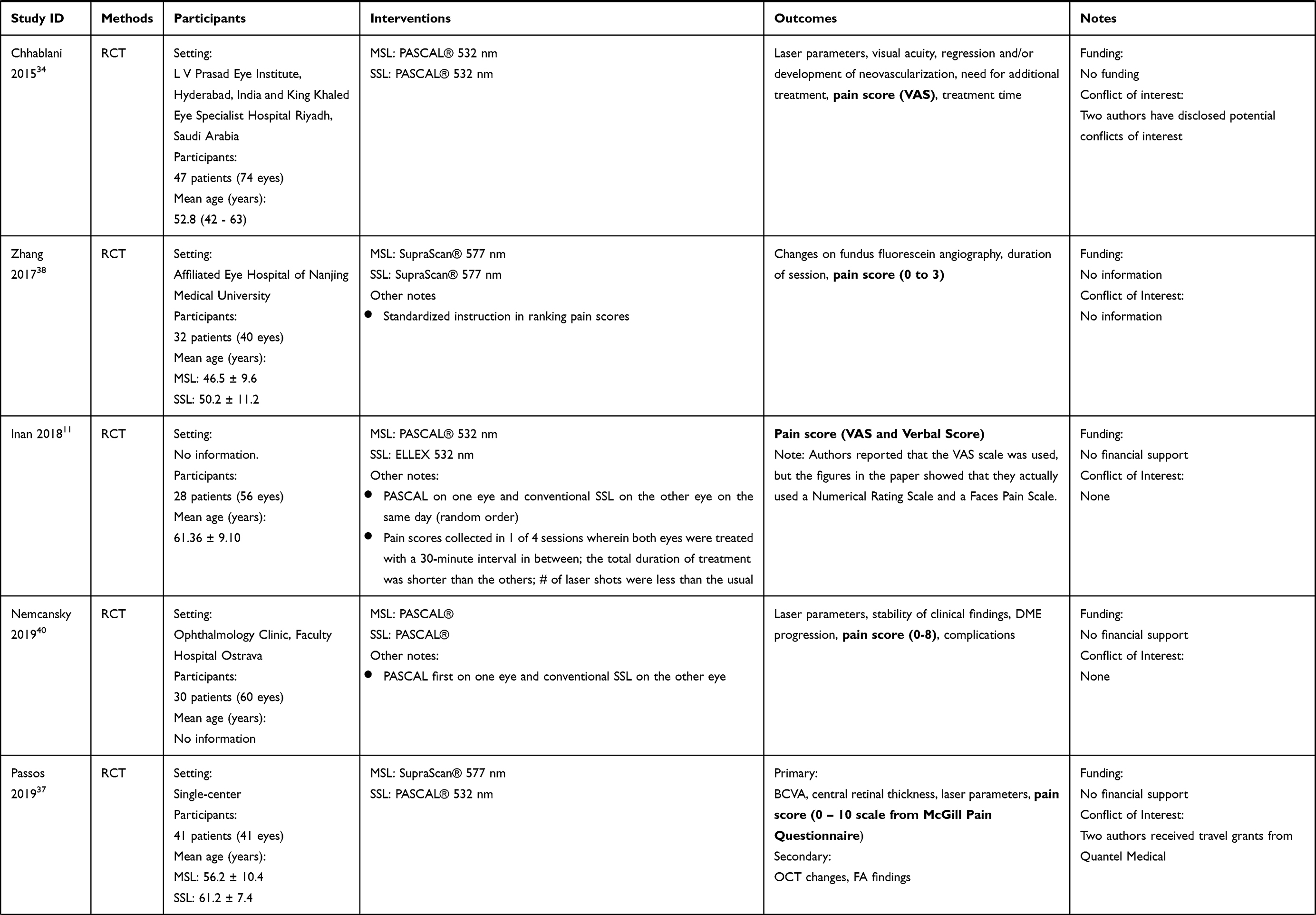 | 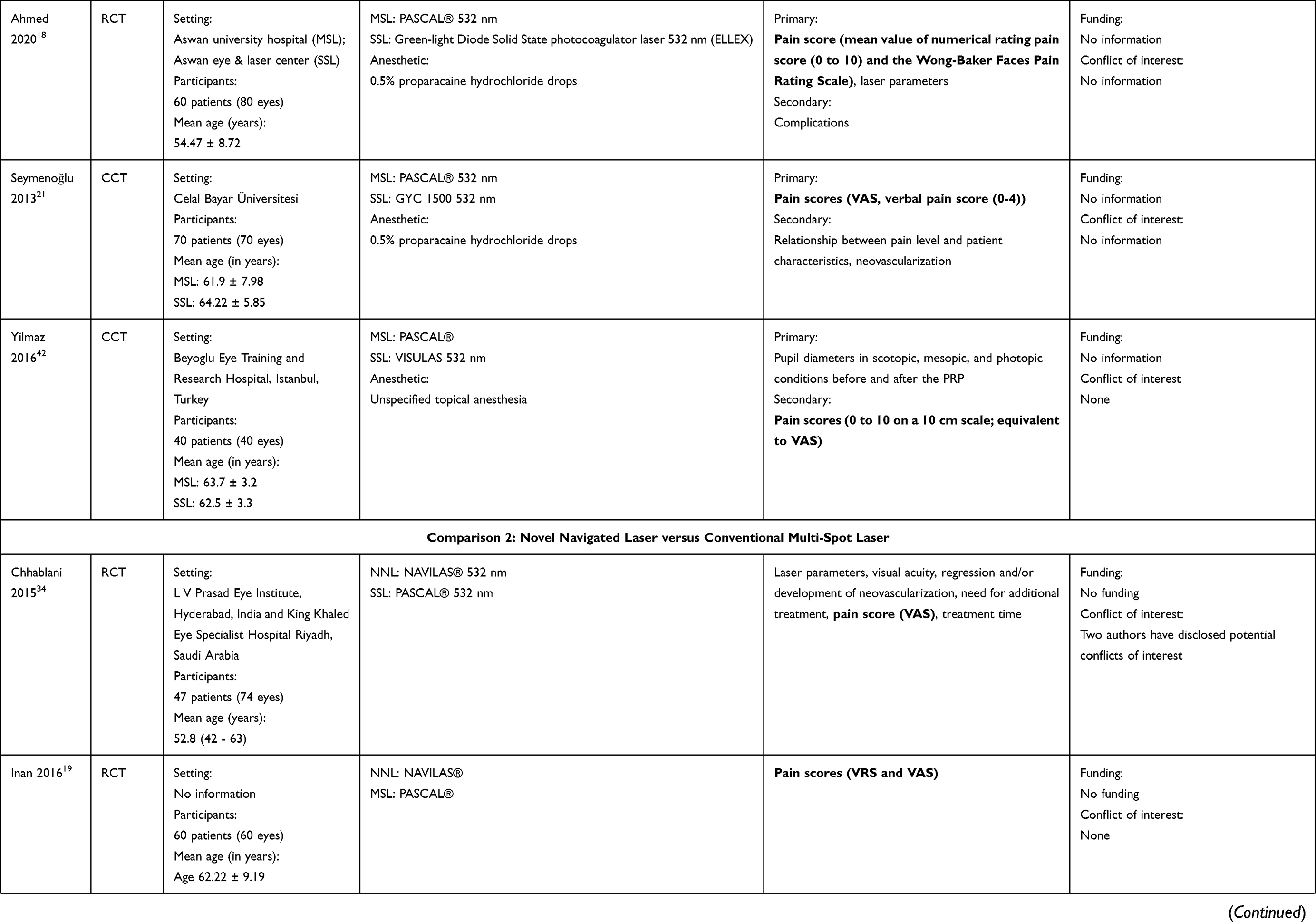 | 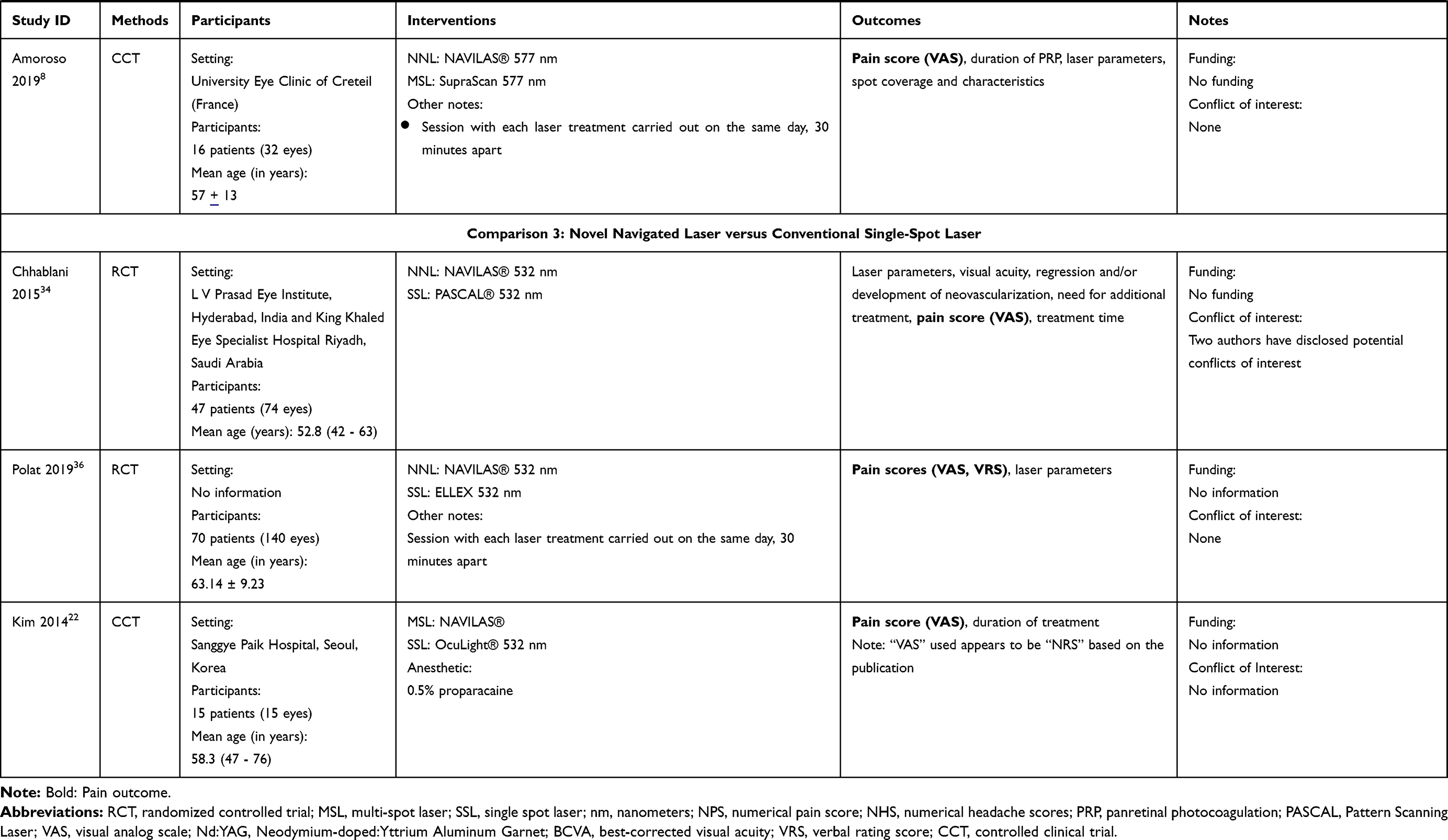 |
Table 1 Characteristics of Included Studies |
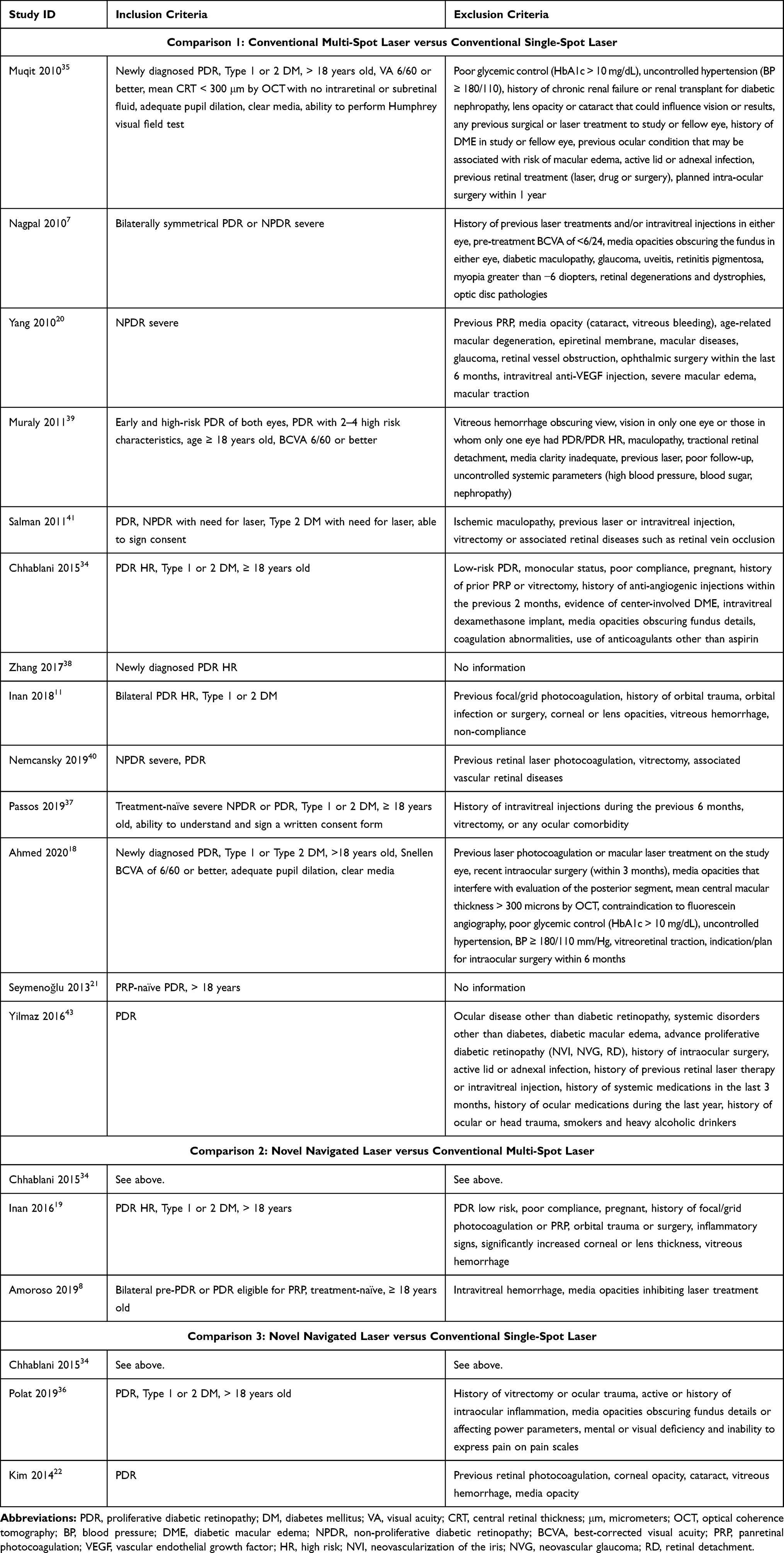 |
Table 2 Inclusion and Exclusion Criteria of Included Studies |
Thirteen of 17 included studies were RCTs, whereas the remaining 4 were CCTs. Majority of the studies were performed in single centers, except for the study of Chhablani et al,34 which was done in 2 hospitals, and the study of Ahmed,18 which was performed in multiple sites from a single center. Six studies studied only 1 eye per patient, 6 studies used the other eye of the patient as a comparison, and 5 studies intervened on a mix of unilateral and bilateral cases. The sample size ranged from 15 to 150 eyes. From the studies that provided the age of participants, Muqit et al35 studied the youngest age group (MSL: 45.8 ± 9.7 years old; SSL: 45.8 ± 10.5 years old) and Polat et al36 studied the oldest age group (63.14 ± 9.23 years old). Majority of the studies utilized 532-nm wavelength for both laser groups. Passos37 compared 577-nm conventional MSL and 532-nm conventional SSL, Zhang38 compared 577-nm conventional MSL and 577-nm conventional SSL; Amoroso8 used 577-nm lasers for both NNL and conventional MSL. Significant differences in laser methodology among patients across all studies were observed. Table 3 summarizes the list of laser machines, settings and parameters used in all included studies.
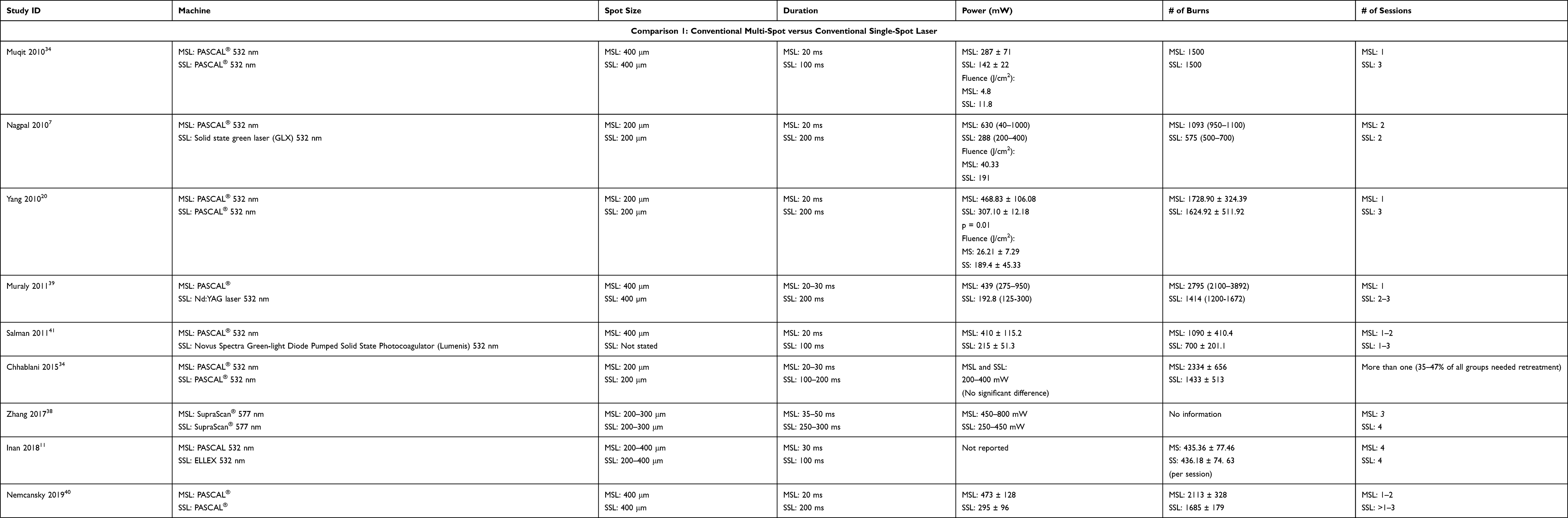 |
Table 3 Laser Parameters in Included Studies |
VAS was the most commonly utilized pain scale; it was used in 10 of the 17 studies included. The report of Muraly et al39 was the only study where pain outcomes were reported by the physician based on observations of the patient’s reactions. Ahmed18 used the mean value of the numerical rating pain score and the Wong-Baker Faces Pain Rating Scale. Nemcansky et al,40 Salman et al,41 and Zhang et al38 used numerical scales with range of 0 to 8, 0 to 5, and 0 to 3, respectively. Muqit et al35 used a Numerical Pain Scale from 0 to 10. Seymenoğlu et al,21 Inan et al,11 Inan et al,19 and Polat et al36 also reported VRS separate from the VAS score. Only the study of Muqit et al35 measured duration of pain and recorded word descriptors for pain.
Risk of Bias of Included RCTs
Figure 2 displays the assessment of the risk of bias of the included RCTs. Only 4 of the 13 included RCTs specified the method of random sequence generation in the methodology. Only 1 study specified the method of allocation concealment and was classified as having low risk of bias arising from the randomization process (Domain 1); the rest were classified as having some concerns of bias in this domain. In the evaluation of bias due to deviations from the intended protocol (Domain 2), the reviewers decided that knowledge of the intervention by the care providers should not result to deviations from the intended protocol, hence all studies were judged as having low risk for bias in this domain. However, we judged the protocol Ahmed et al18 as having some concerns of bias since the SSL and MSL procedures were conducted in different settings. In the assessment of bias due to missing outcome data (Domain 3), majority of the studies were assessed to be at low risk for attrition bias due to the short follow-up period. Complete data was reported in all studies except for the study of Polat et al,36 where pain scores of 8 of 29 patients who underwent PRP using 100-millisecond shots were not reported. In the evaluation of bias in measurement of the outcome (Domain 4), we found serious concerns in the study of Muraly et al,39 where pain outcomes were defined by unmasked physicians who were also performing the laser procedure. The studies of Polat et al,36 Inan et al,11 and Inan et al19 were assessed as having high risk of bias in selection of the reported result (Domain 5) given that the number of laser shots were standardized for the two procedures and were not reflective of usual clinical practice. The reviewers also found high risk of bias in the report of Ahmed et al18 since two different pain scales were averaged. Overall, the reviewers found that only one study had low risk for bias, 4 were at high risk for bias, and the rest had some concerns for bias.
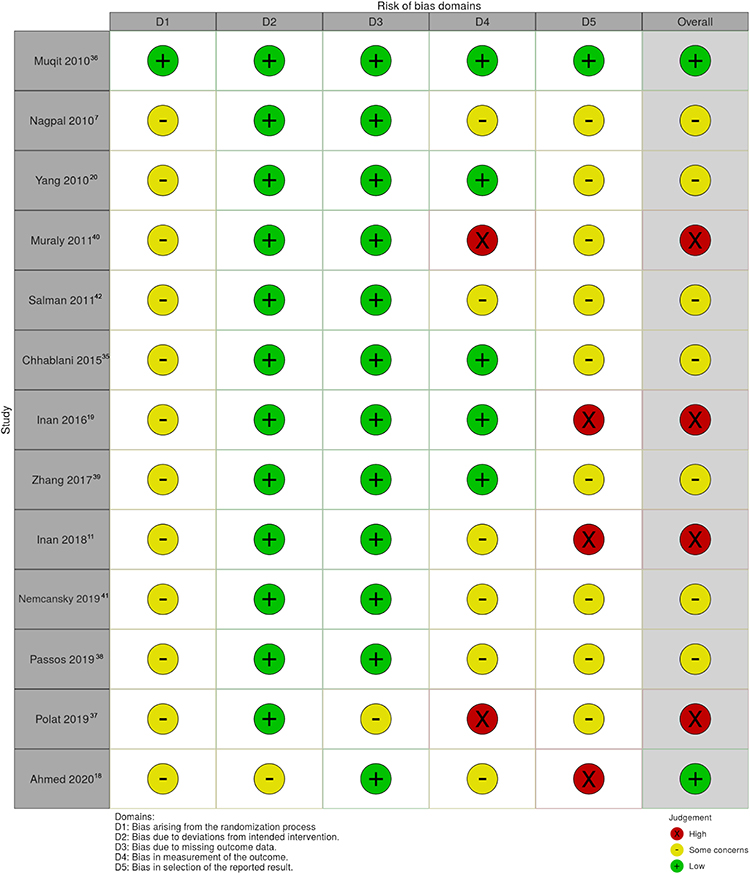 |
Figure 2 Risk of bias assessment of included RCTs. |
Risk of Bias of Included CCTs
Figure 3 shows the assessment of the risk of bias of the included RCTs. In the evaluation of bias due to confounding (Domain 1), the reviewers found serious concerns in the methodology of Kim et al22 where both interventions were performed on the same eye. NNL was used for the superior, nasal, and inferior quadrants during the first session, then conventional SSL was done in the temporal retina a week later. The coverage of a larger area may have resulted to greater ciliary nerve stimulation, thereby causing greater pain. Thus, reported pain scores with NNL may have been falsely higher while scores with conventional laser were falsely lower in this study design. No confounding factors were noted for the other studies. The reviewers did not find significant concerns in the selection of participants (Domain 2), classification of interventions (Domain 3), deviations from intended interventions (Domain 4), missing data (Domain 5), measurement of outcomes (Domain 6), and selection of the reported result (Domain 7). Overall, three CCTs appeared to have low risk of bias, and only the study of Kim et al22 was assessed to have serious risk of bias.
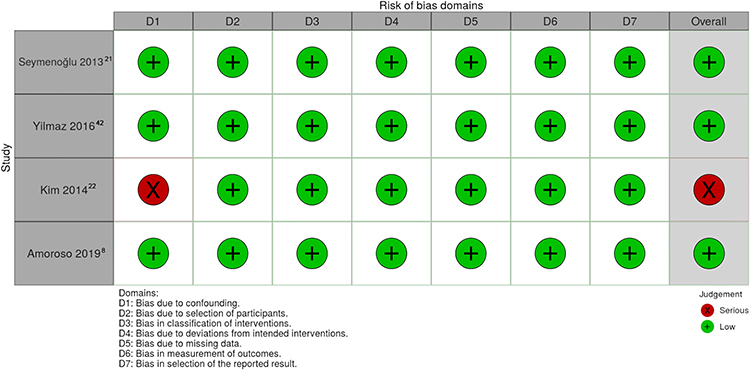 |
Figure 3 Risk of bias assessment of included CCTs. |
Results of the Intervention
Comparison 1: Conventional MSL versus Conventional SSL
Eleven RCTs (Figure 4) and 2 CCTs were included in this comparison. Two groups investigating the effect of laser on macular edema in the study of Salman et al41 were excluded from this review. The reviewers decided not to conduct a meta-analysis since no two studies were sufficiently similar, and this was supported by a large I2 statistic (>96%) when the 11 RCTs are included. As illustrated in the Forest plot for Comparison 1 (Figure 4), all included RCTs favored conventional MSL over conventional SSL in terms of pain. The studies published by Nemcansky et al40 and Passos et al37 crossed the line of no effect. The calculated mean difference of pain scores between the two groups reported across the included studies ranged from 0.5 to 6 VAS points favoring conventional MSL over conventional SSL. No significant changes in the results are found when the results of studies with high risk of bias are removed from the analysis.
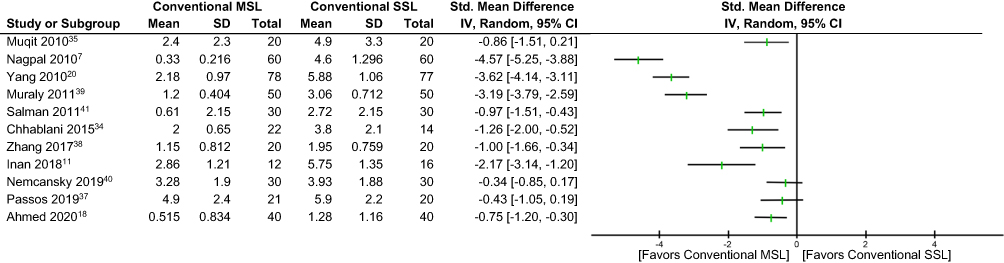 |
Figure 4 Forest plot comparing conventional MSL and conventional SSL. |
Two CCTs likewise favored conventional MSL. Seymenoğlu et al21 conducted a CCT where 35 eyes of 35 patients underwent conventional MSL in 1 session and the same number of eyes underwent conventional SSL in 2 sessions. VAS scores were 2.17 ± 1.18 and 5.54 ± 3.28 for conventional SSL and conventional MSL, respectively. In another CCT by Yilmaz et al42 which studied 40 eyes of 40 patients with diabetic retinopathy, VAS pain scores were 1.7 ± 1.4 versus 5.2 ± 3.0 for conventional MSL and conventional SSL (p = 0.001), respectively.
Comparison 2: NNL versus Conventional MSL
Only two RCTs (Figure 5) and 1 CCT were included for this comparison. For both RCTs shown in Figure 5, pattern NNL appears to be more beneficial compared to conventional MSL in terms of pain, using a pulse duration of 30-ms for both groups. The calculated mean difference of pain scores is equivalent to 0.7 to 2 VAS points favoring NNL over conventional MSL.
 |
Figure 5 Forest plot comparing NNL and conventional MSL (Pulse duration: 30-ms). |
The CCT conducted by Amoroso et al8 also found significantly higher VAS scores among patients who underwent 577-nm pre-planned NNL versus 577-nm conventional MSL, with pulse durations set at 20-ms (2.4 ± 1.6 versus 7.1 ± 2).
Chhablani et al34 also presented data that allows comparison of pain scores among individuals who underwent long-pulse pattern NNL (100-ms) compared to those who underwent conventional MSL (30-ms). The mean VAS score was lower for those who received NNL compared to those who underwent conventional MSL, although the confidence intervals had an overlap (1.5 ± 0.56 versus 2.0 ± 0.65).
Comparison 3: NNL versus Conventional SSL
Two RCTs (Figure 6) and 1 CCT were included for this analysis. All studies in this comparison used the pattern mode of NAVILAS®. The study of Chhablani et al34 found that pain scores were significantly lower for patients who underwent 30-ms NNL compared to scores reported by the 100-ms conventional SSL group (1.00 ± 0.31 versus 3.8 ± 2.10). Furthermore, VAS scores were still lower for the NNL group compared to the conventional SSL group when the NNL pulse duration was set at 100-ms (1.50 ± 0.56 versus 3.8 ± 2.10). The study of Polat et al36 where patients underwent NNL on one eye and conventional SSL on the other eye also found lower pain scores with NNL even when the pulse duration was set at 100-ms for both treatment arms, although this study reported incomplete data. Figure 6 shows the Forest Plot comparing pain scores using long-pulse (100-ms) NNL versus conventional SSL. The computed mean difference of pain scores is equivalent to 1 to 2 VAS points favoring long-pulse NNL over conventional SSL.
 |
Figure 6 Forest plot comparing long-pulse NNL and conventional SSL (pulse duration: 100-ms). |
The CCT of Kim et al22 also showed a significantly higher mean VAS score among patients undergoing conventional SSL versus short-pulse NNL (6.9 ± 1.1 versus 3.3 ± 1.2). Although the study design has a serious risk of bias, the reviewers believe that this bias effectively lowers VAS scores in the conventional SSL group given that a smaller area is treated with this laser, further supporting that NNL is less painful compared to conventional SSL.
Discussion
Pain during panretinal photocoagulation is attributed to thermal effects on the choroid, stimulation and direct photocoagulation of long and short ciliary nerves, and diffusion of heat into the retinal nerve fiber layer.35,36,43,44 Pain with PRP has been described with terms such as “ache”, “pinprick-like” and “sharp” among others; other side effects such as photophobia, anxiety, and nausea were also reported.45 Pain responses are thought to be influenced by different factors such as culture, individual pain threshold, degree of fundus pigmentation, sex, duration of diabetes, experience of prior laser therapy, retinal location of laser administration, and wavelength used.11,21,36,43,44,46 There is conflicting evidence on the role of sex in pain scores; initial studies have claimed that females report higher pain scores after PRP, but the observation was not consistent across different studies.11,35 Lower pain scores among patients with longer duration of diabetes are attributed to chronic damage in retinal pain neurons, following a mechanism similar to that of diabetic neuropathy.11,36 Polat et al36 identified previous laser experience as an important factor in the expression of pain during laser therapy. In their study, stratification between “experienced” and “inexperienced” group revealed lower reported pain scores among experienced patients treated with conventional SSL.36 A similar observation was reported in the study of Inan et al.11 However, both of these studies demonstrated overall high risk of bias; hence, further studies may be needed to support this theory. Another important factor that affects pain responses is the area of photocoagulation. It is known that administration of laser shots at the horizontal periphery causes more pain due to the direct stimulation of the ciliary nerves.21
A good understanding of pain in relation to laser platforms can allow treatment optimization.8 Majority of the studies in this review employed a 532-nm green laser. The use of longer wavelengths, specifically those in the red to infrared range, allows deeper penetration into the sensory-rich choroid and greater pain sensation.11,46 Theoretically, use of light with shorter wavelengths may improve patient comfort during the procedure.11 In the report of Passos et al,37 pain tolerance and photophobia levels were not statistically different for patients who underwent 577-nm MSL and 532-nm SSL. In this study, it is possible that additional pain brought about by the use of the longer wavelength was compensated by the shorter pulses of the MSL. In the report of Muraly et al,39 where pain scores were based on the physician’s observations of the patient’s responses to treatment, a greater proportion of patients who underwent conventional SSL experienced moderate to very severe pain compared to those treated with conventional MSL. However, it is difficult to give weight to the findings of this study as it is subject to detection bias.
Multi-spot pattern lasers have gained popularity due to ease of its use. A single depression of the foot pedal delivers multiple laser shots in shorter pulses, thus shortening treatment time. Although the shorter pulse duration deviates from the treatment protocol specified in the ETDRS, several studies report that it does not decrease the effectiveness of PRP for diabetic retinopathy.7,10,34,44 Inan et al11 reported lower pain scores using conventional MSL on one eye versus SSL on the other eye when the number of spots are equalized per eye. This method, however, does not replicate usual practice as more laser spots are required to complete PRP by MSL. The effect of this bias may favor conventional MSL versus conventional SSL. Results of studies with low to some risk of bias show that MSL is more tolerable for patients in comparison to conventional SSL despite the higher number of spots administered. Shorter pulses lead to shorter time for thermal and inflammatory changes to take place thereby diminishing choroidal and retinal damage.14,20,35,44,45 The 20 to 30-millisecond pulse duration used in MSL balances adequate administration of therapeutic laser and reduction of collateral damage.7,14,41,47 Muqit et al attributed the lower pain scores in conventional MSL to the pattern application, which may have resulted to pain habituation (i.e. decreasing pain responses throughout duration of PRP) and improved comfort. In this study, pain during the entire duration of the laser procedure was reported by 55% of eyes that underwent conventional SSL versus 15% for those who underwent conventional MSL.35 Another advantage of using short-pulse over long-pulse settings is the preservation of the patient’s visual fields, as the burns expand less over time.7,8 Nagpal et al7 found that 200-μm spots expanded to 430-μm and 310-μm for conventional SSL and conventional MSL, respectively, after 3 months of therapy. In addition, treatment time is significantly reduced, which may also improve compliance.8,11,45 Nagpal et al7 reported reduced total time of 1.43 minutes using conventional MSL compared to 4.53 minutes using conventional SSL.
Findings of this review are consistent with an earlier report of Al-Hussainy et al,44 where lower pain scores were recorded with shorter pulse settings despite a higher total power administered compared to long-pulse, low power settings. Short-pulse laser therapy causes less tissue photocoagulation when compared to long-pulse laser, thereby requiring significantly more spots and a higher total power than long-pulse conventional SSL to complete therapy.35,40,41 This suggests that laser fluence, the product of power and time over a given area, rather than total power alone, determines pain perception. Studies have demonstrated that a reduction in laser fluence results into a corresponding decrease in pain scores and vice versa.7,10,11,41 Nagpal et al reported lower fluence with conventional MSL compared to conventional SSL when both treatments are administered in 2 sessions (40.33 J/cm2 vs 191 J/cm2).7
The NAVILAS® NNL platform makes use of a frequency doubled, Neodymium-doped Yttrium orthovanadate (Nd:YVO4) solid-state laser photocoagulation system. It is capable of infrared and color retinal imaging and fundus fluorescein angiography. The laser applications are pre-planned on the retinal image display, allowing precise and efficient administration of laser spots and uniform energy distribution. It also has a “eye tracking” feature that improves safety and accuracy.36,48,49 In a comparison of pain scores of patients undergoing laser with NNL and conventional MSL (PASCAL®), Inan et al19 found that 13.3% of patients had no pain using the NNL while those in the conventional MSL all had some degree of pain. Amoroso et al8 conducted a CCT on bilateral eyes of 16 patients using 577-nm NNL on one eye and conventional MSL on the other eye. It was found that mean pain scores using conventional MSL were thrice the mean scores obtained using NNL (7.1 + 2.1 versus 2.4 + 1.6, p <0.001). This was the highest VAS score reported associated with PRP in all the studies included in this review, but the results may have been influenced by the non-randomized study design. This is also the only study that compared pain scores using the pre-planned mode of NAVILAS®, in contrast to other studies by Kim,22 Chhablani,34 Polat,36 and Inan19 where the pattern mode was employed. Amoroso et al8 attributed lower pain scores using NNL to the short breaks in between the application of each spot, allowing retinal tissue restoration and decreased pain stimulation. Spatial summation of pain is also minimized using the pre-planned mode of the NNL wherein the linear delivery yields a greater separation of the first and last laser spots. In contrast, conventional MSL automatically applies the spots in clusters which can cause greater spatial summation of pain.8
Novel navigated laser systems may be set to deliver both short and long pulse durations, allowing adherence to the ETDRS guidelines. Chhablani et al34 and Polat et al11 investigated the difference in pain scores among patients undergoing NNL versus conventional SSL using 100-ms pulse duration for both groups. As seen in the results of Comparison 3, both studies reported significantly lower VAS scores using the NNL system compared to conventional SSL systems.34,36 Chhablani et al34 stated that the use of infrared imaging in NNL instead of the white light used in conventional laser lessens the pain experienced by patients. The delivery of pattern laser in sudden pulses with NNL also avoids repeated pain stimulation in comparison to single-spot laser therapy.34 This review shows that the newer NNL technology effectively lessens the pain experience of patients, even when pulse durations are the same. At a set pulse duration of 100-ms, the improved patient experience with the newer laser was attributed to differences in the method of laser beam positioning, heat radiation, and choroidal heating.36 Refractive properties of the contact lens used with NNL under topical anesthesia allowed less tilting for peripheral laser administration thereby improving patient comfort.19,34–36
Only the study by Chhablani et al34 uniquely studied all comparison groups of interest. Four groups were included in the study: short-pulse NNL (30-ms), conventional MSL (30-ms), long-pulse NNL (100-ms), and conventional SSL (100-ms). Average VAS scores were 1.0 ± 0.31, 2.0 ± 0.65, 1.5 ± 0.56, and 3.8 ± 2.10, respectively, indicating the benefit of using navigated pattern laser when looking at pain as the primary outcome. This study also shows that conventional SSL with long pulse durations (100 to 200-ms) yields the highest pain scores.34
This is the first systematic review that aimed to compare pain scores as a primary outcome among patients with diabetic retinopathy undergoing conventional SSL, conventional MSL, and NNL. Qualitative analysis from moderate-quality evidence showed a trend favoring NNL over conventional MSL, and conventional MSL over conventional SSL when looking at pain as the primary outcome. Ophthalmologists should take this into account when choosing the method for laser therapy for their patients, especially those with low pain tolerance. Administrators of ophthalmic treatment facilities can also take this into consideration when acquiring laser machines.
The review did not analyze the differences in the effectiveness of the different types of laser in the management of advanced diabetic retinopathy. The current review yielded 17 studies with a total of 783 patients and 1961 eyes. Majority of the RCTs included in this review had some concerns for bias; included CCTs demonstrated low risk of bias. A limitation of this study is the incomplete data available for some of the included studies and possible reporting bias. The magnitudes of the differences in pain scores should be interpreted with caution, given that there were significant variations in the laser settings used. A meta-analysis was deemed impractical due to marked heterogeneity in methodology among included studies.
Conclusions
Pain is an undesirable adverse effect of panretinal photocoagulation that may affect compliance to therapy. It is important for ophthalmologists to seek ways to minimize discomfort of the patients during any ocular procedure. With available evidence from largely heterogenous, moderate-quality studies in this systematic review, there is a benefit in using MSL over SSL for PRP among patients with diabetic retinopathy, focusing on pain as an important adverse outcome. Furthermore, NNL systems yield even lower pain scores in comparison to the conventional SSL and MSL systems.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Atlas D. International Diabetes Federation. IDF Diabetes Atlas; 2019.
2. Duh EJ, Sun JK, Stitt AW. Diabetic retinopathy: current understanding, mechanisms, and treatment strategies. JCI Insight. 2017;2(14):e93751. doi:10.1172/jci.insight.93751
3. Schwartz SS, Epstein S, Corkey BE, et al. A unified pathophysiological construct of diabetes and its complications. Trends Endocrinol Metab. 2017;28(9):645–655. doi:10.1016/j.tem.2017.05.005
4. Leasher JL, Bourne RRA, Flaxman SR, et al. Global estimates on the number of people blind or visually impaired by diabetic retinopathy: a meta-analysis from 1990 to 2010. Diabetes Care. 2016;39:1643–1649. doi:10.2337/dc15-2171
5. Sinclair SH, Schwartz SS. Diabetic retinopathy – an underdiagnosed and undertreated inflammatory, neuro-vascular complication of diabetes. Front Endocrinol. 2019;10:843. doi:10.3389/fendo.2019.00843
6. Stitt PAW, Curtis TM, Chen M, et al. The progress in understanding and treatment of diabetic retinopathy. Prog Retin Eye Res. 2016;51:151–186. doi:10.1016/j.preteyeres.2015.08.001
7. Nagpal M, Marlecha S, Nagpal K. Comparison of laser photocoagulation for diabetic retinopathy using 532-nm standard laser versus multispot pattern laser. Retina. 2010;30(3):452–458. doi:10.1097/IAE.0b013e3181c70127%0A
8. Amoroso F, Pedinielli A, Astroz P, Semoun O, Capuano V. Comparison of pain experience and time required for pre-planned navigated peripheral laser versus conventional multispot laser in the treatment of diabetic retinopathy. Acta Diabetol. 2020;57(5):535–541. doi:10.1007/s00592-019-01455-x
9. Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: clinical application of Diabetic Retinopathy Study (DRS) findings. Diabetic Retinopathy Study (DRS) Report Number 8. Ophthalmology. 1981;88:583–600. doi:10.1016/S0161-6420(81)34978-1
10. Mirshahi A, Lashay A, Roozbahani M. Pain score of patients undergoing single spot, short pulse laser versus conventional laser for diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2013;251(4):1103–1107. doi:10.1007/s00417-012-2167-5
11. Inan S, Polat O, Yıgıt S, Inan UU. PASCAL laser platform produces less pain responses compared to conventional laser system during the panretinal photocoagulation: a randomized clinical trial. Afr Heal Sci. 2018;18(4):1010–1017. doi:10.4314/ahs.v18i4.22
12. Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy. ETDRS report number 9. Ophthalmology. 1991;98(5):S766–S785. doi:10.1016/S0161-6420(13)38011-7
13. The Diabetic Retinopathy Study Research Group. Indications for photocoagulation treatment of diabetic retinopathy. Diabetic retinopathy study report number 14. Invest Ophthalmol Vis Sci. 1994;27:239–253.
14. Blumenkranz MS, Yellachich D, Andersen DE, et al. Semiautomated patterned scanning laser for retinal photocoagulation. Retina. 2006;26(3):370–376. doi:10.1097/00006982-200603000-00024
15. Çeliker H, Bulut AE, Şahin Ö. Comparison of efficacy and side effects of multispot lasers and conventional lasers for diabetic retinopathy treatment. Turk J Ophthalmol. 2017;47(1):34–41. doi:10.4274/tjo.75032
16. Zakrzewski P, O’Donnell H, Lam W. Oral versus topical diclofenac for pain prevention during panretinal photocoagulation. Ophthalmology. 2009;116(6):1168–1174. doi:10.1016/j.ophtha.2009.01.022
17. Vaideanu D, Taylor P, McAndrew A, et al. Double masked randomised controlled trial to assess the effectiveness of paracetamol in reducing pain in panretinal photocoagulation. Br J Ophthalmol. 2006;90:713–717. doi:10.1136/bjo.2005.076091
18. Ahmed T, Howaidy A, El-amin AA, Selim K. PASCAL laser produces less pain responses compared to conventional laser system during the panretinal photocoagulation. Egypt J Hosp Med. 2020;78(1):110–114. doi:10.12816/ejhm.2020.68358
19. Inan UU, Polat O, Inan S, Yigit S, Baysal Z. Comparison of pain scores between patients undergoing panretinal photocoagulation using navigated or pattern scan laser systems. Arq Bras Oftalmol. 2016;79(1):15–18. doi:10.5935/0004-2749.20160006
20. Yang JW, Lee Y. Comparison of the effects of patterned and conventional panretinal photocoagulation on diabetic retinopathy. J Korean Ophthalmol Soc. 2010;51(12):1590–1597. doi:10.3341/jkos.2010.51.12.1590
21. Seymenoğlu G, Kayıkçıoğlu Ö, Başer E, İlker SS. Proliferatif diyabetik retinopati nedeniyle panretinal fotokoagulasyon yapilan hastalarda ağri cevabinin karşilaştirilmasi: 532 nm standart lazer vs multispot patern taramali lazer comparison of pain response of patients undergoing panretinal photocoagula. Turk J Ophthalmol. 2013;43(4):221–225. doi:10.4274/tjo.43.03264
22. Kim MS, Lee SW, Kim JS. [Comparison of the Time Required for Panretinal Photocoagulation and Associated Pain between Navilas(R) and Conventional Laser Therapy in Diabetic Retinopathy]. J Korean Ophthalmol Soc. 2014;55(8):1150–1154. doi:10.3341/jkos.2014.55.8.1150
23. Wu WC, Hsu KH, Chen TL, et al. Interventions for relieving pain associated with panretinal photocoagulation: a prospective randomized trial. Eye. 2006;20:712–719. doi:10.1038/sj.eye.6701989
24. Richardson C, Waterman H. Pain relief during panretinal photocoagulation for diabetic retinopathy: a national survey. Eye. 2009;23:2233–2237. doi:10.1038/eye.2008.421
25. Ko BW, Shim JW, Lee BR, Cho H. Analgesic effects of tramadol during panretinal photocoagulation. Korean J Ophthalmol. 2009;23:273–276. doi:10.3341/kjo.2009.23.4.273
26. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(jul21 1):b2535. doi:10.1136/bmj.b2535
27. Sterne JAC, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
28. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:I4898. doi:10.1136/bmj.l4898
29. McGuinness LA, Higgins J. Risk-of-bias VISualization (robvis): an R package and shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020;1–7. doi:10.1002/jrsm.1411
30. Walter SD, Yao X. Effect sizes can be calculated for studies reporting ranges for outcome variables in systematic reviews. J Clin Epidemiol. 2007;60:849–852. doi:10.1016/j.jclinepi.2006.11.003
31. Higgins JPT, Thomas J, Chandler J, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020). Cochrane; 2020. Available from: www.training.cochrane.org/handbook.
32. Röckl A, Blum M. Panretinal laser photocoagulation with reduced pulse duration – first experience with linear multispot cascades. Klin Monatsbl Augenheilkd. 2012;229:52–55. doi:10.1055/s-0031-1273432
33. Chhablani J, Mathai A, Rani P, Gupta V, Arevalo JF, Kozak I. Comparison of conventional pattern and novel navigated panretinal photocoagulation in proliferative diabetic retinopathy. Invest Ophthalmol Vis Sci. 2014;55(6):3432. doi:10.1167/iovs.14-13936
34. Chhablani J, Sambhana S, Mathai A, Gupta V, Arevalo JF, Kozak I. Clinical efficacy of navigated panretinal photocoagulation in proliferative diabetic retinopathy. AJO. 2015;159(5):884–889. doi:10.1016/j.ajo.2015.02.006
35. Muqit MMK, Marcellino GR, Gray JCB, et al. Pain responses of pascal 20 ms multi-spot and 100 ms single-spot panretinal photocoagulation: Manchester Pascal Study, MAPASS report 2. Br J Ophthalmol. 2010;94(11):1493–1499. doi:10.1136/bjo.2009.176677
36. Polat O, Inan S, Baysal Z, Yigit S, Inan U. Comparison of navigated laser and conventional single-spot laser system for induced pain during panretinal photocoagulation. Lasers Med Sci. 2019;35:687–693. doi:10.1007/s10103-019-02886-2
37. Passos RM, Camilla JB, Eduardo OX, Maia M, Eid M. Comparison of 577-nm multispot and standard single-spot photocoagulation for diabetic retinopathy. Ophthalmologica. 2018. doi:10.1159/000493280
38. Zhang S, Cao G, Xu X, Wang C. Pattern scan laser versus single spot laser in panretinal photocoagulation treatment for proliferative diabetic retinopathy. Guoji Yanke Zazhi. 2017;17(2):205–208.
39. Muraly P, Limbad P, Srinivasan K, Ramasamy K. Single session of pascal versus multiple sessions of conventional laser for panretinal photocoagulation in proliferative diabetic retinopathy: a comparitive study. Retina. 2011;31(7):1359–1365. doi:10.1097/IAE.0b013e318203c140
40. Nemcansky J, Id AS, Nemcanska S, Masek P, Langrova H, Studnicka J. Single session of pattern scanning laser versus multiple sessions of conventional laser for panretinal photocoagulation in diabetic retinopathy: efficacy, safety and painfulness. PLoS One. 2019;14(7):e0219282. doi:10.1371/journal.pone.0219282
41. Salman AG. Pascal laser versus conventional laser for treatment of diabetic retinopathy. Saudi J Ophthalmol. 2011;25:175–179. doi:10.1016/j.sjopt.2011.01.006
42. Yilmaz I, Perente I, Saracoglu B, Yazici AT, Taskapili M. Changes in pupil size following panretinal retinal photocoagulation: conventional laser vs pattern scan laser (PASCAL). Eye. 2016;30(10):1359–1364. doi:10.1038/eye.2016.135
43. Belmonte C, Garcia-hirschfeld J, Gallar J, Neurociencias ID, Fisiologia DD, Alicante UD. Neurobiology of ocular pain. Prog Retin Eye Res. 1997;16(1):117–156.
44. Al-Hussainy S, Dodson PM, Gibson JM. Pain response and follow-up of patients undergoing panretinal laser photocoagulation with reduced exposure times. Eye. 2008;22(1):96–99. doi:10.1038/sj.eye.6703026
45. Muqit MMK, Gray JCB, Marcellino G. Fundus autofluorescence and fourier domain optical coherence tomography imaging of 10 and 20 millisecond pascal retinal photocoagulation treatment. Br J Ophthalmol. 2008;93:513–525. doi:10.1136/bjo.2008.144287
46. Hirano T, Iesato Y, Murata T. Multicolor pattern scan laser for diabetic retinopathy. Int J Ophthalmol. 2014;7(4):5–8. doi:10.3980/j.issn.2222-3959.2014.04.16
47. Jain A, Blumenkranz MS, Paulus Y, et al. Effect of pulse duration on size and character of the lesion in retinal photocoagulation. Arch Ophthalmol. 2008;126(1):78–85. doi:10.1001/archophthalmol.2007.29
48. Kernt M, Cheuteu R, Haritog- C. Focal and panretinal photocoagulation with a navigated laser (NAVILAS®). Acta Ophthalmol. 2011;89(8):e662–e664. doi:10.1111/j.1755-3768.2010.02017.x
49. Kozak I, Luttrull JK. Modern retinal laser therapy. Saudi J Ophthalmol. 2015;29(2):137–146. doi:10.1016/j.sjopt.2014.09.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.