Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Comparison of Neurofactor Changes and Prognosis in Elderly Patients with Spontaneous Intracerebral Hemorrhage Treated with Endoscopic versus Conventional Craniotomy Surgery
Authors Lei C, Li C, Chen X, Zhou G, Zheng X, Zhang Z, Qu X ![]()
Received 13 February 2025
Accepted for publication 1 June 2025
Published 24 October 2025 Volume 2025:21 Pages 1509—1519
DOI https://doi.org/10.2147/TCRM.S521299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Chao Lei,1,2 Chong Li,1,2 Xing Chen,1,2 Gaosheng Zhou,1,2 Xiaxia Zheng,1,2 Zhaohui Zhang,1,2 Xingguang Qu1,2
1Department of Critical Care Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang, People’s Republic of China; 2Department of Critical Care Medicine, Yichang Central People’s Hospital, Yichang, People’s Republic of China
Correspondence: Xingguang Qu, Email [email protected] Zhaohui Zhang, Email [email protected]
Objective: To compare the clinical efficacy, neurofactor changes, and prognosis in elderly patients with spontaneous intracerebral hemorrhage (ICH) treated with endoscopic surgery versus conventional craniotomy.
Methods: A retrospective analysis was conducted on 88 elderly patients with spontaneous ICH admitted from July 2021 to April 2024. Based on surgical method, patients were assigned to either the conventional craniotomy group (n=44) or the endoscopic surgery group (n=44). Surgical efficacy (hematoma evacuation rate, surgical duration, intraoperative blood loss), short-term prognosis (ICU stay, hospital stay, GOS, NIHSS, ADL scores), serum neurofactors (SOD, NSE, NGF, BDNF), inflammatory markers (WBC, CRP, PCT), and complication rates were compared.
Results: (1) The endoscopic group had significantly shorter surgical time and lower blood loss than the craniotomy group (P< 0.05), with similar hematoma evacuation rates (P> 0.05). (2) ICU and hospital stays were significantly shorter in the endoscopic group (P< 0.05). Postoperative GOS and ADL scores were higher, and NIHSS scores were lower in the endoscopic group at 3 months (P< 0.05). (3) Compared with preoperative levels, both groups showed a decreasing trend in SOD and NSE and an increasing trend in NGF and BDNF after surgery, with the observation group showing more significant and sustained changes over time (P < 0.05). (4) Although postoperative inflammatory markers increased in both groups, the observation group had milder elevations and faster downward trends (P < 0.05). (5) The complication rate was lower in the endoscopic group (6.82% vs 22.73%, P< 0.05).
Conclusion: Compared to conventional craniotomy, endoscopic hematoma evacuation in elderly ICH patients results in milder inflammatory responses, more favorable neurofactor changes, fewer complications, and improved recovery. However, these findings require further validation due to the retrospective design and limited sample size.
Keywords: spontaneous intracerebral hemorrhage, elderly, endoscopic surgery, neurofactors, prognosis
Introduction
Spontaneous intracerebral hemorrhage (ICH) is a common and life-threatening condition, typically caused by the rupture of blood vessels in the brain, leading to the infiltration of blood into the brain tissue or ventricular system, resulting in acute neuronal injury and dysfunction.1 Risk factors for ICH include hypertension, arteriosclerosis, and cerebrovascular malformations, often presenting with acute onset, high disability, and significant mortality.2,3 With the aging population, the risk of cerebrovascular rupture significantly increases due to decreased vascular elasticity and exacerbated arteriosclerosis, leading to a rising incidence of ICH among the elderly, making it a global public health issue.4,5 Moreover, elderly patients are often accompanied by underlying conditions such as hypertension, diabetes, and coronary heart disease, which result in reduced physiological and metabolic capacities, weakened immune function, and increased cerebrovascular fragility.6 Therefore, the treatment and prognosis assessment of spontaneous intracerebral hemorrhage in the elderly are more complex, often associated with higher mortality and complication rates. As a result, minimizing surgical trauma and improving the patient’s quality of life have become important challenges in the field of neurosurgery.
Surgical treatment remains the primary approach for ICH, particularly for patients with large hematomas or intraventricular hemorrhage, where timely hematoma evacuation, reduction of intracranial pressure, and relief of brain tissue compression typically lead to significant improvement in neurological function.7 However, traditional craniotomy, while effectively evacuating hematomas, involves large incisions, long recovery times, and a high incidence of complications. In particular, elderly patients often experience slower postoperative recovery, with serious complications such as infections, brain edema, and rebleeding being common.8,9 Therefore, selecting the most appropriate treatment method for elderly ICH patients is crucial. In recent years, with the continuous advancement of minimally invasive surgical techniques, clinical endoscopic surgery has gradually been applied in the field of neurosurgery and has become an important method for treating spontaneous intracerebral hemorrhage. Compared with traditional craniotomy, clinical endoscopic surgery offers advantages such as smaller trauma, less blood loss, and faster recovery, making it especially suitable for elderly patients.10,11
However, despite the growing recognition of the advantages of minimally invasive techniques in the academic community, the application of endoscopic surgery still has some limitations. Firstly, endoscopic surgery requires high technical expertise, particularly during the operation, where the experience and skill level of the surgeon are critical to the success of the procedure. Secondly, endoscopic surgery is not suitable for all types of intracerebral hemorrhage, especially when the hematoma is deep or located in difficult-to-reach areas, where it may not be possible to fully evacuate the hematoma, leading to suboptimal treatment outcomes. Additionally, complications such as incomplete hematoma evacuation during surgery, postoperative bleeding, or infection may occur, especially in elderly patients, who may experience slower recovery and face increased risks postoperatively. Therefore, although endoscopic surgery offers significant advantages for elderly patients, its limitations and risks must be weighed, and treatment should be tailored to suitable patient groups.
This study aims to retrospectively analyze 88 elderly patients with spontaneous intracerebral hemorrhage and compare the efficacy differences between endoscopic surgery and traditional craniotomy in treating spontaneous intracerebral hemorrhage. We hope to provide more scientific evidence for clinical practice and promote the widespread application of minimally invasive surgery in elderly patients.
Subjects and Methods
Study Subjects
A retrospective analysis was conducted on the clinical data of 88 elderly patients with spontaneous intracerebral hemorrhage admitted to our hospital from July 2021 to April 2024. (1) Inclusion criteria: ① Patients who met the diagnostic criteria for spontaneous intracerebral hemorrhage as defined in the Guidelines for the Diagnosis and Treatment of Stroke,12 and were confirmed by cranial CT or MRI; ② Age ≥ 70 years; ③ Indicated for surgical treatment with stable vital signs and tolerable for surgery; ④ No history of severe coagulopathy and with normal coagulation function; ⑤ No prior surgical intervention for hematoma evacuation; ⑥ Complete clinical data including neurological function scores, inflammatory factor levels, and neurofactor levels; ⑦ Informed consent obtained from patients or their legal representatives, including permission for data usage and sample preservation. (2) Exclusion criteria: ① Secondary intracerebral hemorrhage due to vascular malformations, tumors, or thrombosis; ② Severe comorbidities such as end-stage organ failure; ③ Active preoperative infections; ④ Very poor neurological baseline or short expected survival; ⑤ Uncorrectable coagulopathies; ⑥ Severe cognitive or psychiatric disorders; ⑦ Serious intraoperative complications or early postoperative death; ⑧ Incomplete follow-up or missing data. Notably, although this study employed a retrospective design, a subset of preoperative venous blood samples was collected and stored in the hospital’s biobank under prior informed consent as part of standard clinical care. The use of these samples for research purposes was reviewed and approved by the Medical Ethics Committee. This study was approved by the Yichang Central People’s Hospital Medical Ethics Committee (Approval No.: PW24-SS0015) and conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Surgical Methods
All surgical procedures in both the control and observation groups were performed by the same experienced neurosurgical team, who had received standardized training in both conventional craniotomy and endoscopic hematoma evacuation techniques. This was done to minimize inter-operator variability and ensure consistency in surgical quality across both groups.
Control Group
The patients in the control group underwent conventional craniotomy surgery. Preoperative preparation included general anesthesia and endotracheal intubation. The patients were placed in the supine position, with the head rotated to the opposite side to obtain the best surgical view. Preoperative planning was based on cranial CT images, combined with the hemorrhage site and hematoma size, to determine the appropriate surgical approach. After incising the scalp to expose the surgical area, a drill was used to create a hole in the skull with a diameter controlled between 0.5 and 1.0 cm. A burr was then used to remove a square bone window approximately 8 cm × 6 cm in size. The size of the bone window was adjusted according to the location of the brain hemorrhage and the size of the hematoma to ensure sufficient exposure of the lesion. Once the bone window was opened, the dura mater was exposed using a microscope. A cruciate incision was made to tear the dura mater and suspend it to ensure a clear field of view. Next, a brain puncture needle (2.7 mm in diameter and 100 mm in length) was used for precise puncture into the hematoma cavity. A 5 mL syringe was connected for aspiration to confirm the location of the hematoma and to aspirate the old blood. During the hematoma evacuation process, excessive stimulation of brain tissue was avoided, ensuring no significant blood clots were left behind. A cortical fenestration procedure was then performed, with the fenestration diameter approximately 1.5 cm. Under the guidance of a microscope, the puncture path was followed to enter the hematoma cavity, and the hematoma was further evacuated until completely cleared. The systolic blood pressure was then continuously raised to approximately 140 mmHg for 5 minutes to ensure no active bleeding before repositioning and fixing the bone flap. A subcutaneous drainage tube was then placed to drain any excess fluid. A CT scan was performed 24 hours postoperatively. If no significant epidural hematoma or subcutaneous hematoma was observed, the drainage tube was removed.
Observation Group
Patients in the observation group underwent clinical endoscopic surgery. Preoperative preparation included general anesthesia and endotracheal intubation. The patients were placed in the supine position with the head maintained in a neutral position to ensure stable surgical visibility. The appropriate surgical approach and puncture site were selected based on preoperative cranial CT scans. During the procedure, the Karl Storz endoscope system (diameter 4 mm, length 18 cm, 0° rigid lens) was used for endoscopic guidance. The puncture point was accurately located through the endoscopic sleeve. The puncture target was located 23 mm from the maximum layer of the hematoma, with the puncture point marked based on the projection location on the surface of the body from the preoperative CT images. The surgical incision was made 3 cm behind the hairline and 3–4 cm to the side of the midline. The length of the incision was controlled between 4–5 cm. After scalp incision, a milling cutter was used to remove a circular bone window of approximately 3 cm in diameter, providing sufficient space for the endoscope to guide the procedure. Once the dura mater was exposed, a cruciate incision was made to suspend the dura mater and provide a clear view of the surgical field. The puncture site was determined based on preoperative CT images, with the distance from the puncture point to the midline sagittal plane (typically 3–4 cm) used for localization. The direction of the puncture was kept parallel to the sagittal plane, and the puncture was aligned along the imaginary line connecting the puncture target and its surface projection. The puncture depth was determined based on preoperative imaging to ensure the depth from the puncture target to the outer layer of the frontal bone was consistent with the CT images. In the treatment of subcortical hemorrhage, the puncture point was chosen at the location where the hematoma was closest to the brain surface, and throughout the procedure, care was taken to avoid disturbing major cerebral blood vessels, nerves, or functional brain regions. Under direct endoscopic visualization, careful hematoma evacuation was performed, ensuring no residual blood clots remained. The systolic blood pressure was then raised, and a thorough evaluation of the bleeding site was performed using the multi-angle view of the endoscope to assess for active bleeding. After observing for 5 minutes with no active bleeding, the dura mater was sutured, the bone window was repositioned and securely fixed with titanium plates, and the scalp was sutured layer by layer.
Observation Indicators
Surgical Efficacy
Including the duration of the surgery, intraoperative blood loss, and hematoma clearance rate, all of which were recorded by the medical staff of our hospital. The hematoma clearance rate was calculated as follows: Hematoma clearance rate = (preoperative hematoma volume - postoperative residual hematoma volume) / preoperative hematoma volume × 100%, with hematoma volume calculated using 3D Slicer software.
Prognosis
The patients’ hospitalization time and ICU stay time were recorded. Follow-up was conducted via phone or outpatient visits 3 months post-surgery. During follow-up, the Glasgow Outcome Scale (GOS),13 the National Institutes of Health Stroke Scale (NIHSS),14 and the Activities of Daily Living (ADL)15 scores were assessed. To minimize assessment bias, these subjective scoring evaluations were performed by clinicians who were blinded to the patients’ treatment group assignments. The GOS has a total score of 5 points, with higher scores indicating better prognosis. The NIHSS ranges from 0 to 42 points, with higher scores indicating more severe neurological impairment. The ADL scale has a total score of 100, with higher scores indicating better functional ability in daily living.
Neurofactor Indicators
Blood samples (10 mL) were collected from the antecubital vein preoperatively and 3 days postoperatively, placed in anticoagulant tubes, centrifuged at 3000 rpm for 10 minutes, and the serum was separated and stored at −80°C until tested. Serum levels of superoxide dismutase (SOD), neuron-specific enolase (NSE), nerve growth factor (NGF), and brain-derived neurotrophic factor (BDNF) were measured using enzyme-linked immunosorbent assay (ELISA).
Inflammatory Factor Indicators
Remaining serum samples were collected preoperatively and 3 days postoperatively. White blood cell count (WBC), C-reactive protein (CRP), and procalcitonin (PCT) levels were measured using an automatic biochemical analyzer.
Complications
Including hemorrhage, infection, subcutaneous fluid accumulation, and electrolyte imbalances, all of which were recorded by the medical staff of our hospital.
Statistical Analysis
GraphPad Prism 8 software was used for plotting, and SPSS 22.0 software was used for statistical processing. Count data were expressed as percentages (%) and analyzed by χ²-test. Measurement data were expressed as ( ). Independent-sample t-tests were used for comparisons between the two groups, and paired t-tests were used for comparisons within the same group. A P value of <0.05 was considered statistically significant.
). Independent-sample t-tests were used for comparisons between the two groups, and paired t-tests were used for comparisons within the same group. A P value of <0.05 was considered statistically significant.
Results
Comparison of Clinical Data
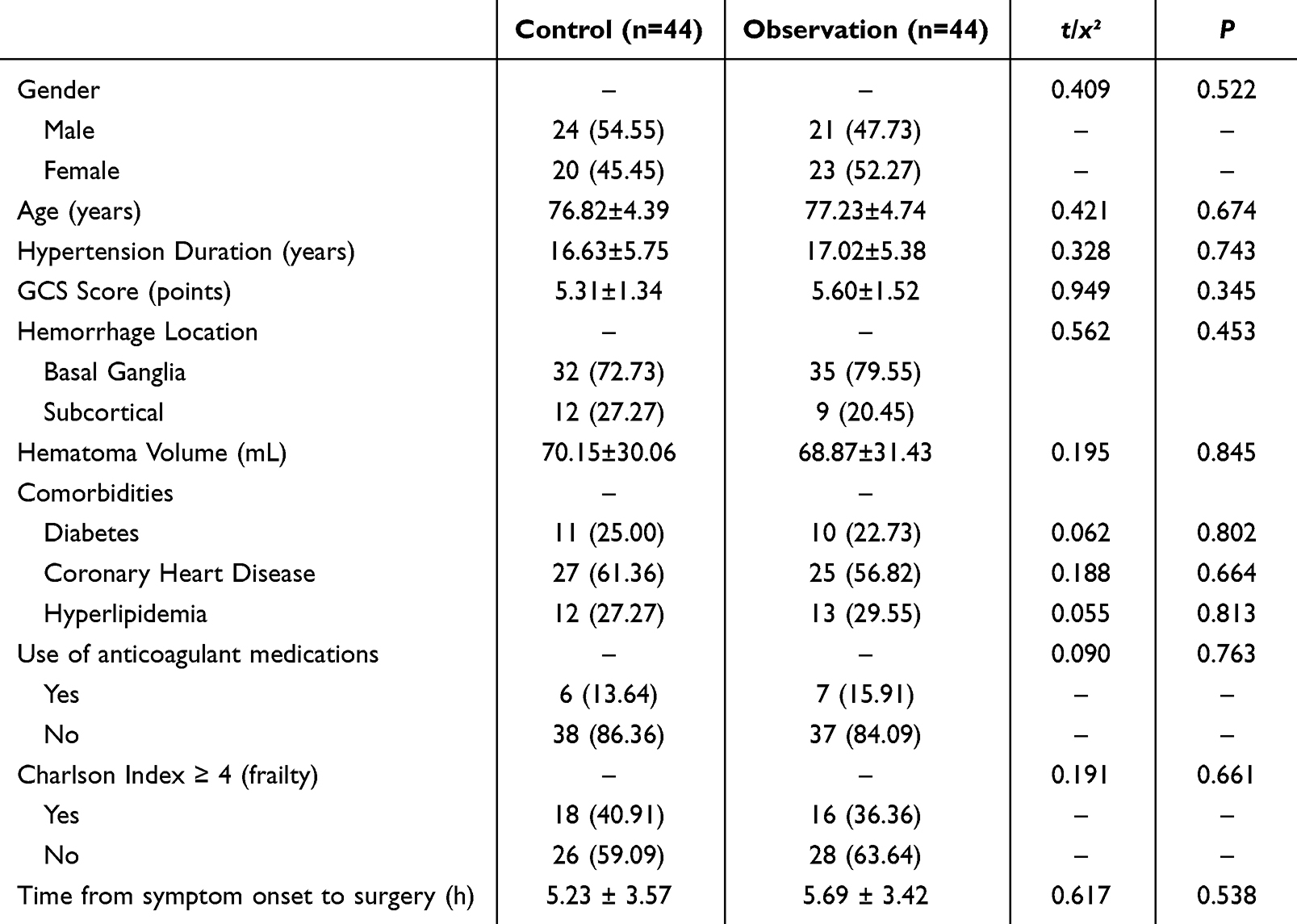
There were no statistically significant differences between the two groups in terms of sex, age, duration of hypertension, Glasgow Coma Scale (GCS) score at admission, hematoma location, hematoma volume, comorbidities, use of anticoagulant medications, preoperative frailty status (assessed by Charlson Comorbidity Index), or time from symptom onset to surgery (P > 0.05), indicating good comparability between the two groups. See Table 1 for details.
 |

Comparison of Surgical Efficacy
The hematoma clearance rate, operation duration, and intraoperative blood loss were (95.37±3.89, 165.82±59.81, 95.86±25.07) in the control group, and (96.03±3.75, 149.37±36.54, 78.35±16.34) in the observation group. There was no significant difference in hematoma clearance rate between the two groups (P > 0.05). However, the observation group had significantly shorter operation duration and less intraoperative blood loss compared to the control group (P < 0.05), as shown in Figure 1.
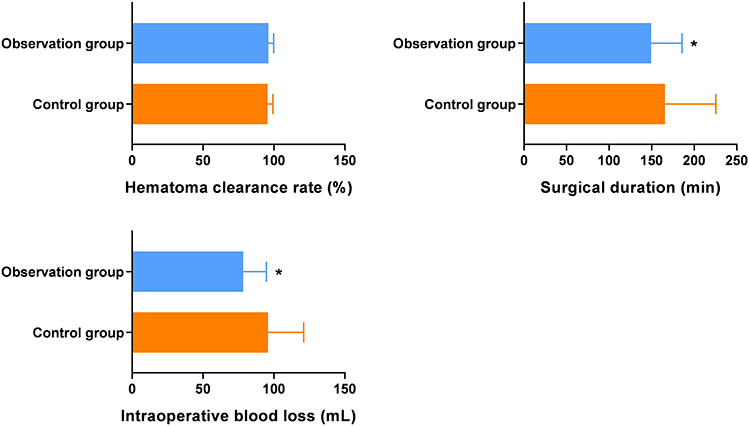 |
Figure 1 Comparison of Surgical Efficacy ( Note: Compared with the control group at the same time point, *P < 0.05. |

Comparison of Prognosis
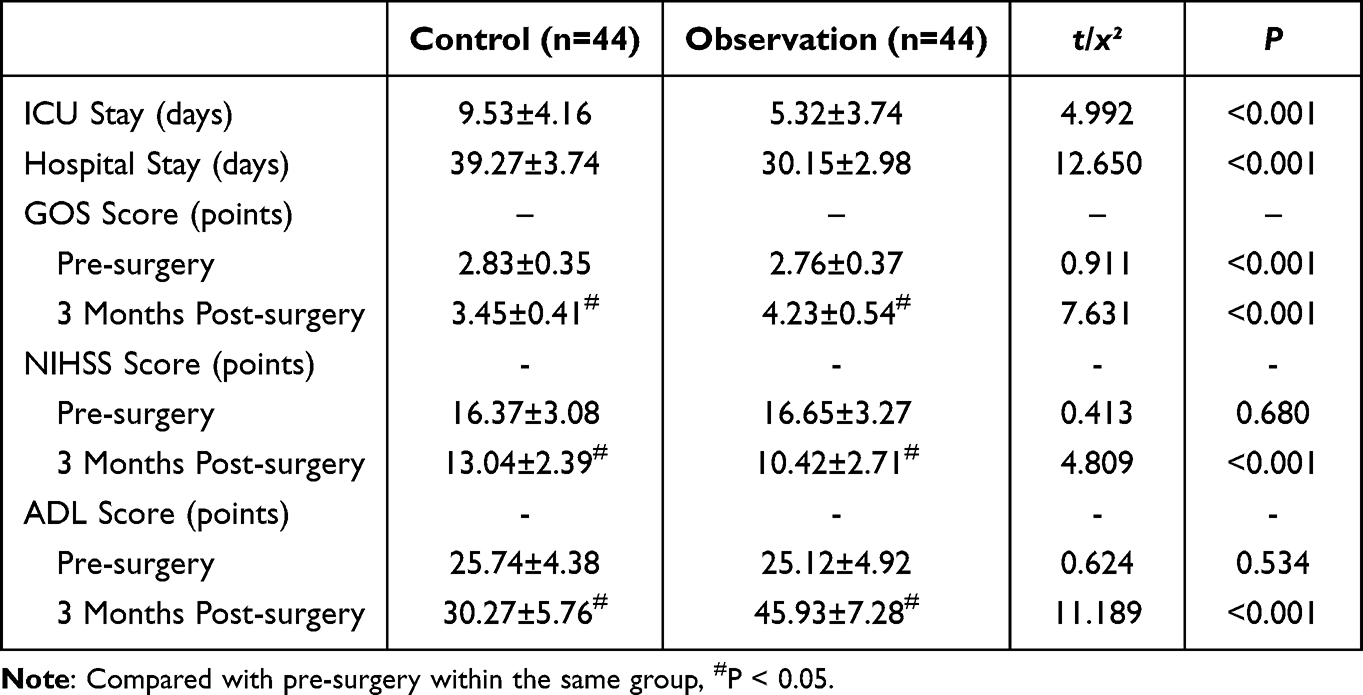
The observation group had significantly shorter ICU stay and hospital stay compared to the control group (P < 0.05). The GOS scores and ADL scores at 3 months after surgery were higher than before surgery in both groups, while the NIHSS scores were lower than before surgery. The observation group showed a larger change in these scores (P < 0.05), as shown in Table 2.
 |

Comparison of Neurobiomarker Levels
In the control group, the levels of SOD were (43.19±7.32), (18.36±4.07), and (20.45±4.92); NSE were (80.65±7.24), (30.43±5.38), and (28.73±5.16); NGF were (13.54±3.65), (17.38±4.32), and (19.56±4.85); BDNF were (14.23±3.35), (19.42±4.21), and (21.07±4.92) at pre-surgery, 3-day post-surgery, and 7-day post-surgery, respectively.
In the observation group, corresponding levels were SOD (45.62±6.53), (11.25±3.41), and (13.62±3.83); NSE (81.35±6.82), (22.36±3.44), and (20.71±3.92); NGF (14.72±3.31), (29.43±5.36), and (32.85±5.77); BDNF (13.63±2.85), (36.34±6.68), and (39.21±6.94).
Compared with preoperative levels, both groups showed a decreasing trend in SOD and NSE and an increasing trend in NGF and BDNF after surgery, with the observation group showing more significant and sustained changes over time (P < 0.05), as shown in Figure 2.
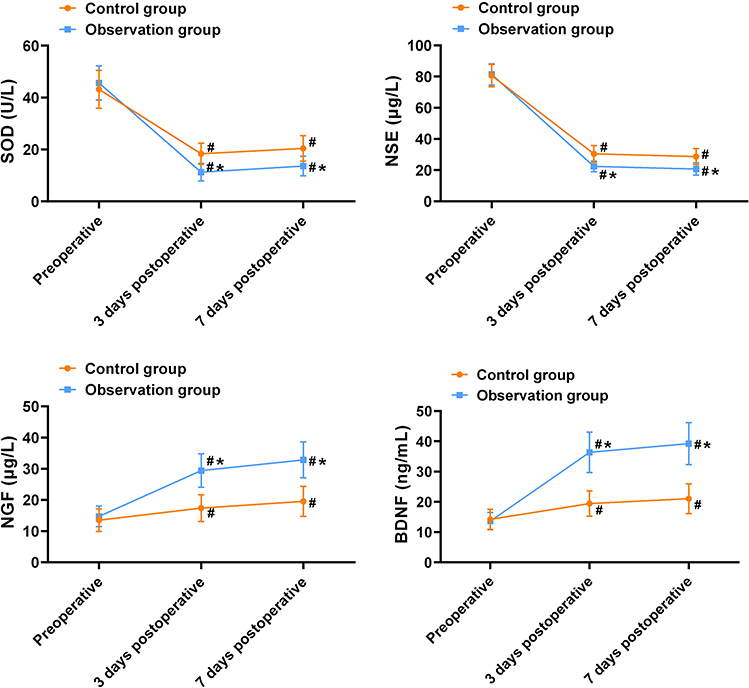 |
Figure 2 Comparison of Neurobiomarker Levels ( Notes: Compared with the control group at the same time point, *P < 0.05; Compared with pre-surgery within the same group, #P < 0.05. |

Comparison of Inflammatory Factor Levels
The control group showed WBC values of (7.11±1.14), (12.03±4.35), and (11.45±3.97); CRP (9.21±1.24), (69.07±8.13), and (65.84±7.69); PCT (0.08±0.03), (0.33±0.07), and (0.31±0.08). The observation group showed WBC values of (7.52±1.18), (9.09±2.74), and (8.72±2.63); CRP (9.43±1.16), (31.56±5.92), and (28.14±5.37); PCT (0.09±0.03), (0.14±0.03), and (0.13±0.03).
Although postoperative inflammatory markers increased in both groups, the observation group had milder elevations and faster downward trends (P < 0.05), suggesting lower postoperative systemic inflammation. Results are shown in Figure 3.
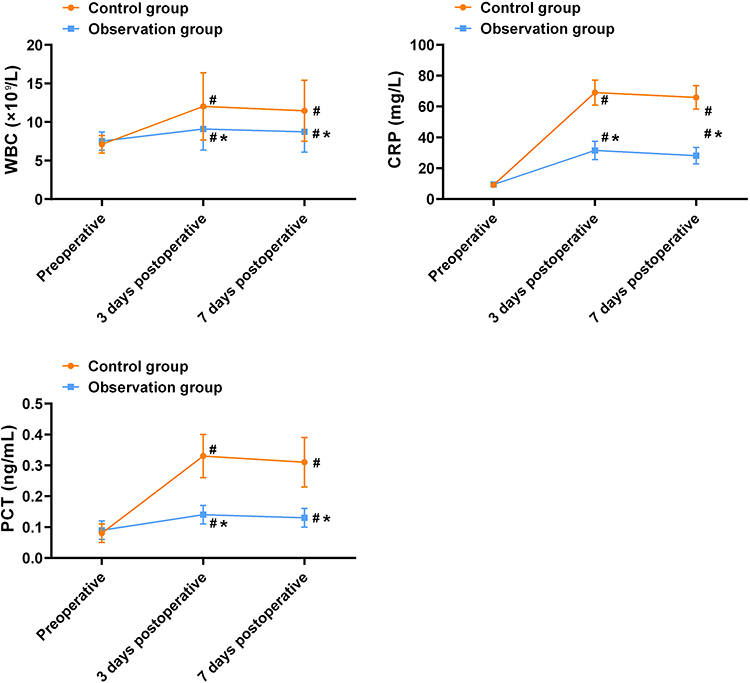 |
Figure 3 Comparison of Inflammatory Factor Levels ( Notes: Compared with the control group at the same time point, *P < 0.05; Compared with pre-surgery within the same group, #P < 0.05. |

Comparison of Complications
The total incidence of complications was lower in the observation group (6.82%) compared to the control group (22.73%) (P < 0.05), as shown in Table 3.
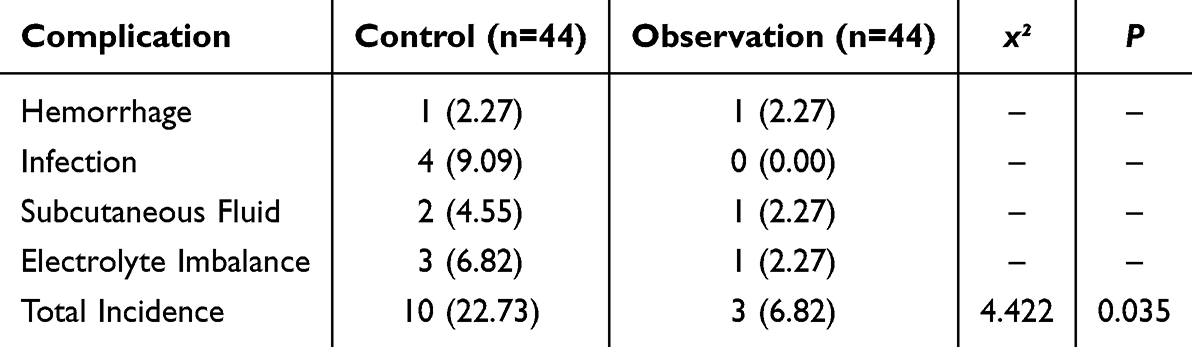 |
Table 3 Comparison of Complications [n(%)] |
Discussion
Spontaneous intracerebral hemorrhage is a common and often fatal condition in elderly patients, typically accompanied by severe neurological deficits and poor prognosis.16 Despite the significant effectiveness of traditional craniotomy in treating spontaneous intracerebral hemorrhage, with the continuous development of minimally invasive techniques, clinical endoscopic surgery has gradually emerged as a novel and effective treatment modality. The purpose of this study was to compare the clinical efficacy of endoscopic surgery versus traditional craniotomy in treating elderly patients with late-stage spontaneous intracerebral hemorrhage, and to explore the impact of these two surgical approaches on patients’ neurological factors, inflammatory factors, and postoperative prognosis. Recent high-quality clinical studies have further supported the value of minimally invasive surgery in ICH treatment. The MISTIE III trial, a large multicenter randomized controlled study, demonstrated that image-guided minimally invasive surgery combined with thrombolysis could safely reduce hematoma volume and perihematomal edema, with potential improvement in functional outcomes among patients with large ICH, although the primary endpoint did not reach statistical significance.17 Additionally, several updated meta-analyses have reaffirmed the benefits of minimally invasive approaches over conventional craniotomy, indicating lower mortality, better functional recovery, and fewer complications, particularly in elderly or high-risk populations.18,19 These findings provide further evidence to support the clinical use of endoscopic evacuation in selected ICH patients and reinforce the present study’s conclusion that endoscopic surgery may be advantageous in elderly patients.
In this study, no significant differences were found between the two groups regarding postoperative hematoma clearance rates (P > 0.05). This result is consistent with previous related studies,20,21 indicating that both surgical methods are generally comparable in terms of hematoma clearance effectiveness. This phenomenon may be closely related to the technical methods used during the surgeries. Traditional craniotomy allows for direct exposure of the lesion, providing sufficient operational space for clearing large or complex hematomas. On the other hand, endoscopic surgery clears the localized hematomas with fine endoscopic equipment. Although this method has limitations in terms of operational space, its advantages in precise localization and accurate operation due to its minimally invasive nature enable it to achieve a similar hematoma clearance effect as traditional craniotomy. Nevertheless, when treating different types of brain hemorrhage, minimally invasive surgery still requires individualized assessment based on the patient’s specific condition. Additionally, the observation group had a significantly shorter surgical duration and intraoperative blood loss compared to the control group (P < 0.05). This result suggests that endoscopic surgery offers a distinct advantage over traditional craniotomy in terms of the surgical process and control of intraoperative blood loss. The reason for this may be that endoscopic surgery uses minimally invasive techniques with small incisions, effectively reducing direct damage to brain tissue and the traction on blood vessels during surgery,22 thus lowering the risk of intraoperative bleeding and shortening the surgical time. Moreover, shorter surgery times also mean less trauma to the patient, reducing the postoperative recovery burden and further improving the patient’s postoperative prognosis.
Regarding prognosis, this study showed that the ICU stay and hospitalization duration in the observation group were significantly shorter than those in the control group (P < 0.05). The shortened postoperative recovery time is closely related to the degree of surgical trauma.23 Due to the smaller trauma of endoscopic surgery, patients recover faster after surgery, with lighter postoperative immune responses and inflammatory reactions, allowing for quicker recovery and reduced reliance on intensive care. In contrast, traditional craniotomy, due to its greater trauma, may cause more pronounced inflammatory responses and immune reactions after surgery, leading to longer ICU stays and hospitalization. More importantly, the improvement in GOS scores, ADL scores, and NIHSS scores in the observation group was significantly greater than in the control group (P < 0.05). These assessment indicators not only reflect the patients’ neurological recovery but also reveal changes in their postoperative quality of life. The reason for this improvement is likely due to the minimally invasive nature of endoscopic surgery, which causes less intraoperative damage, enabling patients to maintain a higher level of independent living after surgery, thereby improving their overall quality of life.
Neurotrophic factors and oxidative stress-related biomarkers play important roles in the repair process following brain injury and have increasingly been considered closely associated with patient prognosis in recent years.24 This is particularly relevant in elderly patients with ICH, where changes in these biomarkers may possess predictive value. SOD, a key antioxidant enzyme in the body, scavenges free radicals and reduces oxidative damage in brain tissue, thereby minimizing secondary brain injury.25 In the present study, the observation group exhibited significantly elevated SOD levels after treatment, suggesting that endoscopic surgery effectively alleviated postoperative oxidative stress. Previous research26 has shown that increased postoperative SOD levels may be associated with neuroprotective effects and better neurological outcomes. NSE is a highly specific biomarker of neuronal injury, and elevated levels usually indicate neuronal apoptosis or necrosis.27 In this study, NSE levels on postoperative days 3 and 7 were significantly lower in the observation group compared to the control group, indicating that endoscopic surgery can effectively reduce the extent of postoperative neuronal damage. Literature28 has pointed out that persistently elevated NSE levels are closely related to poor neurological outcomes, suggesting that NSE may have prognostic value. In addition, NGF and BDNF, as key neurotrophic factors, play critical roles in neuronal regeneration, synaptic plasticity, and reconstruction of neural networks. Studies29 have shown that elevated levels of NGF and BDNF are positively correlated with neurological recovery after stroke and may serve as biological indicators of neural repair capacity. In this study, the levels of NGF and BDNF at 3 and 7 days postoperatively were significantly higher in the observation group than in the control group, indicating that endoscopic surgery not only contributes to neuroprotection but may also promote functional recovery by upregulating repair-related factors. However, considering the limited sample size and follow-up duration in this study, the prognostic value of these biomarkers in elderly ICH patients requires further validation through large-scale studies with long-term follow-up.
Additionally, inflammatory responses represent an important physiological process following cerebral hemorrhage. However, excessive activation of inflammation may exacerbate brain damage and hinder postoperative recovery.30,31 This study found that although WBC, CRP, and PCT levels increased at 3 and 7 days postoperatively in both groups, the magnitude of these changes was significantly smaller in the observation group (P < 0.05). This indicates that endoscopic surgery has a significant advantage in reducing postoperative inflammatory responses. Minimally invasive procedures reduce tissue trauma, thereby effectively suppressing the postoperative inflammatory response. In contrast, traditional craniotomy, due to greater surgical trauma, triggers more pronounced immune reactions, leading to significantly elevated inflammatory markers.32,33 Therefore, endoscopic surgery plays an important role in controlling postoperative inflammation, helping to reduce complications and improve patient outcomes.
Regarding the incidence of complications, this study found that the overall complication rate in the observation group (6.82%) was lower than that in the control group (22.73%) (P < 0.05). This difference further validates the minimally invasive advantage of endoscopic surgery. The reduced surgical trauma associated with endoscopic procedures lowers the risk of postoperative complications such as bleeding and infection. In contrast, traditional craniotomy, due to its invasiveness, is more likely to cause complications such as cerebral edema, infection, and rebleeding, thereby increasing the patient’s treatment burden. Thus, endoscopic surgery not only offers better neurological recovery but also effectively reduces the incidence of postoperative complications, ultimately improving patients’ quality of life.
The results of this study provide new clinical insights for the treatment of elderly patients with late-stage spontaneous intracerebral hemorrhage, demonstrating that endoscopic surgery offers superior clinical outcomes compared to traditional craniotomy. It significantly improves postoperative prognosis, neurological factor levels, quality of life, and reduces the incidence of complications. For elderly patients, endoscopic surgery, as a minimally invasive treatment approach, effectively alleviates postoperative physical burdens and enhances patients’ quality of life. However, this study also has some limitations. First, it is a retrospective analysis, which may have selection bias and missing information. Second, the sample size is relatively small and only from a single hospital, which may affect the external validity of the results. Future studies could further validate these conclusions through multicenter, large-sample prospective randomized controlled trials. In summary, endoscopic surgery provides a safer and more effective treatment option for elderly patients with late-stage spontaneous intracerebral hemorrhage, and it has important clinical application value.
Conclusion
Endoscopic surgery demonstrates superior clinical efficacy compared to traditional craniotomy in the treatment of elderly patients with late-stage spontaneous intracerebral hemorrhage. It significantly enhances postoperative neurological recovery and quality of life while reducing complication rates. As a minimally invasive approach, endoscopic surgery effectively alleviates the postoperative burden in elderly patients and offers a safer, more effective clinical option. Despite the limitations of this study, including its retrospective design and limited sample size, the findings highlight the important clinical value of endoscopic techniques. Further validation through large-scale, multicenter prospective studies is warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cai Y, Zhong X, Wang Y, et al. [Predictive value of magnetic resonance spectroscopy combined with diffusion weighted imaging in patients with secondary brain insult after spontaneous intra-cerebral hemorrhage]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(11):1336–1339. Dutch. doi:10.3760/cma.j.cn121430-20200331-00247
2. Xiong M, Wang S, Zhang Y, et al. Influential factors for large volume of spontaneous supratentorial intracerebral hemorrhage. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2020;45(12):1398–1402. doi:10.11817/j.issn.1672-7347.2020.190614
3. Alqahtani MS, Asiri MA, Al-Ajlan FS. Rethinking spontaneous intracerebral hemorrhage: leveraging innovation and recent data to shape the future of care. World Neurosurg. 2024;191:330–332. doi:10.1016/j.wneu.2024.08.148
4. Guo R, Yan S, Li Y, et al. A novel machine learning model for predicting stroke-associated pneumonia after spontaneous intracerebral hemorrhage. World Neurosurg. 2024;189:e141–e152. doi:10.1016/j.wneu.2024.06.001
5. Wiśniewski K, Zaczkowski K, Podstawka M, et al. Predictors of 30-day mortality for surgically treated patients with spontaneous supratentorial intracerebral hemorrhage and validation of the surgical swedish intracerebral hemorrhage score: a retrospective single-center analysis of 136 cases. World Neurosurg. 2024;186:e539–e551. doi:10.1016/j.wneu.2024.03.172
6. Chaisawasthomrong C, Saetia K. Independent factors associated with 30-day in-hospital mortality from acute spontaneous intracerebral hemorrhage. World Neurosurg. 2024;184:e774–e783. doi:10.1016/j.wneu.2024.02.035
7. Grasso G, Torregrossa F. Shunt dependency in patients with intraventricular hemorrhage: a perspective on challenges and opportunities. World Neurosurg. 2023;180:86–87. doi:10.1016/j.wneu.2023.09.036
8. Rao X, Zhang J, Yu K, et al. Effect of early external ventricular drainage on perihemorrhagic edema and functional outcome in patients with intraventricular hemorrhage. World Neurosurg. 2023;175:e1059–e1068. doi:10.1016/j.wneu.2023.04.069
9. Noiphithak R, Ratanavinitkul W, Yindeedej V, et al. Outcomes of combined endoscopic surgery and fibrinolytic treatment protocol for intraventricular hemorrhage: a randomized controlled trial. World Neurosurg. 2023;172:e555–e564. doi:10.1016/j.wneu.2023.01.080
10. Yamamoto T, Watabe T, Yamashiro S, et al. Safety of endoscopic surgery for spontaneous intracerebral hemorrhage in the registry of intracerebral hemorrhage treated by endoscopic hematoma evacuation in Japan. World Neurosurg. 2024;189:e370–e379. doi:10.1016/j.wneu.2024.06.058
11. Dammers R, Beck J, Volovici V, et al. Advancing the surgical treatment of intracerebral hemorrhage: study design and research directions. World Neurosurg. 2022;161:367–375. doi:10.1016/j.wneu.2022.01.084
12. Cao Y, Yu S, Zhang Q, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of intracerebral haemorrhage. Stroke Vasc Neurol. 2020;5(4):396–402. doi:10.1136/svn-2020-000433
13. Yin R, Zhang X, Wei JJ, et al. [Efficacy and outcomes of shunt surgery for secondary hydrocephalus]. Zhonghua Yi Xue Za Zhi. 2023;103(25):1936–1939. Danish. doi:10.3760/cma.j.cn112137-20230226-00276
14. Liu Y, Yin YY, Lu QL, et al. [Clinical analysis of dual enhanced antiplatelet therapy after cerebrovascular intervention for reducing the risk of cerebral infarction recurrence]. Zhonghua Yu Fang Yi Xue Za Zhi. 2024;58(7):1062–1068. Wolof. doi:10.3760/cma.j.cn112150-20240115-00054
15. Liu HL, Song YN, Wang XX, et al. [Effects of whole-course multimodal analgesia on postoperative pain and rapid recovery in elderly patients with urological tumors]. Zhonghua Yi Xue Za Zhi. 2023;103(41):3245–3251. Danish. doi:10.3760/cma.j.cn112137-20230725-00089
16. Wilson M, Incontri D, Vu S, et al. Association of anticoagulant use with hemorrhage location and etiology in incident spontaneous intracerebral hemorrhage. Stroke. 2024;55(11):2677–2684. doi:10.1161/STROKEAHA.124.048243
17. Hanley DF, Lane K, McBee N, et al. Thrombolytic removal of intracerebral hemorrhage in cerebral hemorrhage evacuation (MISTIE III). Lancet. 2019;393(10175):1021–1032. doi:10.1016/S0140-6736(19)30195-3
18. Xu X, Chen X, Li F, et al. Minimally invasive surgery versus conservative treatment for spontaneous intracerebral hemorrhage: a meta-analysis. World Neurosurg. 2018;114:e529–e536.
19. Zheng J, Wang D, Li M, et al. Comparison of endoscopic surgery, stereotactic aspiration, and craniotomy in spontaneous intracerebral hemorrhage: a systematic review and network meta-analysis. World Neurosurg. 2022;158:e606–e618.
20. Hegde A, Prasad GL, Menon G. Decompressive craniectomy in spontaneous intracerebral hemorrhage: a comparison with standard craniotomy using propensity-matched analysis. World Neurosurg. 2020;144:e622–e630. doi:10.1016/j.wneu.2020.09.016
21. Xiao ZK, Duan Y-H, Mao X-Y, et al. Traditional craniotomy versus current minimally invasive surgery for spontaneous supratentorial intracerebral haemorrhage: a propensity-matched analysis. World J Radiol. 2024;16(8):317–328. doi:10.4329/wjr.v16.i8.317
22. Pedersen CB, Andersen MS, Poulsen FR, Munthe S. [Endoscopic evacuation of deep intracerebral spontaneous haematoma]. Ugeskr Laeger. 2021;183(41):V01210083. Luxembourgish
23. Xiao T, Wan J, Qu H, Jiang W, Zhou X. Endoscopic surgery versus minimal puncture drainage surgery for treatment of supratentorial intracerebral hemorrhage. Turk Neurosurg. 2020;30(4):565–572.
24. Li H, Han F, Meng J, et al. [Research progress on mechanism of traumatic brain injury promoting fracture healing]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024;38(1):125–132. Danish. doi:10.7507/1002-1892.202310045
25. Akyol ME, Demir C, Görken G. Investigation of oxidative stress level and antioxidant enzyme activities in operated and nonoperated patients with spontaneous intracerebral hematoma. J Neurol Surg a Cent Eur Neurosurg. 2024;85(1):21–25. doi:10.1055/a-1938-0067
26. Masomi-Bornwasser J, Kurz E, Frenz C, et al. The influence of oxidative stress on neurological outcomes in spontaneous intracerebral hemorrhage. Biomolecules. 2021;11(11):1615. doi:10.3390/biom11111615
27. Gusev E, Solomatina L, Bochkarev P, Zudova A, Chereshnev V. The role of systemic inflammation in the pathogenesis of spontaneous intracranial hemorrhage in the presence or absence of effective cerebral blood flow. J Clin Med. 2024;13(15):4454.
28. Kimura F, Kadohama T, Kitahara H, et al. Serum neuron-specific enolase level as predictor of neurologic outcome after aortic surgery. Thorac Cardiovasc Surg. 2020;68(4):282–290. doi:10.1055/s-0038-1677511
29. Sun L, Xiao K, Shen XY, Wang S. Impact of transcranial electrical stimulation on serum neurotrophic factors and language function in patients with speech disorders. World J Clin Cases. 2024;12(10):1742–1749.
30. Zhang J, Liu C, Xiao X, et al. The trends of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and systemic immunoinflammatory index in patients with intracerebral hemorrhage and clinical value in predicting pneumonia 30 days after surgery. World Neurosurg. 2024;188:e108–e119. doi:10.1016/j.wneu.2024.05.048
31. Devlin P, Ishrat T, Stanfill AG. A systematic review of inflammatory cytokine changes following aneurysmal subarachnoid hemorrhage in animal models and humans. Transl Stroke Res. 2022;13(6):881–897.
32. Durocher M, Knepp B, Yee A, et al. Molecular correlates of hemorrhage and edema volumes following human intracerebral hemorrhage implicate inflammation, autophagy, mRNA splicing, and T cell receptor signaling. Transl Stroke Res. 2021;12(5):754–777. doi:10.1007/s12975-020-00869-y
33. Ohashi SN, DeLong JH, Kozberg MG, et al. Role of inflammatory processes in hemorrhagic stroke. Stroke. 2023;54(2):605–619. doi:10.1161/STROKEAHA.122.037155
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.