Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of Efficacy Between a Phospholipid-Hydroxypropyl Guar Nanoemulsion and Castor Oil-Based Lubricating Eyedrops
Authors Mashouf J, Wan K, Hall B ![]()
Received 14 May 2025
Accepted for publication 8 August 2025
Published 15 August 2025 Volume 2025:19 Pages 2759—2764
DOI https://doi.org/10.2147/OPTH.S540474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jay Mashouf,1 Keith Wan,1 Brad Hall2
1Scripps Optometric Group, San Diego, CA, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Jay Mashouf, Scripps Optometric Group, 10549 Scripps Poway Pkwy Ste, San Diego, CA, 92131, USA, Tel +1858-530-2800, Email [email protected]
Purpose: To compare dry eye symptoms using the SANDE questionnaire as well as corneal and conjunctival staining with two propylene glycol lubricating eyedrops that contain very different excipients.
Methods: This was a single site, prospective, double-masked, randomized-controlled study with two arms comparing Systane Complete Multi-Dose Preservative Free (MDPF) eyedrops (Systane group) and Walgreen’s Lubricant Balance eyedrops (WLB group). Participants were 18– 65 years of age, had a total score of 20– 55 inclusive on the Symptom Assessment iN Dry Eye (SANDE) questionnaire at the screening visit, and were not current contact lens wearers. Subjects were randomized to either Group. Data were collected for corneal and conjunctival staining, non-invasive tear break-up time (NITBUT), and global SANDE score.
Results: A total of 70 participants completed the study (35 in each group). After 2 weeks of eyedrop use, the Systane group had a significantly greater reduction in global SANDE score (− 9.9 ± 14.7) compared to the WLB group (− 4.13 ± 8.6; p = 0.05). Also, the Systane group had a significantly greater reduction in total staining score (− 2.8 ± 1.8) compared to the WLB group (− 0.9 ± 1.5; p < 0.001). In addition, the Systane group had a greater increase in NITBUT (3.1 ± 2.9) compared to the WLB group (2.2 ± 4.5), but this was not significant (p = 0.32).
Conclusion: The results of this study suggest that eyedrops with the same active ingredient, but different excipients, can have differences in performance. Participants reported less dry eye symptoms and presented with reduced clinical signs of dry eye with Systane Complete MDPF compared to those who used WLB. Systane Complete MDPF eyedrops may be a good option for practitioners to recommend for patients with mild to moderate symptoms of dry eye.
Plain Language Summary: Dry eye disease (DED) is characterized by, but not limited to, symptoms of dryness, irritation, and burning. First line treatment is often lubricating eyedrops, however, there are many options that can confuse both practitioners and patients. Further complicating eyedrop selection is that even products with the same active ingredient can have different inactive ingredients that may result in different outcomes for patients. Lubricating eyedrops containing propylene glycol have been demonstrated to achieve good clinical outcomes for patients. However, there is a lack of understanding on the efficacy of lubricating eyedrops with the same active ingredient, but different inactive ingredients. The purpose of this study is to compare MDPF two propylene glycol lubricating eyedrops that contain very different inactive ingredients. The results of this study suggest that eyedrops with the same active ingredient, but different inactive ingredients, can have differences in performance.
Keywords: systane, dry eye disease, propylene glycol, hydroxypropyl guar, phospholipid, castor oil, lipid
Introduction
Dry eye disease (DED) is a multifactorial ocular disorder that is characterized by, but not limited to, symptoms of dryness, irritation, and burning.1,2 The first line option in the management of DED is often lubricating eyedrops.3 However, there are a vast array of lubricating eyedrops available on the market which may confuse both practitioners and patients. In addition, there is a lack of scientific evidence comparing the multitude of options which makes recommending a specific drop for a specific DED patient difficult.2–4 Even products with the same active ingredient can have different inactive ingredients that may result in different outcomes for patients.
Systane Complete Multi-Dose Preservative Free (MDPF) eyedrops (Alcon Laboratories, Inc, Fort Worth, TX USA) contain propylene glycol 0.6% as the active ingredient. In addition, Systane Complete MDPF is a sterile white nanoemulsion containing propylene glycol, hydroxypropyl guar, mineral oil, dimyristoyl phosphatidylglycerol (a phospholid), polyoxyl 40 stearate, sorbitan tristearate, boric acid, sorbitol, and edetate disodium.5,6
Walgreens Lubricant Balance (WLB; Walgreen Co, Deerfield, IL USA) is a private label brand of eyedrops with the same active ingredient as Systane Complete MDPF (propylene glycol 0.6%).7 The inactive ingredients for WLB are boric acid, castor oil, disodium edetate hydrate, polyoxyethylene sorbitan monooleate, potassium chloride, purified water, sodium borate, and sodium chloride, as well as benzalkonium chloride (BAK), a preservative.7
The Symptom Assessment iN Dry Eye (SANDE) questionnaire asks participants to answer 2 questions using a visual analog scale.8 It asks about symptom (eyes feeling dry or irritated) frequency from “Rarely” to “All of the Time” and severity from “Very Mild” to “Very Severe”.8 The SANDE questionnaire has been demonstrated to be a reliable test of dry eye symptoms.8,9
Lubricating eyedrops containing propylene glycol have been demonstrated to achieve good clinical outcomes for patients.10–12 However, there is a lack of understanding on the efficacy of lubricating eyedrops with the same active ingredient, but different excipients. The purpose of this study is to compare MDPF two propylene glycol lubricating eyedrops that contain very different excipients.
Methods
An independent institutional review board approved the study (Salus IRB, approval number JM-23-02), as the study was conducted in private practice. Written informed consent was obtained from all subjects before participation. The study was conduction in accordance with the tenets of the Declaration of Helsinki, and Good Clinical Practice (GCP), and International Harmonization (ICH) guidelines. The study was registered in a clinical trials database (clinicaltrials.gov; NCT06219577).
This was a single site, prospective, double-masked, and randomized-controlled two-arm study of 2 lubricating eyedrops. Inclusion criteria were adults (age 18 to 65 inclusive) with mild to moderate symptoms of dry eye, which was defined as a score on the Symptom Assessment iN Dry Eye (SANDE) questionnaire of 20 to 55 inclusive at the screening visit. Subjects were excluded who had ocular anterior segment infection, inflammation, abnormality, or active disease, history of herpetic keratitis or ocular surgery, thermal meibomian gland expression procedure including Lipiflow, iLux, or TearCare, or blepharitis debridement procedure including BlephEx within 1 year prior to the screening visit, non-invasive tear break-up time (NITBUT) < 2 seconds or > 10 seconds (CA-800, Topcon Healthcare), sodium fluorescein staining < 3 (clinically normal eye) or > 10 (severe dry eye) using the NEI 5 zone scale, pregnant or lactating, currently using contact lenses, or had any change in eyedrop regimen in the last 90 days.
At the baseline visit, subjects were randomized to receive either Systane Complete MDPF (Systane Group) or Walgreen’s Lubricant Balance (WLB Group). Randomization was conducted using block randomization, which was determined prior to recruitment and applied to sequentially enrolled participants. Product labels were removed from the eyedrop bottles and both subjects and examiners were masked. Subjects were instructed to use the eyedrops four times per day for 2 weeks. Data were collected for corneal and conjunctival staining, NITBUT, and global SANDE score. The global SANDE score is determined by multiplying the frequency score by the severity score and taking the square root of the result. A lower score on the SANDE is indicative of lower frequency and severity of dry eye symptoms. Corneal and conjunctival staining were assessed with sodium fluorescein and Wratten filter using the Academy of Ophthalmology 5 quadrant scheme (central, nasal, temporal, superior, and inferior), with each quadrant graded (0–3) giving a total score of 0–15 per eye. Note that the nasal and temporal scores considered both the cornea and conjunctiva when scoring. One eye from each subject was randomly selected for staining and NIBUT analysis.
The primary endpoint was to compare the change in total score from baseline to 2 weeks on the SANDE questionnaire between groups. Other endpoints included change in corneal staining from baseline to 2 weeks between groups, the change in NITBUT from baseline to 2 weeks between groups and change in total score from baseline to 1 week on the SANDE questionnaire between groups.
Statistical analyses were performed using the statistical software R (version 4.4.0; The R Foundation for Statistical Computing, Vienna, Austria). Normality was confirmed using the Shapiro–Wilk normality test. The change in total score on the SANDE questionnaire from baseline to 2 weeks was compared using the Welch two-sample t-test. A fixed-sequence methodology was used on the other endpoints. With this approach, the endpoints were ordered in the following sequence: change in corneal and conjunctival staining from baseline to 2 weeks, change in NITBUT from baseline to 2 weeks, change in total score on the SANDE questionnaire from baseline to 1 week. Testing began on the first endpoint in the sequence at the full alpha level and testing was stopped if an endpoint was not significant. A p-value ≤ 0.05 was considered significant. Using an estimated difference in means between groups (SANDE total score), a pooled standard deviation of 6, a beta of 0.1, and an alpha of 0.05, it was estimated that 32 subjects would be needed. To account for dropout and to increase the power of the study, the sample was increased to 35 subjects in each group.
Results
Thirty-five (35) subjects were enrolled in each group, for a total of 70. Of the 35, 25 were female and 10 male in the Systane group and 18 were female and 17 were male in the WLB group. Mean age was 41.8 ± 14.2 years in the Systane group and 39.4 ± 15.1 years in the WLB group. There were no adverse events related to either eyedrop.
Table 1 summarizes the SANDE scores at baseline, and after 1 and 2 weeks of use. Both the Systane and WLB groups had improved scores on the SANDE questionnaire after 1 and 2 weeks of eyedrop use compared to baseline. The change in score was higher in the Systane group, which was significant after 2 weeks of use (p = 0.05). Fixed-sequence testing was stopped before the significance for the change in baseline to week 1 could be determined.
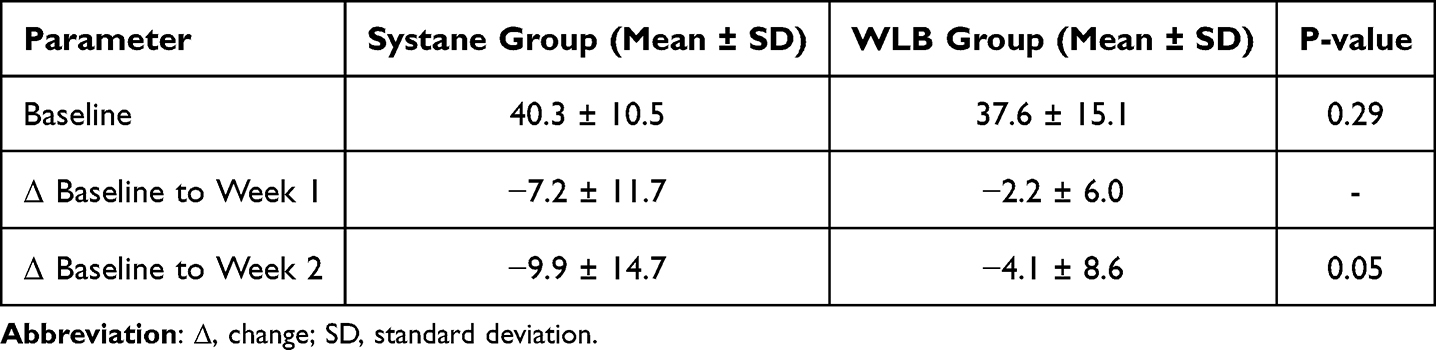 |
Table 1 Baseline and Changes in Score on the SANDE Questionnaire |
Table 2 summarizes the sodium fluorescein staining scores at baseline, and after 2 weeks of eyedrop use. The Systane group had a significantly higher score at baseline (p < 0.05). Both the Systane and WLB groups had improved scores after 2 weeks of eyedrop use compared to baseline. The change in score was significantly higher in the Systane group after 2 weeks of eyedrop use (p < 0.001).
 |
Table 2 Baseline and Changes in Corneal and Conjunctival Staining |
Table 3 summarizes the NITBUT at baseline, and after 2 weeks of eyedrop use. Both the Systane and WLB groups had improved scores after 2 weeks of eyedrop use compared to baseline. The change in NITBUT was numerically higher in the Systane group after 2 weeks of use but was not statistically significant (p = 0.32).
 |
Table 3 Baseline and Changes in NITBUT |
Discussion
With many lubricating eyedrops available, it can be confusing for patients to know which drops to use. Product labelling can also add to the uncertainty. For example, the package insert for WLB eyedrops states “Compare to Systane Balance Lubricant Eye Drops active ingredient” which may imply that lubricating eyedrops with the same active ingredient will perform the same.7 This study compared changes in dry eye symptoms using the SANDE questionnaire as well as corneal and conjunctival staining between Systane Complete MDPF and WLB eyedrops. The eyedrops have the same active ingredient (propylene glycol 0.6%), but different inactive ingredients. In general, this study provides clinical evidence that Systane Complete MDPF may be more effective in relieving dry eye symptoms and decreasing ocular surface staining than WLB, which may be due to differences in the inactive ingredients.
There are two notable differences in the inactive ingredients between these eyedrops. The first is BAK, a preservative, which is only found in the WLB eyedrops. Many tissue culture, animal studies, and clinical studies have demonstrated the negative effects of BAK on ocular tissues.13–18 Of particular relevance for this study are the increased symptoms related to DED with the use of BAK, such as reported discomfort and tearing, corneal and conjunctival staining, and higher scores (indicative of more disability) on the ocular surface disease index (OSDI) questionnaire.17,18 It is also worth noting that Systane Complete MDPF contains hydroxypropyl guar, with the aim to increase the retention time of the active ingredient (propylene glycol 0.6%) on the ocular surface.5,6 In addition, Systane Complete MDPF includes dimyristoyl phosphatidylglycerol, which is a proprietary phospholipid, compared to the castor oil in the WLB eyedrop.11
Both Systane Complete MDPF and WLB groups had a lower mean score on the SANDE questionnaire at 2 weeks compared to baseline. This was a mean change of 10 and 4 compared to baseline for the Systane and WLB groups, respectively. We are not aware of any other studies comparing Systane Complete MDPF to a private label brand of eyedrops. However, there have been other reports of clinical outcomes with Systane Complete MDPF. Muntz et al12 observed an improvement on the SANDE questionnaire of 25 compared to baseline immediately after instilling Systane Complete eyedrops. Craig et al11 reported an improvement on the SANDE score of approximately 10 compared to baseline after 30 days, similar to our study results at 2 weeks. Yeu et al10 used a different visual analog scale and observed that ocular discomfort score was reduced by 17 after 28 days compared to baseline when using Systane Complete MDPF. Differences in our study may be explained by the lower sample size or different patient populations.
The Systane Complete MDPF and WLB groups had lower corneal and conjunctival staining scores after 2 weeks of eyedrop use compared to baseline; a mean change of 3 and 1, respectively. Craig et al11 observed no change in corneal or conjunctival staining scores after 30 days of eyedrop use compared to baseline for Systane Complete but did after 120 days. Differences in our study may be explained by the lower sample size (35 compared to 50) or different patient populations.
The Systane Complete and WLB groups also had lower NITBUT after 2 weeks of eyedrop use compared to baseline; a mean change of 3.1 seconds and 2.2 seconds, respectively. Yeu et al10 observed that Systane Complete increased tear film break-time by 1.5 seconds at 2 weeks compared to baseline, similar to our study, although the sample was higher in their study (134 subjects). Muntz et al12 reported that Systane Complete increased tear film break-time by 2.8 seconds immediately after instillation compared to baseline, similar to our study.
A limitation of this study was the relatively short follow period. A time period of 2 weeks gives a good indication of short-term symptom relief for patients, but we are not able to draw conclusions about the long-term clinical outcomes between Systane Complete and WLB eyedrops. In addition, only subjects with mild to moderate symptoms of dry eye were included, thus we are also not able to draw conclusions about the clinical outcomes of the two groups in cases of severe dry eye symptoms. Finally, there was no data collected on the subtype of dry eye (aqueous-deficient, evaporative, or mixed).
In conclusion, the results of this study suggest that eyedrops with the same active ingredient, but different excipients, can have differences in performance. Participants reported less dry eye symptoms and presented with reduced clinical signs of dry eye with Participants subjectively and objectively exhibited less dry eye symptoms after using Systane Complete MDPF compared to those who used WLB. Systane Complete MDPF eyedrops may be a good option for practitioners to recommend for patients with mild to moderate symptoms of dry eye.
Data Sharing Statement
Data are not available for sharing.
Funding
This study was supported with an investigator-initiated study grant (89908509) from Alcon Vision, LLC, Fort Worth, TX.
Disclosure
The authors report no other conflict of interest for this work.
References
1. Simpson TL, Situ P, Jones LW, Fonn D. Dry eye symptoms assessed by four questionnaires. Optometry Vision Sci. 2008;85(8):692–699. doi:10.1097/OPX.0b013e318181ae36
2. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
3. Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database Syst Rev. 2016;2(2):CD009729. doi:10.1002/14651858.CD009729.pub2
4. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
5. Garofalo R, Kunnen C, Rangarajan R, Manoj V, Ketelson H. Relieving the symptoms of dry eye disease: update on lubricating eye drops containing hydroxypropyl-guar. Clin Exp Optom. 2021;104(8):826–834. doi:10.1080/08164622.2021.1925208
6. Srinivasan S, Williams R. Propylene glycol and hydroxypropyl guar nanoemulsion - safe and effective lubricant eye drops in the management of dry eye disease. Clin Ophthalmol. 2022;16:3311–3326. doi:10.2147/OPTH.S377960
7. Walgreens. Eye Drops Lubricant Balance (Package Insert). USA; 2024.
8. Schaumberg DA, Gulati A, Mathers WD, et al. Development and validation of a short global dry eye symptom index. Ocul Surf. 2007;5(1):50–57. doi:10.1016/S1542-0124(12)70053-8
9. Gulati A, Sullivan R, Buring JE, Sullivan DA, Dana R, Schaumberg DA. Validation and repeatability of a short questionnaire for dry eye syndrome. Am J Ophthalmol. 2006;142(1):125–131. doi:10.1016/j.ajo.2006.02.038
10. Yeu E, Silverstein S, Guillon M, et al. Efficacy and safety of phospholipid nanoemulsion-based ocular lubricant for the management of various subtypes of dry eye disease: a phase IV, multicenter trial. Clin Ophthalmol. 2020;14:2561–2570. doi:10.2147/OPTH.S261318
11. Craig JP, Muntz A, Wang MTM, et al. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: a six-month multicentre, double-masked randomised controlled trial. Ocul Surf. 2021;20:62–69. doi:10.1016/j.jtos.2020.12.006
12. Muntz A, Marasini S, Wang MTM, Craig JP. Prophylactic action of lipid and non-lipid tear supplements in adverse environmental conditions: a randomised crossover trial. Ocul Surf. 2020;18(4):920–925. doi:10.1016/j.jtos.2020.08.004
13. Ammar DA, Noecker RJ, Kahook MY. Effects of benzalkonium chloride-preserved, polyquad-preserved, and sofZia-preserved topical glaucoma medications on human ocular epithelial cells. Adv Ther. 2010;27(11):837–845. doi:10.1007/s12325-010-0070-1
14. Izzotti A, La Maestra S, Micale RT, Longobardi MG, Sacca SC. Genomic and post-genomic effects of anti-glaucoma drugs preservatives in trabecular meshwork. Mutat Res. 2015;772:1–9. doi:10.1016/j.mrfmmm.2014.11.006
15. Kahook MY, Noecker RJ. Comparison of corneal and conjunctival changes after dosing of travoprost preserved with sofZia, latanoprost with 0.02% benzalkonium chloride, and preservative-free artificial tears. Cornea. 2008;27(3):339–343. doi:10.1097/ICO.0b013e31815cf651
16. Kim JH, Kim EJ, Kim YH, et al. In vivo effects of preservative-free and preserved prostaglandin analogs: mouse ocular surface study. Korean J Ophthalmol. 2015;29(4):270–279. doi:10.3341/kjo.2015.29.4.270
17. Uusitalo H, Egorov E, Kaarniranta K, Astakhov Y, Ropo A. Benefits of switching from latanoprost to preservative-free tafluprost eye drops: a meta-analysis of two Phase IIIb clinical trials. Clin Ophthalmol. 2016;10:445–454. doi:10.2147/OPTH.S91402
18. Tomic M, Kastelan S, Soldo KM, Salopek-Rabatic J. Influence of BAK-preserved prostaglandin analog treatment on the ocular surface health in patients with newly diagnosed primary open-angle glaucoma. Biomed Res Int. 2013;2013:603782. doi:10.1155/2013/603782
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.