Back to Journals » Clinical Ophthalmology » Volume 14
Comparison of Biometry Measurements Using Standard Partial Coherence Interferometry versus New Scheimpflug Tomography with Integrated Axial Length Capability
Authors Haddad JS ![]() , Barnwell E, Rocha KM
, Barnwell E, Rocha KM ![]() , Ambrosio Jr R
, Ambrosio Jr R ![]() , Waring IV GO
, Waring IV GO
Received 11 November 2019
Accepted for publication 10 December 2019
Published 4 February 2020 Volume 2020:14 Pages 353—358
DOI https://doi.org/10.2147/OPTH.S238112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jorge Selem Haddad,1,2 Eliza Barnwell,1 Karolinne Maia Rocha,1 Renato Ambrosio Jr,2,3 George O Waring IV4
1Storm Eye Institute, Medical University of South Carolina, Charleston, SC, USA; 2Universidade Federal de São Paulo, São Paulo, Brazil; 3Universidade Federal do Estado do Rio de Janeiro, Rio de Janeiro, Brazil; 4Waring Vision Institute, Mt. Pleasant, SC, USA
Correspondence: Jorge Selem Haddad
Storm Eye Institute, Medical University of South Carolina, 167 Ashley Ave, Charleston, SC 29425, USA
Tel +1 843 327 7934
Email [email protected]
Purpose: To compare biometry measurements obtained by a partial interferometer biometer (IOLMaster 500) to the new Scheimpflug tomography with an integrated axial length biometer module (Pentacam AXL).
Patients and Methods: Cataract patients who underwent biometric measurements with the IOL Master 500 and the Pentacam AXL from July to November 2017 were enrolled in this study. Comparisons were performed for axial length (AL), keratometry (K), and anterior chamber depth (ACD). The Pearson correlation coefficient and the 95% limits of agreement (LoA) were calculated. Paired Student’s t-tests and Bland-Altman plots were used to assess the differences between devices.
Results: One hundred and sixty-six eyes of 92 patients were analyzed. There were no statistically significant differences in AL (p=0.558) or flat K (p=0.196) values between the IOL Master 500 and Pentacam AXL measurements. Statistically significant differences were found between the two devices with respect to steep K, ACD, and mean K measurements (p< 0.001).
Conclusion: Both devices provided similar measurements of AL and flat K, though there were statistically significant differences in ACD, steep K, and mean K measurements.
Keywords: anterior chamber depth, axial length, biometry, IOLMaster 500, partial coherence interferometry, pentacam AXL
Introduction
Accurate biometry measurements are critical to achieving target refraction of emmetropia following cataract surgery. New surgical techniques in conjunction with technological advances have improved the accuracy of biometry data and intraocular lens calculations.1,2
A number of devices have proven to be reliable in calculating pre-cataract surgery measurements, including low-coherence reflectometry (Lenstar LS 900, Haag-Streit AG), Scheimpflung camera-based devices (Galilei G6, Ziemer Ophthalmic Systems AG; Pentacam, Oculus, Wetzlar, Germany)3–5 and partial coherence interferometry (IOLMaster 500 and 700, Zeiss, Oberkochen, Germany).6 The IOLMaster device is currently the most widely used device for biometric measurements.7
The Pentacam is a non-contact tomographer that provides tomographic maps of the anterior and posterior corneal surfaces, corneal thickness, and anterior chamber depth (ACD) by using a rotating Scheimpflug camera to image the anterior segment of the eye with proven efficacy and accuracy.8,9 The new Pentacam AXL combines the Scheimpflug camera device with an additional partial coherence interferometry (PCI) module to measure axial length (AL) in conjunction with anterior segment biometry measurements.10 While the IOL Master 500 and the Pentacam AXL both use PCI technology to measure AL, the IOL Master 500 measures only the anterior corneal curvature to calculate corneal power, whereas the Scheimpflug device has the ability to measure posterior corneal curvature in addition to anterior corneal curvature. The IOL Master 700 now has the ability to measure both the anterior and posterior corneal curvature with integrated OCT, and metrics have been developed for total keratometric measurements of both surfaces. This is a valuable capability of the Pentacam, as studies have shown that ignoring posterior astigmatism can lead to miscalculation of corneal power.11 Studies have compared the IOL Master 700 and Pentacam AXL; however, to the best of our knowledge, this is the most extensive comparative analysis of the IOL Master 500 and Pentacam AXL, which is essential due to the widespread use of the IOL Master 500. The purpose of this study was to compare ocular biometry measurements obtained by partial coherence interferometry (IOLMaster 500) and the new Pentacam AXL module.
Materials and Methods
This retrospective study enrolled 92 patients (166 eyes) with cataracts who underwent femtosecond laser-assisted cataract surgery at the Waring Vision Institute, South Carolina, between July 2017 and November 2017. The study protocol was approved by the Medical University of South Carolina Institutional Review Board. Informed consent was waived as the data were collected as a part of standard practice of care and adhered to the tenets of the Declaration of Helsinki. Exclusion criteria included (1) patients with corneal diseases that may interfere with the capture of topographic measures (eg, scars), (2) patients who were pregnant or breastfeeding, (3) history of ocular herpes, (4) history of corneal dysplasia or conjunctival lesions, (5) patients taking medications that may interfere with corneal surface (eg, Isotretinoin, Roacutan®), or (5) any other severe anterior or posterior segment pathology that may interfere with measurement accuracy.
Optical biometry measurements (IOLMaster 500, software version 7.99) including AL, keratometry (K), and ACD were correlated with Pentacam AXL (software version 6.08r19) AL, K (within the central 3-mm optical zone), and ACD measurements. Pentacam AXL measurements were taken automatically to avoid operator-dependent factors.
Statistical Analysis
Data analysis was performed using R 3.4.1 (R Core Team, 2017, Vienna, Austria). Paired Student’s t-tests were conducted for all pairs. Correlations are presented as Bland-Altman plots and by the Lin coefficient of agreement (rc), where values close to 1 indicate good agreement. In the Bland-Altman plots, the dashed lines indicate the 95% limits of agreement for the mean difference between the measurements of the compared devices (Pentacam AXL and IOLMaster 500).
Results
One hundred and sixty-six eyes of ninety-two patients were enrolled in this study. The mean age was 69.3 ± 9.2 years (range 26 to 88 years). Of these individuals, 20 patients had measurements performed only in one eye, while 73 patients had both eyes measured. Since the study intended to assess the agreement between the devices, we considered each eye to be independent of the other with a total sample of 73 * 2 + 20 = 166 eyes.
Table 1 shows the AL, ACD, and K measurements taken by both devices. We reported the p-values, upper and lower limits of agreement of corneal curvature (flat and steep Ks), ACD, and AL for measurements taken with the IOL Master 500 and Pentacam AXL.
 |
Table 1 Means and Standard Deviations of the Differences |
No statistically significant differences were observed for mean AL or flat K measurements between the IOL Master 500 and the new AXL module (Figures 1 and 2). The Bland–Altman analysis of AL measured with the Pentacam AXL and the IOL Master 500 showed a mean difference of −0.002 mm, an upper limit of agreement of 0.086, and a lower limit of agreement of −0.09, with p = 0.058. For flat K, there was a mean difference of −0.064 mm, an upper limit of agreement of 0.0678, and a lower limit of agreement of −0.807, with p = 0.058. Statistically significant differences were found for mean K (p<0.001), steep K (p<0.001), and ACD (p<0.001 (Figures 3–5)). Also, we performed an analysis and divided the AL into a subgroup for small, medium, and long eyes. We did not find any statistical differences.
 |
Figure 1 Bland-Altman plot for axial length according to Pentacam and IOL Master measurements. |
 |
Figure 2 Bland-Altman plot for keratometry flat according to Pentacam and IOL Master measurements. |
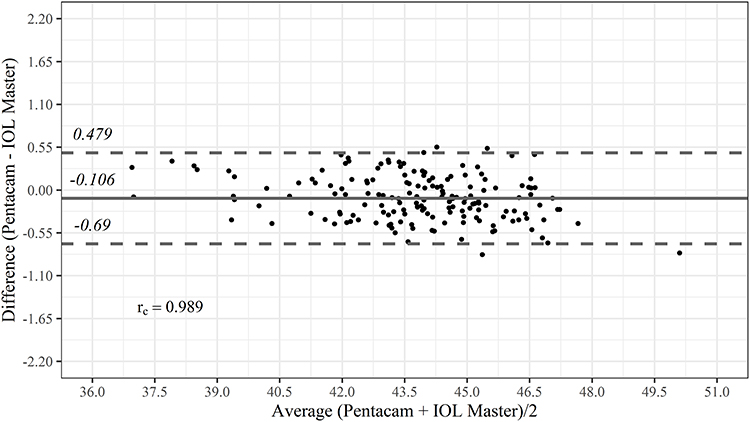 |
Figure 3 Bland-Altman plot for keratometry mean according to Pentacam and IOL Master measurements. |
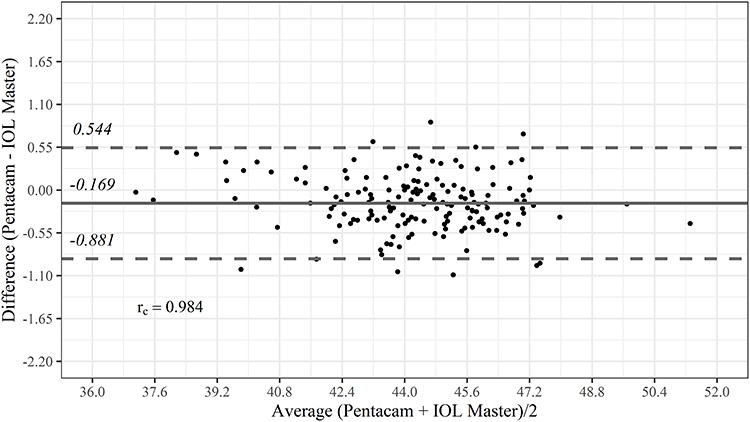 |
Figure 4 Bland-Altman plot for steep keratometry according to Pentacam and IOL Master measurements. |
 |
Figure 5 Bland-Altman plot for anterior chamber depth according to Pentacam and IOL Master measurements. |
The mean numerical difference in mean K was −0.106 D (range −0.150 to −0.061 D), while the mean numerical difference of steep K was −0.169 D (range −0.223 to −0.114 D). The mean numerical difference for ACD was 0.049 mm (range 0.027 to 0.072 mm).
Discussion
Scheimpflug imaging is widely used in clinical practice due to its accurate and reliable measurements of the anterior segment of the eye. The Pentacam provides accurate K and ACD measurements, as well as a variety of indices to help diagnose ectasias and corneal diseases.12 The newest version comes with an additional module, the AXL, which measures the AL from the anterior cornea vertex to the retinal pigment epithelium for biometry calculation. With the integration of high-resolution tomography and optical biometry, the Pentacam AXL has a number of potential advantages. Advanced generation intraocular lens calculators, including post corneal refractive calculators, are integrated and allow for real-time calculation of IOL powers. Total K measurements of not only the anterior and posterior corneal surface powers, but also the relative meridional contribution, are also novel and may aid in the evaluation of posterior corneal astigmatism. As described by Koch and Kohnen, the magnitude of posterior corneal astigmatism is approximately 0.30 D. Taking this information into account when calculating toric IOL in patients with astigmatism may lead to more accurate results.11,13 Furthermore, the ability to have a combined device can streamline workflow, efficiencies, space, and cost. However, the validation of biometric data is required to justify the use of a single consolidated device.
The IOL Master 500 uses the principle of partial coherence interferometry, and its successor, the IOL Master 700, incorporates optical coherence tomography.14,15 Both devices produce similar results, but the latter has been shown to have higher accuracy for posterior subcapsular and dense cataracts.7 The IOL Master projects six light spots onto the cornea in a hexagonal pattern to assess anterior corneal curvature and performs measurements using a 2.3-mm radius. In contrast, the Pentacam’s simulated K measurements are generated using anterior and posterior corneal elevation values in the central 3 mm.16 Repeatability and accuracy of both the IOL Master and Pentacam have been described in the literature.16
Shajari et al found no statistically significant differences in K, ACD, or AL among IOL Master 500, IOL Master 700, and Pentacam AXL measurements in a sample size of 79 eyes.17 Another recent study by Sel et al found that measures from the IOL Master 700 and Pentacam AXL devices may be interchangeable for ACD and AL measurements, but measurements of mean K were statistically and clinically different.18 Likewise, Dong et al found statistically significant differences in K between the Pentacam and IOLMaster 500, while another study showed that Pentacam’s simulated K was found to be within less than 0.50 D of the IOLMaster 500 95% of the time.19,20
Our study is one of the largest in the literature comparing the IOLMaster 500 and Pentacam AXL module, with a sample size of 166 eyes. In this study, we found no significant difference in AL or flat K measurements with the Pentacam AXL and IOL Master 500, though we did find statistically significant differences in mean K, steep K, and ACD (Figures 3–5). Since both devices use PCI to measure AL, it is not surprising that the calculations of AL were similar. Interestingly, despite measuring corneal curvature using different technologies, the flat K values obtained by the IOL Master and the new Pentacam module were not statistically significantly different. However, the differences in mean and steep K and ACD could have essential implications on IOL calculations and may signify that these two devices should not be used interchangeably for IOL calculations.
Conclusion
In conclusion, the IOLMaster 500 and the Pentacam AXL provide similar measurements of AL, though K and ACD measurements are statistically different. Given that the Pentacam uses partial coherence interferometry which takes into account the posterior as well as the anterior curvature of the cornea, it has been shown to provide accurate measurements of AL. The Pentacam AXL appears to be suitable for use as an all-inclusive optical biometer and corneal tomographer, as it combines PCI technology for obtaining accurate AL measurements with Scheimpflug technology to obtain ACD and K measurements.
Abbreviations
ACD, anterior chamber depth; AL, axial length; K, keratometry; PCI, partial coherence interferometry.
Disclosure
Dr. Ambrosio and Dr. Waring are consultants for Oculus®, Wetzlar, Germany from which they received grants and persona fees. Dr. Ambrosio also reports personal fees, non-financial support from Zeiss, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmol Scand. 2007;85(5):472–485. doi:10.1111/j.1755-3768.2007.00879.x
2. Sahin A, Hamrah P. Clinically relevant biometry. Curr Opin Ophthalmol. 2012;23(1):47–53. doi:10.1097/ICU.0b013e32834cd63e
3. Ventura BV, Ventura MC, Wang L, Koch DD, Weikert MP. Comparison of biometry and intraocular lens power calculation performed by a new optical biometry device and a reference biometer. J Cataract Refract Surg. 2017;43(1):74–79. doi:10.1016/j.jcrs.2016.11.033
4. Cruysberg LP, Doors M, Verbakel F, Berendschot TT, De Brabander J, Nuijts RM. Evaluation of the lenstar LS 900 non-contact biometer. Br J Ophthalmol. 2010;94(1):106–110. doi:10.1136/bjo.2009.161729
5. Hoffer KJ, Shammas HJ, Savini G. Comparison of 2 laser instruments for measuring axial length. J Cataract Refract Surg. 2010;36(4):644–648. doi:10.1016/j.jcrs.2009.11.007
6. Olsen T. Improved accuracy of intraocular lens power calculation with the Zeiss IOLMaster. Acta Ophthalmol Scand. 2007;85(1):84–87. doi:10.1111/j.1600-0420.2006.00774.x
7. Akman A, Asena L, Güngör SG. Evaluation and comparison of the new swept source OCT-based IOLMaster 700 with the IOLMaster 500. Br J Ophthalmol. 2016;100(9):1201–1205. doi:10.1136/bjophthalmol-2015-307779
8. Barkana Y, Gerber Y, Elbaz U, et al. Central corneal thickness measurement with the Pentacam Scheimpflug system, optical low-coherence reflectometry pachymeter, and ultrasound pachymetry. J Cataract Refract Surg. 2005;31(9):1729–1735. doi:10.1016/j.jcrs.2005.03.058
9. Lackner B, Schmidinger G, Skorpik C. Validity and repeatability of anterior chamber depth measurements with Pentacam and Orbscan. Optom Vis Sci. 2005;82(9):858–861. doi:10.1097/01.opx.0000177804.53192.15
10. Pereira JMM, Neves A, Alfaiate P, Santos M, Aragao H, Sousa JC. Lenstar(R) LS 900 vs Pentacam(R)-AXL: comparative study of ocular biometric measurements and intraocular lens power calculation. Eur J Ophthalmol. 2018;28(6):645–651. doi:10.1177/1120672118771844
11. Tonn B, Klaproth OK, Kohnen T. Anterior surface-based keratometry compared with Scheimpflug tomography-based total corneal astigmatism. Invest Ophthalmol Vis Sci. 2014;56(1):291–298. doi:10.1167/iovs.14-15659
12. Wegener A, Laser-Junga H. Photography of the anterior eye segment according to Scheimpflug’s principle: options and limitations – a review. Clin Exp Ophthalmol. 2009;37(1):144–154. doi:10.1111/ceo.2009.37.issue-1
13. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
14. Vogel A, Dick HB, Krummenauer F. Reproducibility of optical biometry using partial coherence interferometry: intraobserver and interobserver reliability. J Cataract Refract Surg. 2001;27(12):1961–1968. doi:10.1016/S0886-3350(01)01214-7
15. Fontes BM, Fontes BM, Castro E. Intraocular lens power calculation by measuring axial length with partial optical coherence and ultrasonic biometry. Arq Bras Oftalmol. 2011;74:166–170. doi:10.1590/S0004-27492011000300004
16. Visser N, Berendschot TT, Verbakel F, de Brabander J, Nuijts RM. Comparability and repeatability of corneal astigmatism measurements using different measurement technologies. J Cataract Refract Surg. 2012;38(10):1764–1770. doi:10.1016/j.jcrs.2012.05.036
17. Shajari M, Cremonese C, Petermann K, Singh P, Muller M, Kohnen T. Comparison of axial length, corneal curvature, and anterior chamber depth measurements of 2 recently introduced devices to a known biometer. Am J Ophthalmol. 2017;178:58–64. doi:10.1016/j.ajo.2017.02.027
18. Sel S, Stange J, Kaiser D, Kiraly L. Repeatability and agreement of Scheimpflug-based and swept-source optical biometry measurements. Cont Lens Anterior Eye. 2017;40(5):318–322. doi:10.1016/j.clae.2017.03.007
19. Woodmass J, Rocha G. A comparison of Scheimpflug imaging simulated and Holladay equivalent keratometry values with partial coherence interferometry keratometry measurements in phakic eyes. Can J Ophthalmol. 2009;44(6):700–704. doi:10.3129/i09-172
20. Dong J, Tang M, Zhang Y, et al. Comparison of anterior segment biometric measurements between Pentacam HR and IOLMaster in normal and high myopic eyes. PLoS ONE. 2015;10(11):e0143110. doi:10.1371/journal.pone.0143110
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.