Back to Journals » Clinical Ophthalmology » Volume 16
Comparison of Barrett Toric Calculations Using Measured and Predicted Posterior Corneal Astigmatism in Cataract Surgery Patients
Authors Lukewich MK, Murtaza F ![]() , Somani S
, Somani S ![]() , Tam ES
, Tam ES ![]() , Chiu HH
, Chiu HH ![]()
Received 30 November 2021
Accepted for publication 16 May 2022
Published 1 June 2022 Volume 2022:16 Pages 1739—1751
DOI https://doi.org/10.2147/OPTH.S351011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mark K Lukewich,1 Fahmeeda Murtaza,1 Sohel Somani,2– 4 Eric S Tam,2– 4 Hannah H Chiu2– 4
1Temerty Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada; 2William Osler Health System, Brampton, Ontario, Canada; 3Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, Ontario, Canada; 4Uptown Eye Specialists, Vaughan, Ontario, Canada
Correspondence: Hannah H Chiu, Uptown Eye Specialists, 401-7900 Hurontario Street, Brampton, Ontario, L6Y 0P6, Canada, Tel +1 416 292-0330, Fax +1 416 292-0331, Email [email protected]
Aim: To compare residual astigmatism prediction errors across Barrett toric calculations using predicted posterior corneal astigmatism (PCA) and PCA measured using the IOL Master 700 with total keratometry (IOLM).
Methods: A retrospective cohort study was undertaken on patients with corneal astigmatism and no other ocular comorbidities that underwent uneventful refractive femtosecond laser-assisted cataract surgery with toric IOL implantation between May 2019 and November 2019. Toric calculations were performed using the Barrett toric calculator and the following values: predicted PCA with anterior corneal measurements from Pentacam, IOLM standard keratometry (SK), OPD scan, and median measurements from these devices; predicted PCA with IOLM total keratometry (TK); and measured PCA with IOLM SK or IOLM TK. Residual astigmatism prediction error was calculated for each device and method of calculation at postoperative month 1 and 3 using the astigmatism double angle plot tool.
Results: A total of 24 eyes, 10 with-the-rule (WTR), 10 against-the-rule (ATR) and 4 oblique astigmatism, from 24 patients were included in this study. PCA ranged from 0.00 to 0.67 D with a mean of 0.24 ± 0.15 D in all eyes. PCA was significantly greater in WTR eyes (0.32 D) compared to ATR eyes (0.16 D; p < 0.05). In ATR eyes, calculations made using IOLM SK and measured PCA had significantly lower total corneal astigmatism and toric IOL cylinder power compared to calculations made using Pentacam and IOLM TK (p < 0.05). No significant difference in mean absolute or centroid residual astigmatism prediction error was observed across devices or calculation methods. The percentage of eyes with absolute astigmatism prediction errors ≤ 0.5 D was not significantly different across groups.
Conclusion: Barrett toric calculations using predicted PCA and PCA measured using IOLM produced comparable residual astigmatism prediction errors. The incorporation of median measurements did not significantly impact calculation accuracy.
Keywords: astigmatism measurement, femtosecond laser-assisted cataract surgery, toric intraocular lens calculator, Barrett toric calculator
Introduction
Preoperative corneal astigmatism is common among cataract patients.1 It is estimated that approximately 30–45% of patients requiring cataract surgery have greater than 1.0 D of corneal astigmatism, with 15–20% of patients exhibiting corneal astigmatism greater than 1.5 D.1–3 Toric intraocular lenses (IOLs) have been shown to minimize residual corneal astigmatism and facilitate spectacle independence for distance vision following cataract surgery.4 Refractive outcomes are dependent on precise measurement of preoperative corneal astigmatism, accurate and reliable calculation of the ideal cylindrical power and axis of the toric IOL to be implanted, and optimal positioning of high-quality toric IOLs during cataract surgery.5 Despite ongoing advances in each of these areas, a recent meta-analysis found that the average residual astigmatism following toric IOL implantation ranges from 0.18 to 0.77 D.4
Several devices have been developed to measure corneal astigmatism for preoperative planning. The anterior corneal surface is optimally positioned for direct imaging and has been fundamental to our understanding of corneal astigmatism. Anterior corneal astigmatism can be accurately measured using various technologies and remains a prominent variable in toric IOL calculations. Nevertheless, calculations based on anterior corneal measurements alone lead to an overestimation of total corneal astigmatism in with-the-rule (WTR) eyes and an underestimation of total corneal astigmatism in against-the-rule (ATR) eyes, highlighting the important contribution of the posterior cornea to total corneal refractive power.6–10 Posterior corneal astigmatism (PCA) can be predicted using measurements of anterior corneal astigmatism and fixed anterior to posterior corneal thickness ratios, mathematical models and algorithms that have generally been derived from healthy, normal eyes.6,10–13 The posterior corneal surface can also be directly imaged to measure PCA in each individual patient. The IOL Master 700 with total keratometry (IOLM), for example, uses swept-source optical coherence tomography (SS-OCT) and telecentric keratometry to estimate PCA.14 IOLM also measures total corneal astigmatism, expressed as the total keratometry (TK) value, which can be incorporated into existing toric IOL calculators.15 Importantly, incorporation of both predicted or measured PCA into toric IOL calculations has been shown to significantly reduce postoperative refractive errors.8,11–13,16–28 However, the impact of using predicted PCA versus measured PCA on the accuracy of toric IOL calculations remains an area of active investigation.
The Barrett toric calculator is well-suited to address this important question, as PCA is incorporated into each calculation using either direct measurements from a suitable device or the predicted PCA derived from the Barrett toric calculator’s proprietary formula. Barrett toric calculations can be performed using measurements from several devices, enabling direct comparisons of calculation accuracy between different methods of assessing the anterior and posterior cornea. Median measurements taken from three devices can also be used for individual Barrett toric calculations. Importantly, the Barrett toric calculator has consistently been shown to produce low residual astigmatism prediction errors and is considered a reliable and accurate tool for preoperative planning.11,16–18,21,23,24,29–31
The present study was undertaken to assess the impact of using measured versus predicted PCA on the accuracy of toric IOL calculations in a patient cohort undergoing femtosecond laser-assisted cataract surgery (FLACS). Estimates of preoperative total corneal astigmatism and residual astigmatism prediction errors were compared across Barrett toric calculations made using predicted PCA and PCA measured using IOLM. For predicted PCA calculations, additional comparisons were made between Pentacam, OPD scan, IOLM and the median of these measurements to determine whether the method used to assess anterior corneal astigmatism impacts calculation accuracy. Barrett toric calculations performed using the newly developed TK value were also compared to calculations incorporating standard keratometry measurements from IOLM.
Subjects and Methods
Participants
The present study was approved by the William Osler Health System Research Ethics Board (WOHS REB). Given the retrospective nature of our study and the presentation of findings at the aggregate level, patient consent to review medical records was not required by the WOHS REB. All investigations conformed to the tenets of the Declaration of Helsinki. A retrospective chart review was performed between May and November 2019 to identify patients with regular corneal astigmatism that underwent femtosecond laser-assisted cataract surgery (FLACS) with the implantation of a toric IOL at a high-volume surgical center in Ontario, Canada. All efforts were made to maintain patient confidentiality. A unique identification code was applied to each study participant at the onset of data extraction, and all study data were stored in encrypted files to maintain confidentiality. Each study participant had a comprehensive ophthalmological examination as part of their preoperative assessment, including tonometry, slit-lamp biomicroscopy, uncorrected distance visual acuity (UDVA), best corrected distance visual acuity (CDVA), refractive error, and dilated stereoscopic examination of the posterior segment. Preoperative corneal astigmatism was measured using OPD Scan III (Nidek Technologies, Japan), Pentacam (Oculus Pentacam, Germany) and IOLM (Carl Zeiss Meditec Inc., Germany) for surgical planning. Participants were included in the study if they had a monofocal Tecnis toric IOL (Abbott Medical Optics Inc., USA) with a total cylindrical power of 1.0–4.5 D implanted during an uneventful FLACS, were seen in follow-up at 1 month and 3 months postoperatively and had a CDVA equal to or better than 20/40 on Snellen testing, or 0.3 LogMAR units. Participants were excluded from analysis if they had pre-existing ocular pathologies affecting visual acuity, including prior corneal surgeries, ocular trauma, corneal disease, glaucoma, diabetic retinopathy, age-related macular degeneration or other maculopathies. Participants that experienced surgical complications, had prior hard contact lens use, or that exhibited IOL decentration, tilt or misalignment postoperatively were also excluded. One eye from each participant was included in this study. Participants with any missing data both preoperatively and postoperatively were removed from analysis.
Estimation of Preoperative Corneal Astigmatism
Corneal astigmatism was measured by an experienced technician using OPD-Scan III, Pentacam and IOLM according to each manufacturer’s instructions. OPD Scan III measures corneal topography, pupil diameter and standard keratometry (SK) using a built-in Placido disk and refraction using dynamic skiascopy. Pentacam utilizes a rotating Scheimpflug camera to measure the topography of the anterior and posterior cornea, corneal thickness, SK, anterior chamber depth and pupil diameter. IOLM uses SS-OCT and telecentric keratometry to measure SK, corneal thickness, PCA, TK, axial length, anterior chamber depth, lens thickness and white-to-white distance.32
Anterior corneal astigmatism was estimated using SK values for IOLM and simulated keratometry (SimK) values for OPD scan and Pentacam obtained using a refractive index of 1.3375. The Barrett toric calculator v2.0 (available at https://calc.apacrs.org/toric_calculator20/Toric%20Calculator.aspx) was used to estimate total corneal astigmatism, optimal toric IOL cylinder power and axis, and predicted residual refractive astigmatism. For the OPD scan, Pentacam and IOLM SK groups, the measured anterior corneal flat and steep meridians and their respective axes were input into the calculator and PCA was predicted using the Barrett toric calculator’s proprietary formula. For the median measurement calculation, anterior corneal astigmatism measurements from OPD scan, Pentacam and IOLM SK were input into the Barrett toric calculator and predicted PCA was used. The IOLM SK with PCA group utilized SK values and PCA measured using IOLM for Barrett toric calculations. For the IOLM TK and IOLM TK with PCA groups, TK values from IOLM were used with predicted and measured PCA, respectively.
Measurements of axial length, anterior chamber depth, lens thickness and white-to-white distance were derived from IOLM for all Barrett toric calculations. Surgery-induced astigmatism (SIA) was estimated at 0.1 D at 200 for the right eye and 0.1 D at 40 for the left eye.33 The Tecnis toric IOL constant provided by the manufacturer was used for all calculations. The toric IOL power and alignment used in each surgery to achieve a refractive goal of emmetropia was determined by the surgeon based on all available data and surgeon preference.
Femtosecond Laser-Assisted Cataract Surgery
One of three experienced cataract surgeons (S.S., E.S.T., H.H.C.) performed each FLACS using a standard protocol with the implantation of a Tecnis toric IOL. The Catalys Precision Laser System was used to create a 2.5 mm main corneal incision, a 1.2 mm side-port incision, a 5.0 mm diameter anterior capsulotomy, steep meridian corneal markings, 4.5 mm diameter lens fragmentation with grid softening, and limbal relaxing incisions on the steep meridian, as appropriate for each case. Phacoemulsification was then performed and the toric IOL was inserted into the capsular bag and aligned with the steep meridian corneal markings. Toric IOL alignment was recorded at the time of surgery and reassessed at postoperative week 1, month 1 and month 3.
Calculation of Residual Astigmatism Prediction Error
The double-angle plot tool developed by Abulafia et al was used to estimate mean absolute and centroid residual corneal astigmatism prediction errors, as previously described.34 Briefly, subjective postoperative residual astigmatism was measured using manifest refraction performed at postoperative month 1 (POM1) and postoperative month 3 (POM3). The predicted residual astigmatism was estimated using the Barrett toric calculator and adjusted according to the cylindrical power of the implanted toric IOL and actual orientation measured postoperatively. The residual astigmatism prediction error was calculated by subtracting the predicted residual astigmatism at the corneal plane from the actual residual astigmatism at the corneal plane measured using manifest refraction.35 Vector analysis was used for all calculations.
Statistical Analysis
Participants were stratified according to anterior corneal steep meridian into WTR (steep axis between 60° and 120°), ATR (steep axis between 0° and 30° or 150–180°) and oblique astigmatism (steep axis between 31° and 59° or 121–149°) groups. Centroid residual astigmatism prediction errors were converted into x- and y-components and analyzed separately. Data normality was assessed using the Kolmogorov–Smirnov test and the Shapiro–Wilk normality test. Repeated measures ANOVAs with Bonferroni post-hoc testing, or Friedman tests with Dunns post-hoc testing for non-parametric data, were used for statistical comparisons between groups. Paired t-tests were used for comparison of PCA measurements between WTR and ATR eyes. Chi-squared analysis was used to compare the percentage of participants with astigmatism prediction errors of ≤ 0.25 D, ≤ 0.5 D, ≤ 0.75 D and ≤ 1.0 D across devices and calculation methods. All statistical tests were performed using GraphPad Prism 5.0 (GraphPad Software Inc., USA). Data is presented as mean ± standard deviation unless specified otherwise. Differences were considered statistically significant when p < 0.05.
Results
Participant Demographics
A total of 24 eyes from 24 participants were included in this study (Table 1). There were 11 females (45.8%) and 13 males (54.2%) with an average age of 66.4 ± 9.2 years (range 48 to 82 years). Axial length ranged from 22.2 to 27.8 mm with an average of 24.2 ± 1.4 mm. The average anterior chamber depth was 3.2 ± 0.4 mm (range 2.7 to 4.3 mm). Preoperative corneal astigmatism cylinder power ranged from 1.0 to 4.2 D with a mean absolute power of 1.69 ± 0.24 D for all eyes. Toric IOLs implanted during FLACS had an average spherical power of 18.7 ± 4.4 D and an average cylinder power of 2.1 ± 0.9 D. All participants received TECNIS toric model ZCT lenses with the following characteristics: ZCT100 (n = 4), ZCT150 (n = 7), ZCT225 (n = 6), ZCT300 (n = 5), ZCT375 (n = 1) and ZCT450 (n = 1). Ten eyes (41.7%) had WTR astigmatism, 10 eyes (41.7%) had ATR astigmatism and 4 eyes (16.6%) had oblique astigmatism. Given the small sample of eyes with oblique astigmatism, only ATR and WTR eyes were included in the subgroup analyses. In WTR eyes, preoperative corneal astigmatism cylinder power ranged from 1.13 to 4.2 D with a mean of 2.12 ± 0.89 D and a centroid of 1.9 D @ 86° ± 1.37 D. In ATR eyes, preoperative corneal astigmatism cylinder power ranged from 1.0 to 2.26 D with a mean of 1.43 ± 0.42 D and a centroid of 1.25 D @ 175° ± 0.85 D.
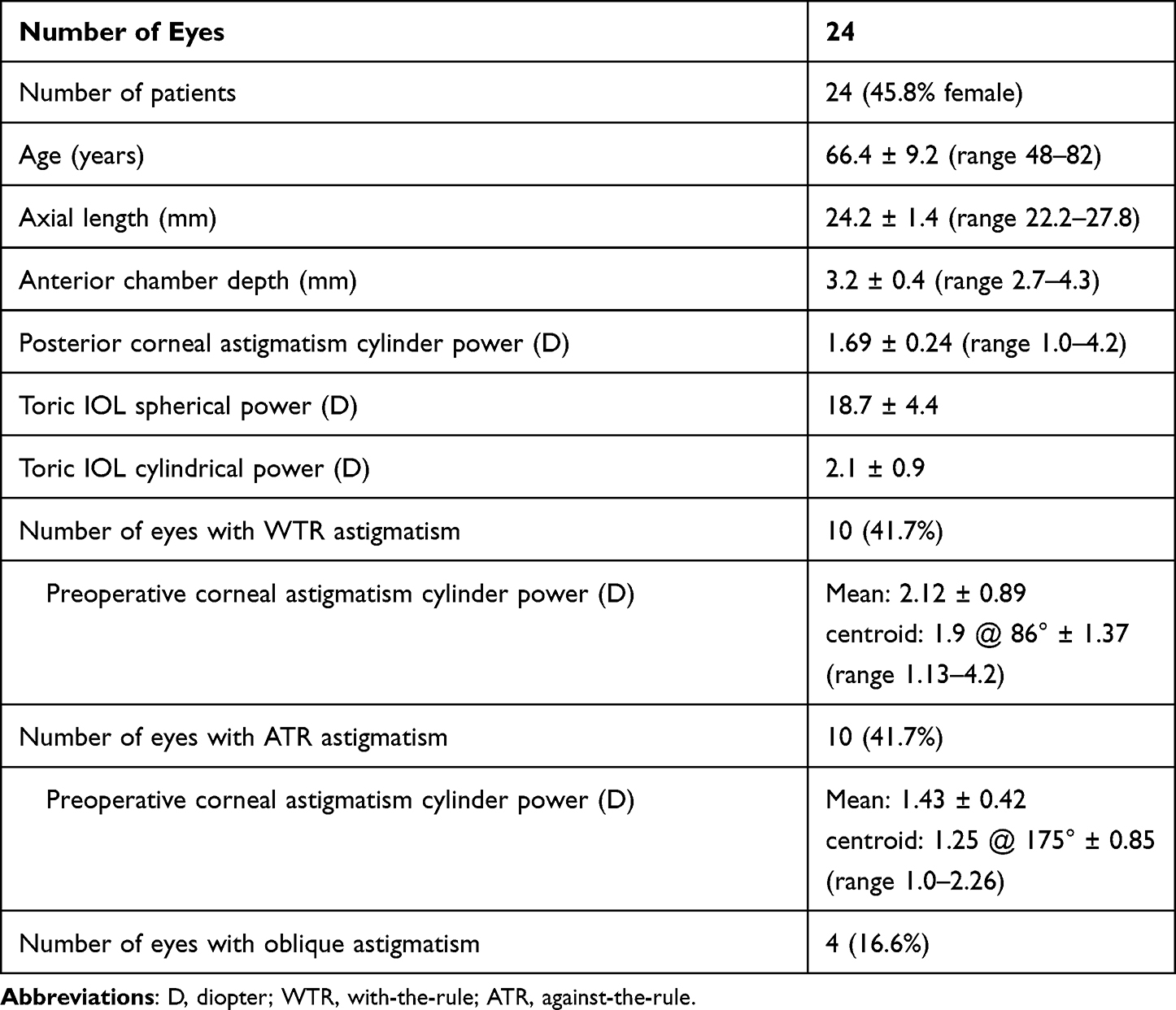 |
Table 1 Patient Demographic and Preoperative Data |
At POM1, UDVA was 0.08 ± 0.11 LogMAR units and CDVA was 0.03 ± 0.06 LogMAR units, and at POM3 UDVA was 0.10 ± 0.10 LogMAR units and CDVA was 0.04 ± 0.06 LogMAR units. Double angle plots of postoperative residual astigmatism are presented in Figure 1 for all, WTR and ATR eyes at POM1 and POM3.
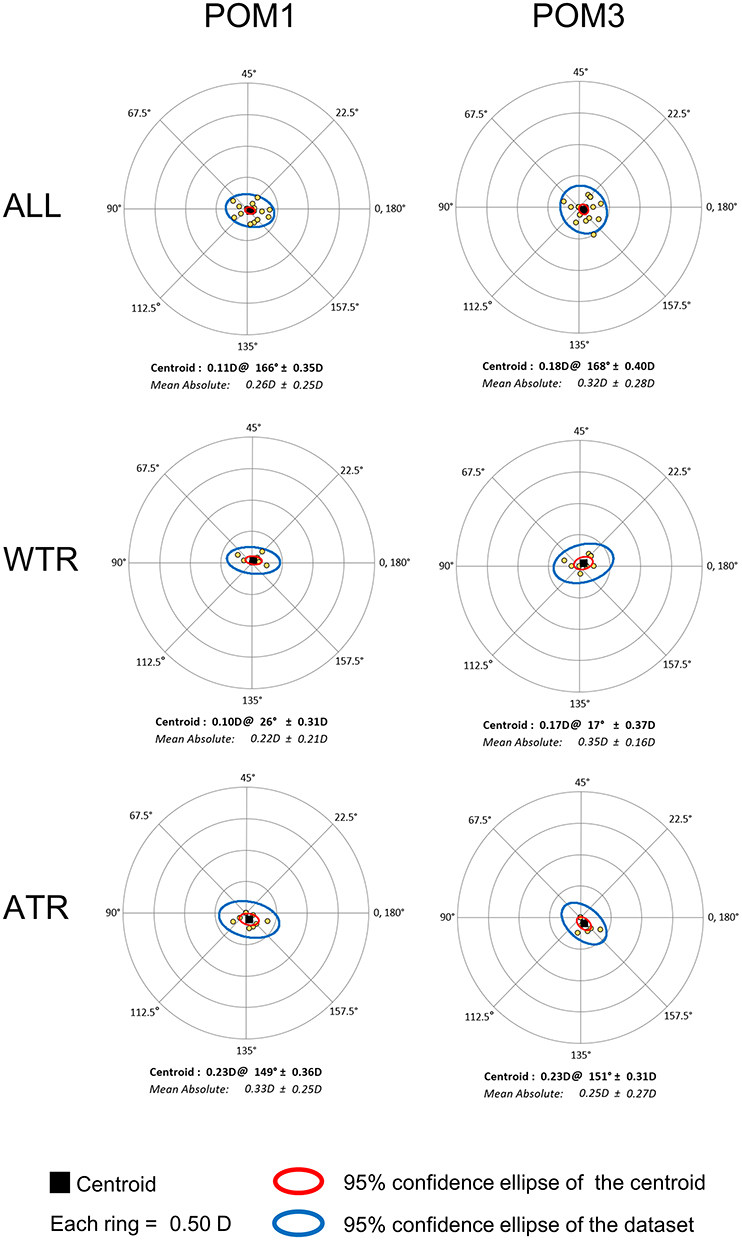 |
Figure 1 Postoperative residual astigmatism. Double-angle plots of postoperative residual astigmatism at postoperative month 1 and 3 in all (top), WTR (middle) and ATR (bottom) eyes. No significant (p < 0.05) differences were observed. |
Anterior Corneal Astigmatism
Anterior corneal astigmatism had a mean absolute power of 1.63 ± 0.78 D for OPD scan, 1.81 ± 0.83 D for Pentacam, 1.69 ± 0.76 D for IOLM SK and 1.66 ± 0.75 D for median measurements across all eyes. Mean absolute anterior corneal astigmatism was significantly higher for Pentacam compared to OPD scan for all eyes (p < 0.05). No significant difference in the mean absolute anterior corneal astigmatism was observed across devices or median measurements when eyes were stratified according to type of astigmatism (WTR: p = 0.55; ATR: p = 0.46). The x-component of the centroid anterior corneal astigmatism was significantly lower for Pentacam (−2.06 ± 0.75 D) compared to OPD scan (−1.55 ± 1.2 D) in WTR eyes (p< 0.01).
Posterior Corneal Astigmatism
PCA measured using IOLM ranged from 0.00 to 0.67 D with a mean of 0.24 ± 0.15 D for all eyes. Mean absolute PCA was significantly greater in WTR eyes (0.32 ± 0.16 D) compared to ATR eyes (0.16 ± 0.07 D; p < 0.05). The centroid PCA was also significantly different between WTR (0.30 @ 86° ± 0.21 D) and ATR eyes (0.07 @ 130° ± 0.17 D; p < 0.001 for x-component; p = 0.058 for y-component).
Preoperative Total Corneal Astigmatism and Toric IOL Cylinder Power and Axis
The estimated preoperative total corneal astigmatism for each device and calculation method is presented in Figure 2 for all, WTR and ATR eyes. Mean absolute total corneal astigmatism was significantly lower in the IOLM SK with PCA group compared to the IOLM TK and Pentacam groups for all eyes (p < 0.05) and ATR eyes (p < 0.01). The x-component of the centroid total corneal astigmatism was significantly lower for IOLM SK with PCA calculations compared to the IOLM TK, OPD scan and median measurements groups in ATR eyes (p < 0.05). No significant difference in mean absolute or centroid total corneal astigmatism was observed across devices or calculation methods for WTR eyes (Figure 2).
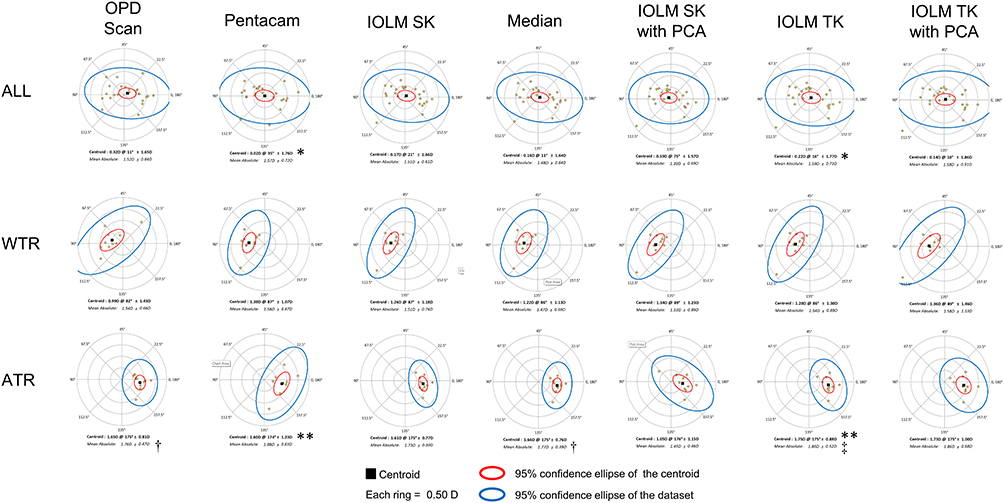 |
Figure 2 Estimated preoperative total corneal astigmatism. Double-angle plots of preoperative total corneal astigmatism estimated using the Barrett toric calculator incorporating measurements from each device or their median values. Barrett toric calculations made using measurements from IOLM SK with PCA produced significantly lower mean absolute total corneal astigmatism compared to IOLM TK and Pentacam groups for all eyes and ATR eyes. IOLM SK with PCA calculations demonstrated significantly lower x-component of the centroid total corneal astigmatism compared to IOLM TK, OPD scan and median measurements groups in ATR eyes. In WTR eyes, significant difference in mean absolute or centroid total corneal astigmatism was observed across devices or calculation methods. *p < 0.05 and **p < 0.01 compared to IOLM SK with PCA; †p < 0.05 and ‡p < 0.01 for x-component of centroid preoperative total corneal astigmatism compared to IOLM SK with PCA. |
The toric IOL cylinder power and axis of alignment recommended by each method of calculation is presented in Table 2. The mean recommended toric IOL cylinder power was not significantly different across calculations for all eyes (p = 0.07) and WTR eyes (p = 0.39). The x-component of the centroid toric IOL cylinder power and axis was significantly lower in IOLM SK with PCA calculations compared to the IOLM TK group in WTR eyes (p < 0.05). In ATR eyes, mean toric IOL cylinder power was significantly lower in the IOLM SK with PCA group compared to the IOLM TK and Pentacam groups (p < 0.05). The x-component of the centroid toric IOL cylinder power and axis recommended by IOLM SK with PCA calculations was significantly lower than that of IOLM TK, Pentacam and OPD scan in ATR eyes (p < 0.05).
 |
Table 2 Recommended Toric IOL Cylinder Power and Axis Calculated Using the Barrett Toric Calculator Incorporating Measurements from Each Device or Their Median Values |
Residual Refractive Astigmatism Prediction Error
The absolute error in predicted residual astigmatism is presented for all eyes across devices and calculation methods at POM1 (Figure 3A) and POM3 (Figure 3B). Mean absolute error in predicted residual astigmatism was highest for OPD scan (0.58 ± 0.52 D) at POM1 and Pentacam at POM3 (0.55 ± 0.32 D). The median measurements group had the lowest mean absolute residual astigmatism prediction error at POM1 (0.40 ± 0.25 D) and POM3 (0.41 ± 0.29 D). Mean absolute prediction errors were not significantly different between devices and calculation methods at POM1 (p = 0.09) and POM3 (p = 0.11) (Figure 3).
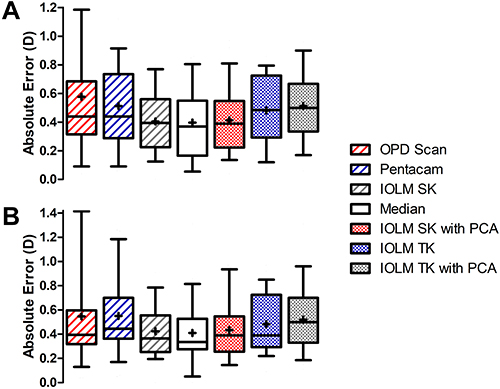 |
Figure 3 Absolute residual astigmatism prediction errors. Box and whisker plots of absolute residual astigmatism prediction errors across devices and calculation methods at postoperative month 1 (A) and postoperative month 3 (B) in all eyes. The mean absolute residual astigmatism prediction error is denoted by the +. Central horizontal lines represent the median prediction errors and whiskers extend to the 10th and 90th percentiles. There was no significant difference in mean absolute prediction error across devices and calculation methods at either time point. |
Double-angle plots of residual astigmatism prediction error are presented for WTR eyes in Figure 4 and ATR eyes in Figure 5. There was no significant difference in mean absolute error in predicted residual astigmatism for WTR or ATR eyes across devices or calculation methods at POM1 (WTR: p = 0.56; ATR: p = 0.43) or POM3 (WTR: p = 0.94; ATR: p = 0.43). The group trend for centroid residual astigmatism prediction error reached statistical significance at POM1 in WTR eyes (x-component: p = 0.049; y-component: p = 0.044), though post-hoc comparisons between devices and calculation methods were not statistically significant. At POM3, there was no significant difference in centroid residual astigmatism prediction error in WTR eyes across groups (x-component: p = 0.051; y-component: p = 0.28) (Figure 4). In ATR eyes, the x-component of the centroid residual astigmatism prediction error was significantly higher in the IOLM SK with PCA group compared to the IOLM TK, Pentacam and median measurements groups at POM1 and POM3 (p < 0.05). The y-component of the centroid residual astigmatism prediction error was not significantly different across calculation methods in ATR eyes at POM1 (p = 0.83) or POM3 (p = 0.87) (Figure 5).
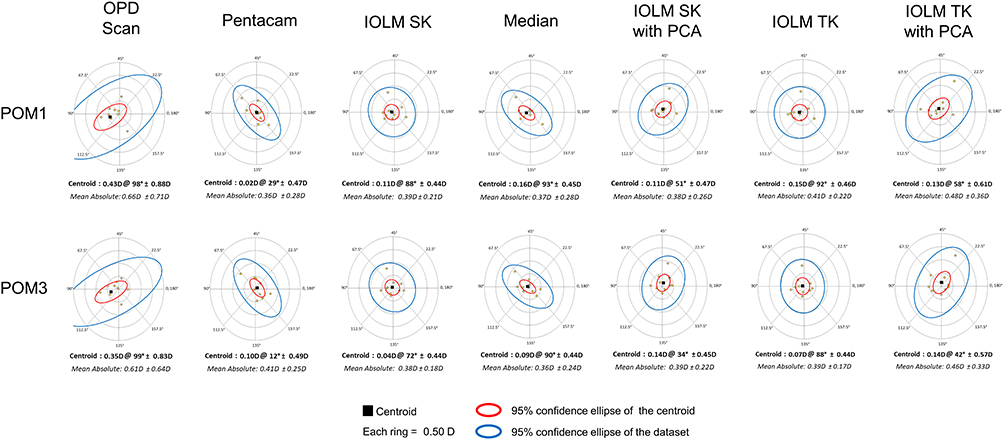 |
Figure 4 Mean absolute and centroid residual astigmatism prediction errors in WTR eyes. Double-angle plots of residual astigmatism prediction errors in WTR eyes at postoperative month 1 (top) and postoperative month 3 (bottom). Mean absolute and centroid residual astigmatism prediction errors were not significantly different across devices or calculation methods at postoperative month 1 or month 3 (p > 0.05). |
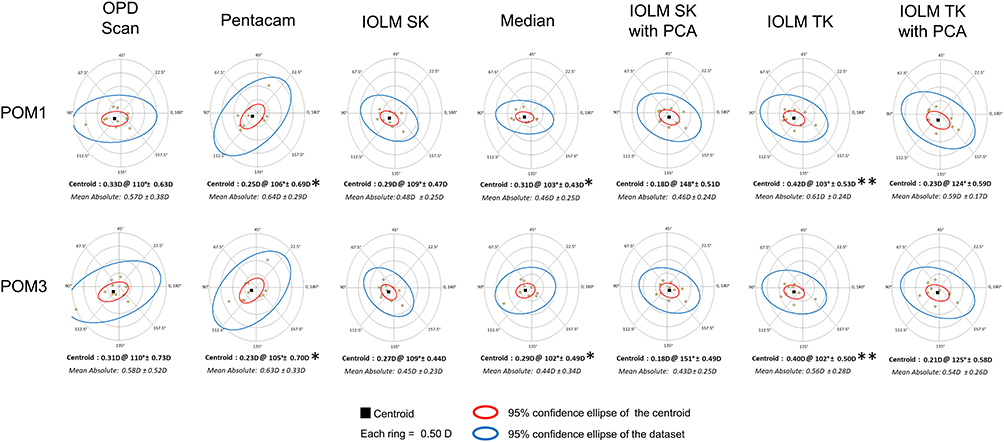 |
Figure 5 Mean absolute and centroid residual astigmatism prediction errors in ATR eyes. Double-angle plots of residual astigmatism prediction errors in ATR eyes at postoperative month 1 (top) and postoperative month 3 (bottom). There was no significant difference in mean absolute residual astigmatism prediction error across groups at either time point. The x-component of the centroid prediction error was significantly higher in the IOLM SK with PCA group compared to the IOLM TK, Pentacam and median measurements groups at postoperative month 1 and 3. The y-component of the centroid was not significantly different across groups at either time point. *p < 0.05, **p < 0.001 for x-component of centroid residual astigmatism prediction error compared to IOLM SK with PCA. |
Figure 6 illustrates the percentage of eyes with absolute residual astigmatism prediction errors ≤ 0.25 D, 0.5 D, 0.75 D and 1.0 D at POM3. No significant difference in the percentage of eyes within each category of absolute error in predicted residual astigmatism was observed when all eyes (Figure 6A), WTR eyes (Figure 6B) and ATR eyes (Figure 6C) were compared across devices and calculation methods (p > 0.05).
 |
Figure 6 Percentage of eyes with absolute residual astigmatism prediction errors ≤ 0.25, 0.5, 0.75 and 1.0 D. No significant difference in the percentage of eyes with absolute prediction errors within each range was observed across devices or calculation methods for all eyes (A), WTR eyes (B) and ATR eyes (C) at postoperative month 3. |
Discussion
Advances in cataract surgery have greatly improved postoperative refractive outcomes, making spectacle independence for distance vision an achievable goal for many patients.4 Toric IOLs have become a powerful tool for correcting corneal astigmatism through cataract surgery and their success is dependent upon accurate measurements of preoperative corneal astigmatism and reliable toric IOL calculations.5 Mounting evidence suggests that PCA should be incorporated into toric IOL calculations to minimize postoperative refractive errors.6–13,16–28 However, it remains unclear whether measured or predicted PCA is best suited for this purpose. Here, we show that residual astigmatism prediction errors are comparable between Barrett toric calculations performed using predicted PCA and PCA directly measured using IOLM. When predicted PCA was used, toric calculations were similar across devices and median measurements. Incorporation of TK values from IOLM into Barrett toric calculations did not significantly improve calculation accuracy over standard keratometry measurements.
The contribution of PCA to the total refractive power of the eye was originally suggested through Javal’s rule, though it was not known at the time that the posterior cornea was responsible for the observed deviation between refractive astigmatism and anterior corneal astigmatism keratometry measurements.36 Direct measurements of PCA were performed in the 1990s using Purkinje imaging.37–39 Several studies have since used rotating Scheimpflug imaging and dual Scheimpflug and Placido disk imaging to demonstrated that PCA has an average magnitude of approximately 0.24–0.42 D and is vertically oriented in the majority of eyes, particularly in patients with WTR anterior corneal astigmatism.7,9,12,20,22,26,39–43 LaHood et al14 measured PCA using the recently released IOLM with SS-OCT and telecentric keratometry and found that PCA ranged from 0 to 1.21 D with an average magnitude of 0.24 D. Similar to Scheimpflug and Purkinje imaging, IOLM measured a vertically oriented steep axis of the posterior cornea in 73% of eyes and PCA was found to be significantly greater in WTR eyes compared to ATR eyes.14 In the present study, an average PCA of 0.24 ± 0.15 D (ranging from 0 to 0.67 D) was measured using IOLM for all eyes and higher PCA was observed in WTR eyes compared to ATR eyes, which aligns with previous studies.
Toric IOL calculations performed using anterior corneal measurements alone have been shown to overestimate total corneal astigmatism in WTR eyes and underestimate astigmatism in ATR eyes.6–10 The Baylor nomogram, Abulafia-Koch formula, Goggin coefficient of adjustment and other mathematical formulas have therefore been developed to account for PCA when only anterior corneal measurements are available. The incorporation of predicted PCA into toric IOL calculations has been shown to significantly reduce residual astigmatism prediction errors.8,11–13,16–24 Many of these methods for predicting PCA were developed using large datasets of corneal measurements from normal, healthy eyes. This has led some to suggest that the direct measurement of PCA may enable more accurate toric IOL calculations in individual patients, particularly in eyes that are considered to be outliers.15 Several studies have compared toric IOL calculations performed using anterior corneal measurements alone to those that account for directly measured PCA. Similar to predicted PCA, in the majority of these studies, the utilization of measured PCA in toric IOL calculations led to lower residual astigmatism prediction errors compared to calculations performed using anterior corneal measurements alone.25–28
Although the utilization of both measured and predicted PCA have been shown to improve toric IOL calculation accuracy, studies directly comparing calculations performed using predicted PCA to those using measured PCA have produced mixed results. Reitblat et al26 demonstrated that vector summation calculations performed using measured PCA generated lower mean absolute residual astigmatism prediction errors in all eyes and lower centroid residual astigmatism prediction errors in WTR eyes compared to predicted PCA calculations performed using the Baylor nomogram. In ATR eyes, however, calculations performed using the Baylor nomogram resulted in lower centroid residual astigmatism prediction errors compared to vector summation using measured PCA.26 Barrett toric calculations using predicted PCA and Holladay calculations using the Abulafia-Koch formula have been shown to produce lower residual astigmatism prediction errors compared to calculations incorporating measured PCA in all, ATR and WTR eyes.18,21 When Barrett toric calculations incorporating predicted and measured PCA were directly compared, no significant difference in residual astigmatism prediction error was observed between groups.44 In each of these studies, PCA was measured using rotating Scheimpflug imaging, and it is unclear whether comparable outcomes occur when other methods of PCA measurement are used.
In the present study, estimated preoperative total corneal astigmatism, recommended toric IOL cylinder power and axis, and postoperative residual astigmatism prediction errors were not significantly impacted by the incorporation of measured versus predicted PCA into Barrett toric calculations. This is evident in comparisons between the IOLM SK and IOLM SK with PCA, and IOLM TK and IOLM TK with PCA groups. The results from this study therefore suggest that comparable clinical outcomes can be achieved when preoperative planning is performed using Barrett toric calculations incorporating predicted PCA and PCA directly measured using IOLM.
Several devices are available for the measurement of anterior corneal astigmatism. Meta-analysis of 127 studies assessing the agreement between biometers found that anterior corneal measurements were generally comparable across devices, though significant inter-device differences do exist.45 Studies comparing toric IOL calculations performed using anterior corneal measurements from different devices have demonstrated variable effects on residual refractive astigmatism prediction errors and no one device has consistently been shown to produce the most accurate calculations.6,16,24,46 In the present study, mean absolute anterior corneal astigmatism was greater when measurements were performed using Pentacam compared to OPD scan. However, no significant difference in estimated preoperative total corneal astigmatism, recommended toric IOL or postoperative residual astigmatism prediction error was observed between Barrett toric calculations performed using predicted PCA and measurements derived from IOLM, OPD scan, Pentacam or their median values.
Fabian et al recently compared Barrett toric calculations performed using SK and TK measurements from IOLM with predicted PCA. Similar to the present study, they found that there was no significant difference in residual astigmatism prediction errors between Barrett toric calculations performed using SK and TK measurements.15 We further extended our analysis to include calculations incorporating measured PCA and found that the IOLM SK with PCA and IOLM TK with PCA groups produced comparable estimates of total corneal astigmatism, recommended toric IOLs and residual astigmatism prediction errors. In comparison to the IOLM TK group, calculations made using IOLM SK with measured PCA generated significantly lower estimates of mean preoperative total corneal astigmatism in all eyes. In ATR eyes, mean total corneal astigmatism and toric IOL cylinder power were approximately 0.40 D and 0.60 D lower, respectively, in the IOLM SK with PCA group compared to IOLM TK group. Centroid residual astigmatism prediction error was approximately 0.13 D lower in the IOLM SK with PCA group compared to IOLM TK group in ATR eyes, which was statistically significant for the x-component but not the y-component of the centroid. These results suggest that IOLM TK measurements are suitable for use in Barrett toric calculations with either predicted or measured PCA.
It is important to highlight that the present study was limited by its retrospective nature and small sample size. Only 4 eyes with oblique astigmatism were included which prevented meaningful statistical comparisons. Future studies involving a greater number of patients with oblique astigmatism are warranted to address the impact of measured versus predicted PCA on toric IOL calculations for oblique astigmatism. Another potential limitation of this study was that SIA was not measured for each individual patient. Although FLACS was used for consistency of corneal incisions across all three surgeons, it is possible that variability in SIA affected our analysis. Furthermore, PCA was only measured using IOLM. Additional studies may wish to directly compare Barrett toric calculations performed using PCA measured using several available devices to determine whether the method of PCA measurement impacts calculation accuracy.
In conclusion, the present study suggests that the incorporation of measured PCA or TK values derived from IOLM into Barrett toric calculations does not result in clinically meaningful differences in the accuracy of these calculations. The Barrett toric calculator produces low residual astigmatism prediction errors across several devices measuring anterior corneal astigmatism when predicted PCA is used. Calculation accuracy was not significantly impacted by the utilization of the median measurements function for Barrett toric calculations.
Acknowledgment
Data from this manuscript was presented in part at the 2020 Canadian Ophthalmological Society Virtual Annual Meeting and the 2020 American Society of Cataract and Refractive Surgery Virtual Annual Meeting.
Funding
Mark K. Lukewich was supported by the Eye Foundation of Canada Summer Scholarship Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferreira TB, Hoffer KJ, Ribeiro F, Ribeiro P, O’Neill JG. Ocular biometric measurements in cataract surgery candidates in Portugal. PLoS One. 2017;12(10):e0184837. doi:10.1371/journal.pone.0184837
2. Hoffer KJ. Biometry of 7500 cataractous eyes. Am J Ophthalmol. 1980;90:360–368. doi:10.1016/S0002-9394(14)74917-7
3. Hoffmann PC, Hutz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36:1479–1485. doi:10.1016/j.jcrs.2010.02.025
4. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
5. Hirnschall N, Findl O, Bayer N, et al. Sources of error in toric intraocular lens power calculation. J Refract Surg. 2020;36(10):646–652. doi:10.3928/1081597X-20200729-03
6. Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803–1809. doi:10.1016/j.jcrs.2013.06.027
7. Tonn B, Klaproth OK, Kohnen T. Anterior surface-based keratometry compared with Scheimpflug tomography-based total corneal astigmatism. Invest Ophthalmol Vis Sci. 2014;56(1):291–298. doi:10.1167/iovs.14-15659
8. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(2):827–835. doi:10.1167/iovs.14-15903
9. Jiang Y, Tang Y, Jing Q, Qian D, Lu Y. Distribution of posterior corneal astigmatism and aberration before cataract surgery in Chinese patients. Eye. 2018;32(12):1831–1838. doi:10.1038/s41433-018-0186-0
10. Goggin M, Zamora-Alejo K, Esterman A, van Zyl L. Adjustment of anterior corneal astigmatism values to incorporate the likely effect of posterior corneal curvature for toric intraocular lens calculation. J Refract Surg. 2015;31(2):98–102. doi:10.3928/1081597X-20150122-04
11. Abulafia A, Koch DD, Wang L, et al. New regression formula for toric intraocular lens calculations. J Cataract Refract Surg. 2016;42(5):663–671. doi:10.1016/j.jcrs.2016.02.038
12. Eom Y, Rhim JW, Kang S-Y, Kim SW, Song JS, Kim HM. Toric Intraocular lens calculations using ratio of anterior to posterior corneal cylinder power. Am J Ophthalmol. 2015;160(4):717–724.e2. doi:10.1016/j.ajo.2015.07.011
13. Canovas C, Alarcon A, Rosén R, et al. New algorithm for toric intraocular lens power calculation considering the posterior corneal astigmatism. J Cataract Refract Surg. 2018;44(2):168–174. doi:10.1016/j.jcrs.2017.11.008
14. LaHood BR, Goggin M. Measurement of posterior corneal astigmatism by the IOLMaster 700. J Refract Surg. 2018;34(5):331–336. doi:10.3928/1081597X-20180214-02
15. Fabian E, Wehner W. Prediction accuracy of total keratometry compared to standard keratometry using different intraocular lens power formulas. J Refract Surg. 2019;35(6):362–368. doi:10.3928/1081597X-20190422-02
16. Abulafia A, Barrett GD, Kleinmann G, et al. Prediction of refractive outcomes with toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(5):936–944. doi:10.1016/j.jcrs.2014.08.036
17. Kern C, Kortüm K, Müller M, Kampik A, Priglinger S, Mayer WJ. Comparison of two toric IOL calculation methods. J Ophthalmol. 2018;2018:2840246. doi:10.1155/2018/2840246
18. Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of astigmatic prediction errors associated with new calculation methods for toric intraocular lenses. J Cataract Refract Surg. 2017;43(3):340–347. doi:10.1016/j.jcrs.2016.12.031
19. Yoon CH, Kim MK. Improving the toric intraocular lens calculation by considering posterior corneal astigmatism and surgically-induced corneal astigmatism. Korean J Ophthalmol. 2018;32(4):265–272. doi:10.3341/kjo.2017.0108
20. Eom Y, Ryu D, Kim DW, et al. Development of a program for toric intraocular lens calculation considering posterior corneal astigmatism, incision-induced posterior corneal astigmatism, and effective lens position. Graefes Arch Clin Exp Ophthalmol. 2016;254(10):1977–1986. doi:10.1007/s00417-016-3446-3
21. Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of methodologies using estimated or measured values of total corneal astigmatism for toric intraocular lens power calculation. J Refract Surg. 2017;33(12):794–800. doi:10.3928/1081597X-20171004-03
22. Kansara N, Cui D, Banerjee K, Landis Z, Scott IU, Pantanelli SM. Anterior, posterior, and non-keratometric contributions to refractive astigmatism in pseudophakes. J Cataract Refract Surg. 2021;47(1):93–99. doi:10.1097/j.jcrs.0000000000000390
23. Ribeiro FJ, Ferreira TB, Relha C, Esteves C, Gaspar S. Predictability of different calculators in the minimization of postoperative astigmatism after implantation of a toric intraocular lens. Clin Ophthalmol. 2019;13:1649–1656. doi:10.2147/OPTH.S213132
24. Abulafia A, Hill WE, Franchina M, Barrett GD. Comparison of methods to predict residual astigmatism after intraocular lens implantation. J Refract Surg. 2015;31(10):699–707. doi:10.3928/1081597X-20150928-03
25. Park DY, Lim DH, Hwang S, Hyun J, Chung TY. Comparison of astigmatism prediction error taken with the Pentacam measurements, Baylor nomogram, and Barrett formula for toric intraocular lens implantation. BMC Ophthalmol. 2017;17(1):156. doi:10.1186/s12886-017-0550-z
26. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217–225. doi:10.1016/j.jcrs.2015.11.036
27. Hoffmann PC, Wahl J, Hütz WW, Preußner PR. A ray tracing approach to calculate toric intraocular lenses. J Refract Surg. 2013;29(6):402–408. doi:10.3928/1081597X-20130515-04
28. Davison JA, Potvin R. Refractive cylinder outcomes after calculating toric intraocular lens cylinder power using total corneal refractive power. Clin Ophthalmol. 2015;9:1511–1517. doi:10.2147/OPTH.S88693
29. Kern C, Kaissi EL, Kortuem K, et al. Comparing refractive outcomes of a standard industry toric IOL calculator using anterior corneal astigmatism and total corneal refractive power. Graefes Arch Clin Exp Ophthalmol. 2020;258(2):345–350. doi:10.1007/s00417-019-04570-1
30. Carmona-González D, Castillo-Gómez A, Palomino-Bautista C, Romero-Domínguez M, Gutiérrez-Moreno MÁ. Comparison of the accuracy of 11 intraocular lens power calculation formulas. Eur J Ophthalmol. 2021;31(5):2370–2376. doi:10.1177/1120672120962030
31. Iijima K, Kamiya K, Iida Y, Shoji N. Comparison of predictability using Barrett universal II and SRK/T formulas according to keratometry. J Ophthalmol. 2020;2020:7625725. doi:10.1155/2020/7625725
32. Donaldson K, Fernández-Vega-Cueto L, Davidson R, et al.; ASCRS Refractive–Cataract Surgery Subcommittee. Perioperative assessment for refractive cataract surgery. J Cataract Refract Surg. 2018;44(5):642–653. doi:10.1016/j.jcrs.2018.02.022
33. Barrett GD Calculating astigmatic correction. presented at the XXXIV congress of the European Society of cataract and refractive surgeons. Denmark: Copenhagen; 2016.
34. Abulafia A, Koch DD, Holladay JT, Wang L, Hill WE. Pursuing perfection in IOL calculations IV: astigmatism analysis, SIA and double angle plots. J Cataract Refract Surg. 2018;44(10):1169–1174. doi:10.1016/j.jcrs.2018.07.027
35. Hill W, Osher R, Cooke D, et al. Simulation of toric intraocular lens results: manual keratometry versus dual-zone automated keratometry from an integrated biometer. J Cataract Refract Surg. 2011;37(12):2181–2187. doi:10.1016/j.jcrs.2011.06.028
36. Koch DD. The posterior cornea: hiding in plain sight. Ophthalmology. 2015;122(6):1070–1071. doi:10.1016/j.ophtha.2015.01.022
37. Royston JM, Dunne MC, Barnes DA. Measurement of posterior corneal surface toricity. Optom Vis Sci. 1990;67(10):757–763. doi:10.1097/00006324-199010000-00002
38. Dunne MC, Royston JM, Barnes DA. Posterior corneal surface toricity and total corneal astigmatism. Optom Vis Sci. 1991;68(9):708–710. doi:10.1097/00006324-199109000-00006
39. Dunne M, Royston JM, Barnes DA. Normal variations of the posterior corneal surface. Acta Ophthalmol. 1992;70(2):255–261. doi:10.1111/j.1755-3768.1992.tb04133.x
40. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
41. Ho JD, Tsai CY, Liou SW. Accuracy of corneal astigmatism estimation by neglecting the posterior corneal surface measurement. Am J Ophthalmol. 2009;147(5):788–795. doi:10.1016/j.ajo.2008.12.020
42. Zhang L, Sy ME, Mai H, Yu F, Hamilton DR. Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(1):84–89. doi:10.1016/j.jcrs.2014.04.033
43. Miyake T, Shimizu K, Kamiya K. Distribution of posterior corneal astigmatism according to axis orientation of anterior corneal astigmatism. PLoS One. 2015;10(1):e0117194. doi:10.1371/journal.pone.0117194
44. Skrzypecki J, Patel MS, Suh LH. Performance of the Barrett Toric Calculator with and without measurements of posterior corneal curvature. Eye. 2019;33(11):1762–1767. doi:10.1038/s41433-019-0489-9
45. Rozema JJ, Wouters K, Mathysen DGP, Tassignon MJ. Overview of the repeatability, reproducibility, and agreement of the biometry values provided by various ophthalmic devices. Am J Ophthalmol. 2014;158(6):1111–1120. doi:10.1016/j.ajo.2014.08.014
46. Reitblat O, Levy A, Kleinmann G, Assia EI. Accuracy of intraocular lens power calculation using three optical biometry measurement devices: the OA-2000, Lenstar-LS900 and IOLMaster-500. Eye. 2018;32(7):1244–1252. doi:10.1038/s41433-018-0063-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.