Back to Journals » Clinical Ophthalmology » Volume 14
Comparison of Anterior Segment Parameters and Axial Length Using Two Scheimpflug Devices with Integrated Optical Biometers
Authors Supiyaphun C, Rattanasiri S ![]() , Jongkhajornpong P
, Jongkhajornpong P ![]()
Received 25 August 2020
Accepted for publication 28 September 2020
Published 23 October 2020 Volume 2020:14 Pages 3487—3494
DOI https://doi.org/10.2147/OPTH.S278701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Chantaka Supiyaphun,1 Sasivimol Rattanasiri,2 Passara Jongkhajornpong3
1Department of Ophthalmology, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Department of Ophthalmology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Passara Jongkhajornpong
Department of Ophthalmology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Tel +662-2012729
Email [email protected]
Purpose: To assess the repeatability of anterior segment parameters and axial length (AL) using Pentacam AXL and Galilei G6 and the agreement between both devices.
Materials and Methods: Eighty-four eyes of 84 participants were measured prospectively with two devices. Outcome measurements included corneal curvatures, anterior chamber depth (ACD), AL, pupil size, and white-to-white distance (WTW). Intra-device repeatability was assessed using intraclass correlation coefficient (ICC), within-subject standard deviation (Sw), test–re-test repeatability (TRT=2.77 Sw), and coefficient of variation (CoV). Agreement between two devices was analyzed using Bland–Altman plots.
Results: For each device, the Sw of corneal curvatures, ACD, and AL were lower than 0.25 D, 0.04 mm, and 0.04 mm, respectively. The ICC was higher than 0.90 in all parameters measured by Pentacam AXL, whereas three parameters measured by Galilei G6 (steep meridian at anterior and posterior cornea, and pupil size) were lower than 0.90. Comparing to Galilei G6, Pentacam AXL led to significantly lower mean anterior cornea curvatures (Km) with the mean difference (95% level of agreement; LoA) of − 0.12 D (− 0.36, 0.12, P< 0.001). For ACD, there was no significant difference between the two devices. Pentacam AXL led to significantly lower AL, pupil size, and WTW, with the mean differences (95% LoA) of − 0.04 mm (− 0.35, 0.27), − 0.18 mm (− 0.71, 0.35), and − 0.35 mm (− 0.61, − 0.10), respectively.
Conclusion: We found good repeatability of corneal curvature, ACD, and AL in both devices. Most parameters obtained from Pentacam AXL were statistically significantly different from those obtained from Galilei G6, except for steep meridians and ACD.
Keywords: Pentacam AXL, Galilei G6, agreement, intra-device repeatability
Introduction
Precise measurement of corneal curvature is key for successful refractive and cataract surgery, especially in the era of topo-guided laser treatment and premium lens implantations (ie, toric intraocular lens (IOL), multifocal IOL, and multifocal toric IOL). Not only is it integral for surgeries, corneal curvature measurement is also an essential investigation for the diagnosis of indolent corneal diseases in both virgin and post-refractive surgery eyes. Since the development of the Placido disc was introduced for evaluating anterior curvatures in 1880,1 corneal assessment technologies have been continuously developed. In addition to measuring anterior corneal curvatures, the application of the Sheimpflug principle enables a non-parallel planar object to be in focus.2 This allows for accurate measurements of both anterior and posterior curvatures as well as corneal thickness, and anterior chamber depth (ACD) within a few seconds,1 making Scheimpflug-based devices the most popular assessment tool for investigating corneal ectasia and pre-operative corneal evaluation.1
To date, there are three corneal topography devices using the Scheimpflug principle; a single camera; Pentacam (Oculus Optikgeräte GmbH), a single camera combined with a Placido disc; the Sirius (Costruzione Strumenti Oftalmici), and a dual cameras combined with a Placido disc; the Galilei (Ziemer Ophthalmic Systems AG). Both single and dual camera devices provide good intra-operator repeatability and inter-session reproducibility for overall measurements, however, the level of within subject coefficient variations (CoV) vary among different studies.3–5 Interdevice agreement of anterior curvature measurement and pachymetry is poor and cannot be used interchangeably, while the mean difference between devices are still inconclusive.6,7 Only one study reported the agreement of posterior curvature based on a limited sample size.4 Recently, Pentacam and Galilei have upgraded its software and integrated optical biometers into their devices for axial length (AL) measurement. The repeatability of each new device has been reported in a few studies8–11 and the inter-device agreement between these devices has not yet been reported. Therefore, this study aimed to assess the repeatability of Pentacam AXL (a single Scheimplug device integrated with partial coherence interferometry; PCI) and Galilei G6 (a dual Scheimplug-Placido disc device integrated with optical low-coherence reflectometry; OLCR) as well as to assess the agreement between these two devices in measuring corneal curvatures (both anterior and posterior corneal surfaces), ACD, AL, pupil size, and white-to-white distance (WTW).
Methods
The study was managed in accordance with the Helsinki Declaration and was approved by the Ethics Committee of Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand. This cross-sectional study was conducted prospectively at the Department of Ophthalmology, Vajira Hospital from March 2019 to July 2019. We enrolled healthy volunteers age ranged from 20–40 years. Informed consent was obtained from all participants before performing all examinations. Exclusion criteria were a history of any ocular surgery or trauma, significant ocular pathology (ie, cataract, corneal opacity, glaucoma, and retinal disease), and contact lens wear within the last 2 weeks. Participants were measured for best corrected visual acuity (BCVA) and received slit-lamp evaluation for any ocular disease. All anterior segment parameters and axial lengths were randomly measured using two devices consisting of Pentacam AXL (software version, 6.08r34, Oculus, Wetzlar, Germany) and Galilei G6 (software version 6.4.1, Zeimer, Port, Switzerland). The parameters of interest included corneal curvature of flat and steep meridians (K1 and K2), steep meridian, mean corneal curvature (Km), astigmatism amplitude, ACD, AL, pupil size, and WTW. For each participant, information from only the right eye was included.
The Pentacam AXL device combines a corneal tomography and additional AL measurement. A three-dimensional model of the anterior segment is constructed based on a rotating Scheimpflug camera (180°) and monochromatic slit-light source of blue light-emitting diode at 475 nm that rotates together around the optical axis of the eye. AL was measured using PCI module. This study used a default program for optical biometry, initially taking 25 Scheimpflug images in one second followed by axial length measurement. The Pentacam AXL calculates two ACDs which are internal (from corneal endothelium to the anterior lens plane) and external (from corneal epithelium to the anterior lens plane). Only external ACD was used for analysis.
The Galilei G6 uses a dual rotating Scheimpflug camera integrated with Placido disc topographer. The flash illumination is the output from a blue light-emitting diode at 470 nm. The device takes images of all anterior segment structures from the cornea to the lens and measures over 122,000 data points per scan. Axial length is measured using OLCR. The measurement includes three parts; 1) anterior corneal curvature by Placido disc, 2) anterior segment measurements by dual Scheimpflug camera, and 3) axial length measurement.
Measurement Techniques
A single experienced examiner (C.S.) performed two sessions of adequate qualified measurements with examination quality specification graded as either OK or high overall quality check in Pentacam AXL and Galilei G6, respectively. All measurements were performed within 15 minutes to avoid diurnal variation effects in a dim room according to the manufacturer’s guidelines. All participants were instructed to look straight at the target of the camera while in an upright sitting positioning with head resting on the headrest and chin on the chinrest. Participants were asked to blink before the start and stop of the scan. After each measurement, participants were asked to sit back and close their eyes for a few seconds before the next measurement.
Statistical Analysis
Statistical analyses were performed using STATA version 16 (TX, US). All continuous parameters were described as means (standard deviation, SD). The Kolmogorov–Smirnov test was used for normality checking. A paired t-test was used to compare all average parameters between two devices within the same subject. A P-value less than 0.05 was considered statistically significant. To determine the intra-device repeatability,3 the within-subject standard deviation (Sw), test–re-test repeatability (TRT=2.77 Sw), within-subject coefficient of variation (CoV) and intraclass correlation coefficient (ICC) were calculated for the two repeated measurements obtained by a single operator.12 TRT indicates an interval within 95% of the differences between measurements is expected to lie. The lower TRT represents the better repeatability. CoV was calculated from the ratio between Sw and the overall mean. The lower CoV indicates the higher repeatability. The closer ICC to one suggests the better measurement consistency.
Average values of the two measurements from each device were used for agreement analysis. The agreement of measured parameters between the two devices was assessed using the Bland–Altman plot analysis. Mean difference and 95% limits of agreement (LoA) were calculated to illustrate the agreement between two devices.13,14 Plots were created to show the mean value (x-axis) against the differences in measurement between two devices.
Results
Of the 96 enrolled participants, 84 eyes of 84 participants (168 qualified sessions) were included into this study. Twelve participants were excluded due to not being able to obtain two qualified scans from both devices in a limited time. The mean age was 28.8 (SD=5.5) years, with female predominance (55, 65.5%). The median BCVA was 0.0 logMAR (range=0.0–0.4 logMAR). The median spherical equivalent was −1.37 diopters (D, range=−13.25–0.875 D). The median astigmatism was 0.75 D (range=0–6.0 D).
Intra-Device Repeatability
All parameters obtained by the two qualified scans were highly repeatable in both Pentacam AXL and Galilei G6 except for the steep meridian of front and back surfaces (Table 1). The TRTs of K1, K2, Km, ACD, AL, pupil size, and WTW in both devices were less than 0.50 D, 0.10 mm, 0.10 mm, 0.80 mm, and 0.30 mm, respectively. The TRT of steep meridian was large as 13.08 degrees in Pantacam AXL and 21.63 degrees in Galilei G6. The CoV of two measurements in both devices were lower than 0.20% for all parameters. The ICC was higher than 0.90 in all parameters measured by Pentacam AXL. While the ICC of three parameters measured by Galilei G6 (i.e., steep meridian at front and back surfaces, and pupil size) were lower than 0.90.
 |
Table 1 Repeatability of All Measurements Using Pentacam AXL and Galilei G6 |
Inter-Device Agreement
Anterior Cornea Parameters
The mean differences of all anterior curvatures except for the steep meridian between two devices were statistically different (Table 2). Pentacam AXL produced significantly lower K1, K2, Km, and magnitude of astigmatism front compared to Galilei G6 with the mean differences (95% LoA) of −0.08 D (−0.34, 0.19), −0.14 D (−0.48, 0.19), −0.12 D (−0.36, 0.12), and −0.06 D (−0.43, 0.31), as shown in Figure 1A–C. The agreement of steep meridian between both devices was not statistically significant with the mean difference (95% LoA) of 0.87 degrees (−11.39, 13.12), see Figure 1D.
 |
Table 2 Mean Differences of All Measurements and 95% Limit of Agreement (LoA) |
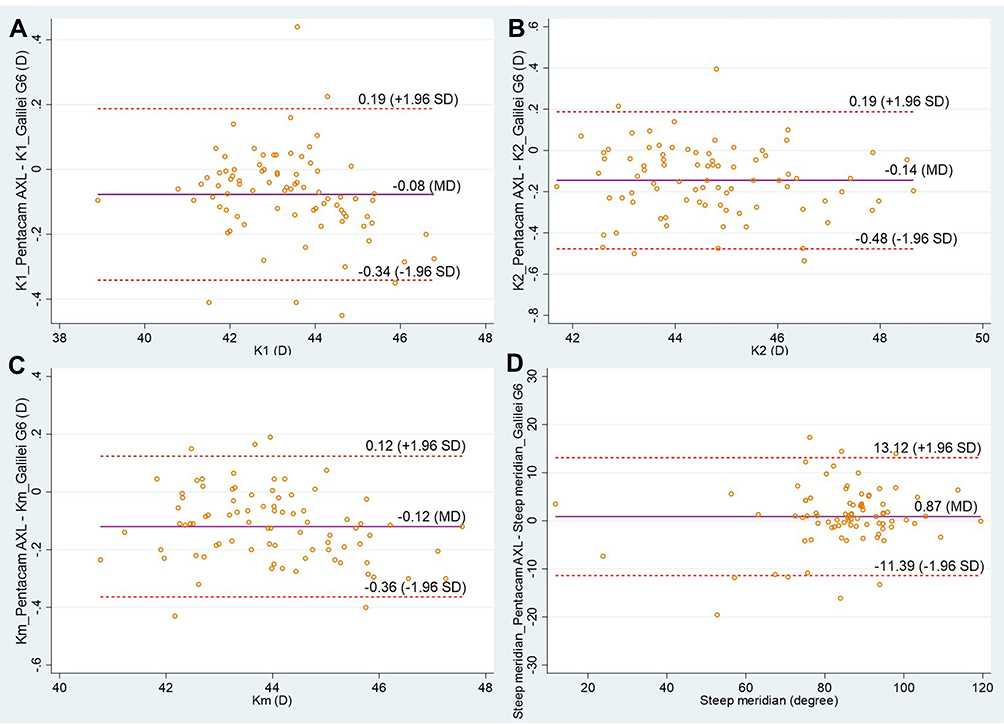 |
Figure 1 Bland–Altman plots showing the agreements between anterior corneal parameters obtained by Pentacam AXL and Galilei G6: (A) K1 (flat K), (B) K2 (steep K), (C) Km (mean K), and (D) steep meridian. The solid line is the mean difference, the dashed lines are the 95% limit of agreement. |
Posterior Cornea Parameters
Pentacam AXL produced significantly lower K1 and steep meridian compared to Galilei G6 with the mean differences (95% LoA) of 0.02 D (−0.09, 0.14) and 2.81 D (−17.31, 22.94), as shown in Table 2. There was a good agreement of K2 between two devices with a mean difference of 0.01 D (−0.13, 0.15).
Anterior Chamber Depth, Axial Length, and Other Parameters
Pentacam AXL produced slightly lower ACD compared to Galilei G6 with the mean difference (95% LoA) of −0.04 mm (−0.35, 0.27), but was not statistically significant (Figure 2). However, Pentacam AXL produced statistically significant lower AL with the mean difference (95% LoA) of −0.02 mm (−0.09, 0.04), P<0.001 (Figure 2B). Pentacam AXL produced significantly lower WTW and pupil size compared to Galilei G6 with mean differences (95% LoA) of −0.35 mm (−0.61, 0.10) and −0.18 mm (−0.71, 0.35), as shown in Table 2.
 |
Figure 2 Bland–Altman plots showing the agreements between (A) axial length and (B) anterior chamber depth obtained by Pentacam AXL and Galilei G6. The solid line is the mean difference, The dashed lines are the 95% limit of agreement. |
Discussion
This study demonstrated the intra-device repeatability and inter-device agreement of all essential parameters including anterior and posterior curvatures, ACD, AL, WTW, and pupil size. The ICC of all parameters except for the steep meridians were higher than 0.90 and 0.85 in Pentacam AXL and Galilei G6 with low TRT values (range=0.02–0.29), respectively, indicating good repeatability of both devices. Previous studies demonstrated that Pentacam AXL had good repeatability in terms of measuring mean K, ACD, AL for both normal and cataract eyes.8,9 Our findings also supported the previous study that Galilei G6 has a good repeatability for measuring AL.10,11 Moreover, we found that Pentacam AXL provides slightly lower mean values of overall measured parameters. For the anterior steep meridian, the TRT values of Pentacam AXL and Galilei G6 were 13 and 22 degrees, indicating the low repeatability of this parameter in both devices. These findings were similar to previous study from Aramberri et al4 showing that the TRTs of anterior flat meridian was high as 41.72 degrees for single Scheimpflug camera (Pentacam HR) and 65.98 degrees for dual Scheimpflug camera (Galilei G2).
To determine the inter-device agreement, the Bland–Altman analysis revealed that mean values of most parameters between Pentacam AXL and Galilei G6 were statistically significantly different. However, the statistical significance did not directly indicate the clinical significance. For corneal curvature measurement, 95% LoA of K1 and K2 (anterior and posterior), Km, and astigmatism were within 0.5 D, whereas 95% LoA of the steep meridian was large, as 13 and 23 degrees at anterior and posterior surfaces. Crawford et al6 showed slightly higher 95% LoA of anterior keratometry (range=−0.5–0.6 D) compared to our study, possibly owing to the small sample size (30 healthy eyes) and different software version. Aramberri et al4 also found that the agreement of anterior cornea parameters between Pentacam and Galilei was very good except for anterior astigmatism, while the posterior cornea had more significant disagreements, but very low clinical relevance. It should be noted that the clinical importance should be determined based on the objectives of measurement, thus both devices can be considered as interchangeable in some clinical situations. Nevertheless, these small differences might have a considerable impact to IOL calculation, particularly in the cases with toric or multifocal toric IOLs. Of the 84 eyes in our study, we observed a difference of astigmatism magnitude between two devices (Pentacam AXL – Galilei G6) of over 0.5 diopters in two eyes (−0.69 and 0.51 D). These differences had an impact on changing one level of cylinder power of the toric IOL calculation.
Our results showed that the mean difference of ACD between Pentacam AXL and Galilei G6 was very low (0.04 mm), corresponding to findings from the previous studies.3,5,7,15,16 However, the 95% LoA was in the range of 0.35 mm, which was higher than previous studies. The discrepancies of measured values between studies could be accounted for by the differences in software versions (Pentacam HR and Galilei G2/G4), subject characteristics, ACD definition (internal and external ACD), and number of repeated measurements.
To the best of our knowledge, we did not find any published studies comparing AL values between Pentacam AXL and Galilei G6. Pentacam AXL (PCI-based device) tended to produce lower AL with the low mean difference of −0.02 mm (95% LoA=−0.09–0.14) compared to Galilei G6 (OLCR-based device). Our findings corresponded with a recent review suggesting that there was good agreement in AL when using different techniques for measurement; the PCI-based device (a laser diode infrared light) vs OLCR-based device (a superluminescent diode), with 95% LoA of less than 0.2 mm.17 Jung et al10 demonstrated no statistical significance between AL measured by Galilei G6 and AL measured by IOL Master 700. Recently, Shajari et al18 also showed that the mean difference of AL between Pentacam AXL and IOL Master 700 was −0.019 mm, and no statistical significance was found between both devices.
WTW was one of the most inconsistent values in our study. A review found that WTW were discrepancies across the studies. They were likely caused by different digital image processing techniques carried out by different devices and because of heterogeneity of patient characteristics.19 In addition, any nose or eyelash shadows, or peripheral corneal lesions can consequently affect computerized detection leading to the variation of WTW measurement.19 Only one previous study reported that Pentacam HR provided approximately 0.05 mm wider distances than Galilei G2 and the 95% LoA was not in a clinically acceptable range.15 Thus, the two devices were considered as non-interchangeable. Pupil size is an important parameter that should be evaluated before cataract surgery. A photopic pupil size of greater than 3.0 mm is recommended for multifocal IOL implantation.20 The 95% LoA between Pentacam AXL and Galilei G6 ranged from −0.71 to 0.35 mm, which might influence the clinical decision for multifocal IOL candidates and the lens models.
This study had some limitations. Firstly, we included only normal eyes without cataracts or any corneal pathology that could restrain the accuracy of measurements. Secondly, we acquired two repeat measurements in each eye for the analysis. This might lead to wider Sw and TRT values (lower intra-device repeatability) and wider mean differences between two devices compared to previous studies. However, we expected that our findings might closely reflect routine practice situations, in which two qualified scans were obtained. Thirdly, we did not compare biometric parameters with other standard optical biometers, ie, IOL Master or Lenstar LS 900. Since sufficient evidence comparing between Pentacam AXL and IOL Master was retrieved,8,10,11,18,21,22 it makes indirect comparisons among various devices possible. Corneal curvatures and axial length measured by Pentacam AXL seemed to have good agreement with those measured by IOL Master.8,18,21 The 95% LoA between both devices was favorable, and the small difference should not have a significant effect to IOL power calculation. Lastly, we did not perform IOL calculations using these parameters, and this will be carried out in future study.
In conclusion, this study demonstrated that both Pentacam AXL and Galilei G6 provide good repeatability in overall parameters, except for steep meridians and anterior astigmatism. Comparing between the two devices, most parameters obtained from Pentacam AXL were statistically significantly different from those obtained from Galilei G6, with the exception of steep meridians and ACD. However, clinical relevance should be considered in individual parameters based on the objective of measurements. Further studies are warranted to clarify the effect of different measurements on the accuracy of IOL calculation and surgical outcomes.
Acknowledgments
The authors thank Ms. Sranya Phaisawang for English editing and proofreading. This study was supported by Navamindradhiraj University Research Fund. This fund had no role in the study design, data collection, and manuscript preparation.
Disclosures
The authors declare that there is no conflict of interest in this paper.
References
1. Martin R. Cornea and anterior eye assessment with placido-disc keratoscopy, slit scanning evaluation topography and scheimpflug imaging tomography. Indian J Ophthalmol. 2018;66(3):360–366.
2. Oliveira CM, Ribeiro C, Franco S. Corneal imaging with slit-scanning and Scheimpflug imaging techniques. Clin Exp Optom. 2011;94(1):33–42. doi:10.1111/j.1444-0938.2010.00509.x
3. Wang Q, Ding X, Savini G, et al. Anterior chamber depth measurements using Scheimpflug imaging and optical coherence tomography: repeatability, reproducibility, and agreement. J Cataract Refract Surg. 2015;41(1):178–185. doi:10.1016/j.jcrs.2014.04.038
4. Aramberri J, Araiz L, Garcia A, et al. Dual versus single Scheimpflug camera for anterior segment analysis: precision and agreement. J Cataract Refract Surg. 2012;38(11):1934–1949. doi:10.1016/j.jcrs.2012.06.049
5. Hernández-Camarena JC, Chirinos-Saldaña P, Navas A, et al. Repeatability, reproducibility, and agreement between three different Scheimpflug systems in measuring corneal and anterior segment biometry. J Refract Surg. 2014;30(9):616–621. doi:10.3928/1081597X-20140815-02
6. Crawford AZ, Patel DV, McGhee CNJ. Comparison and repeatability of keratometric and corneal power measurements obtained by Orbscan II, Pentacam, and Galilei corneal tomography systems. Am J Ophthalmol. 2013;156(1):53–60. doi:10.1016/j.ajo.2013.01.029
7. Salouti R, Nowroozzadeh MH, Zamani M, Ghoreyshi M, Salouti R. Comparison of anterior chamber depth measurements using Galilei, HR Pentacam, and Orbscan II. Optometry. 2010;81(1):35–39. doi:10.1016/j.optm.2009.04.100
8. Sel S, Stange J, Kaiser D, Kiraly L. Repeatability and agreement of Scheimpflug-based and swept-source optical biometry measurements. Cont Lens Anterior Eye. 2017;40(5):318–322. doi:10.1016/j.clae.2017.03.007
9. Ruiz-Mesa R, Abengózar-Vela A, Ruiz-Santos M. Comparison of a new Scheimpflug imaging combined with partial coherence interferometry biometer and a low-coherence reflectometry biometer. J Cataract Refract Surg. 2017;43(11):1406–1412. doi:10.1016/j.jcrs.2017.08.016
10. Jung S, Chin HS, Kim NR, Lee KW, Jung JW. Comparison of Repeatability and Agreement between Swept-Source Optical Biometry and Dual-Scheimpflug Topography. J Ophthalmol. 2017;2017:1516395. doi:10.1155/2017/1516395
11. Shin MC, Chung SY, Hwang HS, Han KE. Comparison of Two Optical Biometers. Optom Vis Sci. 2016;93(3):259–265. doi:10.1097/OPX.0000000000000799
12. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135–160. doi:10.1177/096228029900800204
13. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–310. doi:10.1016/S0140-6736(86)90837-8
14. Giavarina D. Understanding Bland Altman analysis. Biochem Med. 2015;25(2):141–151. doi:10.11613/BM.2015.015
15. Domínguez-Vicent A, Monsálvez-Romín D, Aguila-Carrasco AJD, García-Lázaro S, Montés-Micó R. Measurements of anterior chamber depth, white-to-white distance, anterior chamber angle, and pupil diameter using two Scheimpflug imaging devices. Arq Bras Oftalmol. 2014;77(4):233–237. doi:10.5935/0004-2749.20140060
16. Anayol MA, Güler E, Yağci R, et al. Comparison of central corneal thickness, thinnest corneal thickness, anterior chamber depth, and simulated keratometry using galilei, Pentacam, and Sirius devices. Cornea. 2014;33(6):582–586. doi:10.1097/ICO.0000000000000119
17. Sahin A, Hamrah P. Clinically relevant biometry. Curr Opin Ophthalmol. 2012;23(1):47–53. doi:10.1097/ICU.0b013e32834cd63e
18. Shajari M, Cremonese C, Petermann K, Singh P, Müller M, Kohnen T. Comparison of axial length, corneal curvature, and anterior chamber depth measurements of 2 recently introduced devices to a known biometer. Am J Ophthalmol. 2017;178:58–64. doi:10.1016/j.ajo.2017.02.027
19. Domínguez-Vicent A, Pérez-Vives C, Ferrer-Blasco T, García-Lázaro S, Montés-Micó R. Device interchangeability on anterior chamber depth and white-to-white measurements: a thorough literature review. Int J Ophthalmol. 2016;9(7):1057–1065.
20. Kawamorita T, Uozato H. Modulation transfer function and pupil size in multifocal and monofocal intraocular lenses in vitro. J Cataract Refract Surg. 2005;31(12):2379–2385. doi:10.1016/j.jcrs.2005.10.024
21. Muzyka-Woźniak M, Oleszko A. Comparison of anterior segment parameters and axial length measurements performed on a Scheimpflug device with biometry function and a reference optical biometer. Int Ophthalmol. 2019;39(5):1115–1122. doi:10.1007/s10792-018-0927-x
22. Ventura BV, Ventura MC, Wang L, Koch DD, Weikert MP. Comparison of biometry and intraocular lens power calculation performed by a new optical biometry device and a reference biometer. J Cataract Refract Surg. 2017;43(1):74–79. doi:10.1016/j.jcrs.2016.11.033
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.