Back to Journals » International Journal of Women's Health » Volume 18
Comparison of an Ultrasound-Based System and the Bishop Score for Predicting Labor Induction Timing in Singleton Pregnancies at Term: A Prospective Cohort Study
Authors Wu H ![]() , Wang Y, Yu L, Wang Q, Yang J, Shi J, Xu H, Weng Y, Chai Y
, Wang Y, Yu L, Wang Q, Yang J, Shi J, Xu H, Weng Y, Chai Y
Received 20 December 2025
Accepted for publication 22 February 2026
Published 27 February 2026 Volume 2026:18 590525
DOI https://doi.org/10.2147/IJWH.S590525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Hanglin Wu,1 Yun Wang,1 Liming Yu,1 Qiumeng Wang,1 Jiali Yang,1 Juanjuan Shi,1 Hongmiao Xu,1 Yinan Weng,2 Yun Chai1
1Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Ultrasound, Hangzhou Women’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Yun Chai, Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital, No. 369 Kun Peng Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: This study aimed to evaluate the predictive accuracy of a modified cervical assessment model incorporating objective measurements from the LaborPro system for successful induction of labor (IOL) in term singleton pregnancies.
Patients and Methods: This prospective observational cohort study was conducted at a tertiary center in China between August 2023 and November 2025. The study included women with term singleton pregnancies scheduled for IOL. Objective measurements of cervical length and fetal station were obtained using the LaborPro system, an ultrasound-guided magnetic tracking device. The primary outcome was successful IOL, defined as vaginal delivery within 24 hours of induction onset (VD24). Univariate and multivariate logistic regression analyses were employed to identify independent predictors, and the area under the receiver operating characteristic curve (AUC) was used to compare predictive performance.
Results: Of the 192 eligible women undergoing IOL, 84 (43.8%) achieved VD24. Multivariate analysis identified cervical length and fetal station as significant independent predictors of VD24. Each 1-cm increase in cervical length was associated with a 58% reduction in the odds of VD24 [Odds ratio (OR) 0.42, 95% confidence interval (CI) 0.19– 0.91], whereas each 1-cm descent in fetal station was associated with a nearly fivefold increase in the odds of VD24 (OR 4.84, 95% CI 2.05– 11.46). A combined model integrating objective assessments of cervical length and fetal station with clinical evaluations of cervical position and consistency demonstrated higher predictive accuracy (AUC = 0.856) compared to the traditional Bishop score (AUC = 0.600).
Conclusion: Objective assessment of cervical length and fetal station using the ultrasound-based LaborPro system provides reliable, independent prediction of IOL success. The integrated predictive model significantly outperforms the Bishop score alone. These findings support the clinical utility of objective ultrasound-based evaluations, particularly for optimizing IOL management in nulliparous women.
Keywords: ultrasound-based laborpro system, cervical ripening, induction of labor, prediction model, term pregnancy
Introduction
Induction of labor (IOL) refers to the deliberate initiation of labor prior to spontaneous onset, primarily aimed at reducing the risk of adverse maternal and fetal outcomes associated with prolonged pregnancy or expectant management. Recent national surveys have documented a steady increase in the rate of IOL across multiple countries.1–3 For example, in California, the proportion of deliveries involving IOL increased from 21.0% in 2015 to approximately 29.2% by 2019.4 As the frequency of IOL continues to rise, accurate pre-induction evaluation has become an essential component of clinical decision-making. Numerous factors have been investigated for their predictive value in determining the success of IOL; however, cervical ripening status prior to induction remains one of the most consistently significant predictors of favorable outcomes.5–7 This is particularly critical in nulliparous women, where improving the precision of labor induction success prediction could significantly reduce the incidence of unnecessary cesarean sections and enhance overall maternal and perinatal outcomes.
The Bishop score (BS), which includes assessment of cervical consistency, cervical position, cervical effacement, cervical dilation, and fetal station (FS), is endorsed by multiple clinical guidelines and commonly employed in routine obstetric practice.8–11 Despite its widespread use, the BS relies heavily on subjective clinical judgment, which may lead to variability in scoring between different clinicians. To address this limitation, several alternative methods for evaluating cervical readiness prior to IOL have been explored. These include transvaginal ultrasound measurements, levels of insulin-like growth factor-binding protein-1, interleukin-6, and the presence of vaginal fetal fibronectin.12–17 Systematic reviews comparing these biomarkers and imaging techniques in predicting IOL success have not identified a single method that consistently outperforms others.6,18,19 Moreover, none of these models adequately measures FS, which remains an important component of the BS.
The LaborPro system is an ultrasound-based tool that employs magnetic field and positional tracking technology to objectively assess fetal head station and position, as well as cervical length (CL). Although prior research has demonstrated its utility in monitoring fetal head descent during active labor.20,21 Its application in evaluating cervical readiness before induction remains uninvestigated. The present study aimed to evaluate the predictive accuracy of a modified cervical assessment model that incorporates LaborPro-derived measurements for successful IOL in women with term singleton pregnancies.
Materials and Methods
Study Population and Data Collection
This prospective observational cohort study was conducted between August 2023 and November 2025 at Hangzhou Women’s Hospital, a tertiary-level specialty hospital located in Hangzhou, China. The study design, data collection, and reporting procedures adhered strictly to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Ethical approval for the study was obtained from the hospital’s Medical Ethics Committee (Approval No. 2023-A-100). This study was conducted in accordance with the Declaration of Helsinki, and the confidentiality of all participant information was strictly maintained. Prior to enrollment, all participants provided written informed consent.
Eligible participants included pregnant women with a term, singleton pregnancy in cephalic presentation who were admitted to the hospital for scheduled IOL. Exclusion criteria consisted of: a history of prior cesarean delivery; fetal anomalies or medical contraindications to vaginal delivery (VD); and signs suggestive of imminent spontaneous labor, defined as regular uterine contractions with or without cervical dilation. Upon enrollment, baseline maternal characteristics and obstetric history were recorded in the hospital’s electronic medical record system. Following bladder emptying, patients were positioned in the dorsal lithotomy position and underwent a vaginal examination conducted by at least one experienced obstetrician to assess BS.
The LaborPro system (Trig Medical Ltd, Yokneam, Israel), an ultrasound-guided tracking device, was employed in conjunction with the collaborative input of an obstetrician and a radiology specialist trained in sonography. A low-intensity magnetic field was generated using a magnetic field emitter positioned beneath the patient’s body, with a tissue depth exceeding 5 cm to ensure consistent field penetration. Three compact position sensors (each with a diameter of 1.3 mm) were utilized to detect the magnetic field emitted by the transmitter. The system controller processed signals from these sensors to determine their precise three-dimensional spatial coordinates and orientation in real time. Each sensor was affixed to a distinct anatomical site: the index finger of the examiner, the maternal lumbosacral region (lower back), and the ultrasound probe handle, respectively. This configuration enabled accurate spatial measurement between any two defined points within the examination field, with a reported positional accuracy of 1.0 mm (Figure 1A).
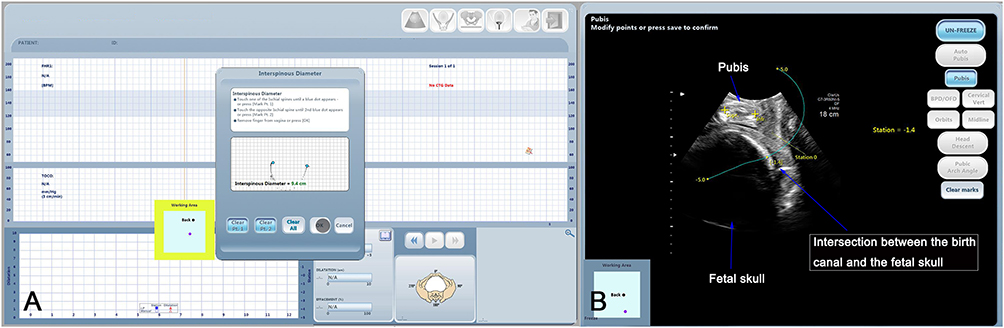 |
Figure 1 Screenshot of the LaborPro system. (A) Distance measurement. (B) Determination of fetal head station. |
CL was defined as the distance from the external cervical os to the point at which the cervical canal interfaced with the fetal presenting part. FS was assessed using infrapubic ultrasound imaging (Figure 1B), consistent with the methodology outlined in a previous study.20 Cervical position was evaluated relative to the imaginary line connecting the two ischial spines. A cervix was classified as anterior when its posterior lip lied above this line, posterior when its anterior lip lied below it, and central in all other cases. To minimize potential bias, the measurements obtained from the LaborPro system were withheld from clinical obstetricians responsible for determining the mode of labor induction and managing subsequent labor progression.
Patients with a BS of 6 or higher were administered intravenous oxytocin via a micro-infusion pump. The initial infusion rate was set at 5 drops per minute and was subsequently adjusted every 15 minutes in increments of 5 drops per minute, based on real-time assessments of uterine contraction frequency. In contrast, patients with a BS less than 6 received cervical ripening induction using either Propess™, a vaginal dinoprostone (10 mg) pessary (Ferring Pharmaceuticals Ltd, United Kingdom), or a Cook’s cervical ripening catheter (Cook Incorporated, Bloomington, Indiana, USA), with the choice determined by the clinical preference of the obstetric team. Indications for early removal of the dinoprostone suppository included the onset of spontaneous labor, rupture of membranes, uterine tachysystole, evidence of fetal distress, completion of a 24-hour duration of placement, or maternal adverse effects such as fever, vomiting, or hypotension. The Cook’s catheter was removed after 12 hours, following which the BS was reassessed. If labor did not commence following the initial IOL, additional methods of labor induction or artificial rupture of the membranes were employed, based on the most recent BS assessment. Failure of IOL was defined as the inability to initiate established labor within 18 hours after membrane rupture, despite continuous oxytocin infusion and active attempts to induce effective uterine contractions.9
Following delivery, labor stage characteristics and pregnancy outcomes were retrospectively collected from electronic medical records. The IOL time interval was defined as the time from the initiation of induction (via intravenous oxytocin, dinoprostone suppository, or Cook catheter placement) to delivery. The primary outcome of interest was successful IOL, defined as VD occurring within 24 hours of the initiation of IOL.22 Participants who achieved VD within 24 hours of IOL onset (VD24) were classified into the VD24 group. Those who delivered vaginally more than 24 hours after the start of IOL were assigned to the No-VD24 group.
Statistical Analysis
Continuous variables were summarized using means (standard deviations) or medians (interquartile ranges), depending on the distributional characteristics of the data. Categorical variables were described using absolute frequencies and corresponding percentages. The differences of quantitative variables between the groups were compared using the t test or Mann–Whitney U-test, while categorical variables were compared using the chi-squared test or Fisher’s exact test, as appropriate. Univariate and multivariate logistic regression models were used to examine associations between predictor variables and successful IOL following cervical ripening. To evaluate the discriminatory power of individual predictors, receiver operating characteristic (ROC) curves were constructed.23 The diagnostic performance of each variable was quantified by computing the area under the ROC curve (AUC) along with its 95% confidence interval (CI). Pairwise comparisons of AUCs were conducted using the DeLong test, with a p‑value < 0.05 considered statistically significant. To assess the stability and robustness of the primary findings, two sensitivity analyses were performed by sequentially excluding multiparous women and women with premature rupture of membranes, given potential differences in labor dynamics in these subgroups. All statistical analyses were carried out using RStudio version 2023.09.1 Build 494 within the R environment version 4.3.3 (released February 29, 2024).
The study was designed with statistical power based on historical data from our institution, which reported a VD24 rate of 50% and an intrapartum cesarean section rate of 15%. The modified cervical assessment protocol incorporated four dynamic indicators, comprising a total of eight measurable variables. According to established sample size estimation guidelines, at least 10 valid observations are required for each distinct category of an estimated parameter to ensure reliable statistical inference. Using this criterion, a minimum of 80 participants was required for the VD24 group.24–27 To account for an anticipated 5% dropout rate, the final estimated required sample size was adjusted to 199 women.
Results
During the study period, a total of 208 women were evaluated for eligibility. Five women were excluded due to cephalopelvic disproportion, and three declined to participate, resulting in the enrollment of 200 women. Of these, eight women experienced spontaneous labor prior to the planned induction, leaving 192 women who proceeded with IOL. Baseline demographic and clinical characteristics of the cohort are presented in Supplementary Table 1. After excluding 33 women who underwent cesarean delivery during labor and three cases with failed IOL, 156 women were included in the final analysis (Figure 2).
 |
Figure 2 Participant enrollment flowchart. |
Table 1 presents maternal characteristics and pregnancy outcomes in the VD24 and No-VD24 groups. Among all women who delivered vaginally, 84 (53.8%) achieved VD24. Women in the VD24 group were more likely to be multiparous and had a shorter CL and lower FS compared to the No-VD24 group. Correspondingly, the VD24 group had a higher BS (P = 0.026). Other maternal characteristics and neonatal weight were comparable between the groups.
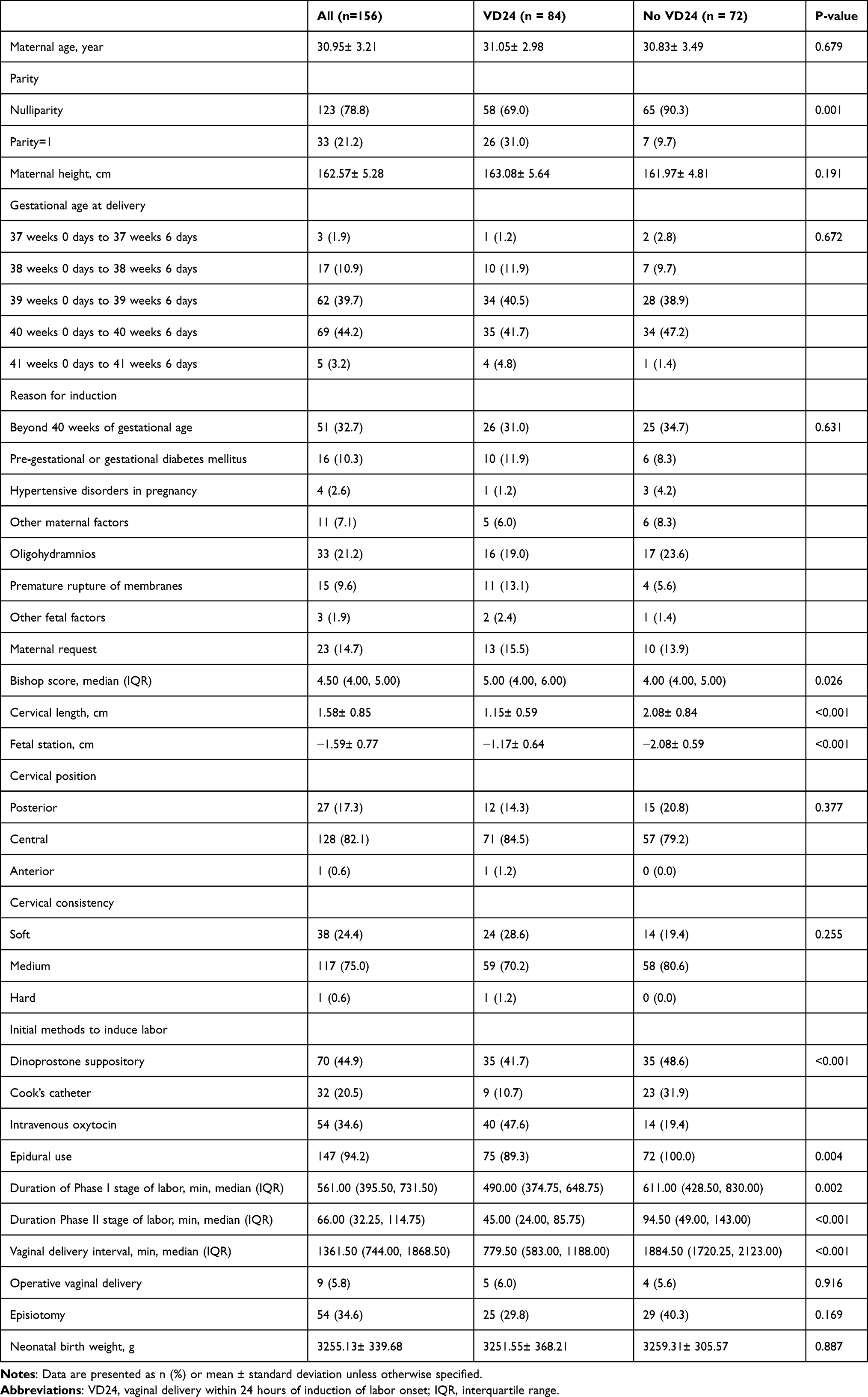 |
Table 1 Baseline Characteristics of All Women Who Delivered Vaginally |
Table 2 shows the results of univariable and multivariable logistic regression analyses for variables associated with successful cervical ripening leading to VD24. In univariable analysis, only CL and FS were significantly associated with VD24 (P < 0.05). Each one-point increase in BS was associated with a 30% increase in the odds of VD24, although this did not reach statistical significance (Odds ratio 1.30, 95% CI 0.99–1.71, P = 0.060). No significant association was observed between VD24 and cervical position or cervical consistency. Multivariable analysis confirmed significant independent associations between VD24 and CL (P = 0.029) and FS (P < 0.001). Specifically, each 1 cm increase in CL reduced the odds of VD24 by 58% (Odds ratio 0.42, 95% CI 0.19–0.91). Furthermore, each 1 cm descent in FS was associated with a nearly fivefold increase in the odds of VD24 (Odds ratio 4.84, 95% CI 2.05–11.46).
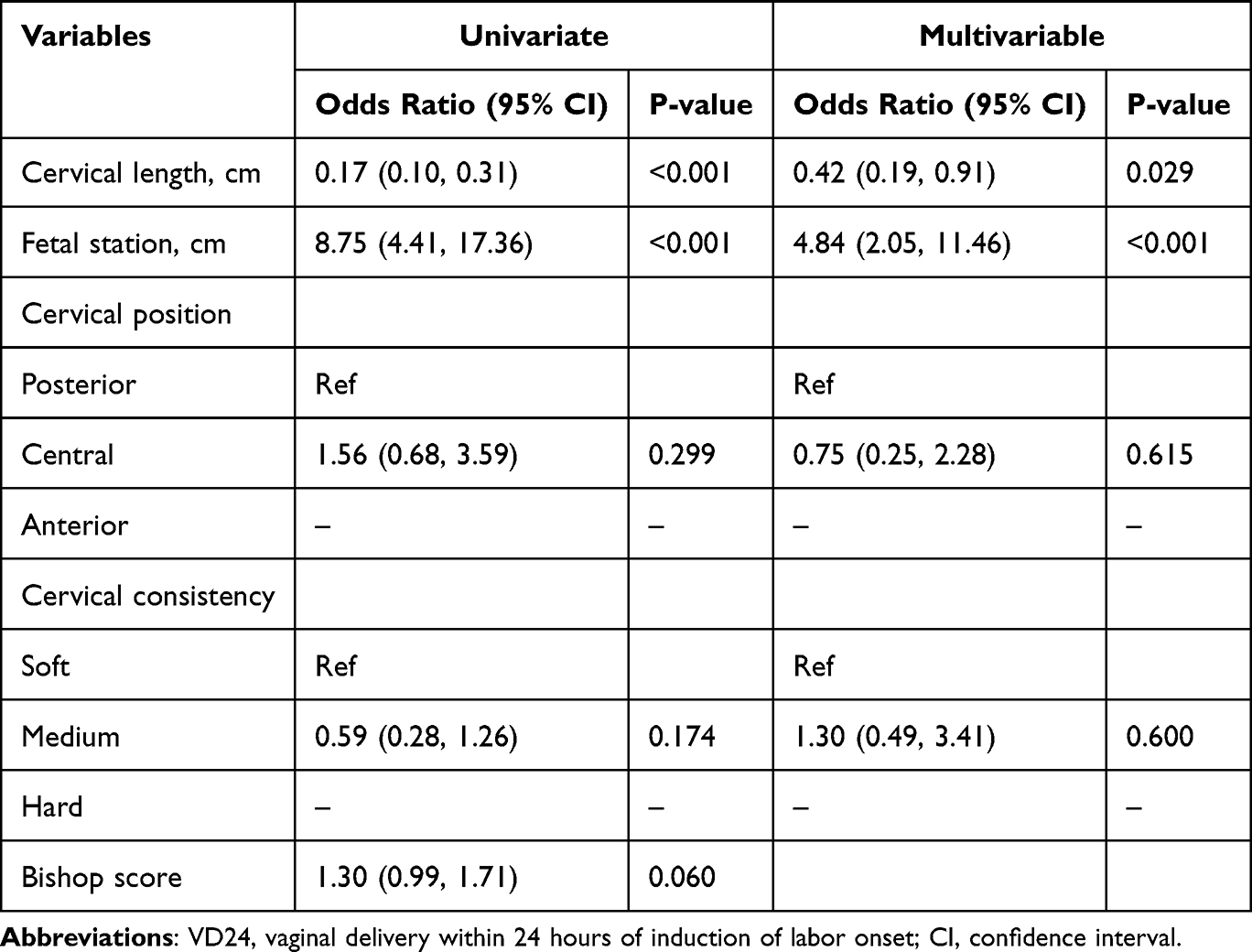 |
Table 2 Univariate and Multivariable Analyses of VD24 |
The AUC for BS in predicting VD24 was 0.600 (95% CI: 0.510–0.690; Figure 3). In comparison, the AUC for a model combining CL and FS was 0.843 (95% CI: 0.785–0.902). To simulate the BS, we integrated CL and FS with cervical position and consistency into a mixed model, which yielded an AUC of 0.856 (95% CI: 0.800–0.913). The DeLong test indicated that the predictive performance of both the CL/FS model and the mixed model was significantly superior to that of the BS alone (P < 0.001). Sensitivity analyses restricted to nulliparous women and to women with intact membranes yielded results consistent with the primary analysis (Supplementary Tables 2, 3, Supplementary Figures 1 and 2).
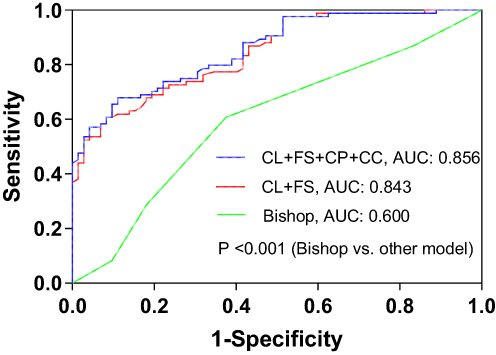 |
Figure 3 Receiver operating characteristic curves for modified cervical assessment models and the Bishop score. Abbreviations: AUC, area under the curve; CL, cervical length; FS, fetal station; CP, cervical position; CC, cervical consistency. |
Discussion
This study identified CL and FS as the key independent predictors of successful IOL. The predictive value for VD24 was significantly higher when CL and FS were measured objectively compared to assessment by the BS. This advantage was consistent across the study population and was particularly pronounced in nulliparous women.
Previous research has generally reported a positive association between shorter pre-induction CL and increased likelihood of successful IOL.12–14,28,29 For instance, a randomized controlled trial involving 154 women with singleton pregnancies at term demonstrated that ultrasound assessment of CL prior to IOL reduced the need for prostaglandin administration when compared to clinical evaluation using the BS.14 Similarly, Kehila et al found that ultrasound measurement of CL was a more accurate predictor of favorable cervical ripening and VD24 in nulliparous women at 41 weeks’ gestation with an unfavorable cervix, compared to BS.29 Additionally, Hamza et al identified a CL ≤25 mm and presence of cervical funneling as significant predictors of successful IOL within 24 hours.30 Our findings are consistent with these observations, showing that each 1 cm increase in CL was associated with a halving of the odds for achieving VD24. Notably, our method for measuring CL differed from previous studies. We employed direct measurement between marked points, an approach more analogous to clinical BS assessment. In contrast, several studies have reported higher predictive accuracy for the BS compared to ultrasound-measured CL.31,32 This discrepancy may be attributable to differences in study population characteristics and the definition of the primary outcome. For instance, the latter two studies defined successful IOL as an induction-to-delivery interval within 12 hours.
In addition to cervical shortening, descent of the fetal presenting part is a key marker of labor onset. Therefore, assessing FS is particularly important when evaluating candidates for labor induction. A high station may prevent adequate contact with the cervix, impeding the initiation of effective uterine contractions, which can reduce the success rate of induction and prolong its duration.33 To our knowledge, our study is the first to evaluate the predictive value of objectively measured FS data. We found that FS was the strongest predictor of successful IOL (p < 0.001), outperforming CL and other variables. This finding aligns with a recent systematic review and meta-analysis, which reported the highest predictive accuracy for successful IOL using sonographic fetal head-perineum distance,34 although this measurement may not perfectly reflect true FS due to individual variation in vaginal length.
Our study found no significant association between cervical position or consistency and successful IOL. This finding supports a recently published prospective observational cohort,35 but contrasts with earlier studies.13,36–38 Two related factors may explain this discrepancy. First, the aforementioned studies employed ultrasonographic variables, including cervical strain elastography, which may provide more objective measures than the digital vaginal examination used in our study. Second, in our cohort, only a small number of women were categorized as having an anterior position or a hard cervix, which likely reduced the statistical power to detect a significant association.
Notably, in the present study, the model demonstrated the highest predictive accuracy for VD24 among nulliparous women. This result may be explained by distinct patterns of labor progression observed between nulliparous and multiparous individuals.33 Nulliparous women generally experience fetal descent later in pregnancy and require full cervical effacement prior to transitioning into active labor. In contrast, multiparous women often exhibit concurrent cervical effacement and dilation, which is associated with shorter labor durations and a greater likelihood of achieving VD24. As a result, the exclusion of multiparous women in the sensitivity analysis led to an improvement in model performance compared to the primary analysis, suggesting that inclusion of this group may have introduced variability that reduced predictive precision.
Our study employed a rigorous prospective cohort design with an adequately sample size, thereby minimizing confounding biases and enhancing the reliability and validity of the findings. The use of the ultrasound-based LaborPro system enabled precise measurement of FS, which is typically not obtainable through conventional ultrasound imaging. Despite these strengths, several limitations should be acknowledged. First, as a single-center study, the generalizability of the results to broader or diverse clinical settings may be limited. Our results were derived from a population where grand multiparity was absent, and thus the findings should be interpreted with caution when applied to women with higher parity. Second, the reliance on the LaborPro system for acquiring highly accurate measurements restricts the feasibility of implementing this approach in regions lacking access to such advanced technology. Third, all participants underwent IOL based on BS, which makes it difficult to determine whether the proposed modified model offers superior clinical utility compared to standard BS-guided decision-making. Lastly, cervical consistency and cervical position were not quantified using ultrasonographic assessment, which may have influenced the overall predictive accuracy of the final model.
Conclusion
Our study demonstrated that CL and FS are reliable, independent predictors of successful IOL. The predictive accuracy achieved through objective measurement of CL and FS using the ultrasound-based LaborPro system was superior to that of the BS alone. Future studies are warranted to validate the predictive value of this modified assessment model, particularly in nulliparous women.
Funding
This study was supported by two research initiatives: the Hangzhou Specialised Scientific Programme for Supporting Biological Duty and Health Industry Development entitled “Study on the Value of Three-dimensional Intrapartum Navigation System in Prenatal Cephalopelvic Disproportion Assessment” (No.2022WJC057), and the Hangzhou Specialised Scientific Programme for Supporting Biological Duty and Health Industry Development entitled “ Value of a Three-Dimensional Labor Navigation System in Assessing Cervical Ripening” (No.2023WJC006).
Disclosure
The authors report no conflicts of interest in this work.
This trial was registered at Chinese Medical Research Registration and Record-filing Information System (MR-33-23-040694).
References
1. Zhu J, Xue L, Shen H, et al. Labor induction in China: a nationwide survey. BMC Pregnancy Childbirth. 2022;22:463. doi:10.1186/s12884-022-04760-6
2. Haavaldsen C, Morken NH, Saugstad OD, et al. Is the increasing prevalence of labor induction accompanied by changes in pregnancy outcomes? An observational study of all singleton births at gestational weeks 37-42 in Norway during 1999-2019. Acta Obstet Gynecol Scand. 2023;102(2):158–10. doi:10.1111/aogs.14489
3. Wood R, Freret TS, Clapp M, et al. Rates of induction of labor at 39 weeks and cesarean delivery following publication of the ARRIVE trial. JAMA Netw Open. 2023;6:e2328274.
4. Rosenstein MG, Chang SC, Tucker CM, et al. Evaluation of statewide program to reduce cesarean deliveries among nulliparous individuals with singleton pregnancies at term gestation in vertex presentation. Obstet Gynecol. 2024;144(4):507–515. doi:10.1097/AOG.0000000000005696
5. Kamlungkuea T, Manonai J, Suriyawongpaisal P, et al. Factors predicting successful vaginal delivery following induction of labor in term pregnancy. Int J Womens Health. 2022;14:245–255. doi:10.2147/IJWH.S347878
6. Ezebialu IU, Eke AC, Eleje GU, et al. Methods for assessing pre-induction cervical ripening. Cochrane Database Syst Rev. 2015;2015(6):CD010762. doi:10.1002/14651858.CD010762.pub2
7. Won YB, Han SW, Kim EH. Clinical factors and ultrasound parameters to predict successful vaginal delivery following labour induction. J Obstet Gynaecol. 2020;40(3):360–366. doi:10.1080/01443615.2019.1647516
8. Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol. 1964;24:266–268.
9. Obstetrics Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association. Guideline of cervical ripening and labor induction during the third trimester pregnancy (2024). Zhonghua Fu Chan Ke Za Zhi. 2024;59:819–828. doi:10.3760/cma.j.cn112141-20240707-00381
10. Kaimal AJ, Reddy UM, Gillispie-Bell V. Cervical ripening in pregnancy: ACOG clinical practice guideline no. 9. Obstet Gynecol. 2025;146:148–160. doi:10.1097/AOG.0000000000005951
11. Robinson D, Campbell K, Hobson SR, et al. Guideline no. 432b: cervical ripening. J Obstet Gynaecol Can. 2023;45(1):56–62.e1. doi:10.1016/j.jogc.2022.11.007
12. Wei N, Wang Z. Multivariate analysis of determinants and development of a predictive algorithm for successful labor induction in nulliparous women. BMC Pregnancy Childbirth. 2025;25:1207. doi:10.1186/s12884-025-08315-3
13. Abdullah ZHA, Chew KT, Velayudham VRV, et al. Pre-induction cervical assessment using transvaginal ultrasound versus Bishops cervical scoring as predictors of successful induction of labour in term pregnancies: a hospital-based comparative clinical trial. PLoS One. 2022;17(e0262387):e0262387. doi:10.1371/journal.pone.0262387
14. Park KH, Kim SN, Lee SY, et al. Comparison between sonographic cervical length and bishop score in preinduction cervical assessment: a randomized trial. Ultrasound Obstet Gynecol. 2011;38(2):198–204. doi:10.1002/uog.9020
15. Okafor CG, Eleje GU, Adinma JI, et al. A randomized clinical trial of premaquick biomarkers versus transvaginal cervical length for pre-induction cervical assessment at term among pregnant women. SAGE Open Med. 2023;11:20503121231158220. doi:10.1177/20503121231158220
16. Garite TJ, Casal D, Garcia-Alonso A, et al. Fetal fibronectin: a new tool for the prediction of successful induction of labor. Am J Obstet Gynecol. 1996;175:1516–1521. doi:10.1016/S0002-9378(96)70100-X
17. Eleje GU, Ezugwu EC, Ugwu EO, et al. Premaquick© versus modified bishop score for preinduction cervical assessment at term: a double-blind randomized trial. J Obstet Gynaecol Res. 2018;44:1404–1414. doi:10.1111/jog.13691
18. Verhoeven CJ, Opmeer BC, Oei SG, et al. Transvaginal sonographic assessment of cervical length and wedging for predicting outcome of labor induction at term: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2013;42(5):500–508. doi:10.1002/uog.12467
19. Londero AP, Schmitz R, Bertozzi S, et al. Diagnostic accuracy of cervical elastography in predicting labor induction success: a systematic review and meta-analysis. J Perinat Med. 2016;44(2):167–178. doi:10.1515/jpm-2015-0035
20. Vitner D, Paltieli Y, Haberman S, et al. Prospective multicenter study of ultrasound-based measurements of fetal head station and position throughout labor. Ultrasound Obstet Gynecol. 2015;46(5):611–615. doi:10.1002/uog.14821
21. Nizard J, Haberman S, Paltieli Y, et al. Determination of fetal head station and position during labor: a new technique that combines ultrasound and a position-tracking system. Am J Obstet Gynecol. 2009;200(4):404.e1–5. doi:10.1016/j.ajog.2008.10.051
22. Volpe N, Ramirez Zegarra R, Melandri E, et al. Association between the cervical sliding sign and successful induction of labor in women with an unfavorable cervix: a prospective observational study. Eur J Obstet Gynecol Reprod Biol. 2022;278:16–21. doi:10.1016/j.ejogrb.2022.09.004
23. Zhou ZR, Wang WW, Li Y, et al. In-depth mining of clinical data: the construction of clinical prediction model with R. Ann Transl Med. 2019;7:796. doi:10.21037/atm.2019.08.63
24. Peduzzi P, Concato J, Feinstein AR, et al. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48(12):1503–1510. doi:10.1016/0895-4356(95)00048-8
25. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
26. Moons KG, de Groot JA, Bouwmeester W, et al. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: the CHARMS checklist. PLoS Med. 2014;11:e1001744.
27. Pavlou M, Ambler G, Seaman S, et al. Review and evaluation of penalised regression methods for risk prediction in low-dimensional data with few events. Stat Med. 2016;35(7):1159–1177. doi:10.1002/sim.6782
28. Vince K, Poljičanin T, Matijević R. Comparison of transvaginal sonographic cervical length measurement and bishop score for predicting labour induction outcomes. J Perinat Med. 2022;50(9):1198–1202. doi:10.1515/jpm-2022-0140
29. Kehila M, Bougmiza I, Ben Hmid R, et al. Bishop score vs. ultrasound cervical length in the prediction of cervical ripening success and vaginal delivery in nulliparous women. Minerva Ginecol. 2015;67(6):499–505.
30. Hamza A, Radosa J, Gerlinger C, et al. Cervical and lower uterine parameter ultrasound and elastographic parameters for the prediction of a successful induction of labor. Ultraschall Med. 2021;42(05):520–528. doi:10.1055/a-1131-7736
31. Bahadori F, Ayatollahi H, Naghavi-Behzad M, et al. Predicting factors on cervical ripening and response to induction in women pregnant over 37 weeks. Med Ultrason. 2013;15:191–198. doi:10.11152/mu.2013.2066.153.fb1ha2
32. Khandelwal R, Patel P, Pitre D, et al. Comparison of cervical length measured by transvaginal ultrasonography and bishop score in predicting response to labor induction. J Obstet Gynaecol India. 2018;68(1):51–57. doi:10.1007/s13224-017-1027-y
33. Hamilton EF, Romero R, Tarca AL, et al. The evolution of the labor curve and its implications for clinical practice: the relationship between cervical dilation, station, and time during labor. Am J Obstet Gynecol. 2023;228(5):S1050–S1062. doi:10.1016/j.ajog.2022.12.005
34. Shi Q, Wang Q, Tian S, et al. Assessment of different sonographic cervical measures to predict labor induction outcomes: a systematic review and meta-analysis. Quant Imaging Med Surg. 2023;13(12):8462–8477. doi:10.21037/qims-23-507
35. Xodo S, Martino M, Baccarini G, et al. What trans-vaginal ultrasound parameters are better correlated with a shorter labor induction to vaginal delivery interval? A prospective observational cohort study. J Matern Fetal Neonatal Med. 2025;38(1):2522997. doi:10.1080/14767058.2025.2522997
36. Hong SJ, Jung YM, Hwang JE, et al. Role of cervical elastography in predicting progression to active phase in labor induction in term nulliparous women. Diagnostics. 2025;15(4):500. doi:10.3390/diagnostics15040500
37. Eser A, Ozkaya E. Uterocervical angle: an ultrasound screening tool to predict satisfactory response to labor induction. J Matern Fetal Neonatal Med. 2020;33(8):1295–1301. doi:10.1080/14767058.2018.1517324
38. Kim EJ, Heo JM, Kim HY, et al. The value of posterior cervical angle as a predictor of vaginal delivery: a preliminary study. Diagnostics. 2021;11:1977. doi:10.3390/diagnostics11111977
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of a Model to Predict Cesarean Delivery as the Outcome of a Failed Labor Induction in Singleton Obese Pregnant Women at Term
Feng Y, Luan Y, Zhou L, Yin C
International Journal of Women's Health 2025, 17:5277-5286
Published Date: 9 December 2025