Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of Amniotic Membrane Extract and Insulin Eye Drops for the Management of Persistent Epithelial Defects: A Multicenter Retrospective Study
Authors Buzzi M ![]() , Mancini A, Vitiello L
, Mancini A, Vitiello L ![]() , Taloni A, Pintus B, Carnevali A, Carnovale-Scalzo G, Calabresi V
, Taloni A, Pintus B, Carnevali A, Carnovale-Scalzo G, Calabresi V ![]() , Lixi F
, Lixi F ![]() , Coco G
, Coco G ![]() , Romualdi G, Lucisano A, Verdiglione M, Mencucci R, Scorcia V, Giannaccare G
, Romualdi G, Lucisano A, Verdiglione M, Mencucci R, Scorcia V, Giannaccare G ![]()
Received 19 August 2025
Accepted for publication 30 November 2025
Published 3 December 2025 Volume 2025:19 Pages 4413—4420
DOI https://doi.org/10.2147/OPTH.S561775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Matilde Buzzi,1,* Alessandra Mancini,2,* Livio Vitiello,3 Andrea Taloni,4– 6 Benedetta Pintus,7 Adriano Carnevali,2 Giovanna Carnovale-Scalzo,2 Valerio Calabresi,7 Filippo Lixi,7 Giulia Coco,8 Giovanni Romualdi,1 Andrea Lucisano,2 Mario Verdiglione,9 Rita Mencucci,1 Vincenzo Scorcia,2 Giuseppe Giannaccare7
1Eye Clinic, Department of Neuroscience, Psychology, Pharmacology and Child Health (NEUROFARBA), University of Florence, Florence, Italy; 2Department of Ophthalmology, University Magna Graecia of Catanzaro, Catanzaro, Italy; 3Eye Unit, “Luigi Curto” Hospital, Azienda Sanitaria Locale Salerno, Polla, Italy; 4Department of Translational Medicine, University of Ferrara, Ferrara, Italy; 5Department of Ophthalmology, Ospedali Privati Forlì “Villa Igea”, Forlì, Italy; 6Istituto Internazionale per la Ricerca e Formazione in Oftalmologia, Forlì, Italy; 7Eye Clinic, Department of Surgical Sciences, University of Cagliari, Cagliari, Italy; 8Ophthalmology Unit, Department of Clinical Sciences and Translational Medicine, University of Rome Tor Vergata, Rome, Italy; 9Apotiga Laboratory, Farmacia Europea, Catanzaro, Italy
*These authors contributed equally to this work
Correspondence: Livio Vitiello, Eye Unit, “Luigi Curto” Hospital, Azienda Sanitaria Locale Salerno, Polla, Italy, Tel +00393491638307, Email [email protected]
Purpose: To compare the efficacy and safety of topical insulin and amniotic membrane extract eye drops (AMEED) in promoting healing of corneal persistent epithelial defects (PEDs) refractory to conventional therapy.
Patients and Methods: This retrospective comparative study included 27 eyes of 24 patients (mean age 61.0 ± 16.6 years) with PEDs treated with either topical insulin (1 IU/mL) or AMEED four times daily. Clinical outcomes included complete epithelial closure, rate of epithelialization, change in best-corrected visual acuity (BCVA), and occurrence of adverse events.
Results: Of 27 eyes, 18 received topical insulin and 9 received AMEED. The mean interval from diagnosis to treatment initiation was 93.4 ± 111.7 days in the AMEED group and 72.5 ± 56.1 days in the insulin group. Complete healing occurred in all eyes (100%) in the insulin group versus 44.4% in the AMEED group. The daily reduction in epithelial defect area during the first two weeks was significantly greater with insulin (P = 0.04). At final follow-up, BCVA improved significantly only in the insulin group (P = 0.006). No adverse reactions were observed in either group; one AMEED-treated eye required amniotic membrane transplantation.
Conclusion: Topical insulin and AMEED are both safe and effective for refractory PEDs, but insulin showed superior epithelial healing and visual recovery. Given its availability, low cost, and favorable safety profile, topical insulin may represent a practical alternative in the management of persistent epithelial defects.
Keywords: persistent epithelial defect, cornea, ulcer, insulin, amniotic membrane extract, corneal ulcer
Introduction
Persistent epithelial defects (PEDs) represent a challenging pathological condition of the cornea that fails to heal within two weeks despite treatment.1 The etiopathogenic mechanisms underlying PEDs are various, including dry eye disease (DED), neurotrophic keratopathy (NK), infectious keratitis, bullous keratopathy and limbal stem cell deficiency, among others.1 Disruption of epithelial homeostasis is often sustained by tear film dysfunction since altered tear composition increases corneal epithelial friction and inflammation.2 Chronic oxidative stress further exacerbates epithelial damage and slows the healing process through elevated production of pro-inflammatory cytokines.3,4 Additional factors such as eyelid abnormalities, genetic predisposition, or abuse of toxic medications can induce or exacerbate PEDs.1,5 The compromised epithelial integrity affects not only corneal transparency but also increases the risk of microbial superinfection, corneal melting or even perforation.1 Therefore, the main goal of PEDs treatment is to create an environment favorable to the migration and proliferation of regenerating epithelial cells,6 preventing the development of serious sight-threatening complications. Treatment options vary based on their underlying cause and disease severity. First-line therapies commonly include washout of epitheliotoxic treatments, preservative-free tear substitutes, ophthalmic ointments and bandage contact lenses (BCLs). More severe cases typically require second-line treatments, such as autologous serum eye drops, tarsorrhaphy, amniotic membrane (AM) transplantation, or conjunctival graft.1 Insulin-based eye drops are among the most promising emerging topical treatments thanks to their effectiveness in stimulating corneal epithelial migration and proliferation, facilitating faster defect resolution.7 Insulin exerts its therapeutic effect primarily through promoting nerve regeneration and activating limbal stem cells. Additionally, insulin and insulin-like growth factor 1 (IGF-1) activate key intracellular signaling pathways such as PI3K/Akt and MAPK/Erk, essential for enhancing epithelial regeneration and improving corneal sensitivity, particularly in NK.8
Similarly, amniotic membrane extract eye drops (AMEED) have recently gained attention, demonstrating considerable potential in accelerating epithelial healing due to their regenerative, anti-inflammatory, and anti-scarring properties.9 The regenerative capacity of AMEED is particularly valuable in corneal epithelial repair, promoting tissue regeneration and providing an ideal biological matrix for healing.10
Persistent epithelial defects (PEDs) affect approximately 0.1–0.5% of patients with corneal diseases and often result in significant visual morbidity and healthcare burden. Although both topical insulin and amniotic membrane extract eye drops (AMEED) have independently demonstrated efficacy in promoting corneal re-epithelialization, no direct comparative studies have been conducted to date. Clarifying their relative effectiveness is clinically relevant to guide therapeutic choice, especially considering differences in availability, cost, and handling requirements.1,9,11
The purpose of this study is to compare the efficacy of AMEED and insulin-based eye drops for the treatment of PEDs, with specific emphasis on healing characteristics and patients outcomes.
Materials and Methods
This retrospective study includes data from consecutive patients with refractory PEDs treated with AMEED or insulin eye drops between February 2023 and December 2024 at three University centers in Italy (University Magna Graecia of Catanzaro, University of Florence, and University of Cagliari). This retrospective study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The protocol was reviewed and approved by the Comitato Etico Territoriale Regione Calabria (protocol n. 51–2025, approval date 27 February 2025). Given the retrospective design and use of anonymized clinical data, the Ethics Committee waived the requirement for obtaining individual informed consent. All patient data were handled in a strictly confidential and anonymized manner to ensure privacy.
Medical charts of patients with a diagnosis of PED who had shown no improvement after receiving standard treatment (preservative-free tear substitutes, ophthalmic ointments, BCLs) and subsequently treated with either insulin eye drops or AMEED were reviewed. Patients were excluded in case of incomplete data of follow-up visits, failure to attend scheduled visits or lack of adequate slit-lamp pictures. Both insulin eye drops or AMEED were administered 4 times a day (every 6 hours). Supportive treatments, including preservative-free tear substitutes and nocturnal ointments were continued for all patients unchanged, along with disease-specific medications (ie, antiviral tablets for patients with history of herpetic keratitis).
Study variables included patient sex, age, treated eye (right or left), ocular diseases, systemic comorbidities, history of previous ocular surgeries and time since PED diagnosis. The etiology was categorized into the following groups: neurotrophic (post-herpetic, trigeminal nerve damage and post-surgical, ie post keratoplasty, glaucoma and vitreo-retinal surgeries), ocular surface diseases (DED, mucous membrane pemphigoid, other) and post-traumatic (chemical burn).
Baseline data included best corrected visual acuity (BCVA), PED area (mm2), presence of stromal ulceration, corneal sensitivity (measured with cotton-swab and classified as normal, reduced or absent), lid position and dynamics, contact lens use and type, concomitant topical and systemic treatments, and surgical treatments. Follow-up data included PED area at each visit, complications or need for surgery, BCVA (final follow-up), time to complete healing, recurrence of the PED, and epithelialization speed (calculated as the difference between PED area at the last available follow-up and at baseline divided by the number of days in which the epithelialization occurred).
For the evaluation of PED area, anterior segment slit-lamp picture of the cornea was obtained at each visit following fluorescein dye administration. The images were analyzed using an image analysis system (ImageJ software, version 1.53, NIH, Bethesda Maryland, USA) to determine the PED area in mm2. Complete healing was defined as the absence of areas of the cornea positive to fluorescein staining except for punctate keratopathy.
Products Preparation
The formulation of insulin eye drops was prepared by a compounding pharmacy (Apotiga-Laboratorio Galenico, Farmacia Europea, Catanzaro, Italy) in a grade D cleanroom at a concentration of 1 IU/mL using insulin in solution for subcutaneous injection (Humalog® sc 5cart 3mL 100 IU/mL, Eli Lilly Italia Spa, Italy). The preparation involved dissolving the insulin in a carefully designed ophthalmic vehicle composed of polyethylene glycol 400 (0.4% w/v) and propylene glycol (0.3% w/v), which serve as demulcents, along with additional excipients to optimize the physicochemical properties of the formulation. The composition includes hydroxypropyl guar (0.16% w/v), boric acid (0.7% w/v), sorbitol (1.4% w/v), potassium chloride (0.12% w/v), sodium chloride (0.1% w/v), and 2-amino-2-methylpropanol (0.57% w/v) as a buffering agent, with purified water used as the solvent. The final pH was adjusted to 7.9 using sodium hydroxide and hydrochloric acid. The formulation is based on a galactomannan-borate polymer matrix, which enhances the retention time of the active ingredient on the ocular surface and allows a controlled and prolonged drug release. Upon instillation, sorbitol facilitates the diffusion of borate, leading to the formation of a polymer network in situ, which contributes to the enhanced mucoadhesion and prolonged therapeutic effect. The entire preparation process was conducted in a Grade D cleanroom, while critical sterilization steps were performed under laminar airflow within an ISO 4.8 (Grade A) isolator. The final solution was filtered through a 0.22 µm sterile filtration system (Stericup® Quick Release, Merck Millipore, MC2, Clermont-Ferrand, France) to ensure sterility before being packaged into 5 mL multidose low-density polyethylene (LDPE) dropper bottles (Acef Spa). The final product was stored at 2–8 °C, with a maximum shelf life of 30 days post-preparation. AMEED were prepared at the Eye Bank of Lucca (Centro Conservazione Cornee “Piero Perelli”, Lucca, Italy). Placentas were collected from elective caesarean delivery donors after informed consent; donors were serologically screened, samples for microbiological testing were taken during the collection and placentas were taken to the tissue bank, where a specialized team processed the tissue in aseptical environment. After rinsing the placenta to remove blood clots, a detachment of the AM by blunt dissection was performed. Then, the AM was rinsed and divided into fragments. Amniotic membrane fragments were then decontaminated in an antibiotic and antimycotic solution containing amphotericin B, penicillin, streptomycin and neomycin sulfate. The following day, each 10 AM fragments were homogenized with 50 mL balanced salt solution (BSS). The obtained AM extract was put into 5 mL vials and stored at −80°C temperature, where it can be preserved up to 2 years. During the preparation process, 5 sterility tests were performed at different timepoints. After thawing, AMEED can be stored at refrigerator temperature (4°C) for up to 7 days.
Statistical Analysis
BCVA was assessed using a Snellen chart. Decimal visual acuity was converted to the logarithm of the minimum angle of resolution (Log MAR) for statistical purposes. Study variables were expressed as mean ± standard deviation (95% confidence interval [CI]). The Shapiro–Wilk test was used to assess the normality of data. The Mann–Whitney U-test was used to compare the reduction rate of corneal ulcer area between patients treated with AMEED and those treated with insulin. All tests were two-sided and a P value < 0.05 was considered statistically significant. All data were entered into Microsoft Office Excel 365 (Microsoft Corp., Redmond, WA) and analyzed with GraphPad Prism (version 10.3.1; GraphPad Software Inc., San Diego, CA). Data is available from the corresponding author upon reasonable request.
Results
A total of 27 eyes of 24 patients (mean age 61.0 ± 16.6 years [95% CI, 54.5–67.6]) affected by PED were included in the study. Of these, 18 eyes were treated with insulin eye drops while 9 with AMEED. Detailed baseline data for the two study groups are reported in Table 1.
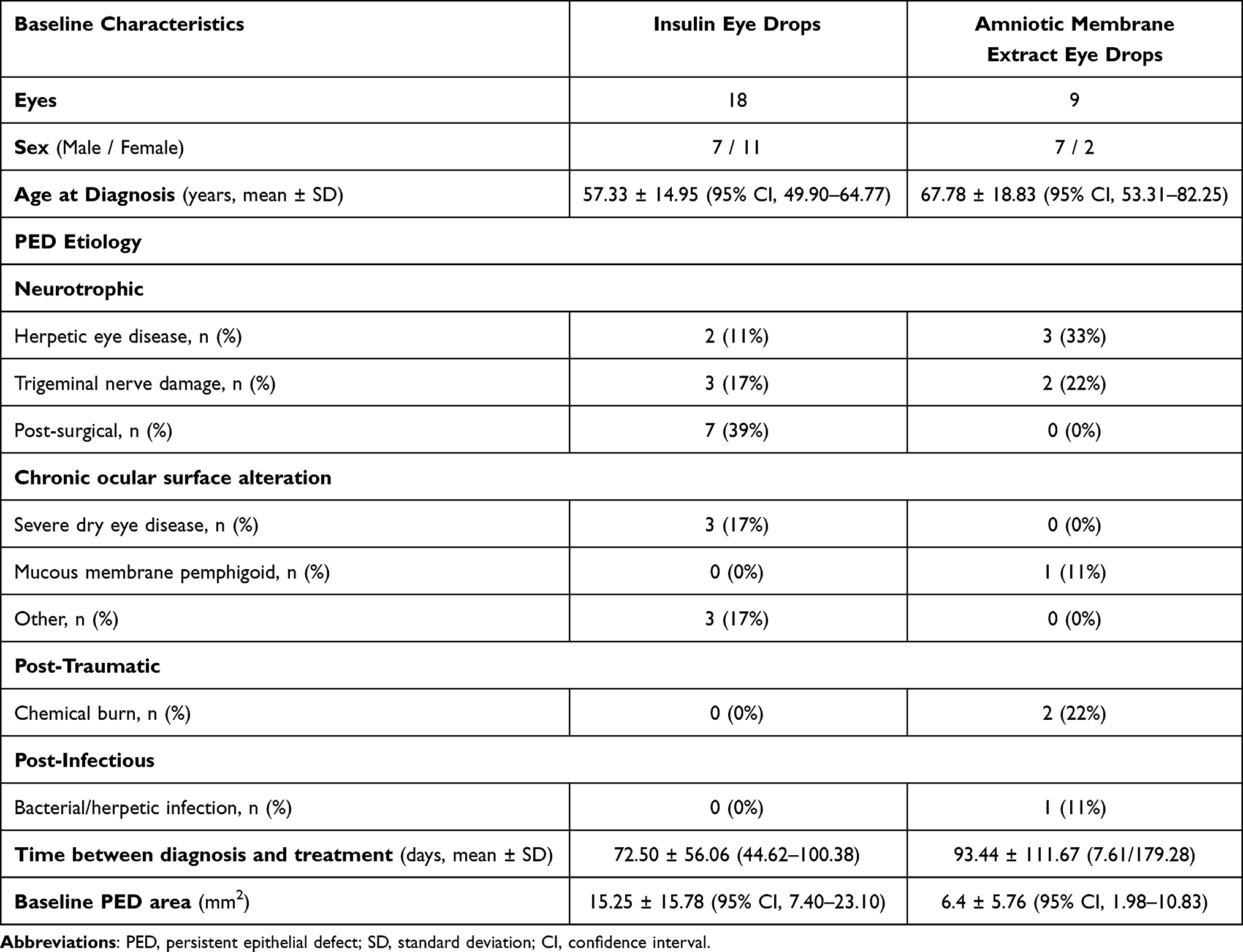 |
Table 1 Demographical and Clinical Data of Patients with Corneal Persistent Epithelial Defects Treated with Topical Insulin Eye Drops and Amniotic Membrane Extract Eye Drops |
The mean time between diagnosis and treatment initiation was 79.5 ± 77.4 days (95% CI, 48.9–110.1). At baseline, BCVA was 1.45 ± 0.81 Log MAR (95% CI, 1.13–1.77) and PED area was 13.27 ± 14.50 mm2 (95% CI, 7.76–18.79). Stromal ulceration was present in 3 eyes (11.1%). The most common PED etiology was neurotrophic. Corneal sensation was absent in 17 eyes (62.7%), reduced in 5 eyes (18.5%), normal in one eye (3.7%), not measurable in 4 eyes. Regarding lid position and dynamics, symblepharon was observed in 5 eyes (18.5%), floppy eyelid syndrome in 2 eyes (7.4%). Three patients in the insulin group (16.7%) received a drug depository contact lens (DDCL) aiming at increasing the topical drug residence time; in one patient of the AMEED group (11%) a BCL was applied due to trichiasis.
Of 9 eyes treated with AMEED and followed-up for 26.6 ± 16.0 days (95% CI, 14.27–38.84; range: 7–63), 4 (44.4%) achieved complete corneal healing. Conversely, all the 18 eyes treated with insulin eye drops healed completely (100%), during a follow-up time of 29.78 ± 11.70 days (95% CI, 23.96–35.60). The epithelial defect area at different time points is shown in box plots for the AMEED group (Figure 1A) and the insulin group (Figure 1B).
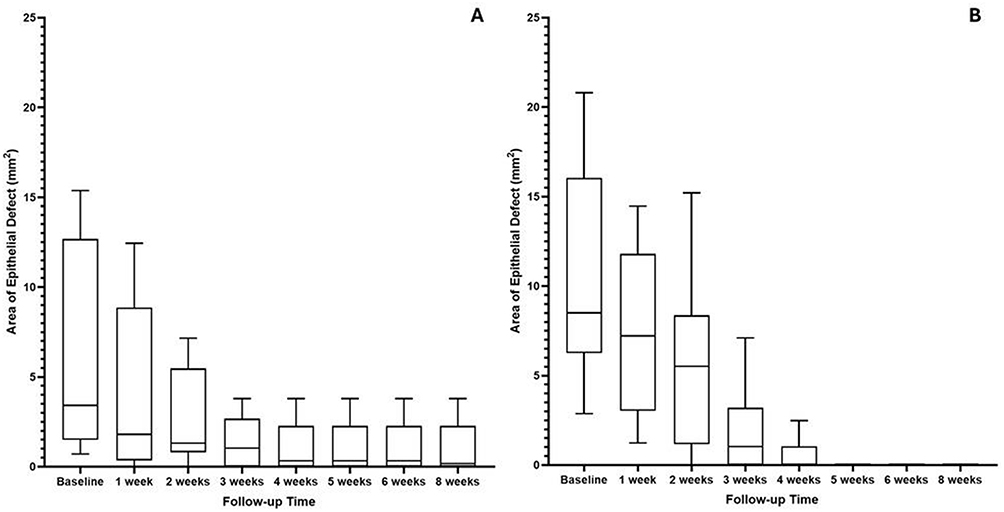 |
Figure 1 (A and B) Box-plot representation of the persistent epithelial defect (PED) area at each follow-up timepoint for the amniotic membrane extract eye drops (AMEED) group (A) and the insulin group (B), showing the distribution and variability of healing within each treatment arm. |
The total reduction in PED area at the final follow-up visit was −4.82 ± 4.95 mm2 (95% CI, −8.63 to −1.01) and −15.25 ± 15.78 mm2 (95% CI, −23.10 to −7.40), respectively for the AMEED and insulin group (P = 0.01). The daily reduction of PED area in the first 2 weeks of treatment was −0.25 ± 0.38 mm2 (95% CI, −0.60 to 0.10) for the AMEED group and −0.86 ± 0.81 mm2 (95% CI, −1.36 to −0.37) for the insulin group (P = 0.04). The epithelialization speed was −0.27 ± 0.28 mm2/day (95% CI, −0.49 to −0.05) for the AMEED group and −0.47 ± 0.34 mm2/day (95% CI, −0.64 to −0.26) for the insulin group (P = 0.12). The rate of daily reduction was −4.22% ± 4.21% (95% CI, −7.46% to −0.99%) for the AMEED group and −3.89% ± 1.64% (95% CI, −4.71% to −3.07%) for the insulin group (P = 0.86). The longitudinal changes of the PED area during the study period in the two groups are shown in Figure 2.
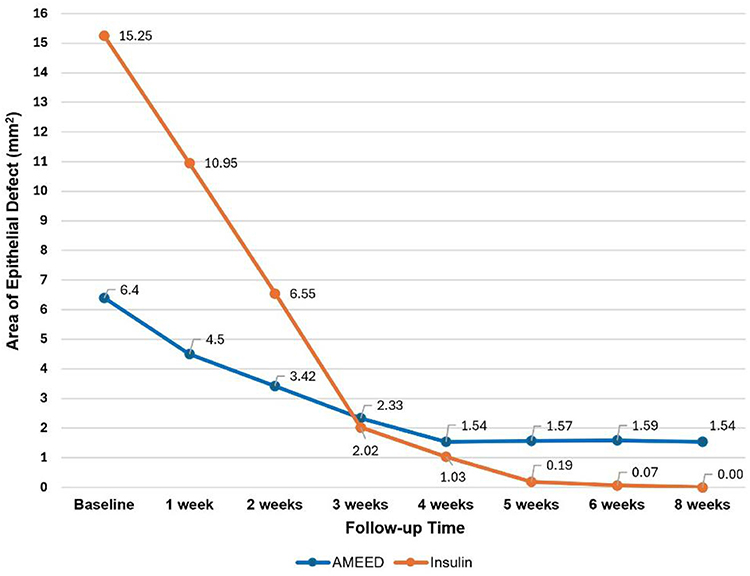 |
Figure 2 Longitudinal trend of the mean persistent epithelial defect (PED) area during treatment in the AMEED and insulin groups, allowing visualization of the comparative healing trajectory between treatments. |
Slit lamp pictures of two representative patients treated with insulin eye drops and AMEED taken at different time points are shown in Figures 3 and 4, respectively.
 |
Figure 3 (A–D) Serial slit-lamp images of a 29-year-old patient with a persistent epithelial defect (PED) owing to neurotrophic keratopathy treated with insulin eye drops. The patient presented a history of failed penetrating keratoplasty, glaucoma and cataract surgery. (A) Baseline presentation showing a PED area of 13.83 mm2. (B and C) Follow-up images at weeks 1 and 2, demonstrating progressive healing. (D) Complete re-epithelialization observed at week 4 of insulin treatment. |
 |
Figure 4 (A–D) Serial slit-lamp images of a 69-year-old patient with a long-standing persistent epithelial defect (PED) treated with amniotic membrane extract eye drops (AMEED). The patient presented severe neurotrophic keratopathy secondary to neurosurgical trigeminal nerve damage. (A) Baseline presentation showing a PED area of 13.40 mm2. (B and C) Follow-up images at weeks 1 and 2 during treatment with AMEED. (D) The non-healing PED ultimately required amniotic membrane transplantation at week 4. |
At the last follow-up visit, BCVA significantly improved in the insulin group compared to baseline (1.27 ± 0.94 Log MAR [95% CI, 0.81–1.74] vs 1.56 ± 0.80 [95% CI, 1.16–1.96], P = 0.006); but not in the AMEED group (1.00 ± 0.78 Log MAR [95% CI, 0.40–1.60] vs 1.18 ± 0.76 [95% CI, 0.60–1.76], P = 0.25). Overall, there was no significant difference in visual gain between AMEED and insulin group (respectively, −0.18 ± 0.31 Log MAR [95% CI, −0.41–0.06] vs −0.28 ± 0.40 [95% CI, −0.49 to −0.08], P = 0.49).
Concerning adverse reactions, both products were well tolerated, with no patients reporting any discomfort associated with their administration. Three cases of corneal neovascularization (33.3%) and one case of stromal scarring (11.1%) were reported in the AMEED group, whereas 5 cases of corneal neovascularization (27.8%) and 3 cases of stromal scarring (16.7%) were reported in the insulin group. One patient in the AMEED group required AM transplantation for long-standing non-healing PED owing to NK (Figure 4). To date, no patient presented to our attention with a disease recurrence after having reached complete healing thanks to study treatment.
Discussion
Insulin eye drops and AMEED have been described in recent literature as promising topical treatments when standard supportive measures fail to resolve PEDs.7,11–22 In the present study, we compared the outcomes of insulin eye drops versus AMEED in patients with refractory PEDs. Our results show that both products were effective in promoting corneal re-epithelialization, with the totality of patients treated with topical insulin achieving complete epithelial healing compared to less than half of patients treated with AMEED. The epithelialization process was better in the insulin group in terms of daily reduction of PED area, but this difference reached statistical significance only in the first 2 weeks of treatment. However, it should be mentioned that eyes receiving AMEED had a longer time interval between PED diagnosis and treatment initiation compared to those receiving insulin. This could likely reduce the outcomes of the therapy, as reported in previous literature.21 Notably, one patient in the AMEED group had a long history of a non-healing PED (319 days) in the context of severe NK following neurosurgical trigeminal nerve damage. Despite partial reduction in the PED size after AMEED treatment, the patient ultimately required AM transplantation. Interestingly, to date no recurrence of epithelial defects was observed after healing in any eye from either group, indicating that both products offer prolonged support for the proliferation and differentiation of epithelial cells.
Three patients with severe recalcitrant PEDs in the context of NK received DDCL insertion concomitant with the initiation of insulin eye drops. This lens is designed to act as a drug depot to increase bioavailability of eye drops on the corneal surface. Its use has been reported in various ocular surface diseases, including recalcitrant NK treated with insulin eye drops.19,20,23–25 The synergistic effect of the use of insulin eye drops combined with the wearing of therapeutic CL guaranteed the healing of the PEDs in all patients, despite the large area of the epithelial defect and the refractory course of the disease.
In terms of visual acuity, patients belonging to the insulin group, but not to the AMEED one, achieved a significant improvement at the last follow-up visit. Although the AMEED group showed numerically better BCVA values both at baseline and at the end of therapy compared to the insulin group, these differences were not statistically significant. None of the eyes experienced a loss of visual acuity during follow-up and both products were well tolerated by all patients throughout the entire duration of the study. Few patients of both groups developed corneal neovascularization or stromal scarring, which should be considered sequelae of long-standing PEDs rather than adverse reactions to treatment.1
Aspects to be considered when comparing insulin eye drops and AMEED are accessibility and costs that can represent significant barriers to the use of AMEED. This product requires refrigeration, has a shelf life of seven days, and involves an expensive manufacturing process. In contrast, insulin offers rapid dispensation to patients, widespread availability and favorable cost-effectiveness profile.
Although this is the first comparative study assessing the outcomes of insulin eye drops and AMEED in refractory PEDs, several limitations should be acknowledged. The retrospective design inherently introduces selection bias and limits causal inference. The heterogeneity of the study population—including sample size, baseline characteristics, PED etiology, and the interval between PED diagnosis and initiation of treatment—may have influenced the findings. The concomitant use of different adjuvant therapies, particularly DDCLs in some insulin-treated eyes, represents an additional confounder. The retrospective design and limited sample size precluded a formal power calculation and may introduce selection bias. However, all cases included complete clinical data and were managed at a single tertiary center, minimizing variability in treatment and follow-up protocols. Furthermore, longer-term data on recurrence rates and visual outcomes would be valuable; their absence represents an additional limitation that should be addressed in future studies.
Conclusion
In conclusion, the present study reports promising results in terms of safety, tolerability, and efficacy for insulin eye drops and AMEED in treating refractory PEDs. In our series, patients treated with topical insulin achieved complete epithelial healing in all treated eyes, while PED healed in less than half of the patients in the AMEED group. No recurrences of epithelial defects after healing were recorded in either group. Given its accessibility, low cost, and favorable safety profile, topical insulin may represent a practical therapeutic option for managing persistent epithelial defects. However, the retrospective design and limited follow-up represent important limitations. Larger, prospective studies with longer follow-up are warranted to strengthen these conclusions and confirm their broader applicability.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Vaidyanathan U, Hopping GC, Liu HY, et al. Persistent corneal epithelial defects: a review article. Med Hypothesis Discov Innov Ophthalmol. 2019;8(3).
2. Doane MG. Interaction of eyelids and tears in corneal wetting and the dynamics of the normal human eyeblink. Am J Ophthalmol. 1980;89(4):507–516. doi:10.1016/0002-9394(80)90058-6
3. Barabino S, Chen Y, Chauhan S, Dana R. Ocular surface immunity: homeostatic mechanisms and their disruption in dry eye disease. Prog Retin Eye Res. 2012;31(3):271–285. doi:10.1016/j.preteyeres.2012.02.003
4. Yagci A, Gurdal C. The role and treatment of inflammation in dry eye disease. Int Ophthalmol. 2014;34(6):1291–1301. doi:10.1007/s10792-014-9969-x
5. Ljubimov AV, Saghizadeh M. Progress in corneal wound healing. Prog Retin Eye Res. 2015;49. doi:10.1016/j.preteyeres.2015.07.002
6. Ziaei M, Greene C, Green CR. Wound healing in the eye: therapeutic prospects. Adv Drug Deliv Rev. 2018;126. doi:10.1016/j.addr.2018.01.006
7. Shanley LJ, McCaig CD, Forrester JV, Zhao M. Insulin, not leptin, promotes in vitro cell migration to heal monolayer wounds in human corneal epithelium. Invest Ophthalmol Vis Sci. 2004;45(4):1088. doi:10.1167/iovs.03-1064
8. Titone R, Zhu M, Robertson DM. Insulin mediates de novo nuclear accumulation of the IGF-1/insulin hybrid receptor in corneal epithelial cells. Sci Rep. 2018;8(1). doi:10.1038/s41598-018-21031-7
9. Murri MS, Moshirfar M, Birdsong OC, Ronquillo YC, Ding Y, Hoopes PC. Amniotic membrane extract and eye drops: a review of literature and clinical application. Clin Ophthalmol. 2018;12. doi:10.2147/OPTH.S165553
10. Baradaran-Rafii A, Asl NS, Ebrahimi M, et al. The role of amniotic membrane extract eye drop (AMEED) in in vivo cultivation of limbal stem cells. Ocul Surf. 2018;16(1):146–153. doi:10.1016/j.jtos.2017.11.001
11. Diaz-Valle D, Burgos-Blasco B, Rego-Lorca D, et al. Comparison of the efficacy of topical insulin with autologous serum eye drops in persistent epithelial defects of the cornea. Acta Ophthalmol. 2022;100(4). doi:10.1111/aos.14997
12. Abdi P, Ghaffari R, Azad N, et al. Topical insulin for refractory persistent corneal epithelial defects. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-63091-y
13. Almeida J, Costa TR, Vivas M, et al. Long-term results of topical insulin treatment for persistent corneal epithelial defects. J Ophthalmic Vis Res. 2024;19(4):397–404. doi:10.18502/jovr.v19i4.13977
14. Balal S, Din N, Ashton C, Ahmad S. Healing of chemical injury-related persistent corneal epithelial defects with topical insulin. Cornea. 2023;42(8). doi:10.1097/ICO.0000000000003145
15. Bonci P, Bonci P, Lia A. Suspension made with amniotic membrane: clinical trial. Eur J Ophthalmol. 2005;15(4):441–445. doi:10.1177/112067210501500403
16. Chen M, Chang CK, Lin SY, Chen M. A pilot study of the short term effectiveness and safety of amniotic fluid in severe dry eye disease. Med Hypothesis Discov Innov Ophthalmol. 2019;8(2).
17. Diaz-Valle D, Burgos-Blasco B, Gegundez-Fernandez JA, et al. Topical insulin for refractory persistent corneal epithelial defects. Eur J Ophthalmol. 2021;31(5):2280–2286. doi:10.1177/1120672120958307
18. Fai S, Ahem A, Mustapha M, Mohd Noh UK, Catherine Bastion ML. Randomized controlled trial of topical insulin for healing corneal epithelial defects induced during vitreoretinal surgery in diabetics. Asia-Pac J Ophthalmol. 2017;6(5):418–424. doi:10.22608/APO.201780
19. Giannaccare G, Coco G, Rossi C, et al. Combined use of therapeutic hyper-cl soft contact lens and insulin eye drops for the treatment of recalcitrant neurotrophic keratopathy. Cornea. 2024;43(1):120–124. doi:10.1097/ICO.0000000000003361
20. Mancini A, Mancini M, Taloni A, et al. Topical insulin used alone or in combination with drug-depository contact lens for refractory cases of neurotrophic keratopathy. Am J Ophthalmol Case Rep. 2024;36. doi:10.1016/j.ajoc.2024.102227
21. Liang L, Li W, Ling S, et al. Amniotic membrane extraction solution for ocular chemical burns. Clin Exp Ophthalmol. 2009;37(9):855–863. doi:10.1111/j.1442-9071.2009.02159.x
22. Qasem A, Karroum R, Khadoor M, Darwish T. Case report topical insulin treatment for neurotrophic corneal ulcer with persistent epithelial defect. J Opht Res Rev Rep. 2024;5(2):1–4. doi:10.47363/JORRR/2024(5)156
23. Daniel Raj Ponniah LR, Ranilakshmi V, Anandan H, Caroline J, Arulanandham A. Novel drug-repository contact lens for prolonging the antimicrobial-cornea interaction for bacterial keratitis treatment: randomised controlled trial results. BMJ Open Ophthalmol. 2022;7(1):e001093. doi:10.1136/bmjophth-2022-001093
24. Daphna O, Mimouni M, Keshet Y, et al. Therapeutic HL-contact lens versus standard bandage contact lens for corneal edema: a prospective, multicenter, randomized, crossover study. J Ophthalmol. 2020;2020:1–5. doi:10.1155/2020/8410920
25. Romano V, Romano D, Semeraro P, et al. Therapeutic hyper-CL soft contact lens in Sjögren’s syndrome. Am J Ophthalmol Case Rep. 2022:28. doi:10.1016/j.ajoc.2022.101685
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Level of Satisfaction Among Patients Using Insulin Administered by Pen vs Vial/Syringe. An Observational Prospective Study
Valladales-Restrepo LF, Delgado-Araujo AC, Oyuela-Gutiérrez MC, Ospina-Arzuaga HD, Machado-Alba JE
Patient Preference and Adherence 2025, 19:65-74
Published Date: 8 January 2025