Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of Ahmed Glaucoma Valve Implantation Alone Versus Combined with Phacoemulsification in Chinese Primary Open-Angle Glaucoma
Authors Fu L, Liu X, Ping Y, Zhuang X, Yao S, Yu S, Wang H, Yao S, Pan W
Received 26 June 2025
Accepted for publication 30 September 2025
Published 4 November 2025 Volume 2025:19 Pages 4067—4076
DOI https://doi.org/10.2147/OPTH.S549432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lin Fu,1 Xinyi Liu,1,2 Yijing Ping,1 Xiaoyu Zhuang,1 Shumeng Yao,1 Shuhan Yu,1 Hexiang Wang,1 Shenglu Yao,1 Weihua Pan1,3
1National Clinical Research Center for Ocular Diseases, Eye Hospital, Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Department of Ophthalmology, People’s Hospital of Yichun, Yichun, Jiangxi, People’s Republic of China; 3Department of Glaucoma, Hangzhou Aier Eye Hopital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Weihua Pan, Email [email protected]
Introduction: To compare the surgical outcomes of Ahmed glaucoma valve (AGV) implantation and combined AGVwith phacoemulsification (Phaco-AGV) in Chinese patients with primary open-angle glaucoma (POAG).
Methods: A total of 43 eyes followed up for 2 years were enrolled. The primary outcome was the success rate. The success rate was defined as an IOP of 5– 21 mmHg (success rate 1) or 5– 18 mmHg (success rate 2), and an IOP reduction of more than 20% with (qualified) or without (complete) glaucoma medications. The secondary outcomes included IOP, glaucoma medications, and complications.
Results: Eighteen eyes underwent AGV and 25 eyes underwent phaco-AGV. There were no differences in the preoperative IOP (25.7 ± 10.7 mmHg vs 26.3 ± 6.2 mmHg, P< 0.05) and medications (2.1 ± 1.4 vs 1.6 ± 0.8, P< 0.05) between the two groups. The complete success rate 1 in the Phaco-AGV group was higher than that in the AGV group at the 2-year (60.0% vs 22.2%, P< 0.05) follow-up. The qualified and complete success rates 2 in the Phaco-AGV group were both higher than those in the AGV group at the 2-year follow-up (all P < 0.05). Patients in the Phaco-AGV group showed significantly lower postoperative IOP at 3 months (P< 0.05), used fewer glaucoma medications at month-3, month-6 and year-2 visits, experienced less encapsulated blebs than those in the AGV group (P< 0.05).
Conclusion: The surgical outcomes of phaco-AGV showed higher success rates and fewer complications than those of AGV in this 2-year study.
Keywords: Ahmed glaucoma valve, phacoemulsification, tube, glaucoma device drainage, Chinese Primary Open Angle Glaucoma
Introduction
Glaucoma often coexists with cataracts. One key underlying factor is oxidative stress in ocular tissues, where the accumulation of reactive oxygen species (ROS) induces oxidative damage to both the lens and the trabecular meshwork. This ultimately leads to reduced lens transparency and abnormally elevated intraocular pressure.1 Long-term treatment with anti-glaucoma drugs promotes rapid formation of nuclear cataracts.2
Surgery is currently the mainstream treatment for glaucoma complicated by cataracts, among which trabeculectomy is the most common. Although trabeculectomy is constantly improving, there is still a high rate of postoperative complications such as choroidal penetration, detachment, and decompensation of corneal endothelial function. Recent reports have shown that phacoemulsification combined with Ahmed glaucoma valve implantation (Phaco-AGV) achieves good visual improvement, promising intraocular pressure control, and few complications in refractory glaucoma patient,3–6 and the current application trend is increasing year by year.7
The Ahmed Glaucoma Valve (AGV) is a glaucoma drainage device (GDD) that has been used for decades to treat refractory glaucoma.8 It was launched in 1993 as the first GDD with a unidirectional valve mechanism that contributed to the prevention of postoperative hypotony and IOP stabilization.9 Cataract extraction can reduce IOP in glaucoma patients with open-angle glaucoma (OAG).10,11 In OAG, cataract extraction results in an average IOP decrease of 13–20% and a 12–56.5% reduction in glaucoma medication.12–14 The mechanism of the IOP-lowering effect of phacoemulsification was proposed to be the remodeling of the trabecular meshwork extracellular matrix15 and Schlemm’s canal expansion after lens extraction.16 However, information on combined phaco-AGV outcomes in Chinese patients remains scarce.
Although it has been increasingly accepted to perform combined cataract and glaucoma surgery as a single operation, many surgeons still prefer to perform phacoemulsification and glaucoma surgery separately, as surveyed by the American Glaucoma Society (AGS).17 The main concern is that cataract surgery may affect the effects of existing glaucoma surgery, such as phacoemulsification, which has already undergone trabeculectomy and can lead to increased postoperative IOP, more flat filtration follicles, or severe anterior chamber inflammation.18–20 Accordingly, the aim of this study was to compare and evaluate the effectiveness and safety profile of Ahmed glaucoma valve (AGV) implantation alone and phaco-AGV surgery and to identify potential limitations of each approach in the Chinese POAG population. Different subtypes of glaucoma can affect the surgical outcomes. For instance, neovascular and uveitic glaucoma may be dominated by severe inflammatory responses,21 and the biometric changes after surgery differ between open-angle glaucoma and angle-closure glaucoma.10 These factors influence IOP and visual acuity. Therefore, we included only patients with primary open-angle glaucoma (POAG) in this study and compared the surgical outcomes of AGV alone and phaco-AGV.
Methods
Study Design and Patient Selection
A retrospective study was conducted by reviewing the medical charts of patients who underwent AGV or phaco-AGV between April 1, 2013, and August 31, 2018, at the Eye Hospital of Wenzhou Medical University. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Wenzhou Medical University (IRB approval number: H2023-035-K-33), and registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2300074639). Written informed consent was obtained from all patients. The inclusion criteria were as follows: (1) at least 18 years of age, (2) failed POAG treatment to achieve the target IOP or control glaucoma progression despite maximum tolerated medical therapy and several antiglaucoma surgeries, (3) intolerance to topical medications or high risk of trabeculectomy failure, and (4) follow-up visits for 2 years postoperatively. The exclusion criteria included (1) patients with previously implanted artificial intraocular lenses (IOLs), (2) patients without lenses, (3) patients complicated with other ocular disorders, including corneal opacity, lens dislocation, ischemic optic neuropathy, and diabetic retinopathy, and (4) patients who underwent additional surgeries (eg, phacoemulsification) at the 2-year follow-up. Patients with glaucoma and cataracts were selected to undergo phaco-AGV when sufficient lens opacity to induce vision reduction was determined by the operating surgeon. All surgeries included in this study were performed by the same experienced surgeon (WH Pan) using a standardized technique.
Procedure
The AGV (Ahmed Glaucoma Valve, model FP7; New World Medical, Inc., California, USA) was primed with a balanced salt solution before implantation. After peribulbar anesthesia and corneal traction suturing, a fornix-based conjunctival flap was created and the Tenon capsule was raised in the superior temporal quadrant in all cases. An AGV plate was inserted into the pocket after posterior dissection between the conjunctiva and the sclera. The AGV plate was fixed 10 mm from the limbus using a 5–0 Prolene suture. If this procedure was combined with phacoemulsification, standard clear corneal phacoemulsification was performed and an artificial intraocular lens was implanted. To maintain the anterior chamber during AGV, viscoelastics were injected through a lateral corneal incision. The tube was then trimmed to 2–2.5 mm in length and inserted along a 23-gauge needle track via an intrascleral tunnel starting 3–4 mm posterior to the corneoscleral limbus, with the bevel oriented anteriorly. The conjunctival incision and Tenon’s capsule were sutured back to the limbus. Subconjunctival dexamethasone and antibiotic eye drops were administered, and the eye was covered with cotton gauze. To reduce inflammation, topical postoperative application of bromfenac sodium was administered four times daily for 1 week, and the combined agent of tobramycin and 0.1% dexamethasone was applied six times daily and then tapered over a period of 8 to 12 weeks depending on the response to therapy.
Patient Examinations
Baseline assessments including IOP measurements, visual acuity (VA), axial length, visual field index (VFI), mean deviation (MD), pattern standard deviation (PSD) of the Humphrey visual field, lens status, and number of topical glaucoma medications were recorded preoperatively. IOP values were compared at follow-up visits at 3 months, 6 months, 1 year and 2 years postoperatively. Anterior segment optical coherence tomography (AS-OCT, Visante OCT, model 1000; Carl Zeiss Meditec) was performed on day 1 and continuously during the follow-up period to detect ciliochoroidal detachment (CCD). The CCD investigation was performed according to our previously published protocol.22 Other postoperative complications and use of topical glaucoma medications were also recorded at each clinic visit.
Definition of Complete Success, Qualified Success and Hypertensive Phase
Complete success 1 and qualified success 1 were defined according to the following criteria: (1) a postoperative IOP value between 5 and 21 mmHg (5<IOP≤21 mmHg); (2) a decrease in IOP of more than 20%; (3) no (complete) or (qualified) glaucoma medication 2, and (4) no de novo glaucoma surgery and no loss of light perception vision. Complete success 2 and qualified success 2 were defined according to the following criteria: (1) a postoperative IOP value between 5 and 18 mmHg (5<IOP≤18 mmHg); (2) a decrease in IOP of more than 20%; (3) no (complete) or with (qualified) glaucoma medication; and (4) no de novo glaucoma surgery and no loss of light of perception.
The hypertensive phase was defined as an increase in IOP to > 21 mmHg from the first week to the third month after surgery, followed by a decrease to ≤ 21 mmHg within 3 months.23–25
Statistical Analysis
All data were analyzed using the IBM SPSS Statistics version 23.0 (IBM Corp., Chicago, IL, USA).The multivariate logistic regression model and chi-square tests 加上 fisherwere used to compare categorical variables, and the results are presented as frequencies and percentages. The normality of the distribution of the numeric variables was analyzed using the Kolmogorov–Smirnov test. The independent Student’s t-test was used to compare parametric parameters, and the Mann–Whitney U-test was used to compare nonparametric parameters. Kaplan-Meier survival curve analysis and Log rank tests were used to evaluate the success rate. The confidence interval level was set to 95% (95% CI) with a corresponding P value threshold of 0.05. The results for the numerical variables are presented as mean ± standard deviation (SD). Statistical significance was set at P < 0.05.
Results
A total of 43 eyes of 35 Chinese patients with POAG who completed the 2-year follow-up were included in this study. Among these eyes, AGV was performed in 18 eyes and phaco-AGV was conducted in the other 25 eyes. The baseline characteristics of the two groups are presented in Table 1. The mean age of the patients in the Phaco-AGV group was 68.6±7.8 years and was significantly older than the 55.2±10.3 years in the AGV group (P ˂ 0.0001; Table 1), so the analysis of covariance was used to adjust for age for the comparisons between the two groups. Regarding the status of the lenses before surgery, all were cataracts in the Phaco-AGV group, and 5 (27.8%) were clear lenses in the AGV group (P = 0.009; Table 1). These two groups did not differ with respect to sex distribution or systemic diseases, such as diabetes, hypertension, AL, baseline medication, IOP, or corrected distance visual acuity (CDVA; P > 0.05; Table 1).
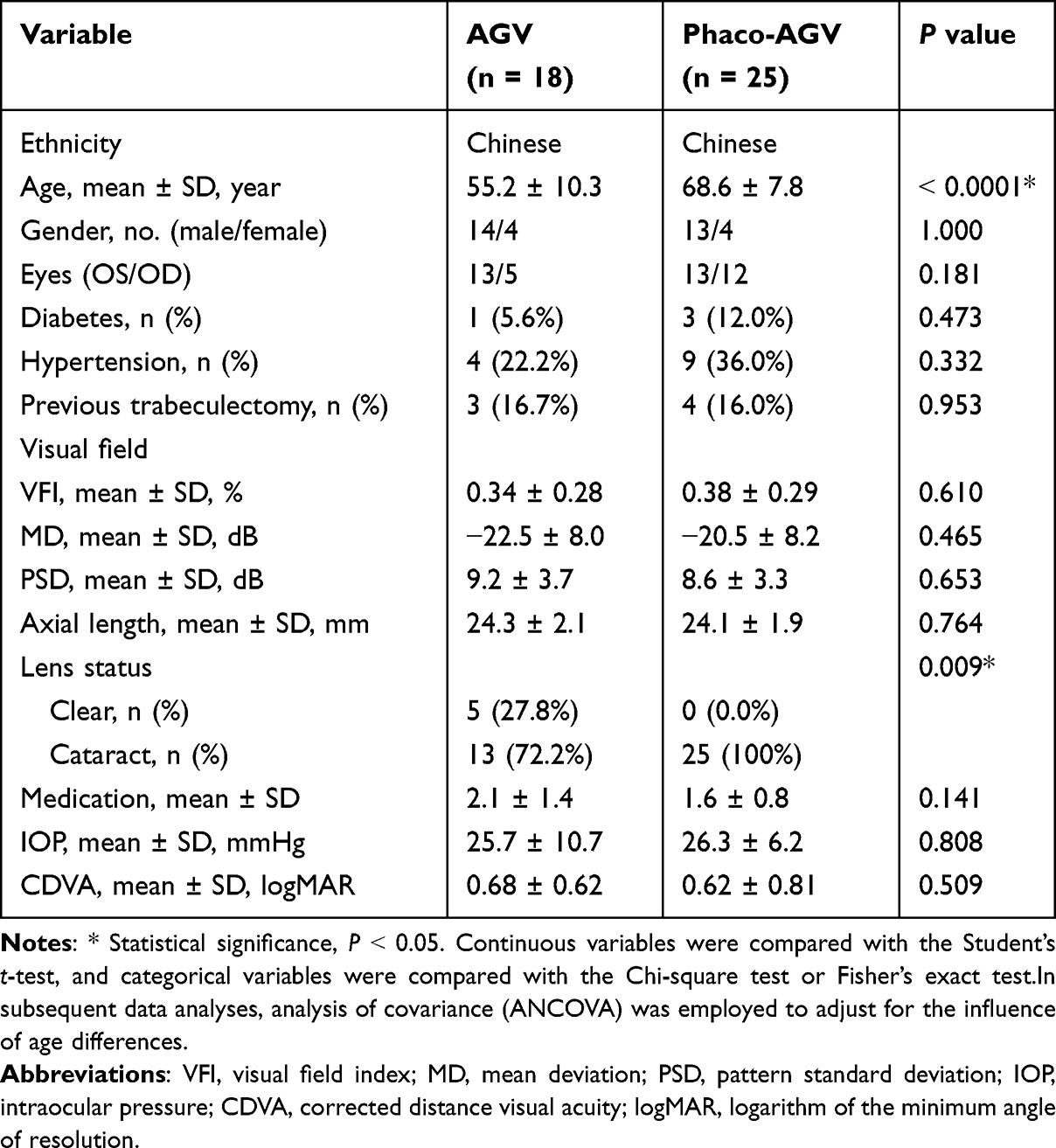 |
Table 1 Baseline Characteristics of the AGV and Phaco-AGV Groups |
Figure 1 illustrates the Kaplan-Meier survival analysis of the qualified success rates for the two surgical groups. At the 1-year follow-up, the qualified success rate 1 was 100.0% in the phaco-AGV group and was higher than 72.2% in the AGV group, but the difference was not statistically significant. At the 2-year follow-up, the qualified success rate 1 was 96.6% in the Phaco-AGV group and was slightly higher than that in the AGV group (72.2%) (P = 0.076); however, the complete success rate 1 was 60.0% in the Phaco-AGV group and was statistically higher than that in the AGV group (22.2%) (P = 0.028). In the AGV group, the mean IOP was 17.3±4.8 mmHg at the 1-year follow-up and 16.4 (7.5) mmHg at the 2-year follow-up. In the Phaco-AGV group, the mean IOP were16.4 (7.5) mmHg and 15.4 (4.5) mmHg at the 1-year and 2-year follow-ups, respectively. In addition, this study used different postoperative IOPs as criteria for surgical success (Table 2). When IOP < 18 mmHg was considered successful, compared to the AGV group, the qualified and complete success rates 2 in the Phaco-AGV group were not significantly higher at year-1 (all P > 0.05). However, there were statistically significant differences at year-2 (all P < 0.05).
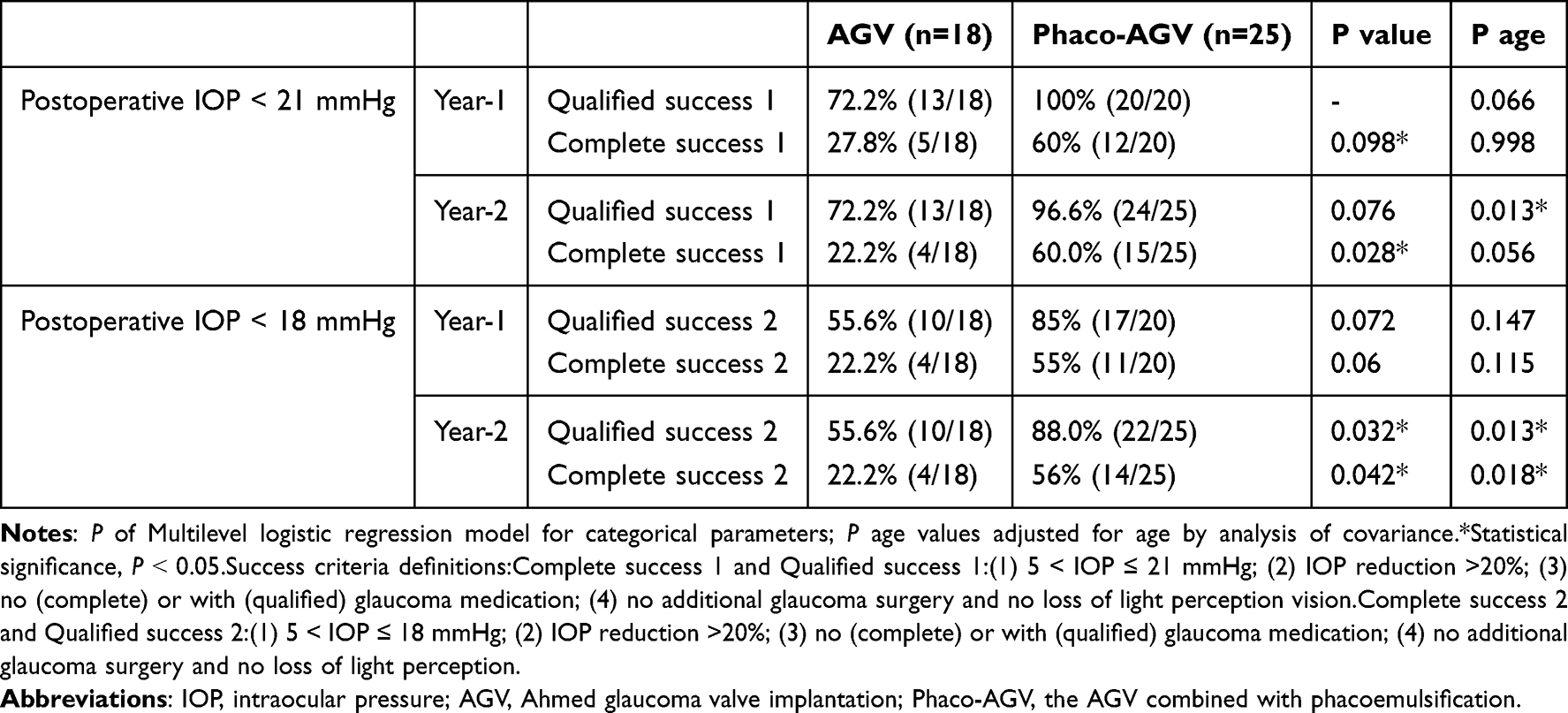 |
Table 2 The Comparisons of Success Rate Between Group AGV and Group Phaco-AGV |
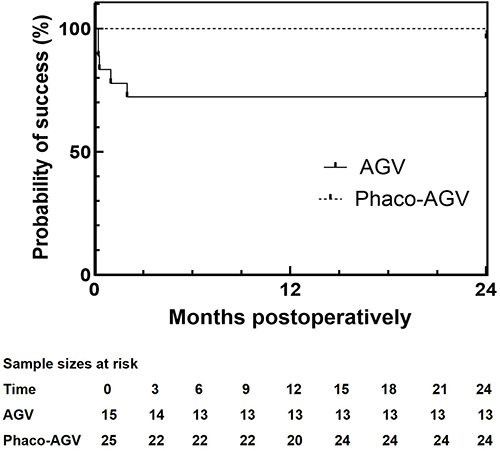 |
Figure 1 The Kaplan-Meier cumulative probability curve of success for theAGV vs Phaco-AGV over time. |
Postoperative IOP assessments illustrated that at the month-3 follow-up, the mean IOP of 13.2±3.2 mmHg in the Phaco-AGV group was significantly lower than that of 18.0±5.9 mmHg in the AGV group (P = 0.002, Figure 2). No differences in IOP at the clinic visits of 6 months, 1 year or 2 years were observed between the two groups (P = 0.075, 0.077, 0.342, respectively, Figure 2).
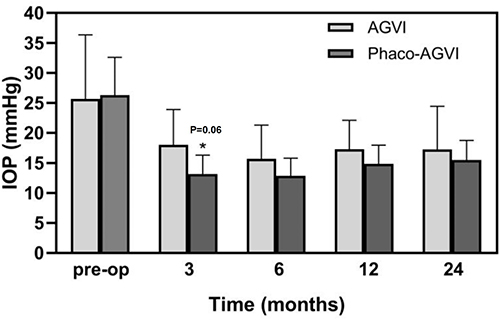 |
Figure 2 Preoperative and postoperative IOP profiles in the AGV and Phaco-AGV groups at each visit. Note: *P value <0.05. Error bars represent thestandard deviation. |
Moreover, except at the 1-year clinic visit, patients in the phaco-AGV group used significantly fewer glaucoma medications than those who received AGV at the month-3, month-6 and year-2 postoperative visits. The mean numbers of glaucoma medications in the Phaco-AGV group were 0.1±0.4, 0.2±0.4 and 0.5±0.6 at 3 months, 6 months and 2 years, respectively, which were significantly less than the numbers of glaucoma medications in the AGV group (0.8±0.9, 1.1±0.9 and 1.4±1.2, P = 0.004, 0.001 and 0.011, respectively, Figure 3 and Table S1). The postoperative CDVA at the final follow-up showed that the mean CDVA in the Phaco-AGV group was 0.51± 0.83, and that in the AGV alone group was 0.75 ± 0.98. Only a trend of better CDVA was observed in the Phaco-AGV group than in the AGV group, but the difference was not statistically significant at the final follow-up (P = 0.227).
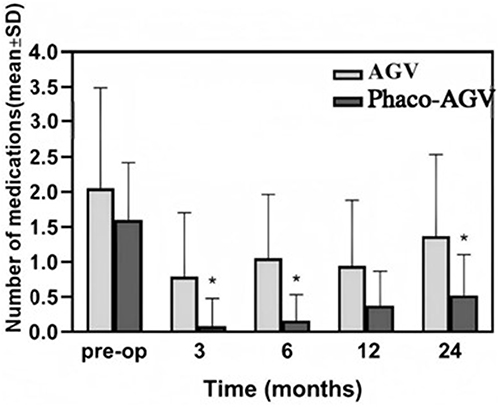 |
Figure 3 Preoperative and postoperative medication profiles during follow-up. Note: * P value <0.05. Error bars represent the standard deviation. |
The postoperative complications are listed in Table 3. Eyes that underwent combined Phaco-AGV showed fewer encapsulated blebs than eyes that underwent AGV (P = 0.009). No differences were observed in the occurrence of early transient hypertension, tube obstruction or malposition, hypotony, or CCD between the two groups. Six (33.3%) eyes demonstrated a transient IOP elevation of >30 mmHg in the AGV alone group, and respectively seven eyes (28.0%) were found a transient IOP elevation from 21.5 mmHg to 51.8 mmHg in the Phaco-AGV group at early postoperative visits (within 1 week after the surgery). Tube obstruction/malposition was found in one eye (5.6%) at 1 d after the surgery in the AGV alone group; the patient underwent anterior chamber irrigation immediately and was found in one eye (4.0%) at 1 week after the surgery in the Phaco-AGV group, and the patient resolved after drainage recanalization. Eight patients (44.4%) in the AGV alone group and two (8.0%) in the Phaco-AGV group developed encapsulated blebs within 6 months after surgery in the AGV alone group; these patients required additional surgery, such as wrapped wall of drainage valve resection and viscoelastic separation. CCD was observed in four (22.2%) eyes in the AGV alone group, which occurred 1 d after surgery and resolved from 3 days to 22 days postoperatively, while 12 (48%) eyes in the Phaco-AGV group had CCD that usually occurred 1 week after surgery and resolved from 5 days to 95 days postoperatively.
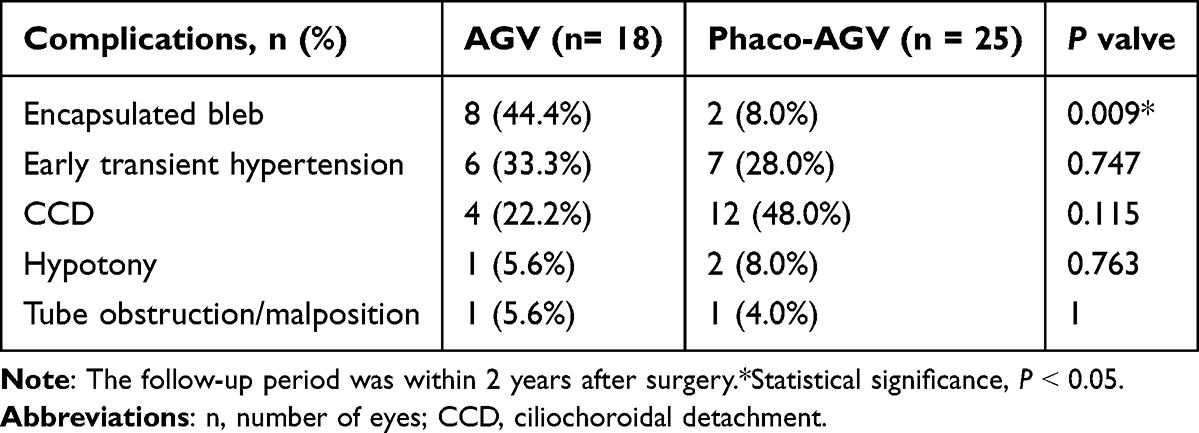 |
Table 3 Postoperative Complications in the Two Groups |
Discussion
In the present study, we found that the surgical success rate was significantly higher in the phaco-AGV group than in the Chinese POAG group after AGV surgery. Regarding complications, eyes that underwent phaco-AGV experienced less postoperative bleb encapsulation, which may contribute to the higher success rate of the combined surgery. Therefore, phaco-AGV appears to be a safe and effective surgical method for treating POAG in China.
The success rates of the combined Phaco-AGV in the present study were promising. Most previous studies used an IOP upper limit of 21 mmHg as the success criterion and included several glaucoma subtypes. However, in our study, IOP upper limits of 21 and 18 mmHg were used as the success criteria. Using a stricter standard of 5–18 mmHg, patients with decreased IOP can be identified for closer monitoring and early intervention. Chung et al reported that the qualified success rate of combined phaco-AGV was 87.5% with a mean follow-up time of 13±5 months.26 Nassiri et al showed that the qualified success rate of combined phaco-AGV was 87.5% 12 months after surgery.3 The qualified success rate in the present study was 96.6% in the phaco-AGV group at the years follow-up. For AGV, the results of this study showed that the qualified success rate of AGV was 72.2% both at one year and two years of follow-up, which did not show a superior effect compared to other studies. Pakravan et al reported qualified success rates of 81.8% and 95.2%for superior and inferior implantation at 1 year,27 which is higher than the success rate in our study. Since the patients included in the above studies were different, it is difficult and not reasonable to compare the success results between combined phaco-AGV and AGV alone directly. In our study, we retrospectively reviewed POAG patients in our hospital and found that phaco-AGV resulted in a higher success rate than AGV alone for POAG in China.
The reasons why phaco-AGV in this study showed higher success rates than AGV alone may be as follows. First, cataract extraction itself can reduce IOP, with a reported 13–26% reduction in IOP and a 12–56.5% reduction in glaucoma medication in OAG one year to 17 months postoperatively, as reviewed from 2009 to 2017.12–14 A recent study also found that Phacoemulsification resulted in a decrease in IOP in the control of POAG, indicating that the change in IOP between the POAG group and non-glaucomatous group was statistically insignificant (p =0.234).28 The possible mechanisms of the IOP-lowering effect of cataract extraction include hyposecretion of the aqueous humor induced by widening of the anterior segment,29 expansion of Schlemm’s canal,30 and resistance reduction in the trabecular meshwork resulting from irrigation during surgery.31 Second, patients in the phaco-AGV group experienced less bleb encapsulation than those in the AGV alone group did. Following AGV implantation, the initial inflammatory response triggered by foreign body rejection and tissue repair leads to the activation of fibroblasts. These cells differentiate into myofibroblasts, which drive excessive extracellular matrix production and tissue contraction. This results in the formation of a dense, collagen-rich encapsulated bleb as part of aberrant subconjunctival wound healing. Scarring is a major cause of failure following filtration surgery; therefore, an encapsulated bleb could result in IOP elevation and surgical failure.32,33 In this study, the lower incidence of bleb encapsulation in the phaco-AGV group, compared to the AGV-alone group, may have contributed to the differences observed in surgical outcomes between the two groups.
Previously, a major concern regarding phacoemulsification combined with GDD implantation was that the procedure triggered more inflammation and complications. Nevertheless, in this study, the postoperative complications of bleb encapsulation were less frequently observed in phaco-AGV than in AGV alone. The effect of phacoemulsification on AGV function is not yet well understood. In theory, cataract extraction may induce the release of inflammatory mediators and cells.34,35 These inflammatory responses may thicken the fibrous capsule around the plate, resulting in hypertensive phase or bleb scarring. However, in practice, patients in the phaco-AGV group experienced less bleb encapsulation than patients who received AGV alone in the current study. However, the underlying mechanism remains unclear.
Histological examination of the excised encapsulated bleb after AGV revealed an absence of inflammatory factors.36 Therefore, inflammation might not be involved in bleb encapsulation. Conversely, the incidence of this complication was lower in the combined phaco-AGV group than in the AGV alone group. The encapsulated bleb consists of an inner smooth surface with dense collagen fibers and an outer vascularized area.37 Hence, it can be postulated that the reduced bleb encapsulation in the Phaco-AGV group may contribute to the increased outflow through the plate, which may prevent elastoid degeneration and transformation of fibroblasts into myofibroblasts.36
Postoperative CDVA in the phaco-AGV group was not significantly different from that in the AGV alone group. This may be because the recruited patients in this study were mostly in the end-stage with a severely damaged visual field, according to the modified Bascom Palmer Glaucoma Staging System.38 The mean MD was −20.5±8.2 dB in the Phaco-AGV group and −22.5±8.0 dB in the AGV group. As previously reported, visual acuity improvement after surgery is associated with the preoperative glaucoma stage in patients.39 In this study, within the AGV group, no patient presented with mild visual field defect (MD < −6 dB) preoperatively, while 2 and 12 patients were classified as having moderate (−12 dB ≤ MD < −6 dB) and severe (MD ≥ −12 dB) defects, respectively. In the phaco-AGV group, mild, moderate, and severe preoperative visual field defects were observed in 1, 3, and 19 patients, respectively.The worse the stage, the less the VA improvement observed. Hence, the benefit of phacoemulsification for end-stage patients mainly consists of a higher success rate than an improvement in visual function.
This study had some limitations. This was a retrospective study and the patients were not randomized to two different surgical methods. Patients in the phaco-AGV group were older than those in the AGV alone group, while younger age may have an impact on bleb encapsulation and result in surgical failure.40 Moreover, the sample size of this study was small. Furthermore, cataract density was not quantitatively assessed or adjusted for, which may represent a potential confounding factor affecting the surgical outcomes. Additionally, the follow-up duration is crucial for evaluating the success of surgical interventions and associated complications in clinical research. Although this study provides two years of follow-up data, the assessment of long-term outcomes is still limited. Future studies with longer follow-ups would greatly contribute to a deeper understanding of the long-term surgical effects and potential late-onset complications, thereby optimizing clinical decision-making and patient management, and are of significant value in guiding research directions.Therefore, a prospective randomized controlled study with a larger sample size is necessary to achieve a more convincing result. In future clinical practice, doctors should comprehensively consider multiple factors, such as the patient’s age, severity of the disease, and presence of any concomitant ocular conditions when selecting the surgical treatment plan, aiming to optimize therapeutic outcomes and reduce the risk of complications, with a view to improving the overall surgical efficacy for the patient.
Conclusions
In this 2-year retrospective study of Chinese patients with primary open-angle glaucoma, combined phacoemulsification and Ahmed glaucoma valve implantation achieved higher postoperative success rates and fewer bleb encapsulation complications compared with AGVI alone. These findings suggest that phaco-AGVI may be a preferred surgical option for POAG patients with coexisting visually significant cataracts. Future large-scale prospective trials are warranted to validate these results and assess long-term outcomes.
Abbreviation
POAG, Primary Open-Angle Glaucoma; AGV, Ahmed Glaucoma Valve Implantation; Phaco-AGV, Phacoemulsification with Ahmed Glaucoma Valve Implantation; IOP, Intraocular Pressure; CDVA, Corrected Distance Visual Acuity; SD, Standard Deviation; CI, Confidence Interval; IRB, Institutional Review Board.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Statement of Ethics
The study protocol was reviewed and approved by [Institutional Review Board of Wenzhou Eye Hospital, Wenzhou Medical University] approval number [H2023-035-K-33].
Written informed consent was obtained from all patients.
Acknowledgment
We would like to express our appreciation for the data analysis consultation with statistician Hengli Lian of our hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Written informed consent was obtained from all participants involved in the study for the publication of their data. This consent included permission to publish any identifiable information and images related to their treatment and outcomes. The study protocol was approved by the Institutional Review Board of Wenzhou Eye Hospital, Wenzhou Medical University, ensuring that all ethical guidelines were followed in accordance with the Declaration of Helsinki.
Funding
The National Natural Science Foundation of China Youth Science Foundation Project (grant no. 82201176) and the Science and Technology Program of Wenzhou City (grant no. Y20210972), and Medical and Health of Zhejiang Province (grant no. 2023KY153) supported the study design.
Disclosure
The authors declare no conflicts of interest regarding the publication of this paper.
References
1. Rejas-González R, Montero-Calle A, Pastora Salvador N, et al. Unraveling the nexus of oxidative stress, ocular diseases, and small extracellular vesicles to identify novel glaucoma biomarkers through in-depth proteomics. Redox Biol. 2024;77:103368. doi:10.1016/j.redox.2024.103368
2. Cennamo M, Favuzza E, Salvatici MC, Giuranno G, Buzzi M, Mencucci R. Effect of manual, preloaded, and automated preloaded injectors on corneal incision architecture after IOL implantation. J Cataract Refract Surg. 2020;46(10):1374–1380. doi:10.1097/j.jcrs.0000000000000295
3. Nassiri N, Sadeghi Yarandi S, Mohammadi B, Rahmani L. Combined phacoemulsification and Ahmed valve glaucoma drainage implant: a retrospective case series. Eur J Ophthalmol. 2008;18(2):191–198. doi:10.1177/112067210801800205
4. Parihar J, Kaushik J, Jain VK, Trehan HS, Mishra A, Baranwal VK. Combined Ahmed valve and phacoemulsification with intraocular lens implantation under infliximab in refractory uveitic glaucoma. Eur J Ophthalmol. 2018;28(3):294–298. doi:10.5301/ejo.5001032
5. Xie Z, Liu H, Du M, et al. Efficacy of Ahmed glaucoma valve implantation on neovascular glaucoma. Int J Med Sci. 2019;16(10):1371–1376. doi:10.7150/ijms.35267
6. Rai AS, Shoham-Hazon N, Christakis PG, Rai AS, Ahmed I. Comparison of the Ahmed and Baerveldt glaucoma shunts with combined cataract extraction. Can J Ophthalmol. 2018;53(2):124–130. doi:10.1016/j.jcjo.2017.08.017
7. Hu cheng XJ, Liang Yuanbo YC, Wu Haixia FK, Xie Yanqian FA, Qu J. Changing patterns of surgical treatment for glaucoma in the eye hospital of wenzhou medical university during the past ten years. Chin. J. Ophthalmol. 2018;54(3):184–188. doi:10.3760/cma.j.issn.0412-4081.2018.03.007
8. Riva I, Roberti G, Katsanos A, Oddone F, Quaranta L. A review of the Ahmed glaucoma valve implant and comparison with other surgical operations. Adv Ther. 2017;34(4):834–847. doi:10.1007/s12325-017-0503-1
9. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1995;120(1):23–31. doi:10.1016/s0002-9394(14)73755-9
10. Young C, Seibold LK, Kahook MY. Cataract surgery and intraocular pressure in glaucoma. Curr Opin Ophthalmol. 2020;31(1):15–22. doi:10.1097/ICU.0000000000000623
11. Masis Solano M, Lin SC. Cataract, phacoemulsification and intraocular pressure: is the anterior segment anatomy the missing piece of the puzzle. Prog Retin Eye Res. 2018;64:77–83. doi:10.1016/j.preteyeres.2018.01.003
12. Chen PP, Lin SC, Junk AK, Radhakrishnan S, Singh K, Chen TC. the effect of phacoemulsification on intraocular pressure in glaucoma patients: a report by the American academy of ophthalmology. Ophthalmology. 2015;122(7):1294–1307. doi:10.1016/j.ophtha.2015.03.021
13. Jimenez-Roman J, Lazcano-Gomez G, Martínez-Baez K, et al. Effect of phacoemulsification on intraocular pressure in patients with primary open angle glaucoma and pseudoexfoliation glaucoma. Int J Ophthalmol. 2017;10(9):1374–1378. doi:10.18240/ijo.2017.09.07
14. Poley BJ, Lindstrom RL, Samuelson TW, R S Jr. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946–1955. doi:10.1016/j.jcrs.2009.05.061
15. Wang N, Chintala SK, Fini ME, Schuman JS. Ultrasound activates the TM ELAM-1/IL-1/NF-kappaB response: a potential mechanism for intraocular pressure reduction after phacoemulsification. Invest Ophthalmol Vis Sci. 2003;44(5):1977–1981. doi:10.1167/iovs.02-0631
16. Poley BJ, Lindstrom RL, Samuelson TW. Long-term effects of phacoemulsification with intraocular lens implantation in normotensive and ocular hypertensive eyes. J Cataract Refract Surg. 2008;34(5):735–742. doi:10.1016/j.jcrs.2007.12.045
17. Vinod K, Gedde SJ, Feuer WJ, et al. practice preferences for glaucoma surgery: a survey of the American glaucoma society. J Glaucoma. 2017;26(8):687–693. doi:10.1097/IJG.0000000000000720
18. Sun X, Dai Y, Chen Y, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Retin Eye Res. 2017;57:26–45. doi:10.1016/j.preteyeres.2016.12.003
19. Ashaye AO, Komolafe OO. Post-operative complication of trabeculectomy in Ibadan, Nigeria: outcome of 1-year follow-up. Eye. 2009;23(2):448–452. doi:10.1038/sj.eye.6702979
20. Patel HY, Danesh-Meyer HV. Incidence and management of cataract after glaucoma surgery. Curr Opin Ophthalmol. 2013;24(1):15–20. doi:10.1097/ICU.0b013e32835ab55f
21. Sun C, Zhang H, Tang Y, et al. Aqueous inflammation and ischemia-related biomarkers in neovascular glaucoma with stable iris neovascularization. Curr Eye Res. 2020;45(12):1504–1513. doi:10.1080/02713683.2020.1762226
22. Xinping Y, Weihua P, Mei R, Jia Q. Supraciliochoroidal fluid incidence at the early stage after trabeculectomy: study with anterior segment optical coherence tomography. Curr Eye Res. 2011;36(9):818–823. doi:10.3109/02713683.2011.593724
23. Jung KI, Park H, Jung Y, Park CK. Serial changes in the bleb wall after glaucoma drainage implant surgery: characteristics during the hypertensive phase. Acta Ophthalmol. 2015;93(4):e248–53. doi:10.1111/aos.12571
24. Nouri-Mahdavi K, Caprioli J. Evaluation of the hypertensive phase after insertion of the ahmed glaucoma valve. Am J Ophthalmol. 2003;136(6):1001–1008. doi:10.1016/s0002-9394(03)00630-5
25. Gu J, Ye WQ, Chen YZ, et al. The incidence and time distribution of early transient intraocular pressure elevation after penetrating canaloplasty. Zhonghua Yan Ke Za Zhi. 2022;58(11):882–889. doi:10.3760/cma.j.cn112142-20220617-00301
26. Chung AN, Aung T, Wang JC, Chew PT. Surgical outcomes of combined phacoemulsification and glaucoma drainage implant surgery for Asian patients with refractory glaucoma with cataract. Am J Ophthalmol. 2004;137(2):294–300. doi:10.1016/j.ajo.2003.08.036
27. Pakravan M, Yazdani S, Shahabi C, Yaseri M. Superior versus inferior Ahmed glaucoma valve implantation. Ophthalmology. 2009;116(2):208–213. doi:10.1016/j.ophtha.2008.09.003
28. Shahid M, Saleem Z, Malik TG, Farqaleet M. Comparison of changes in retinal nerve fiber layer thickness and intraocular pressure between glaucoma and non-glaucoma patients after phacoemulsification. Pak J Med Sci. 2023;39(1):232–235. doi:10.12669/pjms.39.1.6531
29. Lee W, Bae HW, Kim CY, Seong GJ. The change of anterior segment parameters after cataract surgery in normal-tension glaucoma. Int J Ophthalmol. 2017;10(8):1239–1245. doi:10.18240/ijo.2017.08.09
30. Zhao Z, Zhu X, He W, Jiang C, Lu Y. Schlemm’s canal expansion after uncomplicated phacoemulsification surgery: an optical coherence tomography study. Invest Ophthalmol Vis Sci. 2016;57(15):6507–6512. doi:10.1167/iovs.16-20583
31. Bhallil S, Andalloussi IB, Chraibi F, Daoudi K, Tahri H. Changes in intraocular pressure after clear corneal phacoemulsification in normal patients. Oman J Ophthalmol. 2009;2(3):111–113. doi:10.4103/0974-620X.57309
32. Lee SE, Kim KN, Kim WJ, Lee SB, Kim CS. Encapsulated bleb excision with collagen matrix implantation following failed ahmed glaucoma valve implantation. Korean J Ophthalmol. 2019;33(3):214–221. doi:10.3341/kjo.2018.0110
33. Eslami Y, Fakhraie G, Moghimi S, et al. excisional bleb revision for management of failed ahmed glaucoma valve. J Glaucoma. 2017;26(12):1144–1148. doi:10.1097/IJG.0000000000000806
34. Khan H, Alam M, Khan A. Comparison of the safety and efficacy of single injection of subtenon triamcinolone and topical dexamethasone in reducing postoperative inflammation after phacoemulsification and intraocular lens implantation. J Pak Med Assoc. 2016;66(9):1127–1131.
35. Juthani C, Chuck E. Non-steroidal anti-inflammatory drugs versus corticosteroids for controlling inflammation after uncomplicated cataract surgery. Cochrane Database Syst Rev. 2017;7(7):CD010516. doi:10.1002/14651858.CD010516.pub2
36. Thieme H, Choritz L, Hofmann-Rummelt C, Schloetzer-Schrehardt U, Kottler UB. Histopathologic findings in early encapsulated blebs of young patients treated with the ahmed glaucoma valve. J Glaucoma. 2011;20(4):246–251. doi:10.1097/IJG.0b013e3181e080ef
37. Mahale A, Fikri F, Al Hati K, et al. Histopathologic and immunohistochemical features of capsular tissue around failed Ahmed glaucoma valves. PLoS One. 2017;12(11):e0187506. doi:10.1371/journal.pone.0187506
38. Mills RP, Budenz DL, Lee PP, et al. Categorizing the stage of glaucoma from pre-diagnosis to end-stage disease. Am J Ophthalmol. 2006;141(1):24–30. doi:10.1016/j.ajo.2005.07.044
39. Fu L, Chan YK, Li J, Nie L, Li N, Pan W. Long term outcomes of cataract surgery in severe and end stage primary angle closure glaucoma with controlled IOP: a retrospective study. BMC Ophthalmol. 2020;20(1):160. doi:10.1186/s12886-020-01434-9
40. Menglu J, Aimeng D, Huiping Y. Research progress on inhibition of filtration area scarring after implantation of Ahmed glaucoma valve. Chin J Exp Ophthalmol. 2024;42(04):397–400. doi:10.3760/cma.j.cn115989-20201130-00807
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.