Back to Journals » Breast Cancer: Targets and Therapy » Volume 11
Comparison Of Accelerated Partial Breast Radiation Therapy And External Beam Radiation Therapy By Treatment Planning Indices
Authors Hejazi P, Tirtash MJ, Khoshnazar AK
Received 18 August 2019
Accepted for publication 1 October 2019
Published 14 November 2019 Volume 2019:11 Pages 303—307
DOI https://doi.org/10.2147/BCTT.S227686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Peyman Hejazi,1 Maede Jafari Tirtash,2 Alireza Khoshbin Khoshnazar3
1Department of Medical Physics, Semnan University of Medical Sciences, Semnan, Iran; 2Department of Radiotherapy, Mirdamad Oncology and Radiotherapy Center, Gorgan, Iran; 3Department of Biochemistry and Medical Physics, Faculty of Medicine, Golestan University of Medical Sciences, Gorgan, Iran
Correspondence: Alireza Khoshbin Khoshnazar
Department of Biochemistry and Medical Physics, Faculty of Medicine, Golestan University of Medical Sciences, Gorgan, Iran
Tel +98-9113773145
Email [email protected]
Background: Accelerated partial breast irradiation (APBI) is a method in which just bed of lumpectomy with a margin of 1–2 cm is irradiated. Regarding advantages of APBI to whole-brain radiation therapy (WBRT) and limitations for performing other techniques, we compare external beam radiation therapy (EBRT) with three-dimensional conformal radiation therapy (3DCRT), as a type of APBI technique.
Methods: Dosimetric parameters including uniformity index (UI), conformity index (CI), and homogeneity index (HI) beside heart and lung doses were assessed and compared in two techniques. CT images of 24 patients with left-sided breast cancer after lumpectomy were selected. Patients were categorized into three groups based on the volume of breast, respectively, ≤ 1000 cc, 1000–1500 cc, and ≥ 1500 cc. CI, HI, UI and DVH were calculated by DosiSoftIsogray treatment planning software.
Results: Results show the value of UI in APBI method is more than EBRT method significantly (p=0.004). Moreover, that CI in APBI method was more than EBRT (p=0.0000) and nearer to 1. There was no significant difference between HI values between APBI and EBRT methods. As the volume of breast gets bigger, HI values rise, meaning worse homogeneity.
Conclusion: APBI method may be a good method for minimizing side effect and minimizing treatment periods.
Keywords: partial radiation therapy, external beam radiation therapy, breast cancer
Introduction
The most common cancer in women is breast cancer among other cancer, with probability in order of 28.1 in 100,000.1 In 2016, 246,660 new cases of breast cancer were diagnosed comprising 29 percent of all cancers within which 40,450 died, meaning 14 percent mortality.2
Prognosis and treatment method generally depend on stage and vast of metastasis. Method of treatment principally includes surgery (lumpectomy and mastectomy), radiotherapy and systematic treatment (chemotherapy and hormone therapy).3,4
After breast conserves surgery, radiotherapy may reduce the incidence of recurrence to half and mortality rate to 1/6. In many cases, breast-conserving surgery can eliminate any diagnosed microscopic disease. Nevertheless, some microscopic tumors may persist and if not treated result in recurrence or metastasis or both.5 Radiotherapy after surgery reduces local recurrence from 27.2% to 8.8%.6
Breast-conserving radiotherapy is divided generally into two methods: external beam radiation therapy to the whole breast and partial breast radiation.7
External beam radiation therapy (EBRT) involves 50–55 total doses with a daily dose of 1.8–2 Gy to the breast in a period of 5–6 weeks.8
Disadvantages of EBRT include cancer induction to contralateral breast,9 dose receiving by adjacent anatomies like coronary arteries and other sensitive organs10 and requiring patients to be visited in the department for 6–7 weeks.9
Partial breast irradiation (PBI) has been proposed as a solution for the above problems.11 Accelerated partial breast irradiation (APBI) is the method in which just a bed of lumpectomy with a margin of 1–2 cm is irradiated, while fraction dose is escalated and target volume is diminished. The technique let treatment time to be shortened.12,13 As a smaller portion of the breast is irradiated, the number of time must have radiation is reduced, making it more comfortable for patients and their family.
Current researches show that PBI results in less local recurrence rate that is comparable to the recurrence rate of whole breast irradiation. Moreover, the cosmetic consequence was better than for most patients making it a worthy option for patients with smaller tumors.
APBI is performed by two methods: brachytherapy and 3D external conformal radiation therapy.14 Volumetric modulated arc therapy (VMAT), three-dimensional conformal radiation therapy (3DRT), intensity-modulated radiotherapy (IMRT) and proton beam therapy are among 3D external conformal radiation therapy techniques.15
Because of the three-dimensional structure of the breast, an accomplishment of uniform dose distribution in breast volume is laborious. Treatment planning to achieve uniform dose, due to the volume and shape of breast and chest wall movement, is challengeable.16
Regarding the advantages of APBI to whole-brain radiation therapy (WBRT) and limitations for performing other techniques, we compare EBRT with 3DCRT, as a type of APBI technique. Dosimetric parameters including CI, homogeneity index (HI), and UI beside heart and lung doses were assessed and compared in two techniques.
Materials And Methods
CT images of 24 patients with left-sided breast cancer after lumpectomy were selected. CT slices' thickness were 5 mm. Patients were categorized into three groups based on the volume of breast, respectively, ≤ 1000 cc, 1000–1500 cc, and ≥ 1500 cc. Data gathering was randomly performed and including criteria were the side of involved breast and volume of the breast.
During imaging, patients were rested on a breast board in the supine position while her hands were placed on armrest paddle. The breast limits were determined by the physician by clinical palpation and marked by radio-opaque markers for CT acquisition. The upper border was the lower margin of clavicular head, the medial border was midline of the sternum and the lateral border was the midaxillary line. The lower border was taken 2 cm beneath the lower fold of the breast.
Contouring of GTV, PTV, and OAR was fulfilled by the physician according to RTOG protocol. Treatment planning was performed for both group of EBRT and APBI as follows (Figure 1):
- EBRT: Treatment planning was based on two large and two small subfields. Delivered dose was determined 50 Gy with a daily fraction of 2 Gy. The daily dose was so divided to deliver 180 cGy to a large field and 20 cGy to subfield.
- APBI: To reach the optimum dose distribution, beam parameters like gantry and collimator angles and beam weight were changed and modified continuously. Two tangent fields were used to envelop lumpectomy bed, marked by surgical clips, with 1–2 cm margin. The total delivered dose was determined to be 40 Gy with a fraction dose of 4 Gy, twice a day with a minimum spacing of 6 hrs.
Dosimetric factors including CI, HI, UI and DVH were calculated by DosiSoftIsogray treatment planning software.
Definition Of Parameters
Conformity index (CI): It is defined as a ratio between the volume covered by the reference isodose, which according to ICRU is 95% isodose, and the target volume is designated as planned target volume (PTV).
Conformity indexRTOG = TVRI/TV Where TVRI = Reference isodose volume and TV = Target volume.17
Homogeneity index (HI): It is defined as a ratio between the dose reached in 95% of the PTV volume (D≥95%) and the dose reached in 50% (D≥5%) of the PTV volume.18
HI = (D2%−D98%)/D50%
Uniformity index (UI): It is defined as a ratio between minimum doses reached in 5% of the PTV volume (D 5%) and the minimum dose reached in 95% of PTV volume (D 95%).19
UI = D 5%/D 95%
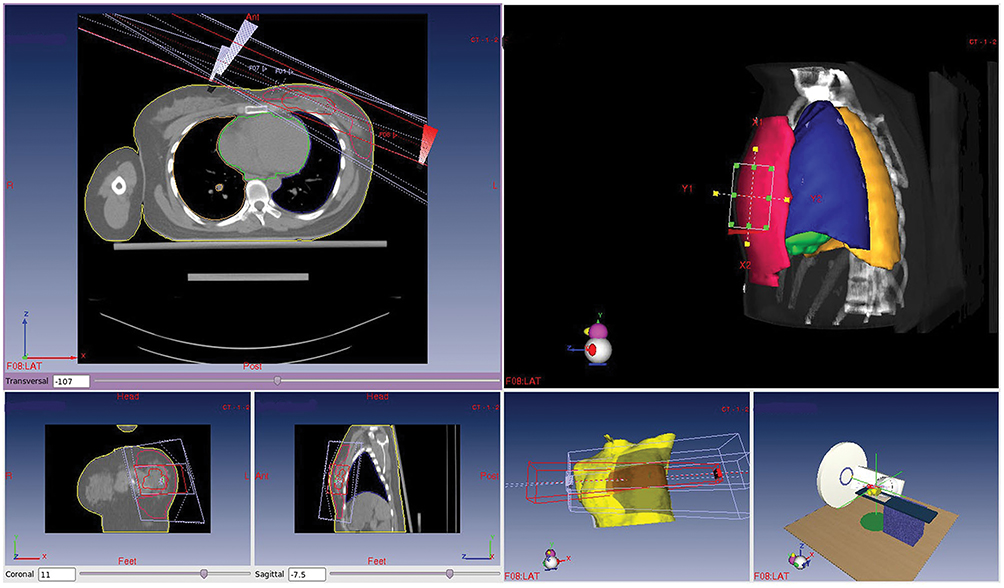 |
Figure 1 Comparison of EBRT and PBI methods. |
Results
As it is shown in Table 1, uniformity index in APBI method is more than EBRT (P=0.004) for all volume groups. It is clear that CI in APBI method was more than EBRT (P= 0.000) and closer to 1 showing better conformity in APBI method. There was no significant difference between two APBI and EBRT methods. As the volume of breast gets bigger, HI values rise, meaning worse homogeneity. The average dose received by the heart and the lung in the APBI method is less than the EBRT method (P=0.05).
 |
Table 1 Comparison Of Uniformity Index (UI), Conformity Index (CI), And Homogeneity Index (HI) Between APBI And EBRT Methods For Three Volumes Of The Breast (Sample Size In Each Volume Group Is 8 Patients) |
As the above table shows, there is no relation between UI, HI and volume of the breast in both methods of irradiation (Table 2).
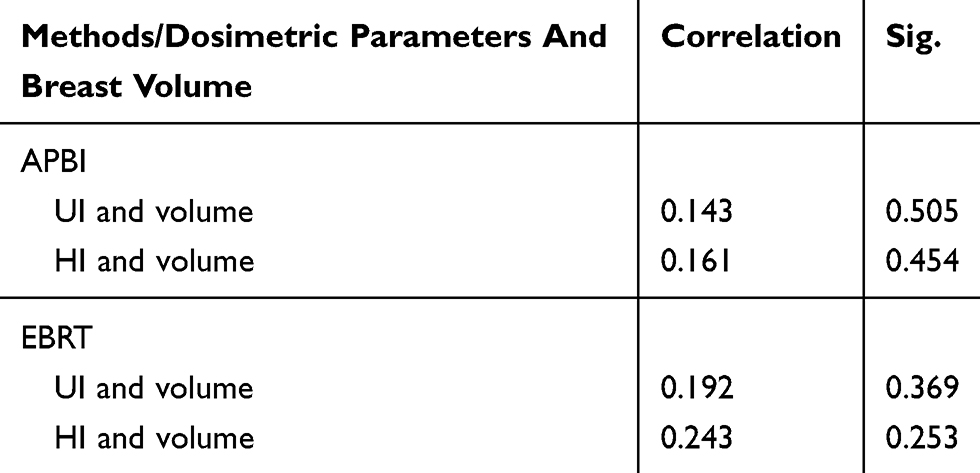 |
Table 2 The Correlation Coefficient Between Dosimetric Parameters (UI, HI) And Breast Volume In Two Methods And Significant P Value |
Discussion
Partial breast irradiation (PBI) has been proposed as a solution for reducing radiotherapy side effects while putting the less mental burden for cancer patients.11 Accelerated partial breast irradiation (APBI) is the method in which just a bed of lumpectomy with a margin of 1–2 cm receives radiation, while fraction dose is escalated and target volume is diminished. This technique caused treatment time to be shortened.12,13 As a smaller portion of the breast is irradiated, the number of time must have radiation is reduced, making it more comfortable for patients and their family.
Current researches show that PBI results in less local recurrence rate that is comparable to the recurrence rate of whole breast irradiation. Moreover, the cosmetic consequence was better than for most patients making it a worthy option for patients with smaller tumors.20
The uniformity index (UI), conformity index (CI) and homogeneity index are three tools for assessment of treatment plans. Of course, there are different definitions for them by different authors. APBI method has been introduced primarily to reduce the radiation side effects.12
Uniformity index gives an idea of total volume homogeneity inside a given prescription isodose which its ideal value is 1 and any value above 1 shows the presence of a high dose region. Our results show that the value of UI in the APBI method is more than the EBRT method significantly (p=0.004) delineating that the first one is not successful regarding uniformity.
Conformity index also can help in the comparison and selection of the best treatment plan. The conformity index equal to 1 shows ideal dose coverage or high conformity. In the case where the conformity index is less than 1, it means the target volume is incompletely radiated. Of course, values up to 1 can rarely be reached. Our results showed that CI in the APBI method was more than EBRT (p= 0.000) and closer to 1. In the higher volume of the breast, there was a greater deviation from RTOG protocol as it was less than 0.9 in the EBRT group.10,11
Homogeneity index (HI) verified that the dose distribution within the target volume is uniform. The ideal value is zero. There was no significant difference between the APBI and EBRT methods. As the volume of breast gets bigger, HI values rise, meaning worse homogeneity. Stewart and colleagues concluded that partial breast irradiation can be a suitable treatment alternative for breast cancer at early stages.21
In 2003, Vicini et al showed that average and median volume of heart and lung received 10, 20 and 30 Gy of prescribed doses, which were less in partial irradiation than EBRT,22 the same result we got in our experience.
Taghian et al showed the PBI method result in suitable coverage of PTV,23 the same result we did take. In 2004, Weed concluded that 3DRT way for APBI approach can better cover PTV while lung dose was a bit higher than other PBI,24 which we did not examine.
Finally, the APBI method may be a good method for minimizing side effects and minimizing treatment periods. Its clinical outcome must be examined more.
Ethics Approval And Consent To Participate
The study is approved by the ethical committee of Golestan University of Medical Sciences. We confirm that participant consent was written informed consent and that the study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Almasi Z, Mohammadian-Hafshejani A, Salehiniya H. Incidence, mortality, and epidemiological aspects of cancers in Iran; differences with the world data. J Buon. 2016;21:994–1004.
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. doi:10.3322/caac.21332
3. Aebi S, Davidson T, Gruber G, Cardoso F, Group EGW. Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2011;22 Suppl 6:vi12–24. doi:10.1093/annonc/mdr371
4. Maughan KL, Lutterbie MA, Ham PS. Treatment of breast cancer. Am Fam Physician. 2010;81:1339–1346.
5. Darby S, McGale P, Correa C; Early Breast Cancer Trialists’ Collaborative G, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707–1716. doi:10.1016/S0140-6736(11)61629-2
6. Early Breast Cancer Trialists’ Collaborative G. Effects of radiotherapy and surgery in early breast cancer. An overview of the randomized trials. N Engl J Med. 1995;333:1444–1455. doi:10.1056/NEJM199511303332202
7. Moore-Higgs GJ, editor Radiation options for early stage breast cancer.
8. Ebert MA, Carruthers B. Dosimetric characteristics of a low-kV intra-operative x-ray source: implications for use in a clinical trial for treatment of low-risk breast cancer. Med Phys. 2003;30:2424–2431. doi:10.1118/1.1595611
9. Kuerer HM, Julian TB, Strom EA, et al. Accelerated partial breast irradiation after conservative surgery for breast cancer. Ann Surg. 2004;239:338–351. doi:10.1097/01.sla.0000114219.71899.13
10. Cuncins-Hearn A, Saunders C, Walsh D, et al. A systematic review of intraoperative radiotherapy in early breast cancer. Breast Cancer Res Treat. 2004;85:271–280. doi:10.1023/B:BREA.0000025411.77758.1e
11. Wallner P, Arthur D, Bartelink H, et al. Workshop on partial breast irradiation: state of the art and the science, Bethesda, MD, December 8- 10, 2002. J Natl Cancer Inst. 2004;96:175–184. doi:10.1093/jnci/djh023
12. Njeh CF, Saunders MW, Langton CM. Accelerated Partial Breast Irradiation (APBI): a review of available techniques. Radiat Oncol. 2010;5:90. doi:10.1186/1748-717X-5-90
13. Kozak KR, Doppke KP, Katz A, Taghian AG. Dosimetric comparison of two different three-dimensional conformal external beam accelerated partial breast irradiation techniques. Int J Radiat Oncol Biol Phys. 2006;65:340–346. doi:10.1016/j.ijrobp.2005.12.053
14. Balaji K, Subramanian B, Yadav P, Anu Radha C, Ramasubramanian V. Radiation therapy for breast cancer: literature review. Med Dosim. 2016;41:253–257. doi:10.1016/j.meddos.2016.06.005
15. Khan F, Gerbi B. Treatment Planning in Radiation Oncology. Wolters kluwer. 2012.
16. Kurian AW, Lichtensztajn DY, Keegan TH, Nelson DO, Clarke CA, Gomez SL. Use of and mortality after bilateral mastectomy compared with other surgical treatments for breast cancer in California, 1998–2011. JAMA. 2014;312:902–914. doi:10.1001/jama.2014.10707
17. Kataria T, Sharma K, Subramani V, Karrthick KP, Bisht SS. Homogeneity Index: an objective tool for assessment of conformal radiation treatments. J Med Phys. 2012;37:207–213. doi:10.4103/0971-6203.103606
18. Feuvret L, Noël G, Mazeron -J-J, Bey P. Conformity index: a review. Int J Radiat Oncol Biol Phys. 2006;64:333–342. doi:10.1016/j.ijrobp.2005.09.028
19. Hsieh CH, Liu CY, Shueng PW, et al. Comparison of coplanar and noncoplanar intensity-modulated radiation therapy and helical tomotherapy for hepatocellular carcinoma. Radiat Oncol. 2010;5:40. doi:10.1186/1748-717X-5-40
20. Tann AW, Hatch SS, Joyner MM, Wiederhold LR, Swanson TA. Accelerated partial breast irradiation: past, present, and future. World J Clin Oncol. 2016;7:370–379. doi:10.5306/wjco.v7.i5.370
21. Stewart AJ, Khan AJ, Devlin PM. Partial breast irradiation: a review of techniques and indications. Br J Radiol. 2010;83:369–378. doi:10.1259/bjr/11505970
22. Vicini FA, Remouchamps V, Wallace M, et al. Ongoing clinical experience utilizing 3D conformal external beam radiotherapy to deliver partial-breast irradiation in patients with early-stage breast cancer treated with breast-conserving therapy. Int J Radiat Oncol Biol Phys. 2003;57:1247–1253. doi:10.1016/s0360-3016(03)01573-6
23. Taghian AG, Kozak KR, Doppke KP, et al. Initial dosimetric experience using simple three-dimensional conformal external-beam accelerated partial-breast irradiation. Int J Radiat Oncol Biol Phys. 2006;64:1092–1099. doi:10.1016/j.ijrobp.2005.09.042
24. Weed DW, Yan D, Martinez AA, Vicini FA, Wilkinson TJ, Wong J. The validity of surgical clips as a radiographic surrogate for the lumpectomy cavity in image-guided accelerated partial breast irradiation. Int J Radiat Oncol Biol Phys. 2004;60:484–492. doi:10.1016/j.ijrobp.2004.03.012
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.