Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Comparison Between Trichoscopic and Histopathological Evaluations of Hair Parameters
Received 9 March 2022
Accepted for publication 27 April 2022
Published 10 May 2022 Volume 2022:15 Pages 843—849
DOI https://doi.org/10.2147/CCID.S365670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Danchen Hu,1– 4 Ping Tu,1– 4 Shuxia Yang1– 4
1Department of Dermatology, Peking University First Hospital, Beijing, 100034, People’s Republic of China; 2National Clinical Research Center for Skin and Immune Diseases, Beijing, 100034, People’s Republic of China; 3Beijing Key Laboratory of Molecular Diagnosis on Dermatoses, Beijing, 100034, People’s Republic of China; 4NMPA Key Laboratory for Quality Control and Evaluation of Cosmetics, Beijing, 100034, People’s Republic of China
Correspondence: Shuxia Yang, Department of Dermatology, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel + 86-13661345723, Email [email protected]
Background: Collecting data on hair counts helps dermatologists diagnose hair diseases more accurately. Quantitative trichoscopy analysis and pathologic examination are two common ways to evaluate hair parameters.
Purpose: The study aims to compare the effect of quantitative trichoscopy analysis and pathologic examination in hair counting and quantify the hair density of average Chinese people.
Methods: Trichoscopy was performed in four scalp regions with a total of twenty-three volunteers without alopecia: frontal, vertex, occipital, and parietal. Hair density parameters were recorded. A 4-mm punch biopsy was performed in the occipital area, and all specimens were transversely sectioned serially and observed to calculate the hair densities.
Results: The average hair density, hairs per follicle unit, and vellus hair ratio from quantitative trichoscopy analysis in the occipital region were 163.07± 28.17/cm2, 1.87± 0.25 and 6.60± 3.95%, lower than those from biopsy significantly (214.97± 48.73/cm2, 2.24± 0.30 and 10.48± 6.43%). The hair shaft diameter measured by quantitative trichoscopy analysis was 74.52± 8.02μm, higher than that by histopathologic examination (68.65± 8.00μm) (p< 0.05).
Conclusion: Quantitative trichoscopy is a noninvasive, quick, and convenient way to evaluate hair density. Histopathologic examination is an invasive way but provides more accurate data. The data obtained from trichoscopy and pathological examination are different to some extent, which cannot be substituted entirely for each other. This study established the reference for hair density in the adult Chinese population.
Keywords: hair, trichoscopy, histopathology
Introduction
Comparison between normal and abnormal scalp is vital for diagnosing hair diseases.1 The hair counts in the normal scalp may help dermatologists diagnose hair diseases more accurately and, therefore, provide a helpful baseline and destination for treatment and research.
There are two ways to obtain data on hair counts, that are quantitative trichoscopy analysis and pathologic examination. Quantitative trichoscopy analysis is a non-invasive and quick method for dermatologists to collect magnified images of scalp area and analyze image data such as hair density and hair shaft diameter, which has been used in various research.2–4 Trichoscopy is used more and more widely in diagnosing hair loss diseases. The method has the great potential to replace scalp biopsy and pathologic examination in some areas for its noninvasiveness. Horizontal sectioning of 4-mm punch biopsy specimens is generally used to diagnose hair diseases, which may provide more precise information about hair follicles. Nevertheless, it is limited in application due to potential physical pain and even scars.
Hair density varies among demographics.5–10 However, data on hair counts in Chinese people are lacking. This study investigates the data of average scalp hair density from histopathology and trichoscopy in the Chinese population and compares the efficacy of quantitative trichoscopy analysis and pathologic examination in hair counting.
Subjects and Methods
Subjects
A cross-sectional study was conducted. The sample size was estimated based on data from a previous study assessing values of hair counts per 4 mm diameter punch biopsy from the scalp of Taiwan people, demonstrating that the mean number of total hair follicles was 20.5±4.6.8 To achieve a confidence level of 95%, the researchers calculated the minimum number with a 10% margin of error, which was 21. Thirty volunteers (fourteen females and sixteen males) were recruited between April 2021 and July 2021. Inclusion criteria were healthy adult volunteers with clinically normal hair and scalp appearance. Exclusion criteria were (1) pregnant or lactating women; (2) history of severe cardiovascular diseases, endocrine diseases, autoimmune disease, or other systemic diseases; (3) presence of androgenic alopecia (AGA), alopecia areata, telogen effluvium (TE), or other hair/scalp disorders; (4) presence of erythema, scales, papules, or other active inflammation on the scalp; (5) hypersensitivity to pain; (6) history of keloid.
This study complied with the Declaration of Helsinki and was approved by the ethics committee of Peking University First Hospital (2020–460.) All the participants were informed about the purpose of the study and written consent was received from each participant before enrollment in the research.
Trichoscopy and Analysis
Hair imaging and measurements were conducted in four regions: right or left frontal hairline, vertex, right or left parietal, and occipital area, using a polarized contact dermoscopy (Fotofinder body studio ATBM, Fotofinder Systems GmbH, Bad Birnbach, Germany). The studied scalp areas were localized at (1) the top of the right or left frontotemporal angle determined by the hairstyle of the volunteer (marked as “frontal”), (2) the mid-point of the connection of the left and right external auditory ear canals (“vertex”), (3) the point 3cm above the auricle attachment point on the right or left side (“parietal”), (4) the mid-point just beneath the occipital carina (“occipital”) (Figure 1). The hairs of the target areas were shaved to about 2mm long.
 |
Figure 1 Measuring points of trichoscopy in frontal (A), parietal (B), vertex (C), and occipital (D) areas. |
The images were taken of each scalp area at a 20-fold magnification. All the parameters were measured by Trichoscale pro 3.2 software Instant Count (Fotofinder Universe 2019, Bad Birnbach, Germany) and corrected manually by an experienced trichologist. The average hair diameter and hair count parameters were calculated by the software automatically.
Histopathologic Examination
A 4-mm punch biopsy was performed in the occipital region of each volunteer, at the same site as the trichoscopy examination site. The biopsy specimens were fixed in the 10% neutral, buffered formalin solution. The fixed specimens were cut horizontally in the middle of the total length and embedded in the blocks, and serial sections were obtained from the epidermis to the fatty layer. All sections were stained with hematoxylin and eosin. All slides were scanned by the Hamamatsu NDP slide scanner (NanoZoomer 2.0RS, Japan) and observed at the viewing platform (NDP.Viewer 2). Hair shaft diameter was measured by mouse pointing and dragging vertically from one edge of the hair shaft to the other edge (Figure 2A). Because some hair shafts may be lost in the process of slide-making, it is usually observed that only some hair shafts were still retained in a section, and all the hair shaft diameters information can be completed through other sections of the same specimen. To simplify the analyses, hair follicles with a shaft whose diameter was less than 0.03 mm were defined as vellus hairs and those shafts of larger diameter were categorized as terminal hairs in this study. All follicular structures were identified at various anatomical levels from the epidermis to the subcutis. Hair parameters including the number of total hairs, terminal hairs, vellus hairs, and follicle units, the ratio of the terminal to vellus hair, and anagen to telogen were recorded (Figure 2B).
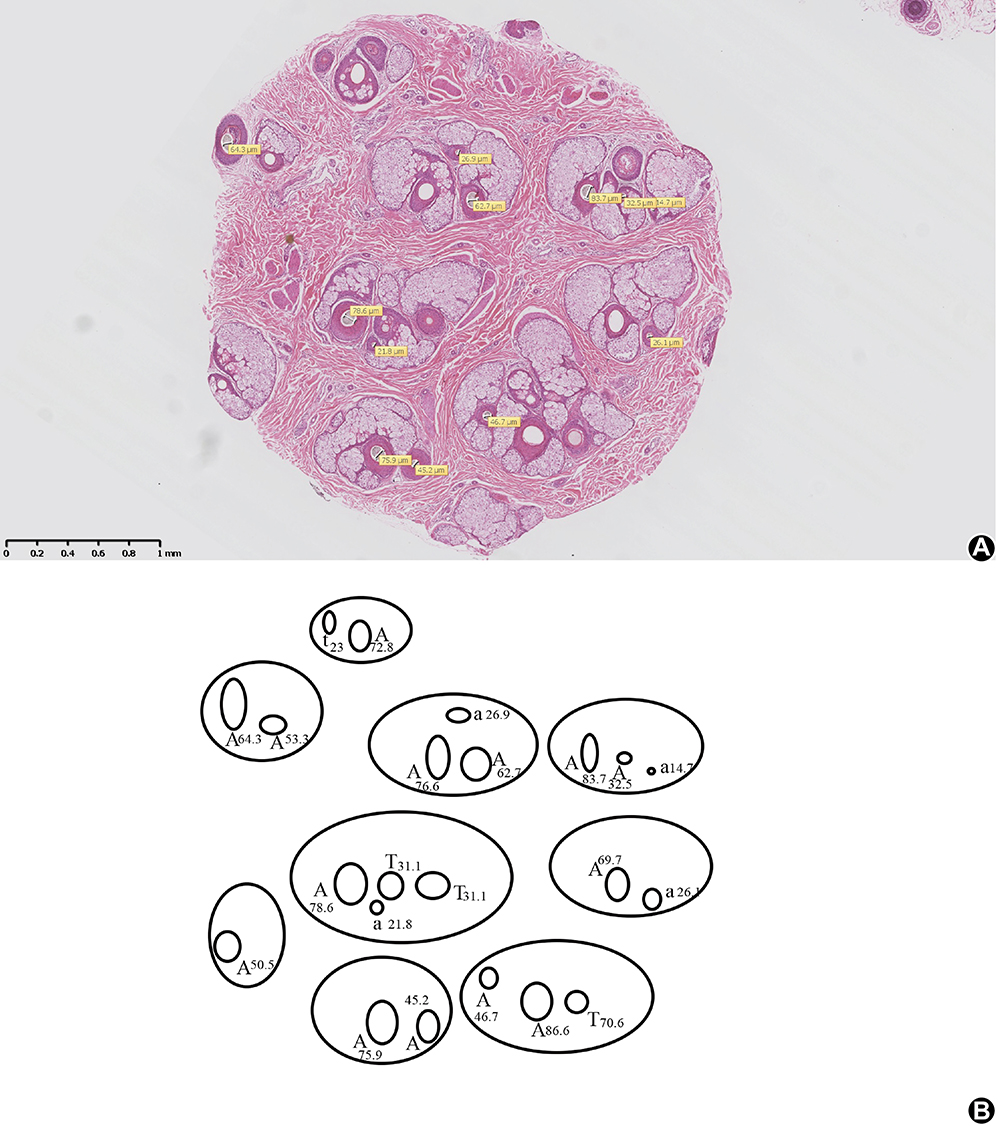 |
Figure 2 Measurement method of histopathological sections. (A) Hair shaft diameter is measured by the mouse pointing and dragging vertically from one edge of the hair shaft to the other edge at the viewing platform (NDP.Viewer 2). The hair shafts missing in this section can be found and measured in the corresponding serial sections. (B) A diagram is made to record hair shaft diameter and the stage of the hair cycle. A: terminal anagen hair. a: vellus anagen hair. T: terminal catagen or telogen hair. t: vellus catagen or telogen hair. |
Statistical Analysis
Quantifiable data was presented as the mean±SD. The parameters of hair density at different scalp sites were evaluated using an analysis of variance. Statistical analysis was performed to compare the hair density parameters of biopsy and trichoscopy by using paired Student’s t-test. Statistical significance was determined as p<0.05.
Results
Thirty scalp biopsy specimens were taken from thirty volunteers, including fourteen females and sixteen males. However, seven subjects showed pathologic manifestations of androgenic alopecia (AGA) (terminal/vellus ratio<35) or telogen effluvium (TE) (telogen ratio>20%11). Therefore, these patients were excluded from statistical analysis.
Among the twenty-three participants, the average biopsy specimen contained 12.17 follicle units and 27 hairs comprising 24.26 terminal and 2.74 vellus hairs, a 12.27:1 ratio, with 91.1% anagen and 8.9% telogen hairs. The mean hair shaft diameter was 68.65±8.00μm, and the mean hair density was 214.97±48.73/cm2.
The data obtained from trichoscopy showed that hair densities varied according to scalp sites, with the highest density in the vertex region and the highest vellus hair ratio in the frontal region. The follicle unit counts and average hair per follicle unit were the lowest in the parietal area compared with other areas. The comparison of hair count parameters on trichoscopy among different scalp regions is demonstrated in Table 1.
 |
Table 1 Hair Counts from Quantitative Trichoscopic Analysis in Different Scalp Regions of 23 Normal Volunteers |
Statistical analysis was performed to compare the hair density parameters in the occipital region of biopsy and trichoscopy by using paired Student’s t-test. The differences in hair count parameters between 4-mm punch biopsy and trichoscopy of twenty-three volunteers are shown in Table 2. The hair density, mean hair per follicle unit and vellus hair ratio from 4-mm punch biopsy were 214.97±48.73/cm2, 2.24±0.30, and 10.48±6.43%, higher than those from quantitative trichoscopy analysis (163.07±28.17/cm2, 1.87±0.25 and 6.60±3.95%). The hair shaft diameter and terminal hair shaft diameter of the biopsy were 68.65±8.00μm and 73.77±6.74μm, less than those of trichoscopy (74.52±8.02μm and 77.87±7.53μm). The differences were statistically significant (p<0.05).
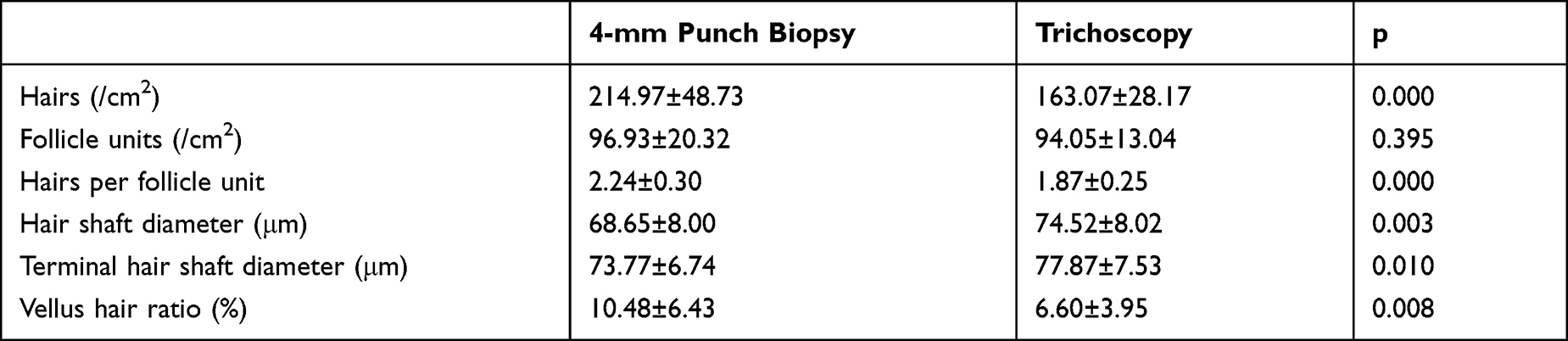 |
Table 2 Comparison of Hair Count Parameters in the Occipital Region Between 4-mm Punch Biopsy Specimens and Quantitative Trichoscopic Analysis |
Discussion
Headington introduced horizontal sectioning of scalp biopsy specimens in 1984,12 and even with a small 4-mm punch biopsy, this method can help trichologists count the number of all follicles in the specimen accurately. However, the application of scalp biopsy is limited due to related pain and scars in clinical practice. With the emergence of dermatoscopy and advances in machine learning and deep learning, quantitative trichoscopy analysis, a form of video dermoscopy combined with an image analysis system, can provide information about hair density and hair diameter, and is used more and more widely in diagnosing hair loss diseases. It has the great potential to replace scalp biopsy and pathologic examination in some areas because of its noninvasiveness.
This study conducted hair imaging and measurements in frontal, vertex, parietal and occipital scalp regions. The results showed hair densities vary in specific sites, and the density in the vertex was the highest, following the previous study.3,4,13–16 The hair density, vellus ratio, and hair shaft diameter in the occipital region were 163.07±28.17/ cm2, 6.60±3.95%, and 74.52±8.02μm.
A biopsy was performed on each volunteer to compare the difference between trichoscopy and histopathologic examination. Due to related pain and potential scars, it is hard for volunteers to accept multiple-spot biopsies. Hence, biopsies were only performed in occipital regions. Excluding the seven suspected AGA or TE patients, the mean number of hairs was 27.00±6.12 in a 4-mm punch biopsy specimen. The mean hair density, vellus ratio, and hair shaft diameter in the occipital region were 214.97±48.73/cm2, 10.48±6.43%, and 68.65±8.00μm. It is widely accepted that the occipital region of the scalp is an unaffected area of AGA, and in a previous study, the occiputs of AGA cases were used to determine reference data for normal scalp.6 However, Khunkhet17 recently found that AGA can involve the occipital area of male patients. We also found that some volunteers whose hair parameter data were excluded from analysis showed pathologic features of AGA in occipital areas, which was in accordance with Khunkhet’s finding, indicating that occipital area may be involved by AGA even in an early stage. So, in this study, the data from healthy Chinese volunteers without hair loss diseases can be made as a reference in the Chinese population.
We compared the hair count parameters of the occipital region from quantitative trichoscopy analysis and 4-mm punch biopsy using paired t-test. The hair density, average follicles per unit, and vellus ratio from the biopsy were higher than those from quantitative trichoscopy analysis. The reason for these differences may be that the quantitative trichoscopy analysis system cannot recognize all grey or vellus hair2 and sheltered hairs, despite having done manual correction. In addition, all the follicles in a specimen can be taken into count in serial horizontal sections, while only follicles with hair shafts can be identified from trichoscopy analysis, which means some telogen follicles without a hair shaft would be ignored. In this study, the hairs recognized by the software were categorized into six different thickness groups, then the software estimated the average hair shaft diameter. So, this estimation instead of direct measurement may cause a higher mean hair shaft diameter from trichoscopy analysis.
Manual correction is vital to obtain accurate data because the software’s ability to recognize the thin hairs or grey hairs is limited. With the development of artificial intelligence, the machine learning algorithm may reduce manual assistance and improve accuracy.18
Quantitative trichoscopic analysis is a non-invasive, uncomplicated, easily reproducible, and less time-consuming method to measure hair density, suitable for follow-up and large sample studies. However, the data of trichoscopy from different studies vary, which may be affected by many other factors in addition to population or device differences. Chen3 reported the average occipital hair shaft diameter and single hair follicle unit ratio of 35 normal Chinese females from quantitative trichoscopic analysis were 68.34±7.70μm and 13.47±8.74%, which were slightly lower than this study (74.52±8.02μm and 33.77±12.78%). However, the occipital vellus hair ratio reported by Chen3 was 8.88±4.23%, higher than 6.60±3.95% in this study. The distinction may be caused by different magnification and count modes. The 50-fold magnification used by Chen3 made more thin hairs be recognized, leading to a higher vellus hair ratio and lower single hair follicle unit ratio, and average hair shaft diameter. In addition to the differences in the trichoscopic equipment and analysis software, whether cutting hairs may explain such variety. Both Birnbaum2 and Lossouarn15 reported the hair density in the vertex area (226 ± 20 VS 248±51/cm2) and occipital area (214 ± 28 VS 224±43/cm2) of Caucasians in the USA. They used different trichoscopic devices and analysis programs. In Lossouarn15ʹs research, the hairs in the examination sites were shaved before trichoscopic examination, while the hairs were not shaved in Birnbaum2ʹs study. Long hairs may lead to underestimated hair count owing to shielding.
In this study, we selected thirty participants without hair loss diseases by taking history and trichoscopic examination according to current criteria. However, seven participants showed pathologic manifestations of AGA or TE. In the subsequent follow-up, corresponding clinical manifestations were shown in the suspected TE patient, which means histopathologic examination can identify catagen or telogen follicles to early diagnose diseases of the hair cycle. Catagen or telogen follicles cannot be identified by a single trichoscopic examination, and instead require continuous, dynamic observation.
Accurate data though the histopathologic examination may provide, invasiveness limits the application, and it is hard to conduct a large sample study based on biopsy. In addition, there should be experienced trichologists or pathologists who have been trained professionally and are familiar with hair pathology, which is a factor that potentially increases the difficulty of popularizing this method.
The limitation of this study is its relatively small sample size. And biopsy was only performed in the occipital region, so the results may not represent other scalp areas. Further studies with large sample size and evaluation of other scalp areas are needed.
Conclusion
This study established the reference of hair density from quantitative trichoscopy analysis and 4mm punch biopsy horizontal section in the Chinese population. Both trichoscopy and pathological examination have their advantages and disadvantages, and the data obtained from these two ways are different to some extent, which cannot be substituted entirely for each other.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sperling LC. Hair density in African Americans. Arch Dermatol. 1999;135(6):656–658. doi:10.1001/archderm.135.6.656
2. Birnbaum MR, McLellan BN, Shapiro J, Ye K, Reid SD. Evaluation of Hair Density in Different Ethnicities in a Healthy American Population Using Quantitative Trichoscopic Analysis. Skin Appendage Disord. 2018;4(4):304–307. doi:10.1159/000485522
3. Chen X, Li X, Chen B, Yin Y, Zhang J, Zhou C. Female Pattern Hair Loss in Female and Male: a Quantitative Trichoscopic Analysis in Chinese Han Patients. Front Med. 2021;8:649392. doi:10.3389/fmed.2021.649392
4. Leerunyakul K, Suchonwanit P. Evaluation of Hair Density and Hair Diameter in the Adult Thai Population Using Quantitative Trichoscopic Analysis. Biomed Res Int. 2020;2020:2476890. doi:10.1155/2020/2476890
5. Whiting DA. Diagnostic and predictive value of horizontal sections of scalp biopsy specimens in male pattern androgenetic alopecia. J Am Acad Dermatol. 1993;28(5 Pt 1):755–763. doi:10.1016/0190-9622(93)70106-4
6. Lee HJ, Ha SJ, Lee JH, Kim JW, Kim HO, Whiting DA. Hair counts from scalp biopsy specimens in Asians. J Am Acad Dermatol. 2002;46(2):218–221. doi:10.1067/mjd.2002.119558
7. Aslani FS, Dastgheib L, Banihashemi BM. Hair counts in scalp biopsy of males and females with androgenetic alopecia compared with normal subjects. J Cutan Pathol. 2009;36(7):734–739. doi:10.1111/j.1600-0560.2008.01149.x
8. Ko JH, Huang YH, Kuo TT. Hair counts from normal scalp biopsy in Taiwan. Dermatol Surg. 2012;38(9):1516–1520. doi:10.1111/j.1524-4725.2012.02462.x
9. Martinez-Luna E, Rodriguez-Lobato E, Vazquez-Velo JA, Cuevas-Gonzalez JC, Martinez Velasco MA, Toussaint Caire S. Quantification of Hair Follicles in the Scalp in Mexican Mestizo Population. Skin Appendage Disord. 2018;5(1):27–31. doi:10.1159/000488782
10. Visessiri Y, Pakornphadungsit K, Leerunyakul K, Rutnin S, Srisont S, Suchonwanit P. The study of hair follicle counts from scalp histopathology in the Thai population. Int J Dermatol. 2020;59(8):978–981. doi:10.1111/ijd.14989
11. Sperling LC, Cowper SE, Knopp EA. An Atlas of Hair Pathology with Clinical Correlations.
12. Headington JT. Transverse microscopic anatomy of the human scalp. A basis for a morphometric approach to disorders of the hair follicle. Arch Dermatol. 1984;120(4):449–456. doi:10.1001/archderm.1984.01650400031009
13. Rutnin S, Chanprapaph K, Pakornphadungsit K, et al. Variation of Hair Follicle Counts among Different Scalp Areas: a Quantitative Histopathological Study. Skin Appendage Disord. 2021;8(1):24–30. doi:10.1159/000518434
14. Mai W, Sun Y, Liu X, Lin D, Lu D. Characteristic findings by phototrichogram in southern Chinese women with Female pattern hair loss. Skin Res Technol. 2019;25(4):447–455. doi:10.1111/srt.12672
15. Loussouarn G, Lozano I, Panhard S, Collaudin C, El Rawadi C, Genain G. Diversity in human hair growth, diameter, colour and shape. An in vivo study on young adults from 24 different ethnic groups observed in the five continents. Eur J Dermatol. 2016;26(2):144–154. doi:10.1684/ejd.2015.2726
16. Rojhirunsakool S, Suchonwanit P. Parietal scalp is another affected area in female pattern hair loss: an analysis of hair density and hair diameter. Clin Cosmet Investig Dermatol. 2018;11:7–12. doi:10.2147/CCID.S153768
17. Khunkhet S, Chanprapaph K, Rutnin S, Suchonwanit P. Histopathological Evidence of Occipital Involvement in Male Androgenetic Alopecia. Front Med. 2021;8:790597. doi:10.3389/fmed.2021.790597
18. Sacha JP, Caterino TL, Fisher BK, et al. Development and qualification of a machine learning algorithm for automated hair counting. Int J Cosmet Sci. 2021;43(Suppl 1):S34–s41. doi:10.1111/ics.12735
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.