Back to Journals » Clinical Ophthalmology » Volume 14
Comparison Between Silicone Oil and Gas in Tamponading Giant Retinal Breaks
Authors Moharram HM ![]() , Abdelhalim AS, Hamid MA
, Abdelhalim AS, Hamid MA ![]() , Abdelkader MF
, Abdelkader MF ![]()
Received 8 November 2019
Accepted for publication 23 December 2019
Published 15 January 2020 Volume 2020:14 Pages 127—132
DOI https://doi.org/10.2147/OPTH.S237783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hossam Mohamed Moharram, Ahmed Shawkat Abdelhalim, Mohamed Abdel Hamid, Mohamed Farouk Abdelkader
Department of Ophthalmology, Faculty of Medicine, Minia University, Minia, Egypt
Correspondence: Mohamed Abdel Hamid
Department of Ophthalmology, Minia University Hospital, Minia 61111, Egypt
Email [email protected]
Purpose: The purpose of this study is to compare anatomical and visual outcomes after using silicone oil (SO) or C 3F 8 gas as tamponades after pars plana vitrectomy (PPV) for retinal detachment (RD) associated with giant retinal tears (GRTs).
Methods: A retrospective chart review was conducted for cases that underwent PPV for GRT-associated RD. We excluded eyes that had prior vitreoretinal surgery, a history of ocular trauma or worse than grade B proliferative vitreoretinopathy (PVR). Baseline demographic and ocular characteristics, surgical details and postoperative anatomical and visual outcomes were recorded and statistically analyzed.
Results: We included 88 eyes; 48 eyes had C 3F 8 gas and 40 eyes had SO as a tamponading agent. Mean age was 39 years. All eyes underwent 23G PPV with no adjuvant scleral buckling and phacovitrectomy was performed for all phakic eyes. Final retinal reattachment was achieved in 86 eyes (97.7%). One eye from each group had recurrent RD. Postoperative vision was significantly better in the gas group (p= 0.008). Prolonged increase of IOP developed in 6 eyes in the SO group and 5 eyes in the gas group. Prolonged uveitis developed in 4 eyes in the gas group and 6 eyes in the oil group (P= 0.04). Epiretinal membranes (ERM) developed in 10 eyes in the gas group and 9 eyes in the oil group. We found no significant difference between both groups regarding postoperative glaucoma or ERM formation.
Conclusion: Both agents achieved similar favorable anatomical outcomes in a series of eyes with fresh GRT-associated RD and low-grade PVR, with better visual outcome and less frequent uveitis associated with the use of gas tamponade.
Keywords: giant retinal tear, silicone oil, perfluoropropane gas, pars plana vitrectomy
Introduction
A giant retinal tear (GRT) is a full-thickness break of the neurosensory retina with a circumferential extent of at least 3 clock hours (≥90°) in the presence of a posterior vitreous detachment (PVD).1 A GRT is present in 1.5% of rhegmatogenous retinal detachments (RRDs). The annual incidence is estimated to be 0.05/100,000 of the general population per year.2 Pars plana vitrectomy (PPV), with or without adjuvant scleral buckling, is the current standard of care for RRDs secondary to GRTs.3 The introduction of heavy perfluorocarbon liquids (PFCLs) has facilitated surgical management of GRTs and increased the success rates from 58% to more than 90%.3,4
Several agents have been used for intraocular tamponade after PPV for GRT, including silicone oil, expansile gases, short or medium-term PFCLs and semifluorinated alkanes.1 To date, silicone oil remains the most frequent choice for endotamponade in such cases.5 Advantages include less incidence of intraoperative retinal slippage, ability to be left in situ for prolonged periods, reduced need for strict postoperative positioning and a well-established safety profile.6,7 Nevertheless, concerns exist about potential complications of its use and removal such as cataract, glaucoma, keratopathy and unexplained vision loss.8,9
The purpose of this study was to compare anatomical and visual outcomes of using silicone oil versus perfluoropropane (C3F8) gas endotamponade after PPV for GRT-associated retinal detachment.
Patients and Methods
This was a retrospective chart review of all cases that underwent primary PPV for GRT-associated RRD at the Department of Ophthalmology, Minia University, Egypt in the period between January 2015 and December 2018. Eyes that had prior vitreoretinal surgery, a history of ocular trauma or worse than grade B proliferative vitreoretinopathy (PVR) were excluded. A written informed consent was obtained from all patients prior to surgery. In patients under 18 years old the consent was signed by their legal guardian. Ethical approval was obtained from Research and Management Committee of the Faculty of Medicine, Minia University. The study adhered to the tenets of the Declaration of Helsinki.
Data collected included baseline demographic and ocular characteristics, surgical details, postoperative anatomic and visual results and the occurrence of any complications. Anatomical outcomes included the proportion of eyes achieving retinal reattachment at final followup after complete gas absorption or silicone oil removal, and the occurrence of any intraoperative or postoperative complications. Functional outcomes included the improvement in LogMAR BCVA after surgery in both endotamponade groups.
Statistical Analyses
The collected data were coded, tabulated and statistically analyzed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Parametric quantitative data were expressed as mean±standard deviation, non-parametric quantitative data as median and interquartile range (IQR), and categorical data as numbers and percentages. Distribution of data was done using Kolomogorov Smirnov test. Comparison between both study groups was done using Independent Samples t-test for parametric quantitative data and Mann Whitney test for non-parametric quantitative data. Analyses were done for qualitative data using Chi-square test (if <20% of cells had an expected count <5) and Fisher’s exact test (if >20% of cells had an expected count <5). P value <0.05 was considered significant.
Results
Baseline Characteristics
We included 88 eyes of 88 patients in our analysis. The mean age was 39 years (range: 12–61 years). Males constituted 54.5% of the study population (48 eyes) and 61.4% of eyes (54 eyes) were right eyes. Most breaks were inferior in location (56.8%) and ≤180° in extent (73.9%). High myopia > −6 D was found in 36 eyes (40.9%), while the rest of GRTs were idiopathic. Only 5 eyes were aphakic (5.7%), 15 eyes were pseudophakic (17%) and the remaining 68 eyes (77.3%) were phakic. Mean preoperative LogMAR BCVA was 1.8 (range: 0–3). Silicone oil was used in 40 eyes (45.5%) while C3F8 was used in 48 eyes (54.5%). Mean follow-up period was 14.3±2.6 months (Table 1).
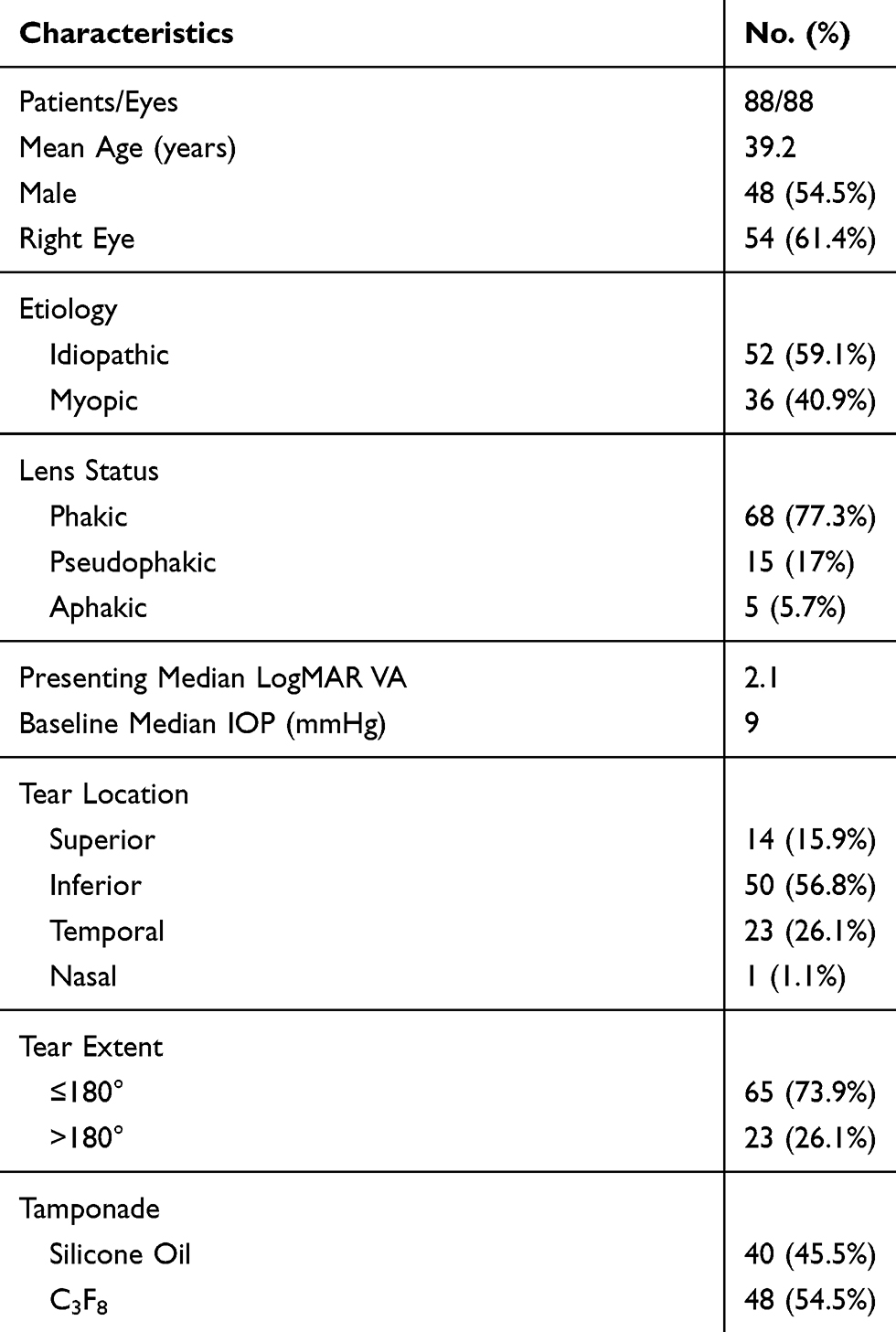 |
Table 1 Baseline Characteristics of the Entire Cohort |
Both tamponade groups were balanced regarding their baseline demographic and clinical characteristics, except for a significantly higher proportion of males in the silicone oil group (70% in silicone group versus 41.7% in gas group, p= 0.008) and a higher baseline intraocular pressure (9.5 mmHg in the silicone group versus 7 mmHg in the gas group, p=0.03) (Table 2).
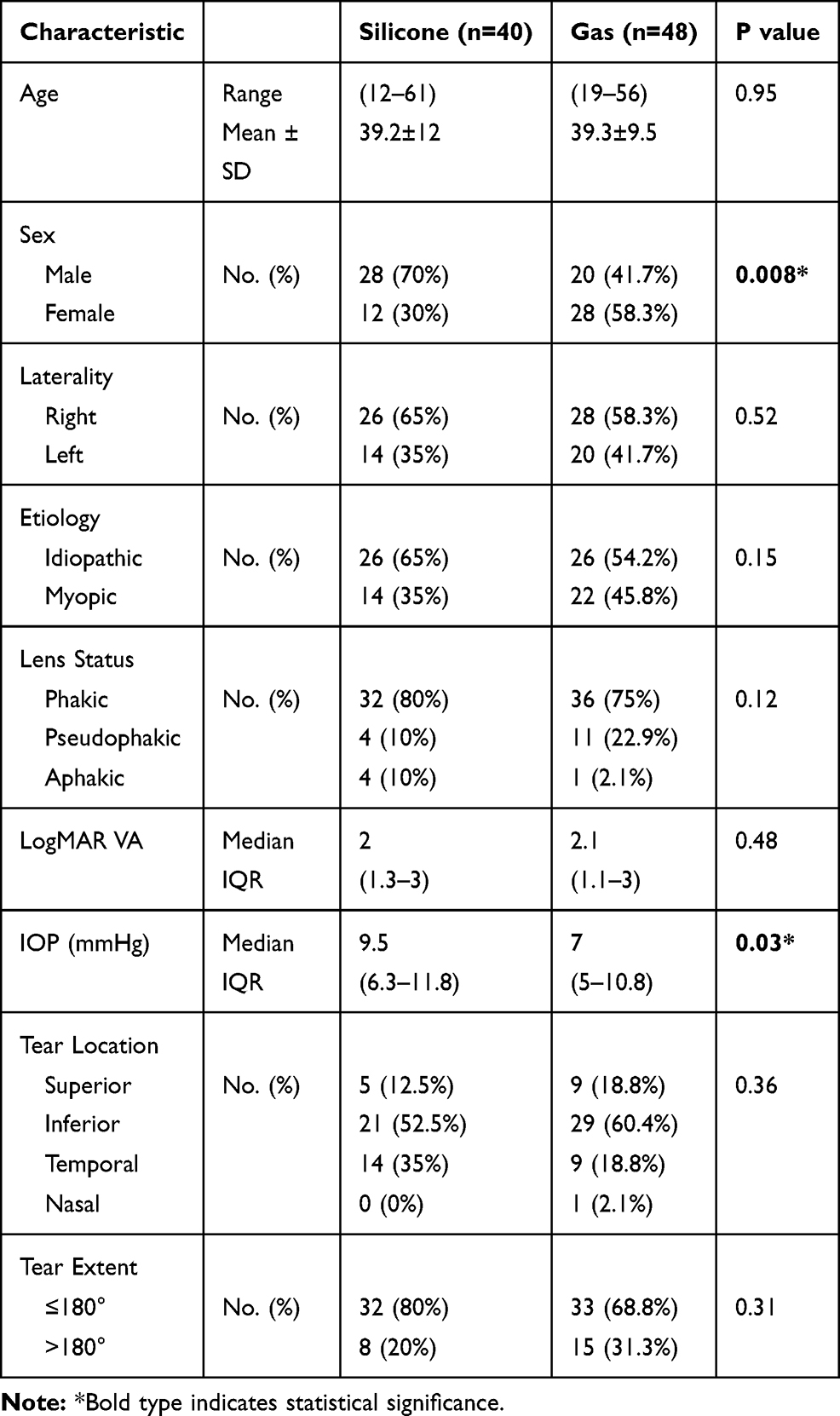 |
Table 2 Baseline Characteristics of Both Tamponade Groups |
Surgical Details
All phakic eyes underwent clear corneal phacoemulsification with single-piece foldable acrylic intraocular lens (IOL) implantation in the bag before starting vitrectomy. A 3-port 23-gauge PPV was performed for all cases. Adjuvant scleral buckling was not performed for any case. After core vitrectomy, PFCL was used to flatten the retina, followed by thorough base vitrectomy and excision of the anterior GRT flap using the vitreous cutter. Endolaser photocoagulation was applied to the posterior edge of the GRT extending anteriorly to the ora serrata and for 360° along the posterior edge of the vitreous base. At surgery conclusion, direct PFCL-silicone oil exchange or PFCL-air exchange and subsequent nonexpansile C3F8 injection (16% conc.) into the vitreous cavity was performed based on surgeon’s discretion. All eyes in the oil group received 2000 centistoke (cSt) silicone oil. Sutures were applied to leaky sclerotomies and whenever silicone oil was used. No serious intraoperative complications were encountered. Postoperative positioning was advised in the appropriate manner to keep the GRT supported by the endotamponade. Silicone oil was removed in all cases 3–6 months after surgery.
Anatomic Outcomes
Retinal reattachment was achieved in 86 eyes (97.7%) at last follow-up. Only 1 eye in the silicone group required a second surgery to achieve final reattachment, while the remaining 85 eyes had primary success. Two eyes were detached at final followup; 1 eye from each endotamponade group. Both eyes underwent subsequent PPV and silicone oil injection, but both redetached after silicone evacuation. Both patients declined further surgery (Table 3).
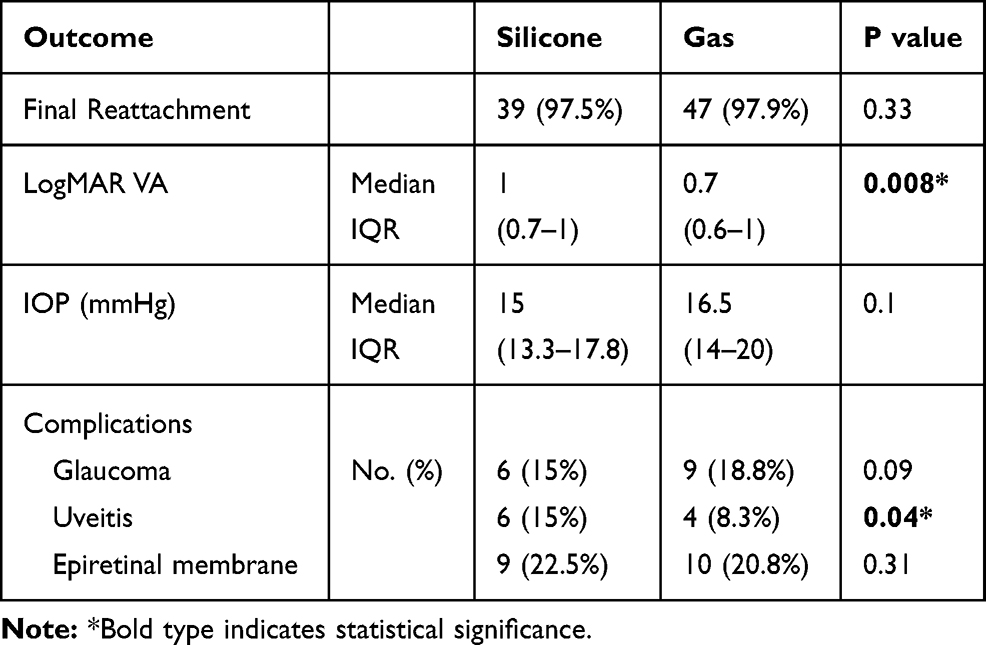 |
Table 3 Postoperative Outcomes of Both Tamponade Groups |
Mean IOP increased from 9.5 mmHg to 15 mmHg in the silicone group (p < 0.001) and from 7 mmHg to 16.5 mmHg in the gas group (p < 0.001). The mean postoperative IOP was within normal range in both groups without the use of antiglaucoma medications, except for 11 eyes that experienced sustained IOP elevation >21 mmHg. There was no significant difference in postoperative IOP between both groups.
Visual Outcomes
We found a significant improvement in LogMAR BCVA in both groups postoperatively. Median BCVA improved from 2.00 at baseline to 1.00 (p < 0.001) in the silicone group and from 2.1 to 0.7 in the gas group (p < 0.001). Postoperative vision was significantly better in the gas group (p= 0.008) (Table 3). Apart from the two eyes that were detached at final followup, which both ended with no light perception, no eyes experienced postoperative vision loss at final follow-up in either group compared to their preoperative vision.
Postoperative Complications
Sustained elevation of IOP > 21 mmHg developed in 11 eyes (12.5%) postoperatively. Nine eyes required antiglaucoma drops to control IOP postoperatively; 4 eyes (10%) in the silicone group and 5 (10.4%) in the gas group. Only two eyes required filtering surgery; both were in the silicone oil group (5%). Postoperative prolonged uveitis for more than 2 weeks developed in 4 eyes in the gas group (8.3%) and 6 eyes in the oil group (15%) (p= 0.04). Epiretinal membranes (ERM) developed in 10 eyes in the gas group (21%) and 9 eyes in the oil group (23%). ERM development was diagnosed clinically using slit-lamp biomicroscopy and diagnosis was confirmed using spectral-domain optical coherence tomography (SD OCT). We found no significant difference between both groups regarding postoperative glaucoma and ERM formation (Table 3). No emulsified silicone oil or retained subretinal PFCL droplets were encountered in any eye.
Discussion
Management of GRTs can be challenging due to difficulty in unrolling the posterior flap edge and high incidence of PVR.1,10 The advent of 3-port PPV has facilitated several aspects in the management of these cases. Primary retinal reattachment rates after PPV alone vary from 77% to 94% and final rates from 89% to 100%.4,11–13 Currently, 23-gauge is the standard modality for dealing with complex vitreoretinal cases.6 Recently, encouraging results have been reported for the use of small-gauge surgery in GRT repair, with success rates of 87–100%.14–17 Our success rate of 97.7% compares favorably with those results. Small-gauge surgery has the added benefits of less retinal mobility with more precision, decreased surgical trauma and postoperative inflammation, reduced sclerotomy complications and shorter surgical times. Management of GRTs with smaller gauges than 23G might be challenging due to instrument flexibility and difficulty reaching the ora serrata.2
The use of adjuvant scleral buckling is a matter of debate in the management of GRTs. Surgeons advocating the use of scleral buckles argue that a high circumferential indentation could counteract any future contraction of the vitreous base and, hence, decrease recurrence rates.18 Others are in favor of radical vitreous base removal without buckling in cases with no significant PVR to avoid potential buckle complications such as fishmouthing, tear slippage and choroidal hemorrhage.19–21 Posterior tear slippage is even more of a risk during fluid-air exchange.22 Addition of a scleral buckle was found to increase level 1 failure rates in the European Vitreo-retinal Society Retinal Detachment Study.5 Our results demonstrate a high success rate with standalone PPV in eyes with PVR grade B or less. This approach is consistent with global trends, as 93.5% of cases in the British Giant Retinal ear Epidemiology Eye Study (BGEES) were managed by PPV alone.12
Adequate base vitrectomy can result in intraoperative damage to the crystalline lens and/or supporting zonules.21,23 All phakic eyes in our study underwent lens removal at the time of PPV. We believe this is imperative in order to achieve thorough vitreous base removal, especially in the absence of a scleral buckle. We also performed prophylactic 360° laser photocoagulation in all cases to decrease the chances of recurrence. The literature suggests higher primary success rates for using prophylactic 360° laser photocoagulation, but to date, no randomized controlled trials have been conducted to support this claim.1,13,24
Silicone oil is the most commonly used intraocular tamponade in GRT surgery, mainly because it is thought to minimize intraoperative tear slippage and also because of the high risk of postoperative PVR in these cases.25 Although success rates reported by studies using silicone tamponade tend to be higher compared to outcomes of using gas tamponade, many studies reported final outcomes with silicone oil remaining in situ.7,26 This is important because redetachment rates of up to 14% have been reported after silicone removal.27–29 Eyes with retained silicone oil can develop maculopathy resulting in poor vision.30 Another concern is that silicone oil removal has been linked to an unexplained phenomenon of vision loss.31–33 The overall incidence of this phenomenon ranges from 3.3% to 5.9%.8,9 This incidence sharply increases to 50% in eyes with macula-on detachments.8 A higher preoperative IOP and longer tamponade duration were found to be associated with this phenomenon.9
We found no difference in anatomical success between the 2 tamponade groups at final followup. This comes in agreement with a recent retrospective noncomparative analysis conducted at the Bascom Palmer Eye Institute that found no difference in primary success or final vision between silicone oil and C3F8 tamponade after PPV for GRT.3 A randomized controlled study conducted by Batman et al demonstrated similar findings.30 On the other hand, the European Vitreo-retinal Society Retinal Detachment study found that silicone tamponade was associated with more cases of level 2 failure after GRT surgery compared to gas, while level 1 failure rates were similar between both groups.5 Several studies have shown a similar safety profile for both agents, with almost similar rates of complications such as cataract, secondary glaucoma, macular pucker and corneal abnormalities.30,34 Silicone oil use was associated with significantly more cases of uveitis in our study, which is similar to what Banerjee et al previously reported.25
Postoperative BCVA in our study significantly improved after surgery in both groups, concordant with previous studies,1 and vision was significantly better in the gas group. Recently, Banerjee et al retrospectively compared the use of silicone and gas tamponades in eyes with fovea-sparing GRT-related RRDs. About 49% of eyes who received silicone tamponade experienced vision loss compared to only 13% of eyes with gas tamponade. Final BCVA was significantly better in the gas group with fewer complications. Although eyes in the silicone group in their study tended to have more complex pathology, regression analysis identified tamponade choice as the only predictive factor for visual outcome. The most common cause for low vision in the oil group was unexplained vision loss after oil removal in 20% of eyes.25 In comparison, none of the eyes that achieved final reattachment in our study experienced vision loss. Eyes in both groups of our study were balanced regarding baseline clinical criteria and we excluded eyes harboring poor prognostic factors for visual recovery such as posttraumatic cases and eyes with prior vitrectomy or severe PVR.35,36 Of note, Banerjee et al studied exclusively macula-on detachments with good preoperative vision, while eyes included in our study all had macula-off detachments with poor preoperative vision.
Glaucoma is a common complication after surgery for GRT with an incidence of about 26%.25 Emulsified silicone oil is associated with the highest rate of postoperative IOP elevation, and this is why we removed the oil after 3–6 months in all our cases.37 Mean IOP significantly increased in both groups of our study, most likely as a result of successful retinal reattachment as retinal detachment is known to reduce IOP. Nine eyes required antiglaucoma drops and two eyes required filtering surgery to control IOP in our study. There was no significant difference in postoperative IOP between both groups, but the imbalance in preoperative IOP between both groups limits the validity of this finding.
In conclusion, gas tamponade achieved a similar attachment rate to silicone oil in a series of eyes with relatively fresh GRT-related RRDs. Eyes in the gas group had a significantly better postoperative BCVA and less frequent uveitis. Limitations of our study include its retrospective nature and relatively short follow-up period. Findings of our study may not be applicable for eyes with more severe PVR or a traumatic etiology. We advocate the use of gas in less complicated GRT cases to avoid potential vision loss that can be associated with silicone oil and to spare the patient a second surgery for silicone evacuation.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Shunmugam M, Ang GS, Lois N. Giant retinal tears. Surv Ophthalmol. 2014;59(2):192–216. doi:10.1016/j.survophthal.2013.03.006
2. Berrocal MH, Chenworth ML, Acaba LA. Management of giant retinal tear detachments. J Ophthalmic Vis Res. 2017;12(1):93–97. doi:10.4103/2008-322x.200158
3. Rodriguez M, Lin J, Townsend JH, et al. Giant retinal tears: clinical features and outcomes of vitreoretinal surgery at a university teaching hospital (2011–2017). Clin Ophthalmol. 2018;12:2053–2058. doi:10.2147/opth.s180353
4. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giant retinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol. 1989;107(5):761–766. doi:10.1001/archopht.1989.01070010779046
5. Adelman RA, Parnes AJ, Sipperley JO, Ducournau D. Strategy for the management of complex retinal detachments: the European vitreo-retinal society retinal detachment study report 2. Ophthalmology. 2013;120(9):1809–1813. doi:10.1016/j.ophtha.2013.01.056
6. Kumar V, Kumawat D, Bhari A, Chandra P. Twenty-five-gauge pars plana vitrectomy in complex retinal detachments associated with giant retinal tear. Retina. 2018;38(4):670–677. doi:10.1097/iae.0000000000001592
7. Mathis A, Pagot V, Gazagne C, Malecaze F. Giant retinal tears. Surgical techniques and results using perfluorodecalin and silicone oil tamponade. Retina. 1992;12(3 Suppl):S7–S10. doi:10.1097/00006982-199212031-00003
8. Moya R, Chandra A, Banerjee PJ, Tsouris D, Ahmad N, Charteris DG. The incidence of unexplained visual loss following removal of silicone oil. Eye (Lond). 2015;29(11):1477–1482. doi:10.1038/eye.2015.135
9. Roca JA, Wu L, Berrocal M, et al. Un-explained visual loss following silicone oil removal: results of the Pan American Collaborative Retina Study (PACORES) Group. Int J Retina Vitreous. 2017;3:26. doi:10.1186/s40942-017-0079-6
10. Schepens CL, Dobble JG, Mc MJ. Retinal detachments with giant breaks: preliminary report. Trans Am Acad Ophthalmol Otolaryngol. 1962;66:471–479.
11. Ambresin A, Wolfensberger TJ, Bovey EH. Management of giant retinal tears with vitrectomy, internal tamponade, and peripheral 360 degrees retinal photocoagulation. Retina. 2003;23(5):622–628. doi:10.1097/00006982-200310000-00003
12. Ang GS, Townend J, Lois N. Epidemiology of giant retinal tears in the United Kingdom: the British Giant Retinal Tear Epidemiology Eye Study (BGEES). Invest Ophthalmol Vis Sci. 2010;51(9):4781–4787. doi:10.1167/iovs.09-5036
13. Rofail M, Lee LR. Perfluoro-n-octane as a postoperative vitreoretinal tamponade in the management of giant retinal tears. Retina. 2005;25(7):897–901. doi:10.1097/00006982-200510000-00013
14. Kunikata H, Abe T, Nishida K. Successful outcomes of 25- and 23-gauge vitrectomies for giant retinal tear detachments. Ophthalmic Surg Lasers Imaging. 2011;42(6):487–492. doi:10.3928/15428877-20110901-01
15. Randolph JC, Diaz RI, Sigler EJ, Calzada JI, Charles S. 25-gauge pars plana vitrectomy with medium-term postoperative perfluoro-n-octane for the repair of giant retinal tears. Graefe’s Arch Clin Exp Ophthalmol. 2016;254(2):253–257. doi:10.1007/s00417-015-3049-4
16. Sigler EJ, Randolph JC, Calzada JI, Charles S. 25-gauge pars plana vitrectomy with medium-term postoperative perfluoro-n-octane tamponade for inferior retinal detachment. Ophthalmic Surg Lasers Imaging Retina. 2013;44(1):34–40. doi:10.3928/23258160-20121221-10
17. Zhang Z, Wei Y, Jiang X, Zhang S. Surgical outcomes of 27-gauge pars plana vitrectomy with short-term postoperative tamponade of perfluorocarbon liquid for repair of giant retinal tears. Int Ophthalmol. 2018;38(4):1505–1513. doi:10.1007/s10792-017-0613-4
18. Ie D, Glaser BM, Sjaarda RN, Thompson JT, Steinberg LE, Gordon LW. The use of perfluoro-octane in the management of giant retinal tears without proliferative vitreoretinopathy. Retina. 1994;14(4):323–328. doi:10.1097/00006982-199414040-00005
19. Freeman HM, Castillejos ME. Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc. 1981;79:89–102.
20. Hoffman ME, Sorr EM. Management of giant retinal tears without scleral buckling. Retina. 1986;6(4):197–204. doi:10.1097/00006982-198606040-00001
21. Kreiger AE, Lewis H. Management of giant retinal tears without scleral buckling. Use of radical dissection of the vitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology. 1992;99(4):491–497. doi:10.1016/S0161-6420(92)31942-6
22. Glaser BM. Treatment of giant retinal tears combined with proliferative vitreoretinopathy. Ophthalmology. 1986;93(9):1193–1197. doi:10.1016/S0161-6420(86)33597-8
23. Camacho H, Bajaire B, Mejia LF. Silicone oil in the management of giant retinal tears. Ann Ophthalmol. 1992;24(2):45–49.
24. Verstraeten T, Williams GA, Chang S, et al. Lens-sparing vitrectomy with perfluorocarbon liquid for the primary treatment of giant retinal tears. Ophthalmology. 1995;102(1):17–20. doi:10.1016/S0161-6420(95)31063-9
25. Banerjee PJ, Chandra A, Petrou P, Charteris DG. Silicone oil versus gas tamponade for giant retinal tear-associated fovea-sparing retinal detachment: a comparison of outcome. Eye (Lond). 2017;31(9):1302–1307. doi:10.1038/eye.2017.167
26. Leaver PK. Vitrectomy and fluid/silicone oil exchange for giant retinal tears: 10-year follow-up. Ger J Ophthalmol. 1993;2(1):20–23.
27. Aylward GW, Cooling RJ, Leaver PK. Trauma-induced retinal detachment associated with giant retinal tears. Retina. 1993;13(2):136–141. doi:10.1097/00006982-199313020-00008
28. Unlu N, Kocaoglan H, Acar MA, Sargin M, Aslan BS, Duman S. The management of giant retinal tears with silicone oil. Eur J Ophthalmol. 2003;13(2):192–195. doi:10.1177/112067210301300211
29. Zilis JD, McCuen BW
30. Batman C, Cekic O. Vitrectomy with silicone oil or long-acting gas in eyes with giant retinal tears: long-term follow-up of a randomized clinical trial. Retina. 1999;19(3):188–192. doi:10.1097/00006982-199905000-00002
31. Cazabon S, Groenewald C, Pearce IA, Wong D. Visual loss following removal of intraocular silicone oil. Br J Ophthalmol. 2005;89(7):799–802. doi:10.1136/bjo.2004.053561
32. Michel G, Meyer L, Naoun O. [Sudden visual loss following silicone oil removal: three patients treated for giant retinal tear]. J Fr D’Ophtalmologie. 2009;32(2):104–111. doi:10.1016/j.jfo.2009.01.003
33. Williams PD, Fuller CG, Scott IU, Fuller DG, Flynn HW. Vision loss associated with the use and removal of intraocular silicone oil. Clin Ophthalmol. 2008;2(4):955–959.
34. Al-Khairi AM, Al-Kahtani E, Kangave D, Abu El-Asrar AM. Prognostic factors associated with outcomes after giant retinal tear management using perfluorocarbon liquids. Eur J Ophthalmol. 2008;18(2):270–277. doi:10.1177/112067210801800216
35. Kertes PJ, Wafapoor H, Peyman GA, Calixto N
36. Scott IU, Murray TG, Flynn HW
37. Montanari P, Troiano P, Marangoni P, Pinotti D, Ratiglia R, Miglior M. Glaucoma after vitreo-retinal surgery with silicone oil injection: epidemiologic aspects. Int Ophthalmol. 1996;20(1–3):29–31. doi:10.1007/bf00212941
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.