Back to Journals » Drug Design, Development and Therapy » Volume 18
Comparison Between Esketamine and Alfentanil for Hysteroscopy: A Prospective, Double-Blind, Randomized Controlled Trial
Authors Weng M, Wang D, Zhong J, Qian M, Zhang K, Jin Y ![]()
Received 3 June 2024
Accepted for publication 5 August 2024
Published 14 August 2024 Volume 2024:18 Pages 3629—3641
DOI https://doi.org/10.2147/DDDT.S472651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Manfred Ogris
Mengcao Weng,1,* Dongdong Wang,2,* Jia Zhong,2 Minyue Qian,1 Kai Zhang,2 Yue Jin1
1Department of Anesthesiology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Anesthesiology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Jin, Department of Anesthesiology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, 3333 Binsheng Rd, Hangzhou, Zhejiang, 310052, People’s Republic of China, Tel +8613456912018, Email [email protected] Kai Zhang, Department of Anesthesiology, the First Affiliated Hospital, Zhejiang University School of Medicine, Wenyixi Road 1367, Hangzhou, 311121, People’s Republic of China, Tel +8615858281107, Email [email protected]
Purpose: This study aimed to establish the 95% effective dose (ED95) of esketamine in combination with propofol for hysteroscopy and then to evaluate its efficacy and safety profile.
Patients and Methods: This prospective, double-blind, randomized controlled trial consisted of two cohorts. In cohort 1, 45 women aged 18– 65 years undergoing hysteroscopy were randomly assigned to either group E (esketamine + propofol) or group A (alfentanil + propofol). Dixon’s up-and-down method was used to determine the ED95 of esketamine and alfentanil. In cohort 2, 86 patients were randomized to group E and group A, with the calculated ED95 dose of the study drugs used for induction. The success rate of anesthesia using the ED95% dose, along with parameters related to anesthesia induction, recovery, and adverse events were also recorded.
Results: The ED95 of esketamine was 0.254 mg/kg (95% CI: 0.214– 1.004), while that of alfentanil was 9.121 μg/kg (95% CI: 8.479– 13.364). The anesthesia success rate was 93.0% in group E and 95.2% in group A (p = 0.664). After resuscitation, both groups achieved a 100% success rate. The induction time was significantly shorter in group E (60.0 [55.0– 70.0] s) compared to group A (67.0 [61.0– 79.3] s) (p = 0.006). Group E had lower rates of respiratory depression (p < 0.001), hypoxia (p = 0.006), minimum perioperative SpO2 (p = 0.010), and hypotension (p = 0.001). Esketamine had less effect on respiratory rate, heart rate, mean blood pressure, and end-tidal carbon dioxide compared to alfentanil (all p < 0.001). There were no significant differences in postoperative pain between the two groups.
Conclusion: This study determined the ED 95 dose of esketamine for intravenous general anesthesia during hysteroscopy. Esketamine showed less respiratory and hemodynamic depression, as well as fewer adverse effects compared to alfentanil. Esketamine is an ideal anesthetic agent compared to alfentanil for hysteroscopic anesthesia.
Trial Registration: www.chictr.org.cn, (ChiCTR2300077283); registered November 3, 2023.
Keywords: esketamine, 95% effective dose, hysteroscopy, propofol
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Yang has been published for this article.
Introduction
With the increased awareness of endometrial lesions in women and the continuous advancement of hysteroscopic technology, the use of hysteroscopy in clinical practice has become increasingly common.1 Known for its minimal invasiveness and rapid recovery, hysteroscopy plays a critical role in the clinical diagnosis and treatment of gynecologic diseases. Despite being a minimally invasive procedure, hysteroscopy involves intraoperative cervical dilation, uterine scraping, and other invasive techniques that cause varying degrees of pain and discomfort to patients, leading to physiological and psychological distress. Currently, clinical anesthesia for hysteroscopic surgery is often involves the combination of propofol with opioids.2–4 These commonly used anesthetic drugs are known to cause significant respiratory and hemodynamic depression, as well as potential side effects such as nausea, and vomiting, sometimes necessitating the use of a laryngeal mask or intubation to assist breathing.5 Balancing the need for optimal analgesia level while the maintaining of respiratory and circulatory stability and promoting rapid postoperative recovery is a notable challenge in the field of clinical anesthesia for hysteroscopy.
Esketamine, a derivative of ketamine that targets N-methyl-D-aspartate (NMDA) receptors to induce sedation and analgesia, has emerged as a promising new option in anesthesia with favorable properties.6 Research suggests that esketamine results in rapid recovery from post-anesthesia, helps prevent the development of nociceptive hypersensitivity, and has minimal effects on respiratory function and hemodynamics.7,8 Currently, esketamine is increasingly being used for anesthesia induction and maintenance of anesthesia for pain management.6 In cesarean delivery, subanesthetic esketamine can provide additional analgesia and sedation, but does not induce significant neonatal depression.9 Other research has shown that esketamine can significantly reduce the risk of post-spinal hypotension during cesarean delivery.10 Compared to sufentanil, esketamine can reduce postoperative nausea and vomiting after thoracoscopic lung resection.11 However, the application of esketamine in hysteroscopy is relatively new. Information regarding the 95% effective dose (ED95) of esketamine in hysteroscopy, as well as its efficacy and safety profile, is currently lacking.
Alfentanil, a short-acting opioid known for its minimal effects on the respiratory and cardiovascular effects compared to other analgesics such as remifentanil and sufentanil, is widely used in clinical practice for its ability to reduce postoperative nausea and vomiting.12,13 Research has shown that in day surgery, alfentanil can reduce coughing and maintain more stable intraoperative hemodynamics during tracheal intubation under general anesthesia, as compared to sufentanil.13,14 In endoscopic retrograde cholangiopancreatography (ERCP), the combination of fentanyl with propofol may reduce spontaneous respiratory inhibition and the incidence of nausea when compared with remifentanil.12
Due to the aforementioned advantages of alfentanil in short surgical procedures, alfentanil was selected as the control to establish the efficacy and safety of esketamine in combination with propofol for intravenous general anesthesia during hysteroscopic procedures and to evaluate whether esketamine is the preferred choice for hysteroscopic anesthesia.
Materials and Methods
Study Design
The study was conducted as a single-center, double-blind, randomized controlled trial. The study was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (2023–114, October 31, 2023), and registered in the China Clinical Trial Registry (www.chictr.org.cn, No. ChiCTR2300077283, November 3, 2023). The study complies with the Declaration of Helsinki. Informed consent was obtained from all participating patients prior to enrollment. Patients, surgeons and the outcome assessors were blinded to the specific group assignments.
The study was divided into two phases: 1) Cohort 1 - dose-finding phase: aimed to determine the ED95 values for the anesthesia of esketamine and alfentanil in patients undergoing hysteroscopy; 2) Cohort 2 - safety and efficacy assessment phase: focused on evaluating the safety and efficacy of esketamine compared to alfentanil at the established ED95 dose.
Patients Eligibility
From November 2023 to January 2024, patients undergoing hysteroscopy were recruited into the study. Inclusion criteria were as follows: 1) patients aged 18–65 years; 2) American Anesthesiologists Association (ASA) physical status I or II; 3) modified Mallampati score ≤3; 4) body mass index (BMI) between 18 and 28 kg/m2. Exclusion criteria included: 1) allergy to anesthetics such as esketamine, opioids, and propofol; 2) cardiac (New York Heart Association cardiac function class 3 to 4, history of myocardial or cerebral infarction within 6 months, cardiac arrhythmia), pulmonary, hepatic, or renal dysfunction; 3) respiratory infection within the past 2 weeks; 4) uncontrolled hypertension; 5) hyperthyroidism; 6) diagnosis of epilepsy, or any psychiatric disorder; 7) history of dependence on analgesic or hypnotic substance; 8) use of benzodiazepines or opioids within the past 3 months; 9) participation in any other drug clinical trial within the past 3 months; and 10) patient refusal to participate in the study.
Dose-Finding
In this phase of the study, all patients underwent an 8-hour fast and abstained from fluids for 2 hours prior to the procedure. Patients were randomized to either the esketamine (E) group or alfentanil (A) group using a randomized table method. Upon arrival in the operating room, patients received oxygen at a rate of 3L/min via a mask. Vital signs, including blood pressure (BP), heart rate (HR), respiratory rate (RR), pulse oxygen saturation (SpO2), end-expiratory carbon dioxide pressure (PetCO2), and bispectral index (BIS) were routinely monitored. Microstream ETCO2 monitoring through the nasal catheter was used to monitor ETCO2.
An intravenous dose of 2 mg/kg propofol was administered intravenously, followed by esketamine (group E) or alfentanil (group A). Based on data from previous studies, the induction doses were set at 0.3 mg/kg esketamine (Jiangsu Hengrui Pharmaceuticals Co., Lianyungang, Jiangsu, China) for the group E and 10 μg/kg alfentanil (Yichang Humanwell Pharmaceutical Co., Yichang, Hubei, China) for the group A.15,16 The hysteroscopic procedure was started when the eyelash reflex disappeared and the modified observer’s assessment of alertness/sedation score (MOAA/S) reached 0–1. A continuous intravenous infusion of propofol at a rate of 4–8mg/kg/h was maintained throughout the procedure. If patients did not achieve adequate sedation, an additional dose of propofol (0.5mg/kg) was administered. If analgesia was insufficient, additional doses of 0.1 mg/kg esketamine or 5 μg/kg alfentanil were administered. The MOAA/S scale is used to describe deep sedation states and is scored from 5 to 0. It is widely used in anesthesia research.17,18 MOAA/S 5 represents a patient who is awake and responds readily to a name spoken in a normal tone; MOAA/S 0 means the patient does not respond to a noxious stimulus.19
Dixon’s up-and-down method was used to determine the ED95 of esketamine and alfentanil. Dixon’s up-and-down design is a classic method for studying the effective dose of an agent, in which the dose of a subject is determined based on the response of the previous subject.20,21 Any physical movement in response to cervical dilation was considered as a “failure”, otherwise it was considered as a “success”. If the patient failed, the next patient received an additional incremental dose on top of the original induction dose; conversely, if the patient succeeded, the next patient received a reduction of one incremental dose. The interval dose was set at 0.03 mg/kg in group E or 1 μg/kg in group A. In the Dixon method, the stopping rule requires at least 6 failure/success pairs.18,22 We decided to stop the study when there were 7 failure/success pairs in each group.
Safety and Efficacy Assessment
Preoperative preparation and monitoring procedures were identical to those used in the first phase of the study, with participants randomly assigned to either group E or group A using a randomized number table method. After induction with intravenous propofol at a dose of 2–3 mg/kg, group E received an ED95 dose of esketamine (0.25 mg/kg), while group A received an ED95 dose of alfentanil (9.12 μg/kg). Drug doses, HR, BP, RR, SpO2, and MOAA/S were recorded at several time points (T0: before induction, T1: immediately after induction, T2: 5 minutes after induction, T3: end of the procedure, T4: awakening/eye opening, and T5: 30 minutes after awakening). PetCO2 and BIS were also recorded at T0-T3. The awakening time and any adverse events were recorded.
If SpO2 falls below 95%, the oxygen flow rate is increased and airway is opened with a jaw thrust maneuver. If SpO2 falls below 90%, the patient receives pressurized oxygen through a face mask, with the possibility of laryngeal mask placement for ventilation if necessary. If hypotension occurs, the patient should receive fluid resuscitation or a dose of 6 mg ephedrine or 40 μg phenylephrine. If hypertension is diagnosed, intravenous administration of 10–25 mg urapidil is recommended. If the patient experiences bradycardia, 0.5 mg of atropine is administered. In case of tachycardia, esmolol at a dose of 0.5–1 mg/kg is administered by intravenous injection. For patients with nausea and vomiting, ondansetron at a dose of 4 mg is administered intravenously. For patients with mental symptoms, propofol at a dose of 0.5–2 mg/kg by intravenous injection or dexmedetomidine at a dose of 0.5–1 μg/kg by intravenous drip are recommended. These drugs can be repeated if necessary.
The propofol maintenance infusion was discontinued at the end of the hysteroscopic procedure. After surgery, all patients were transferred to the post anesthesia care unit (PACU). Pain levels were assessed using the Numeric Rating Scale (NRS) at T4 and T5. The NRS (NRS 0–10, where 0 is no pain and 10 is the worst pain imaginable) is a simple score that has been validated as a measure of postoperative pain intensity.23 In most research studies, an NRS score of ≥4 has been identified as the threshold for moderate pain. Pain relief was administered in the form of flurbiprofen axetil (50mg) when NRS score reached 3 points. For pain scores of 4 points or higher, intravenous fentanyl was administered at a dose of 1 μg/kg. Discharge from the PACU was assessed using the modified Aldrete score, with a score of ≥9 indicating eligibility for discharge.
Outcomes and Definitions
Primary Outcome
The ED95% of esketamine or alfentanil in combination with propofol for general anesthesia in hysteroscopic procedures was determined. In addition, the study evaluated the success rate of anesthesia using the ED95% dose of esketamine.
Secondary Outcome
Secondary outcomes included anesthesia induction, maintenance, recovery-related parameters, adverse events and satisfaction: 1) induction time: the time from the start of drug injection to the disappearance of the patient’s eyelash reflex and the achievement of the desired level of sedation (MOAA/S 0–1); 2) awakening time: the time from the end of anesthetic drug administration to when the patients opened their eyes; 3) cardiovascular or respiratory adverse effects: a) decreased respiratory rate: defined as a RR less than 8 breaths per minute; b) hypoxia: SpO2 level less than 90% lasting more than 1 minute; c) hypotension: MBP decreased more than 20% of the baseline; d) hypertension: MBP increased more than 20% of the baseline; e) bradycardia: HR decrease more than 20% of the baseline for 30s; f) tachycardia: HR increase more than 20% of the baseline for 30s; 4) other adverse reactions: injection pain, nausea and vomiting, headache, dizziness, postoperative psychiatric symptoms, shivering, and restlessness; 5) postoperative pain and analgesic requirements; 6) patient and surgeon satisfaction.
Statistical Analysis
ED95 was estimated using probit regression analysis with Statistical Analysis System (SAS, release 9.4). Sample size calculations were performed using PASS statistical software. Based on the literature reporting hypotension incidence rates of 6.2% and 21.5% during general anesthesia with esketamine and fentanyl combined with propofol (with hypotension being the highest percentage of adverse events),19,24 at a significance level of α=0.05, power of 1-β=0.8, with a 1:1 ratio between groups, and accounting for a 10% drop-out rate, a minimum sample size of 43 cases per group was required.
Normally distributed continuous data were presented as mean (standard deviation, SD), and analyzed using t-tests. Non-normally distributed data were presented as median (interquartile range, IQR) and analyzed using the non-parametric Mann–Whitney U-test. Categorical data were assessed using the chi-square test or Fisher’s exact test. Repeated-measures analysis of variance was used for comparisons of the RR, SpO2, HR, MBP, PetCO2 and BIS. Bonferroni correction was used for comparisons between groups. Statistical analyses were performed with SPSS 24.0 (IBM, USA) or GraphPad Prism 8 (GraphPad Software, USA). A P value less than 0.05 was considered statistically significant.
Results
Dose-Finding
Fifty-four patients were screened for eligibility in cohort 1. A total of 9 patients were excluded for the following reasons: 4 patients with BMI <18 or >28 kg/m2; 3 patients with ASA physical status > II; 2 patients refused. Finally, a total of 45 patients were enrolled in cohort 1, with 24 patients in group E and 21 patients in group A (Figure 1). There were no significant differences observed in age, gender, BMI, chronic diseases, alcohol consumption, ASA physical status, and duration of surgery between the two groups (Table 1). The individual responses to the two drugs, evaluated using Dixon’s up-and-down method, are shown in Figure 2. The calculated ED95 for esketamine and alfentanil were 0.254 mg/kg (95% CI: 0.214–1.004) and 9.121 μg/kg (95% CI: 8.479–13.364), respectively.
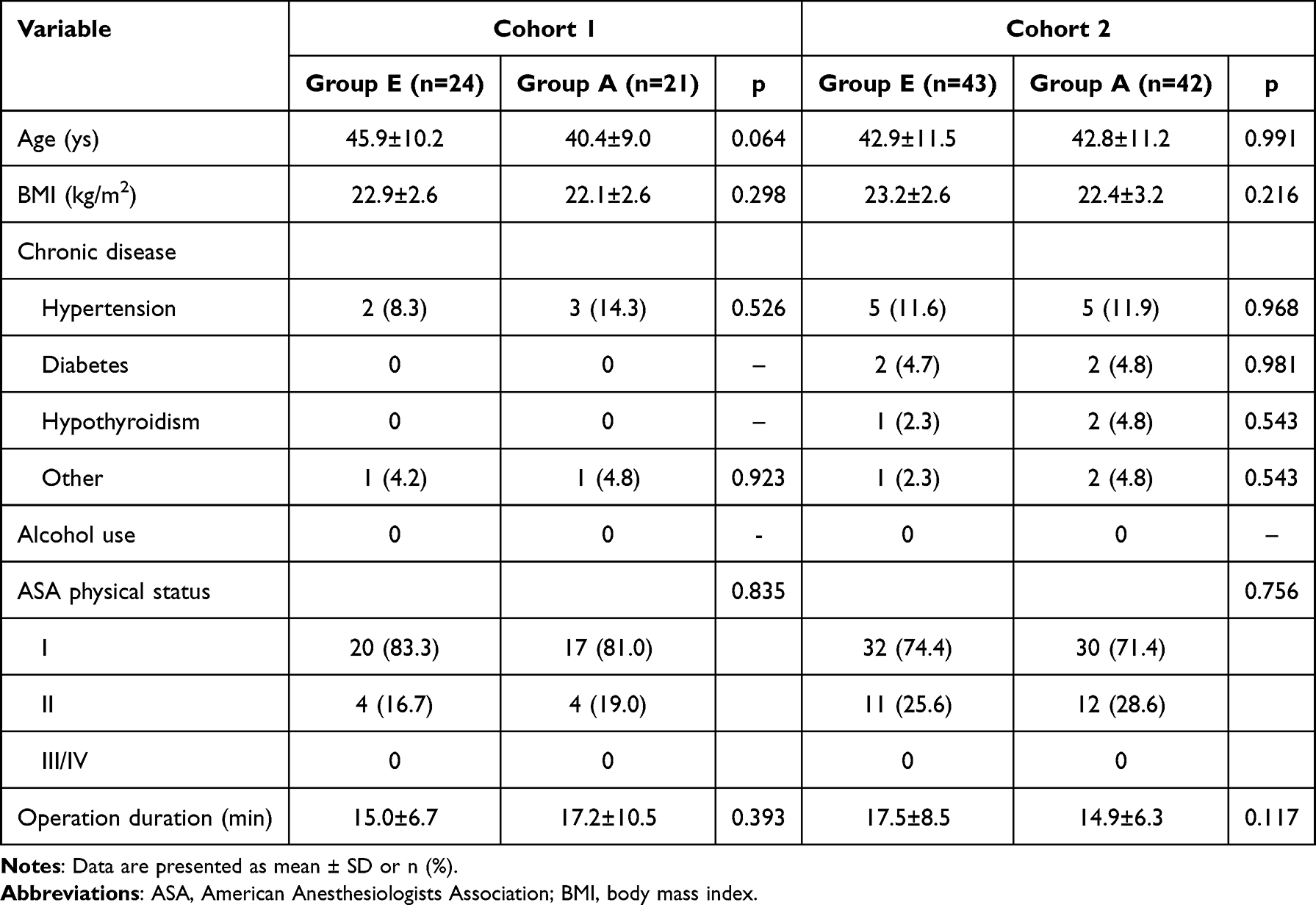 |
Table 1 The Basic Characteristics of the Patients |
 |
Figure 1 Flow diagram. |
 |
Figure 2 Dixon up-and-down plots for cohort 1. |
Safety and Efficacy Assessment
Patient Characteristics
In cohort 2, 91 patients were screened for eligibility. A total of 5 patients were excluded for the following reasons: 2 patients with BMI <18 or >28 kg/m2; 3 patients with ASA physical status > II. Ultimately, a total of 86 patients participated in the safety and efficacy evaluation using the ED95 dose. One patient was excluded due to a procedural change, resulting in the analysis of 85 patients (Figure 1). Patient characteristics, as shown in Table 1, did not differ significantly between the two groups with respect to age, gender, BMI, chronic medical conditions, alcohol use, ASA physical status, and duration of surgery.
Primary Outcome
Anesthetic success rates of anesthesia were 93.0% in group E and 95.2% in group A (p = 0.664). After rescue, both groups achieved a 100% success rate (Table 2).
 |
Table 2 Success Rate, Time Metrics and Propofol Consumption |
Secondary Outcome
Time Metrics and Propofol Consumption
Group E had a shorter induction time (60.0 [55.0–70.0] s) compared to group A (67.0 [61.0–79.3] s) (p = 0.006). However, the awakening time was longer in group E than in group A (time to eye-opening: 5.0 [3.0–7.0] min vs 4.0 [3.0–5.0] min, p = 0.033; time to respond to commands: 7.0 [4.0–8.0] min vs 5.0 [3.0–6.3] min, p = 0.032). There were no significant differences in the total propofol dose between the two groups (5.6±2.0 vs 5.2±1.1 mg/kg, p = 0.253) (Table 2).
Adverse Events and Hemodynamic Indexes
The incidence of respiratory depression was significantly lower in group E (16.3%) compared to group A (52.4%) (p < 0.001). A similar trend was observed for hypoxia (2.3% vs 21.4%, p = 0.006) and hypotension (4.7% vs 33.3%, p = 0.001). Although the bradycardia rate in group E (7.0%) was higher than the group A (2.4%), no significant difference was observed.
The RR, HR, MBP, SpO2 and PetCO2 at different time points are shown in Figure 3. Esketamine had a lesser effect on RR, HR, MBP and PetCO2 compared to alfentanil (all p < 0.001). RR was significantly lower in group A than in group E at time points T1, T2, T3, and T4. There were no statistically significant differences in SpO2 between the two groups at any time points. However, the minimum perioperative oxygenation saturation was higher in group E (95.5% ± 5.9%) than in group A (90.7% ± 10.0%) (p = 0.010). At T1, a statistical difference in HR was observed between the two groups (p < 0.05). MBP was significantly lower in group A than in group E at time points T1 and T2. PetCO2 levels were significantly lower in group E than in group A at time points T1, T2, and T3. In addition, BIS values were higher in the esketamine group than in the alfentanil group at both T2 and T3 (all p<0.05 after Bonferroni correction).
 |
Figure 3 Perioperative RR, SpO2, HR, MBP, PetCO2 and BIS levels. (A–F), mean values with error bars indicate standard deviation; (B), each point represents an individual. Significant differences were observed in RR, HR, MBP, PetCO2 and BIS levels between the two groups (p < 0.001). The variations in RR, SpO2, HR, MBP, PetCO2 and BIS levels changed over time (p < 0.001). *P < 0.05 after Bonferroni correction for inter-group comparisons. T0, before induction; T1, immediately after induction; T2, 5 minutes after induction; T3, end of the procedure; T4, awakening/eye opening; T5, 30 minutes after awakening. Abbreviations: BIS, Bispectral index; HR, heart rate; MBP, mean blood pressure; PetCO2, end-expiratory carbon dioxide pressure; RR, Respiratory rate; SpO2, Pulse Oxygen Saturation. |
In group E, the incidence of injection pain was 7 cases (16.3%), postoperative nausea was 3 cases (7.0%), dizziness was 15 cases (34.9%), and shivering was 1 case (2.3%). In group A, the incidence of injection pain was 7 cases (16.7%), postoperative nausea was 2 cases (4.8%), dizziness was 7 cases (16.7%), shivering was 1 case (2.4%), and restlessness was 1 case (2.4%). However, there was no statistically significant difference between the two groups. None of the patients experienced headache, vomiting, or other postoperative psychiatric symptoms. Both patient and surgeon satisfaction were high (Table 3).
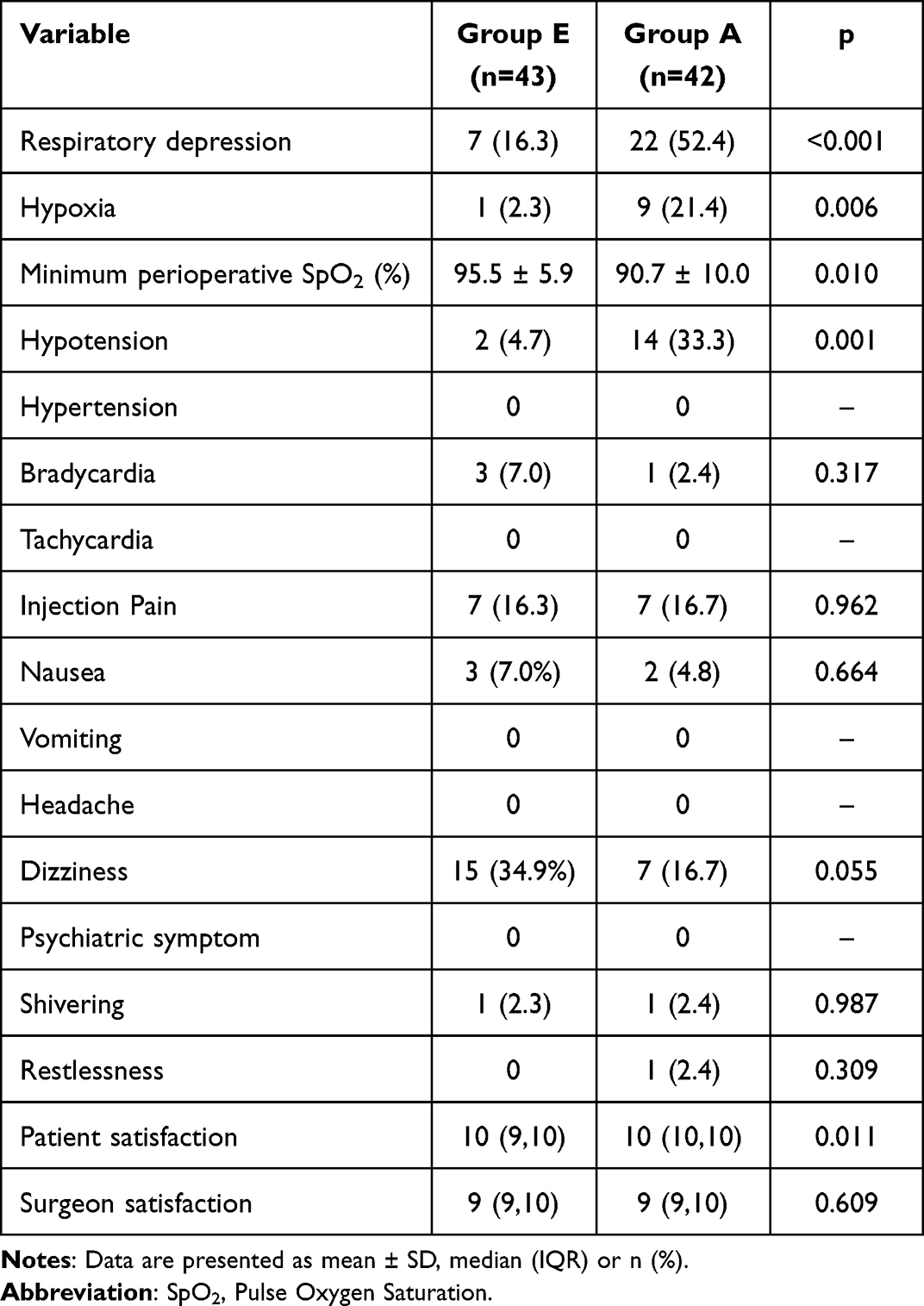 |
Table 3 Adverse Events and Satisfaction |
Postoperative Pain and Analgesic Requirements
The incidence of postoperative pain was 2.3% in group E and 2.4% in group A, with no significant difference between the two groups (p = 0.987). At time point T4, there was one patient in group E (2.3%) with an NRS score greater than or equal to 4. Furthermore, at time point T5, there was also one patient in group A (2.4%) with an NRS score greater than or equal to 4. However, there was no statistically significant difference in NRS scores between the two groups at these time points (all p>0.05). Additionally, the need for additional analgesics during PACU treatment was similar between the two groups (p>0.05), as shown in Table 4.
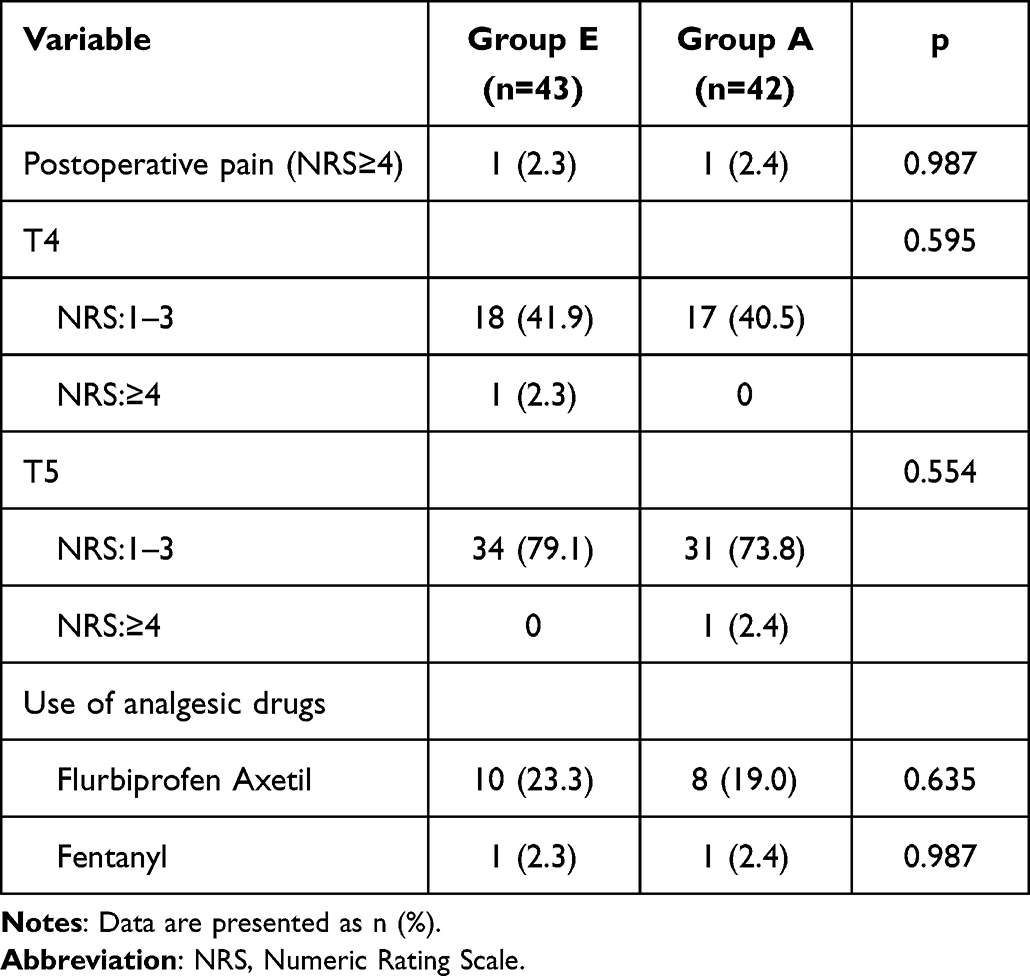 |
Table 4 Postoperative Pain and Analgesic Requirements |
Discussion
The study determined the ED95 values of esketamine and alfentanil in combination with propofol for hysteroscopic procedures and then evaluated their safety and efficacy profiles. The results indicate that the administration of esketamine at the ED95 dose with propofol for intravenous anesthesia can result in satisfactory anesthetic outcomes. Esketamine was associated with less respiratory depression, improved hemodynamic stability, and fewer adverse reactions compared to alfentanil. These results indicate that the combination of esketamine and propofol provides effective and safe anesthesia for hysteroscopy.
It is noteworthy that to date, no studies have specifically determined the ED95 value of esketamine in combination with propofol for hysteroscopic anesthesia. Previous research by Susanne Eberl et al used an esketamine dose of 0.15mg/kg for sedation during ERCP procedures,19 while Yongtong Zhan et al recommended an esketamine dose of 0.2mg/kg for sedation during gastrointestinal endoscopy.24 In our study, the determined ED95 dose of esketamine was 0.254mg/kg, which is similar to the doses reported in these studies. Differences in dosage may be due to differences in surgical requirements for analgesic dosage.
Esketamine, a novel anesthetic derived from ketamine, is known to cause less respiratory depression than to traditional opioid analgesics.25,26 Respiratory depression is a significant concern as it can contribute to serious postoperative adverse events,27 often associated with the use of opioid medications.28 Esketamine has been shown to increase CO2 sensitivity and improve ventilation. In addition, its effects on bronchial smooth muscle result in bronchodilation, which helps alleviate respiratory depression.29 In the current study, significantly fewer cases of respiratory depression were observed with esketamine compared to alfentanil during hysteroscopic procedures. This resulted in maintaining adequate oxygenation levels and potentially reducing the need for invasive procedures such as laryngeal mask insertion or tracheal intubation, thereby shortening recovery time and minimizing adverse reactions.
Furthermore, patients in the esketamine group exhibited more stable perioperative hemodynamics perioperatively when given the ED95 dose. Research suggests that esketamine may block sodium channels in brainstem parasympathetic neurons, inhibit electrical activity in cardiac parasympathetic nerves, and increase cardiac output.30 Additionally, esketamine inhibits norepinephrine uptake by neurons, resulting in increased norepinephrine levels, heightened sympathetic nerve excitation, and increased peripheral vascular resistance.30 These mechanisms counteract the cardiovascular depressant effects of propofol, thereby reducing cardiovascular risks associated with circulatory fluctuations.
Recent research has highlighted that esketamine increases depth of anesthesia and decreases anesthesia recovery time by shortening the peak activation time of PVT glutamatergic neurons.31 Similarly, in the current study, a shorter induction time was observed with esketamine compared to alfentanil, likely due to its ability of enhance depth of anesthesia. However, in this study, no advantage in recovery time was observed with esketamine, which may be due to the shorter duration of hysteroscopy procedures and the short-acting nature of alfentanil as an opioid. Although a slightly longer recovery time was observed in the esketamine group, this may not be clinically significant.
Despite advances in anesthesia techniques that improve the comfort of hysteroscopic procedures, some patients still experience postoperative pain that requires additional medication for relief.32 In this study, no significant difference in postoperative pain scores was observed between the two groups. Esketamine exerts potent analgesic effects by inhibiting NMDA receptors,33 with analgesic efficacy achieved at blood concentrations lower than those required for loss of consciousness.34 The current study also showed that the postoperative analgesic effects of esketamine were comparable to those of alfentanil.
Esketamine is known to have psychotropic side effects such as delirium, agitation, dizziness, nightmares, hallucinations, often in a dose-dependence manner.35,36 Studies have shown that subanesthetic doses of esketamine can reduce the incidence of these psychological symptoms,37 which is consistent with the results of our study. In this study, there were no significant statistical differences were found in dizziness, nausea/vomiting, or psychiatric symptoms between the two groups. This may be due to the use of subanesthetic doses of esketamine in the study. In conclusion, esketamine appears to be a safe option for hysteroscopic procedures.
Alfentanil has a lower impact on respiratory and circulatory function compared to other commonly used analgesics such as remifentanil and sufentanil.12,13 It is increasingly being used in endoscopy and day surgery.15,38 Previous research by Shu-An Dong et al used an alfentanil dose of 10μg/kg for analgesia during ERCP procedures,15 while Andrea L Y Yu et al recommended an optimal dose of 10μg/kg for alfentanil when co-administered with propofol for classic laryngeal mask insertion.39 These findings are consistent with the results of our study. However, esketamine demonstrated milder respiratory depression and more stable hemodynamics compared to alfentanil, suggesting the potential of esketamine as an ideal anesthetic option for hysteroscopic procedures.
In the current study, it was observed that BIS values in the esketamine group were higher than those in the alfentanil group, occasionally exceeding 60. Esketamine has the potential to induce widespread theta-wave activity and spike-wave activity on electroencephalography, resulting in elevated BIS values and interfering with neurophysiological monitoring.40 Therefore, it is important to note that BIS alone should not be used as an indicator of depth of sedation during esketamine anesthesia.
There are several limitations to this study. First, the sample size was relatively small, which may introduce potential statistical bias. Second, the study examined only on the analgesic effects of hysteroscopy, a procedure involving minor surgical trauma, and included only female patients, which limits the generalizability of the results. Finally, pharmacokinetic data, which would help to accurately characterize the dose-exposure-response relationship, were not collected. Therefore, future large-sample, multicenter prospective controlled studies are essential to confirm and further validate the findings of this study.
Conclusion
In conclusion, the study demonstrated that the combination of ED 95 dose esketamine and propofol for intravenous general anesthesia during hysteroscopy was effective, with reduced respiratory depression, improved hemodynamic stability, and minimized adverse effects. Esketamine is proving to be a good choice compared to alfentanil for hysteroscopic anesthesia.
Data Sharing Statement
The datasets used in the current study are available from the corresponding author (Yue Jin) upon reasonable request.
Ethical Approval
The study was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (2023-114, October 31, 2023) and registered in the Chinese Clinical Trial Registry (ChiCTR2300077283). Informed consent was obtained from all participating patients. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors thank the colleagues in the Department of Anesthesiology, and Department of Gynecology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National Natural Science Foundation of China (81971809, 82372159, 82072221), and Zhejiang Provincial Natural Science Foundation of China (LZ22H150002).
Disclosure
The authors report no conflicts of interest with respect to this work.
References
1. Fagioli R, Vitagliano A, Carugno J, Castellano G, De Angelis MC, Di Spiezio Sardo A. Hysteroscopy in postmenopause: from diagnosis to the management of intrauterine pathologies. Climacteric. 2020;23(4):360–368. doi:10.1080/13697137.2020.1754387
2. Ryu JH, Kim JH, Park KS, Do SH. Remifentanil-propofol versus fentanyl-propofol for monitored anesthesia care during hysteroscopy. J Clin Anesth. 2008;20(5):328–332. doi:10.1016/j.jclinane.2007.12.015
3. Lan H, Shan W, Wu Y, et al. Efficacy and Safety of Ciprofol for Sedation/Anesthesia in Patients Undergoing Hysteroscopy: a Randomized, Parallel-Group, Controlled Trial. Drug Des Devel Ther. 2023;17:1707–1717. doi:10.2147/DDDT.S414243
4. Qiu D, Wang XM, Yang JJ, et al. Effect of Intraoperative Esketamine Infusion on Postoperative Sleep Disturbance After Gynecological Laparoscopy: a Randomized Clinical Trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
5. Moharram EE, El Attar AM, Kamel MA. The impact of anesthesia on hemodynamic and volume changes in operative hysteroscopy: a bioimpedance randomized study. J Clin Anesth. 2017;38:59–67. doi:10.1016/j.jclinane.2016.06.023
6. Li X, Xiang P, Liang J, Deng Y, Du J. Global Trends and Hotspots in Esketamine Research: a Bibliometric Analysis of Past and Estimation of Future Trends. Drug Des Devel Ther. 2022;16:1131–1142. doi:10.2147/DDDT.S356284
7. Jonkman K, van Rijnsoever E, Olofsen E, et al. Esketamine counters opioid-induced respiratory depression. Br J Anaesth. 2018;120(5):1117–1127. doi:10.1016/j.bja.2018.02.021
8. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
9. Xu LL, Wang C, Deng CM, et al. Efficacy and Safety of Esketamine for Supplemental Analgesia During Elective Cesarean Delivery: a Randomized Clinical Trial. JAMA Network Open. 2023;6(4):e239321. doi:10.1001/jamanetworkopen.2023.9321
10. Zhang X, Wang J, An XH, et al. Optimum dose of spinal ropivacaine with or without single intravenous bolus of S-ketamine during elective cesarean delivery: a randomized, double-blind, sequential dose-finding study. BMC Preg Childbirth. 2021;21(1):746. doi:10.1186/s12884-021-04229-y
11. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
12. Mazanikov M, Udd M, Kylanpaa L, et al. Patient-controlled sedation for ERCP: a randomized double-blind comparison of alfentanil and remifentanil. Endoscopy. 2012;44(5):487–492. doi:10.1055/s-0031-1291655
13. Li H, Zhang H, Cheng Z, Ji H. Effects of alfentanil hydrochloride on cough and hemodynamics during induction of general anesthesia in daytime surgery. Minerva Surg. 2023;78(6):730–732. doi:10.23736/S2724-5691.21.09341-2
14. Xu Q, Zou X, Wu J, Duan G, Lan H, Wang L. Low-Dose Alfentanil Inhibits Sufentanil-Induced Cough During Anesthesia Induction: a Prospective, Randomized, Double-Blind Study. Drug Des Devel Ther. 2024;18:1603–1612. doi:10.2147/DDDT.S464823
15. Dong SA, Guo Y, Liu SS, et al. A randomized, controlled clinical trial comparing remimazolam to propofol when combined with alfentanil for sedation during ERCP procedures. J Clin Anesth. 2023;86:111077. doi:10.1016/j.jclinane.2023.111077
16. Zheng XS, Shen Y, Yang YY, et al. ED(50) and ED(95) of propofol combined with different doses of esketamine for children undergoing upper gastrointestinal endoscopy: a prospective dose-finding study using up-and-down sequential allocation method. J Clin Pharm Ther. 2022;47(7):1002–1009. doi:10.1111/jcpt.13635
17. Gan TJ, Berry BD, Ekman EF, Muckerman RC, Shore N, Hardi R. Safety evaluation of fospropofol for sedation during minor surgical procedures. J Clin Anesth. 2010;22(4):260–267. doi:10.1016/j.jclinane.2009.08.007
18. Wu X, Liao M, Lin X, Hu J, Zhao T, Sun H. Effective doses of ciprofol combined with alfentanil in inhibiting responses to gastroscope insertion, a prospective, single-arm, single-center study. BMC Anesthesiol. 2024;24(1):2. doi:10.1186/s12871-023-02387-4
19. Eberl S, Koers L, van Hooft J, et al. The effectiveness of a low-dose esketamine versus an alfentanil adjunct to propofol sedation during endoscopic retrograde cholangiopancreatography: a randomised controlled multicentre trial. Eur J Anaesthesiol. 2020;37(5):394–401. doi:10.1097/EJA.0000000000001134
20. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991;15(1):47–50. doi:10.1016/s0149-7634(05)80090-9
21. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
22. Ye E, Wu K, Ye H, et al. Comparison of 95% effective dose of remimazolam besylate and propofol for gastroscopy sedation on older patients: a single-centre randomized controlled trial. Br J Clin Pharmacol. 2023;89(11):3401–3410. doi:10.1111/bcp.15839
23. Gerbershagen HJ, Rothaug J, Kalkman CJ, Meissner W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: a cut-off point analysis applying four different methods. Br J Anaesth. 2011;107(4):619–626. doi:10.1093/bja/aer195
24. Zhan Y, Liang S, Yang Z, et al. Efficacy and safety of subanesthetic doses of esketamine combined with propofol in painless gastrointestinal endoscopy: a prospective, double-blind, randomized controlled trial. BMC Gastroenterol. 2022;22(1):391. doi:10.1186/s12876-022-02467-8
25. Ng J, Rosenblat JD, Lui LMW, et al. Efficacy of ketamine and esketamine on functional outcomes in treatment-resistant depression: a systematic review. J Affect Disord. 2021;293:285–294. doi:10.1016/j.jad.2021.06.032
26. Peltoniemi MA, Hagelberg NM, Olkkola KT, Saari TI. Ketamine: a Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy. Clin Pharmacokinet. 2016;55(9):1059–1077. doi:10.1007/s40262-016-0383-6
27. Laporta ML, Sprung J, Weingarten TN. Respiratory depression in the post-anesthesia care unit: mayo Clinic experience. Bosn J Basic Med Sci. 2021;21(2):221–228. doi:10.17305/bjbms.2020.4816
28. Weingarten TN, Sprung J. Review of Postoperative Respiratory Depression: from Recovery Room to General Care Unit. Anesthesiology. 2022;137(6):735–741. doi:10.1097/ALN.0000000000004391
29. Eikermann M, Grosse-Sundrup M, Zaremba S, et al. Ketamine activates breathing and abolishes the coupling between loss of consciousness and upper airway dilator muscle dysfunction. Anesthesiology. 2012;116(1):35–46. doi:10.1097/ALN.0b013e31823d010a
30. Kamp J, van Velzen M, Aarts L, Niesters M, Dahan A, Olofsen E. Stereoselective ketamine effect on cardiac output: a population pharmacokinetic/pharmacodynamic modelling study in healthy volunteers. Br J Anaesth. 2021;127(1):23–31. doi:10.1016/j.bja.2021.02.034
31. Ren S, Wang Y, Yue F, et al. The paraventricular thalamus is a critical thalamic area for wakefulness. Science. 2018;362(6413):429–434. doi:10.1126/science.aat2512
32. Riemma G, Schiattarella A, Colacurci N, et al. Pharmacological and non-pharmacological pain relief for office hysteroscopy: an up-to-date review. Climacteric. 2020;23(4):376–383. doi:10.1080/13697137.2020.1754388
33. Li J, Wang Z, Wang A, Wang Z. Clinical effects of low-dose esketamine for anaesthesia induction in the elderly: a randomized controlled trial. J Clin Pharm Ther. 2022;47(6):759–766. doi:10.1111/jcpt.13604
34. White MC, Karsli C. Long-term use of an intravenous ketamine infusion in a child with significant burns. Paediatr Anaesth. 2007;17(11):1102–1104. doi:10.1111/j.1460-9592.2007.02329.x
35. Zanos P, Moaddel R, Morris PJ, et al. Ketamine and Ketamine Metabolite Pharmacology: insights into Therapeutic Mechanisms. Pharmacol Rev. 2018;70(3):621–660. doi:10.1124/pr.117.015198
36. Jelen LA, Young AH, Stone JM. Ketamine: a tale of two enantiomers. J Psychopharmacol. 2021;35(2):109–123. doi:10.1177/0269881120959644
37. Han C, Ji H, Guo Y, et al. Effect of Subanesthetic Dose of Esketamine on Perioperative Neurocognitive Disorders in Elderly Undergoing Gastrointestinal Surgery: a Randomized Controlled Trial. Drug Des Devel Ther. 2023;17:863–873. doi:10.2147/DDDT.S401161
38. Zhang J, Liu R, Bi R, et al. Comparison of ciprofol-alfentanil and propofol-alfentanil sedation during bidirectional endoscopy: a prospective, double-blind, randomised, controlled trial. Dig Liver Dis. 2024;56(4):663–671. doi:10.1016/j.dld.2023.09.016
39. Yu AL, Critchley LA, Lee A, Gin T. Alfentanil dosage when inserting the classic laryngeal mask airway. Anesthesiology. 2006;105(4):684–688. doi:10.1097/00000542-200610000-00012
40. De Oliveira GS, Kendall MC, Marcus RJ, McCarthy RJ. The relationship between the Bispectral Index (BIS) and the Observer Alertness of Sedation Scale (OASS) scores during propofol sedation with and without ketamine: a randomized, double blinded, placebo controlled clinical trial. J Clin Monit Comput. 2016;30(4):495–501. doi:10.1007/s10877-015-9745-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.