Back to Journals » Medical Devices: Evidence and Research » Volume 18
Comparing Ultrasound, Chest X-Ray, and CT Scan for Pneumonia Detection
Authors Al Nufaiei ZF ![]() , Alshamrani KM
, Alshamrani KM ![]()
Received 18 October 2024
Accepted for publication 17 February 2025
Published 4 March 2025 Volume 2025:18 Pages 149—159
DOI https://doi.org/10.2147/MDER.S501714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ziyad F Al Nufaiei,1,2 Khalid M Alshamrani2,3
1Respiratory Therapy Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3Radiological Sciences Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia
Correspondence: Ziyad F Al Nufaiei, Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia, Email [email protected]
Background: The clinical methods of diagnosing pneumonia have been for many years chest X-rays (CXR) and computed tomography (CT) scans. However, a relatively new modality that is promising, efficient, and cheap is the lung ultrasound (LUS). The scope of this systematic review focuses on evaluating the diagnostic performance of LUS, CXR, and CT for diagnosing pneumonia.
Objective: The first aim of this review is to assess the diagnostic accuracy of lung ultrasound in comparison with chest X-rays and CT scans.
Methods: PubMed, Cochrane, Embase, and Scopus were electronically searched without date and language limitations were set. Inclusion criteria covered only those diagnostic studies that involved comparing lung ultrasound, chest X-ray, and CT scans in human beings with suspected pneumonia. Both abstraction and quality of studies were assessed by two researchers and the quality was assessed using PRISMA and QUADAS-2 checklists.
Results: There were 13 empirical studies included in the review which referred to different patients and contexts. Although none of the imaging techniques could achieve both high sensitivity and high specificity, CT scans produced the highest sensitivity, with values higher than 95% on all occasions, and specificities ranging between 80% and 90%. Lung US was most helpful in pediatric and acute care populations, whereas CT was preferred when there was uncertainty regarding the presentation.
Conclusion: Lung ultrasound is a very sensitive, specific, practical method of subsequent lung examination; it is useful in environments that need fast bedside assessment and for patients particularly vulnerable to radiation exposure, such as children. Even though chest X-ray remains valuable in excluding pneumonia in outpatient practices, it lacks sensitivity and is therefore less useful in diagnosing early disease. Computed tomography scans are the most accurate type of scans but should only be used in the more severe interventions due to cost and radiation exposure.
Keywords: CT scan, chest X-ray, ultrasound, pneumonia, critical care
Introduction
Pneumonia poses a significant global health threat, particularly affecting the elderly, infants, and individuals with compromised immune systems.1 To achieve early and adequate treatment, proper identification of pneumonia is therefore very important in preventing any complications that might arise. The routine investigations done in the diagnosis of pneumonia are CXR and CT scans which have been widely used as gold standards ever since they proved to be efficient and easy to obtain in the diagnosis of pneumonia.2 However, LUS has been discovered in recent years to be equivalent to conventional methods but is radiation-free and cheaper.3,4
Pneumonia has nonspecific manifestations and may range from mild respiratory signs to the development of severe respiratory failure and other systems manifestations. This variability often makes the diagnosis challenging, especially in the areas where there are few resources in form of CT scans and the like.5 diagnostic tools matter because underdiagnosis or misdiagnosis leads to the wrong treatment, prolonged hospital stay, and increased healthcare costs.6
The most utilized imaging technique in the diagnosis of pneumonia is Chest X-ray, a fast and non-invasive tool which offers details of the lungs. Chest x-ray images view the lungs, heart, and blood vessels and help to determine if the patient has pneumonia.7 However, it fails inaccurate test results, especially in early and slight changes that define pneumonia.8 Chest X-rays can also fail to demonstrate a consolidation or an interstitial pattern in an obese patient or a patient with chronic lung disease.9 Chest X-ray, however, has low test accuracy and cannot identify small lesions although CT scans can.10 However, due to augmentation of radiation dose, cost, and availability, CT scan is less preferable for the initial use, especially in children and pregnant mothers.11 LUS has emerged into the spotlight as a possible replacement or complementary tool to routine imaging for diagnosing pneumonia. Ultrasound utilizes high-frequency sound waves to form images of lung tissue that can help to detect specific patterns of pneumonia-like B-lines, consolidations and pleural effusion.12 It has been proved that LUS has an equal test result accuracy to chest X-rays and is even superior to CT scans in some cases, especially in recognizing consolidations and pleural diseases.13,14
LUS is particularly safe, as it does not require radiation exposure and can be safely used repeatedly in individuals who are sensitive to radiation, such as children and pregnant women.15 Thirdly, LUS can be done at the bedside making it possible to do quick assessments of the patient, especially in emergency or critical care conditions.16 This portability also comes in handy, especially in settings where there is a scarcity of resources to have other imaging techniques.9
Although LUS has been incorporated widely in clinical practice there are still concerns as far as diagnosis of pneumonia is concerned and its definitive role in comparison to conventional tools such as CXR and CT scans. The CT scan has the greatest effect on patients with an intermediate chance of illness and is particularly helpful in ruling out pneumonia. This diagnostic test correction may reduce the prescription of unnecessary antibiotics and enable prompt identification of the patient’s symptoms [The CT scan has the greatest effect on patients with an intermediate chance of illness and is particularly helpful in ruling out pneumonia. This diagnostic correction may reduce the prescription of unnecessary antibiotics and enable prompt identification of a different source of the patient’s symptoms.
Prior systematic reviews have mainly addressed the comparison of two interventions, most often LUS with C-XR.17 Yet, a comparative study incorporating all three modalities ultrasound, chest X-ray, and CT scan has not been adequately investigated. Such a comparison is necessary to determine the strengths and weaknesses of each modality and if it can be used to inform clinicians about the best approach in terms of the modality to use depending on the clinical indications, the patient and the available resources.3,8
This systematic review therefore seeks to help address this gap by comparing the diagnostic accuracy and efficacy of LUS, CXR, and CT in the identification of pneumonia in different populations. This review aims, therefore, at summarizing direct comparative evidence from relevant studies to give a clear and balanced picture of the various applications of each of the described imaging modalities and how these findings can be harnessed to enhance the currently available best practices in clinical management and decision-making processes leading to treatment of patients.
Methodology
The approach used in this systematic review is guided by a structured protocol that aims at identifying the diagnostic performance and efficiency of LUS, CXR, and CT in diagnosing pneumonia. It involves the formulation of a research question, an efficient search, criteria for the selection and rejection of articles, data abstraction, quality assessment of the studies, and synthesis of data.
Research Question and Objectives
The primary research question guiding this systematic review is: The questions to be answered include the following:
How effective and accurate is LUS in diagnosing pneumonia in terms of sensitivity, specificity, and general diagnostic performance compared to chest X-ray and CT scan in both adult and pediatric patients? (Table 1)
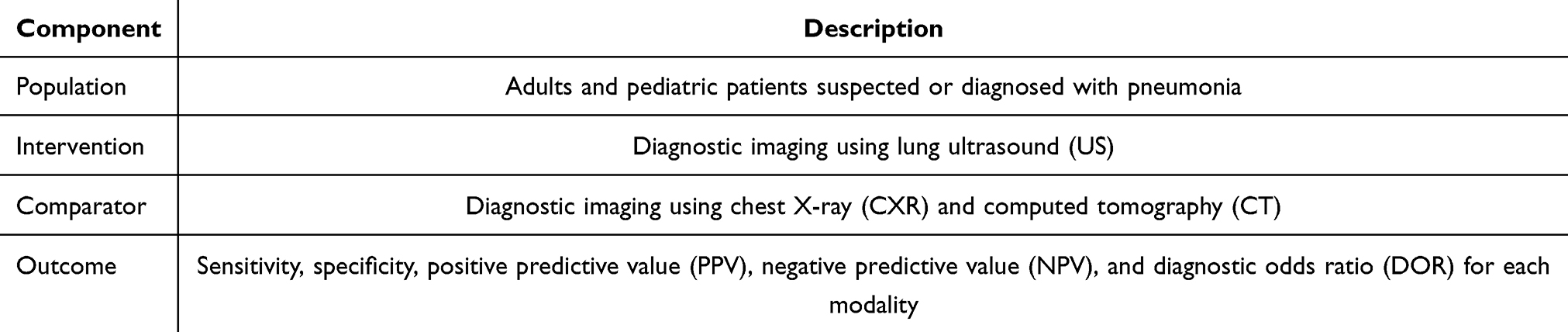 |
Table 1 PICO Framework for Research Question of Recent Study |
Search Strategy
To improve the validity of the obtained results, the Pubmed, Cochrane, Embase, and Scopus database search was carried out without restrictions concerning publication language or year of publication. To identify such articles, the following MeSH terms and free-text terms were used in the search strategy: pneumonia, LUS, chest X-ray, and CT scan. The “AND” as well as the “OR” operators were applied to make the search terms more specific and ensure that all deserving studies were identified. This was done to increase the specificity of the results for relevant publications while also being as comprehensive as possible in the amount of data available, in the time frame from the conception of the topic until the present. Also, the reference lists of all the articles and the relevant reviews included in this study were manually searched to identify any other study that may have been included.
Inclusion Criteria
Studies were included if they met the following criteria: Preference will be given to studies that include the following criteria: 1. investigations that employed original research and specifically compared at least one of the three imaging techniques (US, CXR, CT) used in diagnosing pneumonia; 2. human subjects of any age, although adult and/or pediatric subjects specifically; 3. include study designs like RCT, cohort, cross-sectional, case-control.
Exclusion Criteria
1. published as case reports, narrative reviews, and/or commentaries; 2. did not compare at least two of the modalities; 3. were conducted on animal models or cadaveric specimens; and/or 4. published in languages other than English.
Data Extraction and Quality Assessment
The data extraction process was conducted by two researchers independently without any intervention from other individuals, and a data extraction form with well-defined variables was used to minimize inter-observer variability. Potentially relevant data sources were the study characteristics such as author, date of publication, study type, and participants’ characteristics as well as diagnostic criteria for pneumonia, imaging techniques employed, and outcomes in relation to diagnostic performance including test accuracy, positive predictive value, and negative predictive value. In the event of a disagreement between the two reviewers, discussion was made, or a third reviewer was consulted. The quality of studies that were included in the systematic review was evaluated with help of PRISMA statement for systematic and meta-analyses and the QUADAS-2 tool which is used for evaluating the risk of bias and quality of diagnostic accuracy studies. These assessments were used to categorize the studies as low, medium, or high quality.
Data Synthesis and Analysis
The synthesis of data was conducted in both the qualitative and quantitative analyses. Next a qualitative synthesis was also done to do an analysis of all the studies that have been done on the different imaging modalities for diagnosis of pulmonary embolism, their diagnostic performance across different settings and in different patients. For the level one meta-analysis, the following criteria were planned before the analysis: If the overall variability between the studies appears moderate to low and when the underlying characteristics of the population, Study design, and types of outcomes are similar in all the identified Studies. This review focused on the sensitivity and specificity of each study, but the other secondary measures included positive predictive value (PPV), negative predictive value (NPV), and diagnostic odds ratio (DOR).
Study Outcomes
The frequency of each imaging modality (US, CXR, and CT) used was also considered as an index for evaluation and the two main estimated parameters were sensitivity and specificity of diagnosing pneumonia with usual imaging modalities. The second age-related endpoints were PPV, NPV, and DOR. These outcomes give a thorough appraisal of the diagnostic accuracy of both the testing modalities and can easily be used for comparison of the effectiveness of the two in various clinical situations.
Ethical Considerations
Since the present study is a systematic review, it did not require direct interaction with people or the use of unpublished and/or sensitive data. Therefore, it was not necessary to seek ethical clearances. However, every endeavor was made to uphold the principles of ethical research such as, the process of reporting the findings of the study, declaration of the kind of conflict of interest, if any, and giving credit to the original authors of the studies used in the research.
Results
Study Selection
The PRISMA standards were followed in a recent systematic review to select and screen research papers relevant to the study’s objectives, which focused on “Ultrasound, Chest X-Ray, and CT Scan in Detecting Pneumonia.” In total, 1175 research articles were extracted using this search approach from electronic databases (Figure 1). Just 562 papers were examined using the PRISMA procedures, while 613 articles were disqualified prior to screening. Only those papers were evaluated for eligibility, and 13 research articles remained after exclusion criteria were applied. As shown in (Table 2), 13 papers were included in the most recent systematic review since they satisfied the inclusion criteria. These 13 included studies provided a population of 2719 male and female patients whose ages ranged from 2 to 83 years old. In terms of the clinical setting a total of 7 studies were conducted in adult patients admitted to ED, 3 studies included patients admitted to ICU,2 studies Pediatric department, and one in the geriatrics department. Only 4 studies reported that the operators were trained or licensed operators (Table 3).
 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram illustrating the studies’ selection process. Notes: This figure was adapted from Page MJ, McKenzie JE, Bossuyt PM, et. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. Creative Commons.18 *The studies were identified from the databases. ** The studies were excluded after the initial screening. |
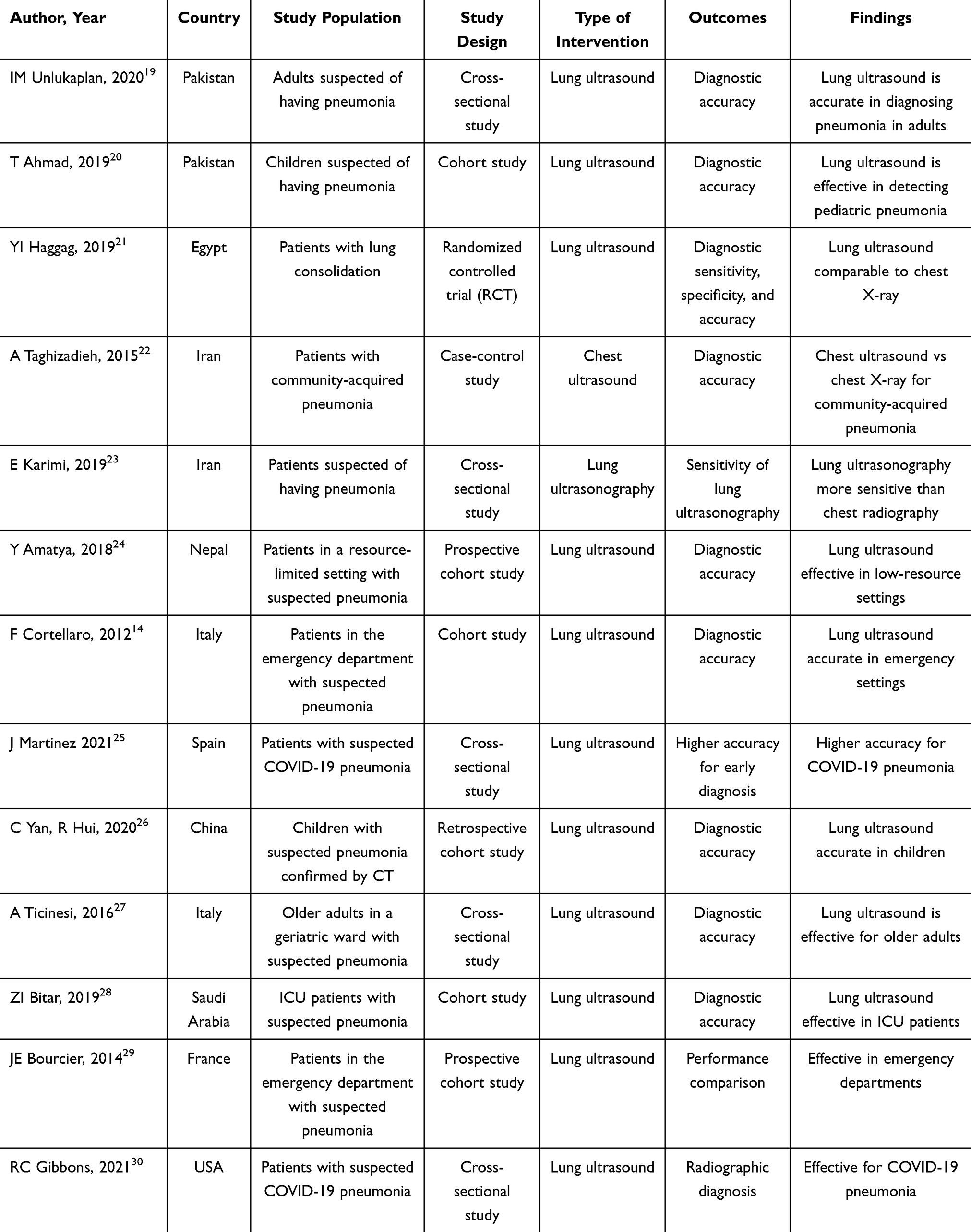 |
Table 2 Characteristics of Included Studies |
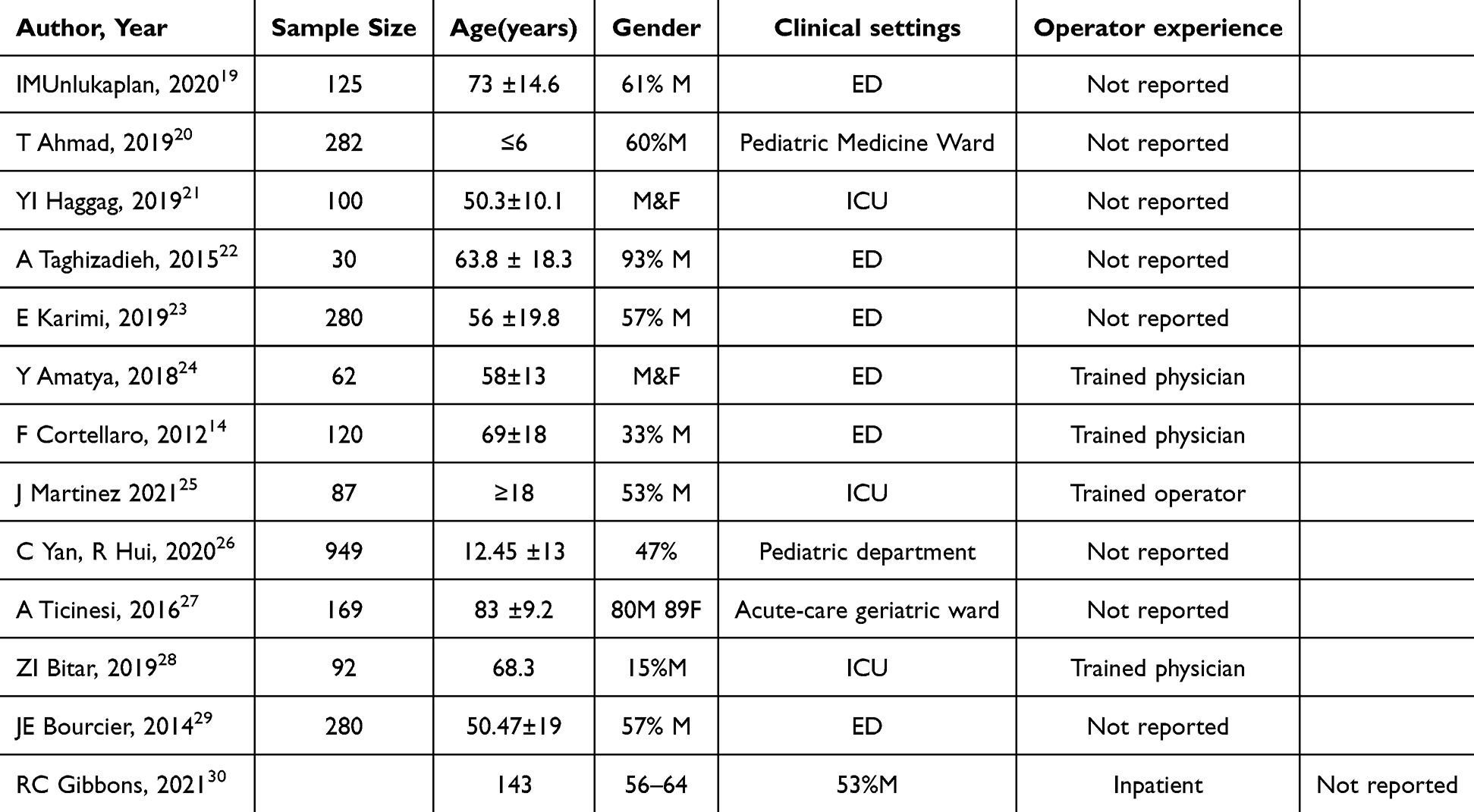 |
Table 3 Characteristics of Enrolled Patients and Their Clinical Settings |
Quality Assessment and Risk of Bias
Table 4 presents a risk of bias assessment using the QUADAS-2 tool, which evaluates the quality of diagnostic accuracy studies. The studies listed in the table generally show low risk across four key domains: patient selection, index test, reference standard, and flow and timing. This consistent low-risk rating across all categories indicates that the studies included were designed and conducted with minimal bias. Thus, the findings from these studies can be considered reliable for assessing the diagnostic accuracy of LUS, chest X-ray, and CT in detecting pneumonia.
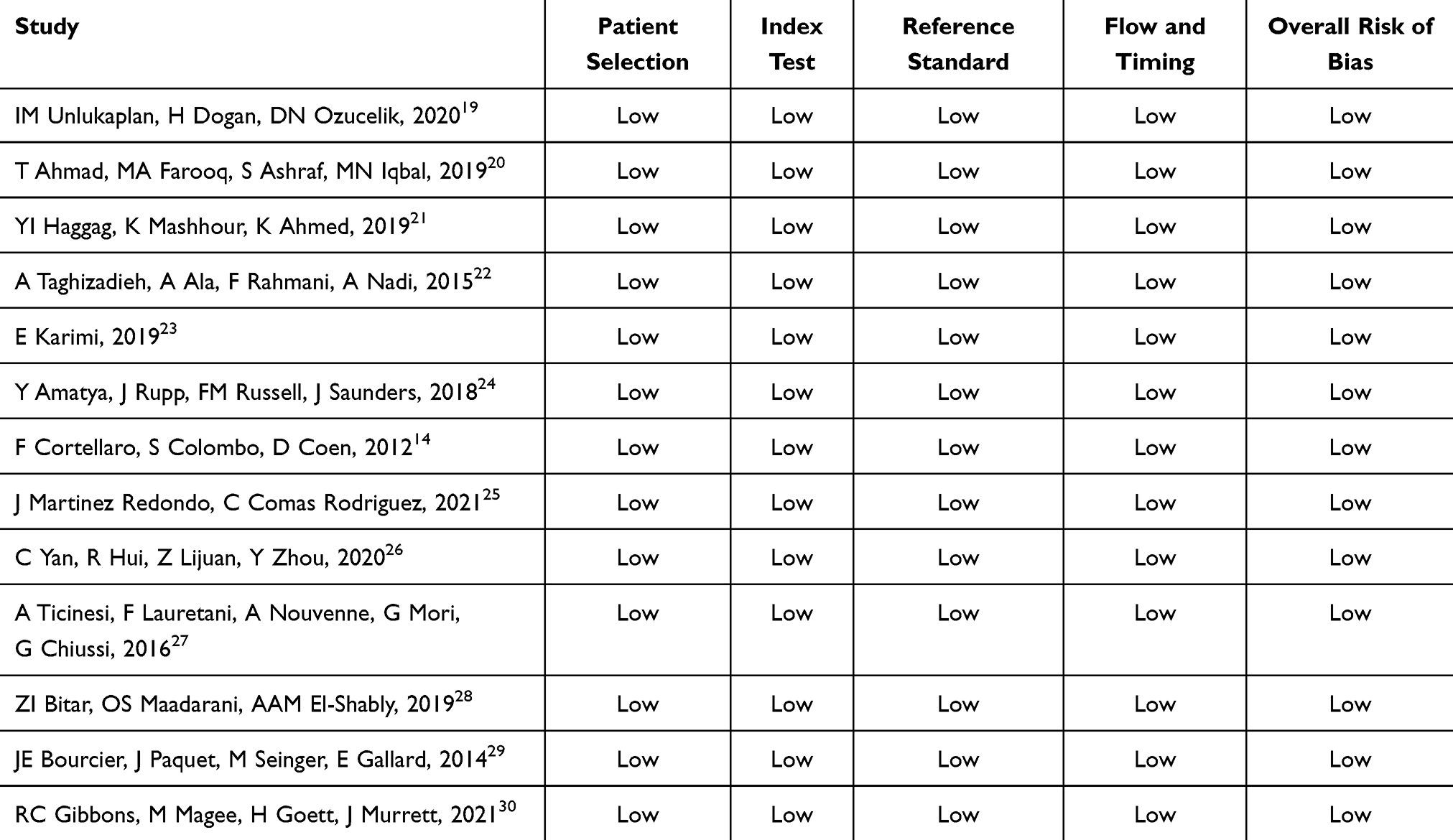 |
Table 4 Risk of Bias Assessment Using Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) Tool |
Outcome of Ultrasound, Chest x-Ray, and CT Scan in Detecting Pneumonia
The test results of the three imaging methods showed different sensitivity and specificity functions. Another study on LUS showed that their sensitivity ranges from 86% to 98% thus making it useful in indicating cases of pneumonia. Recognizing that this modality was most useful in situations where quick, at-the-bedside evaluation is feasible also ruled helpful. The sensitivity of LUS varied from 85% to 95%, which reflected the ability of LUS to accurately rule out pneumonia. One advantage is felt in acute care situations and especially within conditions of resource constraint.
Chest X-ray however produced comparatively lower sensitivity in the range of 70%-85%. This implies that chest X-ray is not very accurate in diagnosing pneumonia especially since the test was carried out on patients who had early signs of pneumonia. On the other hand, chest X-ray has adequate specificity that ranges from 80% to 90%, therefore, indicating the effectiveness of chest X-ray to eliminate pneumonia, while the modifications have low test accuracy in detecting early or mild pneumonia.
CT scans had the highest diagnostic accuracy out of the three different types reaching or surpassing 95% accuracy which makes CT scans the most accurate modality in diagnosing pneumonia, especially in complicated cases wherein other methods may give way to ambiguous results. This. An option also showed high specificity of CT scans, which was usually higher than 90%, which facilitates proper assessment of pneumonia and other pulmonary pathologies.
It also extended the evaluation of these imaging strategies to a more detailed comparison of their performance within various clinical contexts and patients. In parallel, investigation of LUS for adult and pediatric patients revealed a higher efficacy of the former in the latter group including atypical presenting pneumonia and the cases when radiation should be limited. Regarding clinical settings, there was a preference for lung ultrasound in inpatient settings including critical care areas since it is portable and allows for quick examination. Regarding the outpatient criteria, the utilization of chest X-ray and CT scans was quite different, notably the HITN study always involved chest X-rays, however, the utilization of CT scans differed by the availability of equipment and the clinical suspicion of pneumonia.
Discussion
This systematic review presented present study’s data reveal an overview of the diagnostic performance and efficacy of lung US, CXR, and CT in identifying pneumonia in various settings and population samples. The data reported by the present study reveal little uniformity in the efficacy of these imaging techniques as a function of their application.
Diagnostic Accuracy of Lung Ultrasound (LUS)
Lung US across the studies included in this review had a high sensitivity that ranged between 86% and 98% and high specificity that ranged between 85% and 95%. This implies that the US is highly effective in the diagnosis of pneumonia especially where there is a need to quickly assess a patient at the bedside. This high sensitivity is because of the high ability to detect pleural effusions and lung consolidations which are characteristics of pneumonia. This is in concordance with other studies done by Alzahrani et al 2017 which showed that LUS has high sensitivity and specificity in the diagnosis of pneumonia, especially in resource-poor countries.31 Further, Cortellaro et al (2012) observed that lung ultrasound gives several advantages in emergency procedures since it entails faster execution, unlike the conventional techniques that involve radiation.14
Though its diagnostic accuracy has shown to be high depending on the type of pleural abnormality, the method can be heavily dependent on the experience of the scanner and place of practice. Observations have revealed that experience level does influence the curve, and that lung ultrasound may have consequences on the diagnostic results among the less qualified personnel.5 Nevertheless, lung ultrasonography can be effective in different clinical contexts such as intensive care units and pediatrics because of its noninvasive nature and lack of radiation effect.29
Diagnostic Accuracy of Chest X-Ray
The chest X-ray (CXR) is used routinely in the diagnosis of pneumonia and the sensitivity varies from 70% to 85% and the specificity from 80% to 90%. These outcomes received correlation with research by Haggag et al (2019) noting that chest X-ray is less effective than lung ultrasonic in early-stage pneumonia identification but stays helpful to exclude the disease.21 The lower sensitivity of CXR may perhaps be linked to the use of this technique being less capable of detecting small and early consolidations and the dependence on the radiologist’s qualitative evaluation of the images.24 This is a significant limitation, especially when there are unusual features of typical pneumonia or when pneumonia may be associated with another pulmonary disease and this may cause confusion in the distinction.28
Similarly, Cp in a study by Ticinesi et al, (2016) was lower than that of CT scans for complicated cases of pneumonia but CXR stays as the most economical and feasible approach to the diagnosis of OP among outpatients.27 Second, CXR is relatively available and more independent of radiologists’ interpretation since clinicians with even basic radiology knowledge can also easily interpret the CXR image.26
Diagnostic Accuracy of Computed Tomography
This study confirmed previous studies that CT was the most accurate of the three providing high sensitivity which is often over 95% and specificity of over 90%. This makes CT the best reference tool when diagnosing pneumonia, particularly the complicated ones for which other imaging methods are inconclusive.31 CT scans are more diagnostic in diagnosing pulmonary diseases as compared to other imaging techniques because it provide high-resolution images of the lung parenchyma hence enhancing the visualization of small pulmonary changes.32
The current study has been further buttressed by other studies as regards to the high sensitivity and specificity of CT scans. For example, Gibbons et al cited that in a study they conducted in 2021, they were able to determine that CT scans proved to be much more accurate when used in distinguishing pneumonia from other lung conditions including pulmonary embolism or lung cancer. However, the utility of CT is somewhat restricted by its cost, the associated radiation dose, and availability in many centers especially in developing countries.22 Moreover, there is the misuse of CT in cases in which less invasive techniques such as US or CXR could be sufficient for diagnostic purposes despite the fact that radiation exposure is a possible risk for personal damage, especially in pediatric patients.25 However, It has been suggested that there are possibilities of a false positive reading of radiology images in diagnosing pneumonia in patients with other medical conditions, such as congestive heart failure or pulmonary fibrosis when using X-ray or Lung adenocarcinoma or pulmonary siderosis when using CT-scan and atelectasis when using ultrasound [A case of pulmonary siderosis misdiagnosed as pneumonia, CT-scan and X-ray.32
Comparison With Other Studies
The results of this systematic review correlate with prior research on the diagnostic performance of imaging techniques in pneumonia. For instance, another meta-analysis study by Alzahrani et al (2017) acknowledges that LUS was highly sensitive and specific and that more so in children since they are receptive to ionizing radiation.33 A similar observation was made by Lichtenstein & Mezière, 2008 who observed that lung USG was more sensitive than the chest X-ray in identifying lung consolidations and pleural effusion which are signs of pneumonia.5 Nevertheless, Martinez Redondo et al, 2021 like Bitar et al, 2019 have revealed that the accuracy of chest X-rays is questionable, especially in cases of early or atypical pneumonia manifestations. These and other related research highlight the need for other imaging techniques like CT in complicated cases, which require precise diagnosis. This is in agreement with Ye et al (2015) and Balk et al (2018) who identified that CT scans are 97% sensitive and 96% specific in diagnosing pneumonia, especially in critical patients.28,31
Implications for Clinical Practice
The implications of this evidence as derived from this systematic review are of significant value to clinical practice. On account of the high sensitivity and specificity of LUS, it is a useful modality in different clinical contexts, especially in patients in acute care and pediatric patients where speed and limitation on the use of radiation are desirable. The study also indicates that the chest X-ray, while less sensitive than LUC, can be used for initial evaluation and to rule out the presence of pneumonia in outpatients. However, it lacks sensitivity in early-stage pneumonia; this makes other imaging modalities useful in some clinical situations.
Although CT has better diagnostic specificity, it should be only used for the cases in which other imaging studies are non-diagnostic or in situations where there is a need to analyze the extent of lung disease in detail. Because of the cost and radiation risk associated with the usage of CT scans, their application should be appropriate with special consideration to children and areas of low individuality. Therefore, the decision of which imaging modality to use should encompass the clinical scenario that patients are in, the population, which is being served, and the resources available to enhance the diagnostic yield and therefore the patients’ outcome. Future research study should try to provide a more concrete definition of pneumonia and examine the applicability of diagnostic parameters that make use of high-end imaging systems including artificial intelligence-based imaging.
Limitations of the Study
The study’s weaknesses are multi-dimensional. These include: One limitation is that only the articles in English were considered rather than all articles, which could lead to bias. Also, the quality and methodologies used in the studies range from good to poor and hence greatly influence the efficiency and credibility of the results. There is concern that the specificity claimed across different clinical areas contributes to conclusion variability thus complicating generalizability of the results. Only patients with pneumonia are included, which makes it easy to generalize the findings, yet the primary limitations to the generalization of these results are differences in patient populations, clinical settings, and the experience of the clinicians. Clinically, this could be addressed by standardizing the radiology procedures and providing clear guidelines. Moreover, different image modalities have been adopted in the various studies making comparison challenging due to the leading contexts in which they were taken and the level of expertise of the clinicians who undertook the imaging interpretation. This variability may influence the results obtained as to the efficiency and reliability of LUS, chest X-ray, and CT scans in diagnosing pneumonia.
Conclusions
This systematic review aims to summarize the diagnostic performance as well as the efficacy of lung US, CXR, and CT scans in diagnosing pneumonia. The results indicate that there are advantages and limitations of each imaging modality, and these should be used in clinical practice depending on each of these aspects. CT scans should be used to assess complicated cases, but they give the best result accuracy but are expensive, have risks of radiation and are more centralized. Given the fact that LUC possesses high sensitivity and specificity and is noninvasive, it is especially useful in pediatric and critical care settings and areas with limited capabilities to perform advanced imaging studies. Although relatively less sensitive and specific than sputum culture, Chest X-ray continues to be useful in the initial diagnosis and exclusion of pneumonia particularly in OPD patients and in low awareness settings. It is therefore the responsibility of the clinician to weigh factors such as the clinical situation, population targeted and resources available to promote the best imaging outcomes for the patients. Additional future studies should be directed towards implementing new technologies including artificial intelligence imaging for better diagnosis rates and pneumonia patients’ outcomes with careful consideration when used with infants, children, older adults and pregnant women. Further research performing a meta-analysis focusing on specific outcomes like sensitivity, specificity, positive predictive value, and negative predictive value will provide a clearer comparison between the imaging modalities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Torres A, Blasi F, Dartois N, Akova M. Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease. Thorax. 2015;70(10):984–989. doi:10.1136/thoraxjnl-2015-206780
2. Prendki V, Malézieux-Picard A, Azurmendi L, et al. Accuracy of C-reactive protein, procalcitonin, serum amyloid A and neopterin for low-dose CT-scan confirmed pneumonia in elderly patients: a prospective cohort study. PLoS One. 2020;15(9):e0239606. doi:10.1371/journal.pone.0239606
3. Blaivas M, Lyon M, Duggal S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad Emerg Med. 2005;12(9):844–849. doi:10.1197/j.aem.2005.05.005
4. Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008;134(1):117–125. doi:10.1378/chest.07-2800
5. Mizgerd JP. Acute lower respiratory tract infection. N Engl J Med. 2008;358(7):716–727. doi:10.1056/NEJMra074111
6. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72. doi:10.1086/511159
7. Parveen N, Sathik MM. Detection of pneumonia in chest X-ray images. J X-Ray Sci Technol. 2011;19(4):423–428. doi:10.3233/XST-2011-0304
8. Alrajab S, Youssef AM, Akkus NI, Caldito G. Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: review of the literature and meta-analysis. Crit Care. 2013;17(5). doi:10.1186/cc13016
9. Pereda MA, Chavez MA, Hooper-Miele CC, et al. Lung ultrasound for the diagnosis of pneumonia in children: a meta-analysis. Pediatrics. 2015;135(4):714–722. doi:10.1542/peds.2014-2833
10. Ghimire M, Bhattacharya SK, Narain JP. Pneumonia in South-East Asia Region: public health perspective. Indian J Med Res. 2012;135(4):459.
11. Winer-Muram HT, Arheart KL, Jennings SG, Rubin SA, Kauffman WM, Slobod KS. Pulmonary complications in children with hematologic malignancies: accuracy of diagnosis with chest radiography and CT. Radiology. 1997;204:643–649. doi:10.1148/radiology.204.3.9280238
12. Lichtenstein DA. Lung ultrasound in the critically ill. Ann Intensive Care. 2014;4(1):1–12. doi:10.1186/2110-5820-4-1
13. Caiulo VA, Gargani L, Caiulo S, et al. Lung ultrasound characteristics of community-acquired pneumonia in hospitalized children. Pediatr Pulmonol. 2013;48(3). https://pubmed.ncbi.nlm.nih.gov/22553150/.
14. Cortellaro F, Colombo S, Coen D, Duca PG. Lung ultrasound is an accurate diagnostic tool for the diagnosis of pneumonia in the emergency department. Emerg Med J. 2012;29(1):19–23. doi:10.1136/emj.2010.101584
15. O’Grady KAF, Torzillo PJ, Frawley K, Chang AB. The radiological diagnosis of pneumonia in children. Pneumonia. 2014;5(1):38–51. doi:10.15172/pneu.2014.5/482
16. Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577–591. doi:10.1007/s00134-012-2513-4
17. Long L, Zhao HT, Zhang ZY, Wang GY, Zhao HL. Lung ultrasound for the diagnosis of pneumonia in adults: a meta-analysis. Medicine. 2017;96(3):e5713. doi:10.1097/MD.0000000000005713
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
19. Unlukaplan IM, Dogan H, Ozucelik DN. Lung ultrasound for the diagnosis of pneumonia in adults. J Pak Med Assoc. 2024;70(6). https://pubmed.ncbi.nlm.nih.gov/32810093/.
20. Ahmad T, Farooq MA, Ashraf S, Iqbal MN, Masood MK, Omer R. Diagnostic accuracy of lung ultrasound in diagnosis of pediatric pneumonia. National Editorial Advisory Board. 2019;30(9).
21. Haggag YI, Mashhour K, Ahmed K, Samir N, Radwan W. Effectiveness of lung ultrasound in comparison with chest X-Ray in diagnosis of lung consolidation. Open Access Maced J Med Sci. 2019;7(15):2457. doi:10.3889/oamjms.2019.669
22. Taghizadieh A, Ala A, Rahmani F, Nadi A. Diagnostic accuracy of chest x-Ray and ultrasonography in detection of community acquired pneumonia; a brief report. Emergency. 2015;3(3):114.
23. Karimi E. Comparing sensitivity of ultrasonography and plain chest radiography in detection of pneumonia; a diagnostic value study. Arch Acad Emerg. 2019;7(1). https://pubmed.ncbi.nlm.nih.gov/30847443/.
24. Amatya Y, Rupp J, Russell FM, Saunders J, Bales B, House DR. Diagnostic use of lung ultrasound compared to chest radiograph for suspected pneumonia in a resource-limited setting. Int J Emerg Med. 2018;11(1). doi:10.1186/s12245-018-0170-2
25. Martínez RJ, Comas RC, Pujol SJ, et al. Higher accuracy of lung ultrasound over chest X-ray for early diagnosis of COVID-19 pneumonia. Int J Environ Res Public Health. 2021;18(7). https://pubmed.ncbi.nlm.nih.gov/33801638/.
26. Yan C, Hui R, Lijuan Z, Zhou Y. Lung ultrasound vs. chest X‑ray in children with suspected pneumonia confirmed by chest computed tomography: a retrospective cohort study. Exp Ther Med. 2020;19(2):1363–1369. doi:10.3892/etm.2019.8333
27. Ticinesi A, Lauretani F, Nouvenne A, et al. Lung ultrasound and chest x-ray for detecting pneumonia in an acute geriatric ward. Medicine. 2016;95(27):e4153. doi:10.1097/MD.0000000000004153
28. Bitar ZI, Maadarani OS, El‐Shably AM, Al‐Ajmi MJ. Diagnostic accuracy of chest ultrasound in patients with pneumonia in the intensive care unit: a single‐hospital study. Health Sci Rep. 2019;2(1). doi:10.1002/hsr2.102
29. Bourcier JE, Paquet J, Seinger M, et al. Performance comparison of lung ultrasound and chest x-ray for the diagnosis of pneumonia in the ED. Am J Emerg Med. 2014;32(2):115–118. doi:10.1016/j.ajem.2013.10.003
30. Gibbons RC, Magee M, Goett H, et al. Lung Ultrasound vs. chest X-Ray study for the radiographic diagnosis of COVID-19 pneumonia in a high-prevalence population. J Emerg Med. 2021;60(5):615. doi:10.1016/j.jemermed.2021.01.041
31. Ye X, Xiao H, Chen B, Zhang S. Accuracy of lung ultrasonography versus chest radiography for the diagnosis of adult community-acquired pneumonia: review of the literature and meta-analysis. PLoS One. 2015;10(6). https://pubmed.ncbi.nlm.nih.gov/26107512/.
32. Oh SJ, Hwang KE, Jeong ET, Kim HR. A case of pulmonary siderosis misdiagnosed as pneumonia. Respir Med Case Rep. 2018;25:58–60. doi:10.1016/j.rmcr.2018.06.006
33. Alzahrani SA, Al-Salamah MA, Al-Madani WH, Elbarbary MA. Systematic review and meta-analysis for the use of ultrasound versus radiology in diagnosing of pneumonia. Crit Ultrasound J. 2017;9(1). doi:10.1186/s13089-017-0059-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Supraglottic Suction Device in Mechanically Ventilated Patients: A Randomized Controlled Trial
Orozco-Levi M, Tiga-Loza DC, Aya O, Reyes CF, Cáceres-Rivera D, Espitia A, Rey D, Pedrozo Arias KP, Pizarro C, Sanabria-Barrera SM, Serrano-Díaz N, Castillo VR, Ramírez-Sarmiento A
Medical Devices: Evidence and Research 2025, 18:201-212
Published Date: 24 March 2025