Back to Journals » Journal of Pain Research » Volume 11
Comparing the effect of eye movement desensitization and reprocessing (EMDR) with guided imagery on pain severity in patients with rheumatoid arthritis
Authors Ghanbari Nia N, Afrasiabifar A ![]() , Behnammoghadam M
, Behnammoghadam M
Received 5 December 2017
Accepted for publication 7 August 2018
Published 28 September 2018 Volume 2018:11 Pages 2107—2113
DOI https://doi.org/10.2147/JPR.S158981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Nasrin Ghanbari Nia,1 Ardashir Afrasiabifar,2 Mohammad Behnammoghadam1
1Student Committee Research, Yasuj University of Medical Sciences, Yasuj, Iran; 2School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran
Objective: Previous studies reported the reduction of pain following eye movement desensitization and reprocessing (EMDR) and guided imagery; however, the effectiveness of these modalities was not compared. The current study aimed to compare the effects of EMDR and guided imagery on pain severity in patients with rheumatoid arthritis.
Material and methods: In this randomized controlled trial, 75 patients were selected using non-random method, and then allocated into two intervention groups and one control group. Interventions were conducted individually in six consecutive sessions for the intervention groups. The Rheumatoid Arthritis Pain Scale was used for data collection before and after the interventions. Collected data were analyzed with descriptive and inferential statistics in SPSS. Significance level was considered at P<0.05.
Results: The post-intervention mean scores of physiological, affective, sensory-discriminative, and cognitive pain sub-scales for patients in guided imagery group were 16.3±2.2, 13.9±2.2, 30.6±3.4, and 23.2±3, respectively. The post-intervention mean scores of these sub-scales in the EMDR group were 22±1.5, 18.1±1.8, 39.6±2.8, and 29±1.8, respectively. A significant difference was observed in the mean pain score between EMDR and guided imagery groups, and also between each intervention group and the control group (P=0.001).
Conclusion: Guided imagery and EMDR could reduce pain in rheumatoid arthritis, but pain reduction was more following the EMDR than guided imagery.
Keywords: eye movement desensitization and reprocessing, guided imagery, pain, rheumatoid arthritis
Introduction
Joint pain, morning stiffness, and joint dysfunction are among common symptoms of rheumatoid arthritis (RA).1 Fifty-three percent of patients with RA suffer from moderate-to-severe joint pain,2 which can affect their quality of life3 and daily function.4 The use of analgesics, either steroid or non-steroid, is associated with such adverse side effects as gastrointestinal complications.5 Therefore, non-medicinal treatments including psychological and lifestyle interventions,6 as well as cognitive-behavioral therapy7 have been considered for pain management in patients with RA.
EMDR is a cognitive and non-pharmacological method, developed by Shapiro based on the adaptive information processing (AIP) model.8 In this method, a change occurs in cognitive, affect, and physical responses pertinent to memory.9 EMDR may be presented as an alternate method to treating chronic pain. Painful memories appear to be a major factor in maintaining and continuing chronic pain, and untreated painful memories can result in continued pain.10 The literature review showed the effectiveness of this method in reducing pain,11 decreasing anxiety and increasing physical function,12 reducing chronic pain,13 and easing chronic phantom organ pain14,15 has been addressed by different studies.
Guided imagery is among mind-body therapies that use imagination for making changes in physical, emotional, and spiritual dimensions. Imagery can be considered as an activity that produces physiologic and somatic responses. Imagery also is a distraction method; detailed images using all senses to be applied for pain control. This technique uses all senses,16 thereby promoting the self-awareness and self-control in people.17 Chen and Francis showed the effectiveness of guided imagery plus progressive (muscle) relaxation, as adjuvant treatments, in reducing chronic pains.18 The effectiveness of guided imagery in reducing spinal pains,19 chronic pains,20 pain after joint replacement surgery,21 abdominal pain,22 and pain caused by cysts in women23 has been reported in literature.
As mentioned above, different studies have investigated the effects of EMDR and guided imagery modalities on the severity of pain in different patients; however, few studies have compared their effectiveness in reducing the severity of pain in patients with RA. On the other hand, since both methods are among cognitive and mental therapies, the question is whether their effectiveness in reducing pain differs. As a result, this study aimed to compare the effects of EMDR and guided imagery on the severity of pain in patients with RA.
Material and methods
The study population of this randomized controlled trial includes all patients with RA referring to a rheumatology clinic in Yasuj City, 2016. Seventy-five eligible patients with RA were selected using convenience sampling method but allocated among three groups – two intervention groups and one control group – through unmatched block randomization. Because we defined three groups as EMDR or group A, guided imagery or group B, and control or group C. Based on the factorial rule (3!=3×2×1=6), we created six blocks named as ABC, ACB, BAC, BCA, CAB, and CBA. The size of each block was three, and there was a sample of each group in each block but their arrangement varied. Then, we selected blocks from these six blocks by random replacement sampling. The inclusion criteria were a final diagnosis of RA by a rheumatologist, the patient complains of pain, the low score of pain (severe pain) based on applied scale, patient’s ability to perform EMDR and guided imagery and patient’s willingness to participate. Exclusion criteria include a high score of pain (mild pain) based on scale, patient’s unwillingness to participate, hearing and vision problems, patient’s immigration or death, and having an unpleasant memory of forests and natural sceneries. Participants were informed about the confidentiality of information, and opportunity to continue participation or withdraw in each stage. These interventions were conducted after obtaining the written informed consent of the patients and permission of the patient’s physician. The current study was approved by the Ethics Committee of Yasuj University of Medical Sciences (YUMS. REC.1394.130), and registered in the Clinical Trial Registration Center of Iran’s Website (IRCT2016022926846N1).24
The Rheumatoid Arthritis Pain Scale (RAPS) was used to measure the pain severity. This scale is comprised of 24 items, measuring physiological, affective, sensory-discriminative, and cognitive pain subscales. The items are rated on a seven-point Likert scale anchored by 0 (Always) and 6 (Never) with minimum and maximum possible scores of 0 and 144, respectively. Lower scores reflect greater pain severity. The validity of the Persian version of the scale has been already approved.25 We checked the reliability of this scale and a Cronbach’s coefficients 0.73 was reported in test-retest reliability. The RAPS was completed by the patients in two intervention groups a week before starting interventions as well as two weeks after beginning intervention. In the control group, the interval of filling scale between before and post-intervention pain ratings was the same as in two intervention groups. There is no drop-out in this study, and all participated patients completed the study.
EMDR was conducted by patients individually, according to proposed protocol10,26 in six consecutive sessions lasting from 45 to 90-minute,27 held once per day at 7 PM in a quiet room in the rheumatology clinic. The steps of conducting EMDR are shown in Table 1. In the first phase or client history, the patient’s ability to conduct EMDR is assessed by the therapist. After determining the patient’s ability to perform EMDR, intervention is explained for the patient and prepared to do EMDR. In the third phase, disturbing images (targets), and negative beliefs were assessed as well as patient’s believability toward the positive cognition is measured through the VOC scale, seven-point scale in which one stands for completely false and a seven being completely true. The client is asked to hold both the images and negative cognitions in his or her mind while rating it from zero to ten using the subjective units of disturbance (SUD) scale. In the fourth phase or desensitization of the target, the therapist the patient was asked to think about disturbing images then eye bilateral stimulations including alternating eye movements to left and right were taken by the therapist. A complex of desensitization was composed of 24–36 sets of horizontal fingers movements from left to right and vice versa. The goal of desensitization was to decrease SUD to zero. In the fifth phase or installing the positive cognition, the patient is trained to focus on the target image and practice positive thinking during bilateral stimulation recognition until it feels completely true. In the phase of the body scan, problems are assessed by the patient, and the residual symptoms of discomfort or physical pressure were checked. The phase of session closure was developed to ensure that the patient is returned safely to a state of emotional stability directly following treatment. In the last phase or re-evaluation, two SUD and VOC scales were were again completed by the patient that low scores for SUD and high scores for VOC is expected in this phase.
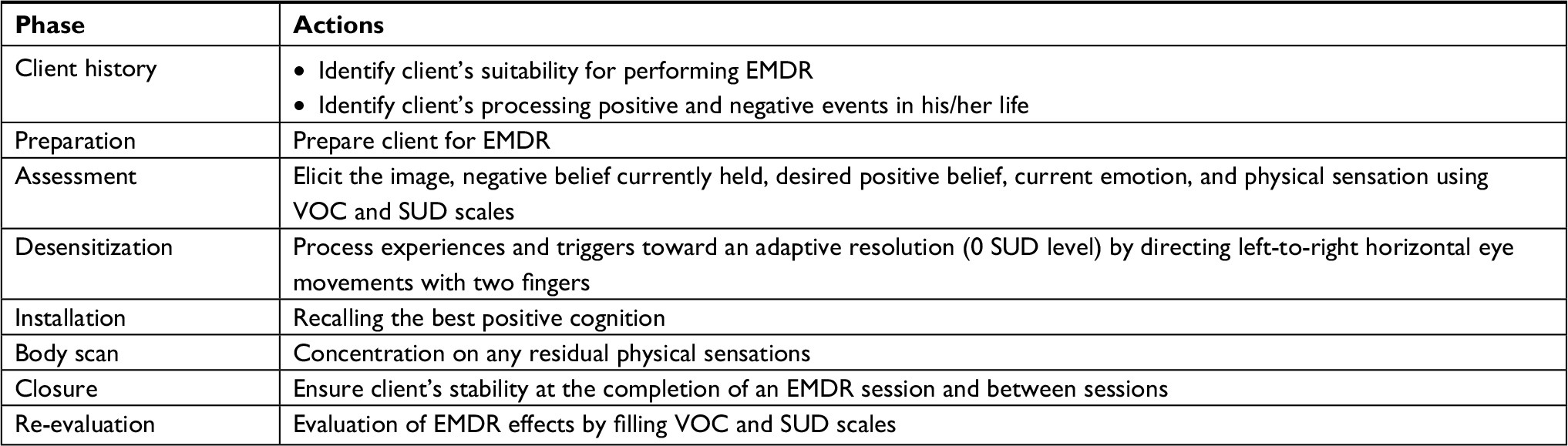 | Table 1 EMDR protocol Abbreviations: EMDR, eye movement desensitization and reprocessing; SUD, subjective units of disturbance; VOC, validity of cognition. |
Guided imagery was carried out individually according to the proposed protocol in six consecutive sessions,16,28 held once per day at 7 PM in a quiet room at the same clinic. In this modality, specific sceneries were used to induce relaxation in the patient on comfortable sitting or reclining position (not lying down) with closed eyes. The patient was also asked to focus on breathing with abdominal muscles. He or she was informed to breathe as it enters through nose and leaves through the mouth. If patient’ thoughts were roam, he or she was educated to bring the mind back to think his or her breathing and relaxed body. The patient was asked to use his /her sensory perception during imagination. Sceneries such as the forest full of green trees, blue sky, and white cloud were used to induce calmness, then, the sound of wind blowing into the trees, the flow of water, and the sound of the birds were added to them. Imagining what steps he or she will need to take by focusing on breathing, body relaxing, being aware of the favorite places, frequently concentrating on breathing, and feeling a sense of relaxation and refreshment to resume activities were examples which are presented step by step in the provided CD. Patients were also asked to listen to the provided CD 30 minutes before sleeping. Patients’ compliance was checked via telephone by the first author.
Due to the limited resources available for this study, placebo-equivalent groups corresponding to EMDR and guided imagery were absent from this study. However, a waitlist control group was available which received treatment as usual and was used in lieu of one or more placebo groups to assess treatment-specific effects.
The collected data was analyzed using descriptive and inferential statistics in SPSS. Significance level and CI were considered at P<0.05% and 95%, respectively. First, distribution of pain scores was checked using the Kolmogorov–Smirnov test. Since the outcome variable had a normal distribution, the one-way analysis of variance (ANOVA) was used for between group comparisons. In addition, the paired sample t-test was employed to make a within-group comparison of the mean pain scores. Our colleagues responsible for collecting and analyzing data were blind to the group of patients.
Findings
In the current study, 75 patients with RA with a mean age of 45.4±11.3 years were allocated EMDR, guided imagery and control groups. According to demographic data, 85.3% (64 patients) of participants were female and 86.7% (65 patients) of them were married. The mean lengths of diagnosis and treatment were 88.8±85 and 75.6±67.6 months, respectively. No statistically significant difference was observed among groups by demographic variables (P>0.05).
The result of the study showed decreased pain severity (increasing mean scores) after interventions of EMDR and guided imagery. Patients in both EMDR and guided imagery groups had significantly scored lower pain severity for four subscales post interventions than those before interventions. The results of within-group comparison using paired samples t-test showed a significant mean difference of pain subscales between after and before interventions in both EMDR and guided imagery groups (P=0.001); whereas, no significant difference was observed in the control group between pre and post interventions (Table 2).
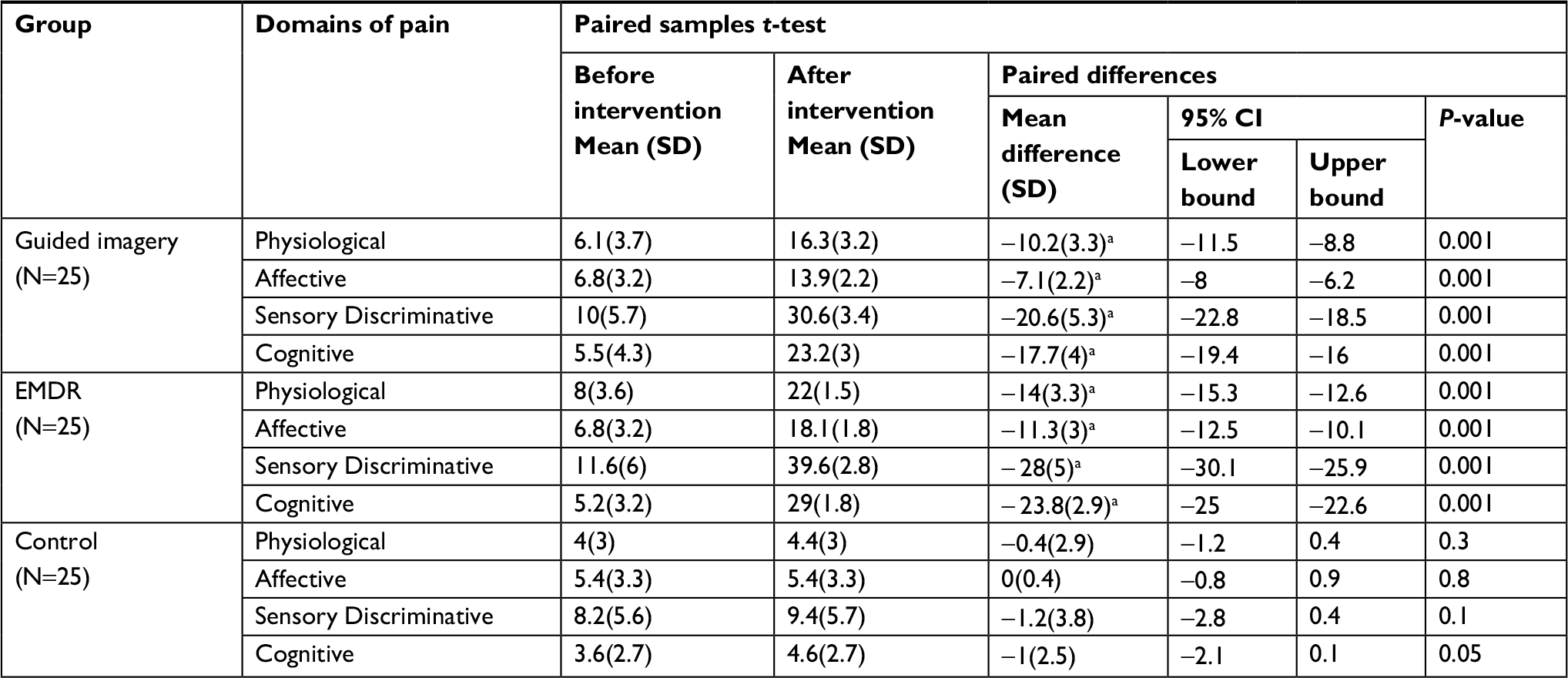 | Table 2 Within-group comparison for a mean difference of pain severity after intervention compared to before intervention in each group Note: aThe mean difference is significant. Abbreviation: EMDR, eye movement desensitization and reprocessing. |
Between-group comparison using one-way analysis of variance (ANOVA) showed no significant difference in subscales of patients’ pain severity in three groups before intervention (P>0.05). However, a significant statistical difference was reported after the intervention among groups. Given these significant differences, post hoc test was used to multiple comparisons for mean pain severity using Bonferroni test. The results showed that EMDR group rated significantly more pain reduction than guided imagery group and the control group (P=0.001). In addition, the guided imagery group also rated significantly more pain reduction than the control group (P=0.001). In other words, EMDR resulted in more pain reduction than guided imagery (P=0.001) (Table 3).
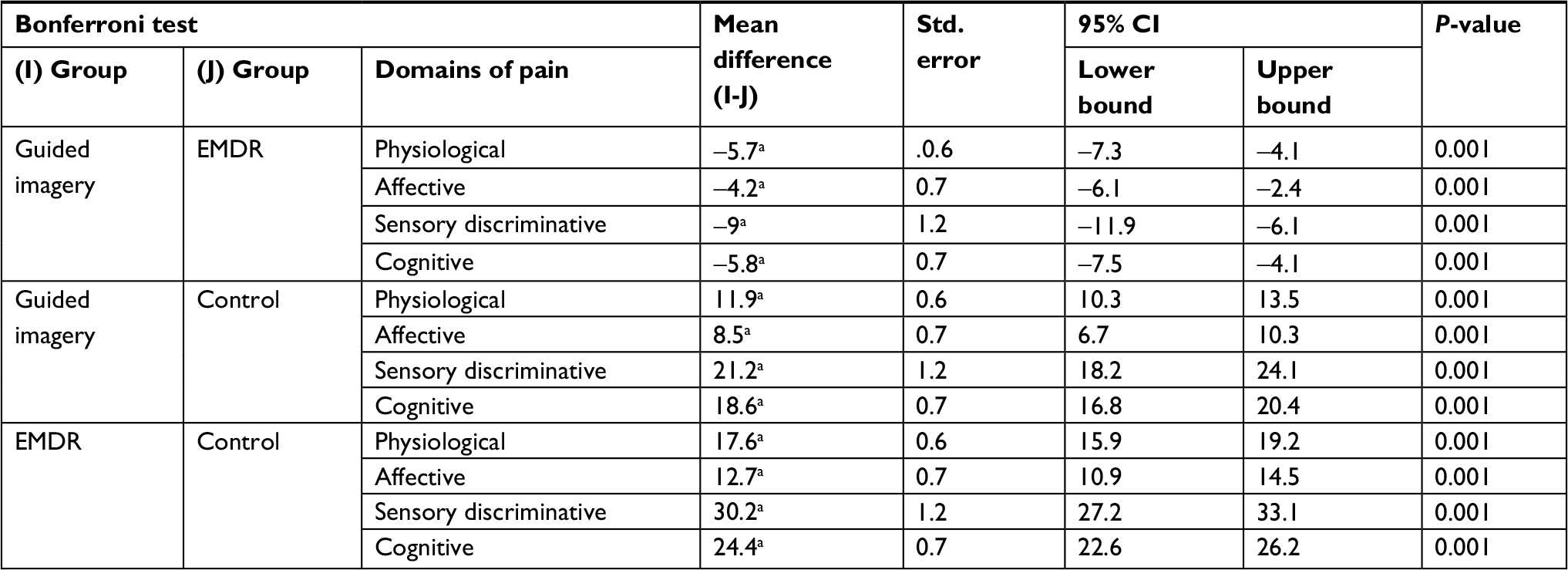 | Table 3 Multiple comparisons (post Hoc test: Bonferroni) for a mean difference of pain severity after interventions Note: aThe mean difference is significant. I and J are labels for identifying groups and their mean difference according to SPSS output. Abbreviation: EMDR, eye movement desensitization and reprocessing. |
Discussion
This study aimed to compare the effects of EMDR and guided imagery on the severity of pain in patients with RA. Findings showed that both EMDR and guided imagery reduced pain in patients with RA ; however, this reduction was more after EMDR intervention.
As it was said earlier in introduction section, the effects of these two interventions on the severity of pain in patients with RA have not been compared or the findings have been different. For example, Forward et al investigated the effect of therapeutic touch and guided imagery on pain and anxiety of patients undergoing joint replacement surgery, and showed greater effectiveness of the former method in this regard.29 Tesarz et al showed the effectiveness of EMDR plus routine care in reducing the pain and morbidity, and promoting quality of life of patients with chronic back pain.30 Another study reported significant reduction migraine headache following EMDR plus routine care, as compared to pharmacotherapy.31 Findings of this study pertaining to EMDR were consistent with studies by Flik and de Ross,32 Estergard33 and Hughes34 pertaining to guided imagery was consistent with studies by Dobson35 and Onieva-Zafra et al,36 but inconsistent with the study by Verkaik et al37 and Nilsson et al.38 The reasons for the inconsistency may be due to the difference in the type of samples, the number of samples, the time of the intervention, and the measurement tool. One of the inconsistency might be found in the content of the exercises and medical history of participants.
Several mechanisms such as adaptive information processing and neurological models have been proposed to explain pain relief following EMDR therapy.39 The EMDR modality contributes to rehabilitation of cognitive system by involving the components of the nervous system.40 It also helps brain process memories in the patient’s nervous system through natural processing of emotional information.41 EMDR can affect rapid eye movement (REM) phase of sleep, stimulation of associated brain nerves42 , and activate the parasympathetic and inhibit the sympathetic systems.43 EMDR can lead to decreasing the pain sensation with the processing of target memories.26 These mechanisms may cause pain reduction in patients. On the other hand, guided imagery activates the central nervous system. The activation of the processing function of the central, peripheral, or autonomic nervous system may help to reduce or eliminate symptoms such as pain. Imagery can break this cycle of pain–tension–anxiety–pain. Relaxation with imagery decreases pain directly by reducing muscle tension and related spasms.15
Although these are interesting findings within the respective fields of both EMDR and guided imagery research, the lack of a placebo group makes it difficult to rule out the placebo effect when interpreting the results as this would serve to augment any treatment-specific effects that are directly attributable to either EMDR or guided imagery. As mentioned in method section, a placebo group was not included in our study due to limited resources. Confidence in our results could be strengthened in future studies with the use of equivalent placebo controls respective to each intervention. For example, given that there is some support that EMDR ameliorates PTSD via taxing the working memory while activating the memory.44 EMDR-equivalent placebo interventions that tax the working memory (otherwise known as an attentional placebo) has been used in placebo-controlled trials of EMDR. Examples include active listening45 and progressive muscle relaxation.46 As for guided imagery, past studies have made use of placebo relaxation techniques47 and listening to a blank CD as a placebo control for guided imagery.48
Although the current study indicated pain reduction in patients with RA following EMDR and guided imagery interventions, this study was associated with some limitations which should be considered in the generalization of finding. First, the severity of pain in patients with RA in remission phase may be less than in patients with RA in the relapsing phase of the disease. Therefore, it is recommended to investigate the effect of these interventions on the severity of pain in patients with RA in the relapsing phase. Second, participants of our study were selected using non-random sampling or convenience method due to the limited study population, so random sampling method is impossible, and the sample size of this study is small. Further investigation with larger sample size and random sampling method was suggested to examine the effects of these interventions.
Given that this study was conducted in patients with RA with chronic pain, it is recommended to compare the effects of EMDR and guided imagery in hospitalized patients with acute pain.
Conclusion
Both EMDR and guided imagery could reduce pain in patients with RA; however, this reduction was more following EMDR than the guided imagery. Management of clinical manifestations particularly pain alleviation is one of the main objectives of the medical management of patients with RA. Given that the simplicity, cost-effectiveness, and non-aggressiveness of such interventions, in addition to further researches, a systematic review and meta-analysis studies are also recommended. The healthcare workers might consider these interventions once the approval of their effectiveness is provided.
Acknowledgments
The authors would like to honor all patients and their families who cooperated patiently in this study as well as Yasuj University of Medical Sciences for its financial support.
Author contributions
MB and NGN evaluated the paper, designed the research, collected data, did sampling, allocated samples to the study groups, implemented interventions, analysed data, compiled the article and wrote the processes; AA monitored interventions, analysed data, and compiled the article. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Cutolo M, Straub RH. Circadian rhythms in arthritis: hormonal effects on the immune/inflammatory reaction. Autoimmun Rev. 2008;7(3):223–228. | ||
Fitzcharles MA, Dacosta D, Ware MA, Shir Y. Patient barriers to pain management may contribute to poor pain control in rheumatoid arthritis. J Pain. 2009;10(3):300–305. | ||
Dougados M. Can we combine patient’s and doctor’s perspective when assessing rheumatoid arthritis disease activity? J Rheumatol. 2007;34(10):1949–1952. | ||
Owens GM. Optimizing rheumatoid arthritis therapy: using objective measures of disease activity to guide treatment. Am Health Drug Benefits. 2015;8(7):354–360. | ||
Solomon DH, Reed GW, Kremer JM, et al. Disease activity in rheumatoid arthritis and the risk of cardiovascular events. Arthritis Rheumatol. 2015;67(6):1449–1455. | ||
Keefe FJ, Somers TJ, Martire LM. Psychologic interventions and lifestyle modifications for arthritis pain management. Rheum Dis Clin North Am. 2008;34(2):351–368. | ||
Ferwerda M, van Beugen S, van Middendorp H, et al. A tailored-guided internet-based cognitive-behavioral intervention for patients with rheumatoid arthritis as an adjunct to standard rheumatological care: results of a randomized controlled trial. Pain. 2017;158(5):868–878. | ||
Hase M, Balmaceda UM, Hase A, et al. Eye movement desensitization and reprocessing (EMDR) therapy in the treatment of depression: a matched pairs study in an inpatient setting. Brain Behav. 2015;5(6):n/a–351. | ||
Shapiro F. The human mind, psychotherapy and EMDR. Actas esp psiquiatr. 2010;38(3):44–46. | ||
Rostaminejad A, Behnammoghadam M, Rostaminejad M, Behnammoghadam Z, Bashti S. Efficacy of eye movement desensitization and reprocessing on the phantom limb pain of patients with amputations within a 24-month follow-up. Int J Rehabil Res. 2017;40(3):209–214. | ||
Tesarz J, Leisner S, Gerhardt A, et al. Effects of eye movement desensitization and reprocessing (EMDR) treatment in chronic pain patients: a systematic review. Pain Med. 2014;15(2):247–263. | ||
Rathschlag M, Memmert D. Reducing anxiety and enhancing physical performance by using an advanced version of EMDR: a pilot study. Brain Behav. 2014;4(3):348–355. | ||
Mazzola A, Calcagno ML, Goicochea MT, et al. EMDR in the Treatment of Chronic Pain. Journal of EMDR Practice and Research. 2009;3(2):66–79. | ||
Schneider J, Hofmann A, Rost C, Shapiro F. EMDR in the treatment of chronic phantom limb pain. Pain Med. 2008;9(1):76–82. | ||
Wilensky M. Eye movement desensitization and reprocessing as a treatment for phantom limb pain. J Brief Ther. 2006;5(1):31–44. | ||
FitzGerald M, Langevin M. Complementary and alternative therapies in nursing. 6th ed. New York: Springer Publishing Company; 2010:63–83. | ||
Hart J. Guided Imagery. Alternative and Complementary Therapies. 2008;14(6):295–299. | ||
Chen YL, Francis AJ. Relaxation and imagery for chronic, nonmalignant pain: effects on pain symptoms, quality of life, and mental health. Pain Manag Nurs. 2010;11(3):159–168. | ||
Charette S, Fiola JL, Charest MC, et al. Guided imagery for adolescent post-spinal fusion pain management: a pilot study. Pain Manag Nurs. 2015;16(3):211–220. | ||
Lewandowski W, Jacobson A, Palmieri PA, Alexander T, Zeller R. Biological mechanisms related to the effectiveness of guided imagery for chronic pain. Biol Res Nurs. 2011;13(4):364–375. | ||
Thomas KM, Sethares KA. Is guided imagery effective in reducing pain and anxiety in the postoperative total joint arthroplasty patient? Orthop Nurs. 2010;29(6):393–399. | ||
van Tilburg MA, Chitkara DK, Palsson OS, et al. Audio-recorded guided imagery treatment reduces functional abdominal pain in children: a pilot study. Pediatrics. 2009;124(5):e890–e897. | ||
Carrico DJ, Peters KM, Diokno AC. Guided imagery for women with interstitial cystitis: results of a prospective, randomized controlled pilot study. J Altern Complement Med. 2008;14(1):53–60. | ||
Iranian Registry of Clinical Trials. Comparison of the effect of eye movement desensitization and reprocessing (EMDR) and guided imagery on the severity of insomnia and pain of rheumatoid arthritis patients. Available from: http://en.irct.ir/trial/22144. | ||
Rezaei F, Neshat Doost H, Molavi H, et al. The relationship between emotional impairment and pain in patients with rheumatoid arthritis. J of Shahid Sadoughi University Of Medical Sciences. 2013;21(4):448–458. | ||
Feener RS. EMDR: Eye movement desensitization and reprocessing a new method in the treatment of performance anxiety for singers. Tallahassee, FL: Florida State University; 2004. | ||
van den Berg DP, van der Gaag M. Treating trauma in psychosis with EMDR: a pilot study. J Behav Ther Exp Psychiatry. 2012;43(1):664–671. | ||
Louie SW. The effects of guided imagery relaxation in people with COPD. Occup Ther Int. 2004;11(3):145–159. | ||
Forward JB, Greuter NE, Crisall SJ, Lester HF. Effect of Structured Touch and Guided Imagery for Pain and Anxiety in Elective Joint Replacement Patients--A Randomized Controlled Trial: M-TIJRP. Perm J. 2015;19(4):18–28. | ||
Tesarz J, Gerhardt A, Leisner S, et al. Effects of eye movement desensitization and reprocessing (EMDR) on non-specific chronic back pain: a randomized controlled trial with additional exploration of the underlying mechanisms. BMC Musculoskelet Disord. 2013;14:256. | ||
Marcus SV. Phase 1 of Integrated EMDR<BR> An Abortive Treatment for Migraine Headaches. Journal of EMDR Practice and Research. 2008;2(1):15–25. | ||
Flik C, de Roos C. Eye movement desensitisation and reprocessing (EMDR) as a treatment for phantom limb pain. Tijdschr Psychiatr. 2009;52(8):589–593. | ||
Estergard L. Eye movement desensitization and reprocessing in the treatment of chronic pain. Walden: Walden University; 2008. | ||
Hughes M. EMDR as a therapeutic treatment for complex regional pain syndrome: A case report. Journal of EMDR Practice and Research. 2014;8(2):66–73. | ||
Dobson C. Outcome results of self-efficacy in children with sickle disease pain who were trained to use guided imagery. Appl Nurs Res. 2015;28(4):384–390. | ||
Onieva-Zafra MD, García LH, del Valle MG. Effectiveness of guided imagery relaxation on levels of pain and depression in patients diagnosed with fibromyalgia. Holist Nurs Pract. 2015;29(1):13–21. | ||
Verkaik R, Busch M, Koeneman T, et al. Guided imagery in people with fibromyalgia: a randomized controlled trial of effects on pain, functional status and self-efficacy. J Health Psychol. 2014;19(5):678–688. | ||
Nilsson S, Forsner M, Finnström B, Mörelius E. Relaxation and guided imagery do not reduce stress, pain and unpleasantness for 11- to 12-year-old girls during vaccinations. Acta Paediatr. 2015;104(7):724–729. | ||
Gerhardt A, Eich W, Seidler G, Tesarz J, et al. Eye movement desensitization and reprocessing in chronic pain conditions. OA Musculoskeletal Medicine. 2013;1(1):1–7. | ||
Zarghi A, Zali A, Tehranidost M. Methodological Aspects of Cognitive Rehabilitation with Eye Movement Desensitization and Reprocessing (EMDR. Basic Clin Neurosci. 2013;4(1):97–103. | ||
Narimani M, Rajabi S. Comparison of efficacy of eye movement desensitization and reprocessing with cognitive behavioral therapy in the treatment of stress disorder. J of Medical Sciences Islamic Azad University. 2010;19(4):236–245. | ||
Ranjbaripour T, Hashemian K, Ahadi H, et al. The effectiveness of therapy Eye Movement Desensitization and Reprocessing (EMDR) on the first night insomnia. J of Clinical Psychology. 2014;4(15):128–139. | ||
Elofsson UOE, von Schèele B, Theorell T, Söndergaard HP, et al. Physiological correlates of eye movement desensitization and reprocessing. J Anxiety Disord. 2008;22(4):622–634. | ||
Gunter RW, Bodner GE. . How eye movements affect unpleasant memories: support for a working-memory account. Behav Res Ther. 2008;46(8):913–931&. | ||
Cvetek R. EMDR treatment of distressful experiences that fail to meet the criteria for PTSD. Journal of EMDR Practice and Research. 2008;2(1):2–14. | ||
Goldstein AJ, de Beurs E, Chambless DL, Wilson KA. . EMDR for panic disorder with agoraphobia: comparison with waiting list and credible attention-placebo control conditions. J Consult Clin Psychol. 2000;68(6):947–956&. | ||
Lahmann C, Nickel M, Schuster T, et al. Functional relaxation and guided imagery as complementary therapy in asthma: a randomized controlled clinical trial. Psychother Psychosom. 2009;78(4):233–239&. | ||
Ikedo F, Gangahar DM, Quader MA, Smith LM. . The effects of prayer, relaxation technique during general anesthesia on recovery outcomes following cardiac surgery. Complement Ther Clin Pract. 2007;13(2):85–94&. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.