Back to Journals » Clinical Ophthalmology » Volume 20
Comparing Refractive Prediction Accuracy of IOL Master 700 and Sirius Utilizing the Barrett Universal II Formula
Authors Yang J, Yang N, Xiang Y ![]() , Li R, Yu X, Jin L, Huang Y
, Li R, Yu X, Jin L, Huang Y
Received 3 September 2025
Accepted for publication 6 January 2026
Published 10 January 2026 Volume 2026:20 560886
DOI https://doi.org/10.2147/OPTH.S560886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Junjie Yang, Nijuan Yang, Yuying Xiang, Rui Li, Xuan Yu, Ling Jin, Yukan Huang
Department of Ophthalmology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
Correspondence: Yukan Huang, Department of Ophthalmology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1277, Jiefang Avenue, Jianghan District, Wuhan, Hubei, People’s Republic of China, Email [email protected] Ling Jin, Department of Ophthalmology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1277, Jiefang Avenue, Jianghan District, Wuhan, Hubei, People’s Republic of China, Email [email protected]
Purpose: To compare the refractive-prediction error (the difference between the predicted post-operative spherical equivalent and the actual spherical equivalent) of IOLMaster 700 and Sirius when their biometric data are fed into the Barrett Universal II formula.
Setting: Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China.
Design: Prospective, observational, single-center, paired-eye study.
Methods: 123 eyes of 93 cataract patients were enrolled. The participants ranged in age from 36 to 91 years, with a mean age of 65.38 ± 14.84 years. Axial length from IOLMaster 700 and corneal curvature, anterior-chamber depth and white-to-white from both devices were entered into the BarErett Universal II calculator to obtain predicted post-operative spherical equivalent (PRP). One week after uneventful phacoemulsification with monofocal intraocular lens implantation, manifest refraction provided the actual spherical equivalent (SE). Prediction error (ΔPRE = PRP - SE) and absolute error |ΔPRE| were primary outcomes.
Results: Both devices produced positive ΔPRE, but the median was lower for IOLMaster 700 than for Sirius (0.41 D vs 0.73 D; p < 0.05). Median |ΔPRE| was also smaller for IOLMaster 700 (0.61 D vs 0.80 D; p < 0.05). Eyes within ± 0.50 D of target refraction numbered 45.5% for IOLMaster 700 versus 26.0% for Sirius (p < 0.05). Subgroup analysis showed no difference in error magnitude between long (AL > 25 mm) and normal axial-length eyes.
Conclusion: Under the Barrett Universal II formula, IOLMaster 700 yields more accurate refractive predictions than Sirius, with smaller systematic drift and absolute error, irrespective of axial length. Thus, IOLMaster 700 with Barrett Universal II is the preferred biometry for superior refractive accuracy. This study offers surgeons practical guidance for improving post-operative visual outcomes and patient satisfaction.
Keywords: IOLMaster 700, Sirius, Barrett Universal II formula, prediction error, cataract surgery
Introduction
With the shift of cataract surgery from a restorative procedure to a refractive procedure, residual refractive error after surgery has become one of the important factors affecting patient satisfaction1–3. Accurate preoperative measurement of corneal curvature and anterior chamber depth (ACD) is a key step in reducing postoperative refractive error.4,5 Inaccurate biometry may lead to incorrect intraocular lens (IOL) power calculation, resulting in postoperative refractive surprise.6 Currently, the IOLMaster 700 (Carl Zeiss Meditec, Germany), based on swept-source optical coherence tomography (SS-OCT), and the Sirius (CSO, Italy), based on Scheimpflug-Placido hybrid imaging technology, are both high-precision non-contact optical biometers commonly used in clinical practice.7,8 However, there are essential differences between the two in terms of measurement principles, light sources, and image processing algorithms,9 which may lead to different values of corneal curvature and ACD obtained from the same patient.10,11
Under the same formula, minor variations in biometric parameters can lead to significant deviations in refractive outcomes. In terms of corneal curvature measurement, the mean difference between different biometric devices can reach up to 0.3 D, and this difference directly affects the accuracy of the final refractive result.12,13 An error of 0.1 mm in ACD measurement can induce approximately 0.25 D of IOL power calculation deviation.14 Existing studies mostly focus on the comparison of the repeatability or consistency of single-parameter measurements by different devices preoperatively, and there is a lack of prospective data comparing the predicted postoperative refraction with the actual postoperative spherical equivalent (SE) after substituting their measurement results into the formula. This study aims to investigate the clinical relevance of measurement variability between ocular biometric systems due to their potential impact on surgical planning and refractive outcomes. Hoffer et al found that the IOL power calculations derived from Revo OCT (spectral-domain optical coherence tomography) and Pentacam AXL (Scheimpflug imaging combined with partial coherence interferometry) under the four classic formulas - Haigis, Hoffer Q, Holladay I, and SRK/T showed a high correlation.15 Both the present study and multiple international guidelines confirm that the Barrett Universal II formula yields fewer refractive surprises than Holladay II, SRK/T, Hoffer Q and Hill-RBF across all axial lengths, while maintaining robust predictive accuracy over varying corneal powers, making it the preferred choice for minimizing post-cataract refractive error.16,17
Therefore, this study adopted a prospective, dual-device paired design to compare the refractive prediction drift characteristics of the IOLMaster 700 and Sirius under the Barrett Universal II formula. Given that the axial length (AL) measurements obtained by the IOLMaster 700 have been extensively validated, the AL data measured by the IOLMaster 700 were uniformly used in this study.18 The corneal flat curvature (K1), steep curvature (K2), ACD, and white-to-white (WTW) measurements were obtained separately using the two devices to assess their impact on refractive prediction. Preoperatively, all patients had the aforementioned parameters measured by both devices and substituted into the Barrett Universal II formula to calculate the predicted postoperative spherical equivalent (SE). One week postoperatively, refraction was performed to obtain the actual SE. The prediction error (predicted SE - actual SE) was used as the primary indicator to compare the refractive prediction differences between the two devices under the Barrett Universal II formula, providing evidence-based guidance for clinical device selection and preoperative planning.
Materials and Methods
Study Design
This study is a prospective, observational diagnostic accuracy study that adheres to the Declaration of Helsinki and the STARD guidelines, and was approved by the Medical Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. The ethical approval number is 2024–0280, and the review date is April 19, 2024. The study population consisted of patients who underwent cataract surgery in the Department of Ophthalmology at Tongji Hospital and voluntarily participated between April 20, 2024, and January 1, 2025. All participants provided written informed consent after fully understanding the purpose, procedures, and potential risks of the study.
The inclusion criteria were as follows: (1) age greater than 18 years; (2) the patient was able to cooperate with fixation and maintain a stable head position to complete all measurements; (3) clinical diagnosis of age-related or secondary cataract, with planned phacoemulsification plus posterior chamber IOL implantation in one or both eyes; (4) preoperatively, K1, K2, ACD and WTW measurements could be completed separately by IOLMaster 700 and Sirius by the same operator on the same visit day; (5) stable manifest refraction SE could be obtained 1 week postoperatively.
The exclusion criteria included: (1) inability to cooperate with fixation or maintain a stable head position, resulting in failed measurements by either device; (2) corneal or ocular surface pathology (eg, significant corneal scar, active keratitis, pterygium) affecting optical measurements; (3) posterior segment pathology (eg, retinal detachment, macular degeneration, vitreous hemorrhage) or optic nerve disease; (4) history of previous intraocular surgery (including refractive surgery, glaucoma filtering surgery, etc.) or systemic diseases that may affect the refractive status; (5) intraoperative or postoperative complications (eg, posterior capsule rupture, intraocular lens malposition) or incomplete follow-up data; (6) patients with corneal edema as indicated by both slit-lamp examination and corneal thickness (CCT) measured by IOLMaster 700 one week postoperatively. Ultimately, a total of 93 cataract patients (involving 123 eyes) were included in this study.
Ocular Measurements
Measurement and Calculation Process
Participants were measured sequentially by the same technician using the IOLMaster 700 and Sirius in the same dark room. For each eye, only the most recent complete and valid single measurement result of each parameter (AL, K1, K2, ACD, WTW) was retained for subsequent analysis. To avoid systematic bias caused by repeated measurements, the average value of multiple measurements was not taken. For both devices, scans with insufficient signal strength (signal-to-noise index<10 for Sirius; composite image quality index<5 for IOLMaster 700) were excluded, ensuring only high-confidence measurements entered the analysis.
All raw data were immediately subjected to irreversible anonymization after collection, and any identifiable information was replaced with a unique study identification number. The anonymized data were then uploaded, stored, and backed up in real-time through an Electronic Data Capture and Management System (EDC) registered with the National Medical Products Administration of China (platform URL: [study.empoweredc.com] (https://study.empoweredc.com), Shanghai), ensuring data integrity and traceability.
The AL, K1, K2, ACD, and WTW measurements obtained from the IOLMaster 700 were entered into the Barrett Universal II Formula (available at [https://calc.apacrs.org/barrett_universal2105/]). An individualized target SE was set, and the system generated the recommended IOL power, denoted as D0. The predicted refractive power (PRP) corresponding to this D0 was recorded as I-PRP for the IOLMaster 700 group. Keeping the IOL power D0 constant, the corresponding measurements of K1, K2, ACD, and WTW from the Sirius were manually entered into the Barrett Universal II Formula. The predicted refractive power calculated under this D0 was recorded as S-PRP.
Surgical Procedure and Postoperative Follow-Up Process
All cataract phacoemulsification surgeries with monofocal IOL implantation were performed by the same experienced surgeon (YK.H).: After routine preoperative disinfection and topical anesthesia with full mydriasis, a lid speculum was placed. Viscoelastic was injected through a 2.6 mm clear corneal tunnel incision. A continuous curvilinear capsulorhexis of 4.5–5.5 mm was performed. The nucleus was emulsified and cortex was completely removed while preserving the posterior capsule. A foldable monofocal IOL was implanted into the capsular bag using an injector and centered. After removing the viscoelastic and confirming the IOL position and normal intraocular pressure, the incision was self-sealed. On postoperative day 1 and week 1, best-corrected visual acuity, refraction, IOLMaster 700 (for CCT measurement), and slit-lamp examination were performed. Patients with posterior capsule rupture during surgery, those requiring a tension ring implantation, and those with corneal edema or abnormal CCT on slit-lamp examination at postoperative week 1 were excluded. The final refractive data were based on the stable results at postoperative week 1.
Comparison of Measurement Accuracy Between IOLMaster 700 and Sirius
At postoperative week 1, the best-corrected visual acuity (BCVA), Sphere, Cylinder, and SE were recorded. The Predicted Refractive Errors (ΔPRE) were calculated by subtracting the SE from the PRP. These were denoted as I-ΔPRE (ΔPRE of IOLMaster 700) and S-ΔPRE (ΔPRE of Sirius). The absolute values were then obtained as |I-ΔPRE| and |S-ΔPRE|. All values were anonymized and entered into the EDC system for subsequent statistical analysis.
Statistical Analysis
Statistical analyses were performed using R software (version 4.3.1; R Foundation for Statistical Computing) and the EasyR platform (www.easyrdata.com, Solutions, Inc., Shanghai). Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are described as frequency (percentage). The normality of data distribution was assessed using the Kolmogorov–Smirnov test. For normally distributed continuous variables, paired t-tests were used to evaluate differences in means; for non-normally distributed continuous variables, the Wilcoxon signed-rank test was used to assess differences in medians. The consistency of categorical variables was analyzed using Cohen’s kappa coefficient to evaluate the agreement between different measurement methods. A two-sided P value < 0.05 was considered statistically significant. To control for type I error, Bonferroni correction was applied for multiple comparisons. Specifically, it was applied to the primary comparisons of device prediction accuracy (ΔPRE and |ΔPRE| between IOLMaster 700 and Sirius), with an adjusted significance level of p < 0.025. The agreement between predicted postoperative refraction and postoperative SE was assessed using Bland-Altman (BA) analysis.
A post-hoc power analysis was performed to assess the adequacy of our sample size. Based on a minimally clinically important difference of 0.25 D in mean paired prediction errors and the observed standard deviation of paired differences (0.62 D) from our 123 paired eyes, the statistical power to detect this difference using a paired t-test at α=0.05 (two-sided) was 99.3%, exceeding the conventional threshold of 80%. The analysis was conducted using PASS software (NCSS, LLC).
Results
Patients’ Characteristics
A total of 93 cataract patients (40 males and 53 females) were included in this study, involving 123 eyes (61 right eyes and 62 left eyes), with a mean age of 65.38±14.84 years.
The median AL of the enrolled eyes was 23.39 mm (interquartile range, IQR 22.86 to 24.95 mm). The K1, K2, ACD, and WTW values measured by IOLMaster 700 and Sirius are shown in Table 1. At the first postoperative week, the median BCVA was 0.10 (IQR 0.00 to 0.30). Manifest refraction revealed a median spherical error of −0.50 D (IQR −2.00 to 0.25), a median cylindrical error of −0.75 D (IQR −1.25 to −0.38), and a median SE of −0.88 D (IQR −2.44 to −0.25).
 |
Table 1 The Numerical Values of Various Parameters for IOLMaster 700 and Sirius |
Ocular Parameter Measurements
Table 2 compares the measurements of ACD, WTW, K1, and K2 obtained with IOLMaster 700 and Sirius. Numerically, no statistically significant differences were found between the two devices for K1, K2, or ACD (all p > 0.05); however, WTW values differed significantly (p < 0.05). The PRP was greater than the post-operative SE in the majority of patients.
 |
Table 2 Comparison of Measurement Data Between IOLMaster 700 and Sirius |
The scatter plot (Figure 1) displays the ΔPRE distribution for each patient. Overall, both devices produced positive ΔPRE shifts. The median ΔI-PRE was 0.41 D (IQR 0.01 to 0.94), smaller than the median ΔS-PRE of 0.73 D (IQR 0.26 to 1.21), p < 0.05. The absolute error |ΔI-PRE| was 0.61 D (IQR 0.29 to 0.98), also lower than |ΔS-PRE| of 0.80 D (IQR 0.49 to 1.30), p < 0.05, indicating that IOLMaster 700 yielded predictions closer to the actual postoperative result.
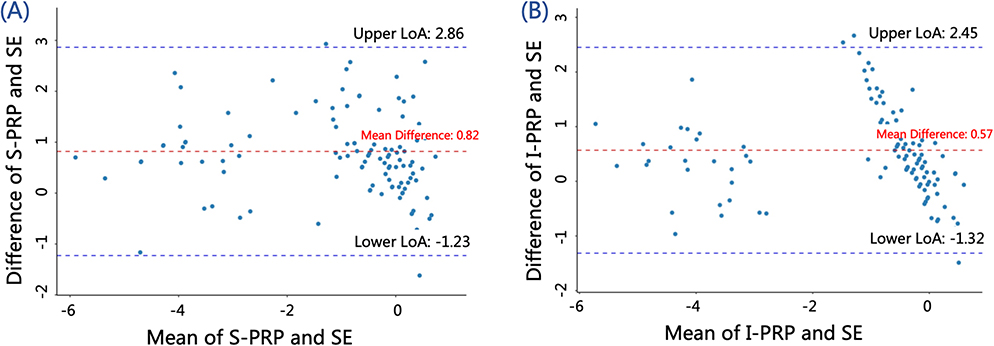 |
Figure 1 Scatter plot of ΔPRE distribution between IOLMaster 700 and Sirius. (A) Distribution of ΔPRE for IOLMaster 700. Each dot represents the measurement error for an individual patient, the red line indicates the average error, and the shaded area represents the 95% confidence interval. (B) Distribution of ΔPRE for Sirius. Each dot represents the measurement error for an individual patient, the red line indicates the average error, and the shaded area represents the 95% confidence interval. |
When an error within ±0.50 D was defined as accurate prediction, 56 eyes (45.5%) in the IOLMaster 700 group met this criterion, compared with 32 eyes (26.0%) in the Sirius group. The IOLMaster 700 group achieved a significantly higher prediction accuracy (p < 0.05).
Inter-Device Agreement Analysis
We performed Bland-Altman analyses between the PRP and the post-operative SE for both IOLMaster 700 and Sirius (Figure 2), using a clinically acceptable threshold of ±0.50 D. For IOLMaster 700, the mean difference (I-PRP − SE) was 0.57 D, with 95% limits of agreement (LoA) from −1.32 to 2.45 D, beyond the ±0.50 D range. Similarly, for Sirius, the mean difference (S-PRP − SE) was 0.82 D, with 95% LoA from −1.23 to 2.86 D, again exceeding the acceptable limits. Thus, both devices demonstrate substantial prediction errors and poor agreement with the actual post-operative SE.
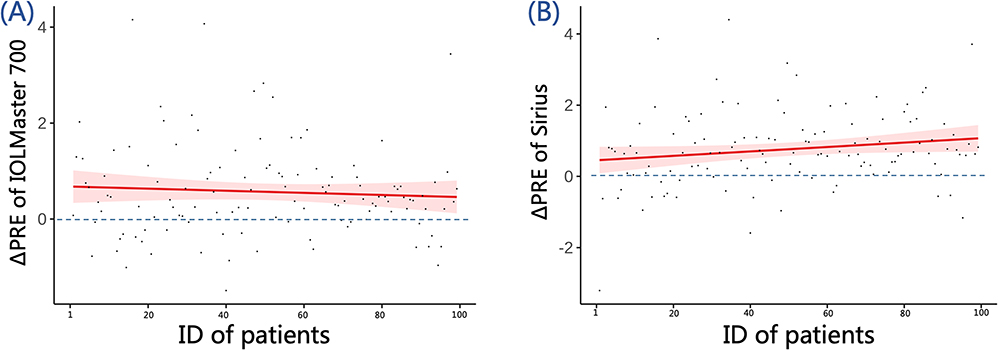 |
Figure 2 Bland-Altman analysis of PRP from IOLMaster 700 and Sirius versus the post-operative SE. (A) Bland-Altman plot for S-PRP and SE, showing the mean difference of 0.82 and 95% limits of agreement at −1.23 and 2.86. (B) Bland-Altman plot for I-PRP and SE, showing the mean difference of 0.57 and 95% limits of agreement at −1.32 and 2.45. |
Axial-Length Subgroup Analysis
To investigate whether prediction errors differ between normal and long axial lengths, we divided the cohort into two groups: eyes with AL>25 mm (long-AL) and those with AL≤25 mm (normal-AL). Subgroup analysis showed that the mean post-operative SE was −3.88D((IQR −4.72 to −1.34) in the long-AL group and −0.62D(IQR −1.38 to 0.00) in the normal-AL group, with significant difference (p < 0.05). However, neither ΔPRE nor |ΔPRE| differed between the two groups (p > 0.05) (Table 3), indicating that although the intended post-operative refractions were distinct, the magnitude of prediction error was comparable.
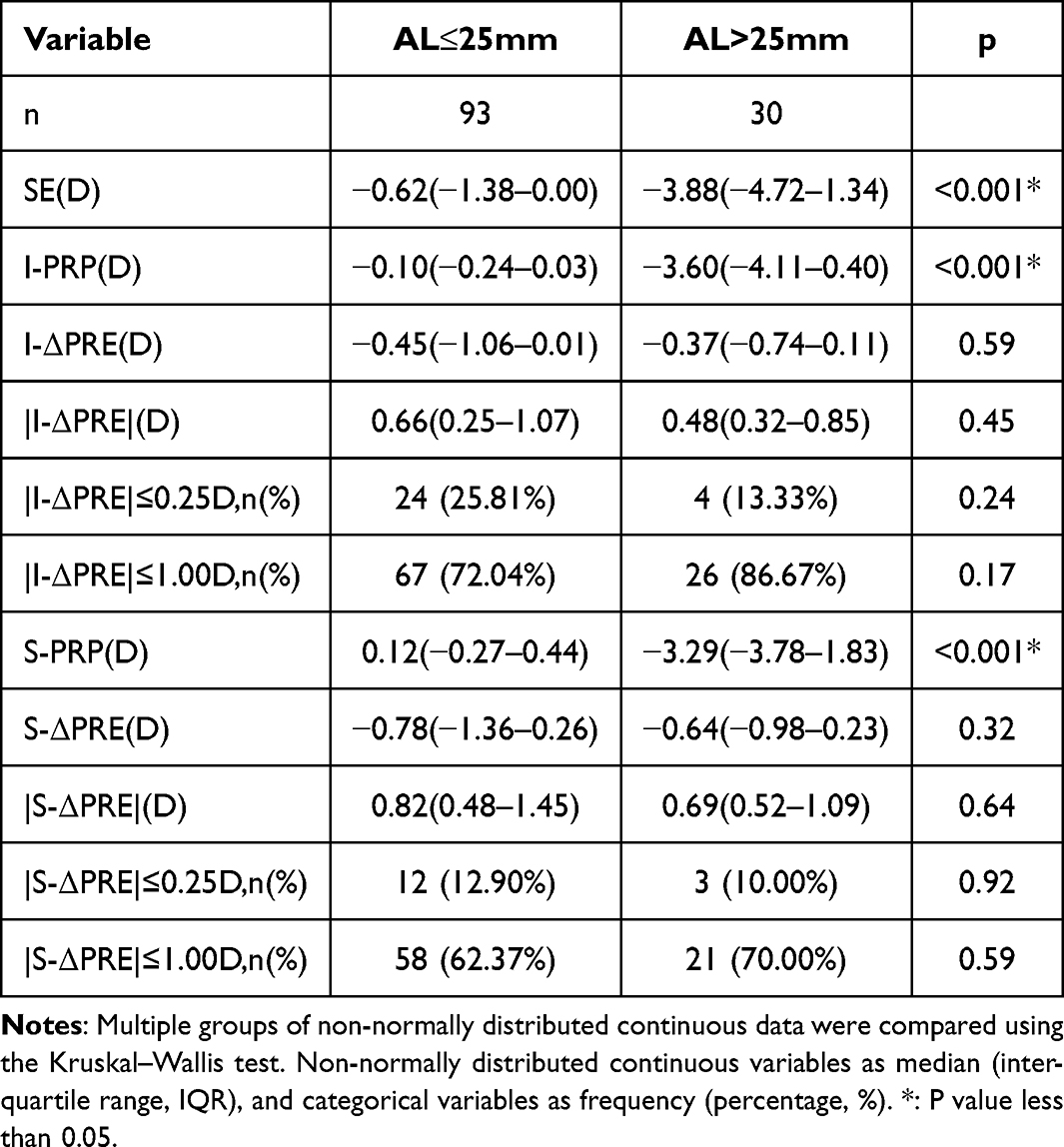 |
Table 3 Comparison of Predictive Errors in Axial Length Subgroups |
Discussion
Modern cataract surgery has entered the era of precision refractive surgery, aiming not only at visual rehabilitation but also at high-quality visual function. According to multicenter data from the European Registry of Quality Outcomes in Cataract and Refractive Surgery, post-operative refractive error is a major reason for suboptimal visual outcomes.19,20 Refractive drift after surgery leaves about 12% of patients with a spherical error of ≥1.0 D,21 which markedly compromises visual quality and quality of life.22 Biometric error is one of the most significant contributors to this post-operative refractive drift.
By utilizing a tunable swept-source laser, SS-OCT delivers markedly higher axial resolution, offering distinct advantages in ophthalmic diagnosis and surgical planning.7 Sirius employs a dual platform that combines a rotating Scheimpflug camera with Placido-disk topography, enabling simultaneous acquisition of high-precision data from both the anterior and posterior corneal surfaces.23 Under fixed Barrett Universal II formula and target IOL power, we compared the refractive-drift characteristics of IOLMaster 700 and Sirius. Both devices produced a positive prediction error; however, the median ΔPRE was significantly lower with IOLMaster 700 (0.41 D; IQR 0.01 to 0.94) than with Sirius (0.73 D; IQR 0.26 to 1.21), p < 0.05, reflecting a smaller overall shift. Moreover, the absolute prediction error was significantly lower with IOLMaster 700 (0.61 D; IQR 0.29 to 0.98) than with Sirius (0.80 D; IQR 0.49 to 1.30), p < 0.05. Suggesting that, within the Barrett Universal II framework and using SE as the benchmark, the raw biometric data from IOLMaster 700 yield predictions closer to the actual post-operative SE. We noted a significant between-device difference in WTW measurements (Table 2, p < 0.001); because WTW directly enters the Barrett Universal II formula’s effective lens position estimate, this discrepancy may partly explain the observed prediction error.
Subgroup analysis further revealed no significant difference in prediction error between long axial-length eyes (AL > 25 mm) and normal axial-length eyes (AL ≤ 25 mm); elongated AL did not increase the prediction error. Consequently, for patients with long eyes, our findings continue to favor the use of IOLMaster 700 combined with the Barrett Universal II formula. Multiple studies have compared the refractive status at 1 week and 4 months after monofocal IOL implantation and found no statistically significant differences,24,25 indicating that 1 week postoperatively is a reliable time point for short-term follow-up. However, capsular bag contraction becomes significantly more pronounced from 1 month onward, markedly affecting IOL position and postoperative refractive status, with considerable individual variability that may introduce additional astigmatic factors.26,27 Therefore, to minimize the confounding effect of capsular contraction on astigmatism measurements, we selected 1 week after surgery as the observation time point for short-term refractive stability. Longer-term follow-up is ongoing and will be reported separately.
Limitations
Limitations of this study include: (1) the single-center design restricts the generalizability of the findings; (2) only one formula was employed, without comparison across multiple formulas. Future studies should incorporate multicenter data and multi-formula analyses to further explore the interplay between devices and calculation algorithms; (3) Although the overall sample size was adequate, the long-axial-length subgroup (AL > 25 mm, n = 30) was relatively small, limiting statistical power and the robustness of conclusions within this stratum; larger prospective cohorts are needed to validate these preliminary findings. (4)Post-operative follow-up in this study was limited to one week, which may not capture long-term refractive stability. Future study protocols adopting postoperative exams at three- and six month periods would generate improved insights regarding postoperative refractive stability between both devices.
Conclusion
In summary, When the Barrett Universal II formula is used, IOLMaster 700 generates significantly more accurate refractive predictions than Sirius, exhibiting a smaller positive drift and a lower absolute prediction error. This advantage persists irrespective of axial length. IOLMaster 700 outperforms Sirius in refractive prediction accuracy under the Barrett Universal II formula. This study systematically characterized the error profiles and postoperative parameter trends of both instruments, showing that using IOL Master 700 in preoperative planning and intraocular lens power selection can be linked to lesser postoperative refraction disparities. The utilization of SS-OCT in contemporary biometry systems creates an opportunity for integrating Artificial Intelligence models to enhance their predictive accuracy. This enabling surgeons to fine-tune surgical planning and effectively reduce actual refractive error.
Value Statement
Known prior to this work: Prior studies mainly compared single-parameter repeatability between IOLMaster 700 and Sirius; their comparative refractive prediction performance under any formula was unexplored.
What this paper adds: 1) First prospective, paired-eye study to quantify Barrett Universal II prediction error for IOLMaster 700 versus Sirius using identical IOL power and post-operative SE as ground truth. 2) Demonstrates IOLMaster 700 yields significantly smaller median absolute error (0.61 D vs 0.80 D) and higher ±0.50 D accuracy (45.5% vs 26.0%) than Sirius.
Abbreviations
ACD, Anterior Chamber Depth; SS-OCT, Swept-Source Optical Coherence Tomography; SE, Spherical Equivalent; AL, Axial Length; K1, flat keratometry; K2, steep keratometry; WTW, White-to-White; CCT, Central Corneal Thickness; IOL, Intraocular Lens; PRP, Predicted Refraction Power; BCVA, Best-Corrected Visual Acuity; ΔPRE, Predicting refractive errors; SD, Standard Deviation; BA analysis, Bland-Altman analysis; LoA, Limits of Agreement.
Data Sharing Statement
The de-identified participant data that support the findings of this study are available from the corresponding author upon reasonable request and with approval of the Medical Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Ethics Statement
This study is a prospective, observational diagnostic accuracy study that adheres to the Declaration of Helsinki and the STARD guidelines, and was approved by the Medical Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. The ethical approval number is 2024-0280, and the review date is April 19, 2024.
Acknowledgments
The authors thank Mr. G.Z for assistance in data acquisition and Solution (Shanghai) Science and Technology Co., Ltd. for providing the EDC system and statistical consultation. We also acknowledge the support of PubMed.pro for literature retrieval and summarization, which greatly facilitated the research process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to beaccountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Khoramnia R, Auffarth G, Łabuz G, Pettit G, Suryakumar R. Refractive outcomes after cataract surgery. Diagnostics. 2022;12(2):243. doi:10.3390/diagnostics12020243
2. Kieval JZ, Al-Hashimi S, Davidson RS, et al. ASCRS refractive cataract surgery subcommittee. Prevention and management of refractive prediction errors following cataract surgery. J Cataract Refract Surg. 2020;46(8):1189–10. doi:10.1097/j.jcrs.0000000000000269
3. Schallhorn SC, Hettinger KA, Pelouskova M, et al. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47(8):991–998. doi:10.1097/j.jcrs.0000000000000560
4. Xu DY, Wang J. Factors affecting the refractive error after cataract surgery. Int Ophthalmol. 2025;45(1):163. doi:10.1007/s10792-025-03543-0
5. Lee NS, Ong K. Factors contributing to long-term refractive error after cataract surgery. Int Ophthalmol. 2023;43(7):2335–2340. doi:10.1007/s10792-022-02630-w
6. Carr F, Gangwani V. Refractive Surprise after cataract surgery secondary to smeared optics of swept-source optical coherence tomography biometer: a case report. BMC Ophthalmol. 2020;20(1):352. doi:10.1186/s12886-020-01629-0
7. Montés-Micó R, Pastor-Pascual F, Ruiz-Mesa R, Tañá-Rivero P. Ocular biometry with swept-source optical coherence tomography. J Cataract Refract Surg. 2021;47(6):802–814. doi:10.1097/j.jcrs.0000000000000551
8. Kanclerz P, Khoramnia R, Wang X. Current Developments in Corneal Topography and Tomography. Diagnostics. 2021;11(8):1466. doi:10.3390/diagnostics11081466
9. Mackenbrock LHB, Łabuz G, Yildirim TM, Auffarth GU, Khoramnia R. Automatic quantitative assessment of lens opacities using two anterior segment imaging techniques: correlation with functional and surgical metrics. Diagnostics. 2022;12(10):2406. doi:10.3390/diagnostics12102406
10. Muzyka-Woźniak M, Oleszko A, Grzybowski A. Measurements of anterior and posterior corneal curvatures with OCT and Scheimpflug biometers in patients with low total corneal astigmatism. J Clin Med. 2022;11(23):6921. doi:10.3390/jcm11236921
11. Lu AQ, Poulsen A, Cui D, et al. Repeatability and comparability of keratometry measurements obtained with swept-source optical coherence and combined dual Scheimpflug-Placido disk-based tomography. J Cataract Refract Surg. 2020;46(12):1637–1643. doi:10.1097/j.jcrs.0000000000000346
12. Xia T, Martinez CE, Tsai LM. Update on Intraocular Lens Formulas and Calculations. Asia Pac J Ophthalmol. 2020;9(3):186–193. doi:10.1097/APO.0000000000000293
13. Shetty N, Kaweri L, Koshy A, Shetty R, Rmma N, Sinha Roy A. Repeatability of biometry measured by three devices and its impact on predicted intraocular lens power. J Cataract Refract Surg. 2021;47(5):585–592. doi:10.1097/j.jcrs.0000000000000494
14. Kim SY, Lee SH, Kim NR, Chin HS, Jung JW. Accuracy of intraocular lens power calculation formulas using a swept-source optical biometer. PLoS One. 2020;15(1):e0227638. doi:10.1371/journal.pone.0227638
15. Kanclerz P, Hoffer KJ, Bazylczyk N, Wang X, Savini G. Optical biometry and IOL calculation in a commercially available optical coherence tomography device and comparison with pentacam AXL. Am J Ophthalmol. 2023;246:236–241. doi:10.1016/j.ajo.2022.09.022
16. Stopyra W, Langenbucher A, Grzybowski A. Intraocular lens power calculation formulas–a systematic review. Ophthalmol Ther. 2023;12(6):2881–2902. doi:10.1007/s40123-023-00799-6
17. Roberts TV, Hodge C, Sutton G, Lawless M. contributors to the Vision Eye Institute IOL outcomes registry. Comparison of Hill-radial basis function, Barrett Universal II and current third generation formulas for the calculation of intraocular lens power during cataract surgery. Clin Exp Ophthalmol. 2018;46(3):240–246. doi:10.1111/ceo.13034
18. Al Barri L, Mercea N, Ionela-Iasmina Y, Munteanu M, Stanca HT. Evaluation of refractive predictive accuracy in intraocular lens power calculations: a comparative study of Swept-source optical coherence tomography and optical low-coherence interferometry. J Clin Med. 2025;14(4):1201. doi:10.3390/jcm14041201
19. Lundström M, Dickman M, Henry Y, et al. Risk factors for refractive error after cataract surgery: analysis of 282 811 cataract extractions reported to the European Registry of Quality Outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2018;44(4):447–452. doi:10.1016/j.jcrs.2018.01.031
20. Lundström M, Dickman M, Henry Y, et al. European Society of Cataract and Refractive Surgeons Femtosecond Laser–Assisted Cataract Surgery Study Collaborators. Femtosecond laser-assisted cataract surgeries reported to the European Registry of Quality Outcomes for Cataract and Refractive Surgery: baseline characteristics, surgical procedure, and outcomes. J Cataract Refract Surg. 2017;43(12):1549–1556. doi:10.1016/j.jcrs.2017.09.029
21. Ostri C, Holfort SK, Fich MS, Riise P. Automated refraction is stable 1 week after uncomplicated cataract surgery. Acta Ophthalmol. 2018;96(2):149–153. doi:10.1111/aos.13545
22. Grzybowski A, Kanclerz P, Muzyka-Woźniak M. Methods for evaluating quality of life and vision in patients undergoing lens refractive surgery. Graefes Arch Clin Exp Ophthalmol. 2019;257(6):1091–1099. doi:10.1007/s00417-019-04270-w
23. Sun B, Hu X, Peng X, et al. Comparative study of the corneal morphological characteristics of keratoconus evaluated using Pentacam, Sirius, and CASIA2. Photodiagnosis Photodyn Ther. 2025;53:104612. doi:10.1016/j.pdpdt.2025.104612
24. Nanda AK, Panda BB, Swain A, Balakrishnan L. Determination of the time of refractive stability after uneventful phacoemulsification in Indian eyes. World J Exp Med. 2024;14(2):95016. doi:10.5493/wjem.v14.i2.95016
25. Charlesworth E, Alderson AJ, de Juan V, Elliott DB. When is refraction stable following routine cataract surgery? A systematic review and meta-analysis. Ophthalmic Physiol Opt. 2020;40(5):531–539. doi:10.1111/opo.12719
26. Feng L, Weeber H, Rozema J. Finite element model of capsular bag contraction and its effect on IOL position. Exp Eye Res. 2025;259:110564. doi:10.1016/j.exer.2025.110564
27. Wang Y, Wang W, Zhu Y, Xu J, Luo C, Yao K. Comparison study of anterior capsule contraction of hydrophilic and hydrophobic intraocular lenses under the same size capsulotomy. Transl Vis Sci Technol. 2022;11(1):24. doi:10.1167/tvst.11.1.24
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.