Back to Journals » Clinical Ophthalmology » Volume 20
Comparative Study of ICL V4c Decentration in Vertical vs Horizontal Implantation: Association with Angle Alpha and Validation of Equivalent Visual Quality
Authors Tang Z, Wu Z ![]() , Guo Z, Zheng L, Zhou X
, Guo Z, Zheng L, Zhou X ![]() , Liu S
, Liu S
Received 6 December 2025
Accepted for publication 24 February 2026
Published 14 April 2026 Volume 2026:20 581238
DOI https://doi.org/10.2147/OPTH.S581238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhongjun Tang,1– 4,* Zhuotong Wu,2– 4,* Ziyi Guo,2– 4 Linda Zheng,5,6 Xingtao Zhou,2– 4 Shengtao Liu2– 4
1Department of Ophthalmology, Minhang Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Ophthalmology and Optometry, Eye and ENT Hospital, Fudan University, Shanghai, People’s Republic of China; 3NHC Key Laboratory of Myopia (Fudan University); Key Laboratory of Myopia, Chinese Academy of Medical Sciences, Shanghai, People’s Republic of China; 4Shanghai Research Center of Ophthalmology and Optometry, Shanghai, People’s Republic of China; 5Sydney Eye Hospital, Sydney, NSW, Australia; 6Royal Prince Alfred Hospital, Camperdown, NSW, Australia
*These authors contributed equally to this work
Correspondence: Shengtao Liu, Department of Ophthalmology and Optometry, Eye and ENT Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected] Xingtao Zhou, Department of Ophthalmology and Optometry, Eye and ENT Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: To compare the decentration of the Implantable Collamer Lens (ICL) V4c and its impact on visual quality between vertical and horizontal implantation techniques.
Methods: 50 patients (80 eyes) were assigned to horizontal (40 eyes) or vertical (40 eyes) implantation groups. Preoperative and 6-month postoperative evaluations included uncorrected (UDVA) and corrected distance visual acuity (CDVA), refractive status, corneal topography, and wavefront aberration analysis. Decentration was measured using the OPD-Scan III aberrometer, compared between implantation methods, and analyzed for associations with preoperative angles α and κ.
Results: At 6 months, 100% of horizontal and 97.5% of vertical implantation eyes achieved UDVA ≥ 20/20, with all eyes maintaining or improving CDVA. Mean decentration was similar between groups (horizontal: 0.42 ± 0.18 mm; vertical: 0.42 ± 0.19 mm; p = 0.915), with temporal displacement predominating. Angle α significantly correlated with decentration in both groups (p = 0.016; p = 0.017), while angle κ showed no association (p > 0.05). The change of higher-order aberrations did not differ between groups (p > 0.05), and decentration magnitude did not clinically affect optical quality (p > 0.05 for all aberration parameters).
Conclusion: Vertical and horizontal ICL V4c implantation demonstrated comparable centration and visual outcomes. Decentration was significantly associated with preoperative angle α, underscoring the clinical importance of angle α assessment for optimal ICL positioning.
Keywords: ICL V4c, decentration, vertical implantation, visual outcomes, angle alpha, wavefront aberrations
Introduction
The global burden of visual impairment persists, largely due to uncorrected refractive errors, while myopia prevalence shows a consistent upward trend.1 In this context, the Implantable Collamer Lens (ICL) V4c, an advanced phakic intraocular lens, has emerged as a key solution for myopia correction. Although extensive evidence supports the safety and efficacy of ICL procedures,2–6 greater emphasis is now placed on attaining highly accurate refractive corrections and superior visual acuity after surgery. The glare, halos, and starburst phenomena that occur during lens decentration can significantly affect patient visual outcomes.7–10
Optimal positioning of an ICL requires alignment between the center of the optical zone and the visual axis. However, owing to the fixation of the ICL in the ciliary sulcus, anatomical variations in the sulcal structure and haptic positioning can prevent ideal alignment.11,12 ICL optical zone decentration can compromise visual quality;13 however, few studies have investigated the factors influencing this decentration.
With an enhanced understanding of the ciliary sulcus anatomy, vertical implantation has gained increasing acceptance as a management strategy for vault and rotational stability. Prior research has demonstrated that vertical implantation achieves superior vault and rotational stability compared with horizontal implantation, establishing it as a safe and effective approach for myopia correction.14–17 However, previous studies examining ICL positioning and decentration have primarily focused on horizontal implantation, with limited investigations into vertical implantation outcomes, and without comparative assessment of visual quality between the two approaches. Here, we aimed to compare ICL decentration and visual outcomes between vertical and horizontal implantation techniques, while also identifying other contributing and associated factors.
Methods
Patient Cohort
This retrospective analysis evaluated 50 patients (80 eyes) who received ICL V4c implantation at the Eye and ENT Hospital of Fudan University, Shanghai, China from May to August 2024. Eligible eyes met the following criteria: anterior chamber depth (ACD) ≥ 2.8 mm and endothelial cell density ≥ 2500 cells/mm2. Exclusion criteria comprised perioperative or postoperative complications (eg, elevated intraocular pressure, significant inflammation, or lens opacity). The study adhered to the tenets of the Declaration of Helsinki and received institutional ethics approval (Ethics Committee of the Eye and ENT Hospital, Fudan University). Written informed consent was obtained from all the patients.
Surgical Method
All ICL implantations were performed by a single experienced surgeon (XZ). The ICL size was based on the white-to-white (WTW) distance and ACD (Pentacam, Oculus Optikgeräte, Wetzlar, Germany). The choice of ICL resizing and implantation orientation followed a standardized protocol based on preoperative anatomical measurements, as previously reported.18 To establish the ICL diopter power, we selected the myopic and astigmatic powers that provided a refractive outcome closest to zero diopters. All implanted lenses in this study were spherical ICL V4c models; no toric ICLs were used.
Preoperatively, after topical anesthesia (0.4% oxybuprocaine), all patients were positioned upright with their gaze fixed on a far target. Cyclotorsion adjustment markers were applied at the 3-, 9-, and 12-o’clock positions using a slit beam to account for potential cyclotorsion during the procedure.
Dilating eye drops and topical anesthesia were administered before surgery. A 3.0-mm clear corneal incision was created temporally. The ICL V4c was then inserted along the predetermined axis (horizontal or vertical orientation) anterior to the native crystalline lens. A standardized ICL surgical protocol was followed, as previously reported.19 Postoperatively, topical antibiotics (0.5% levofloxacin; Santen) and steroids (1.0% prednisolone acetate, Pred Forte; Allergan, Irvine, CA, USA) were administered four times daily for 7 days. Additionally, a topical nonsteroidal anti-inflammatory drug (pranoprofen, Senju, Osaka, Japan) was applied four times daily for 14 days.
Preoperative and Postoperative Assessment
A complete ophthalmic evaluation was performed both before surgery and at the 6-month postoperative follow-up, encompassing visual acuity assessments including uncorrected (UDVA) and corrected distance visual acuity (CDVA) measured with Snellen charts, along with comprehensive refractive evaluation through both manifest and cycloplegic techniques. The examination protocol further incorporated anterior and posterior segment analysis via slit lamp biomicroscopy and fundoscopy, intraocular pressure measurement using non-contact tonometry, and detailed corneal assessment through topography and pachymetry (Pentacam, Oculus, Germany). Additional biometric parameters included WTW distance and axial length measurements (IOL Master, Carl Zeiss, Germany), anterior chamber depth evaluation, and corneal endothelial cell density quantification (SP-3000P specular microscope, Topcon, Japan). Advanced imaging modalities consisted of optical coherence tomography (Optovue, USA) and ultrasound biomicroscopy (Quantel Medical, France) for comprehensive ocular structure analysis.
Decentration and Aberration Measurements
Higher-order aberrations (HOAs) were measured preoperatively and 6 months postoperatively using an OPD-Scan III aberrometer (Nidek Co., Ltd., Gamagori, Japan) for a central 4-mm analytical zone with higher-order aberrations up to the sixth order of the Zernike polynomials. The root mean square value was used to quantify whole-eye HOAs. ICL decentration was quantitatively assessed using the OPD-Scan III aberrometer under standardized mesopic lighting conditions (3 cd/m2) to minimize pupil diameter effects on lens positioning. During measurement, patients maintained fixation on the device’s point light source, with the visual axis defined as the line connecting this target to the fovea. The system’s retrobulbar illumination analysis mode simultaneously identified both the visual axis and the ICL V4c’s anatomical center (360 μm central hole). Decentration was calculated as the linear displacement between these two reference points, consistent with established methodologies described in prior studies.20,21
Statistical Analysis
Statistical analysis was conducted with IBM SPSS Statistics (v20.0, SPSS Inc., Chicago, IL). Continuous variables were expressed as mean ± standard deviation or median with interquartile range (IQR) following verification of normal distribution using the Shapiro–Wilk test. Pearson or Spearman was employed based on the distribution characteristics of the data. Polar coordinate plots illustrating the overall distribution of ICL postoperative eccentricity were generated using R (version 4.4.3, R Foundation for Statistical Computing, Vienna, Austria). Intergroup comparisons were performed with independent t-tests or Mann–Whitney U-Test according to data distribution, while variable relationships were assessed through simple linear regression. A p-value threshold of 0.05 was established for determining statistical significance.
Results
Baseline Characteristics
The study cohort comprised 50 participants (80 eyes) receiving ICL implantation, with the horizontal implantation subgroup consisting of 12 male (48.0%) and 13 female (52.0%) patients. These subjects demonstrated a mean age of 21.0 ± 2.3 years (range 18 to 26 years) and presented with moderate to high myopia, as evidenced by a mean spherical refraction of −6.87 ± 2.08 D (range −11.50 to −3.50 D). The median and IQR of preoperative astigmatic refraction was −1.00 (0.75) D, and mean preoperative refractive spherical equivalent was −7.36 ± 2.06 D (range: −12.00 to −4.25 D).
The vertical implantation cohort comprised 25 patients (44.0% male, n = 11; 56.0% female, n = 14) with comparable demographic characteristics, showing a mean age of 21.2 ± 2.4 years (age range: 18 to 26 years). The mean preoperative refractive sphere was −6.67 ± 1.87 D (range: −10.50 to −3.00 D), median and IQR of preoperative astigmatic refraction was −1.00 (0.25) D, and mean refractive spherical equivalent was −7.17 ± 1.85 D (range: −11.13 to −3.50 D).
Table 1 presents the baseline demographic and clinical characteristics of the study participants, all preoperative parameters showed no statistically significant differences between the two groups (P > 0.05). All implantation procedures were completed without intraoperative complications, and the postoperative course remained uneventful, with no occurrence of sight-threatening adverse events throughout the observation period.
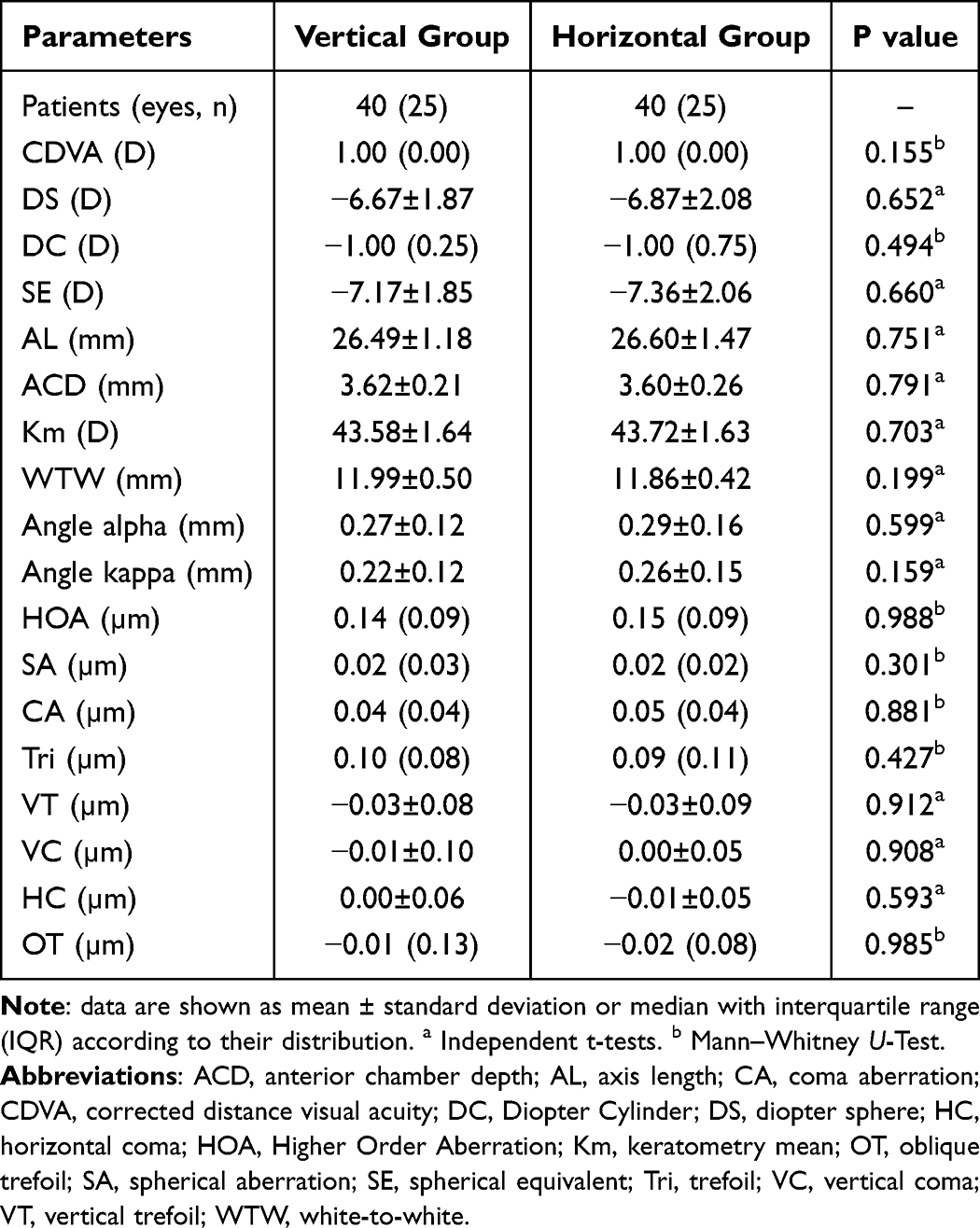 |
Table 1 Preoperative Patient Demographics and Clinical Characteristics |
Postoperative Visual and Refractive Outcomes
Six months postoperatively, visual acuity outcomes demonstrated excellent results across both surgical groups. In the horizontal cohort, all operated eyes (40/40, 100%) attained UDVA of 20/20 or superior, while the vertical group showed nearly equivalent success (39/40 eyes, 97.5%). Notably, CDVA was maintained or enhanced in every case (40/40, 100%) for both implantation approaches, as illustrated in Figure 1A and B. Regarding predictability, the regression equation for achieved versus attempted spherical equivalent (SE) correction was

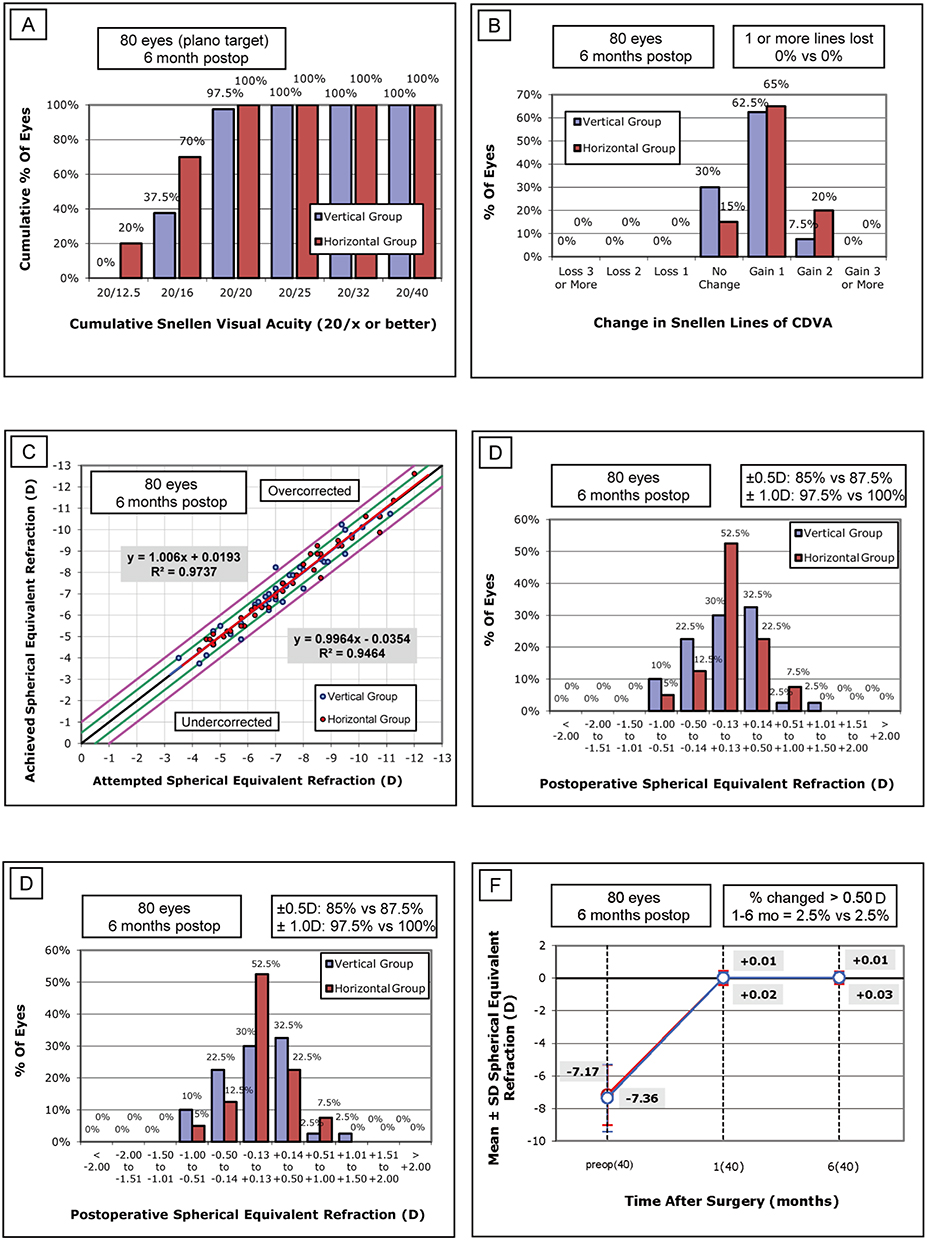 |
Figure 1 Visual outcomes at 6 months postoperatively. (A) Uncorrected Distance Visual Acuity (UDVA); (B) Change in Corrected Distance Visual Acuity (CDVA); (C) Spherical Equivalent Refraction attempted versus achieved; (D) Postoperative Spherical Equivalent Refraction accuracy; (E) Postoperative Refractive Astigmatism; (F) Stability of Spherical Equivalent Refraction over time. |
(R2 = 0.9737) in the horizontal group and

(R2 = 0.9464) in the vertical group (Figure 1C). At 6 months postoperatively for spherical equivalent accuracy, 87.5% of horizontally implanted eyes (35/40) and 85.0% of vertically implanted eyes (34/40) achieved results within ±0.50 D of the target, with all horizontal cases (100%) and 97.5% of vertical cases (39/40) falling within ±1.00 D (Figure 1D). Astigmatic correction presented 80% (32/40) and 75% (30/40) of eyes in the horizontal and vertical groups respectively attaining ≤ 0.50 D residual cylinder, while all eyes (100%) in both groups maintained ≤ 1.00 D (Figure 1E). Refractive stability was exceptional, with merely 2.5% of cases (1/40 per group) exhibiting spherical equivalent variations > 0.5 D during follow-up (Figure 1F).
Postoperative Optical Zone Decentration
Quantitative analysis of ICL decentration revealed comparable results between surgical approaches, with mean total displacement measuring 0.42 ± 0.18 mm (range 0.11 to 0.91 mm) for horizontal implantation and 0.42 ± 0.19 mm (range 0.08 to 0.81 mm) for vertical implantation (p = 0.915). The decentration was vectorially decomposed. In the horizontal implantation group, the mean horizontal decentration was 0.06 ± 0.39 mm (range: −0.62 to 0.76 mm), and the mean vertical decentration was 0.10 ± 0.23 mm (range: −0.59 to 0.63 mm). In the vertical implantation group, the mean horizontal decentration was −0.02 ± 0.41 mm (range: −0.74 to 0.81 mm), and the mean vertical decentration was 0.00 ± 0.21 mm (range: −0.45 to 0.50 mm). No statistically significant differences were observed in either the horizontal or vertical vector components of decentration between the two groups (P = 0.373 and P = 0.055, respectively; Table 2). Spatial distribution analysis (Figure 2) identified a consistent temporal displacement pattern for the central aperture in both techniques. In both the vertical and horizontal implantation groups, 77.5% of eyes exhibited temporal ICL eccentricity. Specifically, in the vertical implantation group, 18 eyes (45.0%) were located in the inferotemporal quadrant, 13 eyes (32.5%) in the superotemporal quadrant, 5 eyes (12.5%) in the superonasal quadrant, and 4 eyes (10.0%) in the inferonasal quadrant. In the horizontal implantation group, 18 eyes (45.0%) were located in the superotemporal quadrant, 13 eyes (32.5%) in the inferotemporal quadrant, 5 eyes (12.5%) in the superonasal quadrant, and 4 eyes (10.0%) in the inferonasal quadrant. Regression analysis demonstrated a clinically relevant correlation between preoperative angle α and total decentration magnitude in both groups (R2 = 0.1404, p = 0.017 for horizontal; R2 = 0.1424, p = 0.016 for vertical), whereas no significant correlation was observed between angle κ and total decentration (R2 = 0.0507, p = 0.162 for horizontal; R2 = 0.0037, p = 0.711 for vertical). Furthermore, we decomposed angle α, angle κ, and total decentration into horizontal and vertical components to investigate their directional correlations. The analysis revealed that angles α and κ exhibited directionally consistent correlations with decentration: in the horizontal direction, both horizontal components of angle α and angle κ showed positive correlations with horizontal decentration; in the vertical direction, neither the vertical components of angle α nor angle κ demonstrated a significant linear correlation with vertical decentration. Figure 3 illustrates the coefficient of determination (R2), P-values, and linear regression equations (where correlations were significant) for the overall, horizontal, and vertical decomposition analyses.
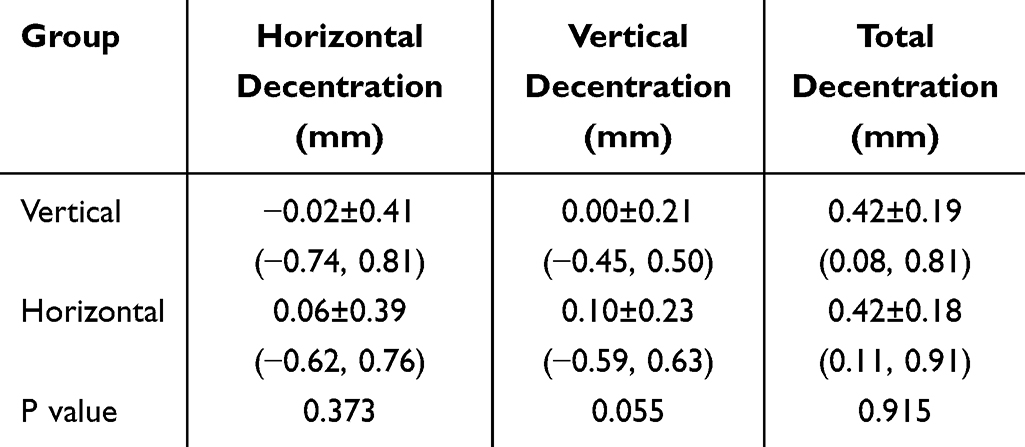 |
Table 2 Comparison of Optical Zone Decentration Between Two Positioning Methods |
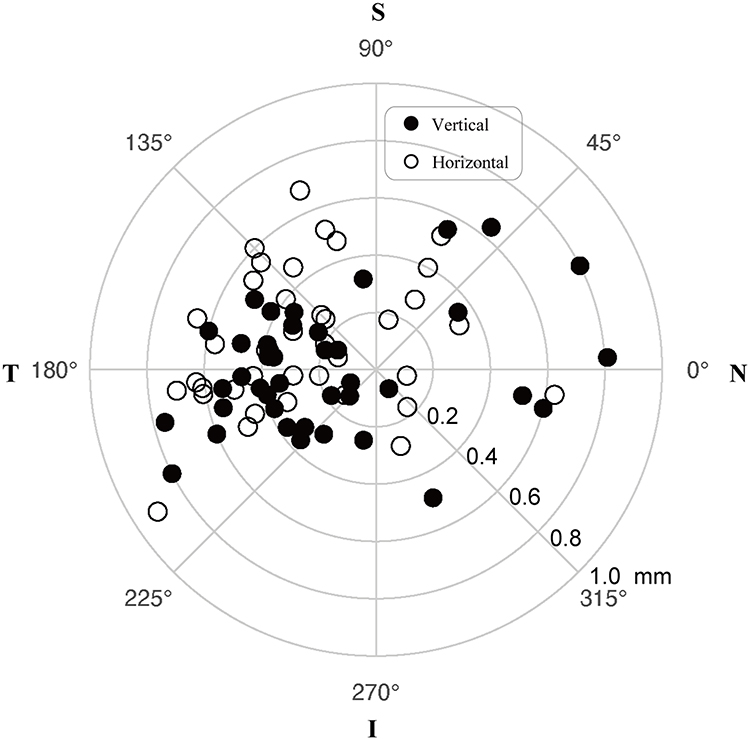 |
Figure 2 Distribution of Optical Zone Decentration. The polar plot illustrates the spatial distribution of the central hole position. Abbreviations: I, inferior; N, nasal; S, superior; T, temporal. Note: Decentration data from left eyes were mirrored to the corresponding positions in the right eye orientation. |
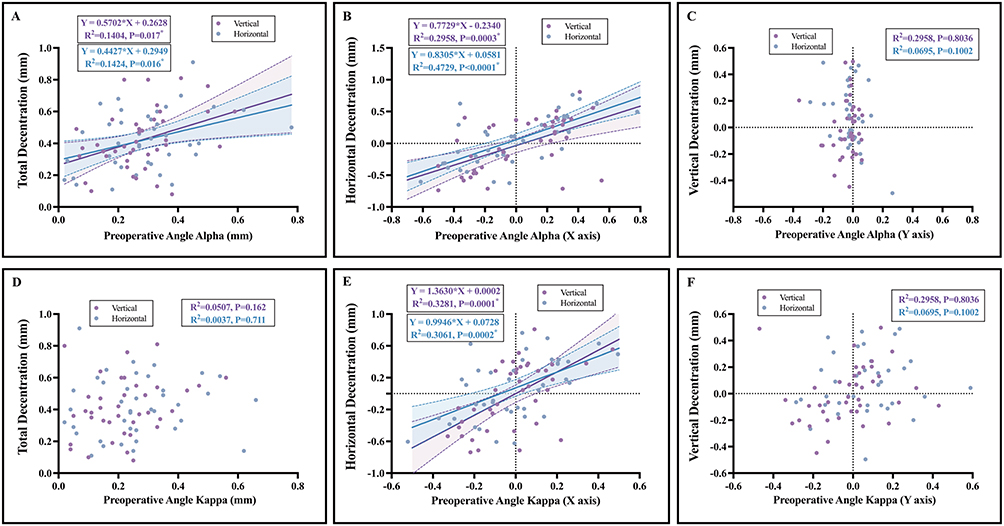 |
Figure 3 Correlation analysis between optical zone decentration and preoperative angles. (A) Angle α vs Total Decentration; (B) Angle α (X-axis component) vs Horizontal Decentration; (C) Angle α (Y-axis component) vs Vertical Decentration; (D) Angle κ vs Total Decentration; (E) Angle κ (X-axis component) vs Horizontal Decentration; (F) Angle κ (Y-axis component) vs Vertical Decentration. Blue lines represent the Horizontal Group; Purple lines represent the Vertical Group. Shaded areas indicate 95% confidence intervals. |
Changes in Postoperative Wavefront Aberrations
Wavefront analysis at 6 months postoperatively demonstrated comparable optical quality between the two implantation techniques across all evaluated parameters (Table 3). No statistically significant differences were observed in the following parameters: total higher-order aberrations (p=0.186), spherical aberration (p=0.200), vertical coma (p=0.707), horizontal coma (p=0.810), vertical trefoil (p=0.470), and oblique trefoil (p=0.884). Changes in coma and trefoil from preoperative to postoperative states were calculated through vector decomposition analysis, which similarly revealed no significant differences in coma (p=0.494) or trefoil (p=0.992).
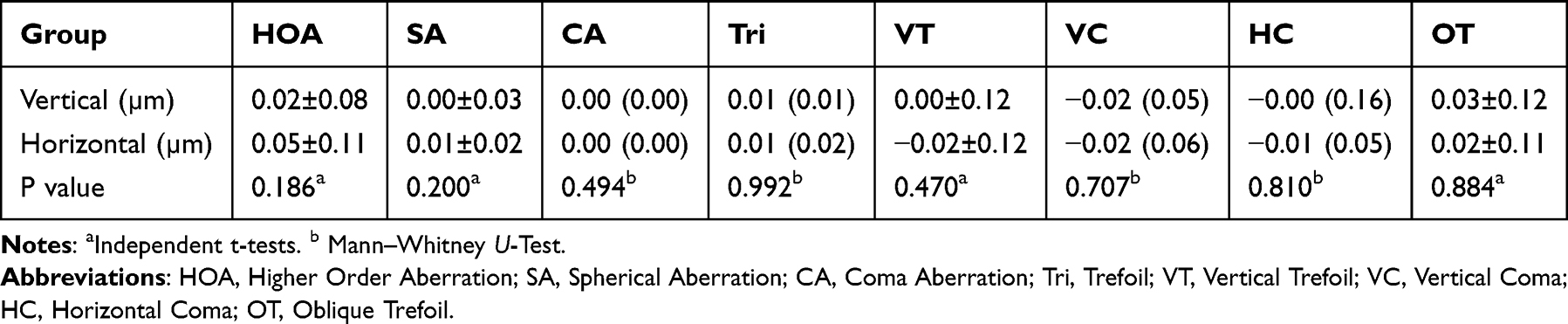 |
Table 3 Comparison of Corneal Higher-Order Aberrations Changes Between Two Positioning Methods |
Correlation analysis demonstrated no significant association between total decentration magnitude and induced corneal aberrations in either group. The coefficient of determination (R2) for all aberration-decentration relationships was < 0.31 (range: 0.009 to 0.308), with p-values consistently > 0.05 (range: 0.054 to 0.954) (Table 4), confirming that optical performance remained unaffected by observed decentration magnitudes within both implantation approaches.
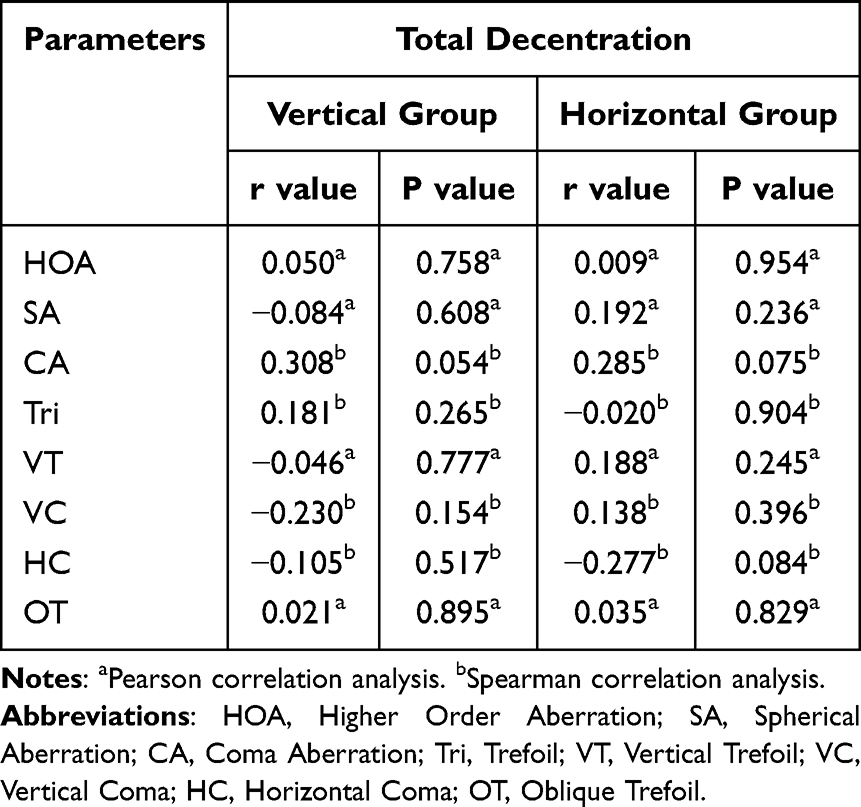 |
Table 4 Correlations Between Total Decentration and Corneal Aberration Changes in the Two Surgical Techniques |
Discussion
Vertical ICL implantation has gained increasing acceptance as an advantageous technique for optimizing the vault height and rotational stability. Studies comparing horizontal versus vertical implantation have documented superior rotational stability with the vertical approach, reporting a mean rotation of 3.27° versus 1.74° in one series15 and 3.02° versus 1.11° in another investigation of toric ICLs.16 The potential for maintaining lower vault heights represents another benefit of vertical implantation,22–25 particularly given that the complications of excessive vault (endothelial cell loss and angle closure) tend to be irreversible, whereas those associated with low vault (particularly cataract formation) may be more manageable. Furthermore, the central hole design facilitates aqueous circulation and reduces the cataractogenic risk and angle closure. Our demonstration of equivalent decentration and optical performance of vertical versus horizontal implantation provides additional support for this emerging surgical approach.
In our study, analysis of the ICL V4c decentration based on the central hole position (KS-AquaPORT) revealed a predominantly temporal distribution of KS-AquaPORT in both the horizontal and vertical implantation groups. Previous studies evaluating ICL V4c decentration demonstrated similar temporal displacement of the KS-AquaPORT, particularly in the superotemporal quadrant, with mean decentration values of 0.34 mm relative to the pupillary axis and 0.47 mm relative to the visual axis.26,27 However, these earlier studies relied on slit-lamp photography combined with topographic coordinate conversion, which entails operator-dependent variability.
Our research team utilized the OPD-Scan III system for quantitative evaluation of KS-AquaPORT centration. Building on our previous findings documenting a mean decentration of 0.38 mm with temporal predominance relative to the visual axis,13 the current study systematically compares decentration characteristics between horizontal and vertical implantation approaches. The results demonstrate nearly identical mean decentration values (horizontal: 0.42 ± 0.18 mm; vertical: 0.42 ± 0.19 mm; p = 0.915), with no statistically significant intergroup differences. Regarding spatial distribution, the decentration was predominantly located temporally. In the vertical implantation group, 18 eyes (45.0%) were located in the inferotemporal quadrant and 13 eyes (32.5%) in the superotemporal quadrant. Correspondingly, in the horizontal implantation group, 18 eyes (45.0%) were located in the superotemporal quadrant and 13 eyes (32.5%) in the inferotemporal quadrant. This pattern occurs because vertical implantation rotates the central hole by 90 degrees around the visual axis compared to horizontal implantation, resulting in distinct spatial distribution patterns while maintaining identical radial distances. In other words, although rotation affects the positional distribution of the central port, it does not alter the magnitude of decentration. Consequently, there was no statistically significant difference in decentration magnitude between vertical and horizontal implantation.
Notably, our analysis revealed significant correlations between the preoperative angle α and total decentration magnitude in both the horizontal and vertical implantation groups, whereas no such relationship was observed for angle κ. We postulate that this association stems from ICL fixation within the ciliary sulcus, with the KS-AquaPORT approximating the sulcus midpoint near the center of the crystalline lens. Because angle α represents the lens center displacement relative to the visual axis, its correlation with ICL decentration is mechanistically plausible.28 To elaborate on this finding, it is crucial to distinguish between anatomical and functional centration. While the ICL V4c is designed to center anatomically within the ciliary sulcus, the visual axis does not always align with this anatomical center. Angle alpha represents the distance between the visual axis and the center of the crystalline lens, which the ICL approximates. Consequently, a large preoperative angle alpha inherently means that the visual axis is significantly offset from the ICL’s anatomical center, even when the lens is perfectly positioned in the sulcus. Our OPD-Scan III measurements, which define decentration relative to the visual axis, therefore capture this “functional decentration”. Our findings underscore the clinical importance of considering angle alpha as a predictor of postoperative functional centration. Conversely, angle κ, which describes the pupillary center offset from the visual axis, demonstrated no significant relationship with ICL decentration.28 This study also found that the horizontal components of both angle α and angle κ showed positive correlations with ICL horizontal decentration, while no significant association was observed for vertical components (Figure 3). This phenomenon can be explained by the anatomical characteristics of the ciliary sulcus: The vertically oval-shaped sulcus, with its shorter horizontal diameter,22 limits the fixation of haptic, enabling the horizontal displacement of the lens center (angle α) and pupil center (angle κ) to synergistically influence ICL positioning through iris-ciliary body tension. In the vertical direction, the deeper sulcus with greater contact area, combined with gravity-assisted stabilization, creates a dual stabilization mechanism that significantly diminishes the regulatory effect of angular parameters. This finding aligns with clinically observed superior rotational stability in vertical implantation,14–16 suggesting that preoperative planning should specifically evaluate the synergistic effects of both angles in patients at high risk of horizontal decentration.
At six months post-surgery, all eyes in the horizontal group (40/40, 100%) achieved uncorrected distance visual acuity (UDVA) of 20/20 or better, while the vertical group demonstrated a nearly equivalent success rate (39/40 eyes, 97.5%). These findings are largely consistent with previous studies.14,16 Regarding aberrations, previous studies have documented increased coma aberrations with greater ICL V4c decentrations and significantly higher HOAs29 and trefoils in cases of large versus small decentrations.30 However, its clinical impact on visual performance appears to be minimal. Multiple studies have shown that KS-AquaPORT positioning does not significantly affect uncorrected distance visual acuity (UDVA), contrast sensitivity under mesopic and glare conditions, total corneal HOAs, or quality-of-life indices.26,27,30 Our findings are consistent with those of a recent study by Niu et al,31 which demonstrated no significant correlations between decentration parameters and postoperative HOAs. This may be attributed to two main factors: first, the spherical optical design of the ICL reduces sensitivity to decentration; second, in our cohort, the average decentration in both groups (0.42 ± 0.18 mm and 0.42 ± 0.19 mm, respectively) remained below 0.5 mm, which may not have reached the threshold to significantly influence higher-order aberrations (HOAs). This may explain the absence of notable aberrative consequences. The absence of intergroup differences in HOAs changes further supports the comparable optical performance of both horizontal and vertical implantation approaches.
Our study has several limitations. First, as a retrospective study, it may be subject to selection bias, this was mitigated by strictly adhering to a standardized preoperative anatomical protocol for grouping assignment, rather than subjective surgeon preference. Additionally, our relatively small sample size and the specific patient population included may limit the generalizability of our findings. Furthermore, lack of decentration data at the early postoperative stage (eg, 1 week) prevented longitudinal analysis of positional stability from the immediate postoperative period. Finally, although we analyzed follow-up data at 6 months postoperatively, further research is needed to determine the long-term visual outcomes and complication rates.
The study demonstrated comparable visual quality and similar decentration outcomes between vertical and horizontal ICL implantation techniques, providing theoretical support for the emerging vertical implantation approach. Furthermore, a significant correlation was observed between preoperative angle alpha and decentration in both groups, highlighting the importance of angle alpha measurement during preoperative evaluations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Zhou X) upon reasonable request.
Ethics Approval and Consent to Participate
Approval for this clinical study was granted by the Ethics Committee of Fudan University’s Eye and ENT Hospital (No. 2021018), with strict adherence to Declaration of Helsinki guidelines. Written informed consent was acquired from all participants after thorough explanation of the study’s procedures and possible effects.
Acknowledgments
Zhongjun Tang and Zhuotong Wu contributed equally as co-first authors. We would like to thank Editage (https://www.editage.cn) for English language editing.
Funding
This work was supported by the National Key Research and Development Program of China (2024YFC2510805), Key Project of the Regional Innovation and Development Joint Fund of the National Natural Science Foundation of China (U24A20708), Shanghai Municipal Health Commission (2023ZZ02019).
Disclosure
The authors declare that they have no competing interests.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–11. doi:10.1016/j.ophtha.2016.01.006
2. Wan Q, Chen L, He P, et al. Five years comparation of efficacy and safety after ICL-V4c implantation for high and super high myopia correction. Ann Med. 2025;57(1):2448282. doi:10.1080/07853890.2024.2448282
3. Du J, Zhou W, Zhao T, et al. Efficacy and safety of implantable collamer lens V4c implantation in 1834 myopic eyes for 1 year of follow-up. J Refract Surg. 2023;39(10):694–704. doi:10.3928/1081597X-20230908-02
4. Zhang Z, Niu L, Liu T, et al. Primary observations of EVO ICL implantation for high myopia with concave iris. Eye Vis. 2023;10(1):18. doi:10.1186/s40662-023-00335-4
5. Chen D, Zhao X, Chou Y, Luo Y. Comparison of visual outcomes and optical quality of femtosecond laser-assisted SMILE and visian implantable collamer lens (ICL V4c) implantation for moderate to high myopia: a meta-analysis. J Refract Surg. 2022;38(6):332–338. doi:10.3928/1081597X-20220411-01
6. Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–1077. doi:10.2147/OPTH.S111620
7. Zhan B, Huang Y, Chen X, et al. Comparison of long-term visual quality after keratorefractive lenticule extraction and implantable collamer lens V4c for high myopia. J Cataract Refract Surg. 2024;50(11):1157–1164. doi:10.1097/j.jcrs.0000000000001523
8. Zhao W, Zhao J, Han T, Wang J, Zhang Z, Zhou X. A comprehensive investigation of contrast sensitivity and disk halo in high myopia treated with SMILE and EVO implantable collamer lens implantation. Transl Vis Sci Technol. 2022;11(4):23. doi:10.1167/tvst.11.4.23
9. Kayhan B, Coskunseven E, Sahin O, Pallikaris I. The effects of implantable collamer lens implantation on higher order aberrations. Int J Ophthalmol. 2019;12(12):1848–1852. doi:10.18240/ijo.2019.12.05
10. Hashemian SJ, Farrokhi H, Foroutan A, et al. Ocular higher-order aberrations changes after implantable collamer lens implantation for high myopic astigmatism. J Curr Ophthalmol. 2018;30(2):136–141. doi:10.1016/j.joco.2017.10.002
11. Shi M, Wei R, Zhou X, Liu S. Pharmacological accommodative changes of haptic position and its impact on vault after ICL implantation. J Refract Surg. 2025;41(1):e22–e28. doi:10.3928/1081597X-20241126-02
12. Wei R, Tang Z, Shi M, et al. Spatial variation in ciliary body morphology and the effect on haptic position and peripheral vault after ICL implantation. J Refract Surg. 2025;41(3):e199–e206. doi:10.3928/1081597X-20250123-01
13. Chen X, Lin IC, Miao H, et al. Effects of decentration of implantable collamer lens V4c on visual quality with the OPD-scan III aberrometer. Am J Ophthalmol. 2024;259:88–95. doi:10.1016/j.ajo.2023.11.008
14. Zhao K, Wan L, Chen X, et al. Comparison of rotational stability of the implantable collamer lens after using a vertical or horizontal implanting orientation. J Cataract Refract Surg. 2025;51(1):9–15. doi:10.1097/j.jcrs.0000000000001545
15. Lee Y, Han SB, Auffarth GU, et al. Vertical implantable collamer lens as a novel method to increase rotational stability. PLoS One. 2024;19(8):e0308830. doi:10.1371/journal.pone.0308830
16. Huang W, Ji Y, Zheng S, et al. The effectiveness and rotational stability of vertical implantation of the implantable collamer lens for the treatment of myopia. J Refract Surg. 2022;38(10):641–647. doi:10.3928/1081597X-20220831-01
17. Jiang Y, Luo Y, Li Y, Lu T. The long-term observation of the rotation of implantable collamer lens as the management of high postoperative vault. Front Med. 2023;10:1104047. doi:10.3389/fmed.2023.1104047
18. Wei R, Cheng M, Niu L, et al. Outcomes of the EVO ICL using a customized non-horizontal or horizontal implanting orientation based on UBM measurement: a pilot study. Ophthalmol Ther. 2022;11(3):1187–1198. doi:10.1007/s40123-022-00498-8
19. Martínez-Plaza E, López-Miguel A, López-de la Rosa A, McAlinden C, Fernández I, Maldonado MJ. Effect of the EVO+ visian phakic implantable collamer lens on visual performance and quality of vision and life. Am J Ophthalmol. 2021;226:117–125. doi:10.1016/j.ajo.2021.02.005
20. He W, Qiu X, Zhang S, et al. Comparison of long-term decentration and tilt in two types of multifocal intraocular lenses with OPD-scan III aberrometer. Eye. 2018;32(7):1237–1243. doi:10.1038/s41433-018-0068-5
21. Zhu X, He W, Zhang Y, Chen M, Du Y, Lu Y. Inferior decentration of multifocal intraocular lenses in myopic eyes. Am J Ophthalmol. 2018;188:1–8. doi:10.1016/j.ajo.2018.01.007
22. Ouchi M. Vault of the phakic intraocular lens during vertical and horizontal fixation within patient comparison. Sci Rep. 2025;15(1):10002. doi:10.1038/s41598-025-95077-9
23. Shimada R, Katagiri S, Horiguchi H, Nakano T, Kitazawa Y. Prediction of vaults in eyes with vertical implantable collamer lens implantation. J Cataract Refract Surg. 2025;51(1):45–52. doi:10.1097/j.jcrs.0000000000001556
24. Ouchi M. Vault changes in eyes with a vertically implanted implantable collamer lens. Sci Rep. 2024;14(1):3484. doi:10.1038/s41598-024-52913-8
25. Matarazzo F, Day AC, Fernandez-Vega Cueto L, Maurino V. Vertical implantable collamer lens (ICL) rotation for the management of high vault due to lens oversizing. Int Ophthalmol. 2018;38(6):2689–2692. doi:10.1007/s10792-017-0757-2
26. Martínez-Plaza E, López-Miguel A, de La Rosa AL, McAlinden C, Fernández I, Maldonado MJ. EVO+ implantable collamer lens KS-aquaPORT location, stability, and impact on quality of vision and life. J Refract Surg. 2022;38(3):177–183. doi:10.3928/1081597X-20220106-01
27. Martínez-Plaza E, López-Miguel A, Fernández I, Blázquez-Arauzo F, Maldonado MJ. Effect of central hole location in phakic intraocular lenses on visual function under progressive headlight glare sources. J Cataract Refract Surg. 2019;45(11):1591–1596. doi:10.1016/j.jcrs.2019.06.022
28. Meng J, Du Y, Wei L, et al. Distribution of angle α and angle κ in a population with cataract in shanghai. J Cataract Refract Surg. 2021;47(5):579–584. doi:10.1097/j.jcrs.0000000000000490
29. Pérez-Vives C, Ferrer-Blasco T, Madrid-Costa D, García-Lázaro S, Montés-Micó R. Visual quality comparison of conventional and hole-visian implantable collamer lens at different degrees of decentering. Br J Ophthalmol. 2014;98(1):59–64. doi:10.1136/bjophthalmol-2013-303787
30. Park MJ, Jeon HM, Lee KH, Han SY. Comparison of postoperative optical quality according to the degree of decentering of V4c implantable collamer lens. Int J Ophthalmol. 2017;10(4):619–623. doi:10.18240/ijo.2017.04.19
31. Niu L, Zhang Z, Miao H, et al. Effects of tilt and decentration of visian implantable collamer lens (ICL V4c) on visual quality: an observational study. BMC Ophthalmol. 2022;22(1):294. doi:10.1186/s12886-022-02499-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.