Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Comparative Study Between the Efficacy of Fractional CO2 Laser/Radiofrequency, PRP and a Combination of Both in the Treatment of Striae Distensae: A Pilot Study
Authors Sany I, Mohamed Sobhi R, Badawi A ![]() , Mohamed Elmaadawi Z, Mostafa PIN
, Mohamed Elmaadawi Z, Mostafa PIN
Received 28 March 2022
Accepted for publication 4 August 2022
Published 19 August 2022 Volume 2022:15 Pages 1687—1694
DOI https://doi.org/10.2147/CCID.S365952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Iman Sany,1 Rehab Mohamed Sobhi,1 Ashraf Badawi,2,3 Zeinab Mohamed Elmaadawi,4 Pakinam Ibrahim Nabil Mostafa1
1Department of Dermatology, Kasr Alainy Medical School, Cairo University, Cairo, Egypt; 2Department of Medical Laser Applications, National Institute of Laser Enhanced Sciences, Cairo University, Cairo, Egypt; 3Department of Dermatology, Faculty of Medicine, University of Szeged, Szeged, Hungary; 4Department of Histology & Cell Biology, Kasr Alainy Medical School, Cairo University, Cairo, Egypt
Correspondence: Pakinam Ibrahim Nabil Mostafa, Lecturer of Dermatology, Kasr Alainy Medical School, Cairo University, PO Box 11519, 4 Gemey St, Garden City, Cairo, Egypt, Tel +201002576451, Email [email protected]
Purpose: The work aims to compare the effect of platelet-rich plasma versus fractional CO22 laser/radiofrequency versus both methods combined in treating striae distensae.
Patients & Methods: The study included ten female patients with striae alba with Fitzpatrick IV skin. Three sites of striae were chosen; one was treated with platelet-rich plasma, another with fractional CO2 /radiofrequency (CO2/RF), and the third received both treatments. Every patient received three treatment sessions one month apart. Patients were photographed, and a skin biopsy was taken from each area before and one month after treatment.
Results: Assessment of the clinical photos showed that fractional CO2/radiofrequency gave a mild improvement in 22%, moderate improvement in 55.5% and marked improvement in 22.5%. Clinically, the combined treatment showed mild improvement in 44% of patients, moderate results in 33% and marked improvement in 23% of patients. The PRP as an only mode of treatment showed poor improvement in 22%, mild improvement in 23% and moderate improvement in 55% of patients. Biopsy results showed a decrease in collagen and elastin after treatment with the solitary methods, while the combined approach resulted in an increase in collagen and a reduction in elastin.
Conclusion: Fractional CO2 laser/radiofrequency combined with PRP or either of them showed clinical improvement to variable degrees with superior results clinically and histologically with the combined method.
Keywords: fractional CO2 laser radiofrequency, platelet rich plasma, PRP, striae distensae
Introduction
Striae Distensae is a common cosmetic concern among the youth around puberty and females in the childbearing period due to pregnancy.1 However, they can occur with obesity and corticosteroid excess as well. The basic idea is dermal stretching. Initially, they are erythematous elevated lines (Striae Rubra). Over time, they become atrophic and white (striae alba) due to local breakdown of elastin and collagen with mast cell enzyme release in mid dermis.2 Genetic predisposition has a role in the development of striae.3 They can occur on the abdomen, breasts, thighs, buttocks and calves.4
Several studies discussed different modes of treatment with variable results. Lasers included pulsed dye laser, Fractional CO2 laser, Nd YAG, Er Glass, Er YAG, and Diode.2 Also, IPL showed thickening of the dermis in some studies.5 Topical tretinoin and topical chemical peels showed some success.6,7 Radiofrequency (RF) has been successful in skin tightening through denaturation of elastic and collagen fibres followed by neocollagenesis.8 Platelet-rich plasma (PRP) delivers autologous growth factors to the tissues enhancing wound healing.1
The work aims to compare the effect of platelet-rich plasma versus fractional CO2 laser/radiofrequency versus both methods combined in treating striae distensae.
Patients and Methods
The study included ten nonsmoker female patients (Fitzpatrick IV skin phototype) with striae alba. Their ages ranged between 18 and 30 years. Seven patients had developed the striae after weight gain, two during earlier pregnancy and one after oral steroid use. We excluded patients with autoimmune diseases, diabetes, pregnancy and keloidal tendency by history. All patients signed informed Consent. Dermatology Research Ethical Committee (REC) of Kasr Alainy Medical School (Cairo University) has approved the study. The study complies with the declaration of Helsinki. Three sites of striae were chosen randomly (by the closed envelope method) in non-sun exposed areas in each patient distant from each other (abdomen, thighs and shoulders). One was treated with fractional CO2/RF, another with PRP injection and the third was treated by both combined fractional CO2/RF followed by PRP. Each patient received three treatment sessions, one month apart.
The assessment was done by photography via a blinded physician committee (3 physicians), where 0–25% improvement was classified as poor, 25–50% mild, 50–75% moderate, and 75–100% marked improvement regarding the thickness of the striae and skin quality. Objective assessment was done by a 2mm skin biopsy from each of the three sites treated in all patients before and one month after the last treatment. The biopsies were stained with Haematoxylin & Eosin (scale 50 μm) (Figure 1), Mallory trichrome for collagen (scale 50 μm) (Figure 2) and Orcein for elastic fibres (scale 50 μm) (Figure 3). We applied a patient satisfaction score from 0 to 5, where 0 is unsatisfied, and five is highly satisfied.
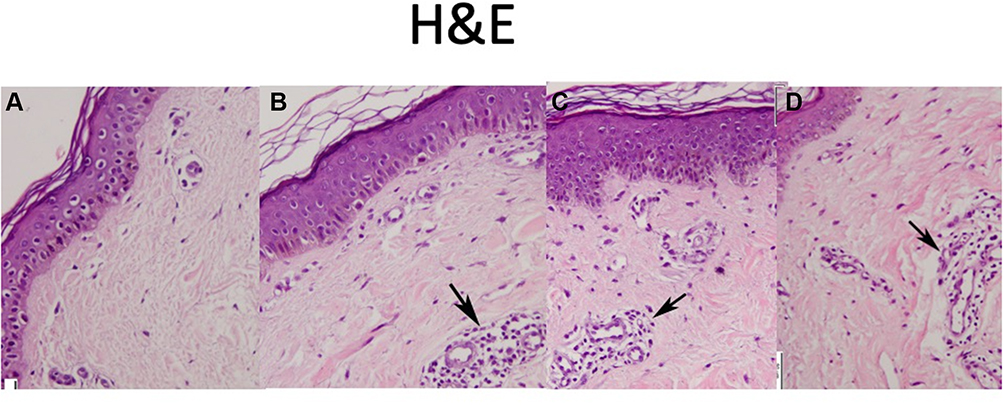 |
Figure 1 Skin biopsy from striae stained with Haematoxylin and Eosin (scale 50 μm). (A) Before treatment, (B) after 3 sessions of combined treatment, (C) after 3 sessions of fractional laser/RF, (D) after 3 sessions of PRP. Note the increase in number of fibroblasts and vascularity in all biopsies after treatment to variable degrees. Black arrows refer to fibroblasts and vascularity increasing after treatment. |
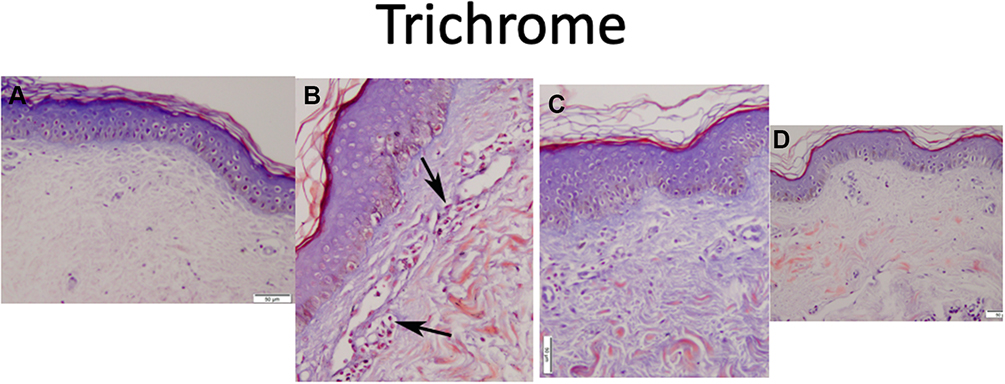 |
Figure 2 Skin biopsy from striae stained with Trichrome stain (scale 50 μm). (A) Before treatment, (B) after 3 sessions of combined treatment, (C) after 3 sessions of fractional laser/RF, (D) after 3 sessions of PRP. Note the increase in collagen fibres. Black arrows show increase in fibroblasts with treatment. |
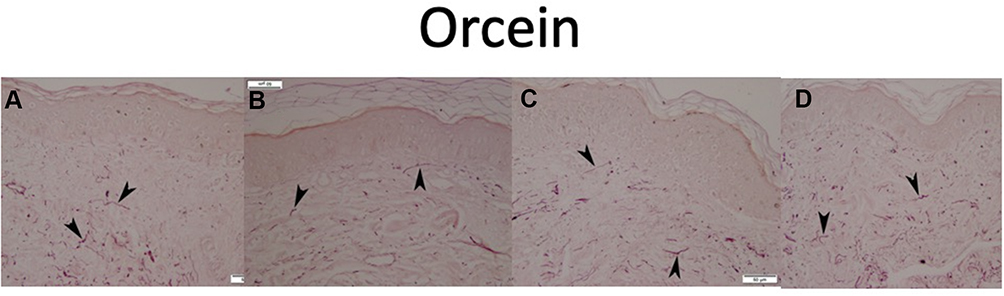 |
Figure 3 Skin biopsy from striae stained with Orcein (scale 50 μm). (A) Before treatment, (B) after 3 sessions of combined treatment, (C) after 3 sessions of fractional laser/RF, (D) after 3 sessions of PRP. Note the lack of increase in elastin. Black arrows point to elastic fibers. |
Platelet-rich plasma (PRP) was prepared using the single spin method where 4cc blood was withdrawn and spun at 3000 rpm for 7 minutes, then activated with calcium (0.1 mL). The upper part separated was injected in the striae as a sole treatment at one site or immediately after the fractional CO2/RF at the combined method site.
Fractional CO2/RF device (DEKA SmartXide C60, Calenzo, Italy) parameters were 20 W, 600 microsecond (Dwell) and 600 micrometer (spacing) for laser and 15 W power and 2.5 sec for radiofrequency with an average radiofrequency dose is 25 J/cm.2 This treatment was done solely or in combination with PRP.
All patients signed written informed consent for procedure, photography and biopsy.
Photomicrographs were captured at x200 magnification using an Olympus microscope (BX51; Olympus, Tokyo, Japan) connected to an Olympus camera (U-CMAD3).
Quantitative Morphometric Study
Quantitative morphometric studies of collagen fibres in Mallory’s Trichrome stained sections and elastic fibres in Orcein stained sections of skin biopsies were performed in the dermis using the binary mode of Leica Qwin 500 LTD image analysis computer system (Cambridge, UK).9 The quantitative morphometric measurements were done in 5 randomly selected non-overlapping high power fields (HPF) using an x40 objective lens. Results were expressed as mean ±SD, and significant differences were evaluated using one-way analysis of variance (ANOVA) test. P value <0.05 was considered to be statistically significant.
Statistical Methods
Data were coded and entered using the statistical package SPSS (Statistical Package for the Social Sciences) version 25. Data were summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were made using the non-parametric Kruskal–Wallis and Mann–Whitney tests. For comparison of serial measurements within each patient (before and after treatment), the non-parametric Wilcoxon signed-rank test was used.10 For comparing categorical data, a Chi-square (Χ2) test was performed. An exact test was used instead when the expected frequency was less than 5.11 Correlations between quantitative variables were done using the Spearman correlation coefficient.12 P-values less than 0.05 were considered statistically significant. Results were expressed as mean± SD and significant differences were evaluated using one-way analysis of variance (ANOVA) test. P value 0.05 was statistically significant.
Results
The study included ten nonsmoker female patients (Fitzpatrick IV skin phototype) with striae alba. Their ages ranged between 18 and 30 years. Seven patients had developed the striae after weight gain, two during earlier pregnancy and one after oral steroid use.
A blinded physician committee’s assessment of the clinical photos of the skin quality and thickness of the striae showed that the combination of PRP with fractional radiofrequency/CO2 showed mild improvement in 44% of patients, moderate results in 33% and marked improvement in 23% of patients (Figure 4). The PRP as an only mode of treatment showed poor improvement in 22%, mild improvement in 23% and moderate improvement in 55% of patients (Figure 5). The fractional radiofrequency/CO2 gave a mild improvement in 22%, moderate improvement in 55.5%, and marked improvement in 22.5% (Figure 6).
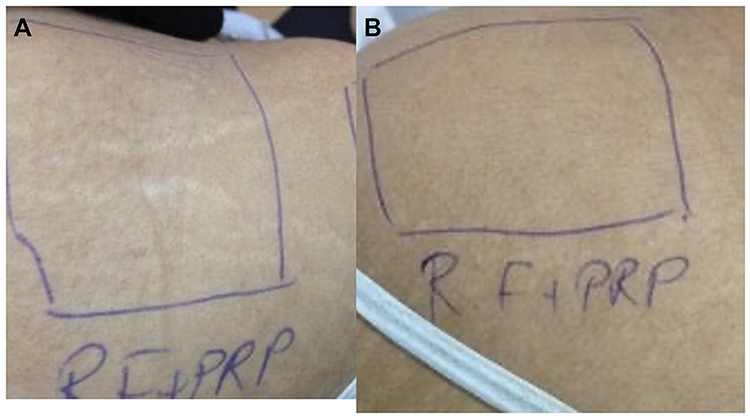 |
Figure 4 (A) Striae on the back before treatment, (B) improvement of striae after 3 sessions of combined treatment. |
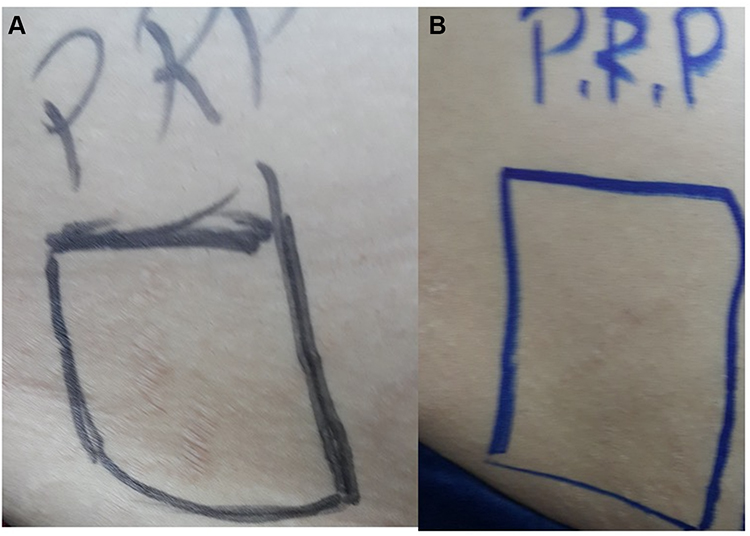 |
Figure 5 (A) Striae on the back before treatment, (B) improvement of striae after 3 sessions of PRP. |
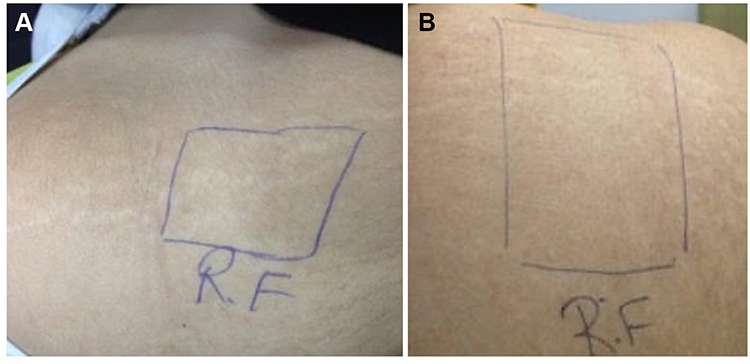 |
Figure 6 (A) Striae on the back before treatment, (B) improvement of striae after 3 sessions of fractional laser/RF. |
An image analyzer assessed the skin biopsies for the trichrome and Orcein stains for collagen and elastic fibres, respectively. Since the sample size was small, non-parametric tests were done for statistical analysis, and thus the median was used for comparison.
Skin biopsies treated by PRP alone showed no increase in the median of collagen and elastic fibres, as shown in Table 1.
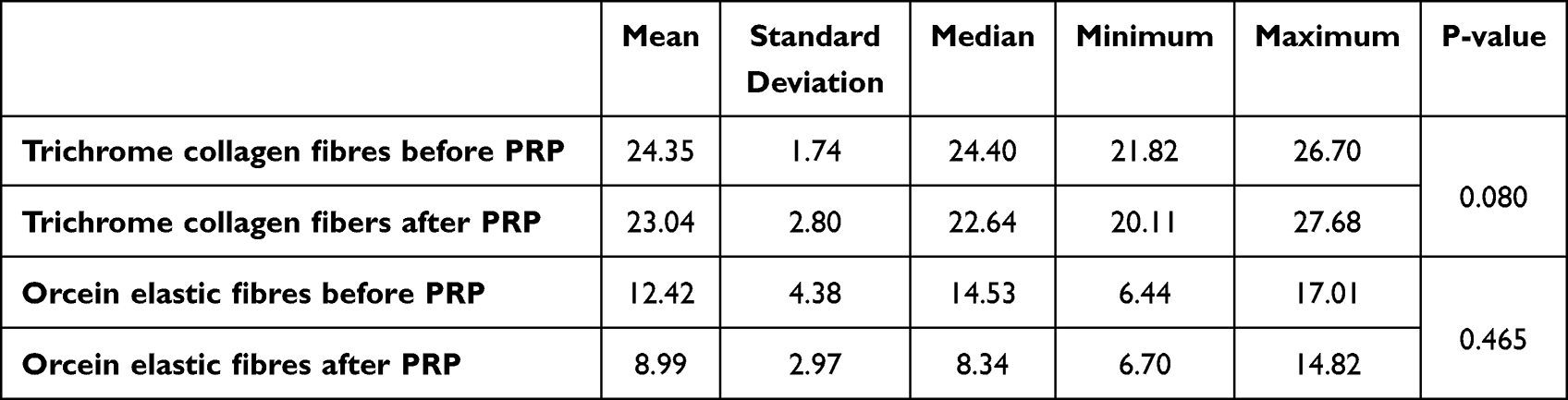 |
Table 1 Comparison Between Before and After in PRP |
There was also no increase in collagen, and elastic fibres were in the lesions treated by fractional RF/CO2 only (Table 2).
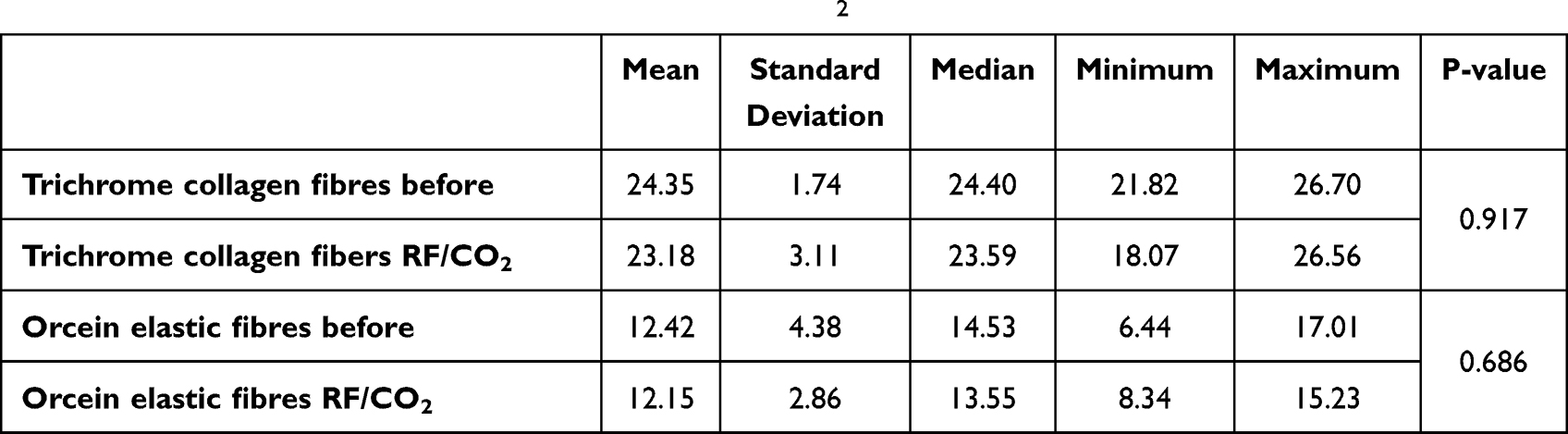 |
Table 2 Comparison Between Before and After in RF/CO2 |
However, there was a statistically significant increase in the median of collagen fibres in the lesions treated by the combined method (p 0.046). However, still, there was no increase in elastic fibres median in the same lesions (Table 3).
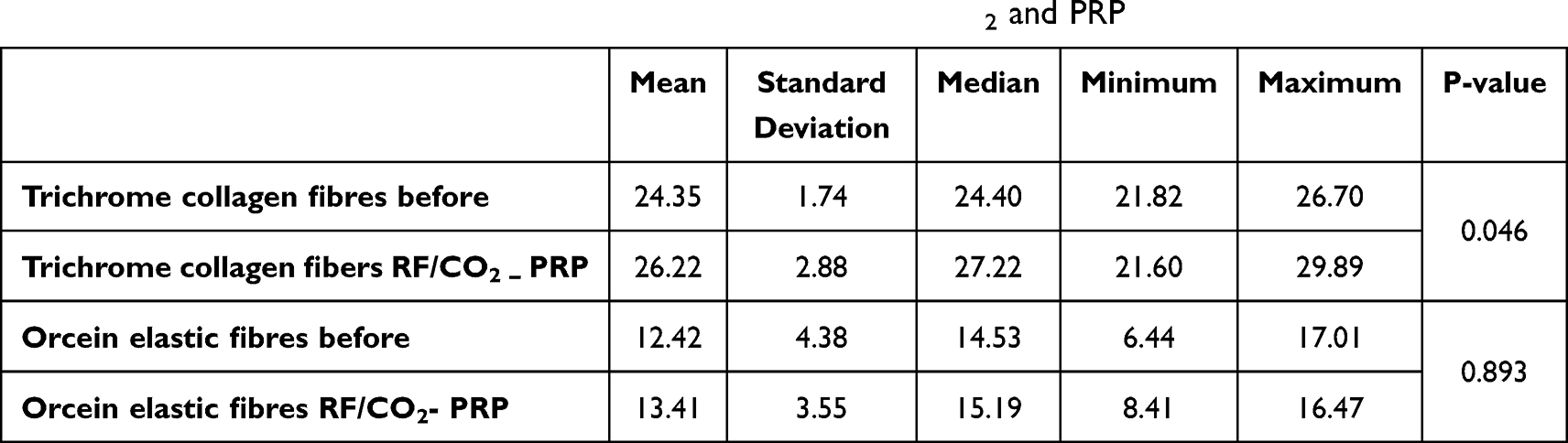 |
Table 3 Comparison Between Before and After in Combined RF/CO2 and PRP |
Regarding the patient satisfaction score, on a scale from 0 to 5, 0 is unsatisfied, and five is highly satisfied, eight patients scored 4, and 2 patients scored 3.
We had 3 cases of post-inflammatory hyperpigmentation (33%) after fractional CO2/RF and combined treatment which resolved one month after the session.
Discussion
Striae distensae (SD) are common, especially in obese, pregnant and with excess corticosteroid use.13 Pathogenesis of SD includes an essential role of mast cells with the release of elastases that degrade the collagen, elastin and fibrillin, resulting in mid dermis elastolysis.13 SD tissue analysis showed decreased procollagen and fibronectin mRNA.14
Unfortunately, treatments have so far been disappointing for patients and doctors. Topical agents such as chemical peeling and moisturizers like cocoa butter have been used. Lasers have been tried, where Pulsed dye laser and Nd Yag have been successful in SD Rubra. Fractional CO2 laser and radiofrequency have shown an increase in collagen production and coagulation of the dermis, helping improve SD.15
Our study has been conducted as a pilot study on 10 Egyptian females (Fitzpatrick IV) with striae distensae alba over the abdomen, thighs and shoulders. Three areas with striae in the same anatomical site in each patient were randomly treated by platelet-rich plasma alone or fractional CO2/radiofrequency alone or by both methods combined.
Clinically, photos assessed by a blinded physician showed all methods lead to variable grades of improvement. Collectively, according to patient satisfaction scores, patients were satisfied. Three patients (combined approach and fractional CO2 /RFlaser) had post-inflammatory hyperpigmentation that improved with treatment.
Surprising results have been shown histopathologically. The elastic fibres did not increase after the three treatments. A constitutional problem could explain the lack of increase in the elastic fibres in this population or race that initially led to the striae. A study has shown that some people have low relaxin levels in their blood. The low relaxin level makes the tissue less lax and thus are at a greater risk of structural disruption of elastic fibre network by stretching.16
Our treatment arm by fractional CO2/ RF alone showed no increase in collagen. However, its increase showed by Pongsrihadulchai et al, who used micro-needling radiofrequency for striae at similar intervals like the current study.17 This difference in outcome may be due to the mode of delivery of radiofrequency. However, Pdngsrihadulchai et al and our study showed clinical improvement despite such histological discrepancy. Also, Sobhi et al4 showed almost equal clinical efficacy when comparing Fractional CO2 to fractional micro-needling radiofrequency. These results are similar to what Al-Himadani et al13 mentioned in their review about the positive role of radiofrequency in striae distensae.
So, we attribute the improvement of patients in the fractional CO2/RF group to the coagulation of the dermis with collagen remodelling as well as epidermal changes.
The fractional CO2 part of the device that we used helps improve the epidermal component through the fractional photothermolysis technology with heat shock proteins and subsequent keratinocyte proliferation, improving epidermal appearance.18 Sobhi et al have shown clinical improvement with Fractional CO2 as a solo treatment for striae.
An increase in the extracellular matrix by fibroblast activation can explain the improvement of the patients treated with PRP as a solitary treatment with the lack of increase in collagen and elastin in the biopsy.1 However, the collagen amount increased when we combined the PRP with the fractional RF/CO2 in the present study. There was a change in cell signalling that we could not find proof of in other studies. So this was our assumption from the interpretation of our results.
A review article showed that histological analysis of punch biopsies before and after PRP (82 subjects) in skin ageing showed that combining PRP with fractional laser resurfacing resulted in increased fibroblasts, increased collagen volume and enhanced collagen organization and increased thickness of the dermal-epidermal junction (DEJ). PRP monotherapy increased the number of fibroblasts, dermal collagen density, elastic fibre deposition, DEJ thickness, epidermal thickness and dermal thickness.19 This finding explains the difference PRP does in tissues alone or the combination treatment protocol. Ibrahim et al have reported similar results where they recommended a combination of PRP with microdermabrasion in striae treatment.20 Also, other studies by Suh et al1 and Kim et al21 suggested using radiofrequency combined with PRP in treating striae.22
On comparing the results of the three groups of the current study, the clinical improvement highlights the possibility of induction of other matrix proteins in the dermis and epidermal improvement, bypassing the deficiency of collagen and elastin in striae distensae. The increase in collagen in the combined method reflects a change in cell signalling towards collagen production, giving the combined approach a more favourable outcome than each method alone. The positive result of this combination demonstrates the diversity of matrix proteins and their ability to mask each others’ deficiencies giving the patient the satisfaction of clinical improvement regarding the skin quality and SD thickness.
The post-inflammatory hyperpigmentation occurred in patients treated with Fractional CO2/RF and those treated with the combined treatment. This side effect is possibly due to the Fractional CO 2 portion of such treatment. Similarly, Sobhi et al had documented such side effects with Fractional CO2 but not with radiofrequency when the study compared their efficacy in striae distensae treatment.
In conclusion, fractional CO2/RF combined with PRP or either of them alone showed variable degrees of clinical improvement, superior clinical improvement and histologically with the combined method. Collagen and elastin quantity proved to be not the sole aim in SD treatment. Improving the epidermal component and improvement of the dermis with possible other extracellular matrix proteins.
We recommend performing further studies with a larger sample size to find superior options for Striae distensae. Also, we recommend testing for extracellular matrix proteins other than collagen and elastin in striae distensae.
Also, we recommend further studies among the Egyptian population to check for the constitutional deficiency of elastic fibres and relaxin. These studies will help improve techniques of treatments as well as find therapeutic alternatives for striae distensae. We recommend trying the three methods used for the SD patients in this study. We recommend thinking of strategies that improve the epidermal and dermal components to bypass the idea of increasing collagen and elastin quantity.
Ethical Approval
Approved by the ethical committee REC (Research Ethical committee Dermatology Department Cairo University) and complies with the Declaration of Helsinki.
Informed Consent
All patients signed written consent.
Acknowlegment
Native English speaker has revised the paper.([email protected]).
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest.
References
1. Suh DH, Lee SJ, Lee JH, Kim HJ, Shin MK, Song MK. Treatment of striae distensae: combined enhanced penetration platelet-rich plasma and ultrasound after plasma fractional radiofrequency. J Cosmet Laser Ther. 2012;14:272–276. doi:10.3109/14764172.2012.738916
2. Aldahan AS, Shah VV, Mlacker S, Samarkandy S, Alsaidan M, Nouri K. Laser and light treatments for striae distensae: a comprehensive review of the literature. Am J Clin Dermatol. 2016;17(3):239–256. doi:10.1007/s40257-016-0182-8
3. Cho S, Park ES, Lee DH, Li K, Chung JH. Clinical features and risk factors for striae distensae in Korean adolescents. J EurAcad Dermatol Venereol. 2006;20(9):1108–1113.
4. Sobhi RM, Mohamed IS, El Sharkawy DA, Abdelwahab MA. Comparative study between the efficacy of fractional micro-needle radiofrequency and fractional CO2 laser in the treatment of striae distensae. Lasers Med Sci. 2019;34(7):1295–1304. doi:10.1007/s10103-019-02792-7
5. Hernandez-perez E, Colombo-Charrier E, Valencia Ibiett E. Intense pulsed light in the treatment of striae densae. Dermatol Surg. 2002;28(12):1124–1130.
6. Ud-din S, McGeorge D, Bayat A. Topical Management of striae distensae (stretch marks) prevention and therapy of striae rubrae and albae. J Eur Acad Derm Venereol. 2016;30(2):211–222. doi:10.1111/jdv.13223
7. Karia UK, Padhiar BB, Shah BJ. Evaluation of various therapeutic measures in striae rubra. J Cutan Aesthet Surg. 2016;9(2):101–105. doi:10.4103/0974-2077.184056
8. Kravaas G, Veitch D, Al-Niaimi F. The use of energy devices in the treatment of striae: a systematic literature. J Dermatol Treat. 2019;30(3):294–302. doi:10.1080/09546634.2018.1506078
9. Kiernan JA. Histological and Histochemical Methods: Theory and Practice.
10. Chan YH. Biostatistics102: quantitative data – parametric & amp; non-parametric tests. Singapore Med J. 2003a;44(8):391–396.
11. Chan YH. Biostatistics 103: qualitative data –tests ofIndependence. Singapore Med J. 2003b;44(10):498–503.
12. Chan YH. Biostatistics 104: correlational analysis. Singapore Med J. 2003c;44(12):614–619.
13. Al-himdani S, Ud-din S, Gilmore S, Bayat A. Striae distensae: a comprehensive review and evidence-based evaluation of prophylaxis and treatment. Br J Dermatol. 2014;170(3):527–547. doi:10.1111/bjd.12681
14. Lee KS, Rho YJ, Jang SI, et al. Decreased expression of collagen and fibronectin genes in striae distensae. Clin Exp Dermatol. 1994;19:285–288. doi:10.1111/j.1365-2230.1994.tb01196.x
15. Lee SE, Kim JH, Lee SJ, et al. Treatment of striae distensae using an ablative 10600 nm carbon dioxide fractional laser: a retrospective review of 27 participants. Dermatol Surg. 2010;36(11):1683–1690. doi:10.1111/j.1524-4725.2010.01719.x
16. Lurie S, Matas Z, Fux A, et al. Association of serum relaxin with striae gravidarum in pregnant women. Arch Gynecol Obstet. 2011;283:219–222. doi:10.1007/s00404-009-1332-5
17. Pongsrihadulchai N, Chalermchai T, Ophaswongse S, Pongsawat S, Udompataikul M. An efficacy and safety of nanofractional radiofrequency for the treatment of striae alba. J Cosmet Dermatol. 2017;16(1):84–90.
18. Katz B. Efficacy of a new fractional CO2 laser in treatment of photodamage and acne scars. Dermatoltherapy. 2010;23:403–406.
19. Maisel-Campbell AL, Ismail A, Reynolds KA, et al. A systematic review of the safety and effectiveness of platelet‑rich plasma (PRP) for skin aging. Arch Dermatol Res. 2020;312(5):301–315. doi:10.1007/s00403-019-01999-6
20. Ibrahim ZAES, El-Tatawy RA, El-Samongy MA, Ali DAM. Comparison between the efficacy and safety of platelet-rich plasma vs microdermabrasion in the treatment of striae distensae: clinical and histopathological study. J Cosmet Dermatol. 2015;14(4):336–346. doi:10.1111/jocd.12160
21. Kim IS, Park KY, Kim BJ, Kim MN, Kim CW, Kim SE. Efficacy of intradermal radiofrequency combined with autologous platelet rich plasma in striae distensae: a pilot study. Int J Dermatol. 2010;51(10):1253–1258. doi:10.1111/j.1365-4632.2012.05530.x
22. Ryu H-W, Kim SA, Jung HR, Ryoo YW, Lee KS, Cho JW. Clinical improvement of striae distensae in Korean patients using a combination of fractionated microneedle radiofrequency and fractional carbon dioxide laser. Dermatol Surg. 2013;39(10):1452–1458. doi:10.1111/dsu.12268
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.