Back to Journals » Clinical Ophthalmology » Volume 19
Comparative Performance of Artificial Tear Drops Assessed with Objective Non-Invasive Imaging
Authors White ER ![]() , Khwaja IA, Fazio N
, Khwaja IA, Fazio N ![]() , Galenchik-Chan A, Langman L
, Galenchik-Chan A, Langman L ![]() , Li DM, Weissbart S, Chou T
, Li DM, Weissbart S, Chou T ![]() , Gorgani FM, Huang L, Tourmouzis K, Rigas B
, Gorgani FM, Huang L, Tourmouzis K, Rigas B ![]() , Honkanen R
, Honkanen R
Received 27 March 2025
Accepted for publication 30 July 2025
Published 27 October 2025 Volume 2025:19 Pages 3973—3989
DOI https://doi.org/10.2147/OPTH.S530087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Emily Rose White,1,* Ishan Amin Khwaja,2 Nicholas Fazio,1,* Andre Galenchik-Chan,3 Lauren Langman,3 Deborah M Li,3 Sarah Weissbart,1 Timothy Chou,1 Farzan M Gorgani,1 Liqun Huang,4 Konstantinos Tourmouzis,5 Basil Rigas,1,4,* Robert Honkanen1,*
1Department of Ophthalmology, Stony Brook University Renaissance School of Medicine, Stony Brook, NY, USA; 2Stony Brook University, Stony Brook, NY, USA; 3Stony Brook University Renaissance School of Medicine, Stony Brook, NY, USA; 4Department of Family, Population and Preventive Medicine, Stony Brook University, Renaissance School of Medicine, Stony Brook, NY, USA; 5Royal United Hospitals Bath NHS Foundation Trust, Bath and North East Somer, UK
*These authors contributed equally to this work
Correspondence: Robert Honkanen, Department of Ophthalmology, Stony Brook University Hospital, Health Science Center, Level 2 Room 152, Stony Brook, NY, 11794, USA, Tel +1-631-444-6476, Fax +1-631-444-1543, Email [email protected]
Purpose: To perform a comparative analysis of 13 over the counter artificial tear formulations and perflourohexyloctane assessing performance using objective, non-invasive imaging. The data provides a rationale to make better informed therapeutic decisions regarding their use.
Patients and Methods: Prospective, sequential study of 13 drop formulations in participants over 18 years of age. Tear meniscus height, non-invasive keratographic break up time, and central lipid layer thickness were measured before and 5 and 15 minutes after drop administration. Outcomes were compared using linear mixed models. Predictors included group (between-subjects), time (within-subjects), and the group by time interaction.
Results: One hundred and thirty-seven participants, mean age 67 years (54.3% female), were evaluated. Most drops showed increased tear meniscus height at 5 and 15 minutes compared to baseline. Changes in non-invasive keratographic break up time and lipid layer thickness were more variable. A few artificial tears demonstrated better performance with regards to tear meniscus height, non-invasive keratographic break up time or lipid layer thickness; but no single drop outperformed others across all three measured endpoints. Perflourohexyloctane did not show better performance in any test parameter.
Conclusion: The performance of various over-the-counter artificial tears can be determined with non-invasive imaging technologies. Certain drops can outperform others with regard to individual test parameters suggesting that personalization or optimization of therapy may be possible. Both active and inactive ingredients contribute to the efficacy of artificial tears. Further work is needed to determine if differences observed here translate into meaningful clinical differences for dry eye disease treatment. This report highlights the complexity of dry eye disease and the need for ongoing work to find optimal ways to treat the ocular surface.
Keywords: dry eye disease, perflourohexyloctane, tear meniscus height, lipid layer thickness, non-invasive keratographic break up time, LipiView II, Oculus Keratograph 5M
Introduction
Dry Eye Disease (DED) is one of the most common disorders encountered in eye clinics with an estimated 4.91 million affected Americans and tens of millions more with subclinical manifestations.1,2 In one study, DED ranked as the sixth most common eye condition.3 The mainstay of DED therapy is over-the-counter (OTC) artificial tears (AT).4 Despite being available without a prescription, AT supplements remain a costly therapy. The market size for AT estimated at 3.5 billion dollars in 2024 is expected to grow from 3.73 billion in 2025 to 6.57 billion in 2034,5 and is approximately 2-fold greater than the combined sales of Restasis (sales of 1.2 billion in 2020) and Xiidra (sales of 487 million in 2022).5,6 AT contribute to the financial burden of DED treatment which has an average yearly cost of over eleven thousand dollars per patient.7
AT are complex formulations comprised of multiple ingredients including astringents, demulcents, emollients, and hypertonicity agents. The composition of AT is guided by a monograph that outlines what can be included in ophthalmic over-the-counter preparations.8 By varying the allowable ingredients (both active and inactive), the various AT substitutes acquire different properties that can provide a substitute for a lack of natural tears, replace poor quality tears on the ocular surface, and/or break the inflammatory cycle incited by tear film instability and decrease ocular surface inflammation.9 Many AT claim that they target different severities of DED or that they may perform better for various subtypes of DED such as disease due to contact lenses wear or extended work on video display terminals.
Despite being the most common DED therapy and claims that certain AT may perform better for certain types of disease,10 scant information is available to guide eye care professionals or patients about how to optimize their AT choices. The American Academy of Ophthalmology Preferred Practice Pattern currently does not provide any specific guidance regarding AT supplementation.11 One meta-analysis indicated that hyaluronic-acid-based formulations may have utility in the treatment of DED over non-hyaluronic acid based formulations and saline.12 Another study compared carboxymethylcellulose-hyaluronic acid and carboxymethylcellulose preparations.13 Frequent limitation of such studies is that they utilize non-comparable measurements as endpoints.14
One explanation for the paucity of data is the limited number of methods previously available to objectively assess AT performance. Unfortunately, DED lacks a gold standard for measurement of disease status.15 Conventional clinical measures of tear film function and architecture such as Schirmer’s tear test, tear osmolarity, and fluorescein tear break up time all involve manipulation of the ocular surface and eyelids or the application of eye drops or dyes which stimulate reflex tearing; all confound attempts to measure the effects of AT.16 Recently introduced imaging technologies that have gained clinical acceptance (reviewed in17–19) make it possible to measure tear film architecture and function in an objective, non-invasive manner techniques. Two devices commonly used in clinical practice that allow such measurements are the Oculus Keratograph 5M® (OK5M) (OCULUS Inc., Arlington, WA 98223, USA) and the LipiView® II Ocular Surface Interferometer (LV2) (TearScience, Johnson & Johnson company).
The OK5M is an advanced keratograph that uses modified optics and a curved keratograph head to provide consistent and uniform illumination across the visible ocular surface (conjunctiva and cornea).20 This device provides noninvasive measurement of tear meniscus height (TMH) (measured from anterior segment images using digital calipers). TMH is the most direct assessment of tear film volume, which when low, may be a key pathogenic mechanism and a diagnostic sign for DED independent of the DED type.15 Noninvasive TMH measurements were reproducible and reliable in one study,21 correlated with OSDI score in a Hispanic population,22 and distinguished DED from normal patients in a third.23
Additional capabilities of the OK5M include the ability to measure non-invasive keratographic break up time (NIKBUT) via automated detection and mapping of tear breakup locations over time. As previously described,14,24 NIKBUT measured in seconds and automatically detected by the device, represents the time between the last complete blink and the first perturbation of placido disc rings projected onto the surface of the cornea. The OK5M generates two measures for NIKBUT: the time at the first breakup of tear film (NIKBUT-first) and the average time of all breakup incidents (NIKBUT-average). Measurement of NIKBUT may be preferable to traditional fluorescein breakup time.16 Measurements of TMH and NIKBUT obtained with the OK5M have been shown to be reliable with good repeatability and reproducibility in patients with and without DED.25 Additionally, we have observed that OK5M measurements of TMH and NIKBUT can be used to follow the evolution of dry eye disease in laboratory models of aqueous deficient DED.26
The tear film’s outermost layer (lipid layer), a barrier to evaporation of the underlying aqueous and mucin layers, can be assessed with the LV2. The LV2 projects monochromatic light onto the cornea and records a 20 second video that analyzes the light reflection and interference pattern from the tear film using interferometry to measure the lipid layer thickness (LLT). Data is displayed in interferometric color units (ICU), where 1 ICU reflects approximately 1 nm of LLT. Low LLT values < 69 nm often indicate more severe lipid deficiency and evaporative dry eye.27
Herein, we present a comparative analysis of 13 over the counter AT formulations and perflourohexyloctane (Miebo®), a recently approved medication that stabilizes the tear film by preventing evaporation. We assess performance using the OK5M and LV2 devices to measure the changes that occur in TMH, NIKBUT and LLT values after eye drop instillation. This report expands upon currently available data in the literature comparing AT performance and may provide a rationale for practitioners and patients to make better informed therapeutic decisions.
Materials and Methods
Patients
This study was approved by the Stony Brook Institutional Review Board and complied with the Declaration of Helsinki. Subjects over 18 years of age were recruited from multi-specialty clinics at an outpatient tertiary eye care center during regular clinic visits. Participants represented a broad spectrum of patients that would be expected in a comprehensive eye clinic. All participants had normal anterior segment exams without recent surgery or acute ophthalmology pathology requiring medical or surgical treatment. For the purpose of this study, participants were not classified according to their baseline DED symptoms or status. In order to minimize known environmental influences on the ocular surface and measurements taken with the devices, all participants were recruited during the summer months (June–August) and all were measured in a temperature (70±5 ℉) and humidity (40±5rH) controlled environment. Participants were enrolled after their eye exam confirmed the absence of active eye pathology. Up to two different eye drop brands were tested on a given day. Each participant received only one of the 2 eye drop brands tested on a given day. Both eyes of each participant were tested using the same study eye drop (when both eyes could be studied).
Measurements
TMH, NIKBUT, and central LLT were measured at baseline and at 5- and 15-minutes following administration of one drop of the study agent dispensed from its commercial bottle. Measurements were taken in both left and right eye for each participant and evaluated independently. The OK5M was used to obtain measures of TMH and NIKBUT as per manufacturer instructions. Briefly, TMH was measured along the lower lid under the center of the pupil with built-in software calipers from a single high-resolution image taken using infrared illumination. For NIKBUT, three successive measurements were taken and the mean of three Average NIKBUT values was used for statistical comparisons. A single measurement of central LLT was obtained using the LV2 as per manufacture guidelines.
Thirteen over the counter (OTC) AT preparations were analyzed. The active and inactive ingredients for each drop are shown in Table 1. Balanced salt saline (BSS), approximately 300 mOsm/Kg, was used as a control. Perfluorohexyloctane (Miebo®) was also studied due to its immediate action on tear film stability.
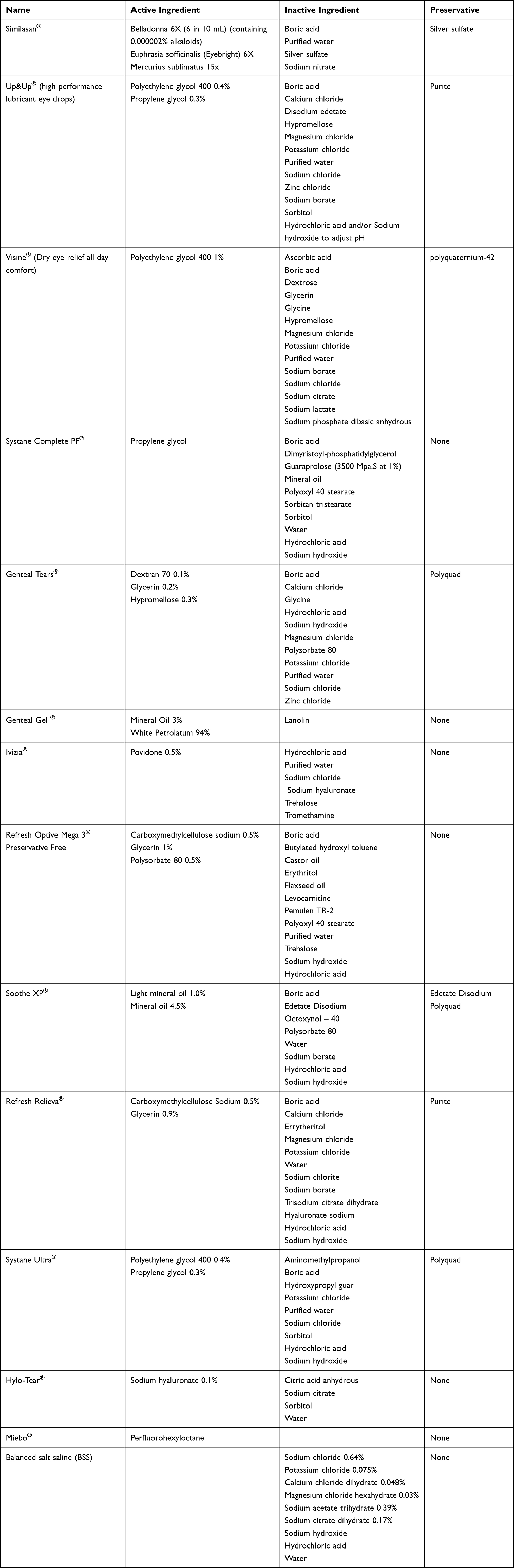 |
Table 1 List of Active and Inactive Ingredients of Utilized Eye Drops |
Statistics
Outcomes were compared between groups using linear mixed models (LMM). Predictors included group (between-subjects), time (within-subjects), and the group by time interaction. The correlation between observations measured repeatedly within each subject (ie, multiple eyes and multiple time points) was modeled using random subject effects and structured variance-covariance matrices. The best-fitting model was selected according to information criteria. Least-square (LS) means and standard error were estimated, plotted, and compared post-hoc to determine the nature of significant effects. All analyses were performed using SAS, version 9.4 (Cary, NC).
Results
A total of 137 patients participated in the study. Mean age was 67.01 years and 54.3% were female. Baseline characteristics of the measured tear film parameters for the entire group and each of the tested tear drops are given in Table 2. No significant differences were seen in mean tear meniscus height between any of the tested drops and baseline for the entire group. With the exception of Hylo-Tear and Up&Up which both had a slightly lower average NIKBUT at baseline, all other tested drops were statistically equivalent to the entire group at baseline. For LLT most eye drops were equivalent to the entire group at baseline, with the exception of Systane Ultra which was slightly higher at baseline, and Soothe XP and Visine which were lower at baseline compared to the entire group.
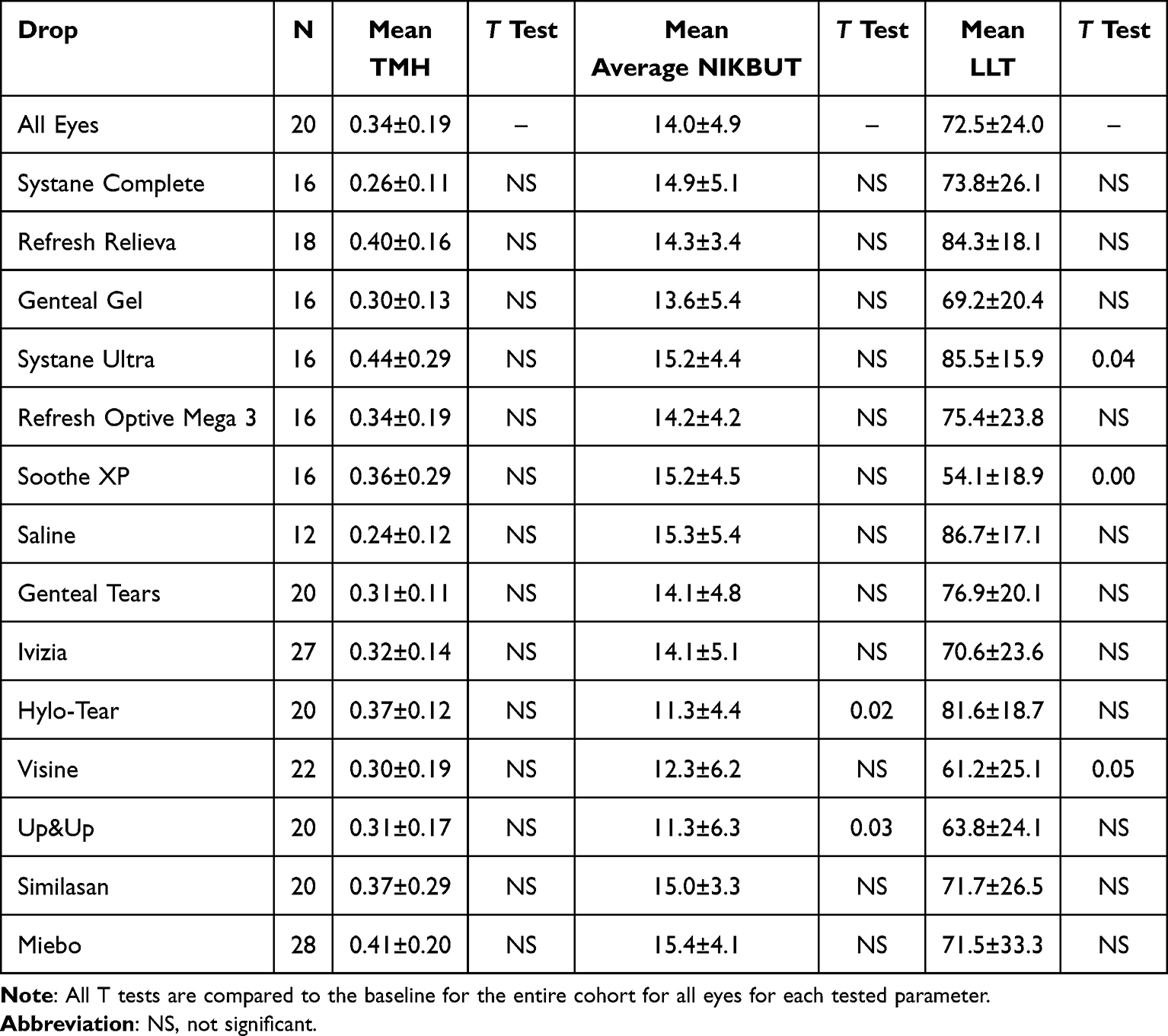 |
Table 2 Baseline Characteristics of Measured Tear Film Parameters for Each Tested Drop |
As seen in Figure 1, almost all drops showed increased TMH at 5 minutes compared to baseline levels. TMH was slightly higher at 15 minutes for most eye drops as well. However, statistical improvement was only reached for Genteal Gel®, Refresh Optive Mega 3®, and Hylo-Tear® at 5 minutes.
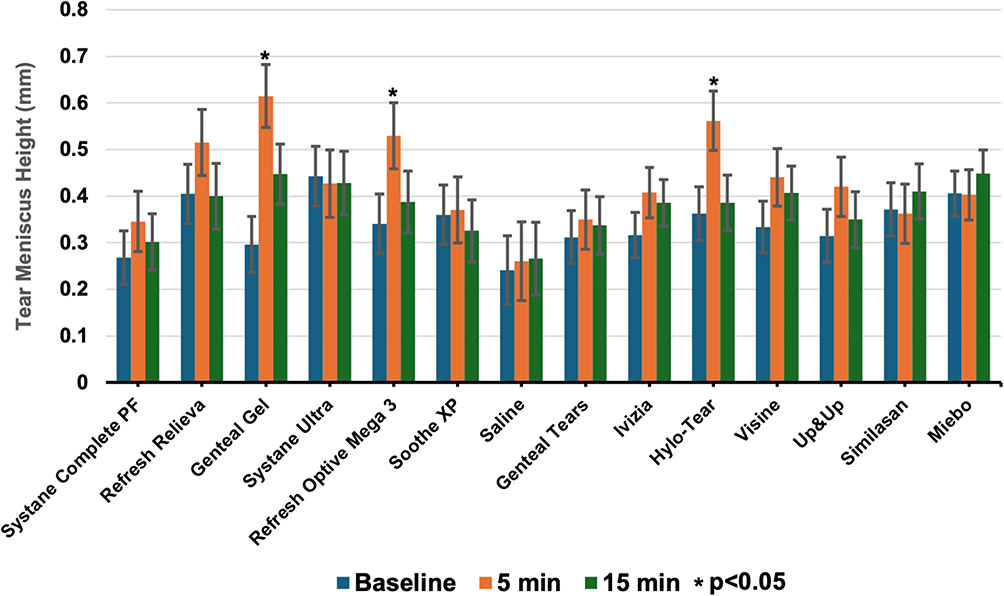 |
Figure 1 Bar graph showing tear meniscus height (TMH) at baseline, 5 minutes, and 15 minutes following drop administration. Asterisks (*) indicate significant change (p<0.05) compared to baseline. Genteal Gel, Refresh Optive Mega 3, and Hylo-Tear outperformed other drops at 5 minutes. By 15 minutes no drops showed statistically significant change from baseline readings. |
Changes in NIKBUT (Figure 2) were more varied than those of TMH with about half of the drops showing some improvement at 5 minutes, and the other half showing no change or a small decline. Only Refresh Relieva® and BSS showed significant improvement at 5 minutes, while Visine®, Up&Up®, and Meibo® showed significant decreases in NIKBUT at 5 minutes.
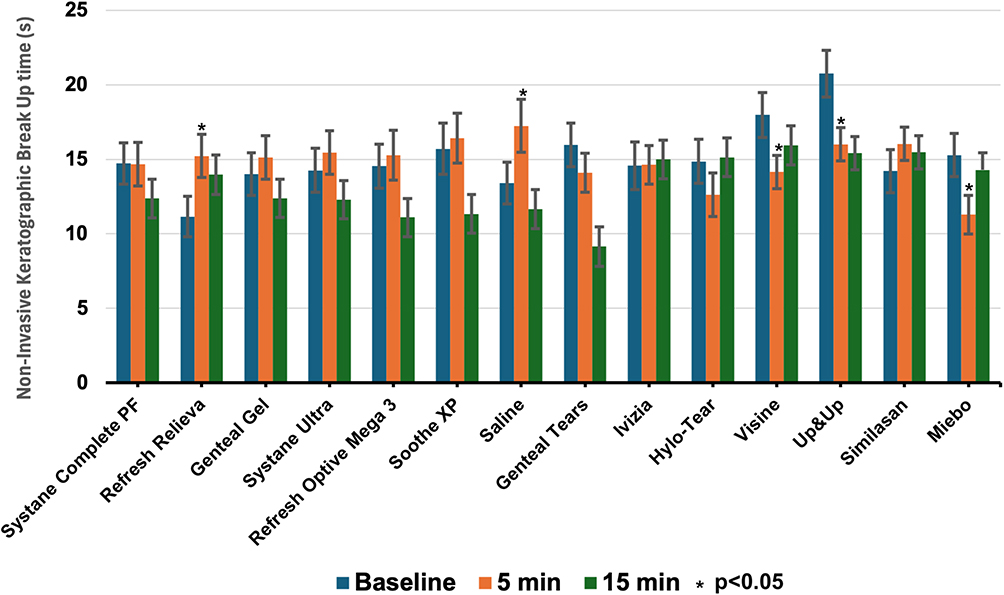 |
Figure 2 Bar graph showing non-invasive keratographic break up time (NIKBUT) at baseline, 5 minutes, and 15 minutes following drop administration. Asterisks (*) indicate significant change (p<0.05) compared to baseline. Refresh Relieva, and Saline (BSS) demonstrated significant improvement at 5 minutes while Visine, Up&Up, and Miebo demonstrated significant detrimental effects at 5 minutes. No drop showed statistically significant improvement at 15 minutes. |
Measured changes in LLT (Figure 3) were also varied with about half showing an increase and the remainder a small decrease at 5 minutes. Although Genteal Gel®, Refresh Optive Mega 3®, BSS, and Miebo® showed an increase in LLT compared to baseline at 5 minutes, none reached statistical significance. Additionally, AT that demonstrated a statistical decrease in LLT at 5 minutes included Refresh Relieva®, Hylo Tear®, Visine®, and Up&Up®.
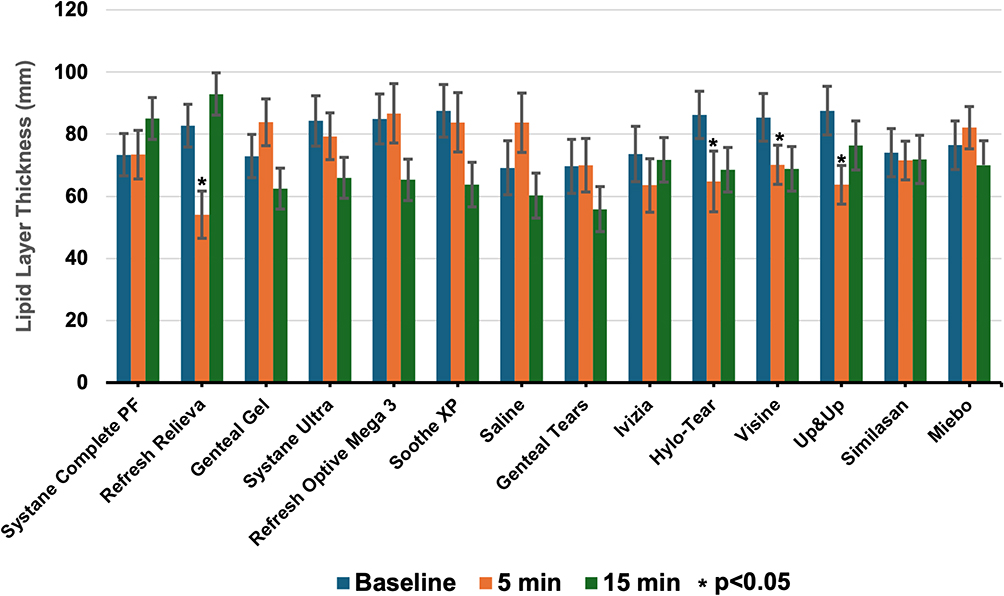 |
Figure 3 Bar graph showing lipid layer thickness (LLT) at baseline, 5 minutes, and 15 minutes following drop administration. Asterisks (*) indicant significant change (p<0.05) compared to baseline. No drop demonstrated significant improvement from baseline at 5 or 15 minutes. Refresh Relieva, Hylo-Tear, Visine, and Up&Up showed deleterious effects at 5 minutes. |
The changes in TMH, NIKBUT and LLT for each drop ranked by percent change at 5 minutes are given in Table 3. At 5 minutes an increase greater than or equal to 10% in magnitude was seen in 10/14 drops for TMH, 5/14 drops for NIKBUT, and 2/14 drops for LLT.
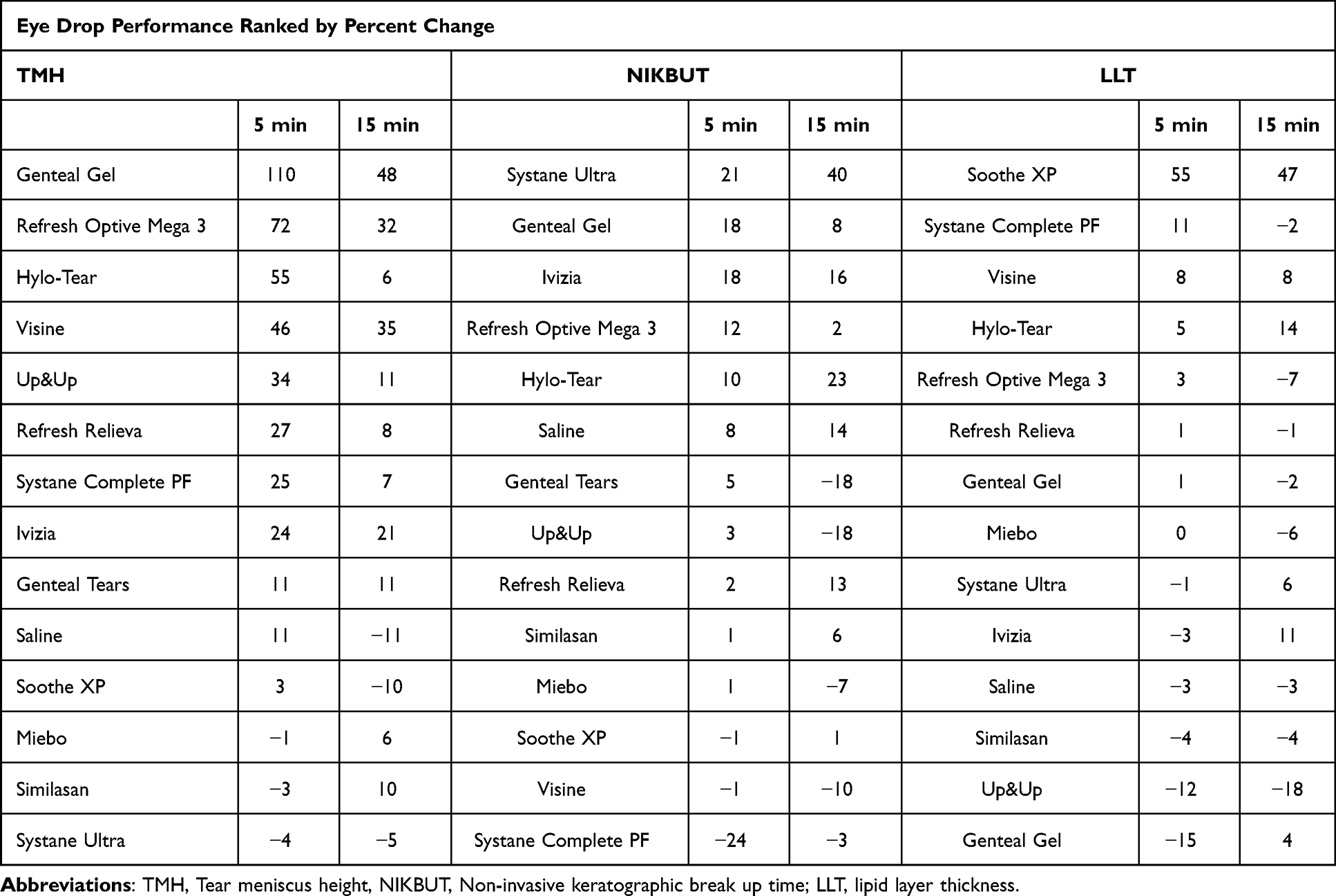 |
Table 3 Percent Change in Eye Drop Performance at 5 and 15 Minutes Compared to Baseline |
The comparative performance of various drops analyzed using a LMM approach that compensated for baseline values of each parameter as well as time are given for TMH, NIKBUT and LLT in Tables 4–6, respectively.
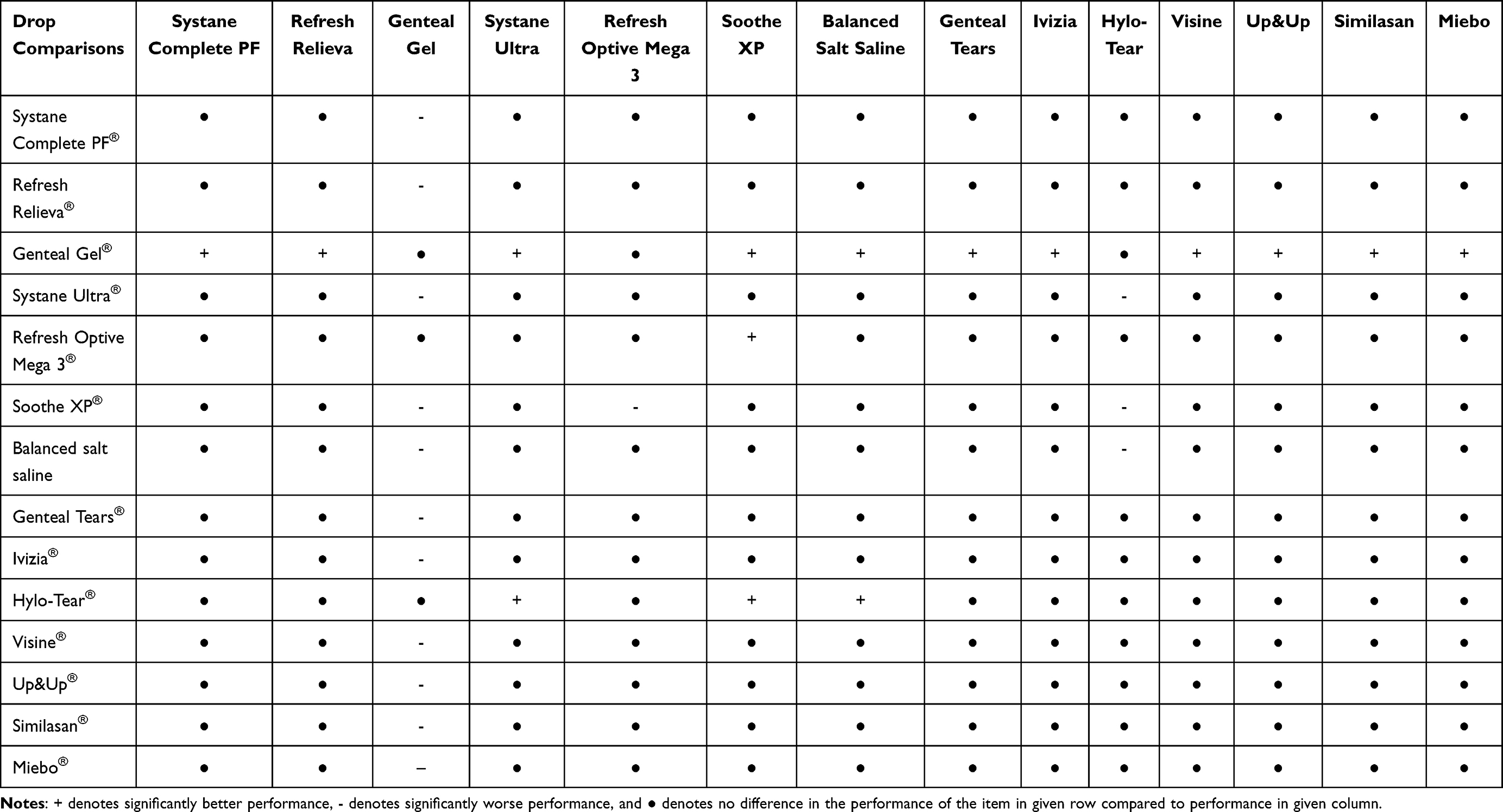 |
Table 4 Comparative Tear Meniscus Height Performance for Various Eye Drops |
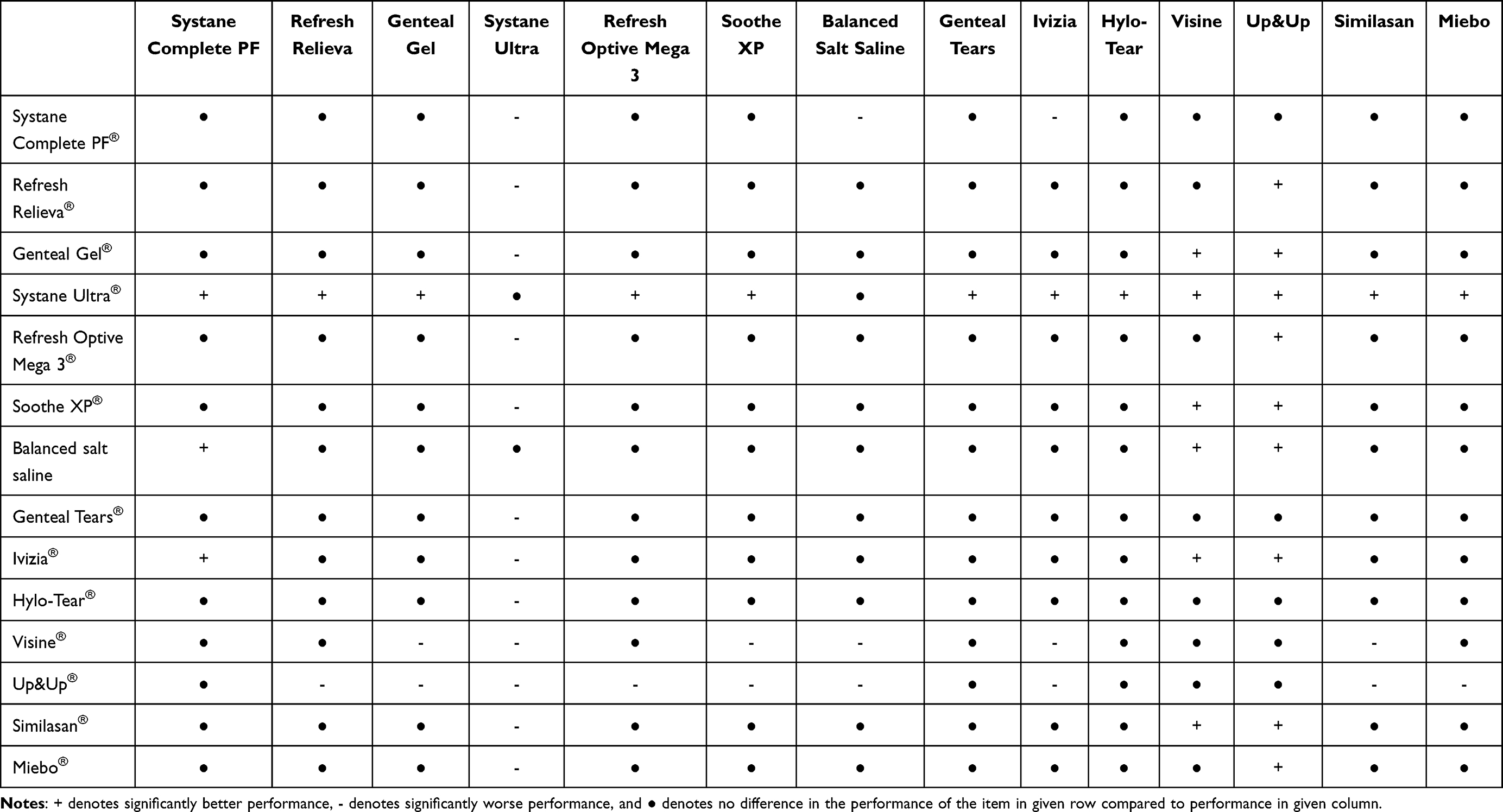 |
Table 5 Comparative Non-Invasive Keratographic Break up Time Performance for Various Eye Drops |
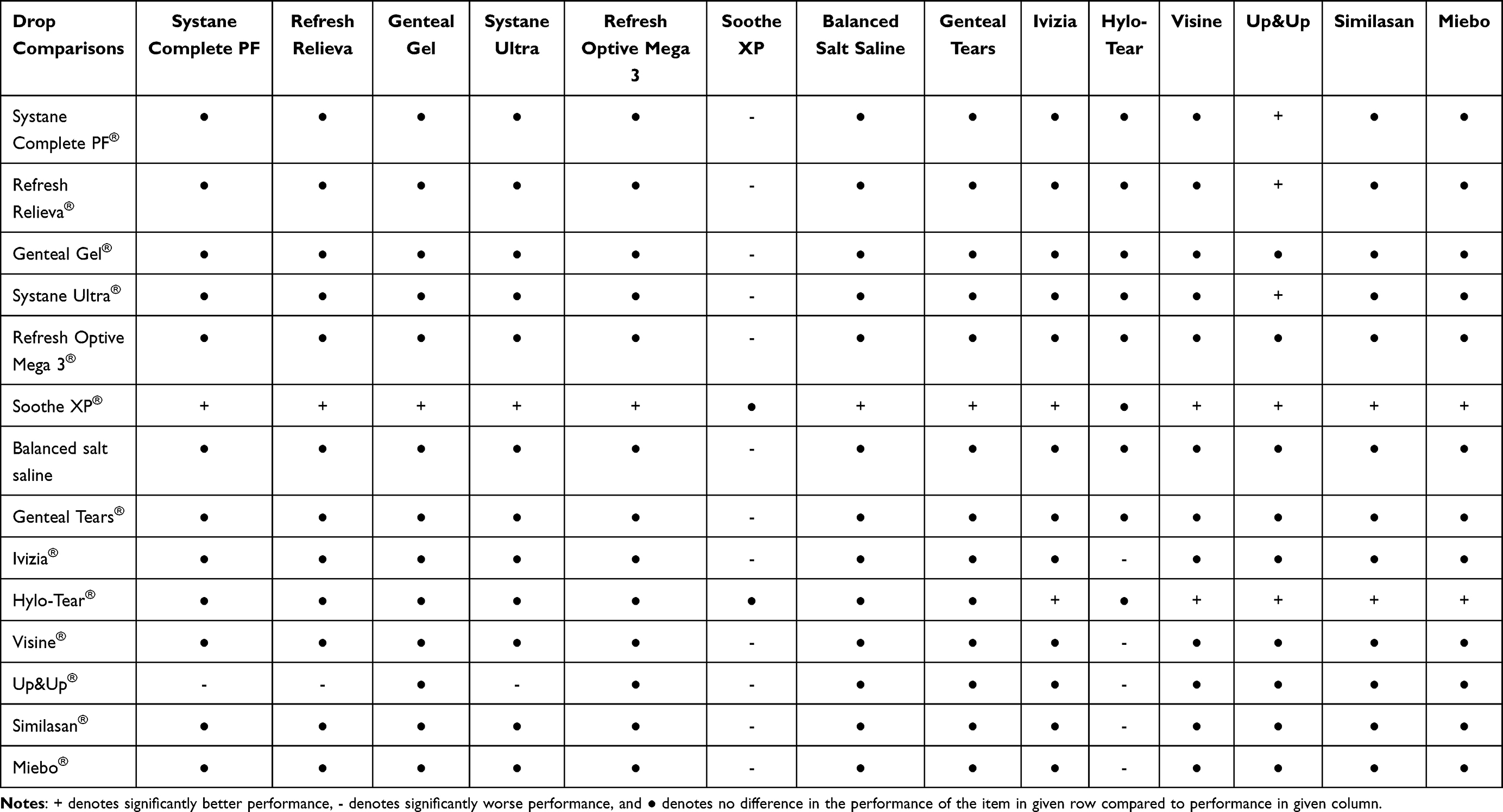 |
Table 6 Comparative Lipid Layer Thickness Performance for Various Eye Drops |
As seen in Table 4, most tested drops show similar performance statistically with regard to TMH. The one exception is Genteal Gel which outperformed all drops other than Hylo-Tears and Refresh Optive Mega 3. Hylo-Tear also performed well, showing better performance than 3 other eye drops tested here.
Fewer drops demonstrated increases in NIKBUT (Table 5). LMM analysis showed Systane Ultra outperformed all other commercially available eye drops tested for NIKBUT and was better but statistically equivalent to BSS drops. Among commercially available drops, Ivizia had the second best performance for NIKBUT, but only outperformed 3/14 drops tested. Up&Up and Visine underperformed relative to most other eye drop supplements.
Few drops showed large changes in LLT in this study (Table 6). Only 2/14 drops tested showed LLT increases >10% at 5 minutes. LMM analysis indicated that only one drop, SootheXP, excelled, outperforming all other drops except Hylo-Tears which performed statistically the same. Hylo-Tear also excelled, outperforming 5 other eye drops.
Discussion
Although the most commonly utilized therapy for patients with DED is AT, no clear guidance is available for use of these therapies, unlike prescription medications. Little comparative information is available to help practitioners or patients make informed decisions about which eye drop might provide better results. This report provides objective data about relative AT performance and may help practitioners make informed decisions about their use.
Herein we provide comparative performance data for a number of common AT supplements, as well as one recently available prescription medication perfluorohexyloctane (Miebo®). Although this study did not evaluate all available OTC AT supplements, the broad selection tested here represents the major categories of active ingredients while inclusion of perfluorohexyloctane provides comparative performance to an approved prescription medication whose mechanism of action is through stabilization of the tear film. Given perfluorohexyloctane’s immediate action, comparisons to AT preparations are reasonable unlike lifitegrast and cyclosporin, which take much longer for their effects to occur.
We assess the ability of these eye drops to acutely change metrics of TMH, NIKBUT and LLT obtained with non-invasive imaging methods following their administration. As these metrics are used to commonly assess the tear film in clinical practice, we believe they should also serve as reasonable measures to assess how well AT supplements applied to the ocular surface mimic the naturally produced tears. Given the volume of each AT drop added to the ocular surface greatly exceeds the volume of the native tear film,28 it is likely that the measurements taken represent the characteristics of the added AT and not the patient’s own native tears.
As measured here, TMH may only reflect the residence time of the added AT drop on the ocular surface rather than tear production or the patient’s natural tear volume. Similarly, as measured here LLT and NIKBUT likely represent how well the various AT supplements mimic the natural tear film and are unlikely to represent actual physiologic responses or changes in a patient’s native tear film. However, if used very frequently, these measurements might indicate which AT products can replicate normal tear functions.
Our data suggests that the various OTC AT do not perform the same with regard to the parameters measured here. No single AT drop outperformed all others with regard to TMH, NIKBUT, and LLT. However, some trends were apparent. For TMH, GenTeal Gel® performed best; for NIKBUT, Systane Ultra® outperformed most other drops; and for LLT, Soothe XP® had the best performance. Of note, this study was limited to changes over 15 minutes and it is possible that different conclusions might be made with a different time endpoint. In addition, drop size of the AT was not controlled for; instead we simply applied a drop from the commercial dispenser, representing the real world clinical experience when using them. We also did not control patients for their underlying DED status, as all drops applied were in excess of the natural tear volume present. Despite these confounding factors, it is clear that the different OTC AT have different properties and may thus allow personalization of therapy.
Our study demonstrates the positive effect of AT on multiple DED parameters which is also consistent with a conclusion from the study by Maity et al.29 Although the study by Maity et al did not show a significant difference between efficacy of any of the tested AT supplements used, this is most likely due to the specific AT drops tested which were different than those studied here. In addition, experimental differences including the patient population studied may also contribute to this discrepancy. Although both studies show beneficial effects of AT, the differences between eye drop performance only highlights the need for further work in this area to determine best practices for patients.
Our results also indicate that OTC AT cannot be compared based solely on the composition of their active ingredients. This is evident from the comparison of NIKBUT between Systane Ultra® and Up&Up®. Both of these drops have polyethylene glycol 400 0.4% and propylene glycol 0.3% as active ingredients. Despite the same active ingredient composition, the drops behave differently in NIKBUT testing, suggesting that the inactive ingredient, hydroxypropyl guar in the case of Systane Ultra®, also has an important impact on drop performance. For this reason, it is probably preferable to refer to them by their brand names, rather than to define them by their generic components.
Comparisons of OTC AT to perfluorohexyloctane did not show any significant changes with regard to TMH, NIKBUT or as might be expected, to LLT. This may be due to the short duration of this study, as perfluorohexyloctane has been shown to improve DED upon prolonged use.30,31 It is also possible that the LV2 interferometry based method to measure LLT of natural tears cannot measure or detect the presence of perfluorohexyloctane.
Conclusion
The performance of various OTC AT can be determined with non-invasive imaging technologies. The study performed here measures how well these AT supplements can acutely mimic the characteristics of the natural tear film. Although no single drop outperforms all others, certain drops can outperform others with regard to individual test parameters suggesting that some personalization of therapy or optimization of therapy may be possible (Table 7). Given that drops with the same active ingredient composition can perform differently (presumably due to the inactive ingredients), further work needs to be done to examine more of the commercially available formulations. In addition, further work needs to be done to determine if the differences in eye drop performance measured here with imaging translate into meaningful clinical differences in DED symptoms and physical findings such as corneal staining with more extended use of these drops. This report highlights the complexity of DED and the need for ongoing work to find optimal ways to treat the ocular surface.
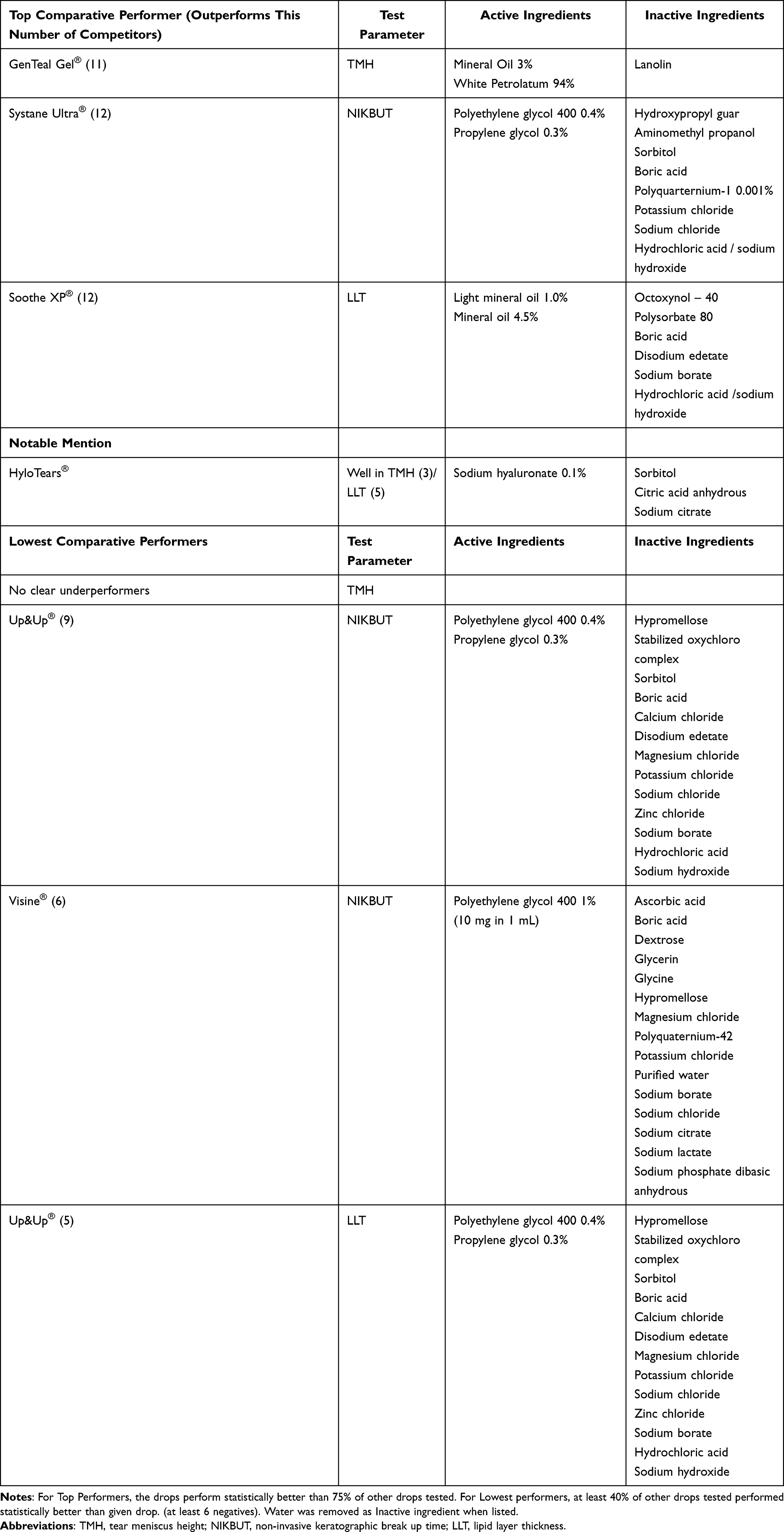 |
Table 7 Comparison of Active and Inactive Ingredients for Best and Worst Performing Eye Drops for Various Dry Eye Parameters |
Acknowledgments
The authors would like to thank Ann Marie Lavorna RN for her dedication and invaluable administrative help with this project.
Disclosure
Dr Basil Rigas reports equity positions from Apis Therapeutics LLC, JCARE Pharmaceuticals, LLC and Medicon Pharmaceuticals, Inc., outside the submitted work. In addition, Dr Basil Rigas has a patent “Treatment of dry eye disease” issued to Apis Therapeutics LLC. The authors report no other conflicts of interest in this work.
References
1. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocular Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
2. Lemp MA, Foulks GN. The epidemiology of dry eye disease: report of the epidemiology subcommittee of the international dry eye WORKSHOP (2007). Ocular Surf. 2007;5(2):93–107.
3. Bradley JL, Ozer Stillman I, Pivneva I, Guerin A, Evans AM, Dana R. Dry eye disease ranking among common reasons for seeking eye care in a large US claims database. Clin Ophthalmol. 2019;13:225–232. doi:10.2147/OPTH.S188314
4. Messmer EM. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int. 2015;112(5):71–81;quiz82. doi:10.3238/arztebl.2015.0071
5. Gotadki R. Artificial Tears Market Research Report Information By Type (Polyethylene Glycol, Propylene Glycol, Cellulose, Glycerin, and Others) by Delivery Mode (Eye Drops, Ointments, and Sprays) by Application (Dry Eye Syndrome, Allergies And Infections, and Others), by Distribution Channel (Hospital Pharmacies, Drug Stores, Retail Pharmacies, and Online Pharmacies), by Region (North America, Europe, Asia-Pacific, and Rest of the World) - Forecast till 2034; 2023. Available from: https://www.marketresearchfuture.com/reports/artificial-tears-market-12059.
6. Liu A. After $3.4B deal and EU withdrawal, Novartis looks to sell Xiidra: Bloomberg; 2023. Available from: https://www.fiercepharma.com/pharma/after-34b-deal-and-eu-withdrawal-novartis-wants-xiidra-gone-sale-some-eye-meds-bloomberg.
7. Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. doi:10.1097/ICO.0b013e3181f7f363
8. Over-the-Counter (OTC) monograph M018: ophthalmic drug products for over-the-counter human use. Food and Drug Administration.
9. Munoz EC, Patino AO, Marin DJ, et al. Immediate impact on tear osmolarity following the application of different ocular lubricants in patients experiencing moderate dry eye symptoms. Cornea. 2024;43(8):1040–1043. doi:10.1097/ICO.0000000000003493
10. Labetoulle M, Benitez-Del-Castillo JM, Barabino S, et al. Artificial tears: biological role of their ingredients in the management of dry eye disease. Int J Mol Sci. 2022;23(5):2434. doi:10.3390/ijms23052434
11. Amescua G, Ahmad S, Cheung AY, et al. Dry eye syndrome preferred practice pattern(R). Ophthalmology. 2024;131(4):P1–P49. doi:10.1016/j.ophtha.2023.12.041
12. Yang YJ, Lee WY, Kim YJ, Hong YP. A meta-analysis of the efficacy of hyaluronic acid eye drops for the treatment of dry eye syndrome. Int J Environ Res Public Health. 2021;18(5):2383. doi:10.3390/ijerph18052383
13. Aragona P, Benitez-Del-Castillo JM, Coroneo MT, et al. Safety and efficacy of a preservative-free artificial tear containing carboxymethylcellulose and hyaluronic acid for dry eye disease: a randomized, controlled, multicenter 3-month study. Clin Ophthalmol. 2020;14:2951–2963. doi:10.2147/OPTH.S256480
14. Hong J, Sun X, Wei A, et al. Assessment of tear film stability in dry eye with a newly developed keratograph. Cornea. 2013;32(5):716–721. doi:10.1097/ICO.0b013e3182714425
15. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocular Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
16. Bron AJ, Abelson MB, Ousler G, et al. Methodologies to diagnose and monitor dry eye disease: report of the diagnostic methodology subcommittee of the International Dry Eye WorkShop (2007). Ocular Surf. 2007;5(2):108–152.
17. Szczesna DH, Alonso-Caneiro D, Iskander DR, Read SA, Collins MJ. Predicting dry eye using noninvasive techniques of tear film surface assessment. Invest Ophthalmol Vis Sci. 2011;52(2):751–756. doi:10.1167/iovs.10-5173
18. Llorens-Quintana C, Rico-Del-Viejo L, Syga P, Madrid-Costa D, Iskander DR. A novel automated approach for infrared-based assessment of meibomian gland morphology. Trans Vision Sci Technol. 2019;8(4):17. doi:10.1167/tvst.8.4.17
19. Roy NS, Wei Y, Kuklinski E, Asbell PA. The growing need for validated biomarkers and endpoints for dry eye clinical research. Invest Ophthalmol Vis Sci. 2017;58(6):BIO1–BIO19. doi:10.1167/iovs.17-21709
20. Instruction Manual Keratograph 5M (G/77000/XXXX/EN – rev05). Instruction Manual.
21. Soares I, Ramalho E, Brardo FM, Nunes AF. Tear meniscus height agreement and reproducibility between two corneal topographers and spectral-domain optical coherence tomography. Clin Exp Optometry. 2024;1–7. doi:10.1080/08164622.2024.2341833
22. Morales‑Mancillas NR, Hernandez‑Camarena JC, Castrejón‑Perez G, Valdez‑García JE. Correlation between the ocular surface disease index and dry eye functional parameters measured with the OCULUS Keratograph 5M in a Hispanic population. Pan-Am J Ophthalmol. 2024;XX(XX):1–6. doi:10.4103/pajo.pajo_74_24
23. Chen M, Wei A, Xu J, Zhou X, Hong J. Application of keratograph and fourier-domain optical coherence tomography in measurements of tear meniscus height. J Clin Med. 2022;11(5):1343. doi:10.3390/jcm11051343
24. Koh S, Ikeda C, Watanabe S, et al. Effect of non-invasive tear stability assessment on tear meniscus height. Acta Ophthalmol. 2015;93(2):e135–9. doi:10.1111/aos.12516
25. Tian L, Qu JH, Zhang XY, Sun XG. Repeatability and reproducibility of noninvasive keratograph 5M measurements in patients with dry eye disease. J Ophthalmol. 2016;2016:8013621. doi:10.1155/2016/8013621
26. Fazio N, White E, Tourmouzis K, et al. Monitoring the evolution of dry eye disease in rabbits with advanced ocular keratography: implications for translational studies. Curr Eye Res. 2025. in press.
27. Chou YB, Fan NW, Lin PY. Value of lipid layer thickness and blinking pattern in approaching patients with dry eye symptoms. Can J Ophthalmol. 2019;54(6):735–740. doi:10.1016/j.jcjo.2019.03.005
28. Willcox MDP, Argueso P, Georgiev GA, et al. TFOS DEWS II tear film report. Ocular Surf. 2017;15(3):366–403. doi:10.1016/j.jtos.2017.03.006
29. Maity M, Allay MB, Ali MH, Basu S, Singh S. Effect of different artificial tears on tear film parameters in dry eye disease. Optometry Vision Sci. 2025;102(1):37–43. doi:10.1097/OPX.0000000000002206
30. Sheppard JD, Kurata F, Epitropoulos AT, Krosser S, Vittitow JL, Group MS. NOV03 for signs and symptoms of dry eye disease associated with meibomian gland dysfunction: the randomized phase 3 MOJAVE Study. Am J Ophthalmol. 2023;252:265–274. doi:10.1016/j.ajo.2023.03.008
31. Tauber J, Berdy GJ, Wirta DL, Krosser S, Vittitow JL; GOBI Study Group. NOV03 for dry eye disease associated with meibomian gland dysfunction: results of the randomized phase 3 GOBI Study. Ophthalmology. 2023;130(5):516–524. doi:10.1016/j.ophtha.2022.12.021
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.