Back to Journals » Journal of Inflammation Research » Volume 10
Comparative effects of the ω3 polyunsaturated fatty acid derivatives resolvins E1 and D1 and protectin DX in models of inflammation and pain
Authors Fonseca FCS, Orlando RM, Turchetti-Maia RMM, Francischi JN ![]()
Received 23 May 2017
Accepted for publication 19 July 2017
Published 29 August 2017 Volume 2017:10 Pages 119—133
DOI https://doi.org/10.2147/JIR.S142424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Flávia CS Fonseca,1 Ricardo M Orlando,2 Regina MM Turchetti-Maia,1 Janetti Nogueira de Francischi1
1Department of Pharmacology, Biological Sciences Institute, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil; 2Department of Chemistry, Exact Sciences Institute, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil
Purpose: Specialized pro-resolving lipid mediators (SPMs), also known as lipoxins, resolvins (Rvs), protectins and maresins, have been implicated in the resolution of the inflammatory process. However, a systematic comparison of their activity in the relief of inflammation and pain models is still lacking.
Materials and methods: The effects of Rvs E1 and D1 and protectin DX (PDX) were assessed in rat paws inflamed by the standard proinflammatory stimulus carrageenan or by histamine, 5-hydroxytryptamine, substance P or prostaglandin E2. The experimental outcomes were the mechanical nociceptive threshold and increase in paw volume as a measure of pain and edema formation, respectively. The analgesic and anti-inflammatory activities of the indicated SPMs were also compared with nonsteroidal (indomethacin and celecoxib) and steroidal (dexamethasone) anti-inflammatory drugs.
Results: Only RvE1 and RvD1 presented analgesic and anti-inflammatory activities in the carrageenan model, and RvE1 was twice as potent as RvD1. Both substances tended to be better analgesics than anti-inflammatory agents, with a modeling profile similar to steroidal anti-inflammatory drugs. However, proinflammatory effects (edema formation) were also detected when the mediators histamine, 5-hydroxytryptamine or substance P replaced carrageenan as the proinflammatory stimuli. The analgesic and anti-inflammatory effects of resolvins were specifically prevented by an antagonist of the leukotriene B4 receptor 1 (BLT1).
Conclusion: Rvs, as analgesic agents, may be better therapeutic agents than nonsteroidal anti-inflammatory drugs, the current choice in the relief of pain of an inflammatory origin. However, the possibility of developing adverse effects cannot be overlooked.
Keywords: specialized pro-resolving lipid mediators, edema, nociception, analgesics, anti-inflammatory drugs
Introduction
Our comprehension of the pathophysiology of inflammation suffered an important and new inflexion when special lipid mediators were found to be related to the endogenous resolution of the inflammatory process.1–3 The resolution of inflammation was no longer considered to be a passive process, but an active process that involved the so-called “resolution” factors. These pro-resolution compounds, known as specialized pro-resolving lipid mediators (SPMs), include several families of substances known as lipoxins, resolvins (Rvs), protectins and maresins.4–6 Lipoxins are derived from ω6 polyunsaturated fatty acids (PUFAs), and Rvs, protectins and maresins are derived from ω3 PUFAs.7 Diverse chemical species belong to each family and, in this sense, Rvs E1 and E2, Rvs D1–D6, maresins 1 and 2, as well as protectin D1 are well-known chemical entities.8
In fact, many conditions that are associated with the relief of inflammatory signs and symptoms are related to these pro-resolution substances, including inhibition of aberrant neutrophil trafficking and activation, stimulation of efferocytosis in apoptotic neutrophils and promotion of antiangiogenic, antifibrotic and anti-infective responses.9,10 In addition, prevention and treatment of pain conditions in mice were also described.11 Individually, a protective effect of resolvin E1 (RvE1) on the development of asthmatic airway inflammation and of resolvin D1 (RvD1) and aspirin-triggered RvD1 on the regulation of histamine (Hist)-stimulated conjunctival goblet cell secretion has been demonstrated.12,13
However, despite the continuous availability of an enormous quantity of information on earlier and new SPMs, comparisons of the various classes of SPMs in simultaneous experimental settings, for instance, in the in vivo models of inflammation and pain, are still scarce in the literature.
Thus, this work aimed to study the effects of the peripheral administration of RvE1, RvD1 and protectin DX (PDX), separately or in combination, in the models of hind paw edema and nociception induced by carrageenan (CG) in rats, in order to compare their potency and efficacy.14,15 Both experimental models are used worldwide as they offer a standard for translational therapeutic responses.16 In addition, the effects of Rvs on paw edema and nociceptive responses induced by known inflammatory mediators released locally by CG,15 such as Hist, 5-hydroxytryptamine (5-HT), substance P (SP) and prostaglandin E2 (PGE2), were also investigated. The analgesic and anti-inflammatory activities of indomethacin (INDO), celecoxib and dexamethasone were also modeled with comparative purposes. Some of the data herein were presented at the 12th World Congress on Inflammation17 in Boston (USA) and at the 48th Brazilian Congress of Pharmacology and Experimental Therapeutics18 in Foz do Iguaçu (Brazil).
Materials and methods
Animals
Male Holtzman rats, weighing 150–180 g (2 months old), were used throughout this study. The animals were provided chow and water ad libitum (n=5–7 per cage), with light/dark cycles of 12 h starting at 7:00 a.m. at the Center of Bioterism of Federal University of Minas Gerais (UFMG, Brazil). The same conditions were maintained in the laboratory where the animals were kept for 1 day before starting the experiments (see below). The project was approved by UFMG Animal Ethics Committee and follows the international and local guidelines and protocols for animal use and welfare (available at: www.mct.gov.br/upd_blob/0238/238057.pdf), with the protocol numbers 199/2014 and 376/2014. All care was taken to reduce any discomfort eventually imposed on the experimental animals.
Induction of hind paw edema and nociception
The main stimulus used to induce hind paw edema and nociception was λ-CG, which was prepared in solutions with the concentration range from 1 to 10 mg mL−1 by dilution in sterile physiologic saline. The CG solutions were injected via intraplantar route (i.pl.) in a volume of 100 μL paw−1 at time zero into the right hind paw. Other proinflammatory stimuli, such as Hist (0.1–1 mg mL−1), 5-HT (10–50 μg mL−1) and SP (10–500 μg mL−1) were also prepared and injected like CG. Aliquots from PGE2 (20 μg mL−1) in ethanol were diluted in saline (2% ethanol) to prepare the final solutions. The injected doses of the agonists followed the routine experiments published previously.19,20
Preparation and administration of RvE1 and RvD1 and PDX
Solutions of RvE1, RvD1 and PDX were prepared in ethanol and kept in a freezer at −80°C until use. On the day of the experiments, aliquots of RvE1, RvD1 and PDX solutions (20, 100 and 100 μg mL−1, respectively) were dissolved in saline according to the literature and immediately used.11 For injections, a volume of 100 μL was given by the i.pl. route in the hind paws of the rats 10 min before the stimuli. Initially, a dose–response curve for each compound was constructed using CG-injected rat paws, taken as the standard proinflammatory stimulus. Control paws were injected with equivalent ethanol solutions (in saline) at the same time. A group of animals injected with different doses of CG (100 or 500 μg per site in a volume of 100 μL) was also injected locally with RvE1 or RvD1 2 h and 50 min after CG to test their efficacy under established inflammatory and painful conditions. Control animals received locally, at the same time, the vehicle for Rvs prepared under similar conditions.
Assessment of hind paw volume
Measurements of hind paw volume (in milliliters) were obtained using a plethysmometer model 7140 (Ugo Basile, Gemonio, VA, Italy) before and 5, 15, 30, 60, 120, 180, 240, 360 min and 24 h after agonist or vehicle injections. The increase in the mean difference between the right and left paw volumes (Δ increase in volume in milliliters) obtained from five animals per group (n=5) at each time point indicated the dimension of paw edema formation. The assessment of hind paw volume always followed the nociception assessment (see below) in the course of the experiments.
Assessment of hind paw nociception
The presence of nociception was detected by a decrease in the nociceptive threshold along time given by an analgesy-meter model 7200 (Ugo Basile) to which the pads of the hind paw of the animals were submitted. Measurements were obtained before and 5, 15, 30, 60, 120, 180, 240, 360 min and 24 h after agonist or vehicle injections. The mean difference between the right and left paw threshold (Δ in grams) obtained from five animals per group (n=5), usually expressed in negative numbers, gave the dimension of paw nociception development. To overcome the eventual conditioned responses, the animals were repeatedly (10-fold) exposed to the experimental situation, without any challenge to the paws, the day before the experiments.
Treatment of animals with standard anti-inflammatory drugs
The following standard anti-inflammatory drugs were used to compare their activity with the analgesic and anti-inflammatory activities shown by RvE1 and RvD1: 1) INDO and celecoxib (CX), nonselective and selective cyclooxygenase (COX)-2 inhibitors, respectively,21 and 2) dexamethasone (DEXA) was used as the standard steroidal anti-inflammatory drug.22 All anti-inflammatory drugs, after dilution in saline (CX and DEXA) or TRIS buffer (10−1 M, pH=8.0 for INDO), were subcutaneously injected into the neck dorsum, in a volume of 1 μL g−1, half an hour before CG. The experimental drugs U-75302, GW1100 and AH7614, selective antagonists of the leukotriene B4 receptor type 1 (BLT1) and the free fatty acid receptors 1 (FFAR1/GPR40) and 4 (FFAR4/GPR120) were also used.23–25 They were diluted with an ethanol–saline solution (vehicle) and further injected i.pl. in a volume of 100 μL, 5 min (in the case of U-75302) and 15 min (for others) before the injections of RvE1. Control animals received the same volume of the respective vehicles. The experimenter was unaware of the animal treatment.
Chromatographic determination of RvE1 and RvD1 and PDX
RvE1, RvD1 and PDX were analyzed using a Waters ACQUITY UPLC™ H-Class system (Waters, Milford, MA, USA), equipped with a binary solvent delivery system. Chromatographic separation of the pro-resolving lipid mediators was achieved by gradient elution using an ACQUITY UPLC BEH C18 column (1.7 μm, 2.1×50 mm) (Waters). The mobile phase was a mixture of water (eluent A) and acetonitrile (eluent B), both with formic acid at 0.01% (v/v), with the following gradient: 0−8 min, 90%−10% A; 8−9 min, 10% A; 9–9.05 min, 10%–90% A; 9.05–10.5 min, 90% A. The column temperature was maintained at 40°C, the flow rate was maintained at 300 μL min−1 and the injection volume was 5 mL. The ACQUITY UPLC system was interfaced with a sequential (tandem mass spectrometry [MS/MS]) TQD triple quadrupole mass spectrometer (Waters Inc., Bedford, MA, USA) equipped with an electrospray ionization source operated in the negative mode (electrospray ionization−). To complement the analytical information, a photodiode array detector (PDA, Model 2998; Waters) was coupled to the outlet of the ultra performance liquid chromatography (UPLC) column, before the mass spectrometry. All conditions of the PDA and MS/MS systems are described in Table 1. The solutions used in the UPLC-PDA-MS/MS analysis were prepared by diluting the commercial standard solutions originally at 20 mg mL−1 (RvE1) or 100 mg mL−1 (RvD1 and PDX) in ethanol (Cayman Chemical, Ann Arbor, MI, USA). The working solution of RvE1 was prepared by transferring in sequence 10 mL (200 ng) of the commercial standard solution, 10 mL of ethanol and finally 180 mL of saline solution (NaCl, 0.9%, w/v) into a standard glass 2 mL vial insert. Similarly, the work solutions of RvD1 and PDX were prepared by transferring in sequence 2 mL (200 ng) of the commercial standard solutions, 18 mL of ethanol and finally 180 mL of saline solution (NaCl, 0.9%, w/v) into a standard glass 2 mL vial insert. Five microliters of work solutions were injected at least twice for each UPLC-PDA-MS/MS condition employed (multiple reaction monitoring mode or the scan mode).
 | Table 1 Conditions of the PDA and MS/MS systems during RvE1, RvD1 and PDX chemical analyses Note: The gradient and UPLC-PDA-MS/MS conditions were based on indications described in the literature.47–49 Abbreviations: MRM, multiple reaction monitoring; MS/MS, tandem mass spectrometry; PDA, photodiode array detector; PDX, protectin DX; RvD1, resolvin D1; RvE1, resolvin E1; UPLC, ultra performance liquid chromatography. |
Data and statistical analysis
The results were expressed as the mean ± standard errors of the mean. GraphPad Prism 5.00 software (GraphPad Software, Inc., La Jolla, CA, USA) was used to determine statistical significance via two-way analysis of variance (with Bonferroni’s posttest) to compare the groups for the time graphs, and Student’s t-test was used to compare the groups for the graphs that correspond to the area under the curve. P-values of <0.05 were considered statistically significant.
Materials
The drugs and reagents were purchased from the following vendors: CG, 5-HT, SP and Trizma base from Sigma Aldrich (St Louis, MO, USA); CX from Pfizer (Guarulhos, SP, Brazil); DEXA from Aché Laboratórios Farmacêuticos S.A. (Guarulhos, SP, Brazil); INDO from Sigma Aldrich (Jurubatuba, SP, Brazil); Hist from Carlo Erba (Cornaredo MI, Italy); AH7614, GW1100, PGE2, RvE1, RvD1 and U-75302 from Cayman Chemicals; ethanol from Cromoline Química Fina (Diadema, SP, Brazil) and sterile physiologic saline from Equiplex Indústria Farmacêutica (Aparecida de Goiânia, GO, Brazil). The chromatography grade acetonitrile and formic acid were supplied by Merck (Darmstadt, Germany). Throughout the UPLC-PDA-MS/MS analysis, high purity water was obtained from a Milli-Q system (EMD Millipore, Billerica, MA, USA).
Results
Concomitant inhibition of hind paw edema and nociception by RvE1 and RvD1
Previous local injection of both RvE1 and RvD1 dose-dependently prevented hind paw edema and nociception induced by CG in comparison with their respective vehicles, as observed in Figures 1A–F and 2A–F. Prevention of these effects was evident early, by 1 h of stimulus administration, and long-lasting (6 h) for both Rvs. However, RvE1 was twice as potent and efficacious as RvD1 in the reduction of the responses of hind paw edema and nociception at 3 and 2 h, respectively (285 and 570 pmol; Figures 1C and 2C). The dose–response curve, however, for both Rvs showed a narrow window of activity. Furthermore, local administration of each resolvin in paws without an inflammatory stimulus did not change the volume or the nociceptive threshold (data not shown). In addition, a combination of effective doses of both RvE1 and RvD1, injected locally, was not superior in terms of the reduction of paw edema and nociception, compared with either resolvin used individually (Figure 3). Noteworthy were the variable results shown by control animals, depending on the ethanol concentration of the respective vehicle (Figures 1 and 2). PDX, administered at a similar dose range, did not affect the paw edematogenic or the nociceptive response triggered by CG (data not shown). For this reason, PDX was not used in further biologic tests.
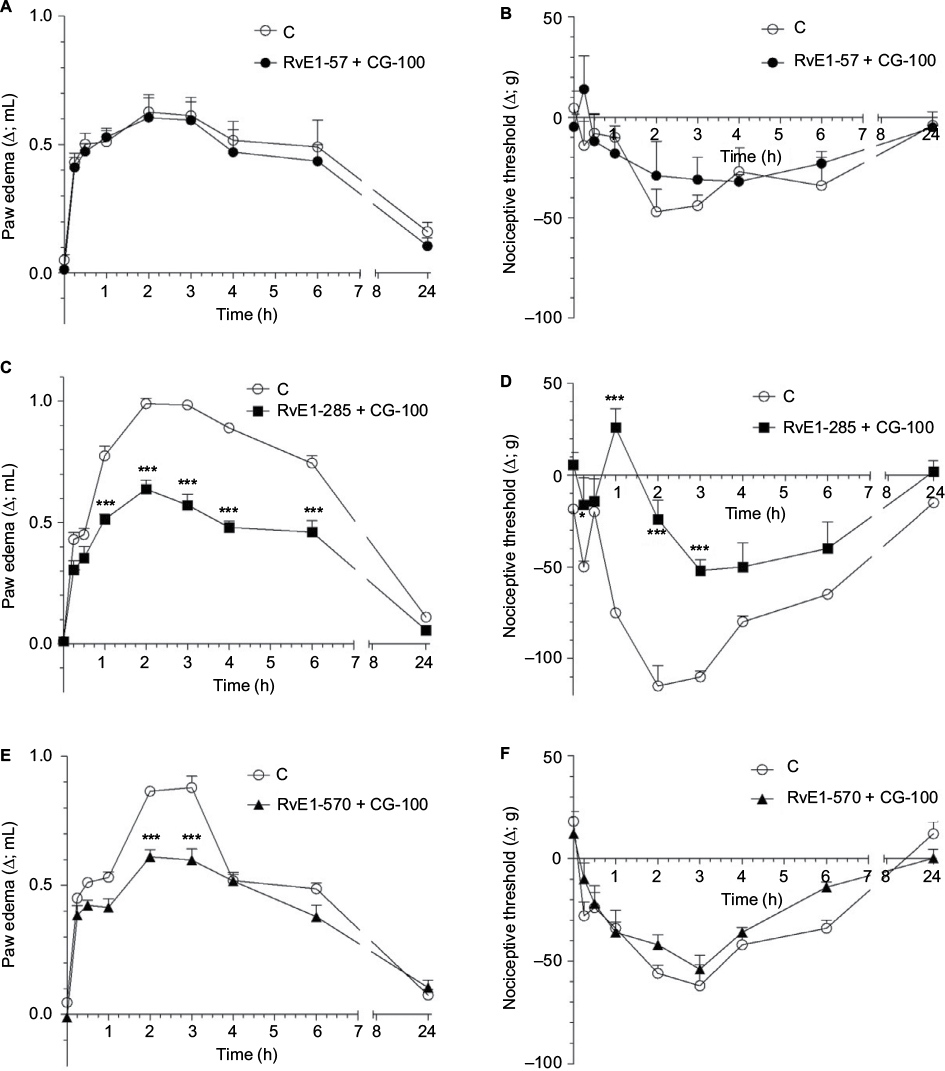 | Figure 1 RvE1 dose-dependently prevents paw edema and nociception development in rats. Notes: RvE1 (57, 285 and 570 pmol) was given 10 min before CG (100 μg); both were injected via i.pl. at a volume of 100 μL. Animals in the C group received the RvE1 vehicle at the same time and route and CG at zero time. In (A, B), the vehicle used was ethanol 1%; in (C, D), the vehicle used was ethanol 5% and in (E, F), the vehicle used was ethanol 10%. (A, C and E) show the volume difference (edema) and (B, D and F) show the difference in paw withdrawal threshold in response to the applied mechanical stimulus between the right and left paws at the depicted times. *P<0.05; ***P<0.001. Abbreviations: C, control; CG, carrageenan; i.pl., intraplantar; RvE1, resolvin E1. |
 | Figure 2 RvD1 dose-dependently prevents paw edema and nociception development in rats. Notes: RvD1 (285, 570 or 1140 pmol) was given 10 min before CG (100 μg); both were injected via i.pl. at a volume of 100 μL. Animals in the C group received the RvD1 vehicle at the same time and route and CG at zero time. In (A, B), the vehicle used was ethanol 1.07%; in (C, D), the vehicle used was ethanol 2.1% and in (E, F), the vehicle used was ethanol 4.3%. (A, C and E) show the volume difference (edema) and (B, D and F) show the difference in paw withdrawal threshold in response to the applied mechanical stimulus between the right and left paws at the depicted times. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: C, control; CG, carrageenan; i.pl., intraplantar; RvD1, resolvin D1. |
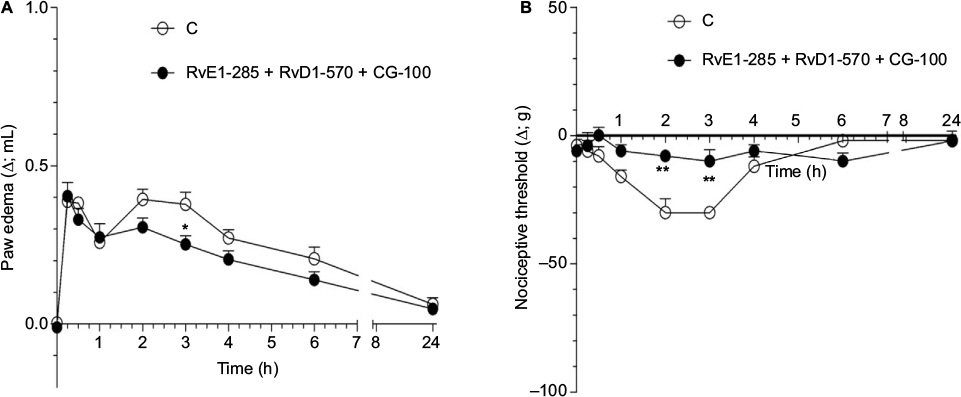 | Figure 3 Effect of pretreatment with the combination of RvE1 and RvD1 on CG-induced edema and nociception in the rat paw. Notes: RvE1 (285 pmol) immediately followed by RvD1 (570 pmol) was given 10 min before CG (100 μg); all were injected via i.pl. at a volume of 100 μL. Animals in the C group received the RvE1 vehicle (ethanol 5%) immediately followed by the RvD1 vehicle (ethanol 2.1%) at the same time and route and CG at zero time. (A) shows the volume difference (edema) and (B) shows the difference in paw withdrawal threshold in response to the applied mechanical stimulus between the right and left paws at the depicted times. *P<0.05; **P<0.01. Abbreviations: C, control; CG, carrageenan; i.pl., intraplantar route; RvD1, resolvin D1; RvE1, resolvin E1. |
RvE1 and RvD1 show a differential profile of anti-inflammatory and analgesic activity
We then tested the effects produced by fixed doses of RvE1 and RvD1 (285 and 570 pmol, respectively) on similar test models using proinflammatory chemical stimuli known to be released by CG in rat hind paws, that is, Hist, 5-HT, SP and PGE2.15 Surprisingly, a different profile of activity was observed when each resolvin was considered separately. For instance, an increase in paw edema and the appearance of hypoalgesia in response to Hist were observed with prior injection of RvE1, whereas no change in paw edema and a decrease in the nociceptive response to Hist were observed with an equipotent dose of RvD1, as shown in Figures 4 and 5. In relation to 5-HT, which per se induces paw edema and nociception,26 RvE1 also increased paw edema, whereas RvD1 promoted a reduction of the edematogenic response, although both Rvs reduced the nociceptive responses due to 5-HT. In addition, both Rvs reduced the nociceptive response and RvD1 increased the edema in hind paws in response to SP. Furthermore, no change in the slight edematogenic effect in hind paws due to PGE2 was observed when the paws were pretreated with Rvs, but a definite reduction of PGE2-induced nociceptive response was observed when both Rvs were used separately (Figures 4 and 5).
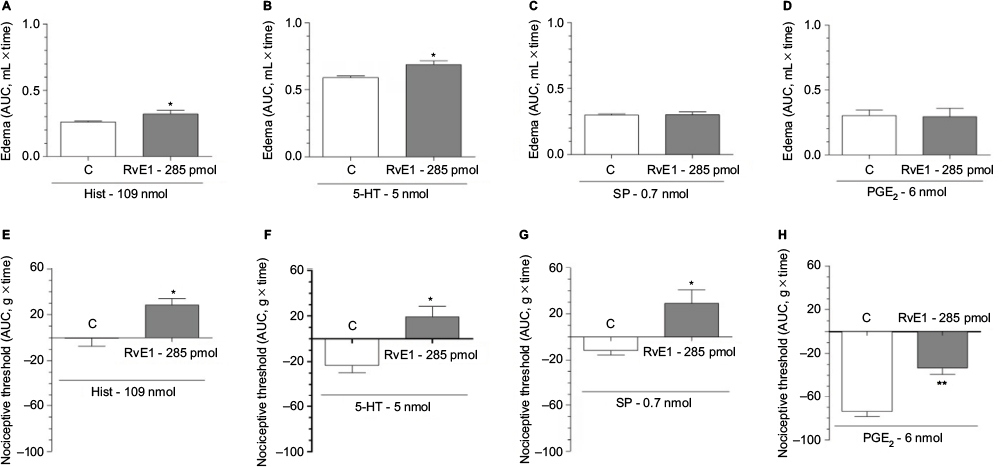 | Figure 4 Effect of pretreatment with RvE1 on edema and nociception induced by Hist (A and E; 109 nmol), 5-HT (B and F; 5 nmol), SP (C and G; 0.7 nmol) and PGE2 (D and H; 6 nmol). Notes: RvE1 (285 pmol) was injected 10 min before each stimuli; all were given via i.pl. at a volume of 100 μL. Animals in the C group received the RvE1 vehicle (ethanol 5%) at the same time and route and the proinflammatory stimulus at zero time. Data are expressed as the mean±SEM of the AUC for the volume difference (edema) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus between the right and left paws over 1 h (A–C and E–G blocks) and 2 h (D and H blocks). *P<0.05; **P<0.01. Abbreviations: 5-HT, 5-hydroxytryptamine; AUC, area under the curve; C, control; Hist, histamine; i.pl., intraplantar; PGE2, prostaglandin E2; RvE1, resolvin E1; SEM, standard error of the mean; SP, substance P. |
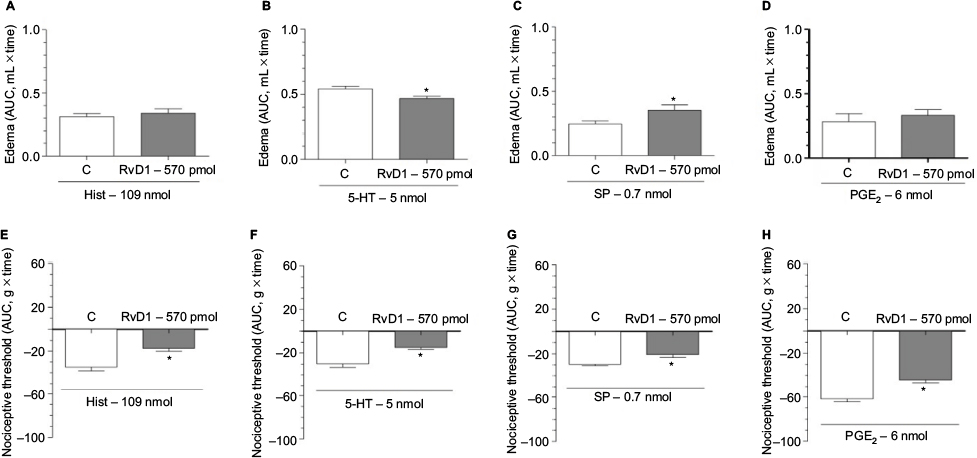 | Figure 5 Effect of pretreatment with RvD1 on edema and nociception induced by Hist (A and E; 109 nmol), 5-HT (B and F; 5 nmol), SP (C and G; 0.7 nmol) and PGE2 (D and H; 6 nmol). Notes: RvD1 (570 pmol) was injected 10 min before each stimuli; all were given via i.pl. at a volume of 100 μL. Animals in the C group received the RvD1 vehicle (ethanol 2.1%) at the same time and route and the proinflammatory stimulus at zero time. Data are expressed as the mean±SEM of the AUC for the volume difference (edema) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus between the right and left paws over 1 h (A–C and E–G blocks) and 2 h (D and H blocks). *P<0.05. Abbreviations: 5-HT, 5-hydroxytryptamine; AUC, area under the curve; C, control; Hist, histamine; i.pl., intraplantar; PGE2, prostaglandin E2; RvD1, resolvin D1; SEM, standard error of the mean; SP, substance P. |
Effects induced by RvE1 and RvD1 injected during ongoing inflammation
Next, we decided to verify whether both Rvs, given during an ongoing inflammatory reaction, would be still effective. The Rvs were injected 10 min before the maximal effects of CG (at 3 h). Two doses of CG (100 and 500 μg paw−1) and simultaneous paw edema and nociception tests were used. Interestingly, RvE1 and RvD1 posttreatment were ineffective at reducing the paw edema and nociception induced by the lower dose of CG (100 μg paw−1; data not shown). However, both Rvs were effective in reducing nociception in response to the higher dose of CG (500 μg paw−1), despite also being ineffective in reducing paw edema with this dose of CG (Figure 6).
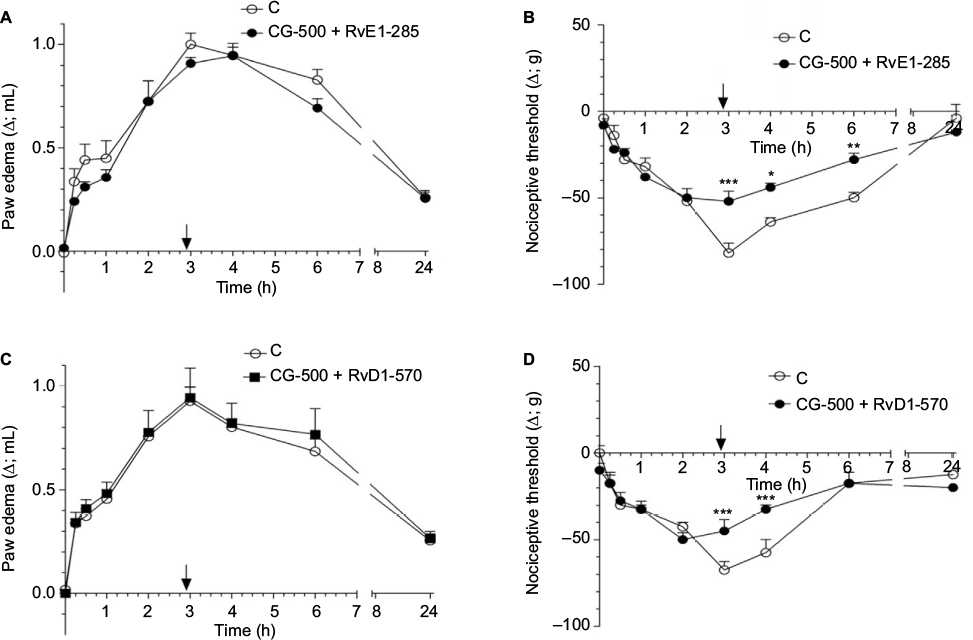 | Figure 6 Effects of posttreatment with RvE1 (A, B) and RvD1 (C, D) on an ongoing inflammatory reaction in the rat paw. Notes: RvE1 (285 pmol) and RvD1 (570 pmol) were given 2 h 50 min after CG (500 μg); both were injected via i.pl. at a volume of 100 μL. Animals in the C group received the RvE1 or RvD1 vehicle (ethanol 5% or 2.1%, respectively) at the same time and route and carrageenan at zero time. The arrow indicates the time of administration of RvE1/RvD1 or vehicle. Data are expressed as the mean±SEM of the volume difference (edema) in (A and C) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus in (B and D) between the right and left paws at the depicted times. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: C, control; CG, carrageenan; i.pl., intraplantar; RvD1, resolvin D1; RvE1, resolvin E1; SEM, standard error of the mean. |
Anti-inflammatory and analgesic activity of standard anti-inflammatory drugs (INDO, CX and DEXA)
For our purposes, the effects produced by three standard anti-inflammatory drugs, INDO, CX and DEXA, were also assessed at two dose levels of CG, 100 and 500 μg paw−1. INDO, at 4 mg kg−1, prevented both paw edema and nociception induced by 500 μg paw−1 CG (Figure 8), although no change in paw edema and nociception was observed with the lower dose of CG (100 μg paw−1; Figure 7). CX, at 30 mg kg−1, only reduced the nociception induced by 500 μg paw−1 CG (Figure 8) and DEXA, at 1 mg kg−1, was shown to be the most effective of the three anti-inflammatory drugs, in the sense that it reduced paw edema and nociception at any dose of CG tested (Figures 7 and 8).
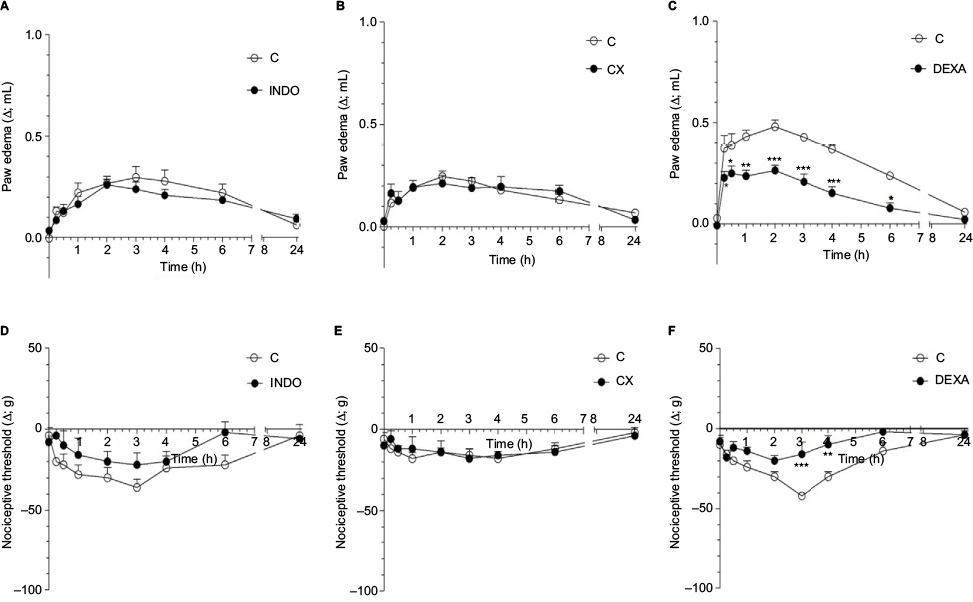 | Figure 7 Effect of pretreatment with INDO (4 mg kg−1), CX (30 mg kg−1) and DEXA (1 mg kg−1) on edema and nociception induced by 100 μg of carrageenan in the rat paw. Notes: These drugs were given subcutaneously 30 min before carrageenan (100 μg), which in turn was injected intraplantarly into the right hind paw of the animals at a volume of 100 μL. Animals in the C group received the vehicle of each drug at the same time and route and carrageenan at zero time. Data are expressed as the mean±SEM of the volume difference (edema) in (A–C) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus in (D–F) between the right and left paws at the depicted times. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: C, control; CX, celecoxib; DEXA, dexamethasone; INDO, indomethacin; SEM, standard error of the mean. |
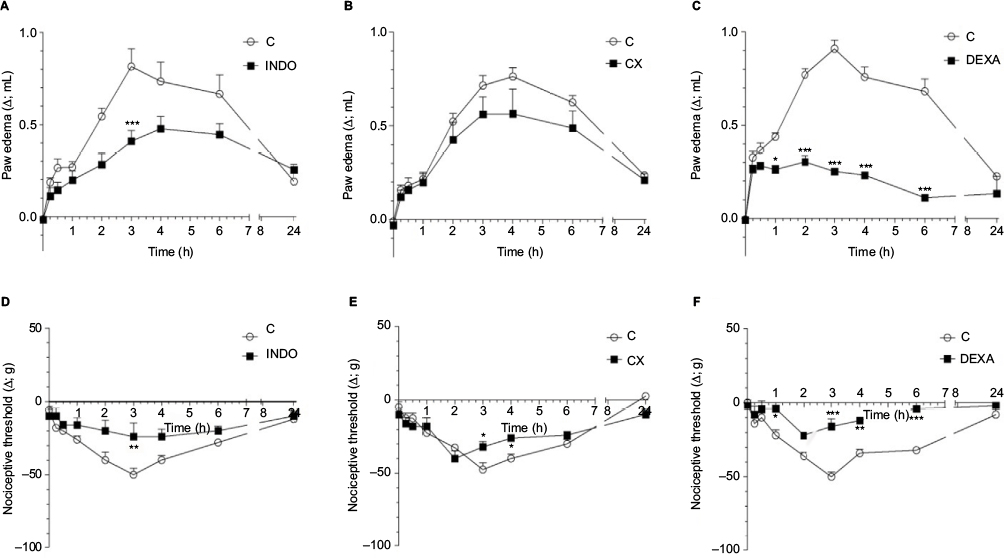 | Figure 8 Effect of pretreatment with INDO (4 mg kg−1), CX (30 mg kg−1) and DEXA (1 mg kg−1) on edema and nociception induced by 500 μg of carrageenan in the rat paw. Notes: These drugs were given subcutaneously 30 min before carrageenan (500 μg), which in turn was injected intraplantarly into the right hind paw of the animals at a volume of 100 μL. Animals in the C group received the vehicle of each drug (Tris in case of INDO and saline in case of the others) at the same time and route and carrageenan at zero time. Data are expressed as the mean±SEM of the volume difference (edema) in (A–C) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus in (D–F) between the right and left paws at the depicted times. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: C, control; CX, celecoxib; DEXA, dexamethasone; INDO, indomethacin; SEM, standard error of the mean. |
Activity of the experimental drugs U-75302, GW1100 and AH7614 on the anti-inflammatory and antinociceptive effects of RvE1
To search for the molecular targets involved in the anti-inflammatory and antinociceptive actions of RvE1, the compounds U-75302, GW1100 and AH7614, selective antagonists of the BLT1 and the free fatty acid receptors 1 (FFAR1/GPR40) and 4 (FFAR4/GPR120), respectively, were used. The compound U-75302 prevented the anti-inflammatory and analgesic activities of RvE1 in both models studied (Figure 9A, D). The compounds GW1100 (Figure 9B, E) and AH7614 (Figure 9C, F) did not affect the responses in both models. Furthermore, local administration of each compound in the paws without an inflammatory stimulus did not change the volume or the nociceptive threshold of the animals (data not shown).
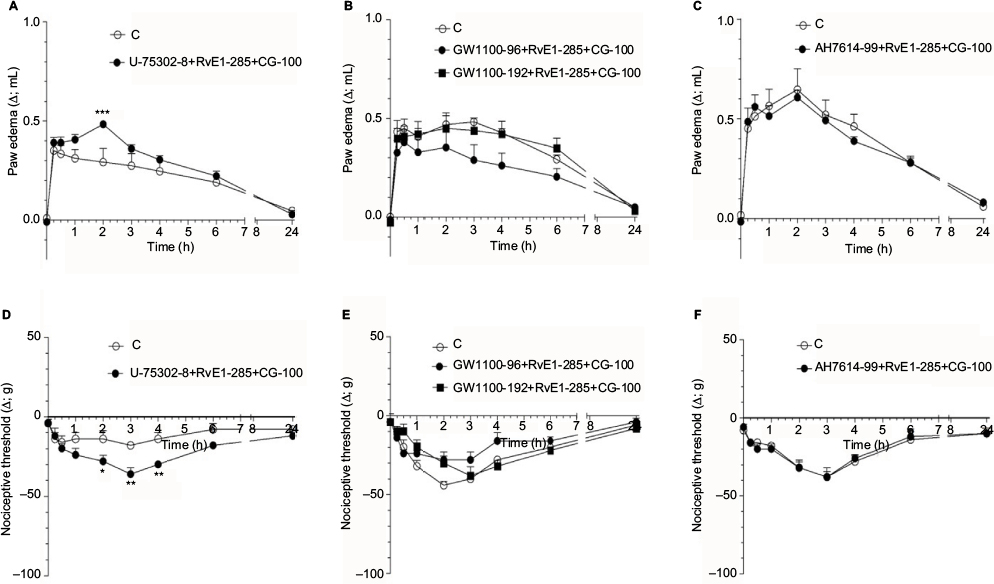 | Figure 9 Effect of U-75302, GW1100 and AH7614 on RvE1-induced relief of edema and nociception induced by CG in the rat paw. Notes: U-75302 (8 nmol), GW1100 (96 and 192 nmol) and AH7614 (99 nmol) were given 5, 15 and 15 min, respectively, before RvE1 (285 pmol), which was given 10 min before CG (100 μg); all were injected via i.pl. at a volume of 100 μL. Animals in the C group received the vehicle (U-75302 – ethanol 6%; GW1100 – ethanol 10% and AH7614 – ethanol 8.7%) and RvE1 at the same time and route and CG at zero time. Data are expressed as the mean±SEM of the volume difference (edema) in (A–C) and the difference in paw withdrawal threshold in response to the applied mechanical stimulus in (D–F) between the right and left paws at the depicted times. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: AH7614, selective antagonist of the free fatty acid receptor 4 (FFAR4/GPR120); C, control; CG, carrageenan; GW1100, selective antagonist of the free fatty acid receptor 1 (FFAR1/GPR40); i.pl., intraplantar; RvE1, resolvin E1; SEM, standard error of the mean; U-75302, selective antagonist of the leukotriene B4 receptor 1 (BLT1). |
Chromatographic determination of RvE1 and RvD1 and PDX present in the commercial samples
To confirm the presence and the chemical structure of the compounds used in this study, chromatography followed by mass spectrometry via UPLC-PDA-MS/MS analysis was carried out. The chromatograms obtained by the UPLC-PDA-MS/MS system revealed only one well-defined and resolved majority peak for each compound analyzed (Figure 10A, D and G). The ultraviolet absorption spectrum of RvE1, RvD1 and PDX showed the profile and maxima absorption characteristics of conjugated triene and diene chromophores (Figure 10B, E, H, respectively). Additionally, the mass spectra obtained in the scan mode showed predominantly the presence of the molecular anions [M – H]− m/z 349, 375, 359 for RvE1, RvD1 and PDX, respectively (Figure 10C, F and I). Finally, no peak was found for the major metabolites 18-oxo-RvE1, 20-OH-RvE1 and 18-oxo-RvD1 in either the multiple reaction monitoring mode or the scan mode with the mass spectrometry (data not shown).
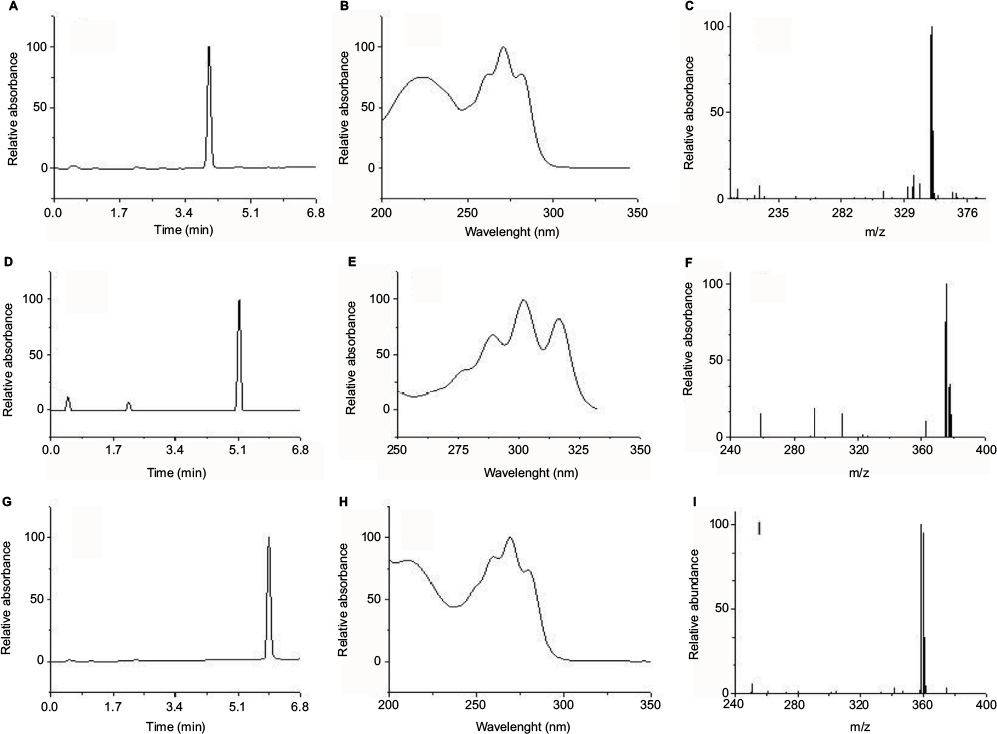 | Figure 10 Chromatograms obtained via UPLC-PDA-MS/MS analysis of RvE1, RvD1 and PDX. Notes: Spectra of RvE1, RvD1 and PDX at 270, 301 and 270 nm are shown in (A), (D) and (G), respectively. The ultraviolet spectra of RvE1, RvD1 and PDX showing the retention times of 4.02, 5.15 and 5.93 are shown in (B), (E) and (H), respectively. The scan mass spectra of RvE1, RvD1 and PDX with the retention times of 4.02, 5.15 and 5.93 are shown in (C), (F) and (I), respectively. Abbreviations: PDX, protectin DX; RvD1, resolvin D1; RvE1, resolvin E1, UPLC-PDA-MS/MS, ultra performance liquid chromatography-photo diode array-tandem mass spectrometry. |
Discussion
SPMs belong to a family of newly described endogenous chemical mediators that are responsible for actively terminating the inflammatory process.27 Among this ever-growing family of substances, lipoxins, Rvs, protectins and maresins are found.28,29 In this study, we demonstrated that the exogenous administration of two such compounds, RvE1 and RvD1, was simultaneously anti-inflammatory (antiedematogenic) and analgesic with varied efficacy when administered peripherally, that is, when administered locally in the rat hind paws. However, PDX, an isomer of PD1,30 was inactive under similar conditions, demonstrating a significant biologic variability among the three compounds. Despite the fact that an alleged anti-inflammatory potential can be attributed to PDX, the indicated experimental models differed from ours in that either the species or the in vitro conditions were used in the indicated studies.31,32 In fact, the effective doses of Rvs to reduce inflammation and pain under our conditions were in the range described in the literature,11,30 although RvD1 was half as potent as RvE1 in the reduction of nociception and paw edema. Moreover, Rvs given in combination (RvE1+RvD1) were not more effective in causing relief of the paw edema and nociception than the compounds given separately, or given at the time of the maximal effect. These results suggest that distinct mechanisms govern whether the treatment with Rvs begins very early or later, when the inflammatory reaction has fully developed. Therefore, molecular modifications that develop during the course of an inflammatory reaction may respond with different sensitivities to the action of Rvs.
The anti-inflammatory activity of RvE1 in mice was attributed to the inhibition of proinflammatory cytokine expression, infiltration of neutrophils and paw edema, whereas the antinociceptive effects of this molecule were related to the inhibition of tumor necrosis factor alpha, postsynaptic current increases and the hypersensitivity of N-methyl-d-aspartate receptors located at the dorsal horn neurons via inhibition of the extracellular signal-regulated kinase pathway.11 It is conceivable that similar mechanisms account for the results observed for both Rvs, but species differences cannot be overlooked,33 especially considering that rat paw edema in response to CG offers the best translational responses in humans.16
However, we could not predict the impact of Rvs on the local effects of other mediators usually released by CG.15 We observed that RvE1 and RvD1 presented differential profiles of activity, considering both experimental models of inflammation and pain when Hist, 5-HT, SP or PGE2 was used. Rvs either promoted or reduced paw edema formation, depending on the proinflammatory mediator used; RvE1 was more relevant in regard to the promotion of Hist- and 5-HT-induced edema, whereas RvD1 was relevant to SP-induced edema. Both Rvs, however, reduced the pro-nociceptive behavior of the main mediators involved in nociception, notably, 5-HT, SP and PGE2.26,34,35 In agreement with our findings, distinct molecular mechanisms of counter-regulatory pathways for RvD1 and RvE1 were also related to allergic airway inflammation, as noted by Levy.36 Taken together, it is conceivable that different molecular mechanisms underlie the anti-inflammatory and analgesic effects of RvE1 and RvD1 and that they present a vocation to relieve pain rather than paw edema, a point of view shared with other researchers.37
The therapeutic potential of SPMs may be incredibly wide and useful in multiple chronic inflammatory diseases.36,38 Presently, RvE1 (Rx-10001) and its synthetic analog (Rx-10045) are under clinical trials for the relief of chronic dry eye.39 Therefore, we decided to compare the therapeutic profiles of RvE1 and RvD1 in our settings with those of recognized anti-inflammatory and analgesic drugs, such as the selective and unselective inhibitors of COX, CX and INDO,21 and with DEXA, a standard steroidal anti-inflammatory drug.40 Strikingly, these drugs, with the exception of DEXA, were ineffective in reduction of inflammation and pain at a low dose level of CG, but they were effective at a higher dose level, clearly showing a dose-dependent response of local tissue to CG inflammation and to the anti-inflammatory and analgesic effects of these nonsteroidal anti-inflammatory drugs. However, the results also show that the presence of COX-2 was necessary for the effectiveness of these drugs, thus clearly suggesting that COX-2 was present only when the stimulus provided by CG was more intense. As mentioned before,19 practically all of the studies in the literature that showed inhibition of COX by selective and nonselective nonsteroidal anti-inflammatory drugs (NSAIDs) used higher levels of stimulation by CG in rat paws, as exemplified by the work of Chan et al41 and Smith et al.42 As both Rvs were effective at both CG doses, it is concluded that the anti-inflammatory and analgesic potential of Rvs is wider than that of NSAIDs. Additionally, in agreement with the work of Lee et al,43 Rvs may not involve the inhibition of COX only, and they are at least as effective as steroidal (DEXA) anti-inflammatory drugs. However, the potential for the promotion of edema formation by Rvs must be considered once SPMs become clinically available, since they can be associated with the eventual development of adverse effects, as shown here.
It was shown by Arita et al,23 using isolated human polymorphonuclear cells, that BLT1 receptors, but not BLT2 receptors, were responsive to RvE1 stimulation. BLT1 receptors are specific receptors for leukotriene B4, which are involved in polymorphonuclear infiltration in human and animal models of leukocyte recruitment and chemotaxis.23,44 In agreement with such studies, a specific antagonist of BLT1 receptors, the experimental compound U-75302, partially and completely reversed the anti-inflammatory and analgesic effects, respectively, of RvE1. However, specific antagonists of FFAR1 and FFAR4, the experimental compounds GW1100 and AH7614,45 respectively, were inactive in the same settings. As FFAR4 receptors function as ω3 polyunsaturated fatty acids, the precursors of both Rvs, and are associated with anti-inflammatory functions,46 it was tempting to verify whether treatment of the animals with such antagonists would modify the effects of Rvs. To our knowledge, this was the first time that the drugs such as GW1100 and AH7614 were studied in the in vivo models of simultaneous inflammation and pain responses. Additionally, our data are in accordance with those of Oh et al46 in that no modification of anti-inflammatory activity shown by Rvs was obtained with both antagonists. Altogether, it can be suggested that BLT1 receptors specifically mediate anti-inflammatory and analgesic actions of RvE1, and that FFAR1/GPR40 or FFAR4/GPR120 receptors do not seem to be the signaling pathways involved in these actions. However, similar studies of RvE1 should be undertaken to make a definitive statement in relation to RvD1.
The low chemical stability of pro-resolving lipid mediators is well known and, for this reason, the quality of our commercial resolvin samples should be confirmed. In an attempt to ensure the quality of our chemical standards and procedures, we verified whether the chemical features of the purchased samples of RvE1 and RvD1 would superimpose those described in the literature.47–49 As shown earlier, the UPLC-PDA-MS/MS results indicated that the transportation, storage and manipulation of Rvs and protectin present in our commercial preparations were properly followed, and therefore, all experimentally obtained results can be totally ascribed to the RvE1, RvD1 and PDX molecules. In addition, further search for the metabolites of these PUFAs other than those specified by the supplier was not detected, indicating that all the present results can be solely ascribed to the referenced lipids.
Limitations of the study
During the development of this study, we noticed that the efficacy of RvE1 and RvD1 to reduce pain and inflammation was in a rather narrow range of doses. In other words, it was as if a window of doses existed for the development of these effects. One contributing factor to this observation could be related to the nature of the vehicle used in our solutions, ethanol in saline, given the lipophilic nature of Rvs. We found in this study that the edematogenic and nociceptive responses were strongly affected by the vehicle, particularly when the ethanol concentration was >5% in the vehicle mixture, which may have contributed to the ceiling of the effectiveness of Rvs. Therefore, the solvent used for lipid dilution, ie, ethanol, was a limiting factor in this in vivo study of Rvs. In fact, we have previously shown that diluted ethanol was hyperalgesic under similar experimental conditions.50
Conclusion
In conclusion, we demonstrated that RvE1 and RvD1, but not PDX, were simultaneously anti-inflammatory and analgesic in experimental models that were closely related to translational studies in humans. Moreover, these SPMs presented a wider spectrum of activity compared to nonselective and selective NSAIDs, the main compounds used therapeutically in the treatment of acute and chronic inflammatory conditions. However, adverse effects, such as edema formation, demonstrated in this study can account for the potential side effects of these drugs in the clinic. The analgesic and anti-inflammatory activities of RvE1 were associated with the specific activation of the BLT1 receptor, a type of leukotriene B4 receptor. Given the ability of Rvs to reduce inflammatory pain, our data expand previous results in the literature for both molecules, thus boosting their therapeutic potential in pain and inflammation and widening the potential of alternative treatments for acute and chronic inflammatory diseases.
Acknowledgments
This work was supported by grants from the following Brazilian research agencies: CNPq, CAPES, FAPEMIG and PRPq – Universidade Federal de Minas Gerais (UFMG). The authors especially thank the Nanobiotechnology Network INCT-Nanobiofar, particularly Professor Ruben Dario Sinisterra Millán for the availability of UPLC-MS/MS equipment and Waters Corporation – Team Brazil for lending the PDA detector. The authors are also grateful to Dr Charles N Serhan for his comments on this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Serhan CN, Clish CB, Brannon J, Colgan SP, Chiang N, Gronert K. Novel functional sets of lipid-derived mediators with antiinflammatory actions generated from omega-3 fatty acids via cyclooxygenase 2-nonsteroidal antiinflammatory drugs and transcellular processing. J Exp Med. 2000;192(8):1197–1204. | ||
Serhan CN, Hong S, Gronert K, et al. Resolvins: a family of bioactive products of omega-3 fatty acid transformation circuits initiated by aspirin treatment that counter proinflammation signals. J Exp Med. 2002;196(8):1025–1037. | ||
Gilroy DW, Lawrence T, Perretti M, Rossi AG. Inflammatory resolution: new opportunities for drug discovery. Nat Rev. 2004;3(5):401–416. | ||
Bannenberg G, Serhan CN. Specialized pro-resolving lipid mediators in the inflammatory response: an update. Biochim Biophys Acta. 2010;1801(12):1260–1273. | ||
Serhan CN, Dalli J, Colas RA, Winkler JW, Chiang N. Protectins and maresins: New pro-resolving families of mediators in acute in fl ammation and resolution bioactive metabolome. Biochim Biophys Acta. 2015;1851(4):397–413. | ||
Dalli J, Chiang N, Serhan CN. Elucidation of novel 13-series resolvins that increase with atorvastatin and clear infections. Nat Med. 2015;21(9):1071–1075. | ||
Kohli P, Levy BD. Resolvins and protectins: mediating solutions to inflammation. Br J Pharmacol. 2009;158(4):960–971. | ||
Serhan CN, Petasis NA. Resolvins and protectins in inflammation-resolution. Chem Rev. 2011;111(10):5922–5943. | ||
Serhan CN, Chiang N. Endogenous pro-resolving and anti-inflammatory lipid mediators: a new pharmacologic genus. Br J Pharmacol. 2008;153(Suppl 1):S200–S215. | ||
Lee H, Surh YJ. Therapeutic potential of resolvins in the prevention and treatment of inflammatory disorders. Biochem Pharmacol. 2012;84(10):1340–1350. | ||
Xu ZZ, Zhang L, Liu T, et al. Resolvins RvE1 and RvD1 attenuate inflammatory pain via central and peripheral actions. Nat Med. 2010;16(5):592–597. | ||
Aoki H, Hisada T, Ishizuka T, et al. Protective effect of resolvin E1 on the development of asthmatic airway inflammation. Biochem Biophys Res Commun. 2010;400(1):128–133. | ||
Li D, Hodges RR, Jiao J, et al. Resolvin D1 and aspirin-triggered resolvin D1 regulate histamine-stimulated conjunctival goblet cell secretion. Mucosal Immunol. 2013;6(6):1119–1130. | ||
Di Rosa M. Biological properties of carrageenan. J Pharm Pharrnac. 1972;24(2):89–102. | ||
Vinegar R, Truax JF, Selph JL, Johnston PR, Venable AL, McKenzie KK. Pathway to carrageenan-induced inflammation in the hind limb of the rat. Fed Proc. 1987;46(1):118–126. | ||
Mukherjee A, Hale VG, Borga O, Stein R. Predictability of the clinical potency of NSAIDs from the preclinical pharmacodynamics in rats. Inflamm Res. 1996;45(11):531–540. | ||
Fonseca F, Francischi J. Resolution factors: will they be good controllers of the inflammatory response? In: Inflammation Research. Vol 64; 2015:S211–S212. | ||
Fonseca F, Orlando R, Augusti R, Turchetti-Maia R, Francischi J. Peripheral Efficacy of Resolution Factors in the Carrageenan-Induced Paw Edema and Hyperalgesia Models in Rats: a Comparison Between Resolvin E1 and D1. In: 48th Brazilian Congress of Pharmacology and Experimental Therapeutics and the 21st Latin American Congress of Pharmacology; 2016. | ||
Francischi JN, Chaves CT, Moura AC, et al. Selective inhibitors of cyclo-oxygenase-2 (COX-2) induce hypoalgesia in a rat paw model of inflammation. Br J Pharmacol. 2002;137(6):837–844. | ||
Frade TI, Dos Reis DC, Cassali GD, Bakhle YS, de Francischi JN. Tissue-selective inflammation in the oral cavity of the rat. Inflammopharmacology. 2016;24:145–153. | ||
Vane JR, Bakhle YS, Botting RM. Cyclooxygenases 1 and 2. Annu Rev Pharmacol Toxicol. 1998;38:97–120. | ||
Goodman & Gilman, Brunton L, Chabner B, Knollmann B. The Pharmacological Basis of Therapeutics. 12th ed. New York, NY: McGraw-Hill; 2012. | ||
Arita M, Ohira T, Sun Y, Elangovan S, Chiang N, Serhan CN. Resolvin E1 selectively interacts with leukotriene B4 receptor BLT1 and ChemR23 to regulate inflammation. J Immunol. 2007;178(6):3912–3917. | ||
Gomides LF, Duarte ID, Ferreira RG, Perez AC, Francischi JN, Klein A. Proteinase-activated receptor-4 plays a major role in the recruitment of neutrophils induced by trypsin or carrageenan during pleurisy in mice. Pharmacology. 2012;89(5–6):275–282. | ||
Briscoe CP, Peat AJ, Mckeown SC, et al. Pharmacological regulation of insulin secretion in MIN6 cells through the fatty acid receptor GPR40: identification of agonist and antagonist small molecules. Br J Pharmacol. 2006;148(5):619–628. | ||
Santos CMF, Francischi JN, Paiva-Lima P, Sluka KA, Resende MA. Effect of transcutaneous electrical stimulation on nociception and edema induced by peripheral serotonin. Int J Neurosci. 2013;123(7):507–515. | ||
Ariel A, Serhan CN. Resolvins and protectins in the termination program of acute inflammation. Trends Immunol. 2007;28(4):176–183. | ||
Shinohara M, Serhan CN. Novel endogenous proresolving molecules: essential fatty acid-derived and gaseous mediators in the resolution of inflammation. J Atheroscler Thromb. 2016;23(6):655–664. | ||
Serhan CN, Brain SD, Buckley CD, et al. Resolution of inflammation: state of the art, definitions and terms. FASEB J. 2007;21(2):325–332. | ||
Christie WW. Resolvins and protectins: chemistry and Biology. AOCS Lipid Libr. 2014:1–6. | ||
Liu M, Boussetta T, Makni-Maalej K, et al. Protectin DX, a double lipoxygenase product of DHA, inhibits both ROS production in human neutrophils and cyclooxygenase activities. Lipids. 2014;49(1):49–57. | ||
Xia H, Chen L, Liu H, et al. Protectin DX increases survival in a mouse model of sepsis by ameliorating inflammation and modulating macrophage phenotype. Sci Rep. 2017;7(1):99. | ||
Le Bars D, Gozariu M, Cadden SW. Animal models of nociception. Pharmacol Rev. 2001;53(4):597–652. | ||
Teodoro FC, Tronco MF, Zampronio AR, Martini AC, Rae GA, Chichorro JG. Peripheral substance P and neurokinin-1 receptors have a role in inflammatory and neuropathic orofacial pain models. Neuropeptides. 2013;47(3):199–206. | ||
Ferreira SH. Prostaglandins, aspirin-like drugs and analgesia. Nat New Biol. 1972;240(102):200–203. | ||
Levy BD. Resolvin D1 and resolvin E1 promote the resolution of allergic airway inflammation via shared and distinct molecular counter-regulatory pathways. Front Immunol. 2012;3:390. | ||
Ji RR, Xu ZZ, Strichartz G, Serhan CN. Emerging roles of resolvins in the resolution of inflammation and pain. Trends Neurosci. 2011;34(11):599–609. | ||
Michalak A, Mosinska P, Fichna J. Polyunsaturated fatty acids and their derivatives: therapeutic value for inflammatory, functional gastrointestinal disorders, and colorectal cancer. Front Pharmacol. 2016;7:459. | ||
Hessen M, Akpek EK. Dry eye: an inflammatory ocular disease. J Ophthalmic Vis Res. 2014;9(2):240–250. | ||
Blackwell GJ, Carnuccio R, Di Rosa M, et al. Glucocorticoids induce the formation and release of anti-inflammatory and anti-phospholipase proteins into the peritoneal cavity of the rat. Br J Pharmacol. 1982;76(1):185–194. | ||
Chan CC, Boyce S, Brideau C, et al. Rofecoxib [Vioxx, MK-0966; 4-(4’-methylsulfonylphenyl)-3-phenyl-2-(5H)-furanone]: a potent and orally active cyclooxygenase-2 inhibitor. Pharmacological and biochemical profiles. J Pharmacol Exp Ther. 1999;290(2):551–560. | ||
Smith CJ, Zhang Y, Koboldt CM, et al. Pharmacological analysis of cyclooxygenase-1 in inflammation. Proc Natl Acad Sci U S A. 1998;95:13313–13318. | ||
Lee JY, Sohn KH, Rhee SH, Hwang D. Saturated fatty acids, but not unsaturated fatty acids, induce the expression of cyclooxygenase-2 mediated through toll-like receptor 4. J Biol Chem. 2001;276(20):16683–16689. | ||
Tager AM, Dufour JH, Goodarzi K, Bercury SD, von Andrian UH, Luster AD. BLTR mediates leukotriene B(4)–induced chemotaxis and adhesion and plays a dominant role in eosinophil accumulation in a murine model of peritonitis. J Exp Med. 2000;192(3):439–446. | ||
Houthuijzen JM. For better or worse: FFAR1 and FFAR4 signaling in cancer and diabetes. Mol Pharmacol. 2016;90:738–743. | ||
Oh DY, Talukdar S, Bae EJ, et al. GPR120 is an omega-3 fatty acid receptor mediating potent anti-inflammatory and insulin sensitizing effects. Cell. 2010;142(5):687–698. | ||
Arita M, Oh SF, Chonan T, et al. Metabolic inactivation of resolvin E1 and stabilization of its anti-inflammatory actions. J Biol Chem. 2006;281(32):22847–22854. | ||
Sun YP, Oh SF, Uddin J, et al. Resolvin D1 and its aspirin-triggered 17R epimer: stereochemical assignments, anti-inflammatory properties, and enzymatic inactivation. J Biol Chem. 2007;282(13):9323–9334. | ||
Balas L, Guichardant M, Durand T, Lagarde M. Confusion between protectin D1 (PD1) and its isomer protectin DX (PDX). An overview on the dihydroxy-docosatrienes described to date. Biochimie. 2014; 99:1–7. | ||
Tatsuo MA, Yokoro CM, Salgado JV, Pesquero SM, Santana MA, Francischi JN. Hyperalgesic effect induced by barbiturates, midazolam and ethanol: pharmacological evidence for GABA-A receptor involvement. Brazilian J Med Biol Res. 1997;30(2):251–256. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.