Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Comparative Effectiveness of Fractional CO2 Laser and Topical Silicone Gel for Postcesarean Scars
Authors Wang Y, Chen M, Wei Z, Song Y
Received 15 January 2026
Accepted for publication 5 April 2026
Published 18 May 2026 Volume 2026:19 596343
DOI https://doi.org/10.2147/CCID.S596343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Yi Wang,1,2 Minjian Chen,1,2 Zhenni Wei,1,2 Yong Song1,2
1Department of Plastic Surgery, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350000, People’s Republic of China; 2Department of Plastic Surgery, Fujian Maternity and Child Health Hospital, Fuzhou, 350000, People’s Republic of China
Correspondence: Yong Song, Department of Plastic Surgery, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, No. 18 Daoshan Road, Gulou District, Fuzhou, 350000, People’s Republic of China, Email [email protected]
Background: Postcesarean scars are common and may cause persistent symptoms and dissatisfaction. Topical silicone gel is widely used as first-line therapy, but its effects are mainly limited to surface hydration and barrier support. Fractional CO2 laser, by contrast, induces controlled dermal microinjury and collagen remodeling. Comparative evidence for postcesarean scars remains limited. This study compared the effectiveness of fractional CO2 laser versus topical silicone gel for improving scar quality, symptoms, and patient satisfaction.
Methods: In this retrospective cohort study, 220 women with postcesarean scars were included (112 treated with fractional CO2 laser and 108 with topical silicone gel). Both groups received standard postoperative scar care according to routine clinical practice. The primary outcome was scar quality at 6 months assessed by the Vancouver Scar Scale (VSS). Secondary outcomes included pain, pruritus, tightness, satisfaction, and safety. Between-group differences were analyzed using unadjusted comparisons and analysis of covariance adjusting for baseline VSS and time from surgery to treatment. Sensitivity analyses included additional covariate adjustment and propensity score–adjusted models.
Results: At 6 months, the laser group was associated with better scar quality compared with the silicone group (VSS total 4.185 ± 1.064 vs 4.619 ± 1.085; unadjusted difference − 0.435, P = 0.003). After adjustment, fractional CO2 laser remained associated with a lower VSS total score (adjusted mean difference − 0.643; 95% CI − 0.891 to − 0.395; P < 0.001). Significant improvements were also observed in vascularity, pigmentation, and height/thickness. Laser treatment further reduced pain, pruritus, and tightness, and produced higher patient satisfaction (all P < 0.001). Adverse events were infrequent and comparable between groups.
Conclusion: Fractional CO2 laser was associated with greater improvements in postcesarean scar quality and related symptoms at 6 months compared with topical silicone gel, with a comparable safety profile.
Keywords: fractional CO2 laser, postcesarean scars, Vancouver Scar Scale, silicone gel, patient satisfaction
Introduction
Cesarean delivery is one of the most commonly performed surgical procedures worldwide, accounting for 21.1% of all live births between 2010 and 2018, a substantial increase from approximately 7% in 1990.1 In China, nearly one third of births are now conducted by cesarean section.2,3 As cesarean rates continue to rise, the number of women living with post-cesarean scars is increasing accordingly. Although advances in obstetric care have improved maternal and neonatal safety, postoperative scarring remains almost universal and is often underaddressed. Beyond cosmetic concerns, cesarean scars may cause symptoms such as pruritus, pain, and tightness, and can negatively affect body image, psychological well-being, and overall satisfaction with childbirth.4 Therefore, optimizing scar quality and symptom burden has become an important yet insufficiently addressed clinical issue.
Scar formation is a complex biological process involving inflammation, fibroblast activity, extracellular matrix deposition, and tissue remodeling.5–7 Disruption of this process can lead to pathological scarring, including hypertrophic scars and keloids, characterized by excessive collagen deposition and persistent inflammation.6 Compared with scars at other anatomical sites, cesarean scars are subject to unique biomechanical and hormonal influences, including sustained tension in the lower abdomen and pregnancy-related endocrine changes, which may predispose to unfavorable outcomes even after optimal wound closure.7 Various interventions have been proposed for postoperative scar management, yet high-quality evidence specific to cesarean scars remains limited.8 Among conservative approaches, topical silicone gel is widely recommended as a first-line therapy.8–11 It primarily acts by improving hydration and barrier function and modulating fibroblast activity.9 Although generally safe and easy to use, its clinical benefits are often modest, particularly in established scars, and adherence may be suboptimal in practice.10,11 Consequently, there is growing interest in alternative strategies that more directly target dermal remodeling.
Laser-based interventions have gained increasing attention for their ability to actively remodel scar tissue rather than merely modifying surface characteristics. Among these, fractional carbon dioxide laser is one of the most extensively studied modalities. By creating controlled microthermal injury within the dermis, it promotes collagen remodeling and reorganization of the extracellular matrix.12 Clinically, this approach has been shown to improve scar texture, thickness, pigmentation, and pliability across various scar types.13,14 However, existing evidence is largely derived from heterogeneous populations, including acne, burn, and mixed surgical scars, with substantial variability in treatment protocols and outcome measures.15–17 As a result, the applicability of these findings to postcesarean scars remains uncertain, given the distinct biomechanical and hormonal characteristics of the postpartum setting. Furthermore, direct comparisons between fractional CO2 laser and standard first-line therapies such as silicone gel are limited, particularly in obstetric populations. These gaps underscore the need for targeted comparative studies in this specific clinical context.
The present retrospective cohort study addresses this gap by comparing fractional CO2 laser therapy with topical silicone gel for the management of post-cesarean scars in a real-world clinical setting. We aimed to provide head-to-head evidence on scar quality, symptom burden, and patient satisfaction using standardized assessment tools. We hypothesized that fractional CO2 laser would be associated with greater improvement in scar characteristics and patient-reported outcomes compared with silicone gel. To our knowledge, this is among the first studies to directly compare these two commonly used modalities in a homogeneous post-cesarean population. By generating comparative data within a single analytical framework, this study seeks to inform clinical decision-making while providing a basis for future randomized controlled trials.
Methods
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Fujian Maternity and Child Health Hospital (IRB approval No. 2022YJ112). As the study involved analysis of de-identified clinical data collected during routine care, the requirement for written informed consent was waived by the ethics committee. All patient information was anonymized prior to analysis, and data access was restricted to authorized investigators only.
Study Design and Setting
This study was a single-center, observational comparative analysis conducted over a three-year period from January 2021 to December 2023 at the Fujian Maternity and Child Health Hospital. Women who had undergone cesarean section and subsequently received either fractional carbon dioxide (CO2) laser therapy or topical silicone gel for postoperative scar management were eligible for inclusion. The study was designed to compare real-world clinical outcomes of the two interventions under routine practice conditions. Treatment allocation was determined by shared decision-making between physicians and patients based on clinical characteristics, patient preference, and treatment availability. Given the non-randomized nature of treatment allocation, potential confounding was addressed using multivariable adjustment and propensity score–based methods as prespecified analytical strategies. Both groups received standard postoperative scar care in accordance with routine institutional practice, including basic topical management when appropriate.
Participants and Eligibility Criteria
Eligible participants were women aged 21 to 37 years who had undergone a lower-segment cesarean section and presented with a visible postoperative scar that had reached the early remodeling phase at the time of intervention. Scars were required to be fully epithelialized and free of wound dehiscence or active infection. Patients were included if they had received either fractional CO2 laser therapy or topical silicone gel as a primary scar management strategy and had completed at least one follow-up evaluation at 3 months or later after initiation of treatment. Exclusion criteria were a history of keloid diathesis or hypertrophic scarring unrelated to the cesarean incision, concurrent use of other scar-modifying interventions such as intralesional corticosteroids or pressure therapy, presence of systemic connective tissue disease, pregnancy at the time of treatment, and incomplete clinical records or unavailable outcome assessments.
Sample Size Estimation
The sample size was determined a priori based on the primary outcome of improvement in standardized scar assessment scores. Assuming a two-group comparison of mean outcome change between the fractional CO2 laser group and the silicone gel group, the required sample size per group was calculated using the following formula for comparison of two independent means:
where n represents the required sample size per group, σ is the estimated standard deviation of the primary outcome measure, δ is the minimum clinically meaningful difference between groups, Zα/2 corresponds to the standard normal deviate for a two-sided significance level α, and Zβ corresponds to the desired statistical power (1−β). Based on prior studies evaluating laser-based scar interventions, the standard deviation of change in scar scores was estimated at approximately 2.5 units, and a between-group difference of 1.0 point in the 6-month VSS total score was considered clinically meaningful based on its interpretability in reflecting noticeable changes in scar characteristics. With a two-sided α of 0.05 (Zα/2 = 1.96) and a power of 80% (Zβ = 0.84), the calculated minimum sample size was 98 participants per group. Allowing for potential loss to follow-up and incomplete data, the target enrollment was increased by approximately 10%, yielding an overall sample size of approximately 220 patients.
Interventions
Patients in the fractional CO2 laser group were treated using a fractional carbon dioxide laser system (eCO2, UltraPulse Encore, Lumenis Ltd., Yokneam, Israel; wavelength 10,600 nm). All procedures were performed by two attending physicians trained in laser dermatologic procedures using a standardized institutional protocol. Before each session, the scar was gently cleansed with sterile normal saline and dried. A topical anesthetic cream containing lidocaine 2.5% and prilocaine 2.5% was applied in a uniform layer over the scar and covered with an occlusive dressing for 40 minutes, after which the cream was completely removed and the area was re-cleansed with sterile saline. Laser treatment was delivered in fractional mode using a combination of Deep FX and SCAAR FX modes, with the following fixed settings: Deep FX (energy 50 mJ, frequency 300 Hz, density 5%) and SCAAR FX (energy 100 mJ, frequency 250 Hz, density 3%), and single-pass coverage along the entire length of the scar. Pulses were placed with minimal overlap to ensure uniform coverage while avoiding excessive thermal stacking. Immediately after treatment, the area was cooled using sterile saline-soaked gauze for 10 minutes, followed by application of a topical anti-inflammatory ointment. Topical silicone gel was used as part of routine postoperative scar care during the treatment period. Patients were instructed to cleanse the treated area twice daily with mild soap and water beginning the next day, apply the emollient twice daily for 5 days, and avoid intentional sun exposure; broad-spectrum sunscreen was recommended when the scar could be exposed. Each patient received three sessions at 5-week intervals. Analgesics were not routinely prescribed; oral acetaminophen was permitted as needed.
Patients in the silicone gel group were treated with a single medical-grade topical silicone gel (Dermatix Ultra, Menarini Group, Florence, Italy). Patients were instructed to apply the gel in a thin, uniform layer covering the entire scar after gentle cleansing and complete drying of the skin. The gel was applied twice daily at fixed times (morning and evening) for 12 consecutive weeks. Patients were instructed to allow the gel to dry for 5 minutes before dressing and to avoid applying additional topical agents over the scar during the treatment period unless medically indicated. Routine scar care, including gentle hygiene and photoprotection, was recommended. Throughout the intervention period, the use of other scar-modifying therapies, including intralesional corticosteroids, pressure therapy, topical retinoids, silicone sheets, microneedling, or other laser and energy-based procedures, was not permitted in either group.
Outcome Measures
The primary outcome was scar quality at 6 months after treatment initiation, assessed using the Vancouver Scar Scale (VSS). The VSS comprises four domains: vascularity (score 0–3), pigmentation (score 0–2), pliability (score 0–5), and height or thickness (score 0–3), with a total score ranging from 0 to 13, where lower scores indicate better scar quality. The 6-month VSS assessment was defined as the clinical evaluation performed at the follow-up visit closest to 6 months after initiation of fractional CO2 laser therapy in the laser group or initiation of silicone gel application in the gel group, with an allowable window of ±2 weeks. The 6-month time point was selected to capture clinically relevant early remodeling outcomes in scar healing.
Secondary outcomes were evaluated at the same 6-month follow-up. Scar-related pain, pruritus, and tightness were quantified using a 10-cm visual analog scale (VAS), where 0 indicated absence of symptoms and 10 indicated the most severe symptoms imaginable. Patient satisfaction with scar appearance was assessed using a 5-point Likert scale (1, very dissatisfied; 2, dissatisfied; 3, neutral; 4, satisfied; 5, very satisfied). Safety outcomes were defined as treatment-emergent adverse events documented in the medical records during the intervention period and follow-up, including persistent erythema lasting longer than 14 days, blistering, infection requiring systemic or topical antibiotic therapy, delayed epithelialization, and post-inflammatory hyperpigmentation.
To ensure reliability and minimize observer bias, outcome assessment was conducted in an assessor-blinded manner. VSS scoring was independently performed by two clinicians who were not involved in treatment delivery and who were blinded to treatment allocation. Prior to evaluation, all identifiers related to intervention type were removed from the medical records and photographic materials, and images were anonymized and coded by an independent study coordinator. When standardized clinical photographs were available, they were reviewed in a randomized order to prevent recognition of treatment patterns. In cases of disagreement between assessors, the final VSS score was determined by consensus following joint review, with both assessors remaining blinded to group assignment.
Data Collection
Clinical data were extracted from the institutional electronic medical record system using a prespecified data abstraction form. The following variables were collected for each eligible patient: age at treatment initiation, body mass index, parity, indication for cesarean section, date of surgery, interval (in weeks) between cesarean delivery and initiation of scar treatment, baseline scar characteristics, treatment modality, and completion of the planned intervention. Outcome data at the 6-month follow-up included VSS scores, VAS scores for pain, pruritus, and tightness, patient satisfaction ratings, and documentation of adverse events. Data extraction was independently performed by two investigators who were blinded to the study hypothesis. A random 10% sample of records was re-reviewed by a third investigator to assess data accuracy. Any discrepancies were resolved by consensus after review of the source records. For patients with multiple follow-up visits within the predefined 6-month window, the assessment closest to 6 months after treatment initiation was selected for analysis. All data were de-identified prior to analysis, and the final dataset was stored on a secure, password-protected server accessible only to study investigators.
Statistical Analysis
The statistical analysis plan was defined prior to data extraction and analysis, including specification of the primary outcome, covariates, and modeling strategy, to minimize the risk of data-driven analyses. Continuous variables are presented as mean ± standard deviation or median with interquartile range, as appropriate, and categorical variables as counts and percentages. Distributional normality was assessed using the Shapiro–Wilk test. Baseline characteristics between the fractional CO2 laser group and the silicone gel group were compared using the independent samples t test for normally distributed continuous variables, the Mann–Whitney U-test for non-normally distributed variables, and the chi-square test or Fisher’s exact test for categorical variables. The primary analysis was prespecified to test the same parameter used for sample size determination, namely the between-group difference in mean 6-month VSS total score (δ). Accordingly, group comparisons were performed using a linear model with the 6-month VSS score as the dependent variable and treatment group as the independent variable. To increase precision and control for potential confounding, an analysis of covariance (ANCOVA) model was applied with adjustment for baseline VSS score and the interval between cesarean delivery and initiation of scar treatment. The treatment effect was expressed as the adjusted mean difference in 6-month VSS score between groups (δ̂) with the corresponding 95% confidence interval. Statistical significance was assessed using a two-sided α level of 0.05, matching the α specified in the sample size calculation. Although the sample size was calculated based on the expected between-group difference in change scores, the primary analysis was conducted using an ANCOVA model with adjustment for baseline VSS, which is statistically equivalent and provides greater precision for estimating the same treatment effect parameter. To minimize temporal variability in scar maturation, the follow-up window was restricted to ±2 weeks around the 6-month time point. Secondary outcomes, including VAS scores for pain, pruritus, and tightness and patient satisfaction at 6 months, were analyzed using analogous linear regression or ANCOVA models, with adjustment for baseline values when available, to provide effect estimates on the same scale as the primary outcome. Safety outcomes were summarized descriptively, and between-group comparisons of adverse event proportions were conducted using Fisher’s exact test. To further address potential selection bias due to non-random treatment allocation, a propensity score was calculated using a logistic regression model including age, body mass index, baseline VSS score, time from cesarean section to treatment initiation, and scar characteristics. The propensity score was incorporated into the outcome model as an adjustment covariate. All statistical tests were two-sided, and a P value of less than 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA).
Results
Study Cohort and Baseline Characteristics
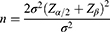
A total of 220 participants were included, comprising 112 in the fractional CO2 laser group and 108 in the silicone gel group (Figure 1). Baseline demographic and obstetric characteristics were largely comparable between groups, including age (30.950 ± 3.364 vs 31.070 ± 3.905 years, P = 0.849) and body mass index (24.339 ± 2.064 vs 23.759 ± 1.704 kg/m2, P = 0.137). The interval from surgery to treatment initiation did not differ (10.861 ± 2.116 vs 11.111 ± 1.938 weeks, P = 0.360), and follow-up timing around the prespecified 6-month target was similar (time in 6-month window, 1.366 ± 8.468 vs −0.139 ± 9.198 days, P = 0.209). Baseline scar severity showed a modest imbalance: the laser group had a higher VSS total score at baseline than the silicone group (8.469 ± 0.986 vs 8.133 ± 0.947, P = 0.010). Other baseline scar features, symptom scores, comorbidities, and treatment-related variables were comparable (Table 1).
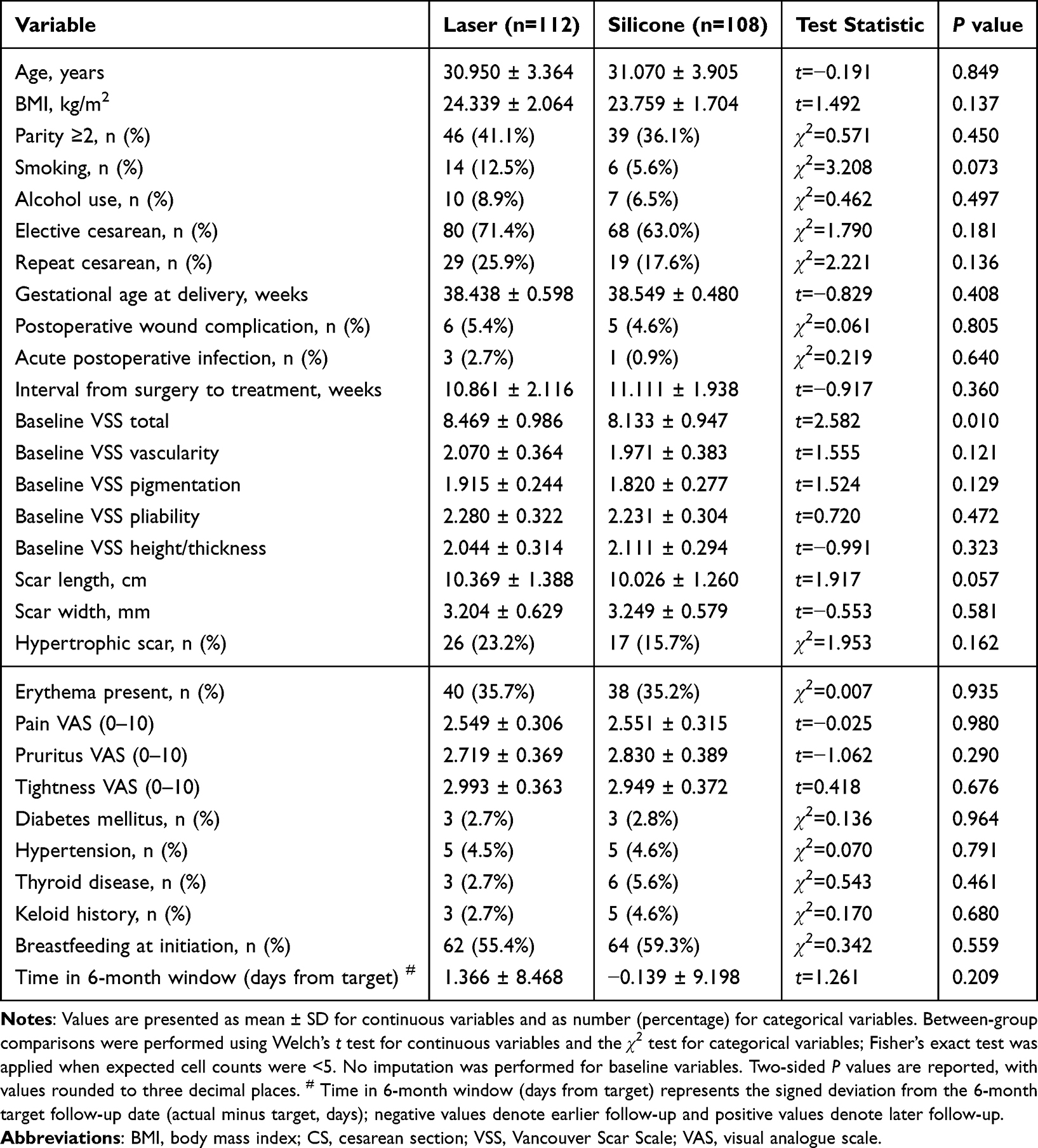 |
Table 1 Baseline Characteristics of Participants by Treatment Group |
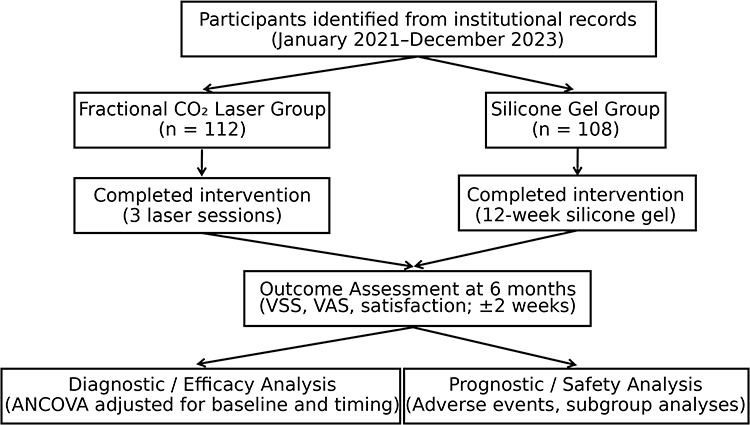 |
Figure 1 Study design and analytical workflow. Patients undergoing cesarean section between January 2021 and December 2023 who subsequently received postoperative scar treatment were identified and included in the study. Participants were assigned to the fractional CO2 laser group (n = 112) or the silicone gel group (n = 108) according to routine clinical practice. Treatments were delivered as specified, and outcomes were assessed at 6 months after initiation (±2 weeks). Scar quality, symptoms, satisfaction, and adverse events were analyzed within a unified comparative framework. |
Primary Outcome: Scar Quality at 6 Months (VSS)
At 6 months, overall scar quality as assessed by the VSS total score favored fractional CO2 laser (4.185 ± 1.064) over silicone gel (4.619 ± 1.085). The unadjusted between-group difference was −0.435 (P = 0.003). After prespecified adjustment for baseline VSS and the interval from surgery to treatment, fractional CO2 laser remained associated with a lower VSS total score (adjusted mean difference, −0.643; 95% CI, −0.891 to −0.395; P < 0.001) (Table 2). The magnitude and precision of adjusted effects across the VSS total and its domains are summarized in Figure 2. Domain-specific analyses demonstrated consistent effects across vascularity (adjusted difference, −0.303; 95% CI, −0.416 to −0.191; P < 0.001), pigmentation (−0.121; 95% CI, −0.225 to −0.017; P = 0.023), and height/thickness (−0.228; 95% CI, −0.336 to −0.119; P < 0.001). The difference in pliability did not reach statistical significance (−0.105; 95% CI, −0.223 to 0.013; P = 0.082) (Table 2 and Figure 2). Representative clinical photographs demonstrating longitudinal changes in scar appearance are shown in Figure 3.
 |
Table 2 Primary Outcome at 6 Months: Vancouver Scar Scale (VSS) and Component Scores |
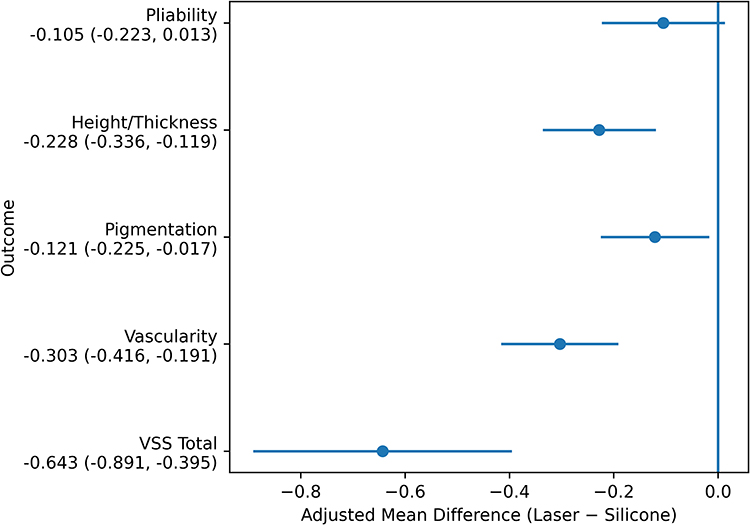 |
Figure 2 Adjusted treatment effects on scar quality at 6 months. Forest plot showing adjusted mean differences (Laser − Silicone) in the Vancouver Scar Scale (VSS) total score and each VSS domain (vascularity, pigmentation, pliability, and height/thickness) at 6 months. Estimates were obtained from analysis of covariance (ANCOVA) with treatment group as the main factor and baseline VSS and the interval from surgery to treatment as covariates. Points indicate adjusted mean differences and horizontal lines denote 95% confidence intervals (CIs). The vertical line at 0 represents no between-group difference. Negative values indicate lower (better) scores in the laser group. |
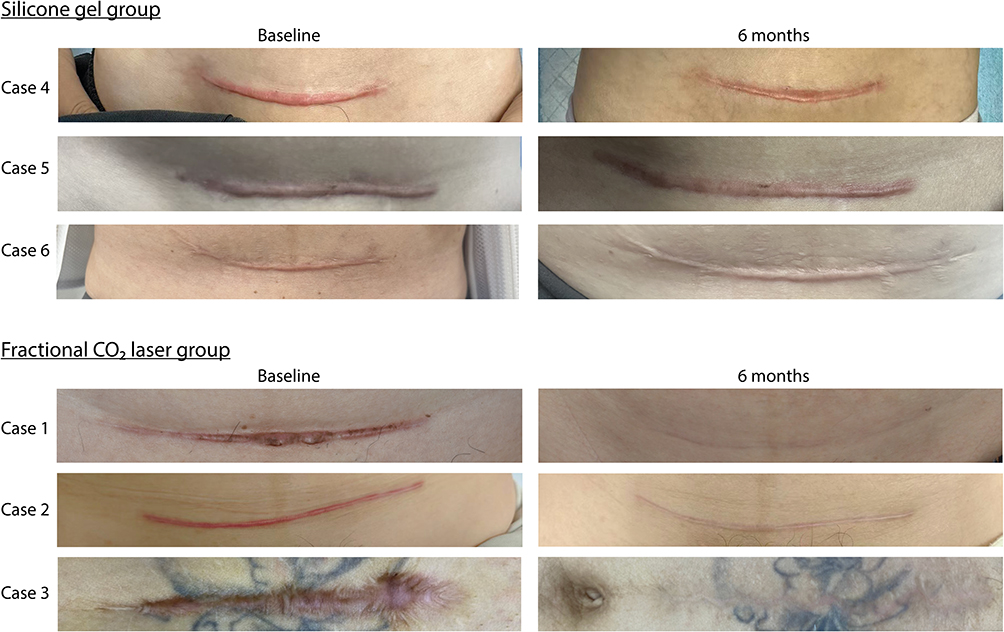 |
Figure 3 Representative clinical photographs of postcesarean scars at baseline and at the 6-month follow-up in each treatment group. |
Secondary Outcomes: Scar-Related Symptoms and Patient Satisfaction
At 6 months, symptom severity assessed by VAS consistently favored the laser group in adjusted analyses. Pain was lower with laser than with silicone gel (1.290 ± 0.575 vs 1.592 ± 0.581; adjusted difference, −0.303; 95% CI, −0.433 to −0.172; P < 0.001). Similar patterns were observed for pruritus (1.327 ± 0.636 vs 1.758 ± 0.612; adjusted difference, −0.386; 95% CI, −0.528 to −0.244; P < 0.001) and tightness (1.488 ± 0.631 vs 1.951 ± 0.663; adjusted difference, −0.475; 95% CI, −0.630 to −0.320; P < 0.001) (Table 3). Patient-reported satisfaction differed markedly between groups (overall χ2 = 55.522, P < 0.001). A greater proportion of participants reported being satisfied or very satisfied (Likert 4–5) in the laser group (30/112, 26.8%) than in the silicone group (3/108, 2.8%). Conversely, dissatisfied or very dissatisfied ratings (Likert 1–2) were less frequent with laser (13/112, 11.6%) than with silicone (58/108, 53.7%) (Table 4).
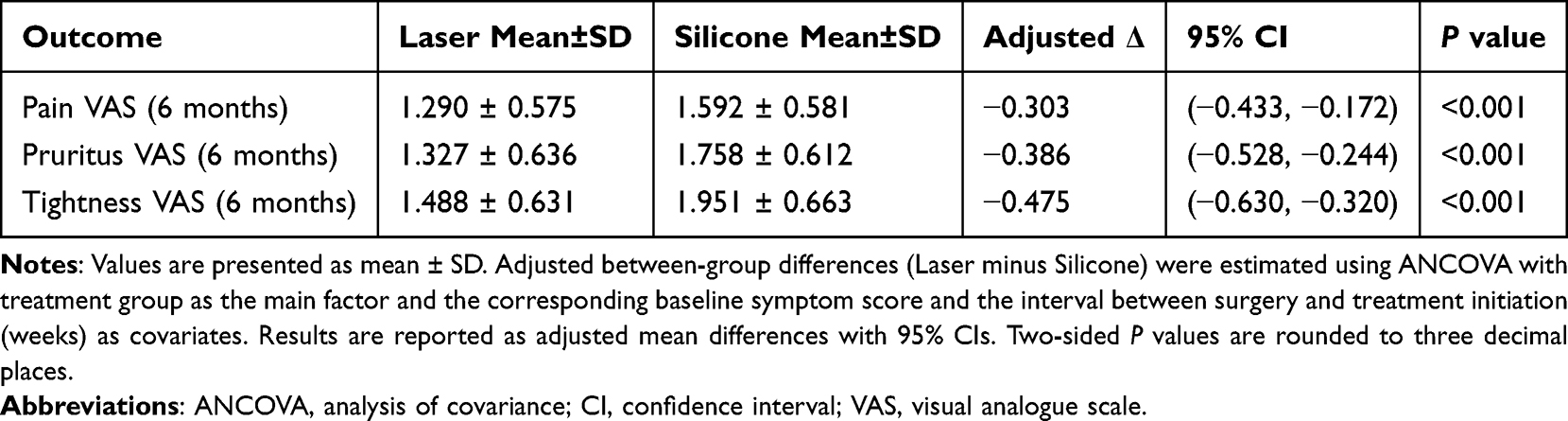 |
Table 3 Secondary Outcomes at 6 Months: Symptom Severity Assessed by VAS |
 |
Table 4 Patient-Reported Satisfaction at 6 Months |
Safety Outcomes
Adverse events were infrequent and did not differ significantly between groups. Any adverse event occurred in 15/112 (13.4%) of participants in the laser group and 11/108 (10.2%) in the silicone group (P = 0.461). Persistent erythema lasting >14 days was observed in 6/112 (5.4%) versus 6/108 (5.6%) (P = 0.861), and blistering occurred in 3/112 (2.7%) versus 1/108 (0.9%) (P = 0.640). No infections requiring antibiotics were reported in the laser group, compared with 1/108 (0.9%) in the silicone group (P = 0.985). Delayed epithelialization was rare (1/112 [0.9%] vs 2/108 [1.9%], P = 0.975), as was post-inflammatory hyperpigmentation (5/112 [4.5%] vs 3/108 [2.8%], P = 0.758). Overall, no safety signal favoring either treatment was identified (Table 5). All adverse events were mild and self-limited, and no treatment discontinuations due to adverse events were recorded.
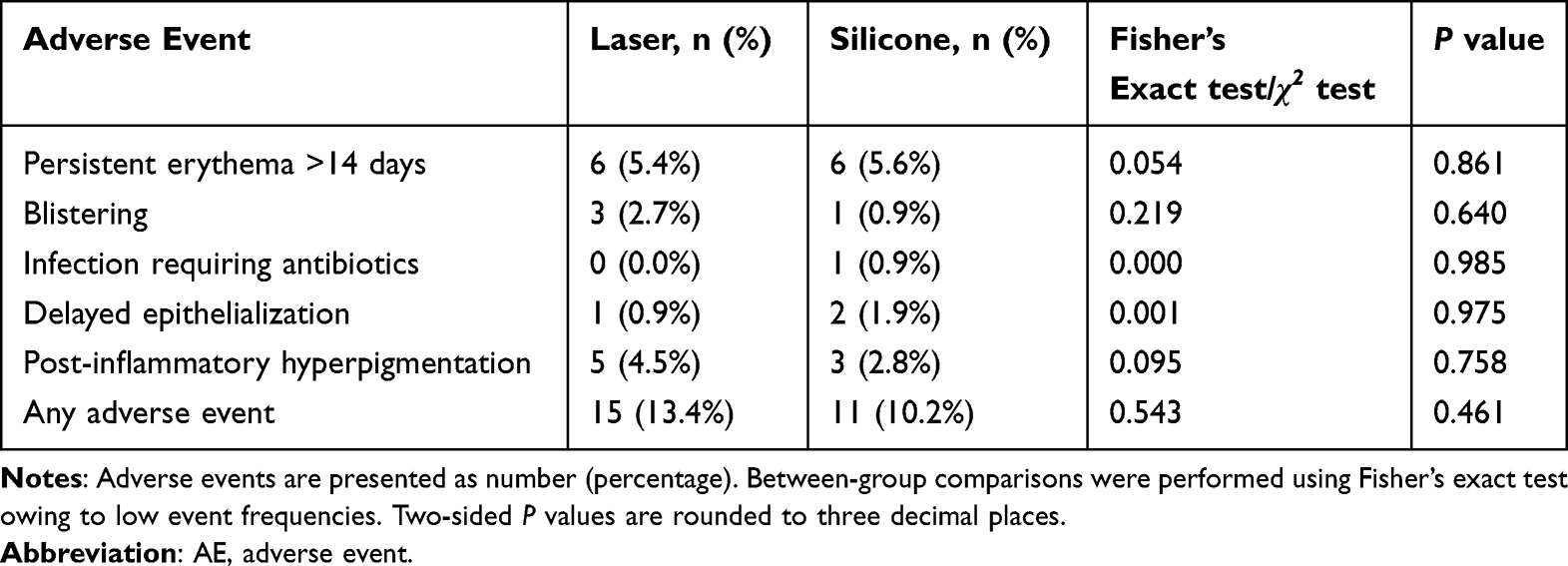 |
Table 5 Safety Outcomes and Adverse Events |
Sensitivity Analyses for the Primary Outcome
The treatment effect on VSS total at 6 months was robust across prespecified sensitivity analyses. The main ANCOVA model yielded an adjusted difference of −0.643 (95% CI, −0.891 to −0.395; P < 0.001). Additional adjustment for age and body mass index produced a similar estimate (−0.662; 95% CI, −0.911 to −0.413; P < 0.001). A propensity score–adjusted model also supported the primary finding (−0.670; 95% CI, −0.922 to −0.418; P < 0.001) (Table 6). The consistency of the estimated treatment effect across models is shown in Figure 4.
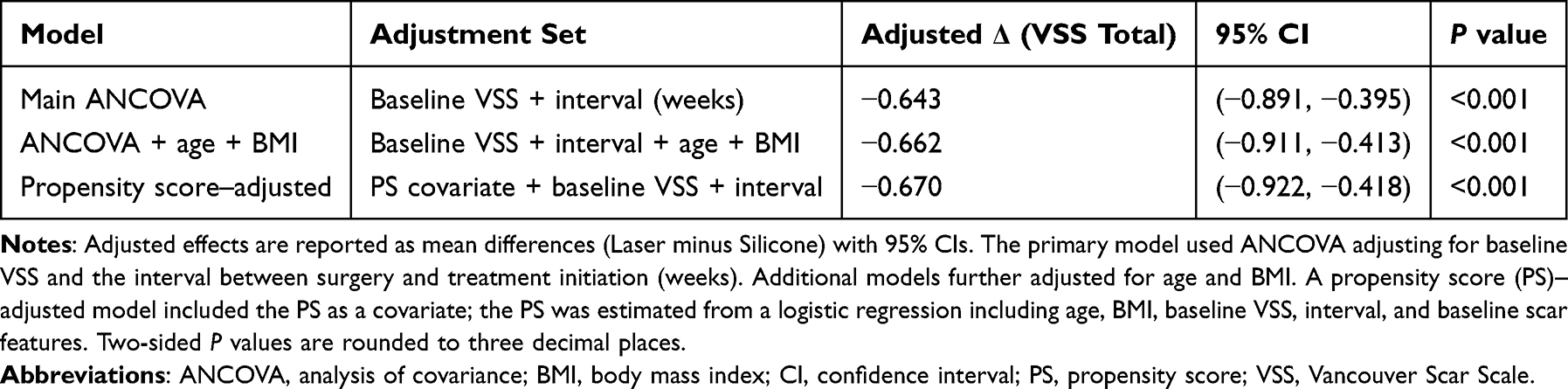 |
Table 6 Sensitivity Analyses for the Primary Outcome (VSS Total at 6 Months) |
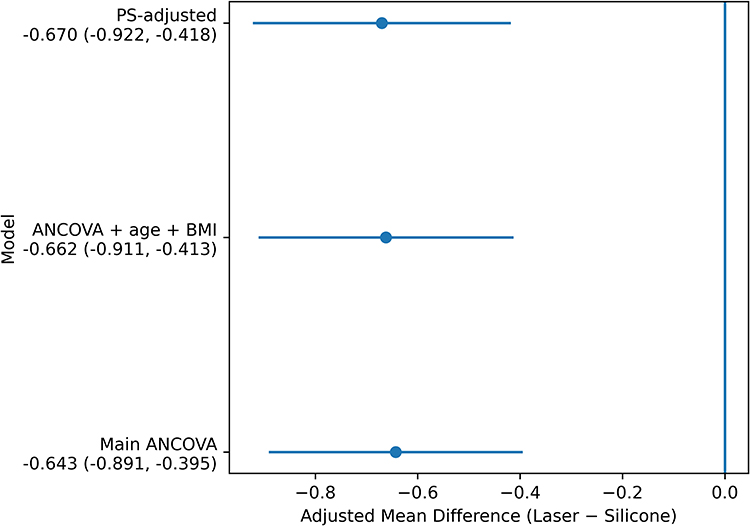 |
Figure 4 Robustness of the primary outcome across analytic models. Forest plot of adjusted mean differences (Laser − Silicone) in VSS total score at 6 months across prespecified sensitivity analyses. The primary ANCOVA model adjusted for baseline VSS and the interval from surgery to treatment. Additional models further adjusted for age and body mass index, and a propensity score–adjusted model incorporating baseline demographic and scar-related covariates. Points represent adjusted mean differences and horizontal lines indicate 95% confidence intervals. The vertical line at 0 denotes no between-group difference. Consistent effect estimates across models demonstrate the robustness of the primary finding. |
Discussion
This study provides a direct comparison of fractional CO2 laser therapy and topical silicone gel for the management of post–cesarean section scars. The primary finding is that fractional CO2 laser was associated with improved scar quality at 6 months, reflected by a lower VSS total score and consistent improvements in vascularity, pigmentation, and height/thickness. While pliability showed a directionally favorable difference, it did not reach statistical significance. These structural benefits were accompanied by significant reductions in symptom burden, including pain, pruritus, and tightness, as well as markedly higher patient satisfaction, with no increase in adverse events. The robustness of the findings was further confirmed by sensitivity analyses, including additional covariate adjustment and propensity score–based modeling, which support the conclusion that the observed effects are unlikely to be explained by baseline imbalances or selection bias.
These findings should be interpreted within the context of routine clinical practice, where different treatment strategies are applied. Cesarean scars develop under unique mechanical and hormonal conditions that can promote fibroblast activation and aberrant collagen deposition.18,19 Silicone gel, widely recommended as a first-line treatment, primarily provides epidermal hydration and barrier effects, which may not be sufficient once dermal architecture is disrupted.20 In contrast, fractional CO2 laser induces controlled microablative injury, promoting collagen synthesis, reorganizing extracellular matrix, and modulating vascularization and inflammation.8,11,21,22 The observed improvements in both objective VSS outcomes and patient-reported symptoms reflect the clinical relevance of dermal remodeling and offer a novel option for post-cesarean scar management. By targeting the underlying biology of scar formation, the study introduces a mechanism-aligned approach to treatment, offering both structural and functional benefits.
This research helps advance the field in several ways. First, it provides comparative effectiveness data in a patient population that has been largely overlooked in previous studies.23–25 Much of the scar literature aggregates data from different surgical sites or etiologies, making it difficult to draw conclusions specific to cesarean scars.23,24 By focusing on a homogeneous cohort and employing standardized, objective outcome measures, this study offers valuable insights into the efficacy of fractional CO2 laser in obstetric care. Second, the inclusion of both objective scar metrics and patient-centered outcomes responds to the growing emphasis on value-based care.26,27 The observed concordance between improvements in scar appearance and reductions in symptoms suggests that dermal remodeling can have meaningful functional benefits, particularly in the postpartum period when women experience both physical discomfort and psychological distress related to body image.
There are several other ways to study the hypothesis explored in this research. A randomized controlled trial (RCT) with concealed allocation would provide the highest level of evidence. However, RCTs in postpartum populations are often difficult to conduct due to patient preferences, logistical constraints, and ethical concerns. Alternative designs such as cluster randomization or stepped-wedge trials could offer a more pragmatic approach while maintaining scientific rigor. Mechanistic studies using noninvasive imaging techniques, such as high-frequency ultrasound or optical coherence tomography, could provide insight into the biological processes underlying scar remodeling following laser treatment. Additionally, studies exploring combination therapies, such as laser with silicone gel or microneedling, could offer valuable insights into the optimal sequencing of treatments for complex or high-risk scars.
The importance and potential applications of fractional CO2 laser therapy extend beyond post-cesarean scar management. In dermatology and plastic surgery, fractional CO2 laser is already widely used for treating various types of scars, including those resulting from trauma or surgery.15,24,28 The findings of this study reinforce the clinical efficacy of this modality, particularly for scars that are mechanically stressed or hormonally influenced, as is the case with cesarean scars. From a broader healthcare perspective, the ability to improve both the appearance of scars and the associated symptoms without increasing adverse events offers a cost-effective solution for postpartum women, particularly in settings where access to laser technology is available. The study also suggests that fractional CO2 laser could be a valuable tool for scar management in other surgical contexts, such as abdominal or bariatric surgery, where similar biomechanical forces are at play.
Looking ahead, several research directions are worth pursuing. First, studies should evaluate the optimal timing of fractional CO2 laser treatment to determine whether early intervention during the remodeling phase produces greater benefits or whether delayed treatment of established scars is equally effective. Second, optimizing dose-response relationships, including laser energy settings, treatment frequency, and number of passes, is essential to achieving the best outcomes with minimal side effects. Long-term follow-up is essential to assess the durability of the treatment effect and identify any late complications or recurrences. Third, cost-effectiveness analyses comparing fractional CO2 laser therapy with other scar management options, such as silicone gel or microneedling, are needed to guide clinical decision-making in resource-limited settings. Finally, personalized approaches to scar treatment, incorporating genetic predisposition, scar phenotype, and patient preferences, could improve outcomes by tailoring therapies to individual needs.
Despite the strengths of this study, several limitations must be considered. First, the retrospective and non-randomized design introduces the potential for selection bias and precludes definitive causal inference. Although adjustment for baseline characteristics and propensity score based methods were applied to reduce measured confounding, residual confounding from unmeasured factors such as socioeconomic status, patient preferences, or variations in surgical technique cannot be excluded. Second, although the analysis adjusted for baseline VSS, the laser group presented with slightly higher baseline VSS scores, which may have influenced the magnitude of observed differences. While statistical adjustment was performed, the possibility of residual imbalance remains, and randomized controlled trials with concealed allocation would be required to fully address this issue. Third, this was a single center study, which may limit the generalizability of the findings to other populations or clinical settings. Multicenter studies across diverse patient populations and treatment environments are warranted to validate these results. Fourth, the follow up period was limited to 6 months, which may not fully capture the long term durability of scar remodeling or potential delayed adverse effects. Longer term studies are needed to better assess sustained treatment outcomes. Finally, although assessor blinding and standardized outcome measures were implemented, patient reported outcomes may be influenced by expectation bias, and subjective perceptions could affect satisfaction ratings.
In conclusion, this study suggests that fractional CO2 laser therapy is associated with improved scar outcomes in women with post-cesarean scars. These findings should be interpreted with caution given the retrospective, non-randomized design and the potential for residual confounding. Therefore, the results are best considered hypothesis-generating and require confirmation in well-designed randomized controlled trials before informing clinical decision-making.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participation
Written informed consent was obtained from all participants. This research was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of The Fujian Maternity and Child Health Hospital (No. 2022YJ112).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Startup Fund for Scientific Research from Fujian Medical University (Grant number:2021QH1190).
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Bikash C, Sarkar R. Topical management of acne scars: the uncharted terrain. J Cosmet Dermatol. 2023;22(4):1191–13. doi:10.1111/jocd.15584
2. Dahm S, Lee G, Cleland H, Menezes H, Ng S. The use of carbon dioxide and intense pulsed light laser for the treatment of hypertrophic burn scars: a case series. Scars Burns Healing. 2023;9:20595131231202103. doi:10.1177/20595131231202103
3. Jafarzadeh A, Torkaman N, Haeri Boroujeni D, Goodarzi A. Systematic review of laser and Light-Based procedural treatments for hidradenitis suppurativa. Lasers Med Sci. 2025;40(1):469. doi:10.1007/s10103-025-04722-2
4. Klosová H, Xinopulos P, Zálešák B, Langová K. Fractional CO2 laser therapy of hypertrophic scars – evaluation of efficacy and treatment protocol optimization. Acta chirurgiae plasticae. 2021;63(4):171–180. doi:10.48095/ccachp2021171
5. Kwon HH, Yang SH, Lee J, et al. Combination treatment with human adipose tissue stem cell-derived exosomes and fractional CO2 Laser for acne scars: a 12-week prospective, double-blind, randomized, split-face study. Acta Dermato Venereologica. 2020;100(18):adv00310. doi:10.2340/00015555-3666
6. Broughton G 2nd, Janis JE, Attinger CE. The basic science of wound healing. Plast Reconstr Surg. 2006;117:12S–34S. doi:10.1097/01.prs.0000225430.42531.c2
7. Janis JE, Harrison B. Wound healing: part I. Basic science. Plast Reconstr Surg. 2014;133(2):199e–207e. doi:10.1097/01.prs.0000437224.02985.f9
8. Khansa I, Harrison B, Janis JE. Evidence-based scar management: how to improve results with technique and technology. Plast Reconstr Surg. 2016;138(3S):165S–178S. doi:10.1097/PRS.0000000000002647
9. Janis J, Harrison B. Wound healing: part II. Clinical applications. Plast Reconstr Surg. 2014;133(3):383e–392e. doi:10.1097/PRS.0000000000000077
10. Zhao T, Li M, Wang J, et al. Comparison of the effects of adipose extracellular matrix/stromal vascular fraction gel injection andCO 2Fractional laser on atrophic acne scar in asians through a 24-week prospective, randomized, split-face study. J Cosmet Dermatol. 2025;24(3):e70131. doi:10.1111/jocd.70131
11. Cai Y, Tian J, Li J, et al. A novel combined technology for treating hypertrophic scars: adipose tissue extract combined with fractional CO2 laser. Front Physiol. 2023;14:1284312. doi:10.3389/fphys.2023.1284312
12. Choi C, Mukovozov I, Jazdarehee A, et al. Management of hypertrophic scars in adults: a systematic review and meta-analysis. Australasian J Dermatol. 2022;63(2):172–189. doi:10.1111/ajd.13790
13. Disphanurat W, Kaewkes A, Suthiwartnarueput W. Comparison between topical recombinant human epidermal growth factor and Aloe vera gel in combination with ablative fractional carbon dioxide laser as treatment for striae alba: a randomized double-blind trial. Lasers Surg Med. 2020;52(2):166–175. doi:10.1002/lsm.23052
14. Gad SE-S, Neinaa YME-H, Rizk OK, Ghaly NE-SR. Efficacy of platelet-poor plasma gel in combination with fractional CO 2 laser in striae distensae: a clinical, histological, and immunohistochemical study. J Cosmet Dermatol. 2021;20(10):3236–3244. doi:10.1111/jocd.14102
15. Gawdat HI, El-Hadidy YA, Allam R, Abdelkader HA. Autologous platelet-rich plasma ‘fluid’ versus ‘gel’ form in combination with fractional CO 2 laser in the treatment of atrophic acne scars: a split-face randomized clinical trial. J Dermatol Treatment. 2022;33(5):2654–2663. doi:10.1080/09546634.2022.2067816
16. Huang J, Chen J, Wo Y, et al. CO 2 fractional laser combined with 5-fluorouracil ethosomal gel treatment of hypertrophic scar macro-, microscopic, and molecular mechanism of action in a rabbit animal model. Rejuvenat Res. 2021;24(2):131–138. doi:10.1089/rej.2019.2204
17. Jafarzadeh A, Hoseini SS, Behrangi E, Roohaninasab M, Goodarzi A. Regenerative medicine for atrophic scars: a systematic review of extracellular vesicles, conditioned media, stromal vascular fraction, and mesenchymal stem cells. Aesthetic Plastic Surg. 2025. doi:10.1007/s00266-025-05284-y
18. Mohamed MM, Sabry HH, Salem RM. Treatment of atrophic acne scars: topical or intralesional plasma gel? Photodermatol Photoimmunol Photomed. 2022;38(1):29–37. doi:10.1111/phpp.12712
19. Peng L, Tang S, Li Q. Intense pulsed light and laser treatment regimen improves scar evolution after cleft lip repair surgery. J Cosmet Dermatol. 2018;17(5):752–755. doi:10.1111/jocd.12684
20. Zhang Y, Liu Y, Cai B, et al. Improvement of surgical scars by early intervention with carbon dioxide fractional laser. Lasers Surg Med. 2020;52(2):137–148. doi:10.1002/lsm.23129
21. Alajlan A, AlHarbi S, Nagshabandi KN, et al. Silicone-based fluid gel versus white paraffin ointment in the treatment of post-fractional ablative CO 2 laser wound: an intra-individual split-face comparative study. J Dermatol Treatment. 2025;36(1):2583235. doi:10.1080/09546634.2025.2583235
22. Du H-X, Hu -Y-Y. Clinical observation of recombinant bovine basic fibroblast growth factor as an adjuvant therapy for patients with atrophic acne scar. Zhongguo yi xue ke xue yuan xue bao. 2022;44(2):208–212. doi:10.3881/j.issn.1000-503X.13708 Danish
23. Fakhraei S, Sazgarnia A, Taheri AR, et al. Evaluating the efficacy of photodynamic therapy with indocyanine green in the treatment of keloid. Photodiagn Photodyn Ther. 2022;38:102827. doi:10.1016/j.pdpdt.2022.102827
24. Lodi G, Mancuso FR, Zingoni T, Fusco I, Cannarozzo G, Sannino M. CO2 laser frenuloplasty for cryotherapy-induced frenulum perforation: a case report. AME Case Reports. 2025;9:44. doi:10.21037/acr-24-165
25. Majid I, Imran S. Fractional carbon dioxide laser resurfacing in combination with potent topical corticosteroids for hypertrophic burn scars in the pediatric age group: an open label study. Dermatol Surg. 2018;44(8):1102–1108. doi:10.1097/dss.0000000000001413
26. Yang Q, Yin Y, Dou W, Fan X, Xue P, Li T. Effect of fractional carbon dioxide laser combined with recombinant bovine basic fibroblast growth factor gel in the treatment of mature scar after facial scald burns: a retrospective cohort study. Lasers Med Sci. 2025;40(1):332. doi:10.1007/s10103-025-04578-6
27. Zhang Z-B, Zhou Z-L, Xing F-X, et al. Analysis of energy and density in treating hypertrophic scar after burn in children with CO 2 dot matrix laser. Int J Lower Extremity Wounds. 2025;24(4):1068–1074. doi:10.1177/15347346221144152
28. Zheng Q, Yu J, Lun X, Wang W, Chen Z. Combined cryotherapy and photodynamic therapy for recurrent generalized giant plantar warts: a case report. Photodiagn Photodyn Ther. 2025;55:104762. doi:10.1016/j.pdpdt.2025.104762
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.