Back to Journals » International Journal of Women's Health » Volume 18
Comparative Effectiveness of Azithromycin versus Erythromycin for Latency Prolongation in Preterm Prelabor Rupture of Membranes < 34 Weeks of Gestation
Authors Chawanpaiboon S ![]() , Pooliam J
, Pooliam J
Received 28 February 2026
Accepted for publication 15 April 2026
Published 21 April 2026 Volume 2026:18 603582
DOI https://doi.org/10.2147/IJWH.S603582
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Saifon Chawanpaiboon,1 Julaporn Pooliam2
1Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynaecology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Clinical Epidemiological Unit, Office for Research and Development, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Saifon Chawanpaiboon, Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynaecology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand, Tel +66 2 419 7000 ext. 4777– 4888, Fax +66 2 418 2662, Email [email protected]
Objective: Preterm prelabor rupture of membranes (PPROM) is a major contributor to preterm birth and neonatal morbidity. Although azithromycin is increasingly used as an alternative to erythromycin for latency antibiotic therapy, comparative data remain limited. This study evaluated whether azithromycin is associated with latency duration and maternal–neonatal outcomes comparable to those of erythromycin in pregnancies complicated by PPROM before 34 weeks of gestation.
Methods: A retrospective cohort study was conducted at a tertiary referral hospital by reviewing medical records from January 2011 through December 2024. Pregnant women with PPROM at 24 to < 34 weeks of gestation who completed latency antibiotic regimens were included and categorized into azithromycin or erythromycin groups. The primary outcome was latency period (time from membrane rupture to delivery). Secondary outcomes included maternal infectious complications and neonatal morbidity and mortality. Multivariable logistic regression was performed to adjust for baseline differences between groups.
Results: A total of 720 participants were included (56 azithromycin; 664 erythromycin). Baseline characteristics were generally comparable, although maternal age, monthly income, and previous PPROM differed between groups. Median latency duration did not differ significantly between azithromycin and erythromycin overall (3.70 vs 3.23 days; P = 0.287) or across gestational-age subgroups. After adjustment for baseline differences, the likelihood of achieving latency ≥ 3 days was similar between groups. Maternal outcomes were largely comparable, although postpartum endometritis occurred more frequently in the azithromycin group with small event numbers. Neonatal outcomes were generally similar; NICU admission was lower, whereas intraventricular hemorrhage was more frequent in the azithromycin group, both based on small numbers.
Conclusion: Azithromycin was associated with latency duration and maternal–neonatal outcomes comparable to those of erythromycin and represents a practical alternative regimen for PPROM management. Prospective studies are warranted to confirm these findings.
Plain Language Summary: When a pregnant woman experiences preterm prelabor rupture of membranes (PPROM), her water breaks too early before labor begins. This can increase the risk of infection and early birth. To help reduce these risks and safely prolong pregnancy, doctors routinely give antibiotics.
Erythromycin has traditionally been used for this purpose. However, azithromycin is increasingly used because it is easier to take, better tolerated, and more widely available in some settings. Despite this, there is still limited evidence directly comparing these two antibiotics.
In this study, we reviewed the medical records of 720 pregnant women with PPROM before 34 weeks of pregnancy who received either azithromycin or erythromycin. We compared how long pregnancy continued after treatment and examined health outcomes for both the women and their babies.
We found that pregnancy was prolonged for a similar length of time in both groups. Most maternal and neonatal outcomes were also similar between the two treatments. Some differences were observed in rare complications, but these findings should be interpreted cautiously because of the small number of cases.
Overall, our results suggest that azithromycin works as well as erythromycin for managing PPROM and may be a practical alternative, especially where erythromycin is less available or more difficult to use. Further studies are needed to confirm these findings and assess long-term outcomes for children.
Keywords: azithromycin, erythromycin, latency period, PPROM, preterm prelabor rupture of membranes
Introduction
Preterm prelabor rupture of membranes (PPROM), defined as rupture of the fetal membranes before he onset of labor and prior to 37 weeks of gestation, affects approximately 2%–3% of pregnancies and contributes to 25%–30% of all preterm births.1,2 PPROM is associated with substantial neonatal and maternal morbidity, including intrauterine infection, respiratory complications, intraventricular hemorrhage, necrotizing enterocolitis, neonatal sepsis, and increased maternal infectious morbidity.1,2 Although the precise pathophysiology of PPROM remains incompletely understood, intra-amniotic inflammation and ascending infection are recognized as major contributors.3,4 Pathogenic microorganisms such as Ureaplasma urealyticum, Mycoplasma hominis, streptococcal and staphylococcal species, and gram-negative enteric bacteria can weaken fetal membranes through the production of proteases and inflammatory mediators, thereby precipitating membrane rupture and leading to adverse perinatal outcomes.5,6
Antibiotic therapy is a cornerstone of PPROM management because it reduces ascending infection, decreases maternal and neonatal infectious morbidity, and prolongs the latency period (the interval between membrane rupture and delivery).7 Broad-spectrum antibiotic regimens have consistently been shown to prolong pregnancy duration, lower the risk of chorioamnionitis, and reduce neonatal infectious outcomes.8 Based on this evidence, the American College of Obstetricians and Gynecologists recommends a 7-day antibiotic regimen for PPROM before 34 weeks of gestation, traditionally consisting of intravenous ampicillin and erythromycin for 48 hours followed by oral amoxicillin and erythromycin for 5 days.9
In addition to recommendations from the American College of Obstetricians and Gynecologists, international guidelines and clinical practice patterns—including those from the Royal College of Obstetricians and Gynaecologists and other global settings—continue to support erythromycin as standard therapy while recognizing azithromycin as an acceptable alternative when erythromycin is unavailable or not tolerated.10,11 Furthermore, consideration of antimicrobial stewardship is important, as azithromycin is widely used for other infectious diseases, its use in obstetric care should be guided by clinical necessity and local practice patterns.
However, erythromycin is associated with limitations including frequent dosing requirements, gastrointestinal adverse effects, and variable availability in some clinical settings, which may affect treatment adherence and implementation in real-world practice. In contrast, azithromycin has emerged as a practical alternative due to its longer half-life, simplified dosing regimen, improved tolerability, and potential anti-inflammatory properties.
When erythromycin is unavailable or contraindicated, azithromycin is recommended as an alternative, with studies suggesting comparable latency prolongation12,13 and substantially reduced treatment cost.13–15 Several studies, including randomized trials, retrospective cohorts, and meta-analyses, have evaluated azithromycin-based regimens and generally reported comparable latency duration and maternal–neonatal outcomes relative to erythromycin.13,16,17 Some evidence also suggests that azithromycin may be associated with lower rates of maternal infectious morbidity, although findings remain inconsistent.13
Recent evidence increasingly supports the use of azithromycin for PPROM. A systematic review and meta-analysis by Seaman et al13 reported no statistically significant difference in latency period between azithromycin- and erythromycin-based regimens, whereas azithromycin demonstrated a lower incidence of chorioamnionitis. Additional retrospective analyses have shown that azithromycin is at least as effective as erythromycin in prolonging latency and may be associated with improved maternal infectious outcomes.18,19 However, variations in antibiotic dosing regimens, heterogeneity in study populations, and limited stratification by gestational age leave uncertainty regarding the optimal antibiotic choice for specific gestational-age subgroups. Despite these findings, important gaps remain, including heterogeneity in antibiotic regimens, limited evaluation in real-world clinical settings, and a lack of stratified analyses across gestational-age subgroups. These limitations create uncertainty regarding whether azithromycin can reliably replace erythromycin across different clinical contexts and patient populations.
At Siriraj Hospital, azithromycin has been used in place of erythromycin for PPROM management for 2 years because of its convenience, tolerability, and availability. This transition in institutional practice provides an opportunity to evaluate the comparative effectiveness of these two regimens in a real-world setting. Nonetheless, no study has evaluated whether azithromycin and erythromycin yield different latency durations or neonatal and maternal outcomes across distinct gestational-age categories (extremely preterm, very preterm, and moderate preterm). Given the differing risks and biological characteristics across these gestational ranges, understanding whether the antibiotics perform similarly in each subgroup is clinically important.
Therefore, this study aimed to compare latency duration and maternal and neonatal outcomes between azithromycin and erythromycin among pregnant women with PPROM before 34 weeks of gestation, with additional stratified analyses by gestational-age groups: extremely preterm (24 to <28 weeks), very preterm (28 to <32 weeks), and moderate preterm (32 to <34 weeks). Given that gestational age is a major determinant of both infectious risk and neonatal outcomes, understanding whether antibiotic effectiveness differs across these subgroups is clinically important. Findings from this study may help inform antibiotic selection for PPROM management and provide real-world evidence to guide clinical practice.
Materials And Methods
Study Design and Setting
This retrospective cohort study was conducted at the Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. Medical records of pregnant women diagnosed with preterm prelabor rupture of membranes (PPROM) before 34 weeks of gestation between January 2011 and December 2024 were reviewed. All eligible cases identified during the study period were included, yielding a total sample of 720 participants. The study protocol was approved by the Siriraj Institutional Review Board (reference: Si-032/2025).
Study Population
Eligible participants were pregnant women admitted with PPROM between 24+0 and 33+6 weeks of gestation who received a complete latency antibiotic regimen. Participants were assigned to 2 groups according to the antibiotic protocol used during admission.
Antibiotic Regimens
In the azithromycin group, women received intravenous ampicillin 2 g every 6 hours plus oral azithromycin 1 g once within the first 48 hours, followed by oral amoxicillin 500 mg 3 times daily for 5 days. In the erythromycin group, women received intravenous ampicillin 2 g every 6 hours combined with oral erythromycin 250 mg every 6 hours for the initial 48 hours. They then continued with oral amoxicillin 250 mg 3 times daily and oral erythromycin 250 mg 4 times daily for 5 days.
Eligibility Criteria
Participants were eligible for inclusion if they had a singleton or twin pregnancy, were diagnosed with PPROM between 24 and < 34 weeks of gestation, and had completed the prescribed latency antibiotic regimen according to their assigned treatment group. Women were excluded if they did not receive antibiotics intended for latency prolongation, had documented contraindications to antibiotic use, or had incomplete or missing clinical information necessary for primary outcome assessment.
Gestational-Age Subgroups
For analytical purposes, enrolled women in both treatment groups were further categorized based on gestational age at the time of membrane rupture into 3 predefined subgroups: extremely preterm (24 to < 28 weeks), very preterm (28 to < 32 weeks), and moderate preterm (32 to < 34 weeks).
Data Collection
Data were retrieved from hospital electronic medical records through a retrospective chart review conducted between January 2011 and December 2024 and were documented using a standardized case record form. Extracted information included maternal baseline characteristics such as age, height, weight, prepregnancy body mass index, gravidity, parity, obstetric history, underlying medical conditions, type of pregnancy, and socioeconomic status. Clinical and obstetric variables were also recorded, including gestational age at PPROM and at admission, cervical swab culture results, administration of corticosteroids and tocolytics, duration from membrane rupture to hospital presentation, and mode of delivery.
Study Outcomes
The primary outcome was the latency period, defined as the time from membrane rupture to delivery measured in hours. Secondary outcomes comprised maternal and neonatal complications. Maternal complications included clinical or histologic chorioamnionitis, postpartum endometritis, indications for delivery, and inflammatory laboratory parameters (white blood cell count, neutrophil percentage, and erythrocyte sedimentation rate). Neonatal outcomes included birthweight, Apgar scores, neonatal intensive care unit (NICU) admission, and respiratory morbidities (respiratory distress syndrome and transient tachypnea of the newborn). Additional neonatal outcomes were neonatal sepsis, necrotizing enterocolitis, intraventricular hemorrhage, apnea of prematurity, anemia of prematurity, retinopathy of prematurity, neonatal death, and length of NICU stay.
Sample Size
Because this investigation was conducted as a retrospective cohort study, the sample size was determined by the total number of eligible patients available during the study period rather than by a predefined sample size calculation. All pregnant women diagnosed with PPROM between January 2011 and December 2024 who met the inclusion criteria were included. A total of 720 cases were identified, comprising 664 women who received erythromycin and 56 who received azithromycin, reflecting real-world prescribing practices during the transition of institutional antibiotic protocols. The unequal group sizes reflect a temporal transition in institutional antibiotic practice, with erythromycin used predominantly in earlier years and azithromycin introduced more recently, rather than selective allocation. These data were analyzed as an observational comparative cohort despite the unequal group sizes.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA). All statistical tests were two-sided, and a P value < 0.05 was considered statistically significant. Continuous variables were assessed for normality and presented as mean (SD) for normally distributed data or median (range) for nonnormally distributed data, whereas categorical variables were expressed as frequencies and percentages.
Comparisons between the azithromycin and erythromycin groups were performed using the independent t test for normally distributed continuous variables or the Mann–Whitney U-test for nonnormally distributed variables. Categorical variables were compared using the chi-square test or Fisher exact test, as appropriate. The primary outcome, latency period from membrane rupture to delivery, was compared between treatment groups overall and within gestational-age subgroups using the same methods according to data distribution. Secondary maternal and neonatal outcomes were analyzed similarly.
Because baseline characteristics differed between groups, multivariable logistic regression analysis was conducted to adjust for potential confounding factors. Latency duration was categorized as <3 days and ≥3 days, and the association between antibiotic regimen and latency category was evaluated after adjustment for maternal age, monthly income ≥30,000 THB, and previous PPROM. Adjusted odds ratios with 95% confidence intervals were reported.
Statistical methods applied in this study are robust to unequal group sizes, and appropriate tests were selected accordingly. In addition, multivariable logistic regression was performed to adjust for baseline differences and reduce potential confounding.
Results
Baseline Characteristics
A total of 720 women with PPROM were included, comprising 56 in the azithromycin group and 664 in the erythromycin group. Baseline characteristics were generally comparable between groups (Table 1). Women who received azithromycin were older than those who received erythromycin (mean [SD], 32.2 [6.5] vs 29.5 [6.8] years; P = 0.004), and a higher proportion had a monthly income ≥30,000 THB (67.9% vs 41.4%; P < 0.001). In contrast, a history of previous PPROM was more common among women in the erythromycin group (24.8% vs 10.7%; P = 0.021).
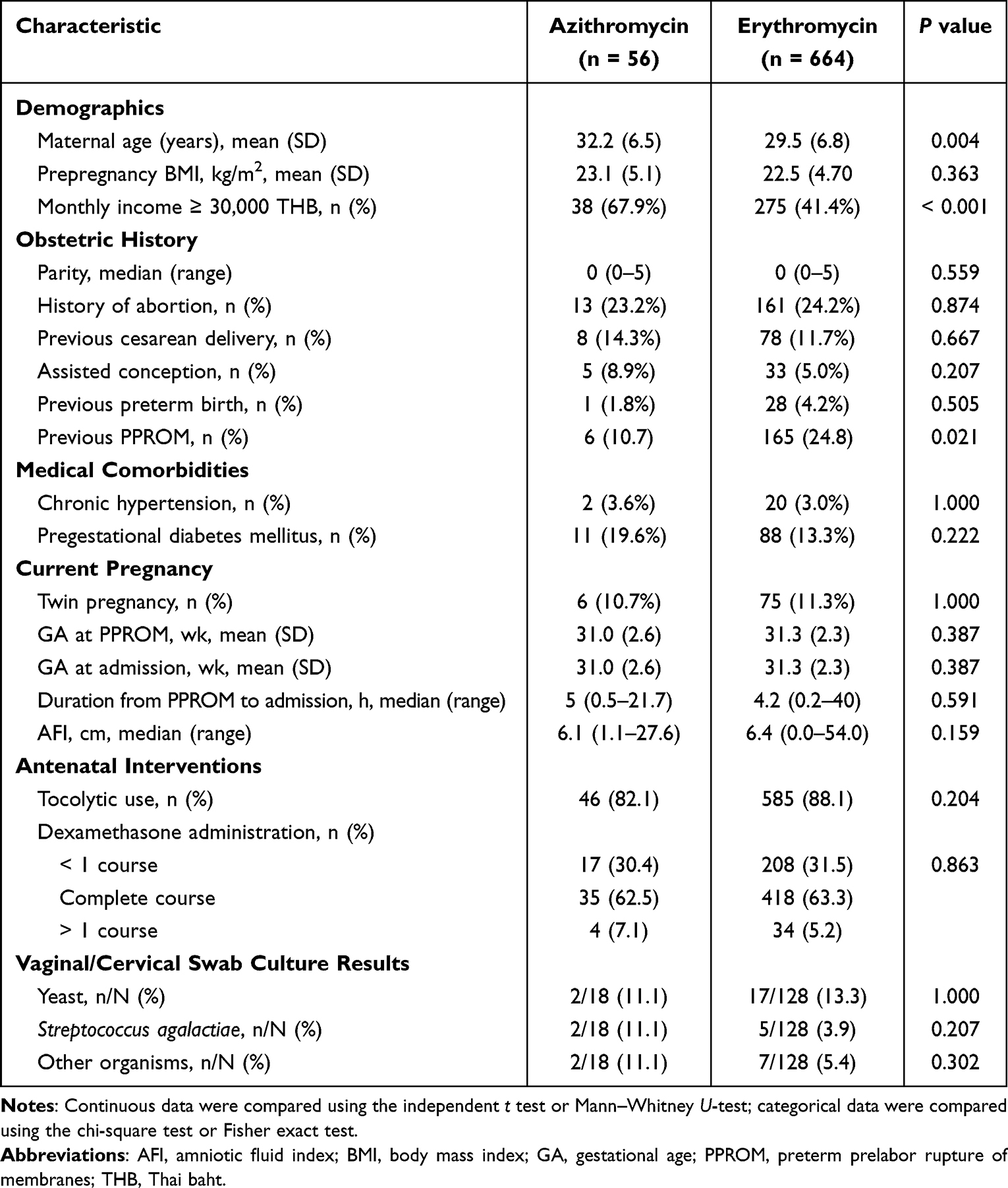 |
Table 1 Baseline Maternal Characteristics by Antibiotic Group (N = 720) |
No statistically significant differences were observed between groups in prepregnancy body mass index, parity, history of abortion, previous cesarean delivery, assisted conception, previous preterm birth, or medical comorbidities. Current pregnancy characteristics, including twin pregnancy, gestational age at PPROM and at admission, duration from membrane rupture to admission, and amniotic fluid index, were also similar between groups. In addition, antenatal interventions (tocolytic use and dexamethasone administration) and vaginal or cervical swab culture results did not differ significantly between treatment groups.
Primary Outcome–Latency Period
Overall, the median latency period was similar between the azithromycin and erythromycin groups (3.70 days [range, 0.34–23.00] vs 3.23 days [range, 0.10–72.38], respectively), with no statistically significant difference (median difference, 0.38 days; 95% CI, −0.33 to 1.10; P = 0.287) (Table 2).
 |
Table 2 Latency Period by Antibiotic Group and Gestational-Age Subgroup |
Subgroup analyses by gestational age also showed no statistically significant differences between treatment groups. In the extremely preterm subgroup (24 to <28 weeks), the median latency was 4.08 days in the azithromycin group and 4.49 days in the erythromycin group (median difference, −0.15 days; 95% CI, −3.65 to 2.66; P = 0.888). In the very preterm subgroup (28 to <32 weeks), the median latency was 4.51 days versus 3.89 days (median difference, 0.45 days; 95% CI, −1.08 to 1.81; P = 0.541). Similarly, in the moderate preterm subgroup (32 to <34 weeks), the median latency was 3.08 days in the azithromycin group and 2.74 days in the erythromycin group (median difference, 0.23 days; 95% CI, −0.60 to 1.08; P = 0.562). Overall, latency duration did not differ significantly between antibiotic regimens across gestational-age categories.
Association Between Antibiotic Regimen and Latency Period ≥3 Days
Unadjusted analysis showed no significant association between antibiotic regimen and achieving a latency period of ≥3 days. Compared with erythromycin, azithromycin was associated with a nonsignificant increase in the odds of latency ≥3 days (odds ratio [OR], 1.399; 95% CI, 0.797–2.454; P = 0.265) (Table 3).
 |
Table 3 Association Between Antibiotic Regimen and Latency Period ≥3 days |
After adjustment for maternal age, monthly income ≥30,000 THB, and previous PPROM using multivariable logistic regression, the association remained nonsignificant (adjusted odds ratio [aOR], 1.406; 95% CI, 0.792–2.495; P = 0.245), indicating that the likelihood of achieving latency ≥3 days did not differ significantly between the azithromycin and erythromycin groups.
Maternal Outcomes
Rates of maternal adverse outcomes were generally comparable between the azithromycin and erythromycin groups (Table 4). The incidence of clinical chorioamnionitis did not differ significantly between groups (21.4% vs 14.2%; P = 0.167). Postpartum endometritis occurred more frequently in the azithromycin group (3.6% vs 0.2%; P = 0.017), although the absolute number of cases was small. Maternal sepsis was rare, with no cases observed in the azithromycin group and one case in the erythromycin group (P = 1.000).
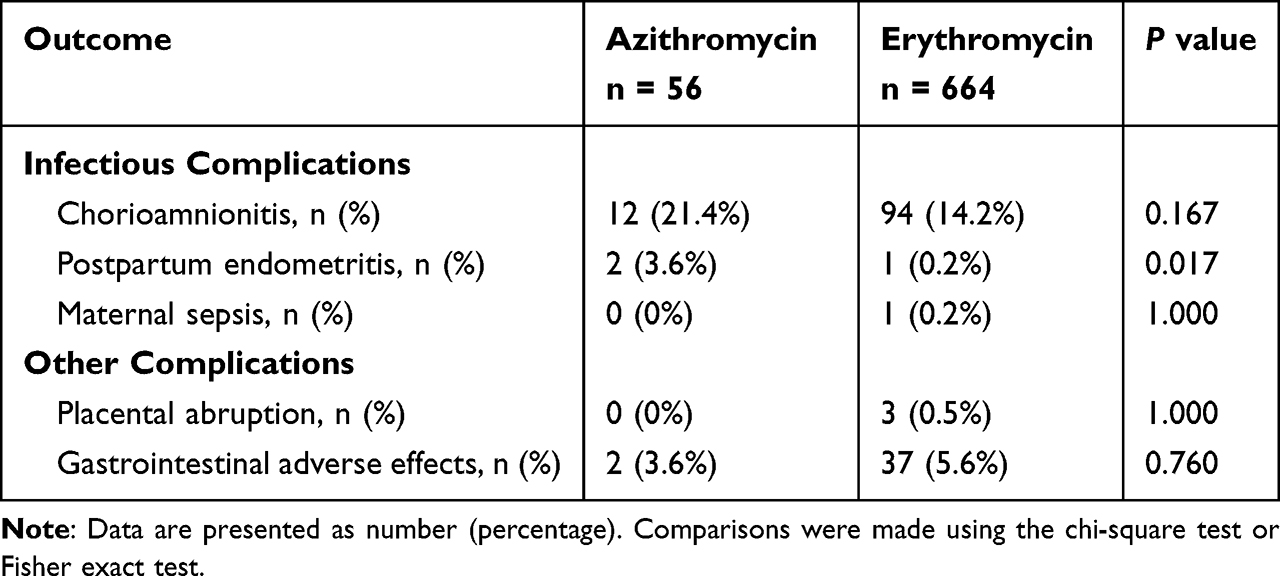 |
Table 4 Maternal Adverse Outcomes by Antibiotic Group |
Other maternal complications, including placental abruption (0% vs 0.5%; P = 1.000) and gastrointestinal adverse effects (3.6% vs 5.6%; P = 0.760), did not differ significantly between treatment groups.
Neonatal Outcomes
Neonatal outcomes were generally comparable between the azithromycin and erythromycin groups (Table 5). Mean birthweight and the proportion of neonates with an Apgar score <7 at 1 minute did not differ significantly between groups. Similarly, rates of respiratory morbidity, including respiratory distress syndrome, transient tachypnea of the newborn, and need for intubation, were comparable.
 |
Table 5 Neonatal Outcomes by Antibiotic Group |
No statistically significant differences were observed in infectious outcomes, including neonatal sepsis and necrotizing enterocolitis. Most complications of prematurity, such as apnea of prematurity, anemia of prematurity, and retinopathy of prematurity, were also similar between groups.
Intraventricular hemorrhage occurred more frequently in the azithromycin group (3.6% vs 0%; P = 0.006), although the number of events was small. Neonates in the azithromycin group had a lower rate of neonatal intensive care unit (NICU) admission (3.6% vs 15.8%; P = 0.017), but among those admitted, the median duration of NICU stay was longer (29 vs 21 days; P = 0.020). Neonatal mortality did not differ significantly between groups (1.8% vs 3.2%; P = 1.000).
Discussion
This study evaluated the effectiveness of azithromycin compared with erythromycin for latency prolongation among women with PPROM before 34 weeks of gestation. Overall, the latency period did not differ significantly between the two antibiotic regimens. Subgroup analyses by gestational age also demonstrated no statistically significant differences in latency duration across the extremely preterm (24 to <28 weeks), very preterm (28 to <32 weeks), and moderate preterm (32 to <34 weeks) groups. Although slightly longer median latency was observed in the azithromycin group in some gestational-age categories, these differences were not statistically significant. These findings indicate that azithromycin provides comparable latency outcomes to erythromycin across gestational-age subgroups.
It should be noted that latency duration in PPROM is multifactorial and may also be influenced by clinical variables such as residual amniotic fluid volume, gestational age at rupture, fetal condition, and the degree of intra-amniotic inflammation, in addition to antibiotic therapy. Oligohydramnios or anhydramnios is consistently linked to shorter latency and earlier delivery in both inpatient and outpatient PPROM cohorts.20–22 Normal/greater residual fluid is associated with prolonged latency and better survival in several studies.20 Higher gestational age at PPROM predicts shorter latency in multiple large series.23 Earlier, “previable” rupture is paradoxically associated with longer latency but worse overall prognosis because extreme prematurity dominates outcomes.23 Markers of labor or uterine activation (uterine contractions, higher Bishop score, greater cervical dilatation, short cervix) predict short latency.24 Twin gestation and fetal growth restriction are also associated with shorter latency.25 Elevated CRP, leukocytosis, or intra-amniotic inflammatory markers (IL-6, MMP-8) correlate with shorter latency and higher risk of adverse outcomes.26 Latency antibiotics are associated with prolonged latency and reduced chorioamnionitis and birth within 7 days.27
Multiple randomized trials, cohort studies, and meta-analyses have consistently reported that azithromycin and erythromycin demonstrate comparable efficacy in prolonging the latency period (the interval from PPROM to delivery).13,17 These regimens have also been associated with similar maternal and neonatal outcomes, including birthweight, Apgar scores, and neonatal survival. Overall, prior studies have shown no statistically significant differences in latency duration between the two antibiotics across various dosing regimens.28
Our findings are consistent with existing literature reporting comparable latency outcomes between azithromycin and erythromycin. A meta-analysis by Seaman et al13 found no statistically significant difference in latency duration, supporting azithromycin as an effective alternative agent. However, most previous studies did not stratify outcomes by gestational age or were limited by smaller sample sizes. By incorporating gestational-age subgroup analysis in a large real-world cohort, our study provides additional granularity that may help refine antibiotic selection in PPROM management.
Potential gestational age–related differences in inflammatory and infectious mechanisms underlying PPROM are biologically plausible. As pregnancy advances, the relative contributions of infection, inflammation, and membrane structural changes may vary compared with extremely preterm cases, in which membrane weakness and intense intra-amniotic inflammation often predominate. Azithromycin has broader anti-inflammatory properties, a longer tissue half-life, and higher intracellular penetration, which may theoretically enhance infection control and inflammatory modulation. Although such pharmacologic characteristics suggest a potential gestational age–dependent effect, our study did not demonstrate statistically significant differences in latency duration across gestational-age subgroups. Further studies with larger balanced sample sizes are warranted to clarify whether gestational maturity modifies antibiotic response in PPROM.
Extremely preterm or midtrimester PPROM (approximately < 28 to 30 weeks of gestation) is more commonly associated with intrinsic membrane structural weakness and pronounced intra-amniotic inflammation, frequently driven by ascending infection. In these cases, bacterial byproducts and pro-inflammatory cytokines stimulate matrix metalloproteinases and other proteolytic enzymes, leading to collagen degradation and progressive weakening of the fetal membranes.29 High rates of intra-amniotic infection together with intense inflammatory signaling—mediated by cytokines such as IL-6 and IL-1β and pathways including HMGB1–DAMP–RAGE—promote extracellular matrix degradation, oxidative stress, and senescence-associated sterile inflammation. This pathological combination is characteristic of very early PPROM.3
Later PPROM, particularly in the late preterm period (34–36+6 weeks of gestation), is characterized by ongoing but often subclinical or low-grade intra-amniotic inflammation rather than overt infection. In this context, the principal concern shifts from acute membrane failure to prolonged fetal exposure to inflammatory mediators, with biomarkers such as IL-6 identifying high-risk intra-amniotic inflammatory states.30 Clinically, gestational age at both PPROM and delivery remains the strongest determinant of neonatal infection and respiratory morbidity, highlighting that similar inflammatory insults may result in markedly different outcomes depending on gestational maturity.1,30
Membrane biology evolves throughout pregnancy, with progressive senescence, oxidative stress, and sterile inflammation preparing term membranes for rupture. When these processes are triggered prematurely or combined with infection, PPROM may occur through different biological pathways at varying gestational ages.31
Cervical and vaginal swab cultures showed no statistically significant differences between the azithromycin and erythromycin groups, with most samples demonstrating either no growth or only low-virulence organisms. This finding is consistent with previous studies indicating that routine cervical cultures have limited sensitivity for detecting intra-amniotic infection in PPROM, as organisms such as Ureaplasma urealyticum and Mycoplasma hominis are frequently implicated but are not reliably identified using standard culture techniques.4,7 Given the absence of detectable differences in cervical pathogens between treatment groups, the comparable latency outcomes observed in this study are unlikely to be explained by differences in identifiable microorganisms alone. Pharmacologic differences between antibiotics, including antimicrobial spectrum and anti-inflammatory properties, may still influence clinical outcomes; however, further studies are needed to clarify these potential mechanisms.3,13
Maternal outcomes were largely comparable between groups. Rates of clinical chorioamnionitis were similar between the azithromycin and erythromycin groups, whereas postpartum endometritis occurred infrequently in both groups.2,19 In the present study, postpartum endometritis was observed more often in the azithromycin group; however, the absolute number of events was small, and this finding should be interpreted with caution. Unmeasured confounding factors—such as duration of labor, mode of delivery, or postpartum antibiotic exposure—may have contributed to this difference. Importantly, rates of chorioamnionitis, maternal sepsis, and gastrointestinal adverse effects did not differ significantly between groups, supporting the overall maternal safety profile of azithromycin.
Neonatal outcomes were generally similar between groups, including respiratory morbidity, neonatal sepsis, necrotizing enterocolitis, and mortality.1,2 The lower rate of NICU admission observed in the azithromycin group is clinically notable but should be interpreted cautiously, as gestational age at delivery and other perinatal factors not fully captured in the analysis may have influenced this finding. Conversely, the higher incidence of intraventricular hemorrhage among azithromycin-exposed neonates warrants careful interpretation. Given the small number of events and the retrospective study design, this difference may reflect variations in gestational age distribution, survival bias, or neonatal management factors rather than a direct drug effect. These findings highlight the importance of cautious interpretation and underscore the need for prospective studies with detailed neonatal and neurodevelopmental follow-up.
Beyond efficacy, azithromycin offers several practical advantages over erythromycin, including simplified dosing, improved tolerability, and fewer gastrointestinal adverse effects, which may enhance adherence in prolonged inpatient management. Cost-effectiveness analyses from previous studies have also suggested lower overall treatment costs with azithromycin. In settings where erythromycin availability fluctuates or where adherence is a concern, azithromycin represents a pragmatic alternative.
Taken together, our findings suggest that azithromycin is a clinically effective alternative to erythromycin for latency management in PPROM, with comparable maternal and neonatal outcomes. These results provide institution-specific real-world evidence that may help inform local clinical practice and antibiotic selection. Nevertheless, given the retrospective design and unequal group sizes, prospective randomized studies with balanced sample sizes are warranted to confirm these findings and to further evaluate neonatal neurological outcomes.
Strengths and Limitations
This study has several strengths. It includes a large cohort from a high-volume tertiary center, providing reliable real-world data. Stratification by gestational age offers clinically relevant insight into treatment performance across prematurity subgroups, which has been underexplored in previous research. The study also reflects actual clinical practice during a period of regimen transition, strengthening its applicability to real-world management scenarios.
However, several limitations should be acknowledged. The retrospective design restricts control over confounding variables and limits the ability to infer causality. A key limitation is the unequal group size, with substantially fewer patients in the azithromycin cohort following the institutional regimen change. This imbalance may reduce statistical power for detecting rare adverse events and may influence subgroup analyses. Differences observed in outcomes such as intraventricular hemorrhage and NICU admission require cautious interpretation because of the small number of events. Additionally, treatment allocation was not randomized; therefore, clinical decisions, maternal condition at presentation, or unmeasured factors may have influenced outcome patterns.
Despite these limitations, the study provides valuable comparative evidence indicating that azithromycin is associated with clinical outcomes comparable to those of erythromycin in PPROM management. Future prospective studies with balanced sample sizes and standardized clinical monitoring are recommended to validate these findings and to assess neonatal neurological outcomes more robustly.
Conclusion
Azithromycin was associated with latency duration comparable to that of erythromycin among women with PPROM before 34 weeks of gestation, with similar maternal and neonatal outcomes. These findings support azithromycin as an effective alternative regimen in clinical practice, particularly in settings where erythromycin availability is limited. Further prospective studies are warranted to confirm these results and to evaluate long-term neonatal outcomes.
Trial Registration
Thai Clinical Trials Registry. Registration number TCTR20241102001. Web link: https://www.thaiclinicaltrials.org/export/pdf/TCTR20241102001
Date of registration: November 2, 2024. Date of initial participant enrollment: January 30, 2025.
Data Sharing Statement
The datasets used and analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval
This study was reviewed and approved by the Siriraj Institutional Review Board, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand (reference: Si-032/2025; approval date: January 15, 2025). Due to the retrospective study design and the use of anonymized medical record data, the requirement for informed consent was waived by the Institutional Review Board. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors acknowledge the financial support provided by the Faculty of Medicine Siriraj Hospital, Mahidol University (reference: R016833007). The authors also thank David Park for English language editing of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, or acquisition, analysis, and interpretation of data; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received financial support from the Faculty of Medicine Siriraj Hospital, Mahidol University (reference: R016833007).
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Agaoglu RT, Öztürk Ö, Ulusoy C, et al. Perinatal outcomes and predictors of neonatal mortality in preterm premature rupture of membranes: a tertiary center experience. BMC Pregnancy Childbirth. 2025;25. doi:10.1186/s12884-025-07688-9
2. Baru L, Behera S, Kalsai PP. Obstetrics outcome in preterm premature rupture of membrane. Azerbaijan Pharm. Pharmacother. J. 2023;41–12. doi:10.61336/appj/22-1-10
3. Menon R, Behnia F, Polettini J, Richardson LS. Novel pathways of inflammation in human fetal membranes associated with preterm birth and preterm pre-labor rupture of the membranes. Semin Immunopathol. 2020;42(4):431–450. doi:10.1007/s00281-020-00808-x
4. Musilová I, Kutová R, Plíšková L, et al. Intraamniotic inflammation in women with preterm prelabor rupture of membranes. PLoS One. 2015;10.
5. Capros H. Ureaplasma in pregnancy. Is there any risk for preterm labor? One Health Risk Management. 2025;6:4–15. doi:10.38045/ohrm.2025.1.01
6. Shi D, Liu C, Cheng Y-H, Cheng H, Zhang Q. Correlation between Escherichia coli infection during pregnancy and maternal-fetal outcomes: a retrospective analysis. BMC Infect Dis. 2025;25. doi:10.1186/s12879-025-10998-0
7. Kacerovský M, Romero R, Štěpán M, et al. Antibiotic administration reduces the rate of intraamniotic inflammation in preterm prelabor rupture of the membranes. Am J Clin Exp Obstet Gynecol. 2020;223:114.e1–114.e20. doi:10.1016/j.ajog.2020.01.043
8. Trahan M-J, Ronzoni S, Roy-Lacroix M, et al. Antibiotic regimens for the management of preterm prelabour rupture of membranes: a multicenter retrospective cohort study. J Obstet Gynaecol. 2025;47:102922. doi:10.1016/j.jogc.2025.102922
9. Prelabor rupture of membranes: ACOG practice bulletin, number 217. Obstet Gynecol. 2020;135(3):e80–e97. doi:10.1097/AOG.0000000000003700
10. Antonucci R, Cuzzolin L, Locci C, Dessole F, Capobianco G. Use of azithromycin in pregnancy: more doubts than certainties. Clin. Drug Invest. 2022;42:921–935. doi:10.1007/s40261-022-01203-0
11. Pitsouni E, Iavazzo C, Athanasiou S, Falagas M. Single-dose azithromycin versus erythromycin or amoxicillin for Chlamydia trachomatis infection during pregnancy: a meta-analysis of randomised controlled trials. Int J Antimicrob Agents. 2007;30(3):213–221. doi:10.1016/j.ijantimicag.2007.04.015
12. Martingano D, Singh S, Mitrofanova A. Azithromycin in the treatment of preterm prelabor rupture of membranes demonstrates a lower risk of chorioamnionitis and postpartum endometritis with an equivalent latency period compared with erythromycin antibiotic regimens. Infectious Dis Obstetrics Gynecol. 2020;2020. doi:10.1155/2020/2093530
13. Seaman R, Kopkin R, Turrentine M. Erythromycin versus azithromycin for treatment of preterm prelabor rupture of membranes: a systematic review and meta-analysis. Am J Clin Exp Obstet Gynecol. 2021;226:794–801.e1. doi:10.1016/j.ajog.2021.12.262
14. Finneran M, Smith D, Buhimschi C. Cost analysis of azithromycin versus erythromycin in pregnancies complicated by preterm premature rupture of membranes. Am. J. Perinatol. 2018;36:105–110. doi:10.1055/s-0038-1667369
15. Ramadan HG, Mahmoud H, Shalan A, Abd E, Zayed E, Gomaa H. Azithromycin versus Erythromycin in Preterm Premature Rupture of Membranes: mansoura Experience. Egypt. J. Fertil. Steril. 2023.
16. Musavi E, Dizaji SH, Chamani M, Mohammadianamiri M. Comparison of azithromycin versus erythromycin on gestation length (prolongation of latency interval) and neonatal outcomes in pregnant women with premature rupture of the membrane: an open-label randomized clinical trial. Int J Pediatr. 2021.
17. Navathe R, Schoen CN, Heidari P, et al. Azithromycin vs erythromycin for the management of preterm premature rupture of membranes. Am J Obstet Gynecol. 2019;221(2):144.e1–e8. doi:10.1016/j.ajog.2019.03.009
18. Abdelfattah LE, Aboshama R, Abdelbadie A, Abulhasan M, Anan M, Abdelaal I. Different azithromycin protocols for management of preterm prelabour rupture of membranes: a randomized clinical trial. BMC Pregnancy Childbirth. 2022;22:22. doi:10.1186/s12884-021-04352-w
19. Aslam S, Farooq N, Maqbool M, Qurrat Ul A, Batool S, Zia S. Comparison of feto-maternal outcome in azithromycin versus erythromycin in management of PPROM; a randomized controlled trial. J Soc Obstetricians Gynaecologists Pakistan. 2025.
20. Greiner D, Balu N, Staab E, Lynden E, Bonebrake R, Dahlke J. Comparison in latency based on amniotic fluid index (afi) in patients with preterm prelabor rupture of membranes (PPROM).
21. Point F, Ghesquière L, Drumez É, et al. Risk factors associated with shortened latency before delivery in outpatients managed for preterm prelabor rupture of membranes. Acta Obstet. Gynecol. Scand. 2021;101:119–126. doi:10.1111/aogs.14287
22. Pylypjuk C, Majeau L. Perinatal Outcomes and Influence of Amniotic Fluid Volume Following Previable, Preterm Prelabor Rupture of Membranes (pPPROM): a Historical Cohort Study. Int J Women’s Health. 2021;13:627–637. doi:10.2147/IJWH.S303120
23. Seravalli V, Colucci C, Di Cencio C, Morucchio A, Barsanti F, Di Tommaso M. Latency to delivery and incidence of adverse obstetric and perinatal outcomes in preterm premature rupture of membranes before 32 weeks. Arch Gynecol Obstetrics. 2025;311:1569–1577. doi:10.1007/s00404-025-07970-3
24. Rouzaire M, Corvaisier M, Roumeau V, et al. Predictors of short latency period exceeding 48 h after preterm premature rupture of membranes. J Clin Med. 2021;11:10. doi:10.3390/jcm11010010
25. Madden N, Andrikopoulou M, Overton E, Gyamfi-Bannerman C. Latency Period after Preterm Premature Rupture of Membranes: singletons versus Twins. Am. J. Perinatol. 2021;40:68–73. doi:10.1055/s-0041-1727277
26. Sohn J-W, Choi E, Park C-W, Moon K, Park J-S, Jun J. Preterm labor and preterm-prom at a lower gestational age are associated with a longer latency-to-delivery even in patients with the same intensity of intra-amniotic inflammation: “carroll-model. Revisited Life. 2022;12.
27. Kantarcı S, Karabulut A, Bulut S, Bölükbaşı M, Kaygun BC, Ekin A. Determination of factors affecting the latent period of periviable premature rupture of membranes: cases and evaluation of newborn outcomes. Journal of Fetal Medicine. 2025.
28. Day KN, Vircks JA, Henricks CE, Reaves KM, Holmes AK, Florio KL. Latency antibiotics in preterm prelabor rupture of membranes: a comparison of azithromycin regimens. Ann Pharmacother. 2024;58(3):234–240. doi:10.1177/10600280231181135
29. Tchirikov M, Schlabritz-Loutsevitch N, Maher J, et al. Mid-trimester preterm premature rupture of membranes (PPROM): etiology, diagnosis, classification, international recommendations of treatment options and outcome. J Perinat Med. 2018;46(5):465–488. doi:10.1515/jpm-2017-0027
30. Vajrychova M, Stranik J, Kupcik R, et al. Quantification of intra-amniotic inflammation in late preterm prelabour rupture of membranes. Sci Rep. 2025;15(1):14814. doi:10.1038/s41598-025-99969-8
31. Menon R, Richardson LS, Lappas M. Fetal membrane architecture, aging and inflammation in pregnancy and parturition. Placenta. 2019;79:40–45. doi:10.1016/j.placenta.2018.11.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent/Refractory Multidrug- and Pre-Multidrug-Resistant Pseudomonas aeruginosa Infection Cases Maintained by Long-Term, Low-Dose Macrolide Administration
Seki M
Clinical Pharmacology: Advances and Applications 2026, 18:600235
Published Date: 12 May 2026