Back to Journals » Medical Devices: Evidence and Research » Volume 13
Comparative Effectiveness Assessment of Two Powered Surgical Stapling Platforms in Laparoscopic Sleeve Gastrectomy: A Retrospective Matched Study
Authors Rawlins L, Johnson BH ![]() , Johnston SS, Elangovanraaj N
, Johnston SS, Elangovanraaj N ![]() , Bhandari M, Cohen RV
, Bhandari M, Cohen RV ![]() , Rheinwalt KP
, Rheinwalt KP ![]() , Fryrear R, Roy S
, Fryrear R, Roy S
Received 22 April 2020
Accepted for publication 4 June 2020
Published 7 July 2020 Volume 2020:13 Pages 195—204
DOI https://doi.org/10.2147/MDER.S256237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Logan Rawlins,1 Barbara H Johnson,2 Stephen S Johnston,2 Nivesh Elangovanraaj,3 Mohit Bhandari,4 Ricardo V Cohen,5 Karl Peter Rheinwalt,6 Raymond Fryrear,2 Sanjoy Roy2
1Allegheny Health Network Bariatric & Metabolic Institute, Pittsburgh, PA, USA; 2Johnson & Johnson Medical Device Company, Cincinnati, OH, USA; 3Mu Sigma, Bangalore, India; 4Mohak Bariatric and Robotic Surgery Centre, Indore, India; 5The Center for the Treatment of Obesity and Diabetes, Hospital Alemão Oswaldo Cruz, Sao Paulo, Brazil; 6St. Franziskus-Hospital, Cologne, Germany
Correspondence: Stephen S Johnston
Director, Real-World Data Analytics and Research, Epidemiology, Medical Devices, Johnson & Johnson, 410 George Street, New Brunswick, NJ, US
Tel +1-443-254-2222
Email [email protected]
Objective: To compare outcomes between the two latest innovations in powered stapling technology, the ECHELON FLEX™ GST system (GST) and the Signia™ Stapling System (SIG), among patients undergoing sleeve gastrectomy for obesity.
Patients and Methods: Using the Premier Healthcare Database of US hospital discharge records, we selected patients undergoing inpatient sleeve gastrectomy with dates of surgical admission between March 1, 2017 (SIG launch), and December 31, 2018. Outcomes measured during the surgical admission included in-hospital hemostasis-related complications (bleeding/transfusion; primary outcome), leak, total hospital costs, length of stay (LOS), and operating room time; 30-, 60-, and 90-day all-cause inpatient readmissions were also examined. We used 1:1 cardinality matching to balance the GST and SIG groups on numerous patient and hospital/provider characteristics, allowing a maximum standardized mean difference (SMD) ≤ 0.05 for all matching covariates. Generalized estimating equations (GEE) accounting for hospital-level clustering were used to compare the study outcomes between the GST and SIG groups.
Results: Of the 5573 identified cases, there were 491 patients in each group (982 total) after matching. The observed incidence proportion of hemostasis-related complications during the surgical admission was lower in the GST group as compared with the SIG group (3 events/491 [0.61%] vs 11 events/491 [2.24%]; odds ratio [SIG=reference] = 0.28, 95% CI=0.13– 0.60, P=0.0012). Differences between the GST and SIG groups were not statistically significant for leak, total hospital costs, LOS, OR time, and all-cause inpatient readmission at 30, 60, and 90 days.
Conclusion: In this retrospective study of 982 matched patients undergoing sleeve gastrectomy, the ECHELON FLEX™ GST system was associated with a lower rate of hemostasis-related complications as compared with the Signia™ Stapling System. Further controlled prospective studies are needed to confirm the validity of this finding.
Keywords: sleeve gastrectomy, surgical staplers, bleeding, leak, cost
Introduction
Surgical staplers are widely used to perform excision of stomach tissue during laparoscopic sleeve gastrectomy, the most common surgical treatment for obesity in the US.1 Innovation in surgical stapling technology has evolved from manual to power-operated staplers. In contrast with manual staplers, powered staplers use battery power to drive the knife blade and staples, thus eliminating the variable grip force of the surgeon.
Previous studies have associated powered staplers with a lower risk of hemostasis-related complications (eg, bleeding, transfusion) and lower overall hospital costs when compared with manual staplers in laparoscopic bariatric surgery and video-assisted thoracoscopic (VATS) lobectomy in the United States.2,3 Additionally, the incorporation of gripping surface technology (GST) in Ethicon’s ECHELON FLEX™ GST system (GST) has been associated with a lower need for staple line interventions such as endoclip placement, cauterization, and oversewing, in comparison with Ethicon’s powered stapler with standard reloads, among patients undergoing laparoscopic sleeve gastrectomy.4 Similar findings have also been reported for VATS lobectomy in Korea, where GST was reported to be associated with lower hemostasis-related complications and lower overall hospital costs as compared with Ethicon’s manual staplers using reloads without GST.5
Currently, two powered stapling systems are predominantly used in clinical practice, Ethicon’s GST and Medtronic’s Signia™ Stapling System (SIG). GST, launched in 2015, has reload surfaces with proprietary pocket extensions to stabilize and hold in place tissue for the deployment of staples with uniform height. SIG, launched in 2017, combines a Medtronic powered stapler handle and other components (such as linear adapter, power shell, stapler insertion guide, manual retraction tool etc.) representing a redesign from the original Endo-GIATM iDriveTM powered stapler, while maintaining same original stapler reloads with Tri-Staple™ technology. Though both staplers deliver battery-powered deployment of the staples and the knife, each technology has adopted a different design approach in achieving similar goals of stapling and transection. Ethicon’s GST stabilizes and controls tissue movement through multi-stage compression, gripping surface technology, and surgeon-controlled power.6 In contrast, Medtronic’s SIG design promotes tissue movement through a single-stage adaptive compression at one of three pre-set device-controlled firing speeds, and a stepped cartridge surface.7,8 As such, interest exists in the potential difference in outcomes, if any, related to the utilization of these two latest powered stapling technologies. However, owing to disproportionate market penetration and limited availability of data on competing powered staplers, the majority of the evidence available on the latest stapling innovation has been related to Ethicon’s technology.
A recent study from Japan, presented a case series that showed potential benefits of lower bleeding at the vascular stump in pulmonary artery transection associated with the use of Ethicon’s ECHELON FLEX™ Powered Vascular Stapler as compared with Medtronic’s iDriveTM powered stapler.9 However, no other comparative assessment between powered staplers is available to the best of our knowledge at the time of this writing. Therefore, we conducted this retrospective study to assess the comparative real-world risk of hemostasis-related complications and other outcomes associated with the use of the powered staplers GST and SIG among patients undergoing laparoscopic sleeve gastrectomy for obesity.
Patients and Methods
Data Source
Study data were extracted from the Premier Healthcare Database® (PHD), which is a population-based hospital research database that contains administrative records routinely contributed by several hundred US hospitals that are members of the Premier healthcare performance improvement alliance, representing approximately 25% of annual US inpatient discharges.10 This database includes discharge-level information on patient demographics, diagnoses, procedures, medical supplies, costs, and hospital and provider characteristics. The PHD has been widely used for epidemiologic and economic research, forming the basis of over 600 peer-reviewed publications since 2006. This study was conducted under an exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4)). International Classification of Diseases, 10th Revision, Clinical Modification and Procedure Classification System (ICD-10-CM/ICD-10-PCS) diagnosis and procedure codes used to query the database for patient selection, measurement of outcomes, and measurement of covariates, are provided in Supplemental Appendix 1.
Patient Selection
Patients selected for the study underwent elective inpatient laparoscopic sleeve gastrectomy as a procedure intended for the treatment of obesity between March 1, 2017 (SIG launch) and December 31, 2018 (latest data available at the time the study was conducted). The first observed inpatient admission meeting these criteria was designated the “surgical admission.” Patients were also required to be at least 21 years of age as of the day of surgical admission. To avoid confounding by surgical approach, patients were excluded from the analysis if they had a procedure code indicative of robotic assistance or a hospital charge master record for a robotic supply. Patients were also excluded if they had a point of origin or admission from another institution, or had zero or negative total hospital costs, room and board, or supply costs.
Classification of Study Groups
Patients were classified as having either GST or SIG used during laparoscopic sleeve gastrectomy based on records in each hospital’s charge master, which is a comprehensive administrative record of billable procedures, equipment fees, supplies, devices, drugs, imaging services, and room and board, among other items. These records were searched for various combinations of model numbers and stapler names specific to each system. The list of charge master descriptions identified by the initial search was reviewed by two separate authors to ensure accuracy. Ultimately, two mutually exclusive groups were established: the GST group and the SIG group.
Measurement of Outcomes
This study’s primary outcome was in-hospital hemostasis-related complications, defined as a composite of either a diagnosis related to hemorrhage and/or acute hemorrhagic anemia, or a procedure code for blood product transfusion recorded during the surgical admission (see Supplemental Appendix 1 for specific diagnosis and procedure codes). As the timing of such bleeding-related events are not specifically determinable in the database, the primary endpoint captures all relevant bleeding related codes recorded intra- and post-operatively during the hospital stay. Secondary outcomes included leak, total hospital costs for the surgical admission from the hospital perspective (ie the cost of the surgical admission to the hospital – rather than charges to the payer/patient or reimbursement from the payer/patient), hospital length of stay, operating room time, and 30-, 60-, and 90-day all-cause inpatient readmission to the same hospital in which the surgical admission occurred.
As there is no specific diagnosis code for leak in the ICD-10-CM taxonomy, leak surrogate diagnoses were used following the coding conventions of Kang et al (2013) based on ICD-9-CM to ICD-10-CM forward mapping and omitting code K91.3: postprocedural intestinal obstruction.11
Total hospital costs were standardized to 2018 US Dollars based on the Medical Care component of the Consumer Price Index. In the Premier Healthcare Database, hospital costs are reported directly by the hospitals from which data are sourced in this database. Costs are determined based on each hospital’s own charge master. Analysis of operating room time was limited to patients with operating room times falling between 30 minutes and 24 hours. Analyses of all-cause hospital readmissions were limited to patients in Institutions that continued to contribute data to the Premier Healthcare Database through or beyond the readmission identification time period of interest (30, 60, or 90 days after the surgical admission).
Measurement of Covariates
Study covariates were measured using records from the surgical admission. Patient demographics included age, sex, marital status, race, payer type, and year of surgical admission. Clinical characteristics included body mass index (BMI, reported in kg/m2), the Charlson Comorbidity Index Score, and the Elixhauser comorbidity index,12,13 accounting for comorbidities including: congestive heart failure, cardiac arrhythmia, valvular disease, pulmonary circulation disorders, peripheral vascular disorders, hypertension uncomplicated, hypertension complicated, paralysis, other neurological disorders, chronic pulmonary disease, diabetes uncomplicated, diabetes complicated, hypothyroidism, renal failure, liver disease (including nonalcoholic steatohepatitis), peptic ulcer disease excluding bleeding, human immunodeficiency virus, lymphoma, metastatic cancer, solid tumor without metastasis, rheumatoid arthritis/collagen, coagulopathy, deficiency anemia, alcohol abuse, drug abuse, psychoses, and depression. Hospital/provider characteristics included urban vs rural hospital, teaching vs non-teaching hospital, hospital US Census Division, hospital bed size category, annual laparoscopic sleeve gastrectomy volume, and surgical specialty of the physician performing the procedure. No other data regarding the existence of, or details about, the bariatric program at each contributing hospital were available in the database.
Statistical Analyses
Full details on the statistical analyses are available in the Statistical Appendix. Briefly, the GST and SIG groups were matched at a 1:1 ratio to establish comparison groups that were closely matched to one another in terms of all above-mentioned patient demographics, patient clinical characteristics, and hospital/provider characteristics.14,15 After matching, univariable regression accounting for hospital-level statistical “clustering” was used to test for statistically significant differences in outcomes between the SIG and GST groups. A p-value of 0.05 was used as the threshold for statistical significance.
Sensitivity Analyses
In addition to the primary analyses, two post hoc sensitivity analyses were conducted. First, an analysis of key study findings was conducted wherein the GST and SIG groups were compared to one another within a hospital that contributed a substantive volume of cases included in both groups. This analysis was conducted as a means by which to examine whether the main study findings would be consistent when holding constant any unmeasured between-group differences driven by hospital/provider-level factors. Second, a confirmatory analysis of the primary outcome findings was conducted in the larger, pre-matching study sample using multivariable regression adjusting for all variables used for matching in the primary analyses.
Results
Patient and Hospital/Provider Characteristics
Before matching, there were 903 patients in the SIG group and 4670 in the GST group. Between-group differences were substantial for many matching covariates (Figure 1). After 1:1 matching, 491 patients from the SIG group were matched to 491 patients in the GST group, coming from a total of 40 individual hospitals. All post-match standardized mean differences were <|0.05|, indicating excellent matching covariate balance between the study comparison groups. The median patient age was 42 years and 84% were female. The three most common comorbidities were hypertension (53%), depression (24%), and chronic pulmonary disease (19%). Nearly one-third of patients had a BMI between 40 and 44.9. The majority (57%) of the procedures were performed in hospitals in the Southern region of the US. Tables 1, 2, and 3 provide additional information on post-match patient demographics, patient clinical characteristics, and hospital/provider characteristics, respectively.
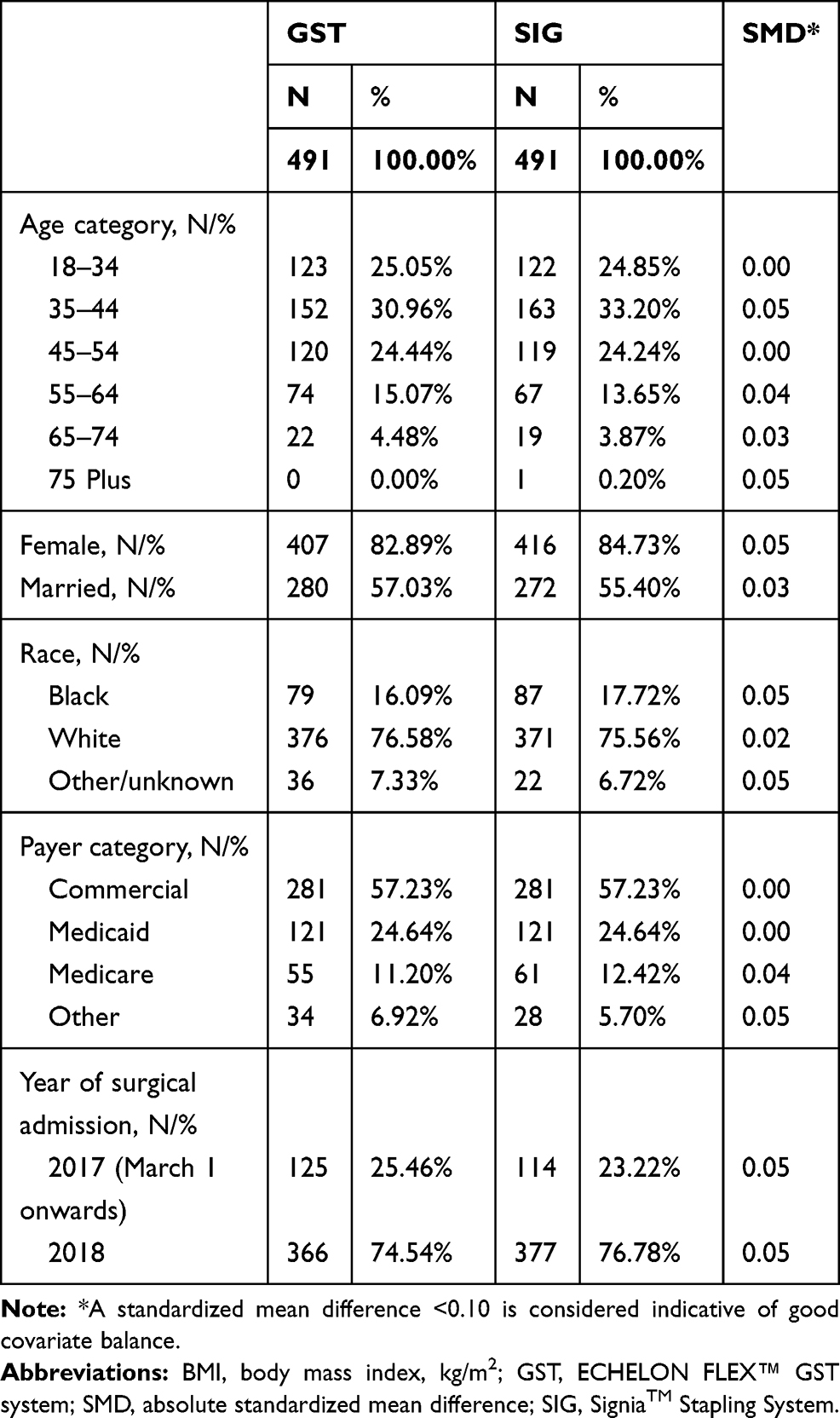 |
Table 1 Patient Demographic Characteristics After Matching |
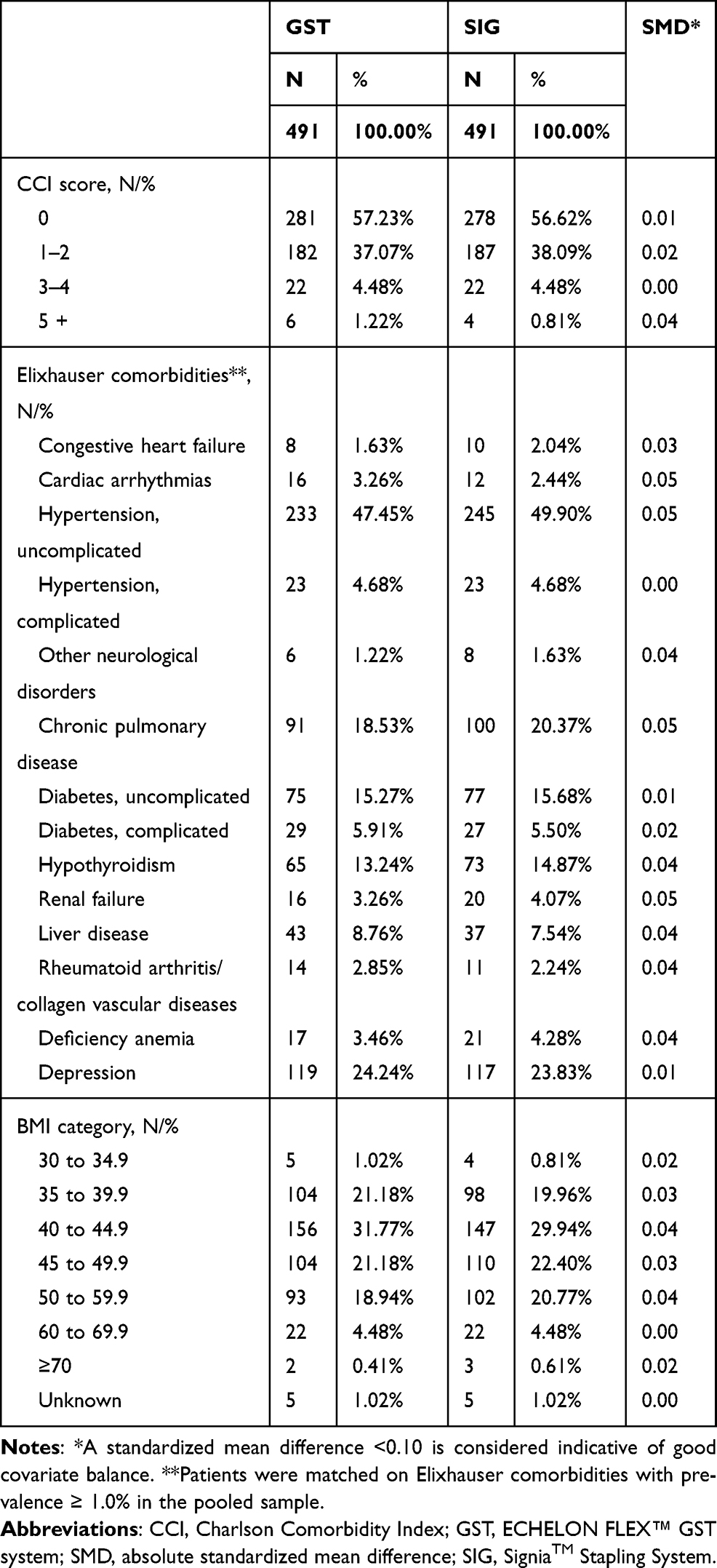 |
Table 2 Patient Clinical Characteristics After Matching |
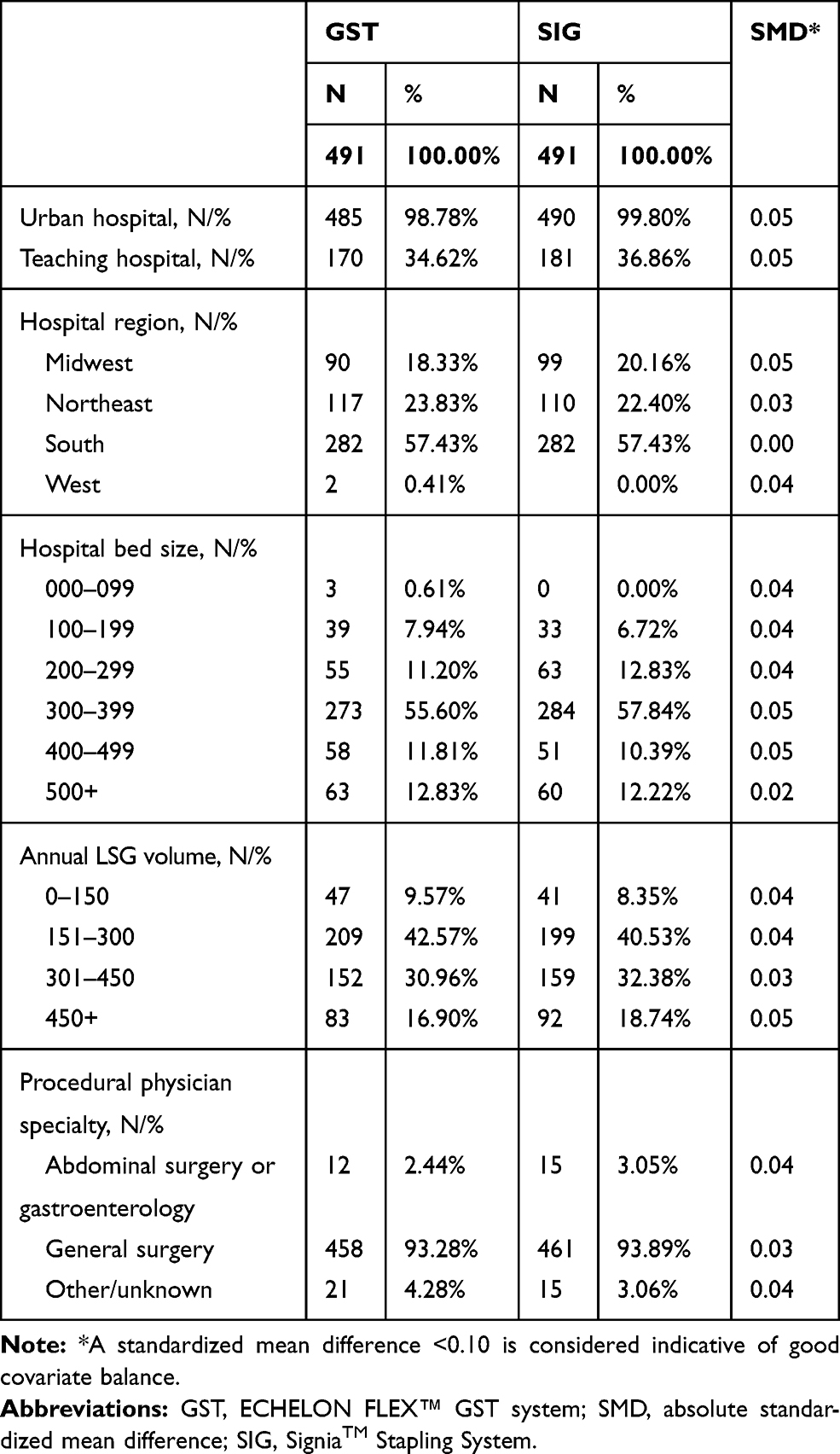 |
Table 3 Hospital/Provider Characteristics After Matching |
 |
Figure 1 Standardized mean differences before and after matching*. Note: *A standardized mean difference <0.10 is considered indicative of good covariate balance. |
Analyses of Primary Outcome
Figure 2 shows the results to the analyses of the primary outcome of in-hospital hemostasis-related complications during the surgical admission. The incidence proportion of hemostasis-related complications was lower in the GST group as compared with the SIG group: 3 patients/491 [0.61%] for GST vs 11 patients/491 [2.24%] for SIG; GEE-based odds ratio [SIG = reference]=0.28, 95% CI=0.13–0.60, P=0.0012; the risk difference between the SIG group and the GST group was 1.63% (95% CI, 0.15%-3.11%, P=0.031). This composite data includes “acute posthemorrhagic anemia” in 2 of 3 events in the GST group and 8 of 11 events in the SIG group; “postprocedural hemorrhage following digestive system procedure” (2 events in the SIG group) and “transfusion” (1 event in the GST group and 3 in the SIG group) (see Table 4).
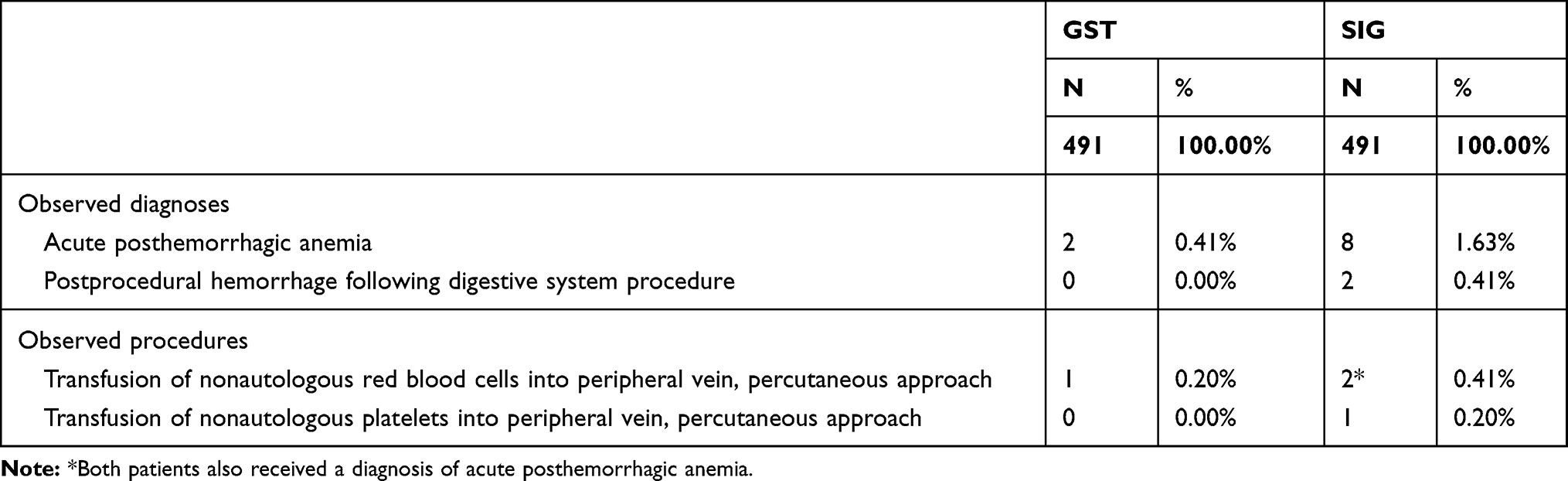 |
Table 4 Distribution of Observed Diagnoses and Procedures for Hemostasis-Related Complications During the Surgical Admission |
 |
Figure 2 Incidence proportion* of patients with hemostasis-related complications during the surgical admission after matching (primary outcome). Notes: *There were 11 patients with hemostasis-related complications in the SIG group and 3 patients with hemostasis-related complications in the GST group (see Table 4 for component diagnoses); the risk difference between the SIG group and GST group was 1.63% (95% CI, 0.15–3.11%, P=0.031); the Generalized Estimating Equations-based odds ratio (SIG = reference) accounting for hospital-level clustering via an exchangeable correlation matrix and robust standard errors was 0.28 (95% CI, 0.13–0.60, P=0.0012). Abbreviations: GST, ECHELON FLEX™ GST system; SIG, SigniaTM Stapling System. |
Analyses of Secondary Outcomes
Tables 5 and 6 show the results of the analyses of secondary outcomes. Regarding surgical admissions, the differences between the GST and SIG groups were not statistically significant for mean total hospital costs ($10,666 for GST vs $11,562 for SIG, P=0.184), mean length of stay (1.6 for GST vs 1.7 days for SIG, P=0.3624), mean operating room time (116.5 for GST vs 116.7 minutes for SIG, P=0.1219), and the incidence proportions of all-cause hospital readmissions within 30 (2.2% for GST vs 2.1% for SIG, P=0.9764), 60 (3.2% for GST vs 2.9% for SIG, P=0.7632), and 90 (3.6% for GST vs 3.2% for SIG, P=0.7968) days after discharge. No surrogate diagnoses for leak were observed in either the GST or SIG groups.
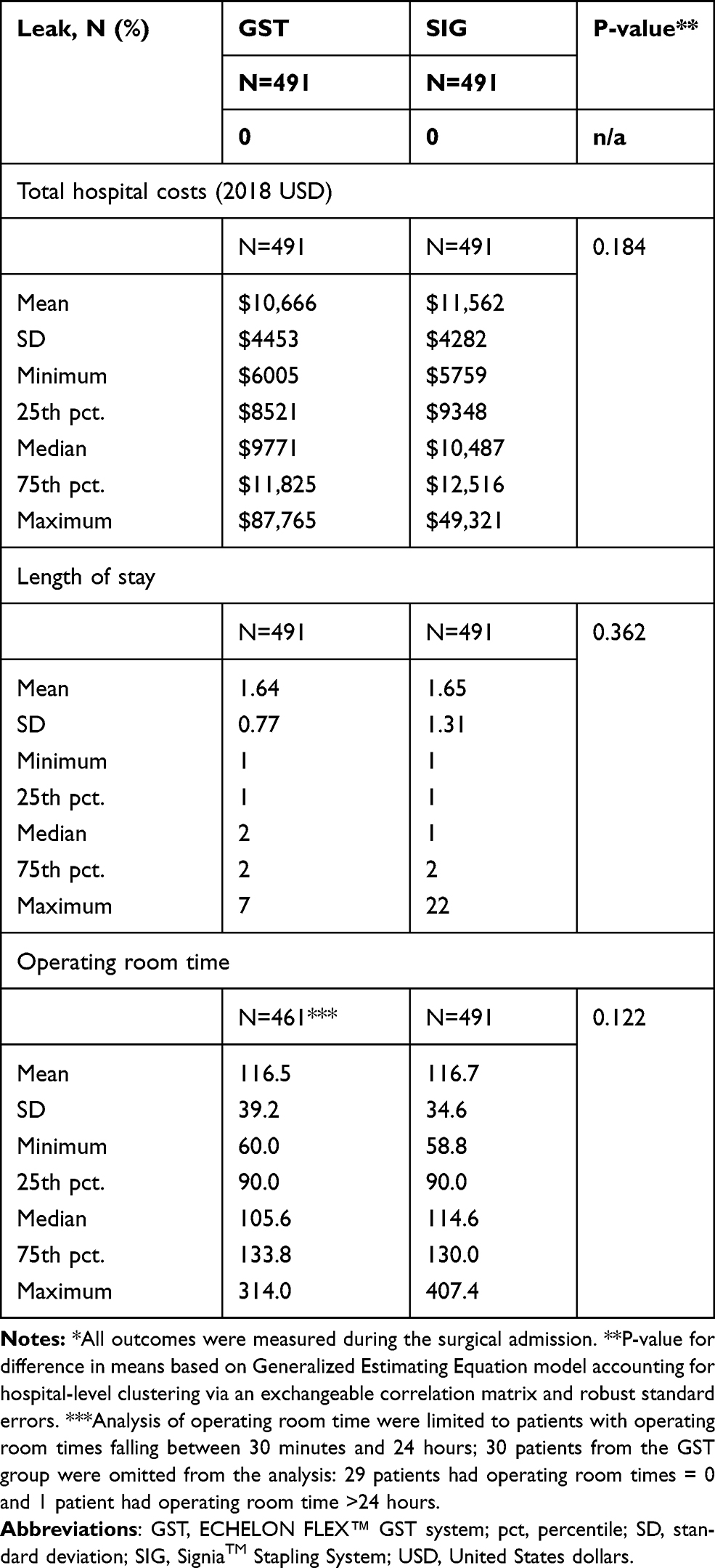 |
Table 5 Distributions of Total Hospital Costs, Length of Stay, and Operating Room Time for the Surgical Admission After Matching (Secondary Outcomes)* |
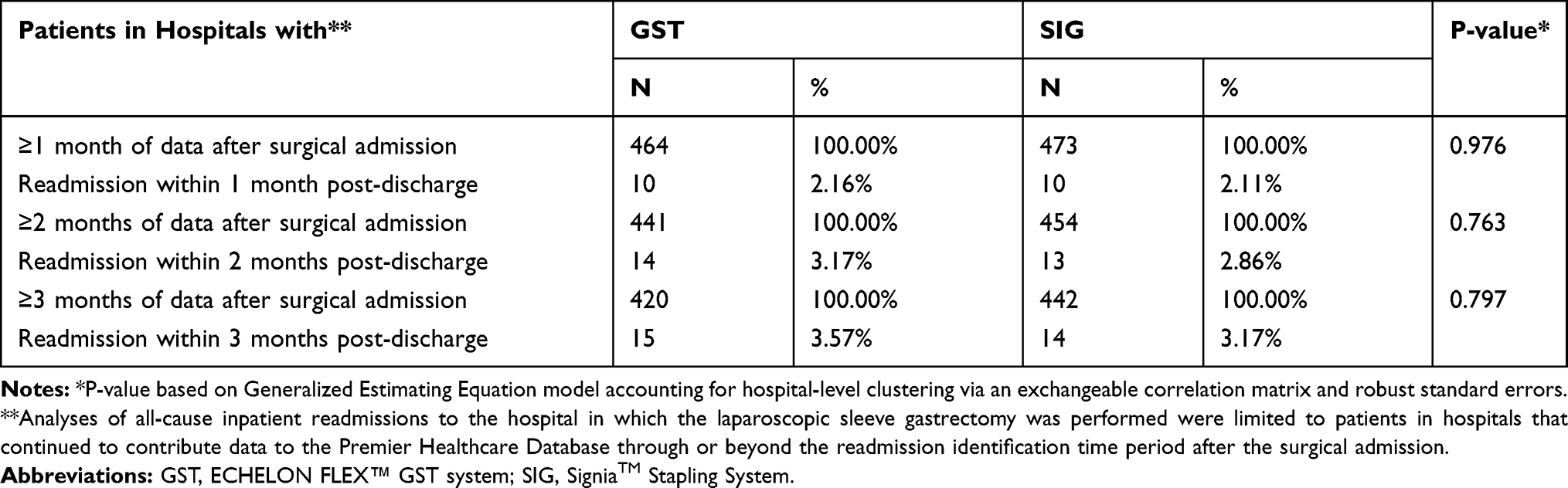 |
Table 6 Incidence Proportions of All-Cause Inpatient Readmission After Matching (Secondary Outcome) |
Sensitivity Analyses
After matching, one non-teaching urban hospital with 300–399 beds contributed a substantive volume of both the GST (N=116) and SIG (N=157); we therefore conducted a post hoc unadjusted analysis of the risk of hemostasis-related complications, total hospital costs, length of stay, and operating room time within this hospital – as a means by which to examine whether the findings would be consistent when holding constant any unmeasured between-group differences driven by hospital/provider-level factors. The trend for hemostasis-related complications was consistent with that of the primary analyses, with the incidence proportion of patients with hemostasis-related complications being 0.86% (1 patient) for GST and 2.55% (4 patients) for SIG, and mean total hospital costs, length of stay, and operating room time being not substantively different from the primary analysis within this hospital setting (total hospital costs GST: $9525 vs SIG: $11,247; LOS, GST: 1.5 days vs SIG 1.8 days; OR time. GST: 107 mins vs SIG 113 mins).
In the confirmatory analysis of the primary outcome findings, conducted in the larger pre-matching study sample (N=5573) using multivariable analyses, findings were nearly identical to the primary analyses. In the total pre-matching sample of 5573 patients, the multivariable-adjusted odds ratio of hemostasis-related complications associated with the use of GST (SIG = reference) was: 0.25, 95% CI = 0.14–0.45, P<0.0001. The multivariable-adjusted risk of hemostasis-related complications was 2.51% for SIG and 0.67% for GST, equating to a mean incremental difference of 1.84%, 95% CI = 0.62%-3.06%, P=0.003. In terms of the nature of the complications, 28/34 (82.4%) events in the GST group and 9/14 (64.3%) events in the SIG group involved diagnoses of acute posthemorrhagic anemia; 6/34 (17.6%) events in the GST group and 2/14 (14.3%) events in the SIG group involved diagnoses of postprocedural hemorrhage following digestive system procedure; 6/34 (17.6%) events in the GST group and 4/14 (28.6%) events in the SIG group were transfusion.
Discussion
To our knowledge, based on literature review, this study reports the first comparative effectiveness assessment between two leading powered stapling systems, Ethicon’s ECHELON FLEX™ GST system and Medtronic’s Signia™ Stapling System. We found that use of GST was associated with a lower risk of in-hospital hemostasis-related complications as compared with the SIG.
The lower in-hospital hemostasis-related complications associated with Ethicon’s powered staplers is consistent with previously published findings in both bariatric and thoracic procedures.2,3,5,8 However, while these earlier publications could not characterize such differences beyond the potential impact of powered firing (as they compared powered to manual stapling technologies), this analysis suggests that, potentially, there are additional differences between the stapling platforms that drive hemostasis-related complications. From an innovation perspective, although certain components of SIG are newer, the TriStapleTM cartridge reload remains the same as in Medtronic’s older manual stapling technology – potentially offering similar tissue effects as observed in the earlier studies. Although the current data lack the necessary clinical granularity to be able to ascribe causal factors to the differences between outcomes using the two study groups, the different design approach in achieving similar goals of stapling and transection may provide some initial hypotheses. Whereas GST stabilizes and controls tissue movement through a multi-stage compression, gripping surface technology, and surgeon-controlled power, SIG promotes tissue movement through a single-stage compression, a stepped cartridge and device-controlled power, thus potentially having different tissue effects intra- and postoperatively.
Among patients in the GST group, mean total hospital costs were $10,647 for patients without hemostasis-related complications and $13,691 for patients with hemostasis-related complications. This difference was more pronounced for the SIG group, with mean total hospital costs being $11,308 for patients without hemostasis-related complications and $22,623 for patients with hemostasis-related complications. There are, however, several factors such as unreported blood transfusion, return to the OR for washouts, prolonged LOS, and others that may drive the cost of managing hemostasis-related complications, many of which could not be accounted for in this analysis.
Differences between the GST and SIG groups were not statistically significant for mean total hospital costs, mean length of stay, and mean operating room time in the surgical admission, as well as all-cause patient readmission at 30, 60, and 90 days after discharge. Although the GST and SIG groups exhibited no statistically significant differences on total hospital costs for the surgical admission, there was nearly a $1000 between-group difference in the magnitude of mean total hospital costs for the surgical admissions ($10,666 for GST vs $11,562 for SIG). A difference of similar magnitude was also observed between the two groups with respect to median total hospital costs ($9771 for GST vs $10,487 for SIG). Precise explanation of the drivers of this difference would require more detailed hospital cost data. To address the potential of GEE models to introduce type 2 errors (false negatives) in the presence of unbalanced clusters, we conducted a sensitivity analysis using the Cochran-Mantel-Haenszel test – an alternative form of non-parametric cluster-adjusted statistical significance testing to test for differences in median total hospital costs between the GST and SIG groups. In this sensitivity analysis, differences in median costs between the two groups was statistically significant (p<0.001).
This study has several limitations. First, SIG has been on the market for a shorter period of time (launched in 2017) in comparison with GST (available since 2015). Consequently, the sample size available for the SIG was small before matching. Furthermore, the sample sizes for groups are not reflective of the national volume of procedures performed with these devices. During the 22-month study period, assuming the Premier Healthcare Database represented approximately 25% of all bariatric cases performed in the US, (264,000 sleeve gastrectomy cases during this period), the 5573 total powered stapling cases available for analysis represented about 2% of the available cases.16 After matching, that number dropped down to about 0.4%. As the SIG and GST groups differed substantially on many matching covariates, the post-match SIG sample size was further diminished, leading to an overall sample size of 982 patients (491 in each group) and small numbers of patients with hemostasis-related complications (3 in the GST group and 11 in the SIG group). However, in the confirmatory sensitivity analysis based on the larger, pre-matches sample of 5573 cases, the study findings were nearly identical 2.51% for SIG and 0.67% for GST, equating to a mean incremental difference of 1.84%, 95% CI = 0.62%-3.06%, P=0.003. Ultimately, there is presently no data source available that can account for a larger proportion of US bariatric surgery volume to address the present study’s research question.
Second, the identification of GST and SIG was based upon the hospital charge master, which may be subject to misclassification. However, the charge master descriptions used to identify the surgical stapler groups in the present analysis were specific and differentiated from one another and most hospitals used only either GST or SIG. In addition, ICD-10-PCS codes do not differentiate between primary vs revision sleeve gastrectomy procedures and hence could not be controlled for in the analysis; however, the selection of the first observed procedure within the database reduced the likelihood of selecting revision procedures within the study period in both study groups.
Third, the study database also restricts our ability to identify and account for several variables which might influence the risk of bleeding: 1) staple line interventions such as over-sewing or imbrication, glues, and buttress; 2) energy devices used to divide the greater curvature vessels; and 3) anticoagulants used to prevent venous thromboembolism. Staple line buttress, including the type and manner in which it is used by the surgeon has been associated with a decreased risk of bleeding in sleeve gastrectomy.17 Energy devices used to divide the great curve vessels come in many forms, such as ultrasonic and advanced bipolar, and are manufactured or reprocessed by many different companies. The standardization or control for these devices was not able to be examined in this study. Furthermore, the technique and skill level of the surgeon using the devices was not able to be assessed in the present study, which may impact proper vessel sealing. Improperly sealed vessels are at risk for rupture when the patient emerges from anesthesia or during hypertensive episodes that occur with extubation. Anticoagulant use was also not accounted for in this study. We do not know if or when anticoagulation for prevention of VTE was utilized, what drug was used and in what dose and frequency. The use of perioperative VTE prophylaxis, especially given before surgery, can affect the risk of hemostasis-related complications. Furthermore, this study is unable to fully assess the risk of bleeding from other common and known sources such as injury to the liver or spleen, mesentery, or abdominal wall. However, there is no reason to believe that such unmeasured variability is likely to differ by choice of the stapler.
Fourth, as noted in the methods section, there is no specific diagnosis code for leak in the ICD-10-CM taxonomy and therefore we used surrogate diagnoses to identify leak; however, we observed no records for such diagnoses. Future analyses based on data sources that can more accurately identify leak are needed.
Finally, as is common with all non-randomized studies, causal linkages cannot be established by the present study. Results of the present study’s sensitivity analyses demonstrate consistency of findings when holding constant any unmeasured between-group differences driven by hospital/provider-level factors, and in the larger, more variable pre-matching sample. Nevertheless, future randomized trials comparing these platforms, and/or further repeated observational studies are needed to confirm the present study’s findings. Until such data are available, the similarity in findings related to hemostasis-related outcomes associated with the use of Ethicon’s ECHELON powered staplers seen in previous observational studies appears to offer face validity to the results of the current analysis.2,3,5
Conclusion
In this retrospective study of 982 matched patients undergoing sleeve gastrectomy, the ECHELON FLEX™ GST system was associated with a lower rate of hemostasis-related complications as compared with the Signia™ Stapling System. No significant differences were observed in mean total hospital costs, length of stay, operating room time, and incidence proportions of all-cause inpatient readmission within 30, 60, and 90 days post-discharge. Further controlled prospective studies are needed to confirm the validity of this finding.
Acknowledgments
A version of the abstract of this paper was submitted to the 2020 International Society of Pharmacoeconomics and Outcomes Research conference. It was accepted as a poster presentation; however, due to the global pandemic the conference was held virtually and without poster sessions. Interim findings of the study were published in abstract form in the Conference Abstract Supplement of Value in Health: DOI:https://doi.org/10.1016/j.jval.2020.04.575
Disclosure
Logan Rawlins, Mohit Bhandari, Ricardo Cohen, and Karl Peter Rheinwalt are paid consultants for Johnson & Johnson for the purposes of professional education and training initiatives: no compensation was provided by Johnson & Johnson in relation to the present study. Dr Logan Rawlins is also consultant for Ethicon and Pacira. Stephen S Johnston, Barbara H Johnson, Raymond Fryrear, and Sanjoy Roy are employees and stockholders of Johnson & Johnson. Nivesh Elangovanraaj is employed by Mu Sigma which was paid by Johnson & Johnson to conduct statistical analyses. The authors report no other conflicts of interest in this work.
References
1. American Society for Metabolic and Bariatric Surgery. Estimate of bariatric surgery numbers; 2011–2018. Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers.
2. Miller DL, Roy S, Kassis ES, Yadalam S, Ramisetti S, Johnston SS. Impact of powered and tissue-specific endoscopic stapling technology on clinical and economic outcomes of video-assisted thoracic surgery lobectomy procedures: a retrospective, observational study. Adv Ther. 2018;35(5):707–723. doi:10.1007/s12325-018-0679-z
3. Roy S, Yoo A, Yadalam S, Fegelman EJ, Kalsekar I, Johnston SS. Comparison of economic and clinical outcomes between patients undergoing laparoscopic bariatric surgery with powered versus manual endoscopic surgical staplers. J Med Econ. 2017;20(4):423–433. doi:10.1080/13696998.2017.1296453.
4. Fegelman E, Knippenberg S, Schwiers M, et al. Evaluation of a powered stapler system with gripping surface technology on surgical interventions required during laparoscopic sleeve gastrectomy. J Laparoendosc Adv S. 2016;27(5):489–494. doi:10.1089/lap.2016.0513
5. Park SY, Kim DJ, Nam CM, et al. Clinical and economic benefits associated with the use of powered and tissue-specific endoscopic staplers among the patients undergoing thoracoscopic lobectomy for lung cancer. J Med Econ. 2019;22(12):1274–1280. doi:10.1080/13696998.2019.1634081
6. Ethicon website. Available from: https://www.jnjmedicaldevices.com/sites/default/files/user_uploaded_assets/pdf_assets/2019-08/ECHELON-FLEX-GST-System-Brochure-066368-170821_0.pdf. Accessed: March 6 2020.
7. Medtronic website. Available from: https://www.medtronic.com/covidien/en-us/products/surgical-stapling/signia-stapling-system.html. Accessed: March 6 2020.
8. Medtronic website. Available from: https://www.medtronic.com/covidien/en-us/products/surgical-stapling/tri-staple-technology.html. Accessed: March 6 2020.
9. Tsunezuka Y, Tanaka N, Fujimori H. The impact of endoscopic stapler selection on bleeding at the vascular stump in pulmonary artery transection. Med Devices (Auckl). 2020;13:41–47. doi:10.2147/MDER.S240343
10. Premier Applied Sciences®, Premier Inc. Premier healthcare database white paper: data that informs and performs. November 4, 2019. Available from: https://learn.premierinc.com/white-papers/premier-healthcaredatabase-whitepaper.
11. Kang CY, Halabi WJ, Chaudhry OO, et al. Risk factors for anastomotic leakage after anterior resection for rectal cancer. JAMA Surg. 2013;148(1):65–71. doi:10.1001/2013.jamasurg.2
12. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. doi:10.1016/0895-4356(92)90133-8
13. Agency for Healthcare Research and Quality. Elixhauser Comorbidity Software for ICD-10-CM (Beta Version) Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality; November 2018. Available from: www.hcup-us.ahrq.gov/toolssoftware/comorbidityicd10/comorbidity_icd10.jsp.
14. Zubizarreta JR, Paredes RD, Rosenbaum PR. Matching for balance, pairing for heterogeneity in an observational study of the effectiveness of for-profit and not-for-profit high schools in Chile. Ann Appl Stat. 2014;8(1):204–231. doi:10.1214/13-AOAS713
15. Visconti G, Zubizarreta JR. Handling limited overlap in observational studies with cardinality matching. Observational Studies. 2018;4:217–249.
16. Website of the the American Society for Metabolic and Bariatric Surgery (ASMBS). Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers. Accessed March 2020.
17. Zafar SN, Felton J, Miller K, Wise ES, Kligman M. Staple Line Treatment and Bleeding After Laparoscopic Sleeve Gastrectomy. JSLS. 2018;22(4):
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.