Back to Journals » International Journal of Women's Health » Volume 17
Comparative Analysis Perinatal Complications Among Women with ART-Induced Pregnancy and Natural Conception
Authors Chai H, Ma R, Cheng F, Chen D, Zhang Y
Received 14 June 2025
Accepted for publication 9 December 2025
Published 30 December 2025 Volume 2025:17 Pages 5733—5746
DOI https://doi.org/10.2147/IJWH.S547161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Hongxia Chai,1 Ruiting Ma,2 Feifei Cheng,2 Dandan Chen,2 Yan Zhang3
1Department of Obstetrics, the First Hospital of Lanzhou University, Lanzhou, People’s Republic of China; 2The 1st School of Clinical Medicine, Lanzhou University, Lanzhou, People’s Republic of China; 3Department of Obstetrics, West Station Branch of the First Hospital of Lanzhou University, Lanzhou, People’s Republic of China
Correspondence: Yan Zhang, Department of Obstetrics, West Station Branch of the First Hospital of Lanzhou University, No. 1 Donggang West Road, Lanzhou, 730099, People’s Republic of China, Tel +86-13919374552, Email [email protected]
Objective: This study conducted a retrospective matched analysis to explore the differences and potential associations in perinatal complications between pregnancies achieved through in-vitro fertilization-embryo transfer (IVF-ET) and natural conception.
Methods: A total of 806 pregnant women who delivered at the Department of Obstetrics, First Hospital of Lanzhou University, China, from January 2019 to August 2024 were included, with 403 cases in the experimental group and 403 matched controls (natural conception) based on admission month and gestational age (± 7 days).
Results: Analysis revealed that the experimental group exhibited significantly higher incidences of multiple gestations, anemia, postpartum hemorrhage, gestational hypertension, gestational diabetes mellitus, and intrahepatic cholestasis of pregnancy compared to the control group. In singleton pregnancy analysis, these differences persisted except for pelvic inflammation. The findings suggest that ART pregnancies may increase perinatal risks through factors such as embryo manipulation, hormonal interventions, and underlying maternal pathologies.
Conclusion: This matched retrospective study highlights that IVF-ET pregnancies are associated with significantly higher risks of multiple gestations and obstetric complications, independent of multifetal pregnancies. The findings underscore the necessity of optimizing embryo transfer strategies, such as promoting single embryo transfer and implementing enhanced monitoring protocols for high-risk complications in resource-limited settings like Northwest China. This study provides regional evidence to support the development of tailored ART guidelines.
Keywords: in-vitro fertilization-embryo transfer, perinatal complications, retrospective matched study, multiple gestations
Introduction
Infertility (defined as the inability to conceive after 1 year of unprotected intercourse) affects 10–15% of reproductive-aged women globally, with etiologies including ovulatory dysfunction, endometriosis, and tubal pathologies.1–3 While assisted reproductive technologies (ART), such as in-vitro fertilization-embryo transfer (IVF-ET), have significantly improved pregnancy rates, their long-term impacts on maternal and fetal health remain debated.4,5 Existing studies suggest that ART pregnancies may elevate risks of multiple gestations, gestational hypertension, and postpartum hemorrhage. However, controversy persists over whether these risks stem from ART procedures themselves, underlying maternal infertility-related pathologies, or confounding factors like multifetal pregnancies.5 Notably, prior research often lacked rigorous matching of baseline characteristics or differentiation between singleton and multiple pregnancies, leading to heterogeneous conclusions.
With the rapid development of ART and the increasing number of ART pregnancies, the safety of this technology and its impact on both maternal and fetal health have garnered heightened scholarly interest.4,5 Certain inquiries indicate that ART is associated with a myriad of pregnancy complications.4,6 Several studies have demonstrated that ART pregnancies are associated with an elevated risk of perinatal complications, encompassing instances of multiple gestations, gestational diabetes, pregnancy-induced hypertension, anemia, postpartum hemorrhage, intrahepatic cholestasis, thyroid pathologies, as well as an increased incidence of cesarean delivery.4–7 However, some academics are of the opinion that the utilization of ART does not elevate the likelihood of unfavorable perinatal outcomes in pregnancy.8 The pathophysiological mechanisms underlying ART-associated complications are multifactorial. Ovarian hyperstimulation leads to supraphysiological estrogen levels, which can impair endothelial function and promote systemic inflammation. In-vitro embryo culture may induce epigenetic alterations affecting placental development and function. Furthermore, underlying maternal conditions such as endometriosis or tubal factor infertility often involve chronic inflammatory states that may synergize with ART procedures to exacerbate adverse outcomes.4–7
Furthermore, due to the significant role that multiple pregnancies play in precipitating perinatal complications, the outcomes of ART pregnancies are typically suboptimal.4,5,9,10 The ambiguity persists regarding whether the augmented risk of adverse pregnancy outcomes is attributable to the ART, the procedural aspects, multifetal gestations, or the patient’s intrinsic infertility issues.5
Similar studies have been conducted internationally, though regional variations in ART practices and patient demographics may influence outcomes.5 Recent meta-analyses and large-scale cohort studies from Europe and North America have consistently reported elevated risks of obstetric complications in ART pregnancies, including preeclampsia, preterm birth, and gestational diabetes. However, most evidence derives from high-resource settings, and data from low- and middle-income regions like Northwest China remain scarce. This study contributes to the global literature by providing region-specific evidence from a matched cohort, thereby enhancing the generalizability and contextual relevance of ART safety assessments.6–10
Northwest China is characterized by relatively limited healthcare resources and lower accessibility to advanced ART technologies compared to eastern regions. Cultural preferences for multiple births and economic constraints often lead to higher rates of double embryo transfers, exacerbating the risk of multiple gestations and related complications. These regional specificities underscore the urgency of developing context-sensitive ART guidelines.
This study aims to systematically compare perinatal complications between IVF-ET and natural conception through a matched retrospective design, controlling for confounders such as admission timing, gestational age, and singleton pregnancies. Its specific objectives include: (1) assessing the incidence of multiple gestations and obstetric complications; (2) evaluating singleton pregnancies to isolate ART-specific risks; and (3) providing evidence for optimized ART protocols. Its clinical implications include: (1) providing evidence for risk stratification of ART to guide individualized embryo transfer strategies, such as single embryo transfer; (2) optimizing pregnancy management for infertile women through targeted monitoring of high-risk complications; and (3) elucidating the synergistic mechanisms between maternal infertility-related pathologies and ART interventions. Compared to previous studies, the innovation lies in: (1) a 1:1 strict matching design to minimize confounding bias; (2) the first large-scale stratified analysis from a single center in Northwest China, addressing regional evidence gaps; and (3) independent analysis of singleton pregnancy data to clarify ART-associated risks independent of multifetal gestations.
Methods
Matched Strategy
A retrospective analysis was performed on pregnant patients who were hospitalized and gave birth in the Department of Obstetrics, the First Hospital of Lanzhou University, Gansu Province from January 2019 to August 2024. A total of 846 cases were included in this study, excluding those with incomplete investigation data and those with mismatched matching criteria, and 806 pregnant patients were eligible. The study group consisted of 403 pregnant patients with IVF-ET assisted pregnancies. In the one-by-one matched control group, a total of 403 pregnant patients who conceived naturally were selected based on the admission month and gestational age (±7 days) of each corresponding case in the experimental group. All clinical data and details of pregnancy and delivery pertaining to both experimental group and matched control group were obtained from the hospital’s medical record information system (Figure 1).
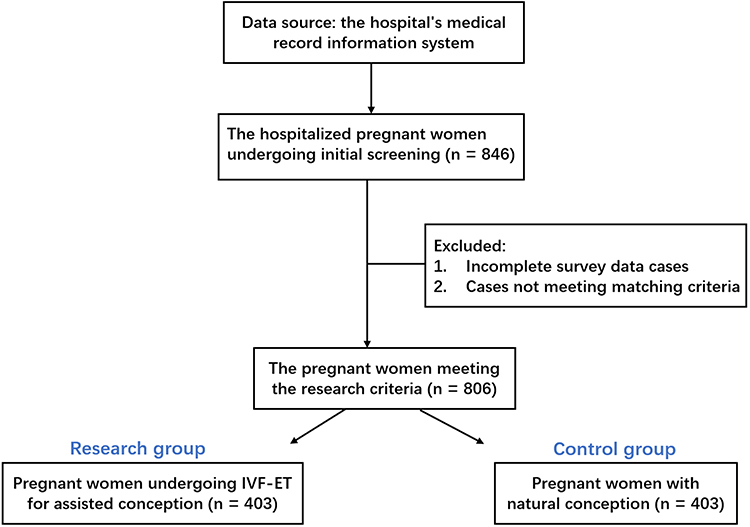 |
Figure 1 Flowchart. |
The following information of the patient were collected through medical record review or structured questionnaires:
Basic characteristics of the patient: age, BMI, social history (smoking, alcohol consumption), educational level, economic status.
Medical history: 1) Gynaecological history: Causes of infertility (such as ovulation disorders, fallopian tube lesions), staging of endometriosis, previous pregnancy complications (such as history of miscarriage); 2) Chronic diseases: hypertension, diabetes.
IVF treatment-related factors: The number of IVF-ET cycles, ovulation induction protocols (such as long protocol/antagonist protocol), medication use during pregnancy, the type of embryos transferred (fresh/frozen), and the number of embryos transferred.
Relevant Definitions
IVF-ET
The full name of in-vitro insemination - embryo transfer, is the whole process of removing eggs from the ovaries artificially, fertilizing them with sperm in-vitro and cultivating them for 3–5 days, and then transferring the embryos into the woman’s uterine cavity for implantation and development into a fetus. IVF-ET includes derivative techniques such as in-vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), preimplantation genetic diagnosis (PGD), and vitrification (GVT).4
Intrahepatic cholestasis of pregnancy (ICP) was diagnosed based on pruritus combined with elevated fasting serum total bile acids (TBA ≥ 10 μmol/L) and/or elevated liver transaminases (ALT > 40 U/L), with resolution postpartum.
Thyroid dysfunction was defined as thyroid-stimulating hormone (TSH) levels outside the pregnancy-specific reference range (first trimester: 0.1–2.5 mIU/L; second trimester: 0.2–3.0 mIU/L; third trimester: 0.3–3.0 mIU/L) or the presence of thyroid peroxidase antibodies (TPOAb > 34 IU/mL).
Delivery refers to the process of pregnancy reaching and exceeding 28 weeks (196 days), from the beginning of labor to the full delivery of the fetus and appendages from the mother. Pregnancy up to 28 weeks and less than 37 weeks (196–258 days) delivery is called preterm delivery; Pregnancy up to 37 weeks but less than 42 weeks (259–293 days) followed by delivery (259–293 days) delivery is called full term; A pregnancy of 42 weeks or more (≥294 days) is considered overdue.
Calculation of gestational age: In experimental group, the birth gestational age was calculated on the day of egg retrieval plus 14 days, and in the matched control group, on the first day of the last menstrual period.5
Variable Collection
The general characteristics we collected included maternal age, ethnicity, antecedent medical conditions as well as endoscopic surgery history. Furthermore, variables pertaining to obstetricians encompassed the parity, number of fetuses, the method of childbirth, the gestational age and the Apgar score. The occurrence of pregnancy and perinatal complications, including abnormal umbilical cord, anemia/postpartum hemorrhage, premature birth, hypertensive disorders of pregnancy, gestational diabetes, fetal distress, adnexal or pelvic inflammation, intrahepatic cholestasis of pregnancy, and perineal laceration.
Apgar score, proposed by Dr. Virginia Apgar in 1953, is a simple and practical preliminary screening index for rapid assessment of the general condition of newborns after birth. The content includes appearance, pulse, grimace, activity and respiration. 2 points for each item can be awarded a score value of 0, 1 or 2 for a total of 10 points. Scores were performed at 1min, 5min and 10min after birth, and Apgar score was 8–10 as normal, 4–7 as mild asphyxia, and 0–3 as severe asphyxia.11
Data were extracted from electronic medical records by two trained, independent researchers using a standardized data collection form, with both researchers blinded to group allocation (IVF-ET vs natural conception). Inter-rater reliability was assessed on a random 10% sample of the records, with a Cohen’s kappa coefficient of >0.85 for categorical variables and an intraclass correlation coefficient (ICC) >0.90 for continuous variables—indicating excellent agreement. Additionally, this 10% random sample was independently verified by a senior obstetrician to further ensure accuracy and consistency. Any discrepancies identified during the data extraction or verification process were resolved through consensus or adjudication by the senior obstetrician.
Statistical Analysis
The sample size was calculated a priori based on the difference in the incidence of postpartum hemorrhage reported in previous literature, setting α=0.05 (two-sided) and β=0.20 (power=80%), which yielded a minimum requirement of 368 cases per group. Accounting for an estimated 10% rate of loss to follow-up or missing data, a total of 405 matched pairs were initially targeted, with 403 pairs ultimately included in the final analysis. All statistical analyses were performed using SPSS (version 26.0; IBM Corp, Armonk, NY, USA) and R software (version 4.2.1). Continuous variables (eg, maternal age, gestational age) were presented as mean ± standard deviation and compared using independent samples t-tests or Mann–Whitney U-tests, as appropriate, with effect sizes reported as mean differences and 95% confidence intervals (CIs). Categorical variables (eg, mode of delivery, complication incidence) were summarized as frequencies (percentages) and compared using the Chi-square test or Fisher’s exact test, with results also presented as odds ratios (ORs) or adjusted ORs (aORs) with 95% CIs where applicable. Multivariable logistic regression models were employed to adjust for potential confounders, including maternal age, BMI, parity, and smoking history, which were selected based on clinical relevance and univariate screening (P < 0.10). Model diagnostics included assessment of multicollinearity via variance inflation factors (VIF < 5), evaluation of linearity for continuous covariates using residual plots, and testing for interaction terms (eg, maternal age × ART) via likelihood-ratio tests (inclusion threshold P < 0.05). Missing data were handled strategically: variables with <5% missing rates were analyzed using complete-case analysis; those with 5–20% missing data were imputed via multiple imputation by chained equations (MICE, generating five datasets), with pooled estimates derived using Rubin’s rules; and variables exceeding 20% missingness were excluded from multivariable modeling.
Results
Integral Analysis
The study collected information on 423 pregnant women who matching criteria, and after excluding data on miscarriage, ectopic pregnancy and other factors that deviated from the experimental criteria, a total of 403 matching data were obtained. Baseline characteristics of the study participants are summarized in Table 1. The two groups were well-matched in terms of maternal age (mean difference 0.20 years, 95% CI: −0.52 to 0.92; P=0.58) and anthropometric measures, including weight at delivery (mean difference 0.50 kg, 95% CI: −0.73 to 1.73; P=0.42) and BMI (mean difference 0.30 kg/m2, 95% CI: −0.17 to 0.77; P=0.21). However, significant differences were observed in obstetric history, with the ART group having a higher proportion of nulliparous women (88.8% vs 64.0%, P<0.001), fewer previous pregnancies, and more frequent abnormal pregnancy history (38.7% vs 22.1%, P<0.001). Additionally, women in the ART group were more likely to have a history of endoscopic surgery (30.5% vs 9.2%, P<0.001) and to deliver via cesarean section (74.2% vs 43.9%, P<0.001). The participants involved in this study exhibited an age distribution ranging from 22 to 46 years. Regression adjustments were made for the variables that were not completely matched (such as BMI and smoking history) to reduce residual confounding and to ensure that the comparability between groups was improved through multivariate analysis during matching (Table 2). Any discrepancy in age between the two groups was not statistically significant, nor was there a pronounced distinction in terms of ethnicity. The data indicated that the experimental group demonstrated a higher incidence of prior endoscopic surgical interventions and a greater propensity towards being primiparous. In addition, the experimental group showed a higher prevalence of prior adverse pregnancy outcomes compared to the control group. The cesarean section rate was significantly higher in the ART group (74.2%, 299/403) than in the natural conception group (43.9%, 177/403; χ2 = 45.6, P < 0.001), reflecting a strong inclination toward surgical delivery in the ART cohort, whereas the natural conception group predominantly underwent vaginal delivery.
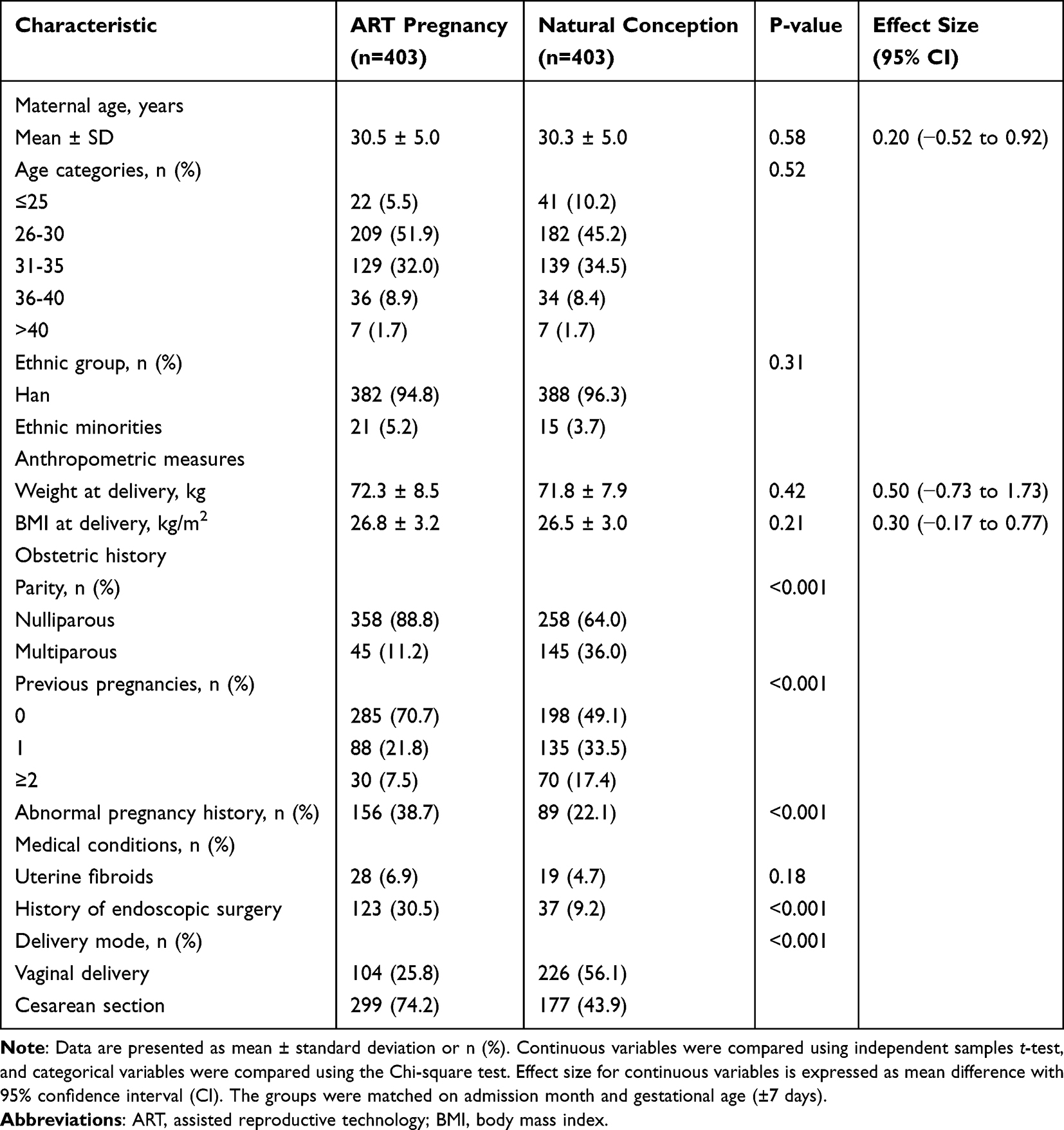 |
Table 1 Baseline Characteristics of the Study Participants |
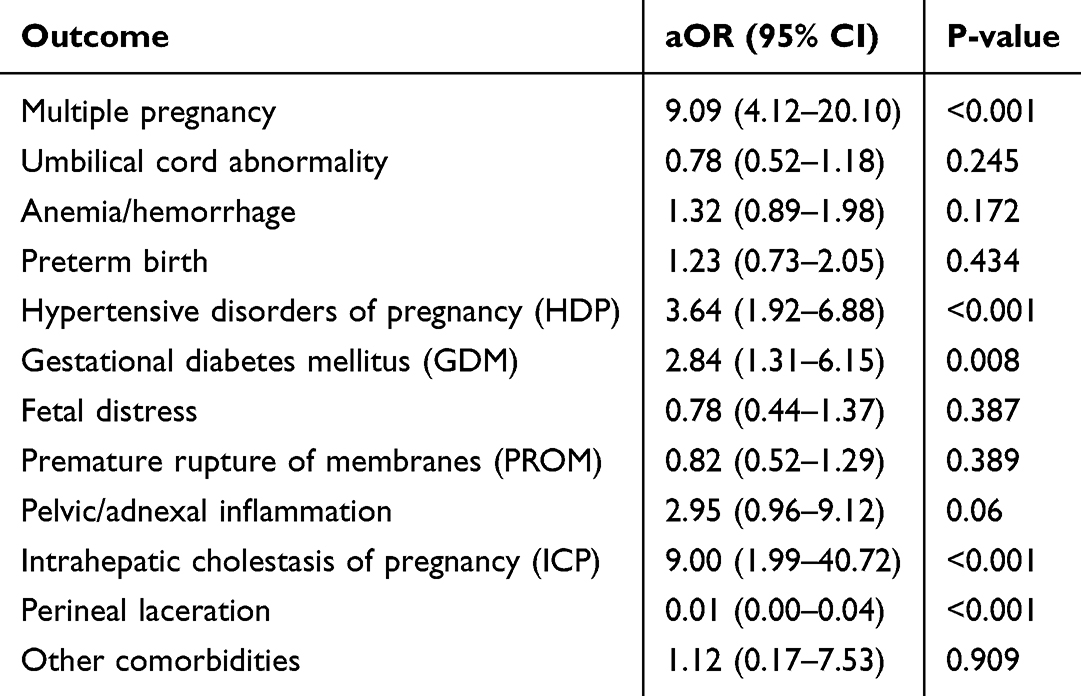 |
Table 2 Multivariable Logistic Regression: Adjusted Odds Ratios (aOR) for ART |
As summarized in Table 3, the ART pregnancies were associated with a significantly elevated incidence of multiple gestations (24.3% vs 3.2%; χ2 = 85.4, P < 0.001). Similarly, anemia or postpartum hemorrhage was more common in the ART group (18.6% vs 8.9%; χ2 = 15.2, P < 0.001). The risks of gestational hypertension (12.4% vs 5.7%; χ2 = 10.5, P = 0.001), gestational diabetes mellitus (15.1% vs 8.2%; χ2 = 7.8, P = 0.005), and intrahepatic cholestasis of pregnancy (7.2% vs 2.5%; χ2 = 9.4, P = 0.002) were also significantly higher in the experimental group. Conversely, no statistically significant differences were observed between the two groups in the incidence of abnormal umbilical cord, premature delivery, fetal distress, or premature rupture of membranes (all P > 0.05). Notably, the rate of perineal laceration was markedly lower in the ART group (0.2% vs 9.4%; χ2 = 35.2, P < 0.001).
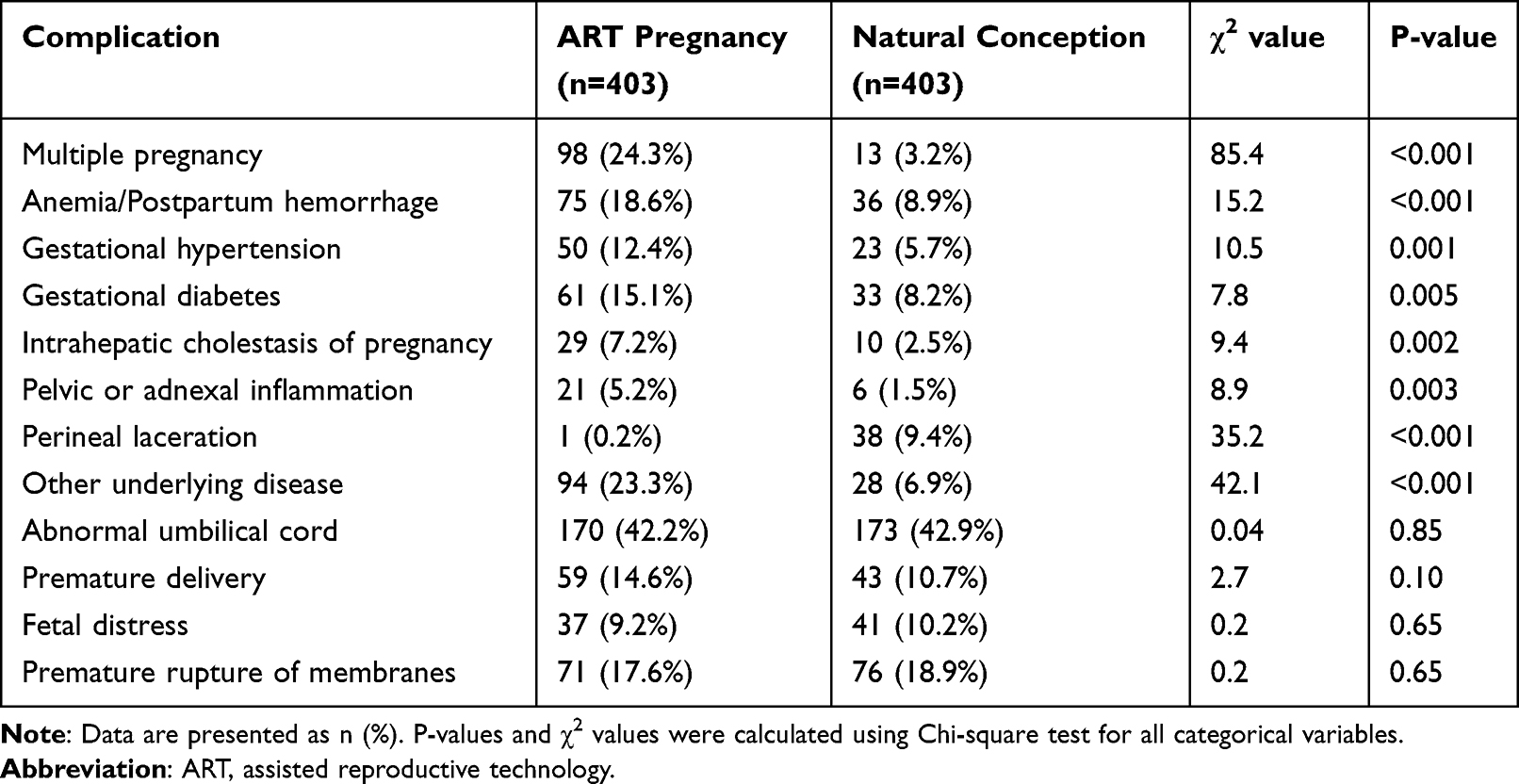 |
Table 3 Comparison of Perinatal Complications Between ART and Natural Conception Pregnancies |
To mitigate the impact of multiple births on specific complications, we meticulously filtered the dataset to include only singleton pregnancies that had been successfully paired. The characteristics of these participants are delineated in Table 4. The analytical findings indicated that, apart from pelvic and adnexal inflammation, the aforementioned disparities still persisted. However, when compared with the outcomes of multiple pregnancies, the assisted reproductive technology (ART) cohort of singleton pregnancies exhibited a more pronounced impact on the incidence of gestational diabetes mellitus and perineal lacerations.
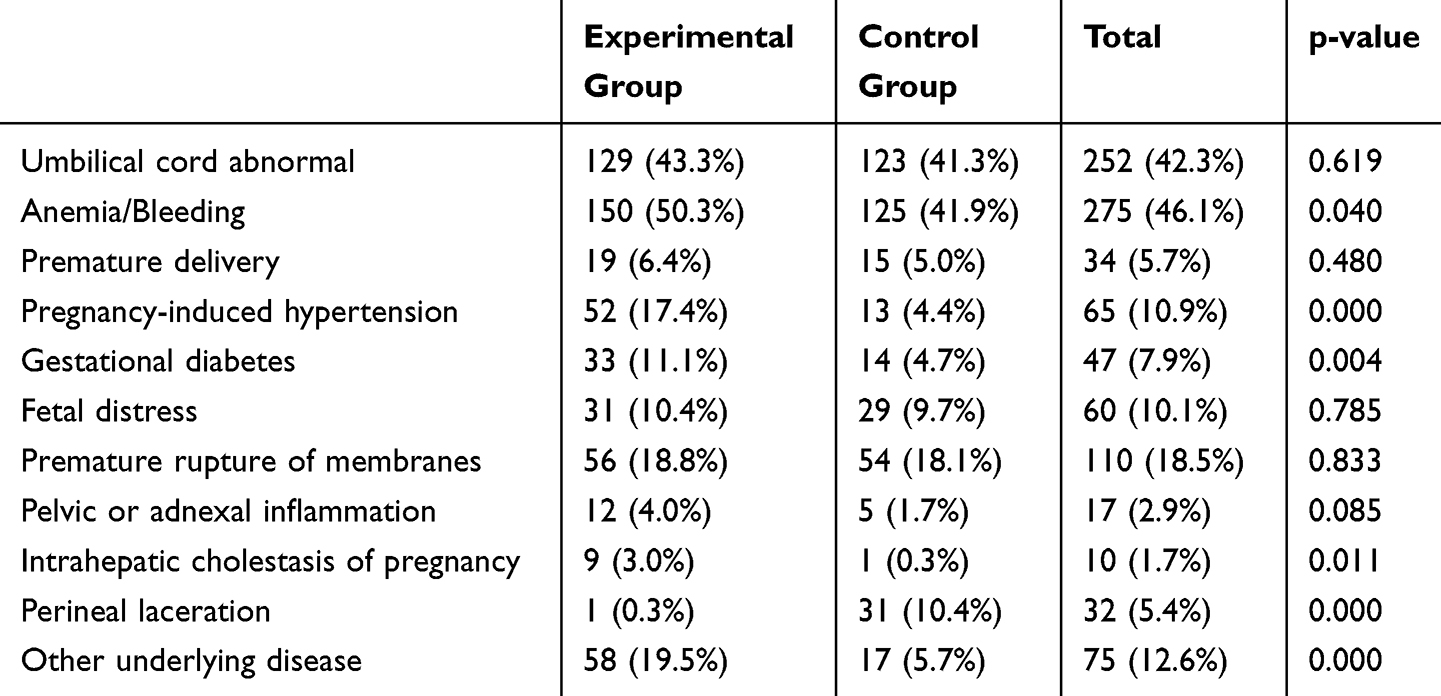 |
Table 4 The Characteristics of Singleton Pregnancy |
Subgroup Analyses
To enhance the granularity of our findings, subgroup analyses were conducted across three critical dimensions: maternal age, infertility etiology, and embryo type. Participants were stratified into four age cohorts (≤25, 26–30, 31–35, and >35 years) to evaluate age-dependent variations in ART-associated complications. As detailed in Table 5, the risks of multiple pregnancy, gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), and preterm birth generally exhibited an increasing trend with advancing maternal age in the ART group. For instance, the risk of GDM was significantly elevated in the >35 years cohort (aOR 2.55, 95% CI 1.80–3.62, P < 0.001), whereas no significant association was observed in the ≤25 years group (aOR 1.20, 95% CI 0.45–3.22, P = 0.716). Conversely, the protective effect of ART on perineal lacerations was most pronounced in the 26–30 and 31–35 years groups. Furthermore, specific complications such as intrahepatic cholestasis of pregnancy and anemia/postpartum hemorrhage showed elevated risks across multiple age strata, particularly in older women. These stratified insights underscore the heterogeneity of ART-related risks and emphasize the necessity of age-personalized clinical counseling and protocol optimization.
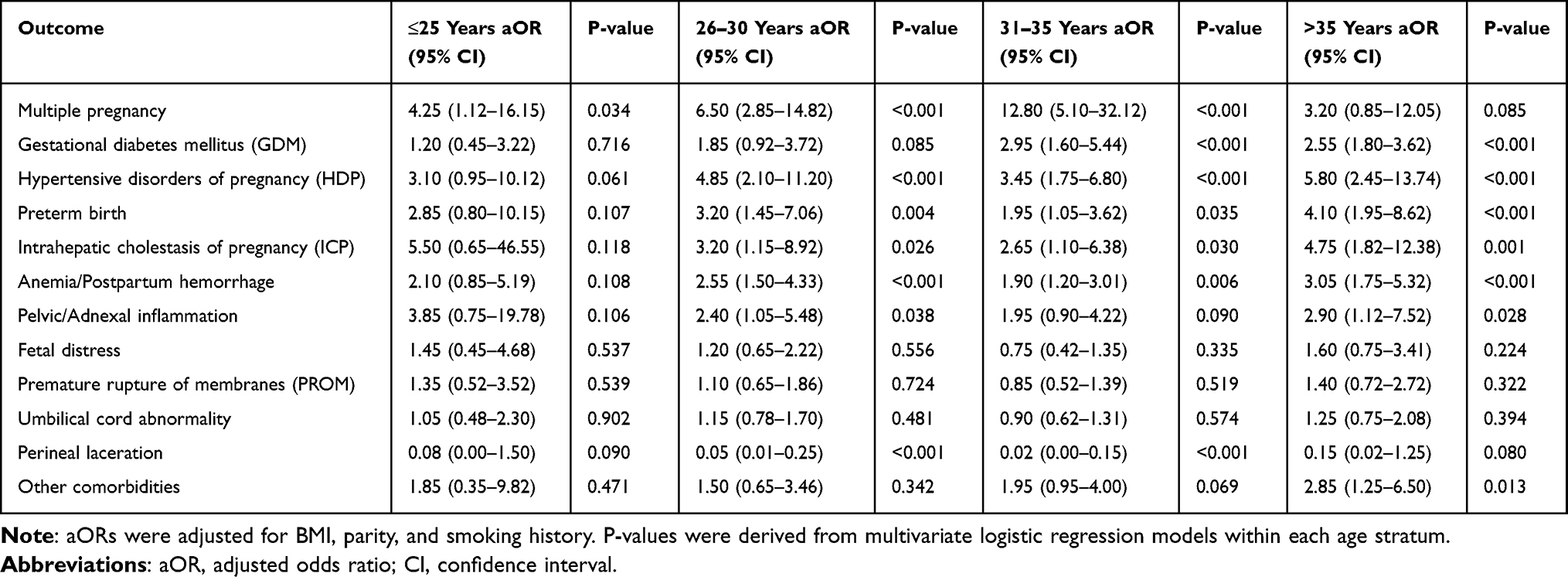 |
Table 5 Stratified Analysis: Adjusted Odds Ratios (aOR) of ART-Associated Perinatal Complications by Maternal Age Group |
Discussion
The purpose of this study was to compare the differences in the incidence of perinatal complications between ART and natural conception groups to further investigate the effects of ART on perinatal complications. According to our search of the relevant literature, although there exist many articles investigating ART and pregnancy complications, there are few matched studies on this topic. For the purpose of this study, a control group was selected and matched for hospital admission date and gestational age within a 7-day window, to mitigate uncertainty as well as error caused by random matching. Analytical findings suggested that the experimental group exhibited an elevated risk of multiple gestations, anemia and post-pregnancy hemorrhaging, pregnancy-induced hypertension, gestational diabetes, pelvic or accessory inflammation, intrahepatic cholestasis of pregnancy, as well as other comorbidities, predominantly thyroid disorders, which was largely consistent with previous studies.4,6,12 In addition, some studies have demonstrated that multiple births significantly contribute to the incidence of gynecological and obstetric complications during gestation.4,10,12 Consequently, we screened the singleton pregnancies data of successful pairs, and the subsequent analysis confirmed that the aforementioned discrepancies, apart from pelvic and adnexal inflammation, still persisted.
Multiple Pregnancy
Assisted Reproductive Technology (ART) is exerting an increasing profound influence on fertility patterns in China.6 It includes all the treatments available to help infertile patients conceive, including but not limited to artificial insemination (AI), in-vitro fertilization-embryo transfer (IVF-ET), intracytoplasmic sperm injection (ICSI), and gamete intrafallopian transfer (GIFT), among others.9,11 In this study, the experimental group consisted of women who underwent IVF-ET. To enhance the success rate of conception, two embryos were implanted into these women at the time of conception. Consequently, the incidence of twin and multiple gestations in ART-related pregnancies significantly exceeds that observed in natural group. The elevated incidence of multiple gestations in ART pregnancies is primarily attributed to the transfer of multiple embryos to improve success rates. However, this practice disrupts natural singleton implantation dynamics, leading to placental crowding, vascular competition, and uteroplacental insufficiency. These factors collectively heighten risks of preterm birth, fetal growth restriction, and maternal hypertensive disorders. Nonetheless, as the fetus progresses in its development, certain embryos may be aborted, resulting in singleton pregnancies. As previously discussed, multiple births are associated with a higher incidence of perinatal complications.4,12,13 Consequently, it is widely acknowledged that contemporary clinical guidelines advocate transferring as few embryos as possible or performing single embryo transfers and impose stricter criteria for multiple embryo transfers.14 This is also the future trend of ART embryo transfer in China.
Postpartum Hemorrhage
Postpartum hemorrhage ranks among the prevalent complications associated with pregnancy and constitutes a predominant factor contributing to maternal mortality.15 The dataset we have analyzed indicates a propensity for an elevated incidence of postpartum hemorrhage in females who have undergone Assisted Reproductive Techniques (ART), which is consistent with some previous studies.4 Nyffot Lt et al noted an increased risk of severe postpartum hemorrhage among women who achieved conception via ART through a case-control study.16
Previous studies have demonstrated that Assisted Reproductive Techniques (ART) have the potential to disrupt the development of the maternal-fetal interface and compromise the integrity of the placenta.17 Furthermore, Romundstad LB et al have documented a significantly elevated incidence of placental previa in pregnancies resulting from ART, as compared to those conceived spontaneously.17 These aberrations in placental structure are identified as definitive risk factors for postpartum hemorrhage.18 This could represent one of the mechanisms underlying postpartum hemorrhage associated with assisted reproductive technologies (ART). Moreover, conditions associated with infertility, such as endometriosis, adenomyosis, and uterine fibroids, are recognized as contributory elements to the risk of postpartum bleeding.19,20 Women who experienced infertility and had gone through ART may seek medical intervention exactly due to these pathologies. In other words, there is a high degree of overlap between women with the above diseases and part of the infertility population. ART may increase postpartum hemorrhage (PPH) risk through placental abnormalities caused by embryo transfer-induced endometrial trauma. Additionally, exogenous progesterone supplementation, commonly used in ART protocols, may impair uterine contractility by downregulating oxytocin receptor expression, reducing postpartum myometrial tone. Hence, it is postulated that the heightened prevalence of PPH within the ART cohort may be attributable to the synergistic effects of ART and the aforementioned medical conditions that are known to precipitate female infertility.
Pregnancy-Induced Hypertension
Pregnancy-induced hypertension (PIH), including chronic hypertension, gestational hypertension, preeclampsia-eclampsia, and concurrent preeclampsia with chronic hypertension, and it also constitutes a predominant source of maternal and perinatal morbidity and mortality.21,22 PIH has great damage to the health of maternal and newborn, and even threatens the life of the mother. Preeclampsia is implicated in microangiopathy and vasoconstriction, resulting in organ dysfunction.22 Also, certain evidence suggests that women affected by preeclampsia are at an elevated risk for chronic renal disease and cardiovascular complication.23 Hormonal hyperstimulation during ovarian induction alters vascular endothelial function, promoting vasoconstriction and systemic inflammation. Epigenetic modifications from in-vitro embryo culture may further dysregulate placental angiogenesis, like reduced placental growth factor, exacerbating maternal endothelial dysfunction and hypertension. In this study, the Assisted Reproductive Technology (ART) cohort exhibited an augmented susceptibility to pregnancy-induced hypertension irrespective of the number of fetuses. However, the etiopathogenesis of ART-associated PIH remains to be fully elucidated; some researchers postulate a correlation with epigenetic modifications and dysregulation of placental immunity.24,25 Moreover, comparative studies have indicated that frozen embryo transfer is associated with a more pronounced impact on the incidence of pregnancy-induced hypertension than fresh embryo transfer,22,25 which may have implications for the refinement of ART protocols in the future.
Gestational Diabetes Mellitus
Our study found the experimental group exhibited a heightened susceptibility to gestational diabetes mellitus when compared to the control cohort, a finding that concurs with the data presented in prior pertinent literature.7,26 The most prevalent form of GDM is type 2 diabetes mellitus, which may be associated with factors such as insulin resistance, alterations in blood volume, and vascular endothelial injury.26 During ART pregnancy, there often have defects in the luteal phase that lead to insufficient progesterone--a hormone that is important for maintaining pregnancy and preventing miscarriage—so it is customary for the mother to take exogenous progesterone to sustain the luteal phase. However, this hormone has the propensity to augment insulin resistance within the organism, potentially triggering dysregulation of glucose metabolism and, subsequentially, precipitating diabetes.7 Furthermore, a recent study has indicated that tumor necrosis factor-α and leptin are closely associated with insulin resistance in pregnant women.27 The elevated risk of pregnancy-induced hypertension (PIH) in the experimental group may be attributed to multifactorial mechanisms. First, hormonal interventions during ovarian stimulation, particularly supraphysiological estrogen levels, could impair endothelial function and promote vasoconstriction via reduced nitric oxide bioavailability.22 Second, epigenetic modifications induced by in-vitro embryo culture may dysregulate placental development, as evidenced by altered expression of angiogenesis-related genes in ART-derived placentas.24 Third, underlying maternal pathologies, such as chronic inflammation associated with endometriosis, may synergize with ART procedures to exacerbate systemic oxidative stress and endothelial dysfunction.19 These hypotheses warrant validation through longitudinal biomarker studies and placental histopathological analyses. Most cases of GDM resolve postpartum, but certain patients face an elevated risk of developing type 2 diabetes later in life. During pregnancy, inadequately managed diabetes significantly elevates the risks of miscarriage, congenital anomalies, pre-eclampsia, preterm birth, cesarean section, and perinatal mortality.28 Therefore, we recommend that patients should undergo examinations every 1 to 2 weeks during the first two months of gestation and on a weekly basis after 30 weeks of gestation.
Intrahepatic Cholestasis of Pregnancy
Intrahepatic cholestasis of pregnancy (ICP) ranks among the most prevalent maternal complications, the main manifestations were increased serum bile acid concentration (TBA ≥ 10 µmol/L), and the resulting pruritus and increased serum aminotransferase levels.29 These symptoms are generally alleviated promptly postpartum and most do not cause severe impact on the maternal. This study suggests that Assisted Reproductive Techniques (ART) may elevate the incidence of ICP. Concurrently, extant studies indicate that ICP not only occurs with greater frequency in ART-conceived pregnancies but also manifests at an earlier gestational stage.6,30 Furthermore, ICP is more frequently observed in twin gestations compared to singleton pregnancies,9,29 and the utilization of ART exactly exacerbates this kind of risk. Impairment of ICP is associated with, some studies indicate, endothelial dysfunction induced by elevated bile acids, renal dysfunction and oxidative stress.31 Despite the fact that ICP does not exert profound effects on maternal generally, it increases the risk of complications such as preterm birth and fetal distress, and perinatal fetal mortality.29 ART-induced hormonal fluctuations, particularly elevated estrogen levels, disrupt hepatic bile acid transporters such as BSEP, MRP2, leading to bile acid accumulation. This cholestasis triggers pruritus and elevates risks of fetal distress via bile acid-mediated placental oxidative stress. There are two aspects to the treatment of ICP: One is to actively treat pregnant women to relieve their symptoms such as pruritus and prevent the occurrence of serious complications; the other is to closely monitor the fetus regularly and deliver as soon as possible after the conditions are satisfied. Current clinical guidelines advocate for rigorous management of pregnancies with TBA levels ≥ 40 µmol/L, given that elevated bile acids are associated with an increased risk of adverse perinatal outcomes, such as preterm birth, pre-eclampsia and perinatal death.9,30,32,33 This threshold should be applied with increased stringency in the context of twin pregnancies.
Pelvic Inflammation Disease
Pelvic inflammatory disease (PID) is a clinical syndrome of the female reproductive system, which is caused by the invasion of microorganisms through the vagina or cervix and ascending infection, causing inflammation of the endometrium, fallopian tubes and other upper reproductive tract structures or peritoneum.34,35 In general, the incidence of pelvic inflammatory disease is relatively low due to the protection of anatomical barriers, cervical mucus plugs, local acidic environment, and immune cells in the genital mucosa. However, the IVF process requires the delivery of embryos formed in-vitro through the cervical mucus barrier into the uterine cavity, which makes the local protective barrier of the reproductive tract impaired.35 Meanwhile, in some reported cases, the process of embryo transfer may promote microorganisms from the cervix to the uterine cavity and fallopian tubes, or it may be transmitted by infected semen to cause inflammation.36 Embryo transfer procedures may breach cervical mucus barriers, introducing pathogens into the upper reproductive tract. Subclinical infections in women with preexisting tubal infertility could reactivate during ART, compounded by immunosuppressive effects of hormonal therapies. However, many pelvic infections are subclinical, and the diagnosis of PID lacks specific tests, and most of them rely on clinical symptoms and signs to assist the diagnosis. When pregnant women’s immunity is reduced, these symptoms will be more obvious.34 Therefore, it is difficult to tell whether pelvic inflammatory disease is a concomitant disease before pregnancy or a complication caused by ART procedures.
In our study, the data analysis showed an increased risk for pelvic inflammation in the experimental group, but when limiting the data to singleton births, there was no significant difference between groups. However, because of the low incidence of pregnancy-associated pelvic inflammatory disease and the small sample size included in the trial, this difference remains questionable. Does ART cause pelvic inflammatory disease, or do women with infertility caused by chronic pelvic inflammatory disease present clinical signs of pelvic inflammatory disease after receiving ART? This still needs follow-up study.
Other Comorbidities
A number of other diseases were identified in this study, the most common of which were thyroid diseases. Previous literature has established that thyroid hormones are essential for the regulation of the female reproductive system to maintain normal menstrual function, fertility, and successful maintenance of pregnancy.37 It is well known that the maternal demand for a variety of hormones increases during pregnancy, and thyroid hormones are among them. Studies have demonstrated that maternal thyroid hormone levels should increase by about 50% during pregnancy to adapt to the changes in the body,37 but this change is difficult to complete in ART pregnancy.37 Also, thyroid autoimmunity (TAI) is a major risk factor for thyroid dysfunction, which increases the risk of subclinical or hypothyroidism during pregnancy.37–39 Thyroid dysfunction caused by the above causes can lead to menstrual cycle disorders and a series of pregnancy complications. In addition, hyperthyroidism may also create a cytotoxic microenvironment that damages mature oocytes, reducing their quality and the possibility of fertilization, adversely affecting fertility and reproductive outcomes.37
There is evidence that TAI-related thyroid dysfunction is also a cause of infertility and has adverse effects on pregnancy outcomes.40 And thyroid hormone deficiency is associated with ovarian stimulation; therefore, pregnant women conceived by ART tend to have worse thyroid function.7,40 ART protocols disrupt the hypothalamic-pituitary-thyroid axis, exacerbating preexisting thyroid autoimmunity. Ovarian stimulation also increases thyroxine-binding globulin, altering free thyroid hormone levels and impairing fetal neurodevelopment. To prevent these adverse effects, TSH and TPOAb are routinely used as initial screening tests in infertile women,37,38 and women with abnormal thyroid function are given levothyroxine supplementation before conception, and thyroid function is monitored regularly during pregnancy.7
Our finding of a significantly higher multiple gestation rate in the experimental group (24.3% vs 3.2%) aligns with previous reports from China and Europe,12 which reported rates of 20–30% following double embryo transfer. However, our observed risk exceeds that in a 2023 meta-analysis,6 likely due to regional preferences for multiple embryo transfers in Northwest China. Notably, recent guidelines advocating single embryo transfer14 have reduced multifetal pregnancies in developed regions,25 highlighting the need for protocol standardization in resource-limited settings.
Strengths and Limitation
This study introduces several methodological and conceptual advancements that distinguish it from prior research. Methodologically, unlike previous studies that often relied on unmatched cohorts or inadequate control of confounding factors, we employed a rigorous 1:1 matched retrospective design, pairing IVF-ET and natural conception groups by admission month and gestational age (±7 days). This approach minimizes bias from temporal or gestational variability, enhancing causal inference regarding ART-associated risks. Analytically, we stratified outcomes by singleton pregnancies—a critical yet understudied subgroup—to disentangle ART-specific effects from the well-documented risks of multifetal gestations. This stratification addresses a key limitation in existing literature, which frequently conflates ART with multifetal complications. Geographically, as the first large-scale investigation conducted in Northwest China, our study fills a regional evidence gap, offering insights into ART outcomes within a population with distinct demographic and healthcare access profiles. Furthermore, we systematically evaluated rarely explored complications (such as pelvic inflammation and thyroid disorders) in ART pregnancies, broadening the scope beyond conventional obstetric outcomes. By integrating rigorous matching, stratified analysis, and region-specific data, this work not only refines risk attribution but also provides actionable evidence for optimizing ART protocols in diverse clinical settings. There are relatively few studies in China on ART and pregnancy complications, and this article may be helpful for future research.
However, this study also has some shortcomings. For example, we only collected data from one hospital in Gansu Province, and the situation in other hospitals and other regions of China cannot be generalized. Moreover, the sample size is small, resulting in insufficient support for data on certain complications (such as pelvic inflammatory disease). In addition, we did not collect data on the specific causes of infertility in the experimental subjects, so we cannot analyze the impact of these factors on infertility and on maternal and neonatal outcomes. Besides, despite efforts to control for confounders through matching and multivariate adjustment, unmeasured factors such as socioeconomic status, psychological stress, or undiagnosed medical conditions may still influence the outcomes. The observational nature of this study limits causal inference, and residual confounding cannot be entirely ruled out. Overall, this study employed a matched retrospective design to enhance comparability between groups; however, as an observational study, it cannot establish causality. The findings represent associations between IVF-ET and perinatal complications, which may be influenced by both measured and unmeasured confounders. Future prospective studies should incorporate biomarkers (eg, placental growth factor, bile acids, inflammatory cytokines) to elucidate mechanistic pathways. Additionally, qualitative research exploring patient and provider perspectives on ART practices in resource-limited settings would inform the implementation of evidence-based policies.
The high rate of multiple gestations and associated complications observed in this study underscores the urgent need for policy interventions to promote single embryo transfer (SET) in Northwest China. Financial subsidies for SET cycles and patient education regarding the risks of multiple pregnancies may help reduce obstetric complications. In regions where cultural preferences for twins persist, culturally sensitive counseling and shared decision-making tools should be developed.
Conclusion
This matched retrospective study demonstrates that IVF-ET pregnancies in Northwest China are associated with significantly higher risks of multiple gestations and obstetric complications, independent of multifetal pregnancies. The elevated rate of multiple gestations (24.3%) aligns with earlier data from China but exceeds rates in regions where elective single embryo transfer (SET) is standard, underscoring a pressing need to adopt evidence-based transfer policies. Our findings advocate for the implementation of strict SET policies, supported by financial incentive programs, and the enforcement of tighter eligibility criteria for multiple embryo transfers in resource-limited settings.
Furthermore, the observed associations likely result from a synergistic effect between ART procedures and underlying maternal pathologies (eg, thyroid autoimmunity, endometriosis). Given the observational nature of this study, the findings warrant validation through prospective cohorts incorporating biomarker analyses to elucidate mechanistic pathways, and randomized trials comparing transfer strategies in this population. By addressing these regional and biological nuances, this study provides a foundation for developing tailored ART guidelines that mitigate risks and improve perinatal outcomes for infertile women.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The First Hospital of Lanzhou University (NO.LDYYLL-2024-678).
Due to the nature of retrospective study and anonymized patient’s information, informed consent is waived with the approval of Ethics Committee of The First Hospital of Lanzhou University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study is funded by Hospital fund of the First Hospital of Lanzhou University (ldyyyn2022-9); 2024 Gansu Province University Teachers’ Innovation Fund Project (2024B-008); Lanzhou University undergraduate research innovation project (20240060071); Lanzhou University undergraduate research innovation project (20250060020).
Disclosure
All authors declare there is no conflict of interest.
References
1. Evers JL. Female subfertility. Lancet. 2002;360(9327):151–159. doi:10.1016/S0140-6736(02)09417-5
2. Gnoth C, Godehardt E, Frank-Herrmann P, Friol K, Tigges J, Freundl G. Definition and prevalence of subfertility and infertility. Hum Reprod. 2005;20(5):1144–1147. doi:10.1093/humrep/deh870
3. Nik Hazlina NH, Norhayati MN, Shaiful Bahari I, Nik Muhammad Arif NA. Worldwide prevalence, risk factors and psychological impact of infertility among women: a systematic review and meta-analysis. BMJ Open. 2022;12(3):e057132. doi:10.1136/bmjopen-2021-057132
4. Lei LL, Lan YL, Wang SY, Feng W, Zhai ZJ. Perinatal complications and live-birth outcomes following assisted reproductive technology: a retrospective cohort study. Chin Med J. 2019;132(20):2408–2416. doi:10.1097/CM9.0000000000000484
5. Tai W, Hu L, Wen J. Maternal and neonatal outcomes after assisted reproductive technology: a retrospective Cohort study in China. Front Med Lausanne. 2022;9:837762. doi:10.3389/fmed.2022.837762
6. Qin J, Liu X, Sheng X, Wang H, Gao S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril. 2016;105(1):73–76. doi:10.1016/j.fertnstert.2015.09.007
7. Xiong Y, Zang X, Xie T, Yang C, Jiang X, Chen M. Additional adverse perinatal outcomes with no effect on neonatal mortality and birth defects in pregnancies conceived by assisted reproductive technology. Front Pediatr. 2022;10:809259. doi:10.3389/fped.2022.809259
8. Fujii M, Matsuoka R, Bergel E, van der Poel S, Okai T. Perinatal risk in singleton pregnancies after in vitro fertilization. Fertil Steril. 2010;94(6):2113–2117. doi:10.1016/j.fertnstert.2009.12.031
9. Grech V, Gatt M. Assisted reproductive technology and multiple pregnancy in Malta - A population based study. Early Hum Dev. 2021;157:105378. doi:10.1016/j.earlhumdev.2021.105378
10. Shan D, Hu Y, Qiu P, et al. Intrahepatic cholestasis of pregnancy in women with twin pregnancy. Twin Res Hum Genet. 2016;19(6):697–707. doi:10.1017/thg.2016.74
11. Modabbernia A, Sandin S, Gross R, et al. Apgar score and risk of autism. Eur J Epidemiol. 2019;34(2):105–114. doi:10.1007/s10654-018-0445-1
12. Luke B, Gopal D, Cabral H, Stern JE, Diop H. Adverse pregnancy, birth, and infant outcomes in twins: effects of maternal fertility status and infant gender combinations; the Massachusetts outcomes study of assisted reproductive technology. Am J Obstet Gynecol. 2017;217(3):
13. Chih HJ, Elias FTS, Gaudet L, Velez MP. Assisted reproductive technology and hypertensive disorders of pregnancy: systematic review and meta-analyses. BMC Pregnancy Childbirth. 2021;21(1):449. doi:10.1186/s12884-021-03938-8
14. Practice Committee of the American Society for Reproductive Medicine and the Practice Committee for the Society for Assisted Reproductive Technologies. Electronic address: [email protected]. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril, 2021; 116(3):651–654. doi:10.1016/j.fertnstert.2021.06.050
15. Knight M, Callaghan WM, Berg C, et al. Trends in postpartum hemorrhage in high resource countries: a review and recommendations from the international postpartum hemorrhage collaborative group. BMC Pregnancy Childbirth. 2009;9:55. doi:10.1186/1471-2393-9-55
16. Nyfløt LT, Sandven I, Oldereid NB, Stray-Pedersen B, Vangen S. Assisted reproductive technology and severe postpartum haemorrhage: a case-control study. BJOG. 2017;124(8):1198–1205. doi:10.1111/1471-0528.14471
17. Romundstad LB, Romundstad PR, Sunde A, von Düring V, Skjaerven R, Vatten LJ. Increased risk of placenta previa in pregnancies following IVF/ICSI; a comparison of ART and non-ART pregnancies in the same mother. Hum Reprod. 2006;21(9):2353–2358. doi:10.1093/humrep/del153
18. Chen C, Liu X, Chen D, et al. A risk model to predict severe postpartum hemorrhage in patients with placenta previa: a single-center retrospective study. Ann Palliat Med. 2019;8(5):611–621. doi:10.21037/apm.2019.09.04
19. Vannuccini S, Clifton VL, Fraser IS, et al. Infertility and reproductive disorders: impact of hormonal and inflammatory mechanisms on pregnancy outcome. Hum Reprod Update. 2016;22(1):104–115. doi:10.1093/humupd/dmv044
20. Nirgianakis K, Kalaitzopoulos DR, Schwartz ASK, et al. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: a systematic review and meta-analysis. Reprod Biomed Online. 2021;42(1):185–206. doi:10.1016/j.rbmo.2020.09.023
21. Elfassy T, Kulandavelu S, Dodds L, et al. Association between hypertensive disorders of pregnancy and interval neurocognitive decline: an analysis of the hispanic community health study/study of latinos. Obstet Gynecol. 2024;143(6):785–793. doi:10.1097/AOG.0000000000005571
22. Omani-Samani R, Alizadeh A, Almasi-Hashiani A, et al. Risk of preeclampsia following assisted reproductive technology: systematic review and meta-analysis of 72 cohort studies. J Matern Fetal Neonatal Med. 2020;33(16):2826–2840. doi:10.1080/14767058.2018.1560406
23. Butalia S, Audibert F, Côté AM, et al. Hypertension Canada. Hypertension Canada’s 2018 guidelines for the management of hypertension in pregnancy. Can J Cardiol. 2018;34(5):526–531. doi:10.1016/j.cjca.2018.02.021
24. Levron Y, Dviri M, Segol I, et al. The ‘immunologic theory’ of preeclampsia revisited: a lesson from donor oocyte gestations. Am J Obstet Gynecol. 2014;211(4):
25. Opdahl S, Henningsen AA, Tiitinen A, et al. Risk of hypertensive disorders in pregnancies following assisted reproductive technology: a cohort study from the CoNARTaS group. Hum Reprod. 2015;30(7):1724–1731. doi:10.1093/humrep/dev090
26. Chen S, Zhou Y, Mu Q, Wang Y. The interaction effect of pre-pregnancy body mass index and maternal age on the risk of pregnancy complications in twin pregnancies after assisted reproductive technology. J Matern Fetal Neonatal Med. 2023;36(2):2271623. doi:10.1080/14767058.2023.2271623
27. Ryan EA. Hormones and insulin resistance during pregnancy. Lancet. 2003;362(9398):1777–1778. doi:10.1016/S0140-6736(03)14942-2
28. ACOG Committee on Practice Bulletins. ACOG practice Bulletin. Clinical management guidelines for obstetrician-Gynecologists. Number 60, March 2005. Pregestational diabetes mellitus. Obstet Gynecol, 2005; 105(3):675–685. doi:10.1097/00006250-200503000-00049
29. Çelik S, Çalışkan C. The impact of assisted reproductive technology in twin pregnancies complicated by intrahepatic cholestasis of pregnancy: a retrospective Cohort study. Z Geburtshilfe Neonatol. 2021;225(1):34–38. doi:10.1055/a-1129-7358
30. Zhang Q, Xu Y, Gong Y, Liu X. The impact of assisted reproductive technology in twin pregnancies complicated by intrahepatic cholestasis: a five-year retrospective study. BMC Pregnancy Childbirth. 2022;22(1):269. doi:10.1186/s12884-022-04610-5
31. Hu YY, Liu JC, Xing AY.Oxidative stress markers in intrahepatic cholestasis of pregnancy: a prospective controlled study. Eur Rev Med Pharmacol Sci. 2015;19(17):3181–3186.
32. Cui D, Zhong Y, Zhang L, Du H. Bile acid levels and risk of adverse perinatal outcomes in intrahepatic cholestasis of pregnancy: a meta-analysis. J Obstet Gynaecol Res. 2017;43(9):1411–1420. doi:10.1111/jog.13399
33. Brouwers L, Koster MP, Page-Christiaens GC, et al. Intrahepatic cholestasis of pregnancy: maternal and fetal outcomes associated with elevated bile acid levels. Am J Obstet Gynecol. 2015;212(1):
34. Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med. 2015;372(21):2039–2048. doi:10.1056/NEJMra1411426
35. Matorras R, Rubio K, Iglesias M, Vara I, Expósito A. Risk of pelvic inflammatory disease after intrauterine insemination: a systematic review. Reprod Biomed Online. 2018;36(2):164–171. doi:10.1016/j.rbmo.2017.11.002
36. Broder S, Sims C, Rothman C. Frequency of postinsemination infections as reported by donor semen recipients. Fertil Steril. 2007;88(3):711–713. doi:10.1016/j.fertnstert.2006.12.062
37. Bucci I, Giuliani C, Di Dalmazi G, Formoso G, Napolitano G. Thyroid autoimmunity in female infertility and assisted reproductive technology outcome. Front Endocrinol. 2022;13:768363. doi:10.3389/fendo.2022.768363
38. Unuane D, Velkeniers B. Impact of thyroid disease on fertility and assisted conception. Best Pract Res Clin Endocrinol Metab. 2020;34(4):101378. doi:10.1016/j.beem.2020.101378
39. Pearce EN. Thyroid disorders during pregnancy and postpartum. Best Pract Res Clin Obstet Gynaecol. 2015;29(5):700–706. doi:10.1016/j.bpobgyn.2015.04.007
40. Rao M, Zeng Z, Zhou F, et al. Effect of levothyroxine supplementation on pregnancy loss and preterm birth in women with subclinical hypothyroidism and thyroid autoimmunity: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(3):344–361. doi:10.1093/humupd/dmz003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.