Back to Journals » Clinical Interventions in Aging » Volume 20
Comparative Analysis of Enucleation Techniques for Large Benign Prostatic Hyperplasia (>80 cm3) in Older Adult Patients: A Single-Center Cohort Study
Authors Hou CP ![]() , Chen YT
, Chen YT ![]() , Lin YH
, Lin YH ![]() , Chen CL
, Chen CL ![]() , Teng TC
, Teng TC ![]() , Juang HH
, Juang HH ![]()
Received 20 August 2025
Accepted for publication 6 November 2025
Published 6 December 2025 Volume 2025:20 Pages 2437—2446
DOI https://doi.org/10.2147/CIA.S558277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Chen Pang Hou,1– 3 Yu-Ting Chen,1 Yu-Hsiang Lin,1,3 Chien-Lun Chen,1,3 Tzu-Chi Teng,1 Horng-Heng Juang3
1Department of Urology, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; 2Department of Healthcare Management, Yuanpei University of Medical Technology, Hsinchu, Taiwan; 3School of Medicine, Chang Gung University, Taoyuan, 333, Taiwan
Correspondence: Chen Pang Hou, Department of Urology, Chang gung Memory Hospital at Linko, 5 Fu-shing Street, Kwei-Shan, Taoyuan, 333, Taiwan, Tel +886 3 328 1200 ext 2137, Fax +886 3 211 8112, Email [email protected]
Purpose: To evaluate and compare the safety, efficacy, and patient-centered outcomes of three enucleation techniques—bipolar transurethral enucleation of the prostate (B-TUEP), thulium laser enucleation (ThuLEP), and robotic-assisted simple prostatectomy (RASP)—in older adult patients (> 60 years) with large-volume benign prostatic hyperplasia (BPH > 80 cm3), a population at increased surgical risk and underrepresented in prior comparative studies.
Patients and Methods: This study retrospectively analyzed 127 patients aged 60 to 90 years who underwent B-TUEP (n=43), ThuLEP (n=58), or RASP (n=26) between 2014 and 2024. All procedures were performed by a single surgeon. Preoperative and 12-month postoperative outcomes—including IPSS, Qmax, post-void residual (PVR), and quality of life (QoL)—were assessed. Complication profiles, including urinary tract infection (UTI), prolonged analgesic requirement (PAR), and unexpected return visits (URV), were evaluated to reflect real-world risks in the older adults population.
Results: All three surgical techniques resulted in significant and sustained improvements in IPSS, Qmax, and PVR, with no significant intergroup differences at 12 months. ThuLEP demonstrated the lowest postoperative pain and analgesic use, RASP had the lowest UTI incidence, and B-TUEP was associated with the shortest operative time. Kaplan–Meier analysis showed comparable long-term medication-free survival across groups (p = 0.085). Quality of life scores improved in all groups, with numerically better outcomes observed in the RASP group.
Conclusion: In older adult patients with large BPH, B-TUEP, ThuLEP, and RASP all offer effective and durable symptom relief with distinct perioperative advantages. Given the heightened risks associated with aging—including infection, delayed recovery, and medication burden—this study underscores the importance of tailored surgical decision-making in patients over 60. All three techniques are viable, and selection should be guided by individual patient priorities and risk profiles.
Keywords: prostatic hyperplasia, laser therapy, prostatectomy, robotic surgery, aged
Introduction
Benign prostatic hyperplasia (BPH) is a common, non-cancerous enlargement of the prostate in aging men, affecting about 10% in their 40s and up to 90% over age 80.1 Its development is influenced by hormones like dihydrotestosterone (DHT), along with aging, genetics, regional, and metabolic factors.2 BPH presents with lower urinary tract symptoms (LUTS), including voiding (eg, weak stream, hesitancy) and storage (eg, frequency, urgency, nocturia) issues.2 Treatment depends on symptom severity and patient preference, ranging from medication to surgery.3 Common medications for BPH include α-adrenergic antagonists, which relax smooth muscles, and 5α-reductase inhibitors, which reduce prostate size via hormonal modulation.3–5 If medications fail or complications arise (eg, retention, infections), procedures like TURP or other minimally invasive options are considered.5 Older adult patients are particularly vulnerable to perioperative complications and may experience different postoperative recovery patterns than younger patients.6 Surgical risks increase with age and larger prostate volumes; studies show older adults patients, especially those ≥75, have higher risks of hemorrhage, cardiovascular events, and blood transfusion after TURP.6–10 The 2020 AUA and 2022 EAU guidelines recommend HoLEP, ThuLEP, and simple prostatectomy over conventional TURP for large prostates (>80 mL), due to TURP’s lower efficacy, longer operative time, and higher risks of bleeding and TUR syndrome.11,12 Recent studies have compared these advanced techniques in patients with prostate volumes exceeding 80 g.13–16 In our prior study, we conducted a comprehensive comparison of B-TUEP, ThuLEP, and RASP for prostates >80 cm3, all performed by a single surgeon.17 Building on our previous work, we compared B-TUEP, ThuLEP, and RASP in prostates >80 cm3, all performed by a single surgeon. Unlike earlier studies, we included both functional and patient-centered outcomes. This study further extends our findings in a larger cohort of patients aged ≥60, with longer follow-up, aiming to inform personalized surgical selection based on patient characteristics.
Materials and Methods
Study Design and Patient Selection
From January 2014 to June 2024, this study prospectively enrolled patients diagnosed with symptomatic BPH at a single tertiary center. Eligible individuals subsequently underwent retrospective analysis if they received one of the following procedures: robotic-assisted simple prostatectomy (RASP), thulium laser enucleation (ThuLEP), or bipolar transurethral enucleation of the prostate (B-TUEP). This study was reviewed and approved by the Institutional Review Board of Chang Gung Memorial Hospital, Taiwan (IRB No. 202500702B0). As patient consent to review their medical records was not required by the Institutional Review Board, all data were fully anonymized before analysis, and no identifiable personal information was used. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All surgeries were performed by a single urologist proficient in all three procedures. Surgical decision-making was patient-centered, employing a shared decision-making (SDM)18 framework that incorporated detailed counseling regarding surgical options. Preoperative assessment included a comprehensive review of medical history, physical examination, digital rectal examination (DRE), prostate-specific antigen (PSA) testing, and transrectal ultrasound (TRUS). In cases of suspicious findings on DRE or TRUS, prostate biopsies were performed to exclude malignancy. Following our protocol, antiplatelet agents were stopped 7 days before surgery, while warfarin or direct oral anticoagulants were withheld for 3–5 days depending on the drug type and renal function, with surgery performed after confirming normal coagulation. All antithrombotic agents resumed for about 7 days postoperatively once hemostasis was secured. Baseline assessments included urodynamic parameters—voided volume (VV), post void residual urine (PVR), and peak urinary flow rate (Qmax)—as well as symptom and quality-of-life scores (IPSS and IPSS-derived QoL).
Inclusion and Exclusion Criteria
Patients were included if they met the following criteria: ECOG (Eastern Cooperative Oncology Group) performance status19 of 0 or 1, age between 60 and 90 years, IPSS ≥ 20, Qmax ≤ 15 mL/s, and prostate volume ≥ 80 g. All participants had received at least three months of pharmacological treatment and met the surgical criteria for bladder outlet obstruction (BPO) as defined by EAU guidelines.20 Exclusion criteria comprised active malignancy, prior prostate surgery, and LUTS attributed to non-BPH etiologies such as neurogenic bladder.
Operative Techniques
B-TUEP procedures utilized the Olympus SurgMaster UES-40 generator and OES-Pro bipolar resectoscope, with settings standardized at 200 W (cutting), 120 W (coagulation), and 60 W for enucleation. ThuLEP was performed using a 120-W thulium: YAG laser (Vela XL, Boston Scientific) delivered through a 600-μm LightTrail fiber via a 26F continuous-flow resectoscope, with isotonic saline used for irrigation. Tissue was morcellated using a Wolf Piranha morcellator. RASP was conducted using the da Vinci Si robotic system via a suprapubic transvesical approach. Techniques for each modality were based on established protocols described in prior literature.21–23
Postoperative Management and Follow-Up
All patients received a 22 Fr three-way Foley catheter for irrigation. Catheters were removed on postoperative day 2 for B-TUEP and ThuLEP, and on day 7 for RASP, unless complications required adjustment. Antibiotic prophylaxis and postoperative treatment were administered by established clinical guidelines.24 Pain was managed with oral acetaminophen for 7 days, and pain severity was documented using the numeric rating scale (NRS)25 on postoperative days 1 and 2. Preoperative voiding-related medications were routinely discontinued one week after surgery, unless specific clinical conditions required ongoing use. The need for continuation was reassessed during follow-up based on the patient’s voiding function. Enucleation efficiency was calculated as the ratio of the enucleated tissue weight to the preoperative transition zone (T zone) volume measured by transrectal ultrasound (TRUS), expressed as a percentage. The functional and clinical follow-up was conducted for 12 months postoperatively for all patients. Patients returned for evaluation at 2 weeks, 3 months, 6 months, and 12 months, and outcomes included IPSS, QoL, Qmax, voided volume (VV), and post-void residual (PVR). Complications were tracked and categorized as follows: Prolonged Analgesic Requirement (PAR) referred to analgesic use beyond one week postoperatively due to persistent pain; urinary tract infection (UTI) was defined as the presence of clinical symptoms such as dysuria, urgency, frequency, or fever ≥38°C, accompanied by pyuria (≥10 white blood cells per high-power field) on urinalysis and requiring antibiotic treatment during follow-up; and Unexpected Return Visits (URV) included any unplanned clinic or emergency visits due to surgery-related events. Medication-free survival, defined as the proportion of patients remaining off BPH medications postoperatively, was analyzed up to 60 months using follow-up data from electronic medical records to assess long-term efficacy across the three surgical groups.
Statistical Analysis
Descriptive data were expressed as mean ± standard deviation for continuous variables and as frequencies with percentages for categorical variables. Categorical variables were compared using the chi-square test, while continuous variables were analyzed using one-way analysis of variance (ANOVA). When significant differences were detected by ANOVA, post hoc comparisons were conducted using Dunnett’s test to identify pairwise differences among the three groups. Changes in numeric rating scale (NRS) pain scores over time were assessed using repeated-measures ANOVA. A p-value of less than 0.05 was considered statistically significant. All analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA).
Results
A total of 644 patients underwent prostate enucleation procedures during the study period. Of these, 168 (26%) patients with prostate volume greater than 80 mL were identified and considered for analysis. After excluding patients with prostate cancer confirmed by pathology (n = 6), those lost to follow-up (n = 23), and those with incomplete data (n = 12), a total of 127 patients completed the 12-month follow-up and were included in the final analysis. Patients were categorized into B-TUEP (n = 43), ThuLEP (n = 58), and RASP (n = 26) groups. The patient selection process is illustrated in Figure 1.
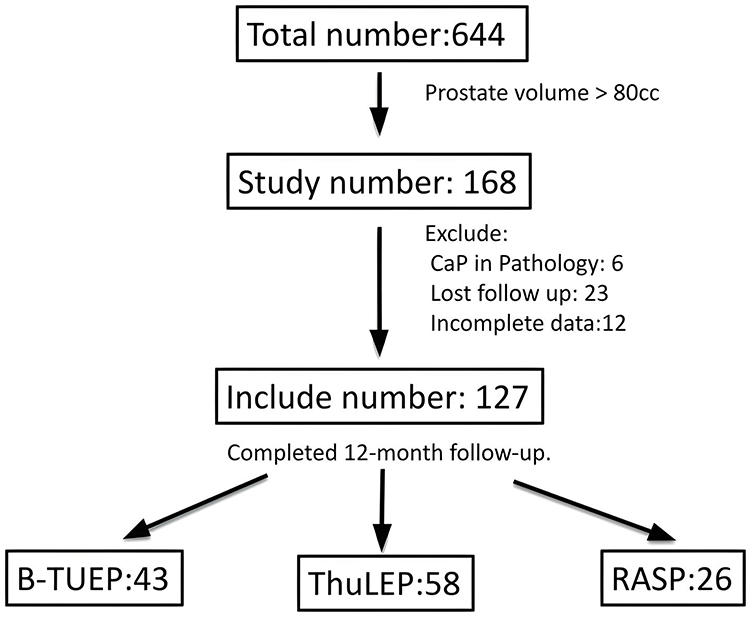 |
Figure 1 The patient selection flowchart. Of 644 patients, 168 had prostate volume >80 cc. After excluding 6 with prostate cancer, 23 lost to follow-up, and 12 with incomplete data, 127 patients completed 12-month follow-up: B-TUEP (n=43), ThuLEP (n=58), RASP (n=26). |
Baseline demographic and clinical characteristics of the study population are presented in Table 1. A significant difference in mean age was observed among the groups (p = 0.043), with RASP patients being notably younger compared to those in the B-TUEP and ThuLEP cohorts. Prostate volume was significantly greater in the RASP group (117.3 ± 23.9 cc) compared to B-TUEP (92.1 ± 13.1 cc) and ThuLEP (90.0 ± 10.7 cc) groups (p < 0.001). No statistically significant differences were observed in preoperative PSA levels, duration of prior medical therapy, IPSS scores, QoL scores, Qmax, PVR, or history of urinary retention. However, the Charlson Comorbidity Index (CCI) was significantly lower in the RASP group compared to the ThuLEP group (p = 0.027), suggesting that RASP patients had fewer baseline comorbid conditions.
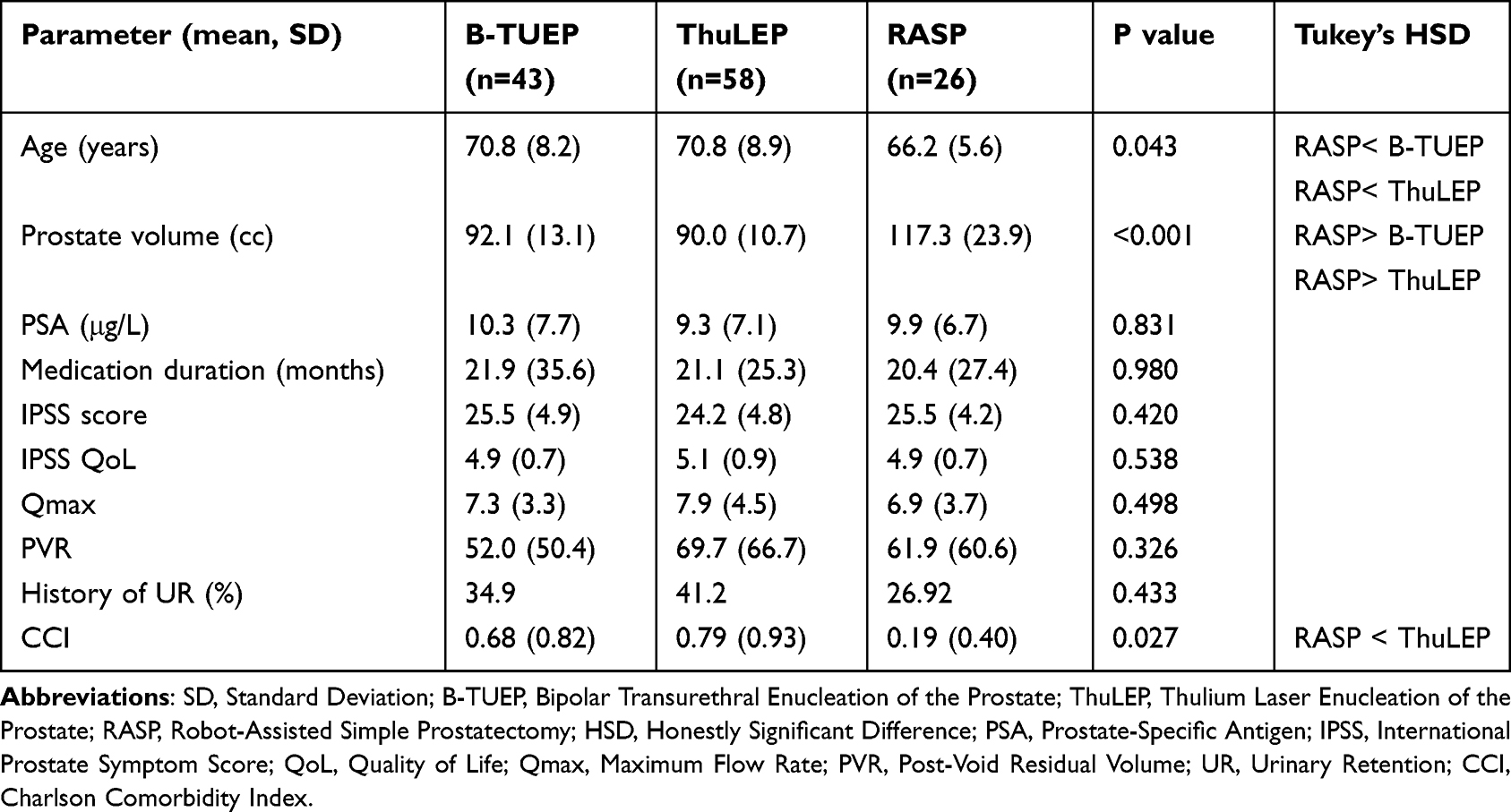 |
Table 1 Patient Characteristics |
The perioperative and postoperative outcomes across the three surgical groups are summarized as Table 2. Operative time differed significantly among groups (p < 0.001), with the RASP group demonstrating the longest duration (197.6 ± 46.5 minutes), followed by ThuLEP (120.4 ± 27.3 minutes) and B-TUEP (102.4 ± 29.3 minutes). Hospital stay was also significantly longer in the RASP group compared to the endoscopic groups (p < 0.001). The proportion of prostate tissue enucleated was highest in the RASP group (106.0 ± 36.6%), with statistically significant differences compared to B-TUEP and ThuLEP (p = 0.002). Postoperative pain, assessed via the numeric rating scale (NRS), was significantly lower in the ThuLEP group on both postoperative day 1 and day 2 (p < 0.001 and p = 0.019, respectively), with the highest pain scores observed in the RASP cohort. Use of intramuscular or intravenous analgesics was most common in the RASP group (38.5%) and least in the ThuLEP group (6.9%) (p < 0.001). The incidence of prolonged analgesic requirement (PAR) was significantly higher in RASP (30.8%) compared to B-TUEP and ThuLEP (p = 0.001). Conversely, the rate of urinary tract infection (UTI) was lowest in the RASP group (7.7%) and significantly higher in the endoscopic groups (p = 0.001). The trial without catheter (TWOC) success rates and unexpected return visits (URV) did not differ significantly among groups. Among patients with unexpected return visits, most in the B-TUEP group were due to hematuria and managed conservatively, corresponding to Clavien–Dindo grade I. In the ThuLEP group, causes included hematuria (5), UTI (3), UR (2), dizziness (1), herpes zoster (1), and abdominal bloating (2), all of which were treated without invasive intervention (Clavien I–II). In the RASP group, one patient with persistent bleeding required reoperation for endoscopic hemostasis (Clavien IIIb), while the remaining cases were managed conservatively (Clavien I).
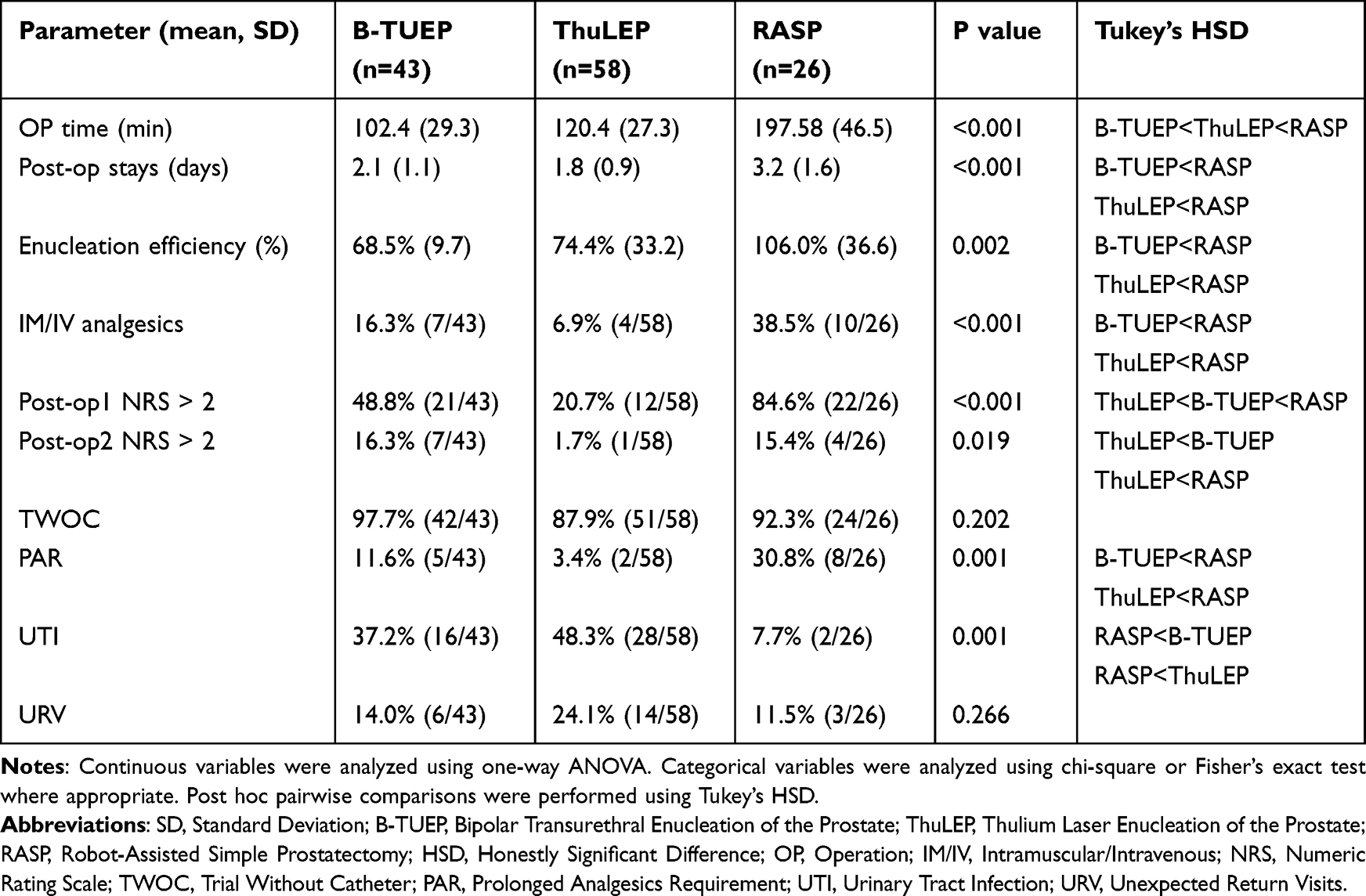 |
Table 2 Perioperative and Postoperative Parameters |
As illustrated in Figure 2, IPSS scores significantly improved across all surgical groups following the intervention and remained stable throughout the 12-month follow-up period. While the RASP group exhibited a slightly greater reduction in IPSS at 3 months, no statistically significant differences were observed among the three groups at any postoperative time point (preoperative p = 0.420; 3 months p = 0.103; 6 months p = 0.445; 12 months p = 0.252), indicating that all procedures provided comparable symptomatic relief. Figure 3 demonstrates that all surgical approaches resulted in a substantial increase in Qmax from baseline to 3 months, with the improvement sustained over 12 months. Although Qmax values increased significantly in each group, no significant intergroup differences were detected at any follow-up point (3 months p = 0.995; 6 months p = 0.981; 12 months p = 0.924), suggesting equivalent efficacy in improving urinary flow across all surgical modalities. As shown in Figure 4, mean post-void residual (PVR) volumes decreased significantly in all groups after surgery, with the greatest reduction occurring by the 3-month mark. This effect remained consistent through the 12-month follow-up. No statistically significant differences in PVR were observed among the groups at any time point (preoperative p = 0.326; 3 months p = 0.962; 6 months p = 0.976; 12 months p = 0.545), indicating that each technique was similarly effective in improving bladder emptying. Finally, Figure 5 illustrates that quality of life (QoL) scores improved significantly postoperatively in all groups. At 3 months, QoL improvements were comparable (p = 0.287); however, at 6 months, the RASP group demonstrated a significantly greater reduction in QoL scores compared to B-TUEP and ThuLEP (p = 0.026). Although the RASP group maintained numerically lower (better) QoL scores in 12 months, this difference did not reach statistical significance (p = 0.054). No patients in the three groups developed postoperative stress or urgency urinary incontinence during the 12-month follow-up. Similarly, no urethral stricture or bladder neck contracture was identified among the 127 patients with prostate volumes >80 g included in this study. Figure 6 reveals the Kaplan-Meier plot representing medication-free survival over 60 months following B-TUEP, ThuLEP, and RASP for BPH treatment. All three surgical methods demonstrated comparable long-term medication-free outcomes, with survival probabilities remaining relatively high throughout the follow-up period. The Log rank test showed no significant difference among the groups (p = 0.085), indicating similar effectiveness in maintaining medication-free status.
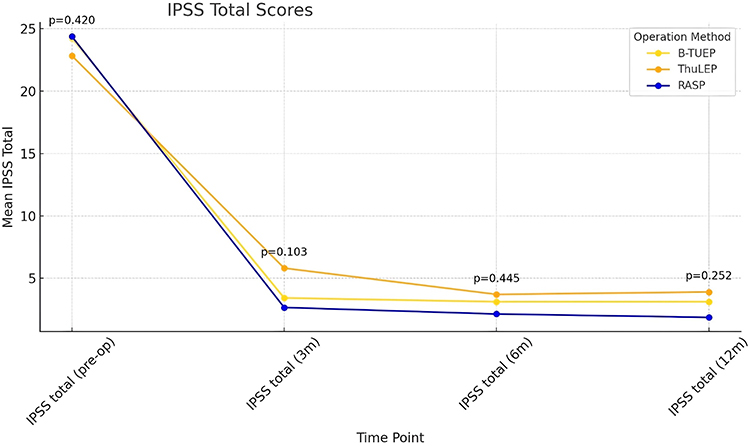 |
Figure 2 Changes in International Prostate Symptom Score (IPSS) total scores over time. IPSS scores significantly improved in all three groups: B-TUEP, ThuLEP, and RASP—after surgery and remained stable throughout 12 months of follow-up. No statistically significant differences were observed among the groups at any time point (p > 0.05). Data are presented as mean ± standard deviation. |
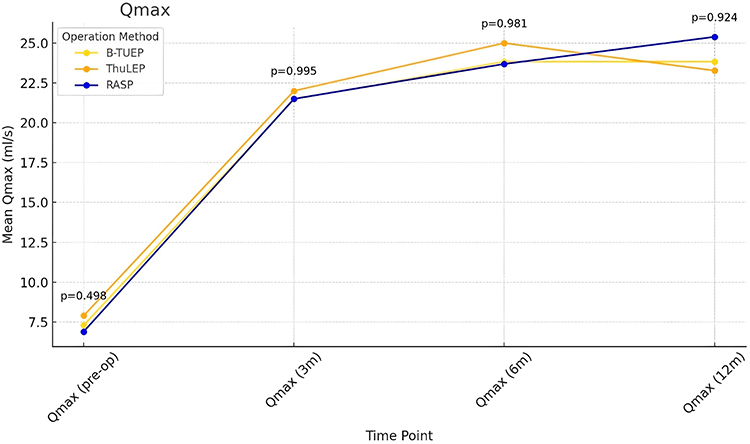 |
Figure 3 Maximum urinary flow rate (Qmax) changes over time. All groups showed significant and sustained improvement in Qmax after surgery, with no significant differences between B-TUEP, ThuLEP, and RASP at any time point. |
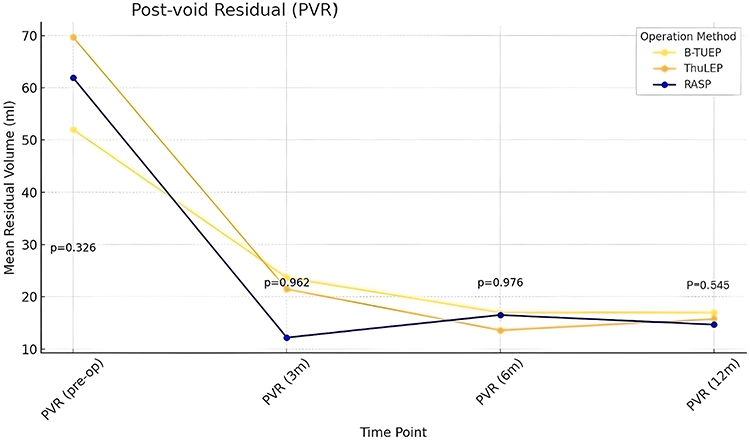 |
Figure 4 Post-void residual (PVR) over time. PVR significantly decreased in all groups after surgery and remained low during follow-up. No significant differences were observed among B-TUEP, ThuLEP, and RASP at any time point. |
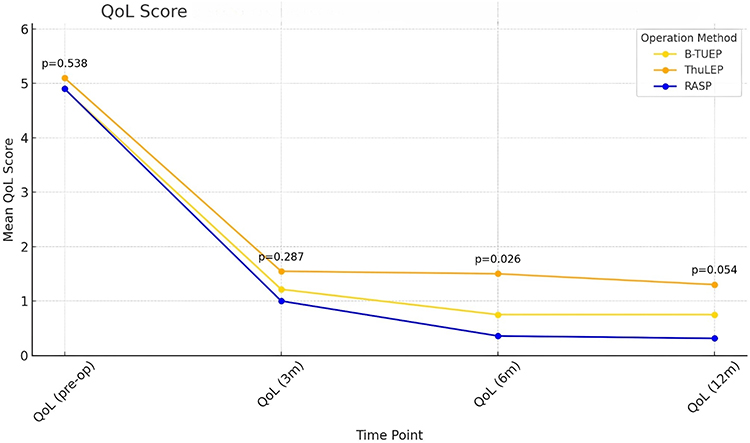 |
Figure 5 Quality of life (QoL) scores over time. QoL scores improved significantly in all groups postoperatively. At 6 months, RASP showed significantly better QoL compared to B-TUEP and ThuLEP (p = 0.026), though this difference was not significant at 12 months (p = 0.054). |
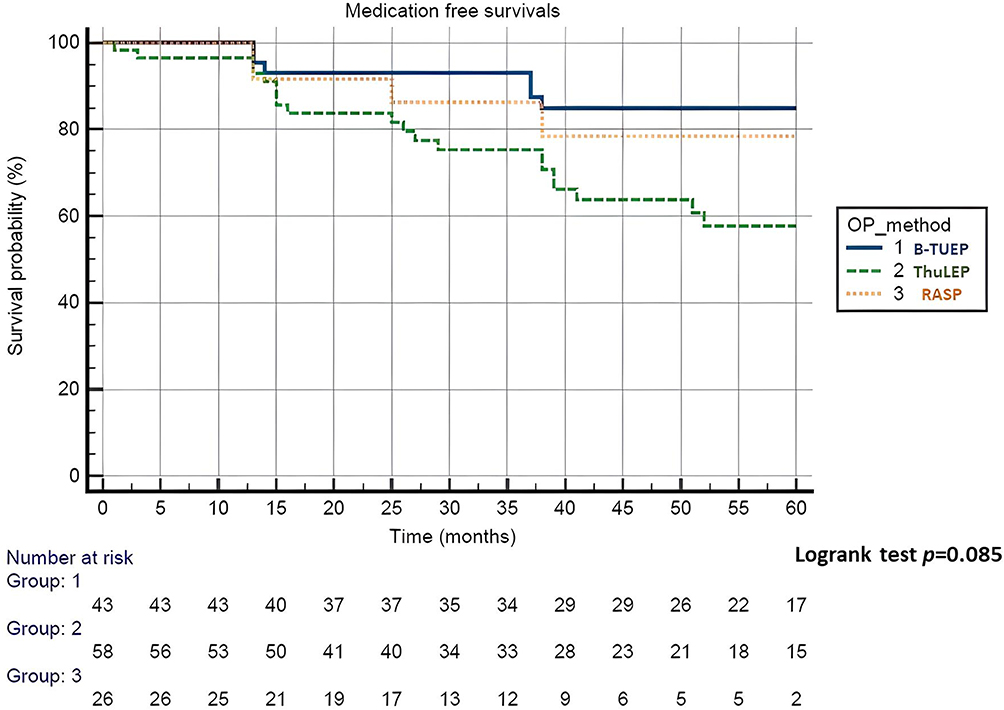 |
Figure 6 Kaplan–Meier curves of medication-free survival. Medication-free survival over 60 months was comparable among B-TUEP, ThuLEP, and RASP groups. No significant difference was observed (Log rank test p = 0.085), indicating similar long-term efficacy in maintaining symptom control without BPH-related medications. |
Discussion
The surgical recommendations for large-volume BPH (>80 mL) have evolved notably in the AUA guidelines. In 2010, open simple prostatectomy (OSP) was the primary recommendation for large prostates, as conventional TURP was considered insufficient for managing glands of this size.26 Minimally invasive techniques were not yet incorporated. By contrast, the 2020 AUA guideline amendment includes holmium and thulium laser enucleation (HoLEP, ThuLEP) and robotic-assisted simple prostatectomy (RASP) as effective alternatives to OSP.11 These procedures are now supported for their comparable efficacy and reduced perioperative morbidity. The updated guideline emphasizes individualized treatment planning, integrating patient factors, surgeon expertise, and institutional resources. This shift reflects broader trends in urologic surgery toward minimally invasive approaches and shared decision-making, offering more options with improved recovery profiles for patients with large prostates. However, current literature contains relatively few head-to-head comparative studies evaluating the advantages and disadvantages of different surgical approaches. Previously, we published a study comparing B-TUEP, ThuLEP, and RASP,17 from which several important conclusions were drawn: All three procedures were found to be effective and safe for large prostates, with unique advantages depending on the clinical priority: functional outcome (RASP), recovery and pain (ThuLEP), or efficiency (B-TUEP). Compared to our previous publication, the current study represents significant methodological and clinical advancement. It features a larger cohort, focuses on older adult patients, extends the follow-up period to 12 months, and incorporates broader safety and patient-centered outcome measures. While both studies found that B-TUEP, ThuLEP, and RASP effectively improve LUTS and flow rates in large prostate patients, the 2025 study offers a more comprehensive evaluation by incorporating longer follow-up, detailed pain and safety endpoints (eg, PAR, UTI, URV), and a focused analysis on older adults patients. The new findings highlight ThuLEP as the most favorable for perioperative comfort and RASP as the safest in terms of infection risk, supporting individualized, patient-centered surgical planning. The 2025 study concludes that the three surgical approaches—B-TUEP, ThuLEP, and RASP—provide comparable improvements in symptom severity (IPSS) and urinary flow rates (Qmax), with no statistically significant differences among them. Importantly, it also reports similar medication-free survival across all procedures, further supporting their long-term therapeutic equivalence.
In our study, the ThuLEP group demonstrated the lowest pain scores on postoperative days 1 and 2, along with the lowest rates of prolonged analgesic use and injectable analgesic administration. We believe this may be attributed to the shallower depth of thermal penetration associated with thulium laser. Comparative studies on the thermal effects of bipolar energy and laser in prostatic tissue have shown that bipolar energy results in a thermal penetration depth of approximately 2.4 ± 0.84 mm, whereas thulium laser exhibits a much shallower penetration depth of around 0.2 mm.27,28 Bipolar energy produces a deeper and thicker layer of thermal necrosis compared with thulium laser, which may induce greater local inflammation and postoperative discomfort, explaining the observed difference in pain levels. The lower incidence of postoperative UTI observed following RASP in our study may be explained by the reduced urethral manipulation and less high-pressure irrigation, which in endoscopic procedures can raise intravesical pressure, disrupt the mucosa, and facilitate bacterial invasion.29
This study has several limitations. All procedures were performed by a single surgeon at a tertiary center, which may limit generalizability. Although patients were prospectively enrolled, data were collected retrospectively, introducing potential bias. Patients in the RASP group had a significantly lower Charlson Comorbidity Index (CCI) compared with the endoscopic groups, suggesting a potential selection bias, as healthier individuals with fewer systemic comorbidities and their physicians were more likely to choose the robotic approach when considering surgical options for large prostates. The 12-month functional outcome follow-up may not capture long-term results, and the smaller RASP group size may reduce statistical power. In addition, the non-randomized design and unequal sample sizes among groups may have limited the ability to detect subtle intergroup differences. Future multicenter studies with longer follow-up, patient-reported outcomes, and cost-effectiveness analyses are needed. Nonetheless, this study offers practical guidance for surgical selection in large BPH, being the first to compare B-TUEP, ThuLEP, and RASP using consistent metrics and introducing medication-free survival as a long-term efficacy measure. Our findings support individualized decision-making: ThuLEP for patients concerned about pain, RASP for those with very large prostates or recurrent UTIs, and B-TUEP for faster recovery. All three techniques demonstrated comparable long-term outcomes.
Conclusions
This study demonstrates that B-TUEP, ThuLEP, and RASP are all effective for treating large-volume BPH, with comparable improvements in LUTS, urinary flow, and medication-free survival over 12 months. Each technique offers unique advantages—ThuLEP for lower postoperative pain, RASP for reduced infection risk, and B-TUEP for procedural efficiency. These findings highlight the value of individualized surgical planning based on patient characteristics and preferences, supporting all three as viable options for managing large prostates in older adults.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roehrborn CG. Benign prostatic hyperplasia: an overview. Rev Urol. 2005;7(Suppl 9):S3–S14.
2. Parsons JK. Benign prostatic hyperplasia and male lower urinary tract symptoms: epidemiology and risk factors. Curr Bladder Dysfunct Rep. 2010;5(4):212–218. doi:10.1007/s11884-010-0067-2
3. Lerner LB, McVary KT, Barry MJ, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline part I—initial work-up and medical management. J Urol. 2021;206(4):806–817. doi:10.1097/JU.0000000000002183
4. Roehrborn CG. Pathology of benign prostatic hyperplasia. Int J Impot Res. 2008;20(Suppl 3):S11–S18. doi:10.1038/ijir.2008.55
5. Davidian MH. Guidelines for the treatment of benign prostatic hyperplasia. US Pharm. 2016;41:36–40.
6. Karki K, Gautam S, Kandel P, et al. Complications of transurethral resection of the prostate in a tertiary care hospital: a descriptive cross-sectional study. Int Arch Urol Complic. 2023;9:087. doi:10.23937/2469-5742/1510087
7. Brierly RD, Mostafid H, Biyani CS, et al. Is transurethral resection of the prostate safe and effective in the over 80-year-old male? BJU Int. 2001;87(6):516–519. doi:10.1046/j.1464-410x.2001.00108.x
8. de Lucia C, Femminella GD, Rengo G, et al. Risk of acute myocardial infarction after transurethral resection of prostate in older adults. BMC Surg. 2013;13(Suppl 2):S35. doi:10.1186/1471-2482-13-S2-S35
9. Krause P, Schmid HP, Kessler TM, et al. Transurethral resection of the prostate in 85+ patients: a multicentre retrospective study. World J Urol. 2022;40(2):403–409. doi:10.1007/s00345-022-04179-w
10. Deininger S, Dieplinger AM, Lauth W, et al. Functional outcome and safety of endoscopic treatment options for benign prostatic obstruction (BPO) in patients ≥75 years of age. J Clin Med. 2024;13(6):1561. doi:10.3390/jcm13061561
11. Parsons JK, Dahm P, Köhler TS, et al. Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline amendment 2020. J Urol. 2020;204(4):799–804. doi:10.1097/JU.0000000000001298
12. Gravas S, Cornu JN, Drake MJ, et al. Management of non-neurogenic male lower urinary tract symptoms (LUTS): EAU guidelines 2022. Eur Urol. 2022;82(1):1–15. doi:10.1016/j.eururo.2022.03.003
13. Umari P, Fossati N, Gandaglia G, et al. Robotic-assisted simple prostatectomy versus holmium laser enucleation of the prostate for lower urinary tract symptoms in patients with large volume prostate: a comparative analysis from a high-volume center. J Urol. 2017;197(4):1108–1114. doi:10.1016/j.juro.2016.10.049
14. Zengin K, Tanik S, Yucel B, et al. A comparison of thulium laser enucleation of the prostate and open prostatectomy: a prospective randomized clinical study. Urolithiasis. 2016;44(6):525–531. doi:10.1007/s00240-016-0911-5
15. Umari P, Lissiani A, Lissiani A, et al. Comparison of holmium and thulium laser enucleation of the prostate: results from a single-center series. Asian J Androl. 2021;23(1):79–83. doi:10.4103/aja.aja_65_20
16. Bertolo R, Garisto J, Dagenais J, et al. Robotic-assisted simple prostatectomy versus open simple prostatectomy: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2020;23(3):446–455. doi:10.1038/s41391-020-0218-9
17. Hou CP, Lin YH, Yang PS, et al. Clinical outcome of endoscopic enucleation of the prostate compared with robotic-assisted simple prostatectomy for prostates larger than 80 cm3 in aging male. Am J Mens Health. 2021;15(6):1–10. doi:10.1177/15579883211064128
18. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
19. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655. doi:10.1097/00000421-198212000-00014
20. Oelke M, Bachmann A, Descazeaud A, et al. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2013;64(1):118–140. doi:10.1016/j.eururo.2013.03.004
21. Liu C, Zheng S, Li H, Xu K. Transurethral enucleation and resection of the prostate in patients with benign prostatic hyperplasia by plasma kinetics. J Urol. 2010;184(6):2440–2445. doi:10.1016/j.juro.2010.07.023
22. Leslie S, de Castro Abreu AL, Chopra S, et al. Transvesical robotic simple prostatectomy: initial clinical experience. Eur Urol. 2014;66(2):321–329. doi:10.1016/j.eururo.2013.12.058
23. Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70(3):195–283. doi:10.2146/ajhp120568
24. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
25. McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185(5):1793–1803. doi:10.1016/j.juro.2011.01.074
26. Huang X, Wang XH, Wang HP, Qu LJ. Comparison of the microvessel diameter of hyperplastic prostate and the coagulation depth achieved with mono- and bipolar transurethral resection of the prostate: a pilot study on hemostatic capability. Scand J Urol Nephrol. 2008;42(3):265–268. doi:10.1080/00365590801965897
27. Maddox MM, Pareek G, Al Ekish S, et al. Histopathologic changes after bipolar resection of the prostate: depth of penetration of bipolar thermal injury. J Endourol. 2012;26(11):1367–1371. doi:10.1089/end.2012.0272
28. Bozzini G, Berti L, Annunziata S, et al. Histological effects of thulium laser prostate enucleation: evaluation of thermal injury depth. J Endourol. 2018;32(5):389–394. doi:10.1089/end.2017.0835
29. Matsukawa Y, Yoshida S, Fujita K, et al. Risk factors for postoperative febrile urinary tract infection after endoscopic prostate surgery: influence of intravesical pressure and irrigation. J Urol. 2017;198(2):373–379. doi:10.1016/j.juro.2017.02.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.