Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Comparative Analysis of Adverse Drug Reactions Associated with Fluoroquinolones and Other Antibiotics: A Retrospective Pharmacovigilance Study
Authors Alshareef H ![]() , Alenzi KA, Albalawi BR, Alanazi RM, Albalawi NS, Alasoufi WS, Alqifari S
, Alenzi KA, Albalawi BR, Alanazi RM, Albalawi NS, Alasoufi WS, Alqifari S ![]() , Ahmed R, Ali MAS
, Ahmed R, Ali MAS ![]()
Received 17 October 2024
Accepted for publication 28 January 2025
Published 5 February 2025 Volume 2025:17 Pages 51—62
DOI https://doi.org/10.2147/DHPS.S497112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rajender Aparasu
Hanan Alshareef,1 Khalidah A Alenzi,2 Budor R Albalawi,3 Rinas M Alanazi,3 Nawal S Albalawi,3 Wedad Saleem Alasoufi,3 Saleh Alqifari,1 Rehab Ahmed,4 Mostafa AS Ali1
1Pharmacy Practice Department, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 2Transformation and Business Development, Tabuk Health Cluster, Tabuk, Saudi Arabia; 3Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 4Division of Microbiology, Immunology and Biotechnology, Department of Natural Products and Alternative Medicine, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia
Correspondence: Hanan Alshareef, Pharmacy Practice Department, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia, Email [email protected]
Background: Fluoroquinolones (FQs) are among the most popular antimicrobials that are highly effective against various infections. Although FQs are the most frequently used and generally tolerated, there are issues with their safety. This study assessed the rate, severity, seriousness, outcomes, and types of FQs adverse drug reactions (ADRs) in reports submitted to a regional spontaneous ADR database.
Methods: This was a retrospective cross-sectional observational study involving all patients with reported ADRs related to FQs or other antibiotics (ABs) that were submitted to the Regional Pharmacovigilance Center (PVC) database between January 2019 and December 2022. Data were extracted in the form of Saudi ADR from the PVC database, which is consistent with the MedWatch ADR form of the U.S Food and Drug Authority (FDA).
Results: In total, 605 ADRs related to antibiotic use were reported. ADRs caused by FQs use were the most frequently reported (177; 29.3%), followed by penicillin (100; 23.4%) and cephalosporin (90; 21%). There was no significant difference in ADRs caused by FQs between men (104; 58%) and women (OR 1.17, 95% CI 0.82– 1.67, p=0.386). FQ-related ADRs were more frequent among those over 40 years-old (OR 1.56, 95% CI 1.09– 2.22, p=0.015). Most of the detected FQ-related ADRs were of moderate severity (157; 88.7%), required interventions (83; 46.9%), and recovered after receiving medical interventions (154; 87%). Patients who received FQs were fourfold more likely to experience neurological adverse events (OR 4.15, 95% CI 2.48– 6.93, p < 0.001).
Conclusion: The FQs drug class exhibited a higher incidence of ADRs than other ABs. Regularly assessing the safety of ABs is crucial to improve public and healthcare providers’ awareness of the correct utilization of ABs and to limit the use of FQs to infections that cannot be effectively managed with alternative ABs.
Keywords: adverse drug reactions (ADRs), fluoroquinolones (FQs), antibiotics (ABs), pharmacovigilance
Introduction
Adverse Drug Reactions (ADRs) are defined as unintended and unpleasant responses associated with the use of a medicinal product for diagnosis, prevention, or treatment, where a probable causal link exists between the drug and the adverse event.1,2 Severe ADRs pose a serious public health risk which lead to fatalities and life-threatening conditions.3 Additionally, severe ADRs, such as renal and liver failure, result in recall of drug products.4,5 Nevertheless, the avoidance of ADRs is challenging owing to a lack of knowledge about ADRs and the unpredictable nature of some ADRs, which raises the expense of drug development and increases failure rates in clinical trials.1,2 Therefore, to improve patient drug safety and reduce risks to pharmaceutical companies, it is necessary to obtain complete and reliable information on ADRs.6 Recognizing the pharmacological mechanisms responsible for ADRs and identifying high-risk patient subgroups are crucial steps for addressing and resolving ADRs.1,2
Fluoroquinolones (FQs) are among the most commonly prescribed antimicrobials that are well-tolerated and highly effective against different types of infections because of their broad-spectrum effectiveness against Gram-positive and Gram-negative bacteria.7–9 Additionally, FQs have excellent pharmacokinetic properties, including high oral bioavailability and a large volume of distribution, and act by inhibiting DNA topoisomerases that are crucial for bacterial DNA replication and transcription.8–10 They demonstrate minimal inhibition of human and host enzymes and have an excellent safety record.10
FQs have been widely prescribed for several types of infections including urinary tract infections (UTI), pneumonia, and tuberculosis (TB).11 Nevertheless, the inappropriate use of antibiotics (ABs) has resulted in increased resistance and ADRs, resulting in increased medical costs, prolonged hospital stays, and increased mortality.7,12,13 Although FQs are generally well tolerated and extensively prescribed, concerns have been raised regarding their safety outcomes.11 The most commonly reported ADRs were mild and reversible and led to discontinuation in less than two percent of patients.11 However, FQs are also associated with serious ADRs, such as recurrent Clostridium difficile infections (CDI), cardiovascular toxicity, musculoskeletal, renal, and liver disorders, and reactions involving the central nervous system (CNS).7,8,10,11,14 The incidence of ADRs resulting in emergency department visits from FQs is 9.2 per 10,000 prescriptions, surpassing the rates associated with other ABs, such as macrolides and cephalosporins.15
Fluoroquinolone-associated adverse events have led to increased scrutiny and regulatory actions, including the implementation of boxed warnings (BW) by the US Food and Drug Administration (FDA), and the European Medicines Agency.7,11 The FDA has issued multiple reports and BW against FQs owing to their potential for severe and long-lasting ADRs affecting the nervous system, muscles, and joints.7,11 Despite these warnings and substantial evidence of ADRs, FQs continue to be inappropriately prescribed in various healthcare settings.16,17 Therefore, they should only be used when their benefits outweigh the risks and alternative options are not available.7,11,18 The economic impact of serious FQ-related ADRs, which can be life-threatening, has been underestimated.18 Studies have shown that BW has little to no impact on prescription patterns owing to a lack of knowledge among healthcare professionals.16,17
The Saudi Food and Drug Authority (SFDA) initiated pharmacovigilance activities that include monitoring ADRs reported for any registered product during its marketing to the National Pharmacovigilance Center.19 They monitor spontaneously reported ADRs from healthcare providers or consumers at the national level.19 Multiple studies have analyzed the pattern of ADRs reports in Saudi Arabia;20–22 however, to our knowledge, no study has specifically analyzed the pattern of reported FQs ADRs in Saudi Arabia. Therefore, this study aimed to assess the rate, severity, seriousness, outcomes, and types of FQs ADRs submitted to the regional spontaneous ADR database, in comparison with other ABs.
Methods
Study Design
This retrospective cross-sectional pharmacovigilance study involved all FQs and other antibiotics ADRs reports submitted to the Tabuk Regional Pharmacovigilance Center (PVC) database.
Data Source
The Tabuk Regional PVC database received electronically reported ADRs for all events across Tabuk regional hospitals in Saudi Arabia. The PVC database was structured based on the ADRs reporting form provided by the SFDA,23,24 which is similar to the MedWatch ADR Form.4,25 Each report contained detailed information, including age, sex, description, seriousness, time at which the event started and ended, duration of use of the suspected drug, recovery, and reaction outcomes. In addition, the Naranjo algorithm was used to assess the causality of the ADRs.26
Study Population
The study population consisted of patients with reported ADRs related to FQs or other ABs identified in the PVC database between January 2019 and December 2022. Any non-antibiotic-related ADRs reports or ADRs reports related to topical use of FQs or other ABs were excluded. The analysis plan is illustrated in Figure 1.
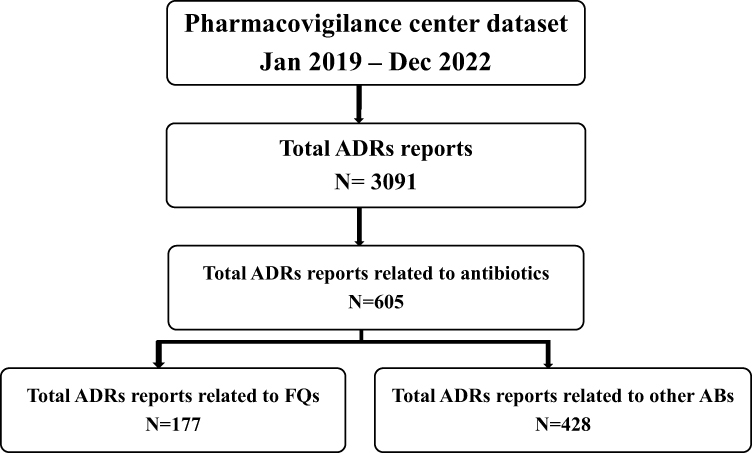 |
Figure 1 Flowchart depicting the analyzed ADR reports from the regional pharmacovigilance database. |
Study Outcomes
The primary outcome of the study was the rate of FQs ADRs reported to the PVC compared to other ABs. Secondary outcomes included severity, seriousness, outcomes, and types of ADRs.
Definitions
Fluoroquinolone antibiotics include the systemic use of (ciprofloxacin, moxifloxacin, and levofloxacin). Other ABs include: all systemically used ABs such as (Penicillin, Cephalosporins, Carbapenem, Aminoglycosides, Glycopeptides, Macrolides, Sulfonamides).
According to the SFDA guidance on ADRs reporting,27 severity describes the intensity of a reaction as mild, moderate, severe, or lethal, whereas seriousness describes the action criteria that are performed after ADRs events, such as hospitalization, prolonged hospitalization, need intervention, life-threatening, or death. Outcomes describe patient status after discontinuing the causative agent, whether the patient recovered, or not. A causality assessment was performed using the Naranjo algorithm.26
Statistical Analysis
Standard descriptive statistics including frequencies and percentages were used to describe categorical data such as patient demographics, severity, seriousness, and ADR outcomes. Univariate logistic regression was performed to determine the odds ratios (ORs) with 95% confidence intervals (CIs) of the potential factors that may be associated with FQ-related ADRs, and to compare the magnitude of severity and outcomes of FQ-related ADRs using other ABs as comparators. The odds of ADR events in patients exposed to FQs were compared with those of other ABs. Only variables with a significance level of p value less than 0.05 were deemed as significant predictors. The post-hoc Bonferroni p-value adjustment was applied to variables with more than two levels and a significant result to determine where the significance lies (0.05/number of comparisons). Data analyses were performed using the SPSS software version 22 (SPSS Inc).
Results
During the study period, 3,091 ADRs were reported to the PVC. Of these, 605 (19.6%) were related to systemic antibiotic therapy. FQs were the highest reported class associated with ADRs (177; 29.3%), whereas 428 (70.7%) ADRs were reported for all other ABs (Table 1). Other than FQs, the antibiotic class with the most frequent reports of ADRs was penicillin (100; 23.4%), followed by cephalosporins (90; 21%). Males were affected by FQs use slightly more frequently than females (104; 58.8%), although this difference was not statistically significant (p=0.386). The proportion of ADRs related to each age group is presented in Table 1, with the age group between 31–40 years old having the highest incidence of ADRs associated with FQs (47; 26.6%).
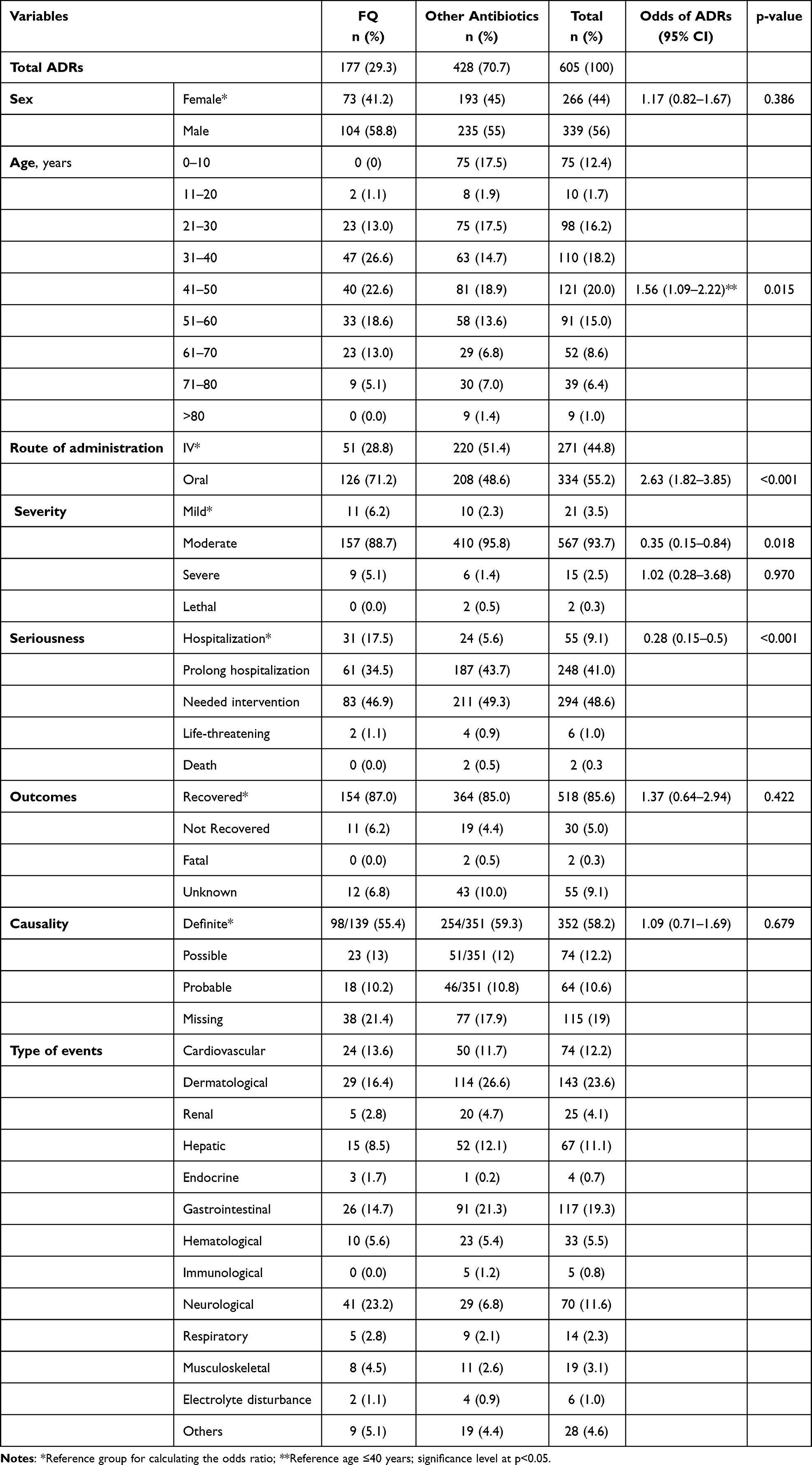 |
Table 1 Analysis of ADRs Caused by FQs and Other Antibiotics |
Compared to other ABs, patients aged >40 years were significantly more likely to experience FQ-related ADRs than those aged ≤40 years (OR 1.56, 95% CI 1.09–2.22, p=0.015). Additionally, oral administration of FQs was more likely to induce ADRs than intravenous (IV) administration (OR 2.63, 95% CI 1.82–3.85, p=0.015). The reported ADRs for each event type are shown in Supplementary Table 1.
Table 2 describes the proportion of ADR reports pertaining to individual antibiotic and types of events. Among all ADRs reports, ciprofloxacin was the most commonly reported antibiotic (100; 16%), followed by amoxicillin-clavulanic acid (63; 10.4%) and levofloxacin (50; 8.3%). The distributions of the individual FQ-related ADRs among the different variables are shown in Figure 2a and b.
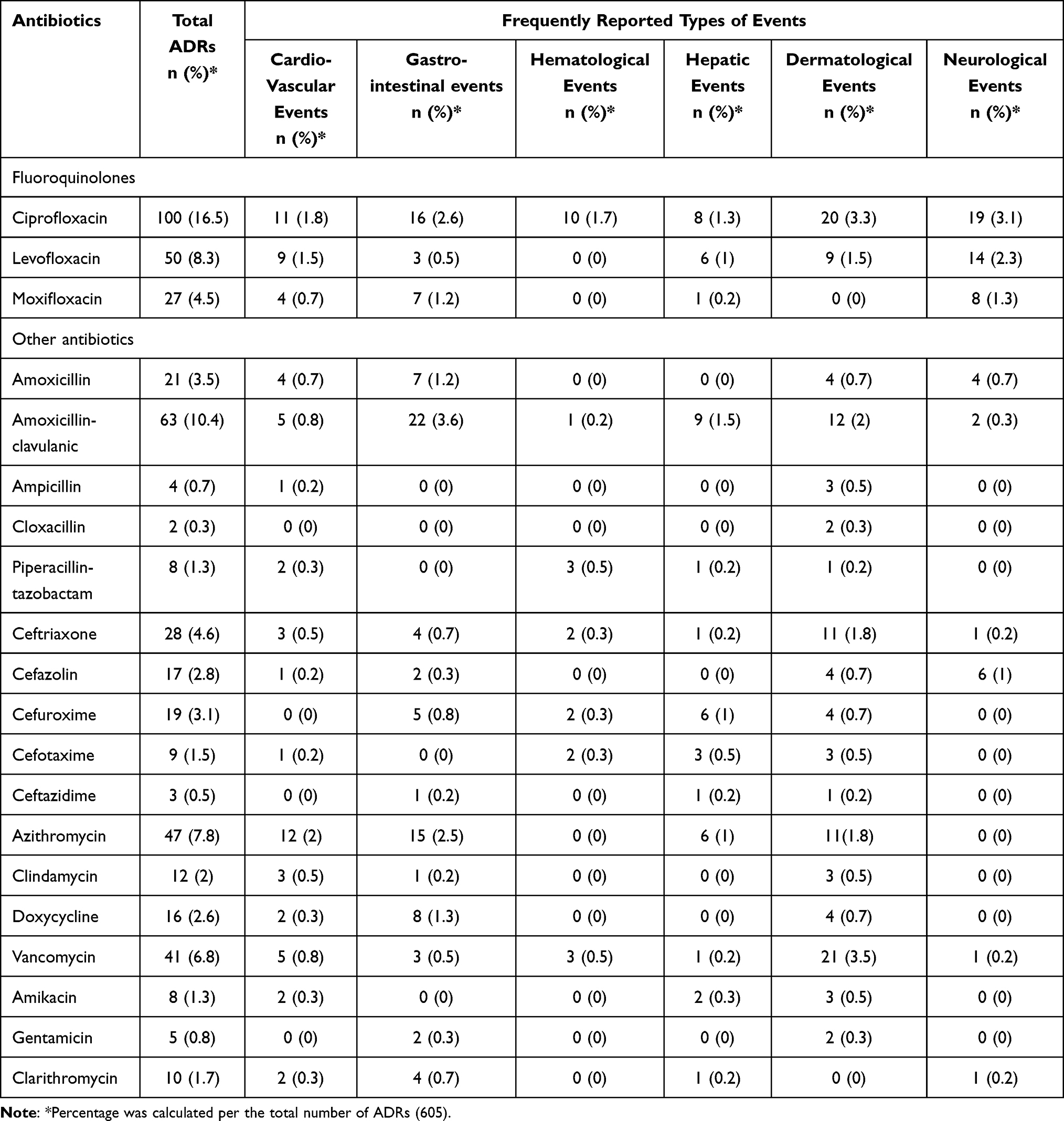 |
Table 2 Types of ADRs Events per Individual Antibiotic Therapy |
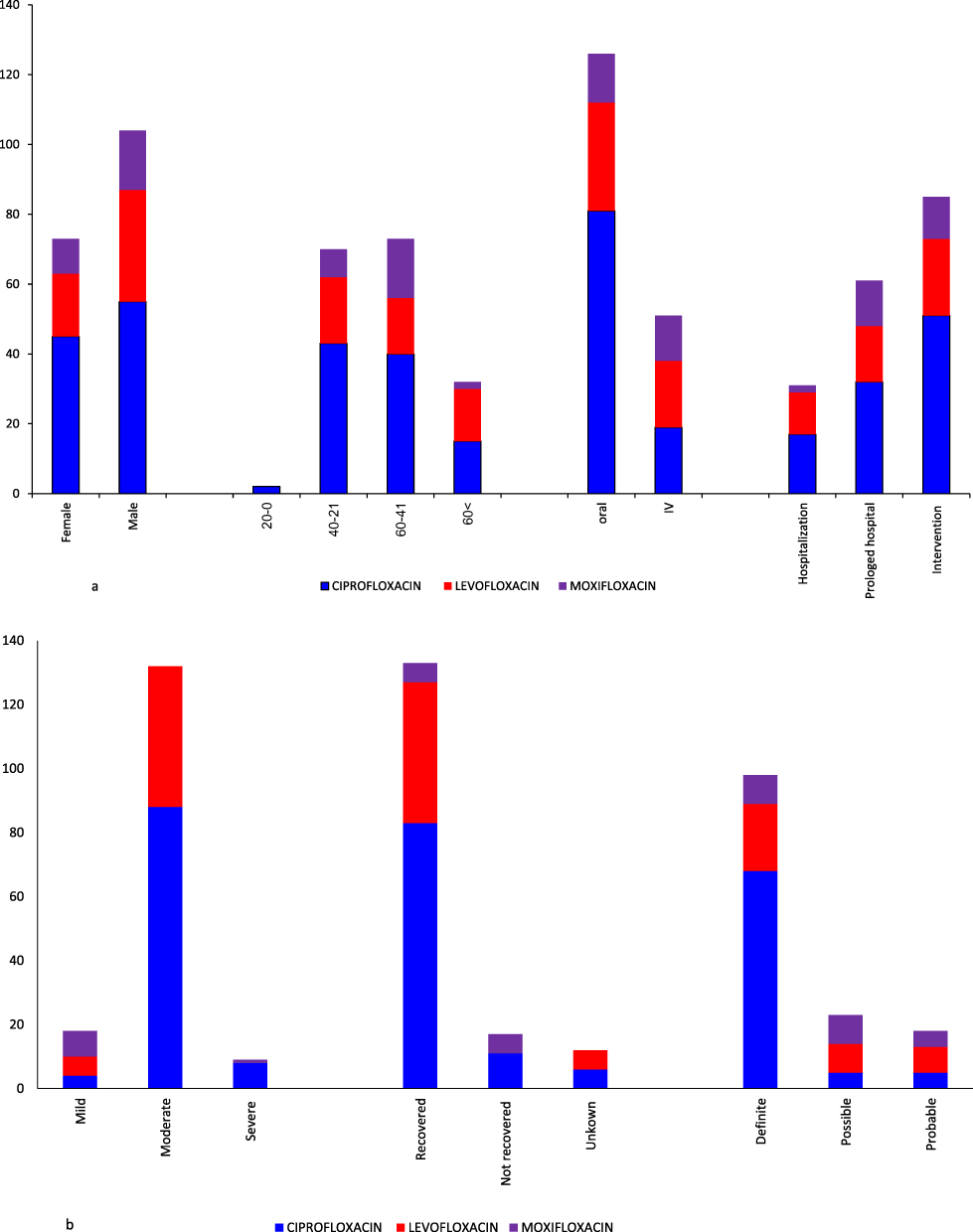 |
Figure 2 (a) Distribution of ADRs for individual FQs by patient demographics and seriousness. (b) Distribution of ADRs for individual FQs by severity, outcomes and Naranjo scale. |
Similar to other ABs, the majority of the detected ADRs of the FQs were of moderate severity (157; 88.7%), and only (9; 5.1%) were classified as severe ADRs. Eight severe FQ-related ADRs were reported in the patients who received ciprofloxacin (Figure 1). There were no reported lethal cases related to FQs compared with two lethal ADRs (0.5%) associated with cephalosporin ABs (Table 1).
Regarding seriousness, only two FQs-related ADRs (1.1%) were reported as life-threatening due to bone marrow suppression and agranulocytosis, 83 patients (46.9%) required interventions, and the remaining ADRs required hospitalization (initial or prolonged). FQs were less likely to cause serious ADRs that required prolonged hospitalization or were life-threatening compared with other ABs (OR 0.28, 95% CI 0.15–0.50, p <0.001). In the other ABs group, only two patients died during hospitalization, both of which were related to anaphylactic reactions after intravenous cefazolin administration, while no patient died due to FQs ADRs, as illustrated in Table 1. Post-hoc tests showed non-significant life-threatening ADRs between FQs and other ABs. Moreover, the occurrence of mild and severe ARDs was not significantly different between FQs and other ABs.
Similar to other ABs in the outcome analysis, most FQ-related ADRs completely recovered (154; 87%). Only (11; 6.2%) patients did not recover and there were no fatalities from the FQs (Table 1). There was no significant difference between the unrecovered cases of FQ-related ADRs and those of other ABs (OR 1.37, 95% CI 0.64–2.94, p =0.42). The estimated Naranjo scores for causality assessment revealed that (98; 55.4%) of the FQs ADRs were definite (Table 1).
As detailed in Table 1, neurological events were the most commonly reported adverse events associated with FQs (41; 23.2%), followed by dermatological (29; 16.4%) and gastrointestinal (26; 14.7%) events. The most commonly reported ADRs for other ABs were dermatological (143; 26.6%), gastrointestinal (117; 21.3%), and cardiovascular (74; 11.7%) events.
As shown in Table 3, patients who were prescribed FQs were fourfold more likely to experience significant neurological adverse events (OR 4.15; 95% CI 2.48–6.93, p <0.001) than those who were prescribed other ABs. The odds of experiencing dermatological events were significantly lower for FQs than for other ABs. There were no significant differences in cardiovascular, gastrointestinal, or hepatic ADRs between the FQs and other ABs.
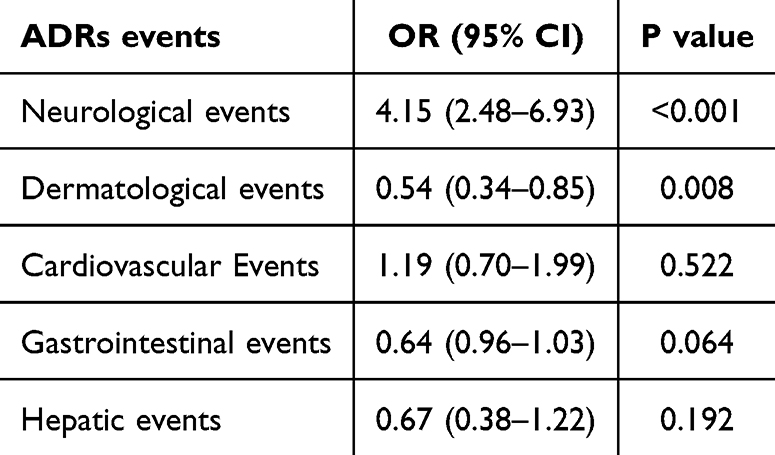 |
Table 3 Odds Ratio and 95% Confidence Interval for FQs ADRs Events vs Other Antibiotics |
As shown in Supplementary Table 2 Ophthalmic ADRs associated with FQs (7 events) were grouped under the “Other” category, rather than the neurological category. Although some ophthalmic effects, such as diplopia, may be linked to extraocular muscle tendinopathy, we acknowledge that these events were not specifically categorized as neurological.
Discussion
Spontaneous reporting of ADRs provides significant scientific value by offering insights into new drug-related adverse effects and the potential generation of early signals.28 Our study offers valuable insights into the evaluation of antibiotic-associated ADRs and highlights the need for caution in prescribing FQs antibiotics, given the range of ADRs associated with these drugs. The study showed that, among all suspected antibiotic-related ADRs, a higher percentage was linked to the use of FQs, constituting 29.3% of all reported ADRs. Ciprofloxacin was the most frequent causative agent among all ABs (16.5%). The findings of this study are consistent with a recent cross-sectional study conducted in Saudi Arabia that analyzed all ADR reports, including ABs over one year.22 They demonstrated that, among the reported cases, FQs were among the top ten suspected drugs causing ADRs (14.9%), with the highest reported events for ciprofloxacin.22 Regional studies examining antimicrobial consumption and prescribing patterns across outpatient, inpatient, and emergency department settings in regional hospitals have reported the highest and most frequent antimicrobial consumption of third-generation cephalosporins (eg ceftriaxone and ceftazidime), aminoglycosides (eg gentamicin), and macrolides (eg azithromycin).29–32 Based on the overall antibiotic prescribing rates, our finding suggested that fluoroquinolone ADRs may have a significantly greater impact.
Our study found no significant association between FQ-related ADRs and patient sex. However, in different scenarios, the existing literature provides evidence of sex variations in clinically significant ADRs owing to the underlying physiological and pharmacological variations in drug disposition and metabolism between males and females.33 Some studies have suggested that chromosomal, hormonal, and pharmacokinetic changes increase the incidence of ADRs in women compared to that in men.10,33,34
Higher rates of ADRs have been linked to older patients due to age-related variables, including changes in drug pharmacokinetics and pharmacodynamics, comorbidities, polypharmacy, and frailty.35 Our results indicated that patients aged >40 years were significantly more likely to experience FQ-related ADRs than those aged ≤40 years. However, this finding should be interpreted cautiously, as the observed association may be partially explained by the higher prescribing rates in this age group rather than increased susceptibility. Further research incorporating prescribing data is necessary to confirm age-related susceptibility to FQ-related ADRs. Notably, no FQ-related ADRs were observed in pediatric patients, likely because of the restricted use of FQs in children due to safety concerns,36 which reflects the rational prescription of FQs antibiotics. Pharmacovigilance studies in the pediatric age group showed that the most frequently reported ADRs were ABs and vaccines.37
In this study, the ADRs for both FQs and other ABs were of moderate severity and required interventions or prolonged hospitalization in which patients received appropriate medical care and then recovered. This finding is consistent with that of a previous study in Malaysia.38 In our study, fewer reactions were severe, two were life-threatening, and none were fatal. Life-threatening ADRs are caused by ciprofloxacin-induced agranulocytosis and bone marrow suppression. Case reports have shown that bone marrow suppression returned to normal with the cessation of ciprofloxacin treatment; however, in one patient, irreversible bone marrow suppression led to severe thrombocytopenia and hemorrhage.39,40
The current study highlighted that FQs use was associated with an increased risk of neurological adverse events, followed by dermatological and gastrointestinal events. FQs have been associated with an increased risk of peripheral neuropathy and central nervous system (CNS) effects, such as encephalopathy, confusion, and psychosis.41,42 In a systematic review and meta-analysis of 39 randomized controlled trials for patients receiving oral FQs or other antimicrobials through primary healthcare centers, FQs were associated with significantly higher neurological and gastrointestinal ADRs than other ABs, while dermatological events were not significant.43 In contrast, a recently published study on quinolone-related spontaneous ADRs reports in Italy showed that the use of third-generation FQs (ie levofloxacin and moxifloxacin) was associated with a high probability of musculoskeletal events, followed by neurological and psychiatric events. The study further revealed that patients aged over 60 years had a higher incidence of musculoskeletal events when treated with FQs.44 Nonetheless, in our study, ciprofloxacin exhibited elevated rates of dermatological, neurological, and gastrointestinal events when compared to levofloxacin and moxifloxacin. This discrepancy may stem from the widespread prescription of ciprofloxacin, owing to its lower cost and greater availability, leading to a higher volume of ciprofloxacin prescriptions. Previous studies in Saudi Arabia have reported that ciprofloxacin was the most frequently used and prescribed quinolone antibiotic, available in oral solid and liquid forms, eye drops, and parenteral formulations.16,45,46 These studies revealed inadequate knowledge among healthcare professionals regarding the indications for FQs, and highlighted a high percentage of inappropriate outpatient ciprofloxacin prescriptions.16,45,46
FQ-related ADRs can be limited by educating the public about the misuse or overuse of FQs and by educating healthcare providers about rational prescribing. Regular monitoring of ADRs helps identify risk factors, reduce future incidences, and promote patient safety. The implementation of antimicrobial stewardship is likely to reduce overall antibiotic prescriptions, and consequently optimize patient safety and decrease antimicrobial resistance. Antimicrobial stewardship programs aimed at regulating FQs prescriptions have been linked to reduced use during hospitalization and discharge, thereby reducing ADRs.47,48 However, our study did not observe any ADRs for FQs prescriptions at the time of discharge. Healthcare providers should carefully consider the risks and benefits of FQs use, especially for common conditions such as uncomplicated urinary tract infections, where alternative antibiotic options may be available.49
The strength of the current study is that the ADRs data were collected from the regional pharmacovigilance center, in which ADR data are not routinely publicly available and that the findings were consistent with observations from other countries. However, our study had several limitations. Data were collected from the Tabuk Regional Pharmacovigilance Center database, one region of Saudi Arabia. However, this study analyzed a large amount of data from hospitals and primary care centers in the Tabuk region. Replication of our results to other regions among diverse populations is necessary to enhance the impact of our findings and to inspire positive changes. This retrospective study was based on continuous reports of patients, physicians, and pharmacists. Thus, our approximations of antibiotic-related ADRs were likely underestimated because some well-known ADRs may have been under-reported. The received dataset did not account for potential drug interactions with other medications that patients may have been taking at the time of the reported ADRs. Drug interactions may have contributed to some of the observed ADRs and highlight the need for caution when interpreting the results. Additionally, we encountered missing data on the length of hospital stay, comorbidities, and polypharmacy which should be assessed regularly to enhance and improve causality assessment and the quality of the database.
Conclusion
The FQs class was associated with the greatest number of ADRs compared with other ABs in the pharmacovigilance database, particularly in patients above 40 years of age. Neurological adverse effects are common which warns healthcare providers to weigh the risks and benefits when prescribing FQs or to restrict their use to infections that cannot be easily managed with other ABs. These findings underscore the importance of close monitoring and appropriate use of these ABs to mitigate the risks associated with their use.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author; however, restrictions apply to the availability of these data, which were used under license for the current study, and thus are not publicly available. However, the data are available from the authors upon reasonable request and with permission from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by Tabuk Institutional Review Board, Tabuk, Saudi Arabia (IRB Protocol No: TU-077/023/215). The study complied with the principles of the Declaration of Helsinki. Participants’ confidentiality was strictly maintained, and the data were received as anonymous electronic database records without identity information. The requirement for informed consent was exempted by ethics committee due to the retrospective observational nature of the study. After IRB approval, the Tabuk Regional Pharmacovigilance Center granted permission to access and utilize the data.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Patton K, Borshoff DC. Adverse drug reactions. Anaesthesia. 2018;73(S1):76–84. doi:10.1111/ANAE.14143
2. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet. 2000;356(9237):1255–1259. doi:10.1016/S0140-6736(00)02799-9
3. Montastruc JL, Lafaurie M, de Canecaude C, et al. Fatal adverse drug reactions: a worldwide perspective in the world health organization pharmacovigilance database. Br J Clin Pharmacol. 2021;87(11):4334–4340. doi:10.1111/BCP.14851
4. MedWatch: the FDA safety information and adverse event reporting program | FDA. Available from: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program.
5. Gallo K, Goede A, Eckert O-A, Gohlke B-O, Preissner R. Withdrawn 2.0—update on withdrawn drugs with pharmacovigilance data. Nucleic Acids Res. 2023;2023:1–5. doi:10.1093/NAR/GKAD1017
6. Khalil H, Huang C. Adverse drug reactions in primary care: a scoping review. BMC Health Serv Res. 2020;20(1). doi:10.1186/S12913-019-4651-7
7. Baggio D, Ananda-Rajah MR. Fluoroquinolone antibiotics and adverse events. Aust Prescr. 2021;44(5):161. doi:10.18773/AUSTPRESCR.2021.035
8. Millanao AR, Mora AY, Villagra NA, Bucarey SA, Hidalgo AA. Biological effects of quinolones: a family of broad-spectrum antimicrobial agents. Molecules. 2021;26(23). doi:10.3390/MOLECULES26237153
9. Chan T, Bunce PE. Fluoroquinolone antimicrobial drugs. CMAJ. 2017;189(17):E638. doi:10.1503/CMAJ.160938
10. Tomé AM, Filipe A. Quinolones: review of psychiatric and neurological adverse reactions. Drug Saf. 2011;34(6):465–488. doi:10.2165/11587280-000000000-00000/FIGURES/TAB4
11. Fluoroquinolone Antimicrobial Drugs Information | FDA. Available from: https://www.fda.gov/drugs/information-drug-class/fluoroquinolone-antimicrobial-drugs-information.
12. Werner NL, Hecker MT, Sethi AK, Donskey CJ. Unnecessary use of fluoroquinolone antibiotics in hospitalized patients. BMC Infect Dis. 2011;11(1):1–7. doi:10.1186/1471-2334-11-187/TABLES/3
13. Donskey CJ. Fluoroquinolone restriction to control fluoroquinolone-resistant Clostridium difficile. Lancet Infect Dis. 2017;17(4):353–354. doi:10.1016/S1473-3099(17)30052-X
14. Hayashi PH, Chalasani NP. Liver injury in the elderly due to fluoroquinolones: should these drugs be avoided? CMAJ. 2012;184(14):1555–1556. doi:10.1503/CMAJ.121270
15. Shehab N, Patel PR, Srinivasan A, Budnitz DS. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008;47(6):735–743. doi:10.1086/591126
16. Mallhi TH, Alanazi AS, Khan YH, et al. Assessment of knowledge regarding safety profile, use, and boxed warnings of fluoroquinolones among healthcare professionals in Saudi Arabia: a potential implication for drug regulatory authorities. Front Med. 2022;9:816320. doi:10.3389/FMED.2022.816320/BIBTEX
17. Buehrle DJ, Wagener MM, Clancy CJ. Outpatient fluoroquinolone prescription fills in the United States, 2014 to 2020: assessing the impact of food and drug administration safety warnings. Antimicrob Agents Chemother. 2021;65(7). doi:10.1128/AAC.00151-21
18. Kuula LSM, Backman JT, Blom ML. Healthcare costs and mortality associated with serious fluoroquinolone‐related adverse reactions. Pharmacol Res Perspect. 2022;10(2). doi:10.1002/PRP2.931
19. Drug safety initiatives | Saudi food and drug authority. Available from: https://www.sfda.gov.sa/en/drug-safety-initiatives.
20. Bin Yousef N, Yenugadhati N, Alqahtani N, et al. Patterns of adverse drug reactions (ADRs) in Saudi Arabia. Saudi Pharm J SPJ off Publ Saudi Pharm Soc. 2022;30(1):8–13. doi:10.1016/J.JSPS.2021.08.014
21. Alayed N, Alkhalifah B, Alharbi M, Alwohaibi N, Farooqui M. Adverse drug reaction (adr) as a cause of hospitalization at a government hospital in Saudi Arabia: a prospective observational study. Curr Drug Saf. 2019;14(3):192–198. doi:10.2174/1574886314666190520105330
22. Alenzi KA, Alanazi NS, Almalki M, Alomrani H, Alatawi FO. The evaluation of adverse drug reactions in Saudi Arabia: a retrospective observational study. Saudi Pharm J. 2022;30(6):735–741. doi:10.1016/J.JSPS.2022.03.018
23. Saudi Food & Drug Authority (SFDA). Saudi Vigilance. Adverse Drug Reactions (ADRs) Reporting Form.
24. Report Form - Tiaquz. Available from: https://ade.sfda.gov.sa/Request/AdeRequest.
25. Craigle VM. The FDA safety information and adverse event reporting program. J Med Libr Assoc. 2007;95(2):224–225. doi:10.3163/1536-5050.95.2.224
26. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/CLPT.1981.154
27. Guidance on Adverse Drug Events Reporting for Healthcare Professionals. Available from: https://www.sfda.gov.sa/en/regulations?tags=2.
28. Pal SN, Duncombe C, Falzon D, Olsson S. WHO strategy for collecting safety data in public health programmes: complementing spontaneous reporting systems. Drug Saf. 2013;36(2):75–81. doi:10.1007/S40264-012-0014-6
29. Alomi YA, Almasoudi AH, Alghamdi GA, Abboud NA. Antimicrobial drug consumption in emergency services at North West (Tabuk) Region hospitals, Saudi Arabia. Pharmacol Toxicol Biomed Reports. 2019;5(3):108–112. doi:10.5530/PTB.2019.5.20
30. Almasoudi AH, Alomi YA, Alghamdi GA, Alshahrani RS. Analysis of antimicrobial medications consumption in inpatient units at North West (Tabuk) Region hospitals, Saudi Arabia. Pharmacol Toxicol Biomed Reports. 2019;5(3):130–134. doi:10.5530/PTB.2019.5.24
31. Almasoudi AH, Alomi YA, Alghamdi GA. Antimicrobial drug consumption in ambulatory care settings, Tabuk Region, Saudi Arabia. Pharmacol Toxicol Biomed Reports. 2019;5(3):97–101. doi:10.5530/PTB.2019.5.18
32. Al Matar M, Enani M, Binsaleh G, et al. Point prevalence survey of antibiotic use in 26 Saudi hospitals in 2016. J Infect Public Health. 2019;12(1):77–82. doi:10.1016/J.JIPH.2018.09.003
33. Moyer AM, Matey ET, Miller VM. Individualized medicine: sex, hormones, genetics, and adverse drug reactions. Pharmacol Res Perspect. 2019;7(6):e00541. doi:10.1002/PRP2.541
34. Zucker I, Prendergast BJ. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol Sex Differ. 2020;11(1). doi:10.1186/S13293-020-00308-5
35. Zazzara MB, Palmer K, Vetrano DL, Carfì A, Graziano O. Adverse drug reactions in older adults: a narrative review of the literature. Eur Geriatr Med. 2021;12(3):463–473. doi:10.1007/S41999-021-00481-9
36. Patel K, Goldman JL. Safety concerns surrounding quinolone use in children. J Clin Pharmacol. 2016;56(9):1060. doi:10.1002/JCPH.715
37. Bouquet É, Star K, Jonville-Béra AP, Durrieu G. Pharmacovigilance in pediatrics. Therapie. 2018;73(2):171–180. doi:10.1016/J.THERAP.2017.11.012
38. Arulappen AL, Danial M, Sulaiman SAS. Evaluation of reported adverse drug reactions in antibiotic usage: a retrospective study from a tertiary care hospital, Malaysia. Front Pharmacol. 2018;9(AUG). doi:10.3389/FPHAR.2018.00809
39. Chaudhry M, Tarneja N, Gundale A, Roa D, Levey R. Bone marrow suppression: a side effect of ciprofloxacin therapy. Am J Ther. 2010;17(5):e167–e168. doi:10.1097/MJT.0B013E3181A4695F
40. Dutta TK, Badhe BA. Ciprofloxacin-induced bone marrow depression. Postgrad Med J. 1999;75(887):571–573. doi:10.1136/PGMJ.75.887.571
41. Zareifopoulos N, Panayiotakopoulos G. Neuropsychiatric effects of antimicrobial agents. Clin Drug Investig. 2017;37(5):423–437. doi:10.1007/S40261-017-0498-Z
42. Wierzbiński P, Hubska J, Henzler M, Kucharski B, Bieś R, Krzystanek M. Depressive and other adverse CNS effects of fluoroquinolones. Pharmaceuticals. 2023;16(8):1105. doi:10.3390/PH16081105/S1
43. Tandan M, Cormican M, Vellinga A. Adverse events of fluoroquinolones vs. other antimicrobials prescribed in primary care: a systematic review and meta-analysis of randomized controlled trials. Int J Antimicrob Agents. 2018;52(5):529–540. doi:10.1016/J.IJANTIMICAG.2018.04.014
44. Scavone C, Mascolo A, Ruggiero R, et al. Quinolones-induced musculoskeletal, neurological, and psychiatric ADRs: a pharmacovigilance study based on data from the Italian spontaneous reporting system. Front Pharmacol. 2020:11. doi:10.3389/FPHAR.2020.00428.
45. Ali MD, Patel M, Banu N, Ahmad A, Hassan YA. Drug utilization pattern and cost-effectiveness analysis of five most common antibiotics used in Saudi Arabia. J Pharm Heal Serv Res. 2021;12(2):242–246. doi:10.1093/JPHSR/RMAA019
46. Ahmed NJ. Pattern of ciprofloxacin prescribing at outpatient setting in Al-Kharj. J Pharm Res Int. 2020:62–66. Published online May 30. doi:10.9734/JPRI/2020/V32I830471
47. Suzuki H, Perencevich EN, Alexander B, et al. Inpatient fluoroquinolone stewardship improves the quantity and quality of fluoroquinolone prescribing at hospital discharge: a retrospective analysis among 122 veterans health administration hospitals. Clin Infect Dis. 2020;71(5):1232–1239. doi:10.1093/cid/ciz967
48. Vaughn VM, Gandhi T, Conlon A, Chopra V, Malani AN, Flanders SA. The association of antibiotic stewardship with fluoroquinolone prescribing in Michigan hospitals: a multi-hospital cohort study. Clin Infect Dis. 2019;69(8):1269–1277. doi:10.1093/CID/CIY1102
49. Mathews B, Thalody AA, Miraj SS, Kunhikatta V, Rao M, Saravu K. Adverse effects of fluoroquinolones: a retrospective cohort study in a South Indian tertiary healthcare facility. Antibiot. 2019;8(3):104. doi:10.3390/ANTIBIOTICS8030104
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.