Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Community Acceptance and Utilization of Maternal and Community-Based Neonatal Care Services Provided by Health Extension Workers in Rural Sidama Zone: Barriers and Enablers: A Qualitative Study
Authors Gebretsadik A ![]() , Melaku N
, Melaku N ![]() , Haji Y
, Haji Y ![]()
Received 24 March 2020
Accepted for publication 17 June 2020
Published 1 July 2020 Volume 2020:11 Pages 203—217
DOI https://doi.org/10.2147/PHMT.S254409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Achamyelesh Gebretsadik,1 Nebiyu Melaku,2 Yusuf Haji1
1School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2Maternal and Child Health Core Process, Southern Nation Nationalities and People Regional Health Bureau, Hawassa, Ethiopia
Correspondence: Achamyelesh Gebretsadik
School of Public Health, College of Medicine and Health Sciences, Hawassa University, PO Box 46, Hawassa, Ethiopia
Tel +251 911303128
Email [email protected]
Purpose: This study assessed the community acceptance and utilization of maternal and community-based neonatal care services, its barriers, and enablers in southern Ethiopia, 2019.
Methods: An exploratory qualitative study was conducted among mothers, health extension workers, their supervisors and coordinators in four districts of Sidama Zone, Hawassa University Demographic Surveillance Site. An in-depth interview has been carried out with eight health extension workers and eight program coordinators and supervisors, while four focus group discussions were held with eligible mothers. Digital recording was applied to record the interview and discussion followed by transcription and thematic analysis through open code.
Results: Study findings reveal that services provided by health extension workers at community level for mothers and their children are highly appreciated and recognized by the community. Most of the communities are free from wrong perception regarding the practices. Their performance was better in focused antenatal care, but postnatal care and community-based neonatal care were reported to be insignificant. Knowledge and skills of HEWs was based on their extended experiences. The challenges and opportunities include workload, road inaccessibility, poor supervision, inadequate drugs and equipment supply, shortage of man power and budget at health posts, distance and topography factors of homes from health posts making the visits more difficult, etc. To improve uptake of the services, increasing the number of health extension workers in the heath post, supportive supervision, continuous essential drugsm and medical supplies were suggested by participants.
Conclusion: This study shows that services provided by health extension workers for mothers and their neonates are highly appreciated by the community, and there is better change in focused antenatal care services, but postnatal care and sick newborn care are still low. Therefore, maternal and neonatal programs should focus on the postnatal home visits and sick newborn care through solving identified barriers.
Keywords: knowledge of HEWs, community-based neonatal care, performance, improvement, Sidama, Ethiopia
Introduction
In Ethiopia, the high maternal and newborn morbidity and mortality reduction Road Map aims to scale up skilled attendance during pregnancy, child birth and the postnatal period and increase basic and comprehensive Emergency Obstetric and newborn care (EmONC).1 On top of the above effort, the Ethiopian Federal Ministry of Health (FMOH) launched the innovative Community-Based Neonatal Care (CBNC) strategy in 2012 for the implementation of a sustainable development Goal; this innovative strategy was aimed to improve maternal and neonatal health with the core principle of the CBNC strategy being ensuring the continuum of care, ie from pregnancy to postnatal periods as well as from the home/community to the health facilities. In such a way, CBNC is expected to improve maternal and newborn care practices and care seeking.2
Moreover, FMOH, the Maternal and Child Survival Program – Newborns in Ethiopia Gaining Attention (MCSP-NEGA) project, and country partners developed a Demand Creation Strategy for Maternal Neonatal and Child Health (MNCH)-CBNC that focused on approaches to address the persistent low demand for CBNC. The resulting strategy supported a systems-strengthening approach that built the capacity of zonal, woreda, Primary Health Care Unit (PHCU) and kebele levels to improve MNCH-CBNC with the aim to contribute to reductions in newborn morbidity and mortality in Ethiopia (UNICEF).3
These newly launched programs mainly utilize the Health Extension program (HEP) as key actors. HEP was launched by FMOH in 2003, implemented by the Ethiopian Government with the aim of achieving universal coverage of primary healthcare among its rural population by 2009, in a context of limited resources. The overall goal of HEP is to create a healthy society and to reduce maternal and child morbidity and mortality rates. As key actors for the implementation of the HEP, Health Extension Workers (HEWs) were deployed to kebeles (villages); model families were trained in communities; and the health development armies (HDAs) were deployed.4
There is widespread consensus on the central role that the community health workers (CHWs) can play in ending preventable maternal, newborn, and child deaths.5 For example, in Ethiopia, the intervention strategy to train and deploy HEWs show great promise in increasing access to treatment and care of pregnant women and their newborns and the HEP has been attributed to significantly improving utilization of maternal and newborn health services.6,7 In addition, a study undertaken in Ethiopia on 101 rural districts confirmed the positive effect of HEWs on maternal and neonatal healthcare practices at scale.8 Another report shows an association between a home-based neonatal care and reduction in neonatal and prenatal mortality in settings with high neonatal-mortality rates and poor access to health facility-based care.9 And also, according to Trend in Maternal and Newborn Health Care Practices in Last ten Kilometer (L10K), in Ethiopia, there was a tendency to an increase in maternal, child, and neonatal health service utilization.10 Besides, CHWs’ knowledge increased their acceptance by the community, and home visits by the HCWs were found to reduce neonatal mortality by two thirds.7,11,12
However, HEP success requires innovative approaches from all corners. For example, a study in Ethiopian HEWs suggested ways for achieving higher performance in primary healthcare would be data driven problem-solving, respectful and supportive relationships with the community, and strong support from zonal and regional health bureaus contributing to woreda performance.13 Similarly, a literature review in low- and middle-income countries (LMICs) shows contextual factors influence CHWs’ performance at the CHW level (eg, motivation or competencies), the end-user level (eg, influencing health-seeking behavior), or by influencing broader CHW programme performance.14
Otherwise, the HEP will fail to achieve its objectives. Evidences tell us that the program is not without challenges. Some of identified challenges for the low performance of HEP in Ethiopia include: dissatisfaction among HEWs, poor community acceptance of the HEP, limitations in designing the HEP package and its intervention strategies, inadequate pre-services and in services training of HEWs, inadequate and untimely supportive supervision and systems, poor drug and medical equipment supply and lack of trust, communication, and dialog, and differing expectations.15,20
Similarly, a community survey conducted 2 years ago in the current study area shows low maternal and neonatal services utilization. For example, only 12% of delivered mothers received postnatal home visits from HEWs, the practices of focused antenatal care was lower than expected, and CBNC practices of the woredas was unsatisfactory.21,23
However, no studies in the current area had explored barriers and enablers to the acceptance and uptake of the CBNC program. And these are the entry points to further explore the problems for low service utilization in the study area and, therefore, identification of major challenges and enablers to the acceptance and utilization of maternal and CBNC services by the community will have paramount importance in solving the community’s health problem. Hence, the current study was aimed to explore community acceptance and utilization of the CBNC services and identification of enablers and barriers to the services provided by HEWs and recommending a suggested solution by stakeholders.
Materials and Methods
Study Settings
The study was carried out in four woredas (districts) of Sidama Zone (Shebadino, Boricha, Dale, and Loka Abaya). Sidama Zone is one of the eighteen Zones of SNNPRS which is located in the north eastern part of the region and bordered with Oromiya in the North, East, and South East, Gedieo Zone in the South, and Wolayta Zone in the West. These woredas are the proposed DSS sites of Hawassa University with a total population of 1,099,345 (male 50.3% and female 49.7%) in 2018/19, as projected based on the 2007 National Census, and total households estimated was 162,919. The study area has one district hospital, 42 health centers, and 147 health posts. The common health problems of infants in these woredas are pneumonia followed by neonatal infections.24
Study Population and Design
The study population include: HEWs who have been working in the study areas health posts for at least 1 year. We have included them because they are the service providers and are the main subjects to be evaluated by this study. Another study group was HEP Coordinators. These are health professionals with a BSc or higher level of education coordinating the program at the district level, one person at each district; a HEW Supervisor is the health center to health post linkage focal who supervises HEWs at their respective Health Posts and to whom they report performance on a weekly basis, he is responsible for five health posts; with two HEWs at each health post), and mothers who had given birth to alive babies in the last year prior to the survey (6-<12 months) in the study area. They were chosen for the fact that they are the direct receiver of the MNCH and CBNC services provided by HEWs.
The supervisory team (Woreda HEP coordinators and PHCU HEW supervisors) are involved in all aspects of program management, including planning, implementation, and monitoring and evaluation. Members of the team are trained in skills needed for supportive supervision (facilitation, interpersonal communication, problem-solving, and analytical skills); oriented to various tools and methods (such as peer review and performance assessment tools); and provided with opportunities to frequently upgrade their technical skills. The supervisors are trained in a specially designed curriculum; therefore, they would provide adequate and pertinent information on the subject area.17
An exploratory qualitative study was therefore conducted among mothers, HEWs, and HEW Supervisors and Coordinators. We preferred it to deeply explore feelings, beliefs, opinions, and shared values.
Sampling and Sample Size Determination
Purposive sampling was applied to select 49 study subjects. And a total of 16 in-depth Interviews (IDIs) conducted, of which eight were with HEWs residing/working in the study area for the last 12 months; four were with HEWs Supervisors at the health center level (one health center at each district); and the remaining four were with HEP Coordinators at the district level, one from each district. Focus Group Discussions (FGDs) were further held with a group size of 8–10 mothers of infants (1–12 months) who had resided in the study area for a year and above. The study team purposly selected two HEWs from each of the four districts selected for IDIs, a total of eight, considering resource constraints. From each district one HEP Coordinator and one HEWs supervisor were selected to include in to IDIs, and for the FGDs, mothers with infants of 6 months to less than a year were identified for the study. The FGD mothers were selected from the health posts not included in the study by respective HEWs not participating in the study. Supervisors and coordinators were not participated in selection of mothers for FGDs and HEWs for IDIs, their role was providing lists of health posts and HEWs in their respective catchment area to choose from. We then randomly selected the health posts and respective HEWs. One HEW selected from each health post considering their experience and interest. The FGDs were conducted outside the health facilities. Accordingly, one FGD per district and a total of four FGDs have also been carried out (Table 1).
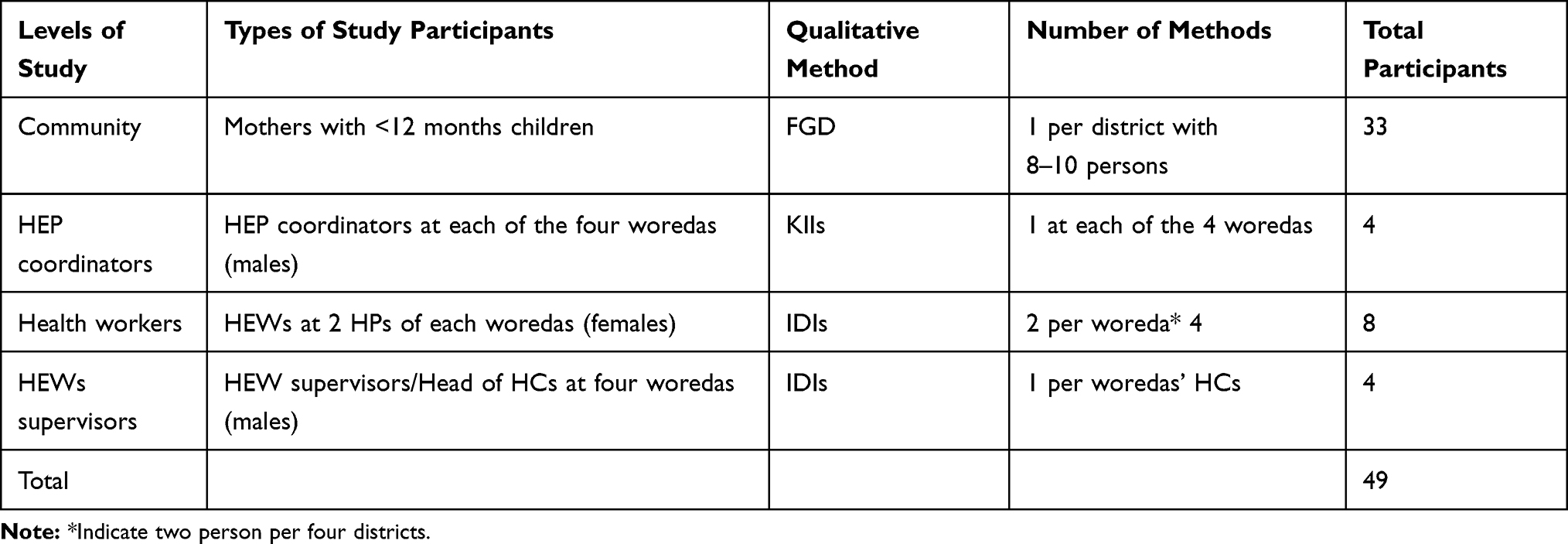 |
Table 1 Description of FGDs and IDIs Participants, Southern Ethiopia, 2019 |
Data Collection and Data Quality Management
The study team developed a semi-structured questionnaire (interview guide) to further elaborate the problem for both IDIs and FGDs. The tools were first developed in English and translated to local language (Sidmu Afo), and to keep the consistence, the tool was back translated to English by another translator. The interview guide includes questions on acceptance of services provided by HEWs, performance of HEWs on MNCH services, knowledge and practices (through impression and experience assessment) of HEWs on focused antenatal care (FANC), delivery, immediate newborn care, postnatal care for mother and baby, neonatal illness, care seeking, enabler/positive factors, barriers, and suggested solutions, all have been field tested. Data were collected between June 1030, 2019, by two trained data collectors (MPH) and one supervisor (MPH in Health promotion). Prior to the beginning of data collection, 2-days of training have been organized by the investigators for the data collectors and supervisors to orient and familiarize the teams with study objectives and the tools. IDIs were carried out using an in-depth guide and semi-structured questions to assess their knowledge on CBNC and practices (see Annex 1).
Data Entry, Analyses, and Processing
Data were tape recorded, notes taken, and then transcribed and translated and thematic analysis done using open code software by investigators. After data were organized in the seven themes, key themes such as barriers and challenges to services uptake and community utilization of the CBNC and maternal services were discussed in depth to ensure our explanation of the data was consistent with what the mothers, HEWs, HEP supervisors, and coordinators stated during data collection. The data were analyzed as per the existing analytical framework of the study objectives, and presented as per their importance and logical orders and triangulated from different sources (respondents).
Results
The qualitative study conducted in southern Ethiopia to explore the community acceptance of antenatal care (ANC), postnatal care (PNC), and CBNC services provided by HEWs, their performance, challenges, positive factors, suggested solutions to improve uptake of the services by the community from HEWs reported important findings. These findings are organized under seven thematic areas as follows:
- Acceptance of the ANC, PNC, and CBNC services provided by HEWs by the community;
- Attitude/or misconceptions of community members in general and women in particular towards the above services and people against these services;
- The performance of HEWs regarding ANC, PNC, FANC, identification, and management of sick newborns;
- Knowledge and practices of HEWs from different perspectives;
- Types of activities to implemented by HEWs to increase uptake and quality of ANC, skilled delivery, PNC, and CBNC;
- Best practices/positive factors to improve uptake of services; and
- Challenges/barriers that hide the increment of uptake of these services.
Acceptance of the ANC, PNC and CBNC Services Provided by HEWs by the Community
The acceptance of services provided by HEWs to mothers and their children such as ANC, PNC, and CBNC was high as responded by FGD mothers, HEP coordinators, HEWs supervisors, and HEWs themselves. Most of the informants from HEP supervisors/coordinators said that the community accepts those services provided by the HEWs. These services are acceptable due to its simplicity and minimum resistance to socio cultural practices. Some also said that there are close relationships among mothers and HEWs. Therefore, the community accepts the HEWs over other health professionals. Some believe that the increment in delivery coverage from 20–67% at the zone was due to community acceptance of the services.
It is good, and we are employing a very good approach towards the community as a whole. Formerly, we faced so many challenges but now it’s much improved. Even when we conduct house to house visit after the pregnant women get birth, we have a very good interaction among mothers. (27 years old HEW from Dale district)
Another HEW stated
ANC was very low in the past as older mothers prevent others from using the services and the services were provided by males, but, after we, HEWs introduced we work as mother and sister, in a friendly manner … the acceptance improved a lot. (32 years old HEW from Boricha district)
Mothers in FGDs know the benefit of some of the programs, like the importance of vaccination and referral to higher health facilities during labor and health education on some common problems like feeding practice. On the other hand, half of the participants were not happy to accept the service because of the unavailability of HEWs in their working area, health posts are closed most of the time and, while they visit there, they are not in a good mood to give care properly. Therefore, participants prefer to go to the nearest health center when they need healthcare or stay at home.
My neighbor gave birth at home safely, because of the grace of God, why do we expose our body outside the home. (FGD mother from Boricha district)
Presence of Misconception/Negative Attitude Towards the HEWs
As stated by almost all interviewed HEWs, the attitude of mothers towards their maternal and neonatal health service delivery currently is positive compared to the previous period. Past time, mothers/community had a lot of misunderstanding about the health services but after continuous community education in collaboration with the women development army (WDA) and Health Development Army (HAD) mothers’ attitude is changing and improving.
Eh … Previously, the community was using traditional drugs for the neonate but, now totally changed. Eh … for ANC they come by themselves and ask us to provide them the services but, we refer them to HC for the first ANC as different investigations are to be done there. Eh … their attitude towards PNC is also good, especially, when our approaches are good. The neonatal care at home is also acceptable because we use chart booklet during diagnosis and management at home. (31 years old HEW from Shebedino district)
Another HEW added
Mothers in this locality love us more than their husbands or than anybody; they do not have any secret to hide from us. During house to house visit, they tell us about their health, their food condition, about their child – nothing hidden from us. (28 years old HEW from Loka Abaya district)
Some of the informants believed that the community assumed HEWs lack some skills in diagnosing and treating neonatal illness, delivery, and postnatal care.
Respondents from four district offices and four health centers in the respective woredas in general believed that no one opposed the services except some older mothers and a few husbands who were preventing women from using delivery and CBNC services. Some mothers complained of fear of evil eyes while HEWs visit their homes for child care.
A 32 year-old HEP supervisor from Boricha district stated:
eh … there is positive attitude by the community towards the services provided by HEWs. Eh … the community complains disrespect at the HC and therefore, prefers the health post (HP) for the services. Eh … as per our catchment area, I have no idea to mention any misconception by the community towards the services provided by the HEWs. Another issue is drug for under five children is absent from the HP in most of the cases and mothers mostly believe that the HEWs do not have drugs but, only advise. (32 years old male HEP coordinator)
Performance of HEWs and Community Satisfaction Regarding ANC, PNC, FANC, Sick Newborn Care
Most of the HEP coordinators said that HEWs have good performance in increasing the ANC coverage of the woreda. The HEWs performances are increasing ANC coverage by about two-thirds in Boricha district, one of the study areas. Most believed that HEWs can properly screen and register and refer pregnant mothers to health centers for first ANC visit as laboratory investigations is mandatory at this stage. However, a reported gap or limitation includes a skill gap of some HEWs, especially in providing focused ANC.
Most of the district HEWs supervisors reported that the degree of identification and management of sick newborns by the HEWs was rated by informants from unsatisfactory to medium, though they had received training. Most of the HEWs do not visit homes so that means no access to the service. In support of supervisors’ idea, most HEWs reported that they are not fully engaged in identifying and managing a sick new born baby, they usually depended on mother’s report.
A 32 year old HEWs supervisor from Boricha district primary hospital stated
… Though problems still existing, HEWs are working towards increasing the performance of focused ANC. Eh … unless HEWs work in collaboration with us, our achievement will be low. (32 years old male HE supervisor)
A 34 year old male HEW supervisor from Mesenkela HC, Dale district stated:
Ok … in my opinion, if properly and closely done by HEWs, the problem will be solved. Eh … they come to HC after managed at the community level by HEWs, however, it is not satisfactory. As to the referral linkage eh … the HEWs identify and treat cases at the HP level but, when it is beyond her capacity, she refers to the HC using the referral format that contains feedback at the end on which we send them the feedback. eh … as a challenge, due to work burden the HEWs may not visit all babies home and could not identify the challenges properly. Therefore, workload and distance of the houses are the commonest challenges. In addition, negligence from the HEWs is also a challenge to these services. Eh … another challenge is drug supply, drugs for under five children is not free of charge except amoxicillin syrups. (34 years old male HEWs supervisor)
Regarding the delivery services, HEWs are not expected to attend labor but to prepare and refer to the health centers. Most said this delivery service is not being provided at HP level even though level four HEWs were trained to provide it. One of the major reasons was HPs were not equipped with the required equipment to provide delivery service and HEWs were told to refer laboring mothers to HC.
The service is given at the HC level and what the HEWs should do is to prepare and refer laboring mothers to the HC (28 years old male HEWs supervisor)
Another point is the issue of early identification and referral of obstetric complications. Informants said there is a practice of this to a lesser extent which is not satisfactory at all.
Most of the HEWs agreed that their level of knowledge and skills on delivery of the services is good. All were well trained for the service they provided such as ANC, PNC, and neonatal healthcare.
Eh … previously, some mothers refuse our services, but now they welcome us and consequently, we provide them adequate information. In general, there are some workloads that may affect the performance and also some refusals from the community though it is currently declining. (22 years old HEW from Loka Abaya district)
View of FGDs
The participants also agreed that previously they were receiving different services that are mentioned as the full package, but currently HEWs are usually unavailable and the health post is usually closed. Even if it is open, they will appoint them to come another time and they will tell them they are busy. However, a few of them mentioned that they are providing health education about breastfeeding and how to care for the child.
When we visit health post on our appointment they appoint us for another time, they were telling us they had urgent duty, so it is difficult to get the desired service from them. For example, when we bring our children for vaccination service also most of the time, they tell us there is no vaccine and stay here for a long time. (FGD mother from Dale district)
Two of the mothers strengthen the idea by saying
… For example, my child is not vaccinated up to now; it is around three months without getting the vaccination. They appoint me for different schedule, but it is difficult to get them on appointment date, so I am getting fed up because of their false promises. The day before yesterday, I came here to get vaccination for my child and I have paid for transportation to reach on time. But when I arrived here, they told me as the date of vaccination schedule was yesterday forced to turn back home without getting the service. (FGD mother from Dale district)
Government and some other nongovernmental organizations sometimes provide wheat flour “Fafa“ and oil for those who face shortage of supplementary food. There was a supply of cereal and wheat flour which was brought for pregnant and lactating women, the HEWs are not fair in distributing the supply … no fairness at all, and they provide it for some women who were not pregnant and lactating. Even they don’t consider our income status. Many pregnant and lactating women were left alone without getting the supply. It is common to face such challenges. (FGD mother from Dale district)
Knowledge and Practices of HEWs in Delivering MNCH Care Services
During the IDIs, HEP coordinators/supervisors stated that experienced HEWs who had served more than 3 years are capable of implementing this, while the newly graduated ones have difficulty in practicing a special CBNC program. To fill these gaps informants claimed that they are frequently updating and refreshing HEWs through different job training and recommend extra trainings for improvements. Some said there are NGOs who support this implementation program.
Eh … I do not say they are competent in their current skills to perform CBNC, they should be trained well for further improvement. They can identify pregnant mothers, eh … may be laboratory test are lacking. The knowledge and skills to implement FANC might be inadequate and therefore, its implementation was not as it is expected. The HEWs are good in identification and linkages of pregnant mothers to HCs. As to labor and delivery, HEWs have knowledge and skills to identify and manage sick newborns but, performance is low similar to postnatal home visits. (28 years old male HEP coordinator)
Regarding labor and delivery services, most of the informants testified that HEWs do not have adequate skills to perform labor and delivery. Some of the reasons mentioned were that HPs were not well equipped to provide services; level II and III HEWs do not have skills to provide it; and also, delivery services are not recommended at the HP level. However, they can perform identification and referral of laboring mothers, sick newborns to the HCs. They recommended further training to be provided on care for neonates.
As to the PNC services, according to the response of informants, HEWs were able to conduct it and knew the schedule, but they do not keep the recommended schedule. Some said HEWs are not committed to these services due to negligence, workloads, lack of information and materials, distance of the houses, etc.
HEWs View
All of the participants reported that they knew about all the maternal and child health service that can be possibly provided at a health post level. Accordingly, all of them mentioned ANC, Post-natal care, neonatal care, including early initiation of breastfeeding, sick child identification and treatment, identification of danger signs for pregnant women, and neonatal and referral services. All of the participants reported that, except delivery service, they are doing all the packages of maternal and child service at household as well as at health post level.
We will give gentamycin for a neonate with infection. We are also providing advice for the mother about kangaroo mother care and frequent breastfeeding for LBW or preterm baby. (27 years old HEW from Shebidino district)
Another HEW added:
Eh … we take vital signs for mother, check whether she has heavy bleeding, fever, foul smelling discharge and headaches during pregnancy and the postnatal period. For the neonates, we check the umbilicus for bleeding and redness … (30 years old HEW from Dale district).
All of the participants have knowledge about the implementation strategies of CBNC. They all mentioned about early pregnant woman’s identification, FANC, postnatal care and identification and management of sick child including neonates. They know the detailed activities of each of the earlier mentioned programs. Here, a HEW stated:
The majority of the participants reported that they know the schedule set by the Federal Ministry of Health CBNC implementation guideline. The home visits stated were at days one, three, seven and then after two weeks of birth if any health problem is existing. If, accidentally, a woman gave birth at home; they will go to the home and provide postnatal care.
Eh … when we come across home birth immediately, we take vital signs like BP, weight, sign of jaundice, for anemia we check her eyes and breathing condition, bleeding, abdomen. (30 years old HEW from Dale district)
Concerning identification and management of sick newborns, HEWs also revealed they have a problem of knowledge and skill to identify and manage but at least they will refer to the nearest health facility for better management. Districts’ health extensions supervisors also reported that the HEWs were not identifying properly because they are not visiting the home due to multiple reasons and not properly managing the case because it is beyond their capacity.
A HEW reported that,
during the home visit, I will examine the newborn baby body temperature, body rash, I will see the umbilicus. Whether the baby breast feed or not and demonstrating the mother how to feed and the attachment, I will measure the baby weight. (30 years old HEW from Loka Abaya district)
Another HEW said:
We ask the mother for any health problem of her baby or any difference from its normal status. Eh … we ask for inability to feed, vomiting everything, eh … if the child has pneumonia or chest in drawing or fast breathing. Eh … we treat from 0–2 months’ babies but, we refer what is beyond our capacity. For example, if the baby is vomiting everything, we do nothing here except calling for ambulance and referring to hospital till the baby reach 45 days of age. Eh … if severe pneumonia we refer to hospital using white paper for referral. After treatment at the hospital the family bring back their child for follow up to us at the HP.
What Can Be Done to Improve the Uptake and Quality Services Provided by HEWs?
Almost all interviewees had a similar view on improving community uptake and quality of services. They suggested the following points: providing education for the community on an ongoing basis and during maternal forum, HEWs should improve declining home visits, proper collaboration with the other community workers like HDAs, kebele leaders, district health office, etc., strengthening the one to five network, frequent provision of training for the HEWs, payincentives for those hard working HEWs, assigning additional HEWs per health posts to minimize the workload, opening the health post at all times, strong commitment from HEWs, close supervision by the district health office, availing medical supplies and necessary drugs continuously and improving the electricity supply to the health posts.
A 28 year old male from Abela district stated:
First, HEWs should create awareness for pregnant mothers on PNC benefits during maternal forum. During the forum, midwives who also participate can identify and propose solution for the poor performance of the HEWs in PNC. In addition, kebele leaders take part in forum so that can help in mobilizing the community. HEWs are poorly committed to their work and to solve this issue we, the PHCU heads, heath extension supervisors should work closely with them. (28 years old HEWs Supervisor)
An FGD mother stated that,
The health posts are empty. At least if they are equipped with basic facilities and avail the service with reasonable price such as sanitation materials (soap and ointments, modes for menstrual hygiene) and others as well, this definitely help us much. Otherwise, only the physical construction of the health post by itself is worth less. (FGD Dale District)
Positive Factors/Best Practices Observed That Favour the Program
Most of the respondents testified that HEWs have a smooth relationship with the community, kebele leaders and HDAs. This is because HEWs were initially selected from the same community for the training thus they knew their work area very well and stayed familiar with the community, their culture, and traditions. Mothers from FGD reported that the presence of a positive attitude towards the program by the community is one of the major factors that can motivate the HEWs.
For instance, a supervisor from one District reported that mothers voluntarily participated in awareness creation for the monthly contribution of money to help the maternal forum by health professionals and mothers, community accompanying laboring mothers to the HC, motivating best performing HEW through awarding.
A kebele named Doya Game, in our district, which is 2–3 km away from the town, there are two volunteer mothers who have been serving the community in collaboration with the HEWs. These mothers are promoting the service given through the health extension program to the community with the ultimate aim of making the kebele free from home delivery. Their motto has been recognized as no woman residing in the kebele delivers at home. (27 years old male HEWs supervisor)
A 28 year old male HEW supervisor explained:
Refreshment trainings are organized regularly, through which HEWs update their knowledge and skill which also motivate them to work
Other HEWs declare that,
Yes … now, for example, for pregnant mother there is a saving program of women groups that when the mother give birth, they prepare porridge, buy clothes for the baby and visit her at the HC. But a mother who gave birth at home will not be given anything even from what she saved.
Challenges and Barriers to Implement CBNC
The majority of the participants responded that lack of a vehicle for moving from house to house during home visits by HEWs; absence of all-weather roads for ambulance services in some kebeles of the studied districts; HEWs overloaded; manpower and budget shortages; long distance between the households in some kebeles; absence of regular monitoring and evaluation of the program by the District Health Office and PHCU; negligence by HEWs due to long time services without promotion and benefits; minimum attention from the government and the community itself; inadequate drugs and equipment supply at the health post; knowledge and skill gaps; lack of infrastructure for basic regular activities like water and electric power supply etc. are some of the challenges mentioned. In addition, some participants also cited the program was not designed for the pastoralist community lifestyle. This was the case of Loka Abaya and Boricha districts where some of the kebeles were inhibited by pastoralists.
Eh … some community leaders and volunteers ask for payment/incentives for mobilizing the public which is considered another bottleneck. In general, community support for the HEP is decreasing and also the support from the district is not as expected, and there is low coordination of the program in general terms. (28 years old male HEWs supervisor)
One of the barriers for this program is the HEWs did not live in their working area due to the fact that the district has no budget to build a residence for the HEWs in their respective work area. As a result, the HEWs feel unhappy to stay there. Previously, some of them were seen living in their locality while others were not. Most of them have been however not willing to live there as the program was not uniform throughout the district. The HEWs are very busy with other tasks like participating in the kebele (the smallest admirative unit) for other non-health activities and as this reduces their effectiveness and efficiency. (27 years old male HEWs supervisor)
One HEW claimed that,
due to the reason that we are living together with the community, the community may undermine our capacity and did not expect us to deliver services instead look for new faces.
Another informant said that:
There is also shortage of medical supplies and medicine for treating a sick child. For example, I am run out of malnutrition treatment foods. I have reported 4–6 months ago, but no one has responded to us … as the result of this malnourished child’s weight is deteriorating. (22 years old HEW Loka Abya district)
… In this kebele there are pastoralists who move from place to place in search of water for their cattle, so that, we do not get them at home. Due to shortage of water, mothers usually waste their time to fetch water and we could not get them at home. Another challenge is food shortage in this area that people usually go out of home in search for foods especially, during dry season. We do face problems with drug and equipment supply … in addition children may not complete vaccination because they move to another place after taking Pentavalent 1 or polio 1. (32 years old HEW Boricha district)
One mother reported that
Because of the irregularity of family planning services in the health post and absence of my preference method I have got pregnant two times without my interest. They are also few in number, and only two HEWs are assigned to meet the needs of thousands of women. (FGD Mother)
Discussion
Acceptance of the Services Provided by HEWs by the Community
The study results revealed that services for mothers and their children provided by HEWs are highly accepted by the community. This is due to the fact that HEWs are recruited from the same community so that they are aware of the community cultural and traditional practices. Another important reason explored was the simplicity of the services, experiences, and their polite approach to the community health needs. Similarly, mother discussants of FGD have no problem with acceptance of the services but, rather, some complained HEWs are not friendly and negligent in serving them at the HP and household level, and of the absence of HEWs from HPs and non-punctuality to their work. Our findings are similar to a previous study conducted in Ethiopia which revealed the fact that HEWs are selected from their community and this enhances trust and engagement with them.25 A study in India associated acceptance of CHW by the community with their knowledge,7 which is similar with our findings. However, a study conducted in Wolaita zone, southern Ethiopia, shows only half of the studied caretakers were satisfied with HEWs services indicating low acceptance.26 Our findings explored that MNCH and CBNC services provided by HEWs are highly valued by the community and indicate a shift of strategy to focus on other factors like health system readiness, coordination, and organization for low performance of the program.
Presence of Misconception/Negative Attitude Towards the HEWs
The study revealed that most of the community members are free from wrong perception regarding the HEWs healthcare practices with the exception of some older women and husbands who prohibit mothers and their children seeking care from HEWs. This is due to the fact that children may cry or develop some complications during vaccination or fear of evil eyes while HCWs visit homes. Another point needing emphasis is the belief that HEWs have no drugs, but only advice. Such a misconception developed due to a shortage of drug supply at the HP. A similar study on pregnant mothers’ utilization of services in southern Ethiopia shows that older women and husbands prevent pregnant mothers from giving birth at the health facility or seeking treatment.27 In addition, a previous study on ICCM utilization from HEWs in Ethiopia shows that mothers were not using the services from HEWs due to factors including wrong perceptions, health posts not being regularly open, a shortage of drugs at the health posts, health posts being very far from their residences, and the inadequate services by HEWs at the health posts.12 Absence of shared misconception in the community is a positive finding of the current study to be encouraged, whereas poor drug supply to the HPs would create doubt among the community as to whether HEWs can treat neonatal and child illnesses or not. Therefore, stakeholders should work to solve such misconceptions either through community education or fulfilling their need by availing the drugs. For example, a systematic review on CHWs revealed the presence of well-functioning health services is vital for CHWs to perform well, including logistics support, equipment, and drug supplies.14
Performance of HEWs Regarding the Services
Performance of HEWs was assumed well and good, for example, FANC coverage of the woredas improved because of their key contribution. However, a big gap is reported in PNC home visits for maternal and neonatal care, and identification and management of sick newborns. As stated by most of the participants PNC performance is very poor due to the fact that PNC is being given at home through home visits by HEWs which is very difficult for them as they might have multiple duties, long distance of houses from health posts and their negligence due to poor supervision. Similarly, previous studies reported low postnatal home visits by HEWs,26,28 and another study in Ethiopia shows a distance of more than 30 minutes’ walk was associated with a lower level of health post utilization of maternal and child health services and would mean that HEWs visits to households was based on the distance of the houses from the health posts.12
It is believed that CHWs can identify pregnant women and newborns in need of medical attention and care, promote and encourage appropriate care seeking, and provide counselling and support for home care practices across the periods of pregnancy, newborn, and childhood.5 Similarly, in the current study HEWs performed well in the identification of pregnant mothers, birth preparedness, and referral to HC through arranging for an ambulance.
The community also reported that HEWs are mostly absent from their work and HPs remained closed during their visits. HEWs appoint mothers on their visits for CBNC services due to drugs shortage or busy work schedule. This can be explained by the fact that half of the mothers reported not to have been satisfied by the services of HEWs as they are not available at working hours, no supply or medicine, including vaccine and family planning materials on a regular basis. Our report is also supported by a qualitative study in Ethiopia on barriers and facilitators to achieve high coverage of PNC by HEWs which shows there were high workloads and an unavailability of HEWs at work, which stated as:
There are only two HEWs. They have lots of activities, which they are expected to perform. Therefore, they cannot cover all mothers in the three days after delivery.29
The current study revealed that identification and managing of sick new born babies is one package of the HEP, however, the implementation of this package at the community level by the HEWs was rated less or not satisfactory by the mothers. As a reason, in addition to poor home visits made by HEWs, skill gaps to manage sick newborns identified and this area need attention by government and HEP coordinators at woreda, zonal, and regional levels, and supportive supervision with clinical support may be essential to increase performance in this regard.
Knowledge and Practices of HEWs from Different Perspectives
HEWs knowledge and practices are based on their level of education and training and experience. For example, those who are level III and serving less than 2 years, especially fresh graduates, could not properly conduct healthcare services to mothers and their children, while level IV and experienced HEWs perform well. To fill these gap informants recommended updating fresh HEWs through different on job trainings and extra training for improvements regularly. However, HEWs deny this by saying they know all the components of mothers and CBNC services and are performing it as well. For example, in India community health workers (equivalent to HEWs in Ethiopia) knowledge was found to increase the utilization of maternal and neonatal healthcare services as well as improved adherence to essential newborn care practices at household.7 The Ethiopian CBNC midline summary report shows the knowledge of HEWs was poor in CBNC, especially in identifying neonatal danger signs.30 Though HEWs should not need to memorize the danger signs they need to at least know the signs that prompt them to refer to the chart booklet to take actions. Another study in southern Ethiopia on neonatal care practices involving a mixed study revealed that mothers complained about HEWs appointments while they visited the HPs for vaccine.20
Our study revealed a knowledge and skill gaps to identify and manage sick newborn by HEWs, but at least they will refer to the nearest health facility for better management. The reason why HEWs are not identifying sick newborns properly might be they are not visiting the home due to their high work load and other factors like lack of confidence, etc.
Ais study done in four major regions of Ethiopia (Amhara, Oromia, SNNPR, and Tigray) also reported that the HEWs had poor knowledge and skill in identification, classification and management of sick newborn babies.31 Another study done in Sidama zone on HEWs reported that they have knowledge and skill gaps and were not supported by proper and regular training. While the HEWs refer the sick neonate to health centers the professionals do not properly accept or provide the proper service for the referred cases. This is mainly because of the disrespecting of the referral from the health post.27
Suggestion to Improving the Uptake and Quality of Services
To increase the uptake and quality of maternal and child health services provided by HEWs in the community, HEP supervisors and coordinators, HEWs and mothers suggested several recommendations. One of these suggestions is increasing the number of HEWs in the heath post as the usually recommended figure is not adequate to undertake multiple tasks at a time. The main reason to increase the numbers of HEWs at HPs is the health extension program package becomes broadened and also they engage in non-healthcare activities which might compete for their time. One suggestion to improve MNCH uptake and the quality of the services is to conduct program-specific supportive supervision. It is believed that enhancing the effectiveness of supervisory activities offers another possible way to improve worker performance in the short term.32 Supervision without adequate continuous essential drugs and medical supplies would not improve the services quality and uptake by the community, this is evidenced by complaints from the community about the lack of drugs at the HP level. Therefore, infrastructure fulfilment should be a priority by the health system and policymakers. These results are consistent with previous studies done in Ethiopia reporting the need for better quality improvement, proper regular refreshment training, continuous CBNC drugs and medical supply, close supervision, etc.27,30
Positive Factors (Enablers) to Improve Uptake and Quality
This study shows that a positive attitude and smooth relationship with the community, kebeles leaders, HDA, and mothers are some of the factors that favor the program positively. Besides, recruitment of HEW for training from the same community so she knows well the cultural and traditional practices creates better relationships. In support of our study, previous studies done in Ethiopia also indicated that there is good communication and coordination of HEWs with kebeles leaders, women development armies, and the community.30,31,33
Moreover, the current study pointed out that saving program by the women’s group to provide a financial award for pregnant women when they give birth, volunteer non-pregnant women a provision of education for the community as well as an award for best performing HEWs all contribute to excellence in HEWs overall engagement. Active and direct involvement of community members towards HEWs work also makes a positive impact in the entire packages. A systematic literature review study done in low- and middle-income countries suggested that there are several cultural practices that influence the community to positively maximize service utilization.14
Challenges/Barriers
As barriers identified by the current study show there is the workload on HEWs leads to them being overburdened by multiple tasks, which might be as a result of a shortage of HEWs at some health posts. According to studies conducted in different corners of Ethiopia and Afghanistan there were similar challenges and barriers that affect the proper implementation of maternal and child healthcare service by the HEWs at community level.20,25,26,33 Particularly, a qualitative study in two regions of Ethiopia on challenges and facilitators of early PNC home visits reported HEWs availability at work site as barriers to timely conducting PNC visits.29 Another study in central Ethiopia confirms a barrier to HEWs home visits for PNC is that the service is not consistent and comprehensive because of the limited number of health workers compared to the demand of services.34 Besides, a study in Ethiopia on the success and challenges on HEWs for 15 (2003–2018) years identified many challenges, as did our study too, which are related to productivity and efficiency of HEWs; their working and living conditions; capacity on health posts; and social determinants of health.35
The absence of regular monitoring and evaluation of the program by the HEP coordinators and supervisors is cited to be a major challenge to better performance of MNCH by HEWs. This might be due to the busy schedule and absence of scheduled supervision from the administrative body based on the FMOH recommendation, and emphasis to be given to these challenges to solve the low performance of maternal and child health services by HEWs at peripheral levels. Our result is consistent with previous reports in Ethiopia, where inadequate and untimely supportive supervision and systems, poor drug and medical equipment supply and lack of trust, communication and dialogue and differing expectations contributed to the low performance of HEWs.20
As stated, our study reported a lack of incentives, proper provision of promotion to education and transfers were the barriers to improving maternal and neonatal care by HEWs. Our results are supported by the study on contextual factors influencing performance of health workers which cited motivation of CHW could be shaped by the health system’s ability to accommodate their expectations in areas of status update, prospect of career development, and incentives. Evidence tells us that the program is not without challenge. As reported by previous literatures there was dissatisfaction among HEWs, poor community acceptance of the HEP, and limitations in designing the HEP package and its intervention strategies.15,17
Moreover, one of the reasons for HEWs absence from their duty that results in poor performance could be poor program coordination between vertical programs and between various NGOs, resulting in training overlaps as stated by a study done in Ethiopia among HEWs.36 The coordination between woreda HEP supervisor, PHCU leaders, Midwives, HDAs, model families and religious leaders have paramount importance in increasing the uptake of the MNCH program at the community level. Hence, interaction amongst local community actors represents a strength that can be utilized in an IEC intervention to promote MNCH and CBNC service utilization.37
Another important barrier to HEWs performance was environmental factor like the hilly nature of some kebeles, road inaccessibility, far nature of households from HPs and from one another. Some kebeles studied had a pastoral nature and it was difficult for HEWs to get to them at the time of visit. This is supported by a previous body of science that households residing between 1–3 km from a CHW were less likely to utilize the services, which tells us that the distance of CHWs and health facilities to their clients might determine uptake of the services.38 A mechanism to tackle physical accessibility issues, expecting improvement of the MNCH and CBNC program will be unlikely, and we, therefore, suggest a policy revision on how to pave a persistent solution to the problem. Due to the hard to reach, pastoral nature of some kebeles in the study area, assigning male HEWs in those kebeles may help improve the services.
The limitations of the current study could be transcription errors, like accidental and/or unavoidable alterations of data could not be ruled out. Another error may be that English language competency would introduce interpretation differences during data analysis. We have minimized such possible errors by revising and discussing together and taking corrective actions accordingly. Moreover, we failed to include some important groups from the community like HDAs/WDAs, model households and community leaders. Their absence might limit our study quality as there are the main supporters of HEPs at community level. Another limitation of this study could be a lack of inclusion of midwives as they are key role players in leading maternal forum with HEWs and provision of more clinical support. As can be seen from the report all of our key informants of supervisory teams are males; hence, our findings might be biased. Finally, knowledge, skills, and performance of HEWs assessment was not supported by observation and skill assessment, but we simply evaluated their impression and experiences.
Conclusions
The results show services provided by HEWs at community level for mothers and their children is highly accepted by the community. Most of the community members are free from wrong perception regarding the HEWs healthcare practices. As to performance of HEWs, there is better change in FANC, but PNC and CBNC are still low. Knowledge and practices of HEWs was based on their level of education and experience. To improve uptake of the services, increasing the number of HEWs in heath post, supportive supervision, continuous essential drugs and medical supplies, etc., have been suggested by respondents. There are identified opportunities and challenges for uptaking services provided by HEWs to mothers and their neonates, some of these challenges are workload, shortage of HEWs at some health posts, road inaccessibility, long distance between the households and health posts, making the visits more difficult. Therefore, MNCH and CBNC programs should focus on the postnatal home visits, CBNC improvement through increasing the number, knowledge, and skills of HEWs. Moreover, availing drugs and equipment at health post level, improving supportive supervision and proper motivation of HEWs are recommended.
Abbreviations
CSA, Central Statistical Agency; CBNC, community-based neonatal care; DHS, Demographic and Health Survey; EDHS, Ethiopian Demographic and Health Survey; EFFMOH, Ethiopian Federal Ministry of Health; FGDS, focus group discussions; HDAs, health development armies; HEP, health extension program; HEWs, health extension workers; HSDP, health sector development program; IDIs, in-depth interviews; MMR, maternal mortality ratio; MNCH, maternal neonatal and child health; NMR, neonatal mortality rate; PNC, postnatal care; SNNPRS, South Nations and Nationalities and Peoples Regional State; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
The proposal was reviewed and approved by the Institutional Review Board (IRB) of the College of Medical and Health Sciences, Hawassa University. Permission to undertake this study was obtained from every relevant authority at all the selected district Health offices. Informed verbal consent was taken from all study participants. All participants were informed about potential risk, benefits, confidentiality, and the right to decline the study. The verbal consent was approved by our ethical committee.
Consent for Publication
Not applicable.
Acknowledgments
First of all, we would like to thank and SIHRT project for financial support of this study. Then, we extend our thanks to Hawassa University, College of Medicine and Health Science for the opportunity and for overall material support. Our special thanks also go to Sideman Zone Health Burro and the four woredas Health Offices for their support in approving the study. Finally, we thank data collectors and study participants.
Authors’ Details
YH (MPH, Assistant professor in Epidemiology), Hawassa University, College of Medicine and Health Science, School of Public Health.
NM (MPH, Regional EPI and Surveillance Technical Assistant and coordinator), Maternal and Child Health Core Process, Southern Nation Nationalities and People Regional Health Bureau, Hawassa, Ethiopia. AG (PhD, Associate professor) Hawassa University, College of Medicine and Health Science, School of Public Health.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that they have no competing interests.
References
1. Federal Democratic Republic of Ethiopia Ministry of Health. Road Map for Accelerating the Reduction of Maternal and Newborn Morbidity and Mortality in Ethiopia. Addis Ababa; 2012.
2. The Federal Democratic Republic of Ethiopia Ministry of Health (FMoH)/MCH Directorate. National Newborn and Child Survival Strategy Document Brief Summary, 2015/16–2019/2020
3. USAID. Maternal and Child Survival Program (MCSP) CBNC/NEGA Project: Implementing a Demand Creation Strategy for Improved Maternal, Newborn, and Child Health Outcomes. Addis Ababa Ethiopia: USAID; 2018:2018.
4. FMoH. Federal Ministry of Health Rural Health Extension Program Implementation Guide Line. Addis Ababa, Ethiopia; 2013.
5. Samira A, Shamim Q, Cathy W, et al. Community health workers: A crucial role in newborn health care and survival. 2014;4(2):020302. doi:10.7189/jogh.04.020302.
6. Nejmudin KB, Christopher HH, Feng Z, Agnes S, Christophe L. Health extension workers in Ethiopia: improved access and coverage for the rural poor. Health Extension Worker Book Cha. 2015;24.
7. Agrawal PK, Agrawal S, Ahmed S, et al. Effect of knowledge of community health workers on essential newborn health care: a study from rural India. Health Policy Plan. 2012;27(2):115–126. doi:10.1093/heapol/czr018
8. Karim AM, Admassu K, Schellenberg J, et al. Effect of Ethiopia’s health extension program on maternal and newborn health care practices in 101 rural districts: a dose-response study. PLoS One. 2013;8(6):
9. Gogia S, Sachde HPS. Home-based neonatal care by community health workers for preventing mortality in neonates in low- and middle-income countries: a systematic review. J Perinatol. 2016;36(S1):S54–S72. doi:10.1038/jp.2016.33
10. JSI, L10K. Trend in the Maternal & Newborn Health Care Practices in L10K Areas. Findings from the Baseline, Midterm and Rapid Community Surveys. Addis Ababa, Ethiopia; 2013.
11. Baqui AH, Ahmed S, El Arifeen S, et al. Effect of timing of first postnatal care home visit on neonatal mortality in Bangladesh: a observational cohort study. BMJ. 2009;339:b2826. doi:10.1136/bmj.b2826
12. Bryan S, Agbessi A, Nathan PM, et al. Determinants of utilization of health extension workers in the context of scale-up of integrated community case management of childhood illnesses in Ethiopia. Am J Trop Med Hyg. 2015;93(3):
13. Fetene N, Linnander E, Fekadu B, et al. The ethiopian health extension program and variation in health systems performance: what matters? PLoS One. 2016;11(5):e0156438. doi:10.1371/journal.pone.0156438
14. Kok MC, Dieleman M, Taegtmeyer M, et al. Which intervention design factors influence performance of community health workers in low- and middle-income countries? A systematic review. Health Policy Plan. 2015;30(9):1207–1227. doi:10.1093/heapol/czu126
15. CNHDE-Center for National Health Development in Ethiopia. The earth Institute at Columbia: 2011.
16. Hailom B. Ethiopian Health Extension Program, Improving Health Through Community Participation, Peer Review at MizHasab Research Center. Addis Ababa, Ethiopia; 2011.
17. FMoH. Health Sector Development Plan III Evaluation Report 20 11/12. Addis Ababa, Ethiopia; 2012.
18. FMoH. Federal Ministry of Health: Health Development Army Implementation Guide Line. Addis Ababa, Ethiopia; 2013.
19. USAID/ETHIOPPIA(MAY 2012): End of Project Evaluation for the Urban Health Extension Program Prepared by Lucy Miz, Rebecca Miles, Mirgisa Kaba, Michael Dejene, and Kuleni Birhanu through the GH Tech. Bridge project www.ghtechproject.com.
20. Maryse CK, Aschenaki ZK, Daniel GD, et al. A qualitative assessment of health extension workers’ relationships with the community and health sector in Ethiopia: opportunities for enhancing maternal health performance. Hum Resour Health. 2015;13(1):80. doi:10.1186/s12960-015-0077-4
21. Gebretsadik A, Teshome M, Mekonnen M, Alemayehu A, Haji Y. Health extension workers involvement in the utilization of focused antenatal care service in rural sidama zone, Southern Ethiopia: a cross-sectional study. Health Serv Res Manage Epidemiol. 2019;6:1–8. doi:10.1177/2333392819835138
22. Gebretsadik A, Alemayehu A, Teshome M, Mekonnen M, Haji Y. Home-based neonatal care by Health Extension Worker in rural Sidama Zone southern Ethiopia: a cross-sectional study. Pediatric Health Med Ther. 2018;9:147–155. doi:10.2147/PHMT.S179339
23. Haji Y, Teshome M, Alemayehu A, Mekonnen M, W Gebrieal F, Tsasdik A. The levels of neonatal care practices at health facilities and home deliveries in rural sidama zone, Southern Ethiopia. J Prim Care Community Health. 2018;Volume 9:1–10. doi:10.1177/2150132718812181
24. SNNP regional state and Sidama Zone Administration, Socio-economic profile 2015. Finance and Economics Department, Socio Economic Data Analysis and Dissemination Core Process. Sidama Zone. Hawassa, Ethiopia; 2015.
25. Callaghan-Koru JA, Seifu A, Tholandi M, et al. Newborn care practices at home and in health facilities in 4 regions of Ethiopia. BMC Pediatr. 2013;13:198. doi:10.1186/1471-2431-13-198
26. Yoseph DD, Yohannis BK. Satisfaction of caretakers on community based newborn care and its predictors inboloso sore district, Southern Ethiopia. Res Square. 2019. doi:10.21203/rs.2.15580/v1
27. Kea ZA, Tulloch O, Datiko DG, Theobald S, Kok M. Exploring barriers to the use of formal maternal health services and priority areas for action in Sidama zone, southern Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):96. doi:10.1186/s12884-018-1721-5
28. Amare Y, Pauline S, Joanna S, Berhanu D, Zelee H. Early postnatal home visits: a qualitative study of barriers and facilitators to achieving high coverage. BMC Public Health. 2018;18:1074. doi:10.1186/s12889-018-5922-7
29. Berhanu D, Avan BI. Community Based Newborn Care: Quality of CBNC Programme Assessment - Midline Evaluation Report, March 2017. London: IDEAS, London School of Hygiene & Tropical Medicine; 2017.
30. Tura G, Fantahun M, Worku A. Neonatal care practice and factors affecting in Southwest Ethiopia: a mixed method study. BMC Int Health and Human Rights. 2015;15:18. doi:10.1186/s12914-015-0050-2
31. Jackson R, Tesfay FH, Godefay H, Gebrehiwot TG. Health extension workers’ and mothers’ attitudes to maternal health service utilization and acceptance in Adwa Woreda, Tigray Region, Ethiopia. PLoS One. 2016;11(3):e015074. doi:10.1371/journal.pone.0150747
32. Rowe AK, de Savigny D, Lanata CF, Victora CG. How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet. 2005;366(9490):1026–1035. doi:10.1016/S0140-6736(05)67028-6
33. Karen ME, Khaksar Y, Zelaikha A, et al. Can community health worker home visiting improve care-seeking and maternal and newborn care practices in fragile states such as Afghanistan? A population-based intervention study. BMC Med. 2018;16(1):106. doi:10.1186/s12916-018-1092-9
34. Save the children. Rapid Assessment on Barriers to Early Pregnancy Identification Focused Antenatal Care, Skilled Birth Attendance and Postnatal Care Service Utilization in East Shewa Zone, Oromia Region. Final Report. Professional researchers and trainer’s plc, January 2015
35. Yibeltal A, Yalemzewod AG, Peter SH, et al. Community health extension program of Ethiopia, 2003–2018: successes and challenges toward universal coverage for primary healthcare services Global Health. 2019;15:24. doi:doi:10.1186/s12992-019-0470-1
36. Ye-Ebiyo Y, Kitaw Y, Girma S, Desta H, Seyoum A, Teklehaimanot A. Study on health extension workers: access to information, continuing education and reference materials. Ethiopian J Health Dev. 2007;21(3):240–245.
37. Dynes MM, et al. Factors shaping interactions among community health workers in rural Ethiopia: rethinking workplace trust and teamwork. J Midwifery Women’s Health. 2014;59(No. Supplement 1):S32–S43. doi:10.1111/jmwh.12135
38. Mukanga D, Tibenderana JK, Peterson S, et al. Access, acceptability and utilization of community health workers using diagnostics for case management of fever in Ugandan children: a cross sectional study. Malar J. 2012;11(1):121. doi:10.1186/1475-2875-11-121
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.