Back to Journals » International Medical Case Reports Journal » Volume 18
Combined Superior Mesenteric Artery Syndrome and Nutcracker Syndrome in a Young Male Patient Presenting as Atypical Vomiting and Rapid Weight Loss: A Case Report
Authors Dahir Alasow MO ![]() , Elmi AM, Haji AM, Jama SMA, Hirei HH
, Elmi AM, Haji AM, Jama SMA, Hirei HH ![]() , Osman AA
, Osman AA ![]()
Received 26 February 2025
Accepted for publication 22 July 2025
Published 25 July 2025 Volume 2025:18 Pages 937—942
DOI https://doi.org/10.2147/IMCRJ.S519808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tanvi Dhere
Mohamed Osman Dahir Alasow, Abdinasir Mohamed Elmi, Abdirahman Mahmud Haji, Shuayb Moallim Ali Jama, Hanan Hassan Hirei, Ahmed Adam Osman
Radiology Department, Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Osman Dahir Alasow, Radiology Department, Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital, 30 Street, Albarako, Hodan District, Mogadishu, Somalia, Tel +252615428952, Email [email protected]
Abstract: Superior mesenteric artery (SMA) syndrome, also known as Wilkie syndrome, is an uncommon condition marked by the compression of the third segment of the duodenum between the SMA and the aorta, often occurring after rapid weight loss, particularly in young, slim individuals. Symptoms consist of epigastric pain, bloating, and vomiting. Nutcracker syndrome (NCS) is characterized by the compression of the left renal vein (LRV) between the superior mesenteric artery and the aorta. This condition results in venous varices and elevated pressure within the LRV, which may manifest as hematuria, proteinuria, pelvic congestion, and flank pain. Although each of these syndromes is infrequent, their simultaneous incidence is remarkably occasional. This case report examines a young male patient diagnosed with both SMA syndrome and NCS, emphasizing the importance of considering these conditions in the differential diagnosis of abdominal and renal symptoms.
Keywords: superior mesenteric artery syndrome, nutcracker syndrome, left renal vein, vomiting, duodenal obstruction
Introduction
Superior mesenteric artery (SMA) syndrome, or Wilkie syndrome, is defined by the compression of the third segment of the duodenum between the aorta and the SMA. The syndrome is uncommon, occurring in 0.13% to 0.3% of cases, predominantly affecting young, thin females. Rokitansky first documented vascular compression of the duodenum in 1861, and the illness typically occurs following rapid weight reduction.1,2 Symptoms of SMA syndrome encompass either chronic or acute episodic epigastric discomfort, bloating, or vomiting. Due to the complexity of the being diagnosed, it is essential to identify alternate causes of duodenal obstruction. However, the patient generally possesses a prolonged history of symptoms.2,3
Nutcracker syndrome (NCS) is defined as anterior compression of the left renal vein (LRV) between the SMA and the aorta or, less usually, posterior compression of the aorta and the vertebral column. It is also a rare entity. The causes are frequently associated with anatomical variations.1 The LRV experiences an increase in pressure as a result of the formation of venous varices around the renal pelvis, ureter, and gonadal vein due to compression of the LVR in NCS. Hypertension, flank pain, left-sided varicocele, pelvic congestion, hematuria, and orthostatic proteinuria are some of the clinical signs and findings. The diagnosis can be established by comparing the clinical presentation and radiologic findings, whether or not an invasive LRV pressure measurement is performed.1,4
The presence of both nutcracker syndrome and superior mesenteric artery syndrome (SMAS) together is extremely rare. We describe the imaging results of a young man patient who had both diseases in this case report.
Case Report
A 15 year-old male presented to the pediatric emergency department with nausea and sudden-onset vomiting, left flank pain around hours postprandially for three consecutive days. The patient has previous history for visiting a local clinic multiple times for therapy for the same symptoms, which yielded no improvement. The patient consistently reported bilious projectile vomiting, partially digested meals, and abdominal distension; he also noted frequent retching throughout a few months ago. A nasogastric tube was inserted for bowel decompression. The patient’s height was 1.61 m, weight was 44 kg, and body mass index was 16.9 kg/m². During the examination, his body temperature was 36.7°C, his pulse was 58 beats/min, and his respiration rate was 19 breaths/min. Additionally, his blood pressure was 120/70 mmHg. During the physical examination, he presented as very unwell, exhibiting a soft and flat abdomen. We conducted laboratory blood analyses. A complete blood count and biochemical tests yielded results within the normal range. During radiologic assessment of the abdomen, there were highlighted a markedly enlarged abdomen containing food debris and a fluid interface, without dilation of small or big bowel loops or presence of pneumoperitoneum (Figure 1). Given the clinical presentation and radiologic assessment, we suspected duodenal blockage due to a peptic ulcer. Consequently, we conducted a contrast-enhanced abdominal computed tomography (CT) scan. The CT scan indicated the presence of SMA syndrome: a reduced distance between the SMA and the aorta (4.70 mm) with an angle of 18.0°, distension of the stomach and duodenum up to the obstruction zone, and a narrowed caliber of the third section of the duodenum (3 mm). Antero -posterior axis of CT demonstrated results consistent with NCS syndrome: a markedly reduced diameter of the left renal vein, measuring 3 mm in the aortomesenteric area, whereas the remainder of the renal vein from the hilum to the site of compression exhibited a notable diameter of 10 mm (Figures 2–4). The findings confirmed the diagnosis of SMA syndrome in conjunction with NCS. The patient received conservative treatment with enteral and parenteral feeding, although it proved ineffective. As a result of significant weight loss. He underwent a Roux-en-Y duodenojejunostomy procedure. Three days post-surgery, the patient commenced oral fluid intake, demonstrating that fluid pass through the anastomosed regions without obstruction. He was discharged from the hospital following his recovery and had the ability to tolerate soft foods and drinks.
 |
Figure 1 Plain abdomen X-ray image. At supine image, a grossly distended stomach with food particles and a fluid-filled level. |
 |
Figure 2 Axial CT with a contrast of the abdomen (A) shows the diffuse dilated of the stomach and the dilated 1st and 2nd part of the duodenum abdomen (blue and green arrow) that then tapers in diameter as it reaches the superior mesenteric artery in the midline above the spine (white arrow), also the decreased aortomesenteric angle compressed the third portion of the duodenum. (B) Showing narrowing of the left renal vein as it crosses to the left between the SMA and the aorta. |
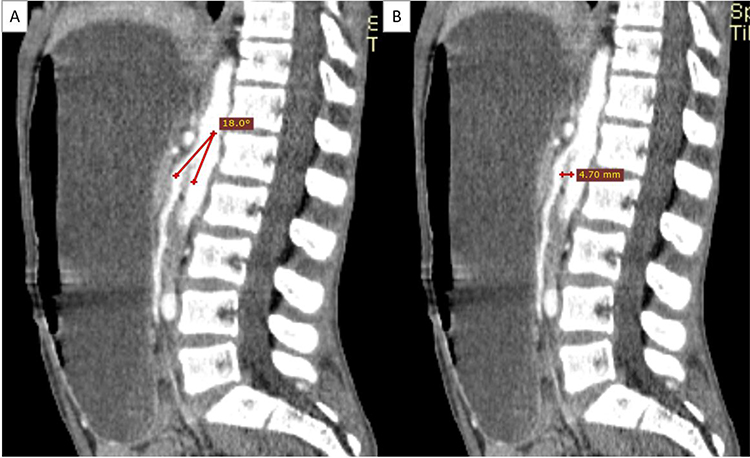 |
Figure 3 (A and B) Sagittal view of CT scan of abdomen and pelvis showing an acute narrowing aorto-mesenteric angle of 18° and a reduced aorto-mesenteric distance of 4.7mm. |
 |
Figure 4 (A and B) Axial and 3D reconstructed CT images describe a decreased aorto-mesenteric distance with left renal vein compression between the aorta and superior mesenteric artery (SMA) indicative of nutcracker syndrome. The left renal vein is dilated from the renal hilum (white arrow) and mild distal dilatation is also visualized on this 3D image. It shows a short aorto-mesenteric distance with SMA compressing the left renal vein which runs a dilated course from the hilum of the left kidney (white arrow). Also, mild dilatation of the left distal renal vein in a 3D reconstructive image indicates nutcracker syndrome. |
Discussion
Rokitansky first delineated the SMA condition in 1861. Wilkie published the initial series in 1927; hence, SMA syndrome is often referred to as Wilkie’s syndrome. Cast syndrome, arteriomesenteric duodenal compression, aortomesenteric artery compression, and duodenal vascular compression are terms that denote the same disorder.1,5 SMA syndrome is a rare disorder that can lead to distal segment of the duodenum. To the best of our knowledge, the specifics of the incidence remain unknown. It is more common in female adolescents and decreases the aortomesenteric angle and aortomesenteric distance by obstructive the duodenum. The typical aortomesenteric angle and distance range from 25° to 60° and 10 mm to 28 mm, respectively; in this case, the angle was 13.7° and the distance was 5.25 mm. The presentation of this syndrome may vary from an acute illness to a delayed onset, depending upon the etiology and severity of the duodenal obstruction.
The most characteristic symptoms include post-prandial epigastric fullness, pain, belching, and bilious vomiting. Meals and dorsal decubitus increase the condition, although left lateral deviation and knee-chest postures may provide relief.6 SMA syndrome is a condition characterized by nonspecific symptoms, often requiring radiological assessment or diagnostic confirmation. It can be diagnosed through an upper gastrointestinal barium x-ray, endoscopic gastroduodenoscopy, or abdominal CT scan. These tests may reveal external compression of the third segment of the duodenum and a narrowed angle between the aorta and superior mesenteric artery. Multiple radiographic anomalies suggest SMA syndrome.7
Our patient was typical young, thin male experienced severe nausea and vomiting for three days straight, accompanied by abdominal distension and partially digested food. Despite a nasogastric tube placement for gastric decompression, the issue persisted, indicating a potential health concern. We therefore conducted a contrast-enhanced abdominal computed tomography (CT) scan. The CT scan then revealed symptoms of SMA syndrome, including a distended stomach and duodenum until the clamp zone, a decreased caliber of the third portion of the duodenum (3mm), and a space of 4.70 mm between the SMA and the aorta and an 18.0° angle. The left renal vein exhibited a substantially reduced caliber of 3mm in the aortomesenteric space, and the renal vein from the hilum to the compression site had a prominent caliber of 10 mm, as revealed by AP-CT. These findings are consistent with NC syndrome. Our case represents an uncommon simultaneous presentation of both SMA and NC syndromes in comparison to previous studies. The literature has only reported a few cases with this dual presentation, highlighting the significance of a thorough radiologic evaluation in patients with unexplained renal and gastrointestinal symptoms. Our imaging results corroborate earlier research suggesting that anatomic congestion in the aortomesenteric region may impact the duodenum and left renal vein at the same time, which leads to overlapping clinical symptoms. Enteral or parenteral nutrition is given but this was not considered as a conservative treatment for the disorder due to his underweight status at the time of symptom onset. The patient underwent a Roux-en-Y duodenojejunostomy without intraoperative complications. Oral fluid intake was initiated on postoperative day three, demonstrating effective transit through the anastomotic sites without evidence of obstruction or delayed gastric emptying. Following a favorable recovery course, the patient was discharged in stable condition, exhibiting tolerance to both soft solids and oral fluids without gastrointestinal distress.
The Nutcracker phenomenon (NCP) is a benign condition in which the left renal vein is compressed between the aorta and the superior mesenteric artery (SMA). This compression restricts the passage of blood from the kidney and results in the dilation of the distal segment of the renal vein. Symptomatic compression of the left renal vein between veins that are associated with nutcracker morphology is referred to as nutcracker syndrome.2 Nutcracker syndrome (NCS) is a rare entity with a small number of cases, primarily due to anatomical variants such as a posterior renal ptosis, an excessively elevated course of the LRV, and an aberrant SMA branching from the aorta, rather than the logical cause of weight loss and subsequent reduction in the adipose plane.1
A variety of symptoms, including hematuria, pain (including dyspareunia, pelvic pain, and low back pain), and varicocele (pelvic varices in women), are typical of nutcracker syndrome. This triad, however, is not consistently present.8
Coexistence of SMA and nutcracker syndrome is comparatively rare, making clinical diagnosis remains challenging and managing of patients with both syndromes requires a multidisciplinary approach.9,10
The primary objective for SMA syndrome is weight restoration: decompression of the duodenum and stomach to alleviate symptoms, fluid resuscitation, and correction of electrolyte imbalances, aiming to optimize nutrition through enteral jejunal feeding, total parenteral nutrition (TPN), or a combination of both. One of the surgical procedures that has been reported is a gastrojejunostomy. Another is Strong’s surgery, which involves dividing the Treitz ligament and mobilizing the duodenum. A safe and effective technique for lowering symptoms and improving quality of life is duodenojejunostomy.6,9
The treatment for NCS is contingent upon age and clinical manifestations. For patients under 18, the optimal approach is cautious treatment with a minimum of two years of observation, meanwhile up to 75% will see complete clearance of hematuria. Nephrectomy, LRV transposition with or without Dacron wedge insertion between SMA and aorta, renal autotransplant, renal-to-IVC shunt, medial nephropexy with excision of renal varicosities, and gonadocaval bypass are among the surgical techniques that have been used to treat persistent hematuria.11
Conclusion
This case report describes what a young man with the rare combination of superior mesenteric artery (SMA) syndrome and nutcracker syndrome (NCS) did in the diagnosis and treatment of these two conditions. Imaging tests and clinical signs showed that the person had SMA syndrome, which is characterized by duodenal obstruction caused by pressure on the SMA and aorta. The problem was fixed with surgery. Additionally, NCS was found by accidentally pressing on the left renal vein, which made the patient’s care more difficult. This case underscores the importance of a multidisciplinary approach to therapy and the necessity of considering both conditions in patients who present with gastrointestinal and renal symptoms. Surgical treatment for SMA syndrome and close monitoring of NCS were very important in making the patient healthier, showing the special way needed for such uncommon and complicated cases.
Ethical Approval
Ethical approval for this study was waived by ethical committee of Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital.
Consent for Publication
Written informed consent was obtained from the patient’s parents for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Disclosure
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript. This manuscript has not been submitted to, nor is under review at, another journal or other publishing venue.
References
1. Diab S, Hayek F. Combined superior mesenteric artery syndrome and nutcracker syndrome in a young patient: a case report and review of the literature. Am J Case Rep. 2020;21:1–5. doi:10.12659/AJCR.922619
2. Ahmad KS, Alenazi NA, Essa MS, Alrushdan MS, Al-Shoaib AM. Laparoscopic duodenojejunostomy for superior mesenteric vein syndrome associated with nutcracker phenomenon: the first case report. Am J Case Rep. 2019;20:1108–1113. doi:10.12659/AJCR.917172
3. Shi Y, Shi G, Li Z, Chen Y, Tang S, Huang W. Superior mesenteric artery syndrome coexists with nutcracker syndrome in a female: a case report. BMC Gastroenterol. 2019;19(1):1–5. doi:10.1186/s12876-019-0932-1
4. Güngörer V, Öztürk M, Arslan Ş. A rare cause of recurrent abdominal pain; the coexistence of Wilkie’s syndrome and nutcracker syndrome. Arch Argent Pediatr. 2023;121(1):1–5.
5. Yakan S, Calıskan C, Kaplan H, Deneclı AG, Coker A. Superior mesenteric artery syndrome: a rare cause of intestinal obstruction. diagnosis and surgical management. Indian J Surg. 2013;75(2):106–110. doi:10.1007/s12262-012-0423-x
6. Aourarh B, Bangda Y, Berrag S, et al. An atypical cause of vomiting: coexisting Wilkie’s syndrome and a left renal malformation mimicking a nutcracker phenomenon—A case report. SAGE Open Med Case Rep. 2023;11:10–13. doi:10.1177/2050313X231176395
7. Inal M, Daphan BU, Bilgili MYK. Superior mesenteric artery syndrome accompanying with nutcracker syndrome: a case report. Iran Red Crescent Med J. 2014;16(10):14–16. doi:10.5812/ircmj.14755
8. Neirouz K, Mohamed H, Aziz A, Belleh ZE, Mestiri H, Dhouha B. Weight loss as a potential trigger for nutcracker syndrome after a complex surgery: about a case report. Int J Surg Case Rep. 2024;123(September):110286. doi:10.1016/j.ijscr.2024.110286
9. Khan H, Al-Jabbari E, Shroff N, Barghash M, Shestopalov A, Bhargava P. Coexistence of superior mesenteric artery syndrome and nutcracker phenomenon. Radiol Case Rep. 2022;17(6):1927–1930. doi:10.1016/j.radcr.2022.03.063
10. Abenavoli L, Imoletti F, Quero G, et al. The diagnosis of Wilkie’s syndrome associated with nutcracker syndrome: a case report and literature review. Diagnostics. 2024;14(17):1844. doi:10.3390/diagnostics14171844
11. Polguj M, Topol M, Majos A. An unusual case of left venous renal entrapment syndrome: a new type of nutcracker phenomenon? Surg Radiol Anat. 2013;35(3):263–267. doi:10.1007/s00276-012-1027-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Investigation and Management of the Abdominopelvic Vascular Compression Syndromes in Patients with Ehlers–Danlos Syndrome and Hypermobility Spectrum Disorder
Bruessel P, Govender M, Frahm-Jensen G
Vascular Health and Risk Management 2026, 22:592420
Published Date: 27 March 2026