Back to Journals » Patient Preference and Adherence » Volume 20
Combined IKAP-Based Continuity Care and Bundle Care in Patients Undergoing Cerebrovascular Interventional Surgery: A Retrospective Study
Authors Shen L, Jia W, Mei X, Lyu J
Received 28 October 2025
Accepted for publication 4 March 2026
Published 7 April 2026 Volume 2026:20 565669
DOI https://doi.org/10.2147/PPA.S565669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Liuyan Shen,1,* Weigui Jia,2,* Xue Mei,3 Jing Lyu4
1Department of Neurosurgery, The 904th Hospital of the Joint Logistics Support Force of Chinese People’s Liberation Army, National Advanced Stroke Center, Wuxi, People’s Republic of China; 2Department of Neurosurgery, Suzou Kowloon Hospital, Shanghai Jiaotong University Shool of Medicine, Suzou, 215028, People’s Republic of China; 3Department of General Surgery, 904th Hospital of Joint Logistics Support Force, Wuxi, Jiangsu, 214044, People’s Republic of China; 4Department of Neurosurgery, Jiangnan University Medical Center, Wuxi, Jiangsu, 214002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Lyu, Email [email protected]
Background: Cerebrovascular interventional surgery requires comprehensive postoperative care for long-term recovery. While bundle care standardizes acute management, it often lacks structured post-discharge support. This study evaluated the added benefit of combining Information-Knowledge-Attitude-Practice (IKAP) theory-based continuity care with bundle care.
Methods: A retrospective comparative study was conducted on 88 patients treated between April 2022 and April 2024. Based on the standard care protocol at admission, patients were non-randomly assigned to a control group (n = 44, receiving bundle care) or an observation group (n = 44, receiving bundle care plus a 3-month IKAP-based continuity care program). The IKAP program included structured WeChat-based education, bi-weekly behavioral coaching, and family support. Outcomes assessed at baseline and 3 months included disease knowledge awareness rate, psychological resilience (Connor-Davidson Resilience Scale, CD-RISC), activities of daily living (Barthel Index, BI), sleep quality (Pittsburgh Sleep Quality Index, PSQI), self-management ability, and patient satisfaction. Analysis of covariance (ANCOVA) was used to compare post-intervention scores between groups, adjusting for baseline values.
Results: Baseline characteristics were comparable between groups (all P > 0.05). At 3 months, the observation group showed a significantly higher disease knowledge awareness rate (93.2% vs. 77.3%, χ2= 4.423, P = 0.035). After adjusting for baseline scores, the observation group also demonstrated significantly greater improvements in psychological resilience (all CD-RISC subscales, P < 0.001), BI score (adjusted mean: 86.8 vs. 73.9, P < 0.001), PSQI score (8.2 vs. 9.8, P = 0.004), and all domains of self-management (all P < 0.001, with large effect sizes Cohen’s d: 1.07– 2.18). Overall patient satisfaction was higher in the observation group (90.9% vs. 70.5%, P = 0.020).
Conclusion: Integrating IKAP-based continuity care with bundle care was associated with better short-term recovery outcomes compared to bundle care alone after cerebrovascular intervention. This model warrants prospective validation.
Keywords: cerebrovascular interventional surgery, bundle care, information-knowledge-belief-behavior theory continuity care, multidisciplinary combined treatment and rehabilitation care, effectiveness, impact
Introduction
Cerebrovascular diseases, encompassing both ischemic and hemorrhagic stroke, constitute a leading global cause of mortality, long-term disability, and healthcare expenditure, profoundly compromising patients’ quality of life.1 Endovascular interventional therapies—such as mechanical thrombectomy for acute ischemic stroke and embolization for intracranial aneurysms—have significantly advanced acute management, improving recanalization rates and short-term outcomes for eligible patients.2 Nevertheless, the post-procedural recovery trajectory remains complex and prolonged. Survivors frequently face persistent physical impairments, psychological sequelae (eg, anxiety, depression), sleep disturbances, and the ongoing demands of secondary prevention, all of which challenge optimal rehabilitation and elevate recurrence risk.3,4
In this context, nursing interventions play a pivotal role in bridging acute treatment and long-term recovery. Bundle care—a standardized, evidence-based set of coordinated practices delivered as a unified package—has been widely implemented in neurovascular settings to enhance perioperative safety and early outcomes through timely monitoring, complication prevention, and structured discharge planning.5,6 However, its impact is often confined to the inpatient phase. A critical limitation lies in the discontinuity of care after discharge, characterized by fragmented follow-up, insufficient psychosocial support, inadequate reinforcement of self-care knowledge, and limited mechanisms to sustain behavior change in the community.7
To address this gap, a theoretically grounded approach to continuity care is warranted. The Information–Knowledge–Attitude–Practice (IKAP) theory offers a compelling framework for promoting sustained health behaviors.8 Unlike models focusing solely on self-efficacy or stages of change, IKAP posits a sequential, causal pathway: exposure to accurate Information fosters comprehensive Knowledge, which shapes positive Attitudes and beliefs, ultimately driving consistent health-related Practices.9 This linear yet dynamic process is particularly well-suited for chronic conditions requiring daily self-management, such as post-stroke care. While IKAP has demonstrated efficacy in hypertension, diabetes, and coronary disease,10,11 its integration into post-interventional cerebrovascular nursing—especially as a continuity extension of acute-phase bundle care—remains unexplored.
We propose that combining these two approaches is theoretically synergistic: bundle care establishes a stable foundation during the acute phase, while IKAP-based continuity care systematically extends support into the community, reinforcing knowledge, cultivating resilience, and guiding practice over time. This integrated model may thus amplify and sustain the benefits of initial interventions.
Critically, successful recovery hinges on multidimensional outcomes beyond procedural success. Psychological resilience enables adaptive coping with life-altering events;12 Activities of Daily Living (ADL) reflect functional independence; sleep quality serves as both an indicator and facilitator of neurological and emotional recovery;13 and robust self-management—encompassing medication adherence, lifestyle modification, and symptom monitoring—is fundamental to secondary stroke prevention.14 Patient satisfaction, meanwhile, captures the perceived patient-centeredness of the entire care continuum.
Therefore, this study aimed to evaluate the effectiveness of a novel combined nursing intervention—integrating IKAP theory–based continuity care with standard bundle care—in patients undergoing cerebrovascular interventional surgery. We hypothesized that, compared to bundle care alone, the integrated approach would yield significantly greater improvements at 3-month follow-up in: (1) disease knowledge awareness, (2) psychological resilience, (3) ADL performance, (4) sleep quality, (5) self-management ability, and (6) care satisfaction. By testing this model, we seek not only to fill a gap in the literature but also to provide a scalable, theory-driven strategy for enhancing the transition from hospital to home in neurovascular recovery.
Materials and Methods
Ethical Statement
This study was approved by the Medical Ethics Committee of Jiangnan University Medical Center (Approval No. NXGHL24-00000017) and conducted in strict accordance with the ethical principles of the Declaration of Helsinki. Informed consent process has changed from being waived by the Medical Ethics Committee of Jiangnan University Medical Center.
Study Design and Patient Enrollment
A retrospective comparative study was conducted on the clinical data of patients who underwent cerebrovascular interventional surgery for cerebrovascular diseases at our hospital from April 2022 to April 2024. The sample size was estimated using G*Power software (version 3.1.9.7). With an effect size (d) set at 0.65 (based on preliminary data for the primary outcome of self-management score), an alpha level of 0.05, and a desired power of 0.80, a minimum of 39 patients per group was required. Anticipating a potential attrition rate of 10%, we aimed to recruit at least 44 patients per group, resulting in a total target enrollment of 88 patients.
Diagnostic and Procedural Classification
All patients had a primary diagnosis of cerebrovascular disease confirmed by imaging, including acute ischemic stroke, intracranial aneurysm, or symptomatic intracranial/extracranial artery stenosis. Disease severity at admission was assessed using the National Institutes of Health Stroke Scale (NIHSS) for ischemic stroke patients and the modified Rankin Scale (mRS) for all patients. The specific interventional procedures performed were categorized as: (1) Mechanical Thrombectomy for acute large vessel occlusion; (2) Endovascular Coiling (with or without stent assistance) for intracranial aneurysms; (3) Intracranial or Carotid Artery Stenting for symptomatic stenosis.
Inclusion and Exclusion Criteria
(1) patients who met the clinical diagnostic criteria for cerebrovascular diseases and were confirmed by brain imaging examination (computed tomography angiography, CTA, or digital subtraction angiography, DSA); (2) patients who received cerebrovascular interventional surgery (including but not limited to intracranial aneurysm coiling, cerebral arteriovenous malformation embolization, or intracranial arterial stenting) at our hospital and had surgical indications; (3) age ≥ 18 years, regardless of gender; (4) patients who were stable after surgery, conscious, and cognitively normal (Mini-Mental State Examination score ≥ 24); (5) patients and their families who were informed of the research content and signed relevant informed consent. The exclusion criteria were: (1) patients with severe other systemic diseases or comorbidities, such as advanced cancer, end-stage renal disease, severe heart failure (NYHA class III–IV), or acute respiratory failure; (2) patients with severe brain hemorrhage (volume > 30 mL) or large-area cerebral infarction (involving >1/3 of the middle cerebral artery territory) that prevented effective rehabilitation training or self-management; (3) patients with other neurological diseases, such as Parkinson’s disease, epilepsy, etc.; (4) pregnant or breastfeeding women; (5) patients who could not fully understand or execute the research content due to cognitive impairment, language barriers, or other reasons, and those who could not provide informed consent; (6) patients who had allergic reactions or contraindications to the treatments and nursing interventions implemented in the study; (7) patients who could not fully cooperate with the study for various reasons. The enrollment flow of participants is presented in Figure 1.
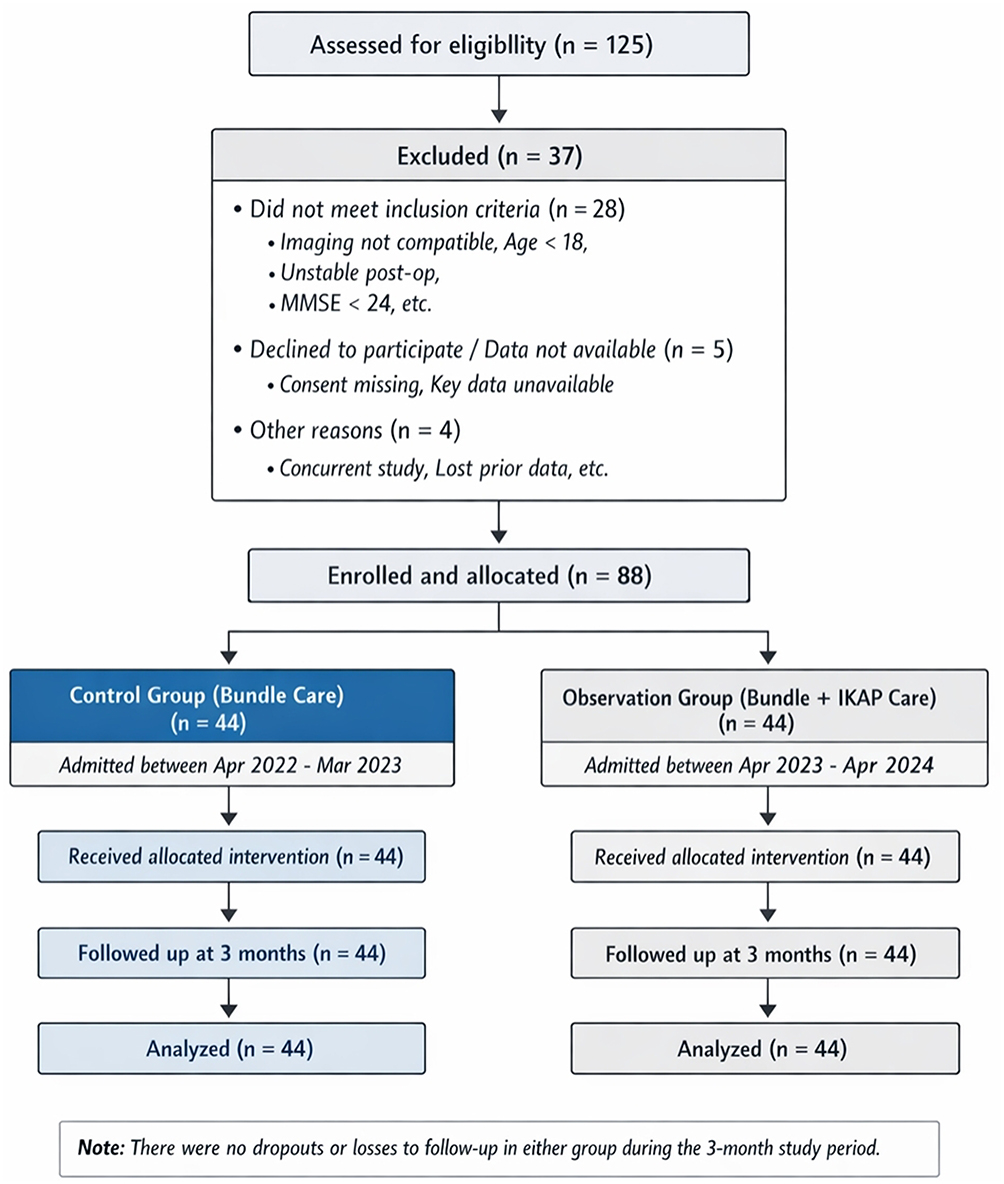 |
Figure 1 Flowchart of patient enrollment, allocation, and follow-up. |
Group Allocation and Rationale
Based on the standard nursing protocols implemented during their hospitalization and post-discharge period, the patients were non-randomly assigned to two groups. This allocation was determined by the standard care model in place at the time of their admission. Patients admitted between April 2022 and March 2023 received the then-standard bundle care intervention and were assigned to the control group (n = 44). Subsequently, based on a quality improvement initiative, the hospital implemented a new, enhanced nursing protocol combining bundle care with IKAP theory-based continuity care for patients admitted from April 2023 to April 2024. These latter patients constituted the observation group (n = 44). This historical control design was employed to evaluate the real-world effectiveness of integrating a new theoretical model into existing clinical practice. We acknowledge that this non-random allocation introduces potential for selection bias. To address this, comprehensive baseline demographic and clinical characteristics (including age, gender, BMI, primary diagnosis, procedural type, disease severity [NIHSS/mRS], and comorbidities) were collected and compared between groups to assess comparability (see Results, Table 1).
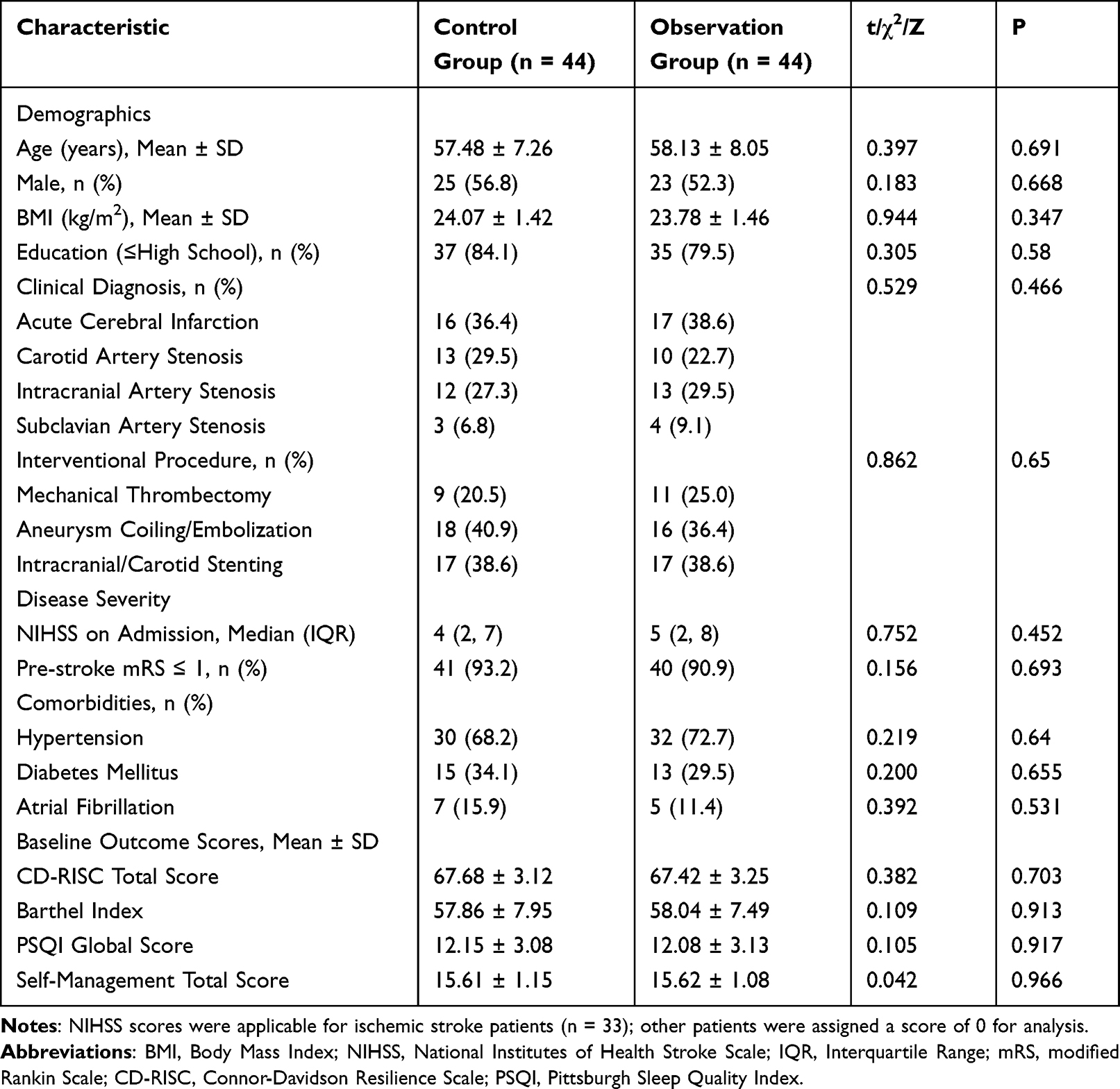 |
Table 1 Comparison of Baseline Demographic and Clinical Characteristics |
Nursing Interventions
All nursing interventions were delivered by a dedicated nursing team. To ensure fidelity and consistency in the implementation of the interventions, a standardized operational manual was developed for both the bundle care and the combined IKAP-Bundle care protocol. The manual detailed each step, communication scripts, and assessment criteria. Intervention fidelity was monitored through: (1) weekly audits by the head nurse reviewing a random sample (20%) of nursing records against a standardized checklist; (2) random patient interviews to confirm receipt and understanding of key intervention components; (3) monthly team meetings to discuss and resolve any implementation challenges. No major protocol deviations were reported.
Control Group: Bundle Care Intervention
The control group received a standardized bundle care intervention, which consisted of the following integrated components applied perioperatively and post-discharge:
- Preoperative Nursing: ① Health Education: Preoperatively, patients were educated on disease and surgery-related knowledge using verbal explanations and visual aids (booklets, diagrams) to ensure a clear understanding. ② Preoperative Preparation and Training: Nurses assisted patients with positioning training and reinforced preoperative basic nursing, including training for bed turning and defecation.
- Intraoperative Nursing: ① Intraoperative Monitoring: Continuous monitoring of vital signs (blood pressure, heart rate, blood oxygen saturation) with immediate reporting of abnormalities. ② Patient Comfort Management: For patients under local anesthesia, emotional support was provided, and comfort measures (eg, soft music) were used. ③ Position Assistance: Nurses assisted in maintaining proper surgical positioning.
- Postoperative and Discharge Nursing: ① Physiological Monitoring and Nursing: Strict bed rest initially, regular comfort assessment, and monitoring for complications (headaches, nausea, vomiting, constipation). ② Postoperative Rehabilitation and Functional Training: A personalized rehabilitation plan (developed with a rehabilitation physician) including speech, physical, and psychological training. ③ Diet and Elimination Management: Guidance on easily digestible, high-fiber diets and hydration; regular turning and skin care for immobile patients. ④ Discharge Preparation and Guidance: A personalized discharge plan covering medication, rehabilitation exercises, and follow-up schedules was provided. A follow-up call was conducted within one week after discharge to assess recovery and adherence.
Observation Group: Combined Bundle Care and IKAP Theory-Based Continuity Care
The observation group received all components of the bundle care plus a structured continuity care program based on the Information-Knowledge-Attitude-Practice (IKAP) theory, extending for three months post-discharge. The program was structured as follows:
- Formation and Training of the Nursing Team: The team (head nurse, charge nurses, senior nurses) received systematic training on the IKAP theory and its application in cerebrovascular disease care, ensuring competency in delivering continuity care.
- Patient Information Collection and Health Record Establishment: Detailed electronic health records were established for each patient. Prior to discharge, nursing staff introduced the continuity care program and guided patients to (a) join a dedicated WeChat group for peer and nurse communication and (b) follow the hospital’s verified public health information channel on WeChat for accessing educational materials and updates.
- Disease Knowledge Dissemination and Health Education (IKAP - Information/Knowledge): A 6-week structured education program was delivered via the WeChat platform: Week 1: Basic disease knowledge; Week 2: Postoperative medication management; Week 3: Neurological rehabilitation exercises; Week 4: Activities of daily living (ADL) training; Week 5: Dietary interventions; Week 6: Mental health management. From Week 2, content from the previous week was reviewed. From Week 7 onward, key topics were cyclically reinforced.
- Behavioral Intervention and Follow-up Support (IKAP - Attitude/Practice): Nurses conducted bi-weekly remote follow-ups (WeChat voice/video calls) for one-on-one behavioral coaching, assessing adherence, and providing personalized guidance. For patients with poor adherence, group discussions or targeted psychological counseling were provided via WeChat to reinforce knowledge and build confidence.
- Family Follow-up and On-Site Support: For patients with persistent non-adherence after remote interventions, nursing staff conducted a single family visit. During the visit, they assessed the home environment, checked medication/diet/exercise compliance, provided on-site guidance, and engaged family members to create a supportive environment.
Both groups received the assigned nursing interventions for a total duration of three months post-discharge before outcome evaluation.
Outcome Measures
All outcome assessments were performed at baseline (pre-intervention) and at the 3-month follow-up, except for satisfaction, which was assessed only at 3 months. To mitigate potential recall and social desirability biases, patients were informed that their responses were confidential and would not affect their care. All scale assessments were conducted through face-to-face or video-call interviews by trained research nurses who were not directly involved in the patient’s daily care. While self-reported measures are essential for capturing patient-perceived knowledge, psychological state, and self-management behaviors, we supplemented these where feasible. For example, the Barthel Index (ADL) score was corroborated with observations from the attending rehabilitation therapist, and medication adherence was cross-checked with pharmacy refill records for a subset of patients during follow-up calls.
- Disease Knowledge Awareness: Assessed using a self-developed cerebrovascular disease knowledge questionnaire (Cronbach’s α = 0.857). It includes 20 items on disease concepts, treatment, medication, and exercises, scored 1–5 per item (total: 20–100). Scores were categorized: Excellent (≥80), Good (60–79), Poor (<60). The awareness rate was calculated as (Good + Excellent cases/Total cases) × 100%.
- Psychological Resilience: Assessed using the Connor-Davidson Resilience Scale (CD-RISC, Chinese version, 20 items, Cronbach’s α = 0.853). It includes three subscales: Toughness, Self-strengthening, and Optimism. Each item is scored 0–4, with higher total scores indicating better resilience.
- Activities of Daily Living (ADL): Assessed using the Barthel Index (BI, Cronbach’s α = 0.834). The total score ranges from 0 to 100, with higher scores indicating better ADL ability.
- Sleep Quality: Assessed using the Pittsburgh Sleep Quality Index (PSQI, Cronbach’s α = 0.836). The global score ranges from 0 to 21, with higher scores indicating poorer sleep quality.
- Self-Management: Assessed using a cerebrovascular disease self-management scale (Cronbach’s α = 0.865), covering disease monitoring, medication, rehabilitation exercise, diet, and emotion management. Higher scores indicate better self-management ability.
- Satisfaction: Assessed using the Newcastle Nursing Service Satisfaction Scale (NSNS, Chinese version, 19 items, Cronbach’s α = 0.846) at 3 months. Scores are categorized: Very Satisfied (≥76), Satisfied (57–75), Fair (38–56), Unsatisfied (<38). Overall satisfaction was calculated as (Very Satisfied + Satisfied cases/Total cases) × 100%.
Statistical Analysis
GraphPad Prism 8 (GraphPad Software, USA) was used for chart creation. Statistical analysis was performed using SPSS 22.0 (IBM Corp., USA). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (Mean ± SD). For between-group comparisons of continuous outcomes at baseline and 3 months, independent samples t-tests were used. Within-group comparisons (baseline vs. 3 months) were performed using paired samples t-tests. Categorical data were presented as numbers (percentages) and compared using the Chi-square test or Fisher’s exact test as appropriate. To control for potential baseline confounding factors (including those highlighted by the reviewer, such as disease severity [NIHSS/mRS], stroke type, key comorbidities, and baseline psychological scores) that showed imbalance (p < 0.10) between groups, analysis of covariance (ANCOVA) was performed for key continuous outcome variables at 3 months, with the baseline score and identified confounders as covariates. A two-tailed p-value < 0.05 was considered statistically significant.
Results
Comparison of Baseline Characteristics
A total of 88 patients were enrolled and completed the 3-month follow-up, with no dropouts or loss to follow-up reported. No intervention-related adverse events were documented during the study period. As detailed in Table 1, the two groups were well-matched at baseline. There were no statistically significant differences in demographic characteristics, clinical diagnoses, procedural types, disease severity indicators, comorbidities, or baseline scores of outcome measures (all P > 0.05).
Disease Knowledge Awareness
At the 3-month follow-up, the observation group demonstrated a significantly higher disease knowledge awareness rate (93.2%, 41/44) compared to the control group (77.3%, 34/44) (χ2 = 4.423, P = 0.035). The distribution of awareness levels is presented in Figure 2.
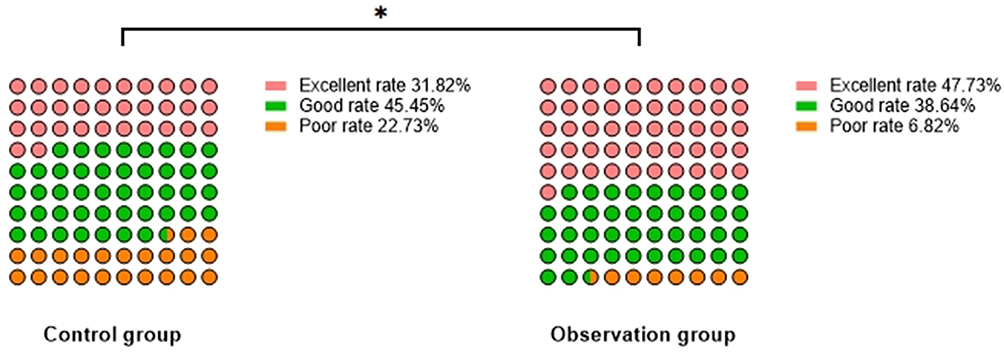 |
Figure 2 Comparison of Disease Knowledge Awareness [n(%)]. Note: Comparison between groups, *P < 0.05. |
Comparison of Psychological Resilience
Both groups showed significant improvement in all CD-RISC subscale scores from baseline to 3 months (all within-group P < 0.05). After adjusting for baseline scores using analysis of covariance (ANCOVA), the observation group exhibited significantly greater post-intervention scores than the control group in toughness (F = 51.63, P < 0.001), self-strengthening (F = 102.10, P < 0.001), and optimism (F = 36.15, P < 0.001) (Table 2).
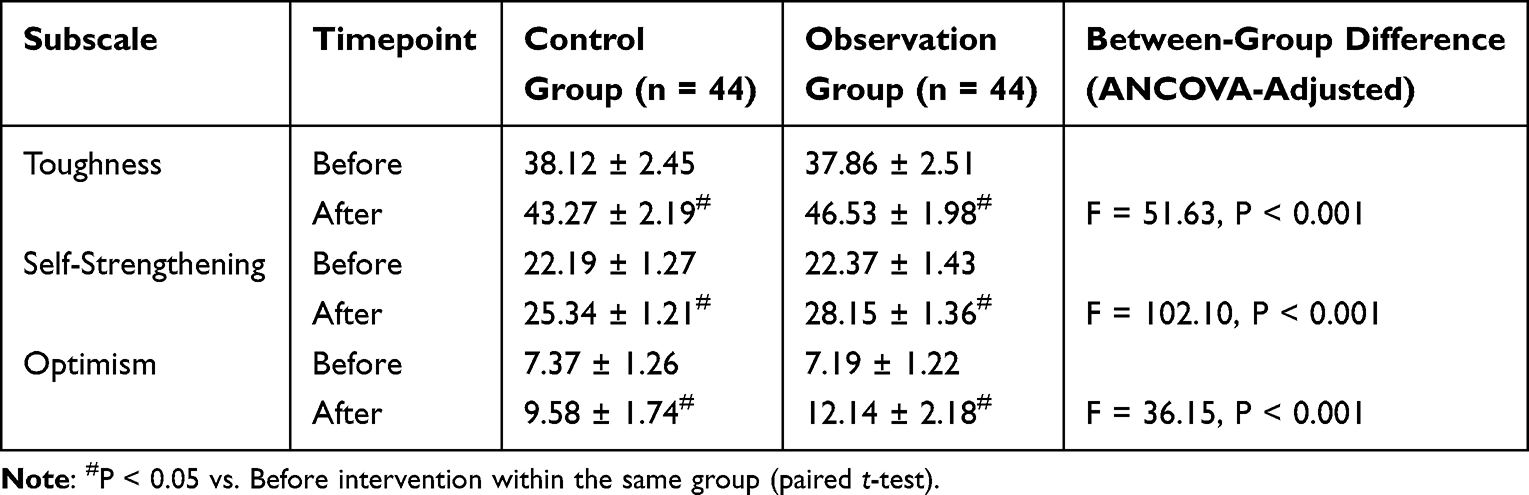 |
Table 2 Comparison of Psychological Resilience Scores (CD-RISC) Before and After Intervention ( |

Comparison of Daily Living Activity and Sleep Quality
Significant improvements in Barthel Index (BI) and Pittsburgh Sleep Quality Index (PSQI) scores were observed in both groups post-intervention (Figure 3). ANCOVA, controlling for baseline scores, revealed that the observation group achieved a significantly higher adjusted mean BI score (86.8 vs. 73.9, F = 58.21, P < 0.001) and a lower adjusted mean PSQI score (8.2 vs. 9.8, F = 9.01, P = 0.004) at 3 months compared to the control group.
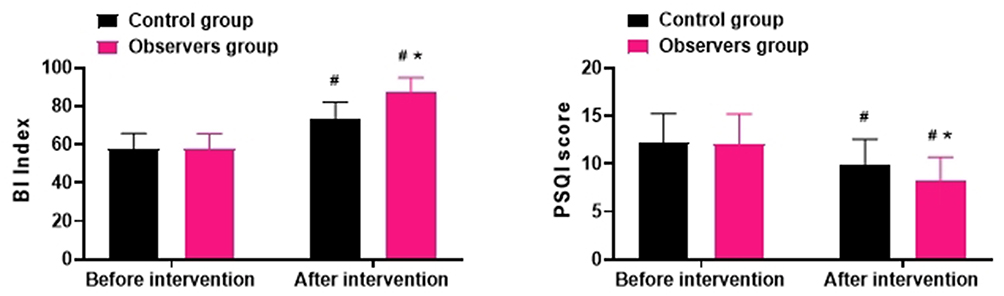 |
Figure 3 Comparison of Daily Living Activity and Sleep Quality ( Notes: Comparison with the control group, *P < 0.05; comparison with pre-intervention within the same group, #P < 0.05. |

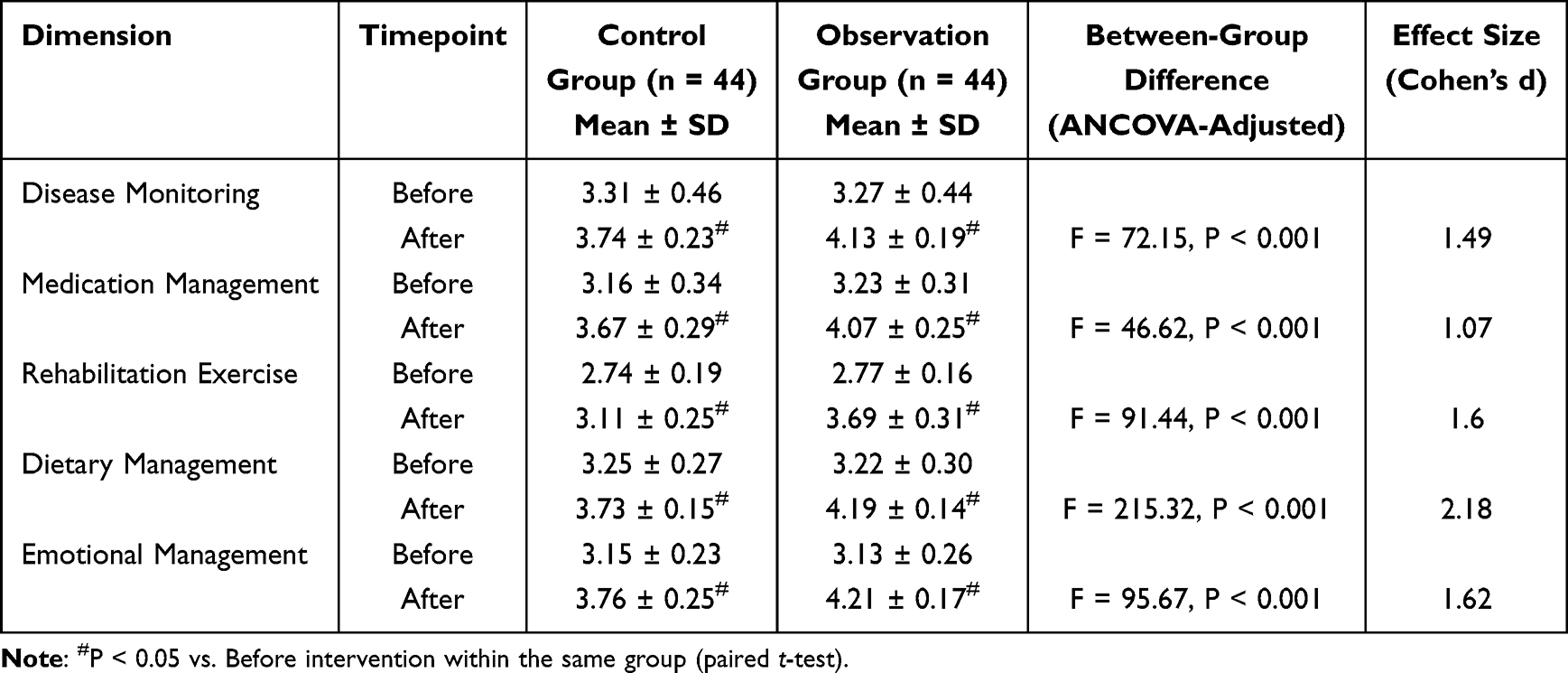
Comparison of Self-Management
All dimensions of self-management improved significantly within both groups (all P < 0.05). The post-intervention scores were significantly higher in the observation group across all five domains (all P < 0.001, ANCOVA adjusted for baseline). The effect sizes (Cohen’s d) for these between-group differences were large, ranging from 1.07 (Medication Management) to 2.18 (Dietary Management) (Table 3).
 |

Patient Satisfaction
Overall satisfaction with nursing care was significantly higher in the observation group (90.9%, 40/44) than in the control group (70.5%, 31/44) (χ2 = 5.436, P = 0.020). The detailed distribution is shown in Figure 4.
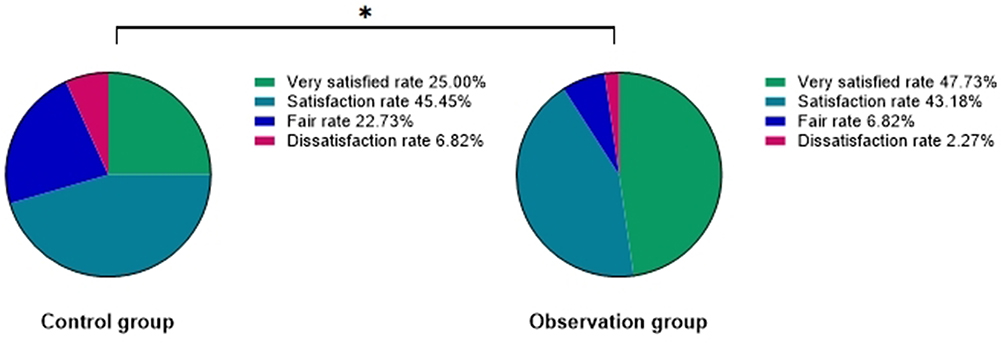 |
Figure 4 Comparison of Satisfaction [n(%)]. Note: Comparison between groups, *P < 0.05. |
Discussion
This study evaluated the effects of integrating IKAP (Information-Knowledge-Attitude-Practice) theory-based continuity care with standard bundle care for patients undergoing cerebrovascular interventional surgery. Compared to bundle care alone, the combined approach was associated with significantly higher rates of disease knowledge awareness, greater improvements in psychological resilience, activities of daily living (ADL), sleep quality, self-management capabilities, and overall patient satisfaction at the 3-month follow-up. These findings suggest that a structured, theory-driven continuity care model may offer multi-faceted benefits in the post-procedural management of cerebrovascular patients.
The enhanced disease knowledge observed in the observation group aligns with the core premise of the IKAP model, which prioritizes systematic information provision and knowledge building. Effective patient education is a cornerstone of chronic disease management, and its importance in secondary stroke prevention is well-established in global guidelines.15 Our structured, multi-channel educational program, delivered via a familiar digital platform (WeChat), may have facilitated better information retention and accessibility compared to conventional one-time discharge instructions. This is consistent with studies demonstrating that repeated, reinforced education improves health literacy and knowledge in cardiac and stroke populations.16,17 By transitioning knowledge dissemination from a passive, inpatient event to an active, prolonged process, the IKAP model likely empowered patients with a clearer framework for understanding their condition and recovery trajectory.
The greater improvements in psychological resilience (encompassing toughness, self-strengthening, and optimism) in the intervention group are noteworthy. Cerebrovascular events are profound psychological stressors, often leading to anxiety, depression, and reduced self-efficacy.18 The IKAP-based care, with its emphasis on transforming knowledge into positive attitudes (“Attitude/Belief” component) and providing ongoing remote support, may have created a buffer against these stressors. Regular check-ins and motivational interviewing could have fostered a stronger therapeutic alliance, while the educational content likely demystified the recovery process, reducing fear of the unknown. This finding resonates with research showing that self-management programs incorporating psychological support can improve mental well-being in chronic illness.19 However, it is important to consider that baseline psychological states, individual coping styles, and levels of family support—factors not fully adjusted for in our analysis—also significantly influence resilience outcomes.20
Improvements in ADL (Barthel Index) and sleep quality (PSQI) are critical patient-centered outcomes. The observed benefits may be attributed to the synergistic effect of improved knowledge, self-management skills, and psychological well-being. Enhanced knowledge about rehabilitation exercises and activity pacing, coupled with behavioral coaching from nurses, likely encouraged more consistent and confident engagement in functional recovery. Similarly, education on sleep hygiene and stress management techniques, integral parts of our IKAP curriculum, may have contributed to better sleep patterns. These results are encouraging as they align with goals of comprehensive stroke rehabilitation.21 Nevertheless, recovery of ADL is multifactorial, influenced by initial stroke severity, the success of the interventional procedure, and the intensity of conventional rehabilitation therapy—variables we attempted to account for through baseline comparison and statistical adjustment but which remain potential residual confounders.
The superior self-management scores across all domains (disease monitoring, medication, exercise, diet, emotion) in the observation group underscore the potential of the IKAP model to translate knowledge and attitude into sustained health practices. Self-management is recognized as a vital component for long-term cardiovascular risk control.22 The IKAP intervention provided not just information but also practical tools, remote accountability, and problem-solving support, which are key elements of effective self-management programs.23 The use of digital tools for follow-up, while effective in our context, introduces considerations of digital literacy and access, which could affect equity in wider implementation.24
High patient satisfaction is a consistent outcome of patient-centered, continuous care models. The significant difference in satisfaction likely reflects the perceived value of extended, accessible support and personalized attention beyond the acute hospital phase. Satisfaction is influenced by meeting patients’ informational and emotional needs, which the IKAP model explicitly targeted.25
Critical Appraisal of Findings and Methodological Considerations
While the results are positive, several important methodological aspects warrant cautious interpretation. First, the non-randomized, historical control design is a key limitation. Although groups were comparable on measured baseline characteristics (Table 1), unmeasured confounding factors—such as subtle differences in disease severity, socioeconomic status, pre-morbid functional status, family support systems, or inherent patient motivation—could account for some of the observed outcome differences. For instance, patients admitted later (observation group) might have benefited from overall temporal improvements in hospital care protocols. Therefore, we interpret these findings as demonstrating a strong association between the combined IKAP-bundle care and improved outcomes, not definitive causation.
Second, the implementation of such an intensive continuity care program has important feasibility implications. It requires a trained, dedicated nursing team, institutional buy-in for non-billable follow-up time, and patient access to and comfort with digital communication tools. Variability in nurses’ communication skills and patients’ engagement with the WeChat platform could have affected the intervention’s delivery and receipt, respectively. Future implementation research should assess cost-effectiveness, nurse workload, and strategies to include patients with limited digital access.
Third, the 3-month follow-up period is suitable for assessing short-term knowledge, behavior adaptation, and initial functional gains but is insufficient to evaluate the sustainability of self-management behaviors, long-term psychological adjustment, or hard endpoints like recurrence rates or mortality. Furthermore, our study focused on average group outcomes. Individual variability in response was not explored; some patients may have derived minimal benefit, possibly due to the intervention’s intensity, personal preferences, or unaddressed barriers.
Conclusion
In this single-center retrospective study, a nursing model combining bundle care with IKAP theory-based continuity care was associated with significantly better short-term outcomes in knowledge, psychological resilience, daily function, sleep, self-management, and satisfaction compared to standard bundle care alone for patients after cerebrovascular intervention. These findings suggest that integrating a structured, theory-driven continuity care framework into post-procedural pathways holds promise for addressing the multifaceted needs of this population. However, the study’s design limits causal inferences. The resource-intensive nature of the intervention and its dependence on digital platforms require consideration for broader scaling. Future prospective, randomized controlled trials with longer follow-up, detailed cost-analysis, and process evaluation are needed to confirm efficacy, assess sustainability, and identify the essential components and target patients most likely to benefit from this combined approach. Such research should also aim to test the model in diverse healthcare and cultural settings to evaluate its generalizability.
Copyright Statement
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR.
Funding
This work has been approved and funded by the science and technology plan of Wuxi Municipal Health Commission. The project number is: T202423.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qu C, Qi SY, Li X, et al. [Predictive value of low-density lipoprotein cholesterol/remnant cholesterol coordination on cardiovascular and cerebrovascular events in elderly patients with hypertension]. Zhonghua Xin Xue Guan Bing Za Zhi. 2023;51(8):844–12. doi:10.3760/cma.j.cn112148-20230107-00017
2. Liu A, Du Y, Ge Z, et al. [Effect of early intervention bundle on clinical prognosis of patients with latent/overt septic shock in emergency department]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(10):1183–1188. doi:10.3760/cma.j.cn121430-20200930-00655
3. Rivera J, Donohoe E, Deady-Rooney M, et al. Implementing a pressure injury prevention bundle to decrease hospital-acquired pressure injuries in an adult critical care unit: an evidence-based, pilot initiative. Wound Manag Prev. 2020;66(10):20–28. doi:10.25270/wmp.2020.10.2028
4. Sheehy L, Taillon-Hobson A, Sveistrup H, et al. Home-based virtual reality training after discharge from hospital-based stroke rehabilitation: a parallel randomized feasibility trial. Trials. 2019;20(1):333. doi:10.1186/s13063-019-3438-9
5. Huo S, Zheng Y, Deng S, et al. [Effect of information-knowledge-attitude-practice theory-based health education on clonorchiasis control among community residents and primary school students in Zhongshan City]. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi. 2023;35(5):517–521. doi:10.16250/j.32.1374.2023023
6. Huo HL, Gui -Y-Y, Xu C-M, et al. Effects of the information-knowledge-attitude-practice nursing model combined with predictability intervention on patients with cerebrovascular disease. World J Clin Cases. 2022;10(20):6803–6810. doi:10.12998/wjcc.v10.i20.6803
7. Wen J, Liu X. Effects of information-knowledge-attitude-practice health education combined with cluster-based care in patients with gestational hypertension. Medicine. 2023;102(41):e35346. doi:10.1097/MD.0000000000035346
8. Liu J, Bai S, Pan H, et al. Caregiver burden and readiness in patients with moderate and severe traumatic brain injury: the chain mediation effect of disease uncertainty and mental resilience. World Neurosurg. 2024;185:e603–e611. doi:10.1016/j.wneu.2024.02.084
9. Hu SJ, Fu SS, Zhu LL, et al. [Therapeutic effect of intravenous thrombolysis with tenecteplase on patients with post awakening branch atheromatous disease]. Zhonghua Yi Xue Za Zhi. 2024;104(23):2173–2178. doi:10.3760/cma.j.cn112137-20231110-01054
10. Li B, Dai M. Effect of information/knowledge/attitude/practice theory-based progressive rehabilitation care on the risk of lower extremity deep venous thrombosis and nutritional status of patients undergoing percutaneous coronary intervention for coronary heart disease. Current Topics Nutraceutical Res. 2024;22(2).
11. Huo HL, Gui YY, Xu CM, Zhang Y, Li Q. Effects of the information–knowledge–attitude–practice nursing model combined with predictability intervention on patients with cerebrovascular disease. World J Clin Cases. 2022;10(20):6803.
12. Park EH, Choi J, Kim PJ, Lee J. Self-care, resilience, and uncertainty in patients after coronary artery bypass graft surgery: a cross-sectional descriptive correlational study. J Cardiovasc Nurs. 2025;40:10–1097. doi:10.1097/JCN.0000000000001074
13. Kimura M, Nakano M, Shiraishi C, et al. Relationship between cardiac rehabilitation and recovery from decline in activities of daily living in patients hospitalized with cardiovascular disease. Circ Rep. 2025;7(11):1051–1059. doi:10.1253/circrep.CR-25-0024
14. Fatema Z, Sigamani A, Manuel D. ‘Quality of life at 90 days after stroke and its correlation to activities of daily living’: a prospective cohort study. J Stroke Cerebrovascular Dis. 2022;31(11):106806. doi:10.1016/j.jstrokecerebrovasdis.2022.106806
15. He M, Lai YQ, Zhang XW, et al. [Characteristics and correlated factors of preoperative sleep disorders in cardiac surgical patients]. Zhonghua Yi Xue Za Zhi. 2024;104(40):3745–3750. doi:10.3760/cma.j.cn112137-20240410-00839
16. Sahely A, Sintler C, Soundy A, et al. Feasibility of a self-management intervention to improve mobility in the community after stroke (SIMS): a mixed-methods pilot study. PLoS One. 2024;19(8):e0286611. doi:10.1371/journal.pone.0286611
17. Yin H. Enhanced Recovery after Surgery (ERAS) in postoperative lung cancer patients: a novel perioperative strategy for preventing venous thromboembolism and improving quality of life. Tohoku J Exp Med. 2024;262(3):201–209. doi:10.1620/tjem.2023.J105
18. Alves LS, Dutra LS, Santos LN, et al. Remote cognitive rehabilitation in patients post-cerebrovascular accident: an experience report. Alzheimers Dement. 2021;17 Suppl 12:e058382. doi:10.1002/alz.058382
19. Cun W, Xu K, Chai Q, et al. Factors affecting the readmission of patients with stroke. World Neurosurg. 2025;194:123572. doi:10.1016/j.wneu.2024.123572
20. Li HR, Guo Y. High-risk factors for delirium in severely ill patients and the application of emotional nursing combined with pain nursing. World J Psychiatry. 2024;14(7):1027–1033. doi:10.5498/wjp.v14.i7.1027
21. Xiong HL, Li Z-X, Lu X, et al. Impact of early refined nursing program on prognosis of middle-aged and elderly patients with cognitive dysfunction combined with cerebral infarction. World J Psychiatry. 2024;14(7):1034–1042. doi:10.5498/wjp.v14.i7.1034
22. Love MF, Sharrief A, Chaoul A, et al. Mind-body interventions, psychological stressors, and quality of life in stroke survivors. Stroke. 2019;50(2):434–440. doi:10.1161/STROKEAHA.118.021150
23. Yin L, Zhang W, Liu L, et al. Application of nursing intervention based on the IKAP model in self-management of patients with gastric cancer. Am J Transl Res. 2022;14(9):6389–6398.
24. Dicpinigaitis AJ, Li B, Ogulnick J, et al. Evaluating the impact of neurosurgical educational interventions on patient knowledge and satisfaction: a systematic review of the literature. World Neurosurg. 2021;147:70–78. doi:10.1016/j.wneu.2020.11.144
25. Mandel M, Tutihashi R, Li Y, et al. MISIAN (Minimally Invasive Surgery for Treatment of Unruptured Intracranial Aneurysms): a prospective randomized single-center clinical trial with long-term follow-up comparing different minimally invasive surgery techniques with standard open surgery. World Neurosurg. 2021;151:e533–e544. doi:10.1016/j.wneu.2021.04.079
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.