Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Combination Therapy with 308-nm Excimer Laser, Compound Glycyrrhizin, and Tacrolimus for Pediatric Facial and Cervical Vitiligo
Authors Qian Y, Wu Y, Li W, Chen Q, Song S, Zhang T
Received 2 January 2026
Accepted for publication 23 March 2026
Published 27 March 2026 Volume 2026:19 593313
DOI https://doi.org/10.2147/CCID.S593313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yingying Qian,1 Yafen Wu,1 Wei Li,1 Qian Chen,1 Siyuan Song,2 Ting Zhang1
1Department of Dermatology, Children’s Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Department of Neuroscience, Baylor College of Medicine, Houston, TX, USA
Correspondence: Siyuan Song, Email [email protected] Ting Zhang, Email [email protected]
Background: Vitiligo is a common acquired depigmenting disorder in pediatric dermatology. Facial and cervical involvement is particularly distressing due to cosmetic disfigurement, leading to psychosocial impairment in children and significant psychological burden for parents. Safe and effective treatment strategies to halt disease progression and promote repigmentation are urgently needed.
Objective: To evaluate the clinical efficacy, onset of repigmentation, safety, and repigmentation patterns of 308-nm excimer laser combined with oral compound glycyrrhizin and topical 0.03% tacrolimus in children with facial and cervical vitiligo.
Methods: A total of 112 pediatric patients were randomized into two groups: treatment group (n=56, 86 lesions) received oral compound glycyrrhizin, topical 0.03% tacrolimus, plus 308-nm excimer laser twice weekly for 16 weeks; control group (n=56, 78 lesions) received compound glycyrrhizin and tacrolimus only. Clinical efficacy, time to initial repigmentation, adverse events, and repigmentation patterns (marginal, follicular, mixed) were assessed.
Results: The overall efficacy rate was significantly higher in the treatment group (89.53%) than in controls (70.51%) (p< 0.05). Initial repigmentation occurred earlier in the treatment group (face: 3.12± 0.45 weeks; neck: 3.74± 0.44 weeks) compared with controls (face: 4.08± 0.50 weeks; neck: 4.54± 0.51 weeks, both p< 0.05). Adverse events were rare (3.57%) and self-limited. Repigmentation patterns differed: treatment lesions showed predominantly mixed repigmentation (65.12%), whereas controls were mainly follicular (57.69%).
Conclusion: Combination therapy with 308-nm excimer laser, compound glycyrrhizin, and 0.03% tacrolimus is safe and effective for pediatric facial and cervical vitiligo, providing faster repigmentation, higher efficacy, and distinct repigmentation patterns compared with medical therapy alone.
Keywords: vitiligo, pediatric, excimer laser, tacrolimus, glycyrrhizin, repigmentation pattern
Introduction
Vitiligo is a chronic acquired depigmenting disorder that affects the skin and mucosa, characterized by progressive loss of functional melanocytes and consequent development of depigmented macules. Epidemiological investigations in China have shown a prevalence of approximately 0.56%, highlighting the significant disease burden in the general population.1 Notably, one-third to one-half of patients develop vitiligo during childhood, and global studies have reported that about 25% of cases have onset before the age of 14.2 Facial and cervical involvement is particularly distressing in pediatric patients, given the high visibility of lesions. Such cosmetic disfigurement often results in psychosocial impairment, including social withdrawal, low self-esteem, and anxiety, and also imposes a considerable psychological burden on parents and caregivers.
Although multiple therapeutic modalities are available—including narrowband UVB phototherapy, excimer light/laser therapy, topical corticosteroids, calcineurin inhibitors, and systemic immunomodulators—the optimal regimen for children remains challenging because of safety concerns, limited tolerance, and the risk of long-term side effects. In recent years, the 308-nm excimer laser, a targeted UVB phototherapy, has emerged as an effective and well-tolerated treatment option. Several clinical trials and pediatric cohort studies have demonstrated that excimer laser therapy can achieve rapid repigmentation and durable responses, especially when combined with topical tacrolimus, compared to monotherapy alone.3,4 Topical tacrolimus, as a calcineurin inhibitor, offers the advantage of local immunomodulation without the adverse effects of topical corticosteroids, making it particularly suitable for use in children.5 In addition, oral compound glycyrrhizin, widely used in some regions of Asia, has been reported to exert immunoregulatory and anti-inflammatory effects, thereby stabilizing disease activity and preventing further progression. Its favorable safety profile makes it a rational adjunctive therapy in pediatric vitiligo management.
Taken together, these findings support the potential benefits of multimodal combination therapy in pediatric vitiligo, particularly for lesions on the face and neck, which are cosmetically sensitive areas. The present study therefore summarizes a clinical observation involving 112 pediatric patients with facial and cervical vitiligo, and systematically compares the efficacy, safety, onset of repigmentation, and repigmentation patterns between combination therapy with 308-nm excimer laser, oral compound glycyrrhizin, and topical tacrolimus, versus medical therapy alone.
Methods
Study Design and Participants
This study was conducted in the Department of Dermatology, Children’s Hospital of Soochow University; patient records were collected between July 2024 and May 2025. A total of 112 children with clinically diagnosed vitiligo affecting the face and/or neck were enrolled. All patients were randomized by a simple randomization method into a treatment group (56 patients, 86 lesions) or a control group (56 patients, 78 lesions).
Eligible patients were required to meet the diagnostic criteria for vitiligo and to have received no prior treatment before enrollment. Patients were excluded if they had poor compliance that prevented treatment, known photosensitivity or coexisting photosensitive disorders, or severe impairment of cardiac, hepatic, or renal function.
The study was approved by the Ethics Committee of the Children’s Hospital of Soochow University (Approval No. 2024C5098). Written informed consent was obtained from the parents or legal guardians of all participants.
Interventions
Patients in the control group were treated with oral compound glycyrrhizin tablets (25 mg per dose, three times daily) in combination with topical tacrolimus 0.03% ointment applied twice daily to the lesions. The treatment group received the same regimen in addition to 308-nm excimer laser therapy (Alma, Israel), which was performed twice weekly at approximately three-day intervals for 16 consecutive weeks.
Prior to laser treatment, the minimal erythema dose (MED) was determined for each patient. The initial irradiation dose was set at 0.5 × MED, with a maximum safe dose of 3 J/cm2 for the face and neck. Dose adjustments were based on the duration of post-irradiation erythema: if erythema lasted for 24–48 hours, the same dose was maintained; if erythema resolved within 24 hours, the dose was increased by 15–20%; and if erythema persisted for more than 48 hours, the dose was reduced by 15–20%. The area surrounding each lesion was covered with custom-made black cloth shields to avoid unnecessary exposure of unaffected skin.
Outcomes
The primary outcome was clinical efficacy, which was evaluated after 16 weeks of treatment. Efficacy was classified as follows: cure, defined as complete disappearance of depigmentation with restoration of normal skin color; marked improvement, defined as repigmentation covering at least 50% of the lesion; improvement, defined as repigmentation covering 10–49% of the lesion; and no response, defined as less than 10% repigmentation or enlargement of the lesion.6,7 The overall efficacy rate was calculated as the proportion of cured and markedly improved lesions among the total.
Secondary outcomes included the time to initial repigmentation, the incidence of adverse events, and the pattern of repigmentation. The time to initial repigmentation was defined as the interval from the start of treatment to the first visible return of pigment on the face or neck. Adverse events, such as burning sensation, erythema, blistering, secondary infection, or folliculitis, were recorded throughout treatment. Repigmentation patterns were classified using standardized digital photographs as marginal, follicular, or mixed. In this study, lesions previously described as showing “central” repigmentation were reclassified as follicular repigmentation, referring to pigment islands arising within the lesion and consistent with perifollicular repigmentation.
Statistical Analysis
All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD) and compared between groups using independent-sample t-tests. Categorical variables were presented as frequencies and percentages and analyzed using χ2-tests. A p-value <0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
A total of 112 children with facial and cervical vitiligo were enrolled, including 56 patients (86 lesions) in the treatment group and 56 patients (78 lesions) in the control group. The mean age was 6.20 ± 0.95 years (range, 4–8 years) in the treatment group and 6.45 ± 1.05 years (range, 3–9 years) in the control group. The mean disease duration was 3.80 ± 2.40 months in the treatment group and 3.65 ± 2.70 months in the control group. There were no significant differences between the two groups in age, sex distribution, disease duration, number of lesions per patient, lesion location, Fitzpatrick skin phototype, clinical subtype, or family history of vitiligo (all p > 0.05). These findings confirmed that the baseline characteristics were well balanced and comparable between groups (Table 1).
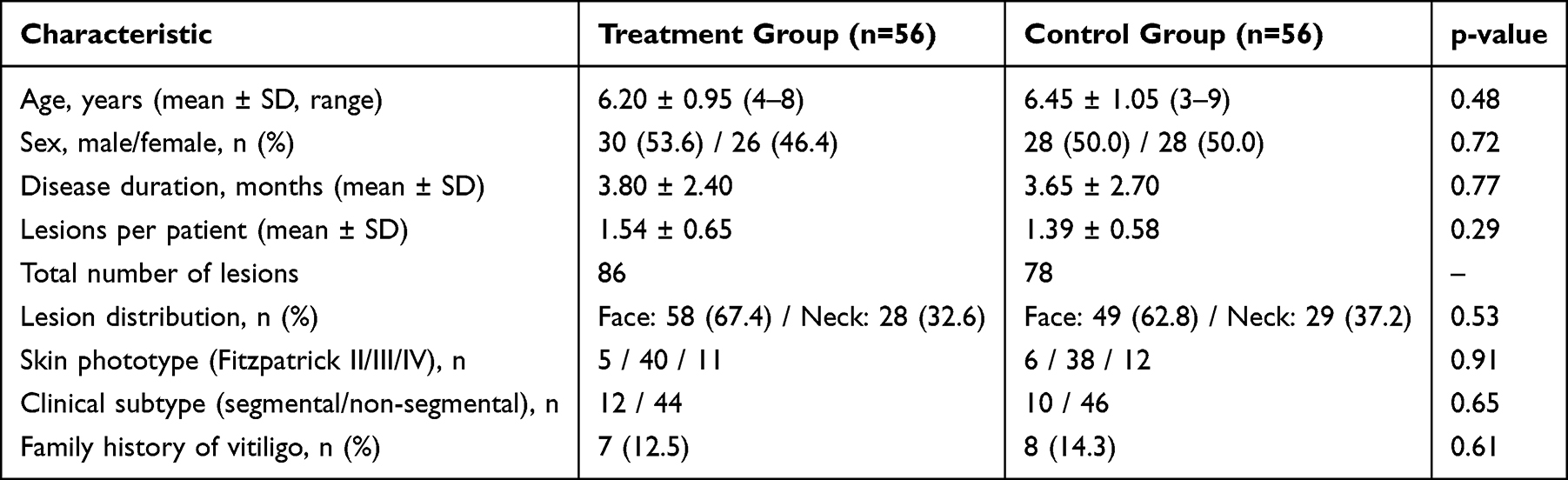 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients |
Clinical Efficacy
After 16 weeks of treatment, the overall efficacy rate in the treatment group was significantly higher than that in the control group. Among 86 lesions in the treatment group, 38 (44.19%) achieved complete repigmentation, 39 (45.35%) showed marked improvement, 7 (8.14%) showed partial improvement, and 2 (2.33%) showed no response, yielding an overall efficacy of 89.53%. In comparison, the control group (78 lesions) showed cure in 17 lesions (21.79%), marked improvement in 38 (48.72%), improvement in 17 (21.79%), and no response in 6 (7.69%), with an overall efficacy of 70.51%. The between-group difference was statistically significant (overall 4×2 distribution: p=0.0031; overall efficacy comparison: p=0.0021) (Table 2). A representative case from the combination-therapy group showing progressive repigmentation over 16 weeks, with a predominantly mixed repigmentation pattern on the lower lip and chin, is shown in Figure 1.
 |
Table 2 Clinical Efficacy After 16 weeks of Treatment |
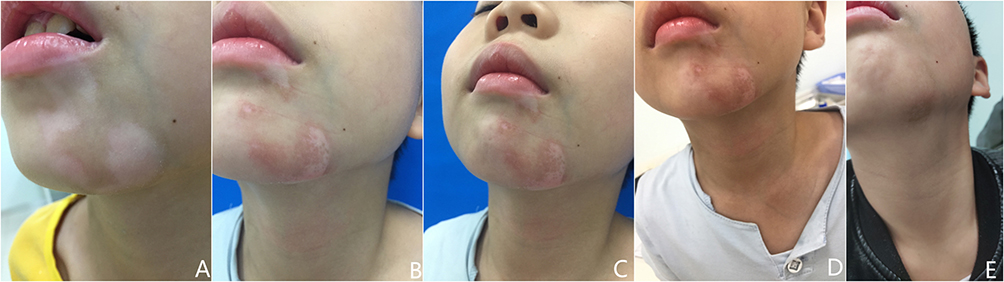 |
Figure 1 Representative case from the treatment group: vitiligo of the lower lip and chin. (A) Before treatment; (B) after 4 weeks; (C) after 8 weeks; (D) after 12 weeks; (E) after 16 weeks of combination therapy. Progressive repigmentation is observed with a predominance of the mixed repigmentation pattern. |
Time to Initial Repigmentation
The onset of repigmentation was earlier in the treatment group than in the control group. In the treatment group, initial repigmentation occurred at 3.12 ± 0.45 weeks for facial lesions and 3.74 ± 0.44 weeks for cervical lesions, whereas in the control group the corresponding times were 4.08 ± 0.50 weeks and 4.54 ± 0.51 weeks, respectively. Both site-specific comparisons demonstrated statistically significant differences (p<0.001) (Table 3). A representative forehead lesion demonstrating marginal repigmentation beginning at the lesion borders during combination therapy is presented in Figure 2.
 |
Table 3 Time to Initial Repigmentation (weeks, Mean ± SD) |
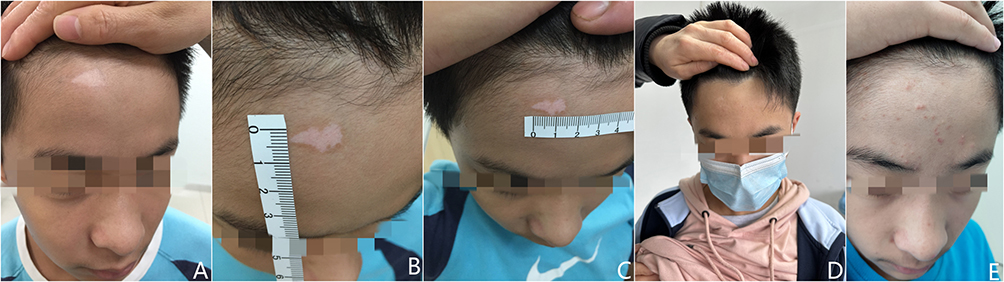 |
Figure 2 Representative case from the treatment group: vitiligo of the forehead. (A) Before treatment; (B) after 4 weeks; (C) after 8 weeks; (D) after 12 weeks; (E) after 16 weeks of combination therapy. Repigmentation begins at the lesion margins, showing a marginal repigmentation pattern. |
Adverse Events
Adverse events were infrequent and mild. Two patients (3.57%) in the treatment group developed localized erythema with fine scaling, which resolved spontaneously after suspending laser therapy for two weeks. No cases of blistering, secondary infection, or systemic adverse effects occurred. The incidence of adverse events did not differ significantly between groups (p>0.05).
Repigmentation Patterns
Repigmentation patterns differed significantly between groups. In the treatment group, mixed repigmentation predominated, accounting for 56 of 86 lesions (65.12%), followed by marginal (20.93%) and follicular (13.95%) patterns. In contrast, lesions in the control group most frequently exhibited follicular repigmentation (57.69%), followed by mixed (23.08%) and marginal (19.23%) patterns. The overall distribution difference between the two groups was highly significant (p=4.17 × 10−9) (Table 4). A representative cheek lesion exhibiting a mixed repigmentation pattern with pigment islands appearing both centrally and peripherally is illustrated in Figure 3.
 |
Table 4 Repigmentation Patterns After Treatment |
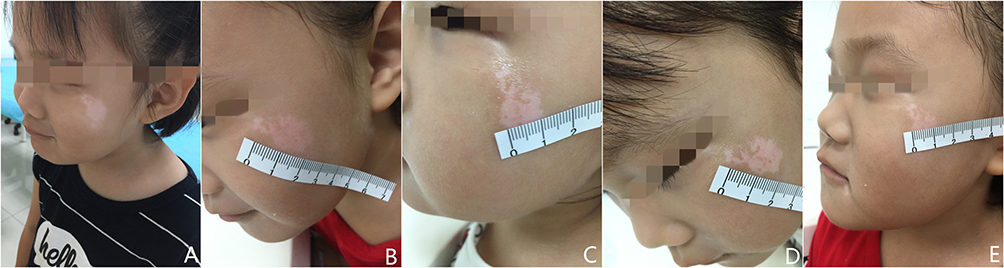 |
Figure 3 Representative case from the treatment group: vitiligo of the left cheek. (A) Before treatment; (B) after 4 weeks; (C) after 8 weeks; (D) after 12 weeks; (E) after 16 weeks of combination therapy. Pigment islands appear within the lesion and at the margins, consistent with a mixed repigmentation pattern. |
Discussion
This randomized clinical observation indicates that adding 308-nm excimer laser to oral compound glycyrrhizin and topical 0.03% tacrolimus improves outcomes for pediatric facial and cervical vitiligo, yielding higher overall efficacy and earlier onset of repigmentation than medical therapy alone. Our findings are consistent with prior pediatric and mixed-age cohorts and trials. In children, topical therapy combined with 308-nm excimer showed superior responses versus excimer monotherapy.3 A recent pediatric randomized controlled trial likewise demonstrated that 308-nm excimer lamp plus tacrolimus outperformed tacrolimus alone for limited vitiligo.4 Open-label data in segmental vitiligo further support the safety and benefit of combining monochromatic excimer light with topical tacrolimus.5 Earlier pediatric series confirmed favorable tolerability and efficacy of the 308-nm excimer laser in children.8 Mechanistic and clinical synergy between topical tacrolimus and 308-nm excimer was shown in a controlled adult study.9 Variable-analysis work identified treatment parameters and patient-site factors that influence laser response,10,11 and a focused review summarized dosing, scheduling, and safety considerations for monochromatic excimer devices in vitiligo.12
Anatomical site remains a major determinant of therapeutic response. UV-sensitive sites such as the face and neck generally repigment faster than acral areas, a pattern also noted in prior excimer cohorts and dosing-frequency studies.10,12–15 Mechanistically, predominant mixed (perifollicular + marginal) repigmentation in the combination arm plausibly reflects activation of both follicular melanocyte reservoirs and perilesional melanocytes. Classic and contemporary work supports the concept that hair-follicle melanocyte (stem/precursor) pools drive perifollicular repigmentation and, together with border spread, account for the clinical patterns observed during UV-based therapies.16
Multiple, non-exclusive biological effects likely underlie the superiority of the combined regimen. Narrowband/monochromatic UVB induces apoptosis of skin-infiltrating T cells and reshapes the cutaneous immune milieu, dampening the autoimmune attack on melanocytes.17 UV exposure also increases keratinocyte-derived endothelin-1, a potent melanogenic and melanocyte-migratory factor, thereby promoting melanocyte proliferation and dendricity within vitiliginous skin.18,19 Topical tacrolimus, by inhibiting calcineurin-dependent T-cell activation locally, complements these effects and has shown clinical synergy with 308-nm excimer in controlled and uncontrolled studies.3,9 In parallel, compound glycyrrhizin—used as an immunomodulator in parts of Asia—has been associated with improved repigmentation when combined with UV-based regimens and exhibits a favorable pediatric safety profile, providing a rationale for its inclusion in a child-friendly, steroid-sparing protocol.20
Safety in our study was excellent, with only transient, self-limited erythema and scaling in a small minority of patients undergoing laser therapy. This aligns with pediatric excimer series and broader reviews of monochromatic excimer light that report low rates of short-term adverse events and no signal for systemic toxicity when appropriately dosed and shielded.8,11,12 Practical aspects (MED-based dosing, facial/neck dose ceilings, and twice-weekly scheduling) follow published experience on parameter selection and treatment frequency for optimizing efficacy while minimizing irritancy.12,13
Finally, durability deserves emphasis. Even after successful repigmentation, relapse is common without maintenance; estimates around 30–40% within the first year have been reported, and twice-weekly tacrolimus maintenance has shown promise in reducing early recurrence.21 Although our trial was limited to 16 weeks and not designed to assess long-term maintenance, these data support counseling families about recurrence risk and considering steroid-sparing maintenance strategies once repigmentation is achieved.
This study has some limitations. It was a single-center study with a relatively short duration of 16 weeks, and longer follow-up is required to assess the durability of repigmentation and the risk of relapse. In addition, simple randomization without blinding may introduce some degree of observer bias, despite the use of standardized photographic documentation. Future multicenter studies with longer observation periods and blinded assessments are warranted.
Conclusions
The combination of 308-nm excimer laser, oral compound glycyrrhizin, and topical 0.03% tacrolimus is a safe and effective treatment option for pediatric facial and cervical vitiligo. This regimen not only improves overall efficacy and accelerates the onset of repigmentation but also induces a characteristic mixed repigmentation pattern. Given its favorable safety profile and cosmetic benefits in sensitive areas, this combination therapy represents a valuable approach for children with vitiligo.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors, Siyuan Song and Ting Zhang, upon reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Children’s Hospital of Soochow University (Approval No. 2024C5098). Written informed consent was obtained from the parents or legal guardians of all participants, and consent for publication of anonymized clinical photographs was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wang X, Du J, Wang T, et al. Prevalence and clinical profile of vitiligo in China: a community-based study in six cities. Acta Derm Venereol. 2013;93(1):62–8. doi:10.2340/00015555-1397
2. Ju HJ, Seo JM, Kim SH, Bae JM, Lee YB. Quality of life in parents of children and adolescents with vitiligo: a qualitative study. Ann Dermatol. 2023;35(6):472–475. doi:10.5021/ad.22.150
3. Li L, Liang Y, Hong J, Lan L, Xiao H, Xie Z. The effectiveness of topical therapy combined with 308-nm excimer laser on vitiligo compared to excimer laser monotherapy in pediatric patients. Pediatr Dermatol. 2019;36(1):e53–e5. doi:10.1111/pde.13726
4. Alshiyab D, Ba-Shammakh SA, Al-Fakih A, et al. Efficacy and safety of 308-nm excimer lamp combined with tacrolimus 0.1% ointment vs tacrolimus 0.1% ointment as monotherapy in treating children with limited vitiligo: a randomized controlled trial. J DermatolTreat. 2024;35(1):2296851. doi:10.1080/09546634.2023.2296851
5. Shah S, Sakhiya J, Deshpande P, Sakhiya D, Inamadar AC. Safety and efficacy of the combination of 308-nm monochromatic excimer light and topical 0.1% tacrolimus ointment in segmental vitiligo: an open-label study. J Clin Aesthet Dermatol. 2020;13(2):E69–E75.
6. Sun Y, Guan X, Wang H, et al. Randomized clinical trial of combined therapy with oral α-lipoic acid and NB-UVB for nonsegmental stable vitiligo. Dermatol Ther. 2021;34(1):e14610. doi:10.1111/dth.14610
7. Renert-Yuval Y, Desai S, Huang V, Walsh S, Rosmarin D, Silverberg N. A review of the vitiligo literature to standardize expression of disease severity. J Drugs Dermatol. 2024;23(10):842–846. doi:10.36849/JDD.8049
8. Cho S, Zheng Z, Park Y-K, Roh MR. The 308-nm excimer laser: a promising device for the treatment of childhood vitiligo. Photodermatol Photoimmunol Photomed. 2011;27(1):24–29. doi:10.1111/j.1600-0781.2010.00558.x
9. Passeron T, Ostovari N, Zakaria W, et al. Topical tacrolimus and the 308-nm excimer laser: a synergistic combination for the treatment of vitiligo. Arch Dermatol. 2004;140(9):1065–1069. doi:10.1001/archderm.140.9.1065
10. Ostovari N, Passeron T, Zakaria W, et al. Treatment of vitiligo by 308-nm excimer laser: an evaluation of variables affecting treatment response. Lasers Surg Med. 2004;35(2):152–156. doi:10.1002/lsm.20057
11. Hadi SM, Spencer JM, Lebwohl M. The use of the 308-nm excimer laser for the treatment of vitiligo. Dermatol Surg. 2004;30(7):983–986. doi:10.1111/j.1524-4725.2004.30302.x
12. Park KK, Liao W, Murase JE. A review of monochromatic excimer light in vitiligo. Br J Dermatol. 2012;167(3):468–478. doi:10.1111/j.1365-2133.2012.11008.x
13. Shen Z, Gao T-W, Chen L, et al. Optimal frequency of treatment with the 308-nm excimer laser for vitiligo on the face and neck. Photomed Laser Surg. 2007;25(5):418–427. doi:10.1089/pho.2007.2086
14. Mitsuma S, Ishigaki E, Sugiyama R, Asamizu T, Yamada K, Kurosaki F. Activation of phenylpropanoid metabolism in sesame by over-expression of carrot calmodulin gene. Biol Pharm Bull. 2004;27(10):1621–1625. doi:10.1248/bpb.27.1621
15. Lin J-Y, Lin C-Y. Nonsurgical lower eyelid rejuvenation using injectable poly- d, l -lactic acid in Asian patients. J Cosmet Dermatol. 2022;21(10):4328–4331. doi:10.1111/jocd.15047
16. Falabella R. Vitiligo and the melanocyte reservoir. Indian J Dermatol. 2009;54(4):313–318. doi:10.4103/0019-5154.57604
17. Sallusto F, Lanzavecchia A. Mobilizing dendritic cells for tolerance, priming, and chronic inflammation. J Exp Med. 1999;189(4):611–614. doi:10.1084/jem.189.4.611
18. Imokawa G, Miyagishi M, Yada Y. Endothelin-1 as a new melanogen: coordinated expression of its gene and the tyrosinase gene in UVB-exposed human epidermis. J Invest Dermatol. 1995;105(1):32–37. doi:10.1111/1523-1747.ep12312500
19. Hara M, Yaar M, Gilchrest BA. Endothelin-1 of keratinocyte origin is a mediator of melanocyte dendricity. J Invest Dermatol. 1995;105(6):744–748. doi:10.1111/1523-1747.ep12325522
20. Mou KH, Han D, Liu WL, Li P. Combination therapy of orally administered glycyrrhizin and UVB improved active-stage generalized vitiligo. Braz J Med Biol Res. 2016;49(8). doi:10.1590/1414-431x20165354
21. Cavalie M, Ezzedine K, Fontas E, et al. Maintenance therapy of adult vitiligo with 0.1% tacrolimus ointment: a randomized, double blind, placebo–controlled study. J Invest Dermatol. 2015;135(4):970–974. doi:10.1038/jid.2014.527
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.