Back to Archived Journals » Open Access Surgery » Volume 16
Colostomy Patient Lived Experience at Public Hospitals of Addis Ababa, Ethiopia: Phenomenology
Received 28 January 2023
Accepted for publication 28 April 2023
Published 9 May 2023 Volume 2023:16 Pages 13—23
DOI https://doi.org/10.2147/OAS.S406211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Luigi Bonavina
Daniel Aboma,1 Mirgissa Kaba2
1Department of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Preventive Medicine, School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Daniel Aboma, Department of Public Health, St. Paul’s hospital Millennium Medical college, Addis Ababa, Ethiopia, Email [email protected]
Background: Colostomy is believed to alter patients’ health, as well as their personal, social, and professional lives. However, there is limited evidence. The aim of this study is to explore the lived experiences of individual with colostomy.
Methods: A phenomenological study was conducted in Public hospitals of Addis Ababa to explore the lived experiences of individuals who had undergone colostomy in the last three months. The study employed purposive sampling to select nine participants who met the specific criteria. Data was collected using a semi-structured interview guide, which included open-ended questions to facilitate detailed responses. The data was analyzed using the content analysis approach.
Finding: In this study, nine married individuals aged between 27– 55 years with colostomies were included, and the research identified four themes. The psychological impacts of colostomy included emotions such as disbelief, shame, despair, sleep disorder, acceptance of life with a colostomy, and difficulty in maintaining a sexual life. Participants also reported physical activity challenges, including difficulty in performing daily activities and sexual issues. Social isolation and stigma were identified as issues faced by individuals with a colostomy; however, social support from family and friends was found to be crucial. Additionally, religious practices were challenging due to the fear of the bag exploding, bending, and standing. Finally, one patient mentioned financial difficulties due to the cost of purchasing extra colostomy bags.
Conclusion: The study emphasizes the challenges faced by patients with colostomy in psychological, physical, financial, and social aspects of their lives. The availability of social and professional support influences the adaptation process, and seeking help from support groups and healthcare professionals is crucial in improving patients’ quality of life and ability to manage their condition.
Keywords: lived-experience, phenomenology, colostomy, Addis Ababa
Introduction
A colostomy is a surgical procedure that involves creating an opening (stoma) in the abdominal wall through which feces can pass out of the body into a bag or pouch.1 This procedure is often performed to treat conditions such as colon cancer, inflammatory bowel disease, or diverticulitis.2 Two major types of colostomy procedures are performed based on the remaining colon and pathologic findings: Temporary and Permanent colostomy.3 While colostomy can be life-saving, it can also have a significant impact on the patient’s quality of life.3 Patients with colostomy may experience a wide range of physical, psychological, financial, and social challenges.4 These challenges may include difficulty in daily activities, sleep disorders, shame, stigma, social isolation, and sexual issues.5
In the United States, over 130,000 intestinal stomas are created each year,6 while in Europe the number is estimated to be around 100,0007 and in Africa the number is generally lower due to limited healthcare resources and a higher burden of communicable diseases.8 The actual number of intestinal stomas may vary based on several factors, including the prevalence of conditions that require stoma surgery, advancements in surgical techniques, and changes in healthcare policies and practices.9 Nonetheless, stoma surgery remains an important treatment option for many people facing serious gastrointestinal conditions.
Physiological issues, specifically anxiety and sexual life, are that colostomy surgery can have a significant impact on patients’ emotional and sexual well-being.10 Anxiety can be related to fears about managing the colostomy bag, potential complications, and changes to body image and self-esteem.11 Sexual dysfunction can result from physical changes, such as pain or discomfort during intercourse, or psychological factors, such as anxiety or depression. A study found that 64% of colostomy patients experienced some form of sexual dysfunction, with the most common issue being loss of libido.12 Another study found that colostomy patients reported high levels of anxiety related to managing the colostomy bag, fear of odor or leakage, and concerns about engaging in social activities.13 This can have a significant impact on patients’ quality of life and may lead to social isolation or depression.
Social interaction is that patients with a colostomy face challenges in maintaining their social interactions due to stigmatization, discrimination, and embarrassment caused by their condition.14 The presence of a colostomy can impact social life, including issues with intimacy, isolation, and difficulty engaging in social activities.15 Stigma can also affect the quality of life of colostomy patients and contribute to anxiety and depression.5 Physical activity is an essential aspect of a healthy lifestyle, and individuals with colostomy face unique challenges in maintaining their physical activity level.16 The experience of living with a colostomy can limit physical activity, leading to a sedentary lifestyle, which can have detrimental effects on overall health and well-being.17
Colostomy patients may face significant financial hardship due to the cost of colostomy care supplies and related medical expenses, as well as potential loss of income and employment.18 The financial burden may lead to decreased access to necessary care and decreased quality of life.19
Therefore, by exploring the lived experiences of colostomy patients and their perspectives on the consequences of colostomies on various aspects of their lives, this study will provide original evidence to advance our understanding of this area. The study will shed light on the physical, psychological, social, and financial challenges faced by colostomy patients and the coping mechanisms they employ to manage these challenges. This knowledge will be valuable to healthcare professionals, support groups, and policymakers in providing appropriate support and care to colostomy patients. Ultimately, the study aims to explore the lived experience of colostomy patients as it improves the quality of life and overall well-being of colostomy patients in Addis Ababa.
Method
Study Design and Period
A phenomenological design was used to explore the lived experiences of individuals who had undergone surgical creation of a colostomy. The data collection period was from July 12, 2022, to August 13, 2022.
Study Setting
The research was conducted in Addis Ababa, Ethiopia’s capital city. Several hospitals, including Ras Desta, St. Paul Hospital Millennium Medical College, Tirunesh Beijing Memorial, Zewuditu Memorial, Yekatit 12, Minilik, and Black Lion Referral Hospital, were utilized. The study’s objectives and data collection procedures were explained in detail to potential participants, and the voluntary nature of participation and the protection of personal information and confidentiality were emphasized. Participants signed an informed consent form before data collection.
Participant Selection Strategy
A purposive sampling approach was used to access participants who were the most representative of the population under investigation. Participants were included if they were adults who had undergone a surgical creation of a colostomy, had lived with a colostomy for at least 3 months, and were hospitalized for reversal or visiting the surgical referral clinic during the study.
Data Collection Method
Semi-structured interviews were conducted as the primary method of data collection. The semi-structured interview guide included an introductory question, “Please describe your life experience from the moment you experienced the colostomy onward”, and several follow-up questions, such as “What did you feel when you first saw it, or after the first colostomy operation?” and “What were the positive and negative experiences you faced after the operation?” The venue and timing of the interviews were chosen by the participants, and all interviews were conducted in the outpatient department room for convenience. Data privacy and confidentiality were protected during the interview process, and a mobile phone recorder was used to record the interviews with the participants’ permission. The interviews lasted between 14 and 20 minutes and were transcribed verbatim. A reverse translation method was used to ensure the accuracy of the translation of the participant’s texts into English. A code was assigned to each interview to ensure the confidentiality of the participants.
Data Analysis
Descriptive analysis was used to examine the participants’ personal data. The voice-recorded interviews were analyzed using content analysis. The interviewer listened to the recordings, took notes, and categorized the information as usable data, and coded the writings. A second researcher who was not aware of the investigation reviewed the categorization. The arrangements were examined by a third senior researcher from Jima University to blind the analysis and ensure the study’s trustworthiness. The data was analyzed using phenomenological data analysis techniques, including identifying significant words and phrases, sorting themes, analyzing individual experiences, and creating sub-themes. Three basic themes were constructed, and generic categories were created using similar language. All participants were questioned to verify the correctness of the researchers’ interpretations of their expressions, and the convenience of the interpretations was substantiated.
To ensure the study’s credibility, data saturation was achieved when the seventh interview was completed, and no new qualitative data materially increased the knowledge of the problem. The study’s trustworthiness was confirmed through triangulation, peer review, and member checking (see Figure 1).
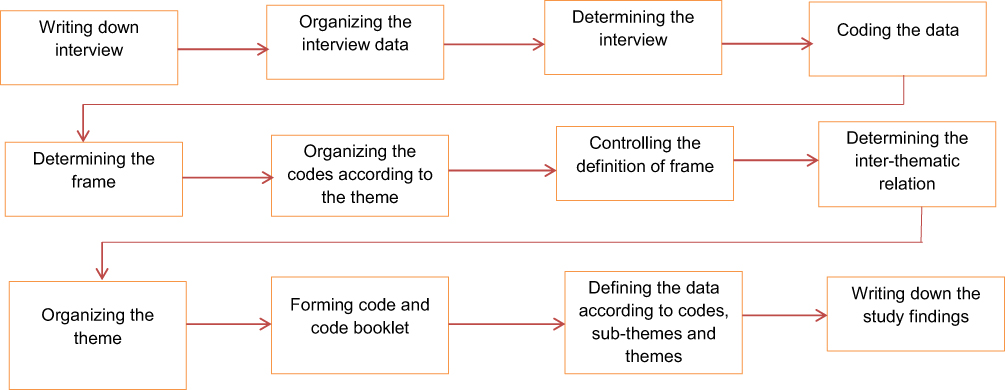 |
Figure 1 Data analysis algorithm. |
Ethical Clearance
This study was conducted in compliance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the St. Paul’s Hospital Millennium Medical College Institutional Review Board (IRB) (date: 08.07.2022, Ref no: 1-2-34/05) before data collection commenced. All participants were fully informed about the study’s purpose, scope, and procedures, and provided written informed consent prior to participation. The informed consent process included a statement that their responses would be anonymized and published in academic journals, and participants gave their written consent for this to occur. The importance of informed consent, confidentiality, and privacy was emphasized, and participants were assured that they could withdraw from the study at any time without affecting their medical care. Measures were taken to ensure the anonymity and confidentiality of participant data before, during, and after the interviews. Participants were also informed that their data would only be accessible to other researchers and used solely for research purposes. After data collection, the interview recordings were kept for a reasonable amount of time before being securely disposed of, and participants were given complete access to the study’s findings upon request.
Finding
Descriptive Results
The study included nine individuals who had undergone colostomy surgery and ranged in age from 27 to 55 years. All participants were married and had been living with a colostomy for a minimum of three months. Among the nine participants, three were female (see Table 1).
 |
Table 1 Descriptive character of the participants living with colostomy |
Themes
The research finding of this study identified four main themes that describe the lived experiences of individuals with colostomy. These themes were psychological effects, social life, physical activity, and economy (see Figure 2).
 |
Figure 2 Main themes for lived experience of individuals with colostomy. |
Theme One: Psychological Effects
Psychological effects, refers to the emotional and mental impact of living with a colostomy. Study participants reported experiencing a range of emotions, including anxiety, depression, and fear, related to their colostomy. They also reported feeling a loss of control and a sense of stigma related to their condition. This theme has six sub-categories based on interviews with individuals who had undergone colostomies for at least three months. The sub-categories are disbelief, shame or embarrassment, sleep disorders, difficulty in maintaining sexual life, accepting life with colostomy, and desperation.
Disbelief
Disbelief was reported as the individuals’ initial reaction to their colostomy. One participant stated,
That tragedy was too much for me to bear. When I opened my eyes, I couldn’t look at the colostomy site. I did not investigate what had happened. I did not even look at it. (5th case, m, 37 years old)
Shame or Embarrassment
Participants reported feeling uncomfortable due to their colostomy. In addition to the stench, gas, and physical appearance, the colostomy itself was a source of embarrassment for them. One participant stated
No one knows. (Pause) I will never bring it up again. Except for my family, I did not tell anyone. (2nd case, f, 47 years old)
Another participant stated
I avoid my friends in order to conceal it from them. I am humiliated. (4th case, m, 32 years old)
Despair
Individuals with colostomies said that they do not know what to do about colostomy care and the other strain that comes with it, and that they sometimes feel desperate. One participant stated
I was on the verge of developing minor mental disorder. I mean, I considered depression. (3rd case, m, 55 years old)
Another participant stated
What can I do if it explodes? Desperation. (4th case, m, 32 years old)
Sleep Disorders
Colostomy individuals claimed that they cannot sleep deeply and must wake up often due to their fear of the device loosening and making the bed unclean. One participant stated
I did not get any sleep. You are unable to sleep. It has so many bad aspects. (1st case, m, 27 years old)
Another participant stated
I suffer from a sleep condition. (2nd case, f, 47 years old)
Accepting Life with Colostomy
Despite having unfavorable feelings for a short while following surgery, many with colostomies have demonstrated that they have accepted the procedure. One participant stated
It had no effect at all. I am very upbeat. I still forget about it. (When I initially saw it) I was unaffected. I was not discouraged. (2nd case, f, 47 years old)
Another participant stated
Nothing changed in my life as a result of the operation, neither before nor after.I have no complaints. (5th case, m, 37 years old)
Theme Two: Physical Activity
Physical activity refers to the impact of colostomy on an individual’s physical ability to engage in activities. Participants in the study reported experiencing limitations in their physical activity due to their colostomy. This included difficulty with exercise and other physical activities, as well as limitations in sexual activity. Individuals with colostomies face difficulties in physical activity and daily activities following their surgery. The subthemes of this category include restrictions in physical activity and difficulty regulating physical activity.
Difficulty in Physical Activity
One of the subthemes in physical activity is difficulties in daily activities. Individuals reported difficulty lying down and standing up after colostomy surgery.
It was tough to lie down and stand up after the colostomy surgery. (5th case, 37 years old)
They also have problems traveling long distances on foot or using transportation.
For example I want to make long distance travel to visit relatives and or attending funeral ceremonies, but it is difficult for me to do. You should not use transport. (7th case, m, 41 years old)
Difficulty in Keeping Sexual Life
Another subtheme of physical activity is difficulties in sexual life. Individuals with colostomies reported having sexual issues and avoiding sexual relationships due to fear of the smell, gas, and sight of the colostomy.
We won’t be able to have sexual relations for around three months, I have not had any intercourse since my procedure. (3rd case, m, 55 years old)
There was no erection. My wife is not interested in sexual relations. Individuals with colostomies also told that they do not have any sexual relationships because they are concerned that their partners may harm their colostomy. “Our sex life has come to an end”. In truth, there is no intimacy. There will be no intimacy since it may smell or produce gas. My wife is also affected. Our intercourse frequency is quite low.
I believe my wife flees because she is terrified of harming the bag. (6th case, m, 31 years old)
Theme Three: Social Life
Social life, relates to the impact that having a colostomy has on an individual’s social interactions and relationships. Participants in the study reported feeling self-conscious and embarrassed about their colostomy, which led to social isolation and difficulty forming new relationships. Some participants also reported facing discrimination and prejudice from others.
Social Isolation/Stigma
Individuals with colostomies face social isolation and stigma due to the presence of the colostomy bag. They reported being unable to take part in social activities and gatherings because of the colostomy.
I am unable to join the community. This is my most significant issue. We used to meet on specific days, but I am no longer able to attend. (4th case, m, 32 years old)
Postoperatively, individuals also had to carry additional items with them, which made getting ready more time-consuming.
You have to carry items you do not need every day. You must bring some stuff with you when you travel. Acceptance of this condition may be simpler without these materials. (7th case, m, 41 years old)
Social Support
Family and friends play a crucial role in helping individuals cope with and care for their colostomy.
My husband was also present. ‘Oh! You can do and learn,’ he said. (2nd case, f, 47 years old)
My family was quite supportive. (1st case, m, 27 years old)
Participants stated that having strong social support was essential for their mental and physical well-being.
Morale is the most crucial aspect of my well-being; my wife has also been really supportive. Everything is done in collaboration. (4th case, m, 32 years old)
Difficulty in Religious Practice
Individuals with colostomies also reported difficulties in religious practices after their stoma operation. They were reluctant to go to the mosque/church because they were afraid that the bag could explode, and they had difficulty in performing prayer due to difficulty in bending and standing.
Church is troublesome. ‘I am not going to mosque anymore. I was used to go’. What church with this? How can you go with this? This explodes there. (8th case, f, 66 years old)
How it is now. I pray on a chair without bending down. (1st case, m, 82 years old)
Theme Four: Economy
Final theme, economy, relates to the financial impact of living with a colostomy. Participants in the study reported facing significant costs associated with the management of their colostomy, including the cost of medical supplies and expenses related to managing their condition. These costs often created financial strain and difficulty for study participants and their families. One patient in our study shared his experience with financial strain related to colostomy material shopping. The patient, a 32-year-old male, reported that his health insurance did not cover all of his colostomy supplies, and he had to purchase extra bags out of pocket. This resulted in additional expenses that he found difficult to manage with his retirement income, which he described as inadequate.
Discussion
First Encounter
The individual’s first interaction with a colostomy can be a challenging experience, and even pre-operative information cannot fully prepare them.1 According to the literature, individuals often feel sorry for them and view the colostomy as a disability when they first encounter it. They may also experience feelings of loss, hatred, embarrassment, and disgust.11 Our study found that even if individuals were informed about the colostomy before the surgery, they still experienced emotional shock upon waking up in the recovery area and seeing the colostomy. According to Persson and Hellström’s qualitative study,20 prior education cannot fully prepare individuals emotionally for their initial encounter with the colostomy. Other research has found that people with colostomies21 are embarrassed about them and try to conceal them.16 Individuals with colostomies often do not want to discuss them with others and only share them with their family due to shame.21 Some of them even refrain from informing their children because they are worried about the odor being offensive.22 Since colostomies can cause uncontrollable flatulence and excrement and appear plain from the outside, people may be hesitant to socialize and avoid taking public transportation.23 The humiliation they feel can be attributed to the issues caused by odor and gas, as well as their disfigured state.24
Earlier studies have found that individuals with colostomy may experience various negative emotions such as denial, fear, anger, resentment, nervousness, sadness, animosity, and desperation.25 Similarly, our research participants expressed feelings of desperation due to the burden of the colostomy. These emotions can be attributed to the new illness and the range of unpleasant emotions they experience. Previous literature has also reported that physical appearance, care burden, and other physical issues related to colostomy can cause fear in individuals, which is consistent with our findings.26
Furthermore, in addition to the fear and negative emotions, individuals with colostomy may face significant psychosocial difficulties due to a lack of support. Studies have demonstrated that psychological issues such as anxiety, social phobia, depression, severe depression, and even suicidal thoughts can occur following colostomy surgery, which is consistent with our findings.27 It is essential to note that while colostomy may improve survival rates, some individuals may choose death over living with a colostomy due to the complications it poses.20 Therefore, emotional support should be provided to individuals both before and after surgery to help them cope with the colostomy. It is crucial to identify and address psychological issues that may arise in the early stages.
Challenges
The challenges related to physical movement and sleeping difficulties following colostomy surgery are consistent with previous research. Our findings suggest that individuals curtail their physical activity due to discomfort and concerns about injuring the colostomy. They also have difficulty sleeping deeply and wake up frequently, hesitating to turn in bed, and even staying awake until morning out of fear of contaminating the bed. This lack of sleep can lead to a range of negative consequences, including an inability to maintain a healthy lifestyle.28 Moreover, our study participants avoid sleeping with their spouses due to the fear of the colostomy bag exploding, which can harm their relationships. This finding is similar to previous research and highlights the need for families to provide social support and encourage adherence to colostomy compliance instructions.29 Healthcare providers should inform patients about the physical activities they can and cannot perform after surgery to maintain their daily activities and improve their quality of life.30
Current study findings reveal that individuals with a colostomy face challenges related to their diet and nutrition due to the restriction of certain foods. This is consistent with previous research, as individuals have difficulty selecting meals and adjusting their diet to avoid gas, bag inflation, and explosion.31 This could be due to a lack of knowledge about suitable foods, and they should understand that their digestive system remains the same, and they need to avoid foods that cause them problems.
In a study conducted by Cooper,32 male subjects experienced erectile dysfunction and retrograde ejaculation, along with emotional difficulties related to their sexual health. Therefore, it is essential to refer male individuals to an urologist outpatient clinic following surgery to discuss their sexual difficulties. The study findings also indicate that individuals with a colostomy may consider themselves unclean and unpleasant, leading to sexual difficulties. This is because they worry about the appearance, smell, and loudness of the colostomy, along with anxiety about colostomy loosening and harm, which diminishes their desire for sexual activities. Similar to previous research, individuals believe that their body has changed after surgery and avoid sexual encounters, feeling that they are no longer attractive.33 Sexual dysfunction can lead to feelings of losing their manhood and negatively affect their relationship with their partners.34
Individuals with a colostomy may also face social isolation due to odors, leaks, gas, and shame. They may avoid social activities such as funerals, meeting with friends, visiting religious places, and making new acquaintances, resulting in social challenges. It is crucial to encourage individuals to participate in social activities, as giving up on these events leads to more serious problems.35 In addition to being unable to work, individuals with a colostomy may experience financial difficulties due to the cost of essential materials, leading to economic scarcity.36 Females in our study were stay-at-home spouses, while most males were farmers who did not face financial difficulties due to their work. However, two participants experienced financial difficulties due to the colostomy, impacting their family life negatively.
Coping
Current study confirms earlier research that individuals with Crohn’s disease or ulcerative colitis and cancer patients find it easier to accept a colostomy as it provides relief from their symptoms or disease. The acceptance of colostomy is also influenced by social and professional support, which helps individuals cope with negative sentiments.37 Strong family relationships and physical and psychosocial support are essential factors for accepting a colostomy and living with it as a bridge to life and survival.38 Proper education and clear communication before the surgery are crucial to minimizing negative feelings towards a colostomy.39 Our study shows that patients who perceive their body image as altered or feel insufficient are less likely to accept the colostomy. While defensive coping mechanisms can be helpful in the short term, patients must learn to live with a colostomy and develop technical abilities for colostomy care in the long term.29
Our study, like an earlier qualitative study, found that most individuals saw the colostomy as a lifeline and accepted it more easily, as they believed it was a way out of a worse condition. Positive coping strategies, such as imagining worst-case situations, were effective for patients who found comfort in them.40 However, it is important to evaluate whether patients have acclimated to their new state and perceive them as normal. Religious beliefs and principles played a role in coping for some participants, as they regarded the colostomy as coming from God and fate.5 Individuals who relied on their beliefs to cope had an easier time accepting the colostomy. It is crucial to consider religious beliefs and principles in helping patients adjust to life with a colostomy.10
Family members and friends play a significant role in colostomy care and support, as they provide both psychological and physical assistance.28 Patients may feel compelled to hide their colostomy or change their clothing in the dark if their social environment perceives it as an issue. Thus, informing family members about the colostomy before surgery and creating a supportive social environment are critical for patient acceptance.37 Health professionals play an essential role in the acceptance and adjustment to life with a colostomy.41 Adequate preoperative education, counseling, and postoperative support from doctors and nurses can reduce negative thoughts and worries about the surgery and enhance patient compliance.
Recommendation
It is recommended that individuals with a colostomy receive emotional support both before and after surgery to help them cope with the physical and psychological challenges that come with the condition. Healthcare providers should educate patients about physical activities they can perform after surgery to maintain their daily activities and improve their quality of life. In addition, patients should be provided with information on suitable foods to help them maintain a balanced diet while avoiding gas, bag inflation, and explosion.
It is also recommended that male patients receive referral to a urologist outpatient clinic following surgery to discuss sexual difficulties, and patients should be provided with information and support regarding sexual dysfunction to prevent negative impacts on their relationship with their partners. Patients should be encouraged to participate in social activities, which may help prevent social isolation, and healthcare providers should be aware of the potential financial difficulties that some patients may face and provide support where possible.
Overall, healthcare providers should recognize the physical, emotional, and social challenges associated with colostomies and provide patients with appropriate support to help them cope with the condition and improve their quality of life.
Limitation
One limitation of this study is the limited availability of colostomy clients after surgery, which raised questions about the maximum gender variation of the sample. Furthermore, the study did not distinguish between participants who had a colostomy due to colorectal cancer and those who had it due to other medical conditions. As a result, the lived experience of having a colostomy in the context of colorectal cancer was not explored separately.
Conclusion
The study shows that individuals with colostomy face physical, psychological, and social challenges. Despite pre-operative education, individuals often experience negative emotions such as loss, hatred, embarrassment, disgust, and desperation. They may face psychosocial difficulties due to a lack of support, leading to anxiety, social phobia, depression, severe depression, and even suicidal thoughts. Physical movement, sleeping, and dietary restrictions also pose challenges for these individuals. Sexual difficulties, social isolation, and financial issues are additional challenges. Coping with colostomy requires emotional support, education, and proper communication with healthcare providers. Encouraging individuals to participate in social activities, identifying and addressing psychological issues, and providing information on suitable foods and physical activities are essential. The findings highlight the need for healthcare providers to understand the challenges faced by individuals with colostomy and develops comprehensive care plans to support them.
Acknowledgment
I would like to express my gratitude to the Saint Paul’s Hospital millennium medical college, school of public health department, and the management for granting permission for this study. Additionally, I would like to extend my sincere appreciation to Dr. Luli Baissa and Fistum Taye, my relatives, for their invaluable contributions to the data collection process.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Souwer ETD, Oerlemans S, van de Poll-Franse LV, et al. The impact of colorectal surgery on health-related quality of life in older functionally dependent patients with cancer – a longitudinal follow-up study. J Geriatr Oncol. 2019;10(5):724–732. doi:10.1016/j.jgo.2019.04.013
2. Nugent KP, Daniels P, Stewart B, Patankar R, Johnson CD. Quality of life in stoma patients. Dis Colon Rectum. 1999;42(12):1569–1574. doi:10.1007/BF02236209
3. Slankamenac K, Slankamenac M, Schlegel A, et al. Impact of postoperative complications on readmission and long-term survival in patients following surgery for colorectal cancer. Int J Colorectal Dis. 2017;32(6):805–811. doi:10.1007/s00384-017-2811-y
4. Arndt V, Merx H, Stegmaier C, Ziegler H, Brenner H. Quality of life in patients with colorectal cancer 1 year after diagnosis compared with the general population: a population-based study. J Clin Oncol. 2004;22(23):4777–4784. doi:10.1200/JCO.2004.02.018
5. Dabirian A, Yaghmaei F, Rassouli M, Tafreshi MZ. Quality of life in ostomy patients: a qualitative study. Patient Prefer Adherence. 2010;5:1–5. doi:10.2147/PPA.S14508
6. Vilz TO, Websky M, Kalff JC, Stoffels B. Intestinal stomata. Coloproctology. 2020;42(6):509–519. doi:10.1007/s00053-020-00503-3
7. Matsunaga T, Miyake T, Ueki T, et al. 「緩和的造設による造設による人工肛門造設がQOLに及ぼす短期および長期的影響」松永知之、三宅貴生、植木達也 ほか。がんと化学療法 [Short- and long-term effects of palliative stoma creation on quality of life]. Gan To Kagaku Ryoho. 2022;49(13):1396–1398. Japanese.
8. Mensah ABB, Yeboah V, Amaniampong E-M, et al. Experiences and coping strategies of colostomy patients in Ghana: a Phenomenological study. 2022:1–18.
9. Pittman J, Rawl SM, Schmidt CM, et al. Demographic and clinical factors related to ostomy complications and quality of life in veterans with an ostomy. J Wound Ostomy Cont Nurs. 2008;35(5):493–503. doi:10.1097/01.WON.0000335961.68113.cb
10. Silva NM, Dos Santos MA, Rosado SR, Galvão CM, Sonobe HM. Psychological aspects of patients with intestinal stoma: integrative review. Rev Lat Am Enfermagem. 2017;25:54.
11. Kimura CA, Guilhem DB, Kamada I, Abreu BS, Modesto KR, Gonçalves JR. Life quality for ostomized patients: a perspective in the health and nursing care process. J Nurs Educ Pract. 2016;7(4):18.
12. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
13. Mahjoubi B, Mirzaei R, Azizi R, Jafarinia M, Zahedi-Shoolami L, Montazeri A. A cross-sectional survey of quality of life in colostomates: a report from Iran. Health Qual Life Outcomes. 2012;10:1–6. doi:10.1186/1477-7525-10-1
14. Ernst J, Mehnert A, Dietz A, Hornemann B, Esser P. Perceived stigmatization and its impact on quality of life - results from a large register-based study including breast, colon, prostate and lung cancer patients. BMC Cancer. 2017;17(1):1–8. doi:10.1186/s12885-017-3742-2
15. Mota MS, Gomes GC, Petuco VM. Repercussions in the living process of people with stomas. Texto e Context Enferm. 2016;25(1):1–8.
16. Nakagawa H, Sasai H, Tanaka K. Physical fitness levels among colon cancer survivors with a stoma: a preliminary study. Medicine. 2020;56(11):1–9.
17. Pittman J, Colwell J, Mulekar MS. Ostomy complications and quality of life of ostomy support belt/garment wearers: a web-based survey. J Wound Ostomy Cont Nurs. 2022;49(1):60–68. doi:10.1097/WON.0000000000000843
18. Azzani M, Roslani AC, Su TT. Financial burden of colorectal cancer treatment among patients and their families in a middle-income country. Support Care Cancer. 2016;24(10):4423–4432. doi:10.1007/s00520-016-3283-2
19. Jafari MD, Jafari F, Halabi WJ, et al. Colorectal cancer resections in the aging US population: a trend toward decreasing rates and improved outcomes. JAMA Surg. 2014;149(6):557–564. doi:10.1001/jamasurg.2013.4930
20. Persson E. Experiences of Swedish men and women 6 to 12 weeks after ostomy surgery. J WOCN. 2002;29(2):103–108.
21. Petersén C, Carlsson E. Life with a stoma—coping with daily life: experiences from focus group interviews. J Clin Nurs. 2021;30(15–16):2309–2319. doi:10.1111/jocn.15769
22. Villa G, Mannarini M, Della Giovanna G, Marzo E, Manara DF, Vellone E. A literature review about self-care on ostomy patients and their caregivers. Int J Urol Nurs. 2019;13(2):75–80. doi:10.1111/ijun.12182
23. Ayaz-Alkaya S. Overview of psychosocial problems in individuals with stoma: a review of literature. Int Wound J. 2019;16(1):243–249. doi:10.1111/iwj.13018
24. He LJ, Zheng MC, Yuet Wong FK, Ying J, Zhang JE. Immediate postoperative experiences before discharge among patients with rectal cancer and a permanent colostomy: a qualitative study. Eur J Oncol Nurs. 2021;51:101911. doi:10.1016/j.ejon.2021.101911
25. Wennman I, Ringheim A, Wijk H. “We are here for you all the way”-patients’ and relatives’ experiences of receiving advanced home care. Am J Hospice Palliative Med. 2020;37:669–674. doi:10.1177/1049909120905259
26. Lim CYS, Laidsaar-Powell RC, Young JM, Kao SCH, Zhang Y, Butow P. Colorectal cancer survivorship: a systematic review and thematic synthesis of qualitative research. Eur J Cancer Care. 2021;30(4):e13421. doi:10.1111/ecc.13421
27. Choudhary M, Kaur H. Experiences of living with intestinal ostomy: a qualitative meta-synthesis. Indian J Palliat Care. 2020;26(4):421. doi:10.4103/IJPC.IJPC_21_20
28. Yuan JM, Zhang JE, Zheng MC, Bu XQ. Stigma and its influencing factors among Chinese patients with stoma. Psychooncology. 2018;27(6):1565–1571. doi:10.1002/pon.4695
29. Tiainen J, Matikainen M. Health-related quality of life after Ileal J-Pouch?Anal anastomosis for ulcerative colitis: long-term results. Scand J Gastroenterol. 2009;34(6):601–605. doi:10.1080/003655299750026065
30. Mirelman D, Corman ML, Veidenheimer MC, Coller JA. Colostomies-indications and contraindications: Lahey clinic experience, 1963–1974. Dis Colon Rectum. 1978;21(3):172–176. doi:10.1007/BF02586563
31. Shaffy KS, Das K, Gupta R. Physical, nutritional and sexual problems experienced by the patients with colostomy/ileostomy: a qualitative study. Nurs Midwifery Res. 2012. doi:10.1177/0974150X20120304
32. Cooper AJ. Couples with sexual problems. Can J Psychiatry. 1985;30(6):461–462. doi:10.1177/070674378503000629
33. Reis H, Sprecher S. Sex in established relationships. Encycl Hum Relationships. 2013;2013:265.
34. Tustin RD. Psychological treatment of sexual problems. Aust N Z J Criminol. 1976;9(4):221–226. doi:10.1177/000486587600900404
35. Stein Backes D, Terezinha M, Backes S, Erdmann AL, Büscher A. Coping strategies of people with pancreatic cancer view project qualidade de vida view project ORIGINAL RESEARCH feelings and expectations of permanent colostomy patients. J Nurs Educ Pract. 2012;2(3). doi:10.5430/jnep.v2n3p9
36. Bemah Boamah Mensah A, Yeboah V, Amaniampong E-M, et al. Experiences and coping strategies of colostomy patients in Ghana: a Phenomenological study. 2022. doi:10.21203/rs.3.rs-1614762/v1
37. Simmons KL. A view from here: psychosocial issues in colostomy care. J Wound Ostomy Cont Nurs. 2014;41(1):55–59. doi:10.1097/01.WON.0000438015.98357.53
38. Britt TW, Greene-Shortridge TM, Brink S, et al. Perceived stigma and barriers to care for psychological treatment: implications for reactions to stressors in different contexts. J Soc Clin Psychol. 2008;27(4):317–335. DOI:10.1521/jscp.2008.27.4.317
39. Gritz ER, Fingeret MC, Vidrine DJ, Lazev AB, Mehta NV, Reece GP. Successes and failures of the teachable moment. Cancer. 2006;106(1):17–27. doi:10.1002/cncr.21598
40. Popek S, Grant M, Gemmill R, Wendel CS, Mohler MJ, Rawl SM. Overcoming challenges: life with an ostomy. Am J Surg. 2010;200(5):640–645. doi:10.1016/j.amjsurg.2010.07.009
41. Cengiz B, Bahar Z. Perceived barriers and home care needs when adapting to a fecal ostomy: a phenomenological study. J Wound Ostomy Cont Nurs. 2017;44(1):63–68. doi:10.1097/WON.0000000000000271
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.