Back to Journals » Clinical Ophthalmology » Volume 20
Collaborative Diagnostic Pathways for Unilateral Orbital Disease: A Clinicopathological Series
Authors Romeo MA ![]() , Gaeta A
, Gaeta A ![]() , Ferraro S, Ottonelli G
, Ferraro S, Ottonelli G ![]() , Manara SAAM, Giannitto C, Lucia AMA, Scorcia V, Giannaccare G, Di Maria A
, Manara SAAM, Giannitto C, Lucia AMA, Scorcia V, Giannaccare G, Di Maria A ![]()
Received 27 October 2025
Accepted for publication 11 February 2026
Published 5 June 2026 Volume 2026:20 576995
DOI https://doi.org/10.2147/OPTH.S576995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Maria Angela Romeo,1 Alessandro Gaeta,2 Silvia Ferraro,3 Giovanni Ottonelli,4 Sofia Ada Assunta Maria Manara,5 Caterina Giannitto,6,7 Ada Maria Antonella Lucia,5 Vincenzo Scorcia,1 Giuseppe Giannaccare,8 Alessandra Di Maria4,7
1Department of Ophthalmology, University Magna Graecia of Catanzaro, Catanzaro, Italy; 2Department of Internal Medicine and Medical Specialties (DIMI), University of Genoa, Genoa, Italy; 3Department of Ophthalmology, University of Catania, Catania, Italy; 4Department of Ophthalmology, IRCCS Humanitas Research Hospital, Rozzano, Milan, 20089, Italy; 5Pathology Unit, IRCCS Humanitas Research Hospital, Milan, Italy; 6Radiology Unit, IRCCS Humanitas Research Hospital, Milan, Italy; 7Department of Biomedical Sciences, Humanitas University, Milan, Italy; 8Eye Clinic, Department of Surgical Sciences, University of Cagliari, Cagliari, Italy
Correspondence: Maria Angela Romeo, Email [email protected]
Purpose: To report a retrospective tertiary-center series of unilateral orbital lesions and to illustrate a structured, experience-based multidisciplinary workflow integrating clinical, radiologic, and histopathologic data to support differential diagnosis and management in real-world practice.
Patients and Methods: This retrospective descriptive case-series included 18 patients with biopsy-confirmed unilateral orbital lesions evaluated between January 2021 and March 2025 at the Oculoplastic and Orbital Surgery Unit, Humanitas Research Hospital, Milan. Demographic, clinical, imaging, and histopathologic data were analyzed. Imaging included computed tomography (CT), magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI), and functional techniques such as MRA, PET/CT when indicated. Histopathology incorporated immunohistochemistry (IHC) and proliferative indices (Ki-67). Outcomes included final diagnosis, treatment, and early recurrence.
Results: 18 patients were included: dermoid cysts (n = 3), vascular malformations (n = 6), neurofibroma (n = 1), idiopathic orbital inflammation (n = 2), meningioma (n = 1), and epithelial malignancies (adenoid cystic carcinoma, basal cell carcinoma, squamous cell carcinoma, mucinous carcinoma, Merkel cell carcinoma; n = 5). Characteristic MRI and IHC patterns enabled accurate subclassification and guided informed-individualized management decisions, ranging from observation or image-guided sclerotherapy to complete surgical excision or multidisciplinary oncologic therapy. No recurrence occurred among benign lesions. Malignant epithelial tumors required adjuvant radiotherapy or systemic therapy according to histologic subtype and TNM stage.
Conclusion: A systematic, multidisciplinary approach integrating cross-sectional imaging and histopathologic assessment underpins effective diagnostic and therapeutic decision-making in unilateral orbital disease. The proposed workflow, derived from institutional practice, offers an illustrative and reproducible framework for clinical reasoning and therapeutic decision-making based on real case scenarios. Its adaptability lies in the use of structured clinical–radiologic algorithms, which may help optimize individualized management, facilitate timely referral, and reduce unnecessary invasive procedures, particularly within tertiary referral settings.
Plain Language Summary: Orbital disorders are uncommon conditions that can manifest with swelling, displacement of the eye, or visual changes. Because similar symptoms may result from very different diseases, ranging from benign cysts or vascular malformations to inflammatory or malignant tumors, reaching the correct diagnosis can be challenging and often requires input from different medical specialists.
In this study, patients with an orbital lesion affecting only one eye were evaluated through a structured, step-by-step diagnostic process. Ophthalmologists first assessed the clinical presentation, radiologists interpreted targeted CT and MRI features, and pathologists analyzed tissue samples using microscopic and immunohistochemical techniques. The team then discussed each case together to integrate these findings, refine the diagnosis, and agree on the most appropriate management strategy for each patient.
The multidisciplinary team developed individualized treatment plans collaboratively, balancing the need for tumor control, vision preservation, and cosmetic outcome. This shared decision-making approach helped distinguish lesions suitable for careful observation or minimally invasive treatment from those requiring surgery or additional oncologic therapy.
Overall, this experience shows that close collaboration between specialists improves diagnostic accuracy, supports safer and more personalized care, and helps guide evidence-based treatment choices for people with unilateral orbital disease.
Keywords: diagnostic algorithm, multidisciplinary management, ophthalmic oncology, orbital disease, orbital MRI, orbital PET/CT, orbital surgery
Introduction
Orbital lesions comprise a broad spectrum of congenital malformations, inflammatory disorders, vascular anomalies, and benign or malignant neoplasms. Among the parameters guiding initial diagnostic assessment, laterality represents a clinically relevant discriminator. Bilateral orbital involvement often reflects systemic or inflammatory processes, whereas unilateral lesions are more frequently encountered in tertiary referral settings and may warrant targeted imaging and, when indicated, biopsy for histopathological confirmation.1,2 (Table 1)
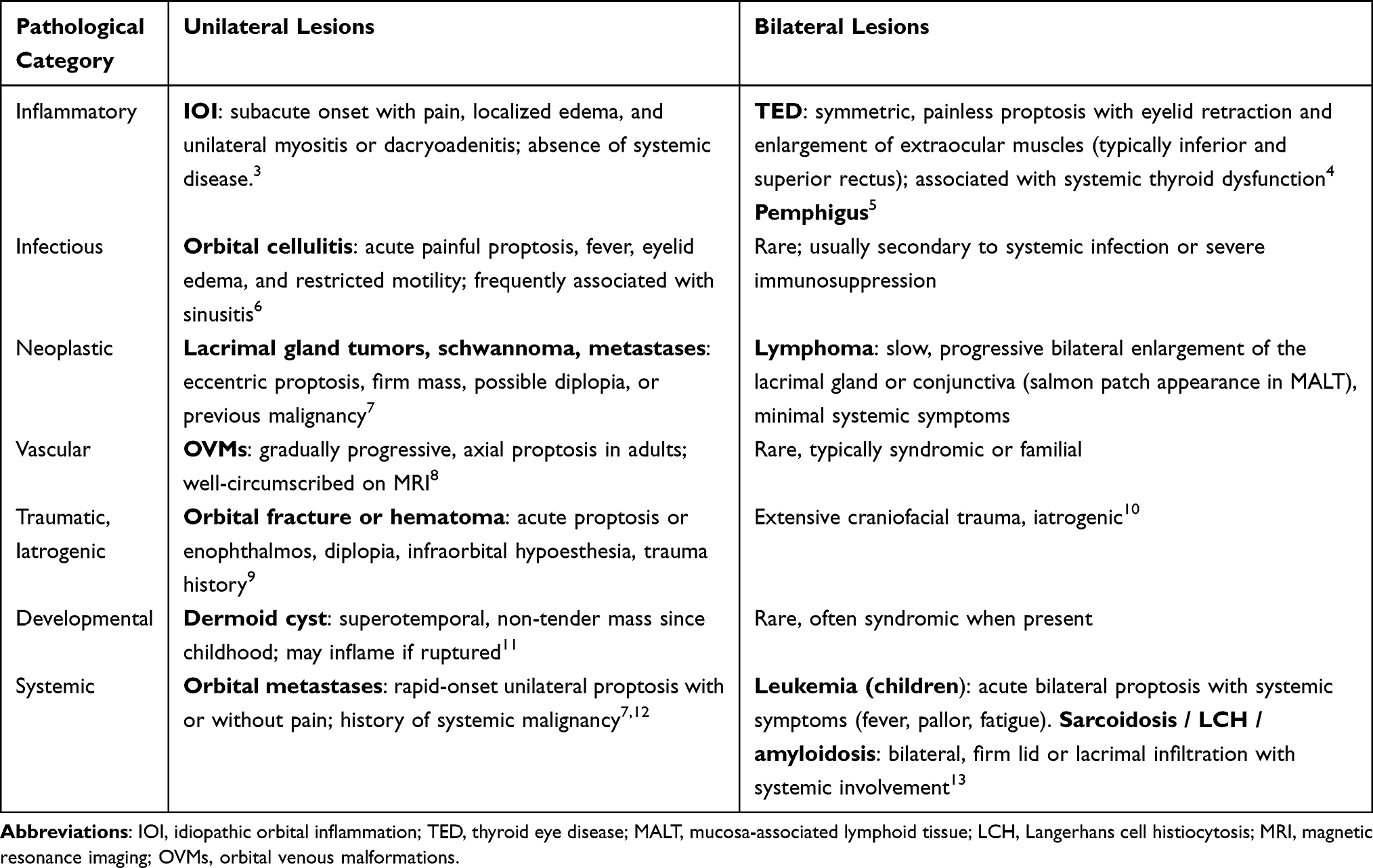 |
Table 1 Laterality Helps Separate Focal Processes (Often Unilateral) from Systemic or Infiltrative Disorders (Commonly Bilateral) |
A structured evaluation based on symptom chronology, anatomical compartmentalization, and systemic associations allows early refinement of the differential diagnosis and may reduce unnecessary invasive procedures (Table 2 and Table 3)
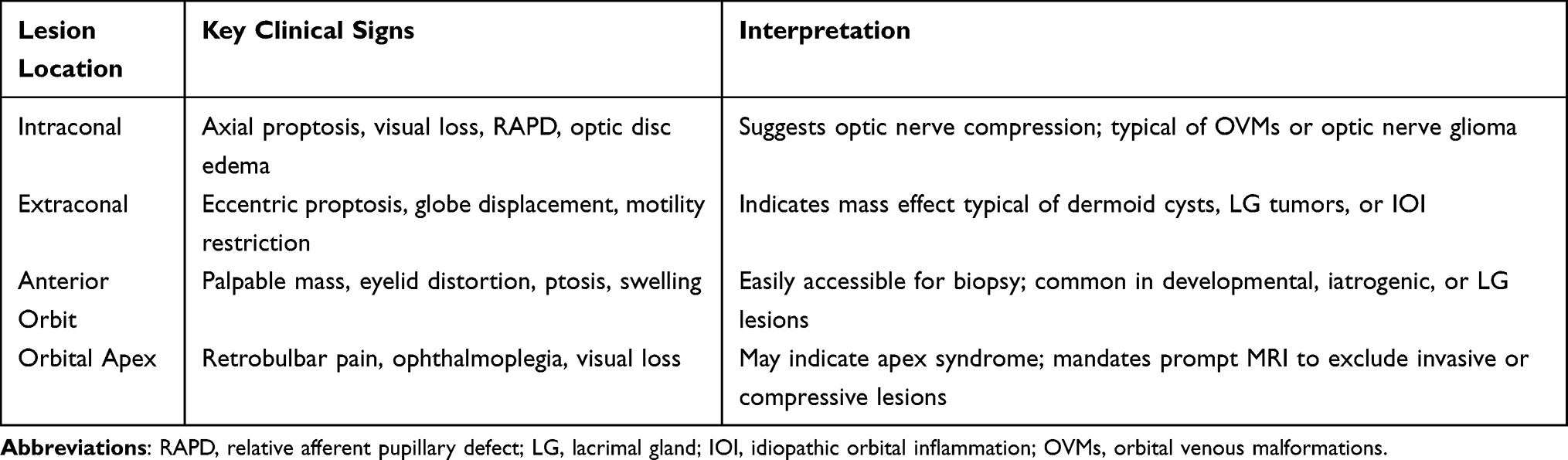 |
Table 2 Lesion Localization Based on Clinical Signs |
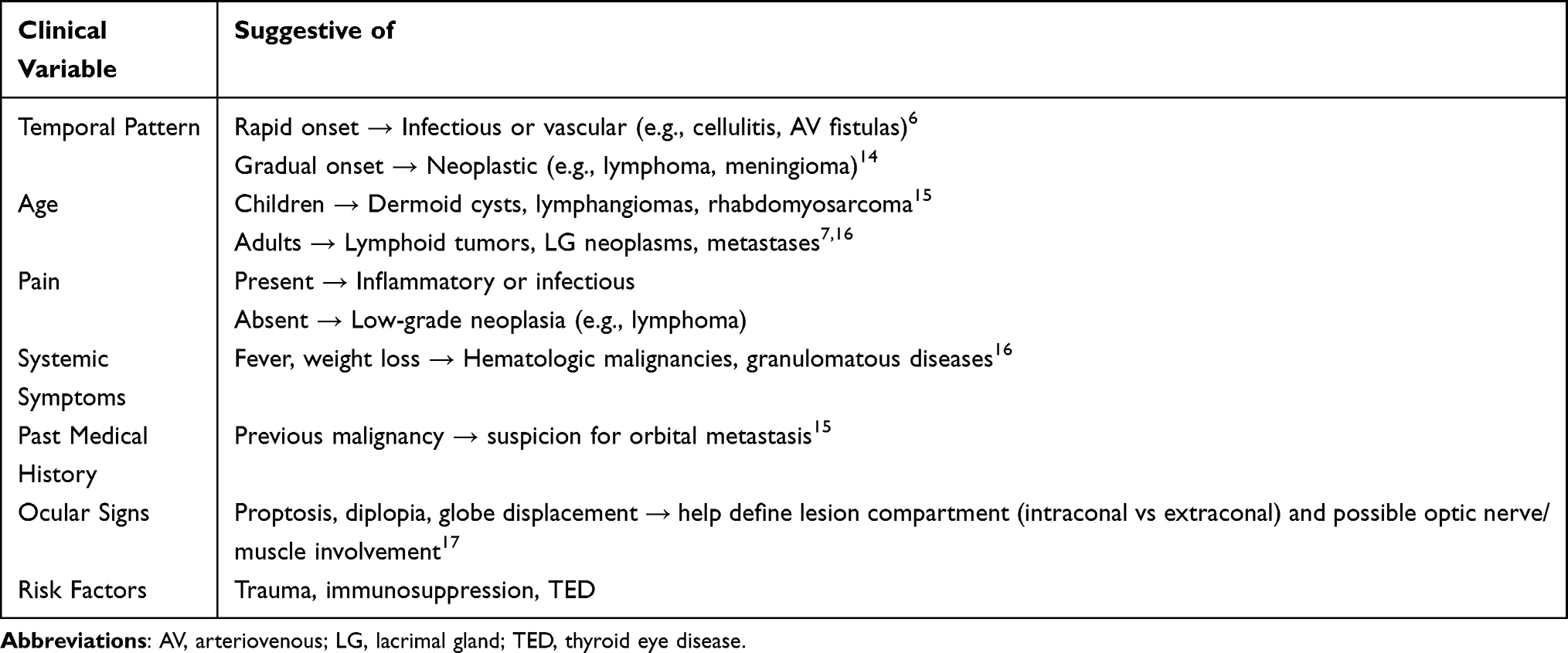 |
Table 3 Targeted History Narrows the Differential Before Imaging |
Imaging underpins work-up and surgical planning: ultrasound for anterior and cystic lesions, CT for osseous changes or calcifications, and contrast-enhanced MRI for soft-tissue or apical involvement. Functional modalities such as MRA or PET/CT further assist in delineating vascular or systemic extension.18 In resource-limited settings, ultrasound and CT may represent first-line screening tools, with MRI reserved for selected cases requiring advanced soft-tissue characterization. (Table 4)
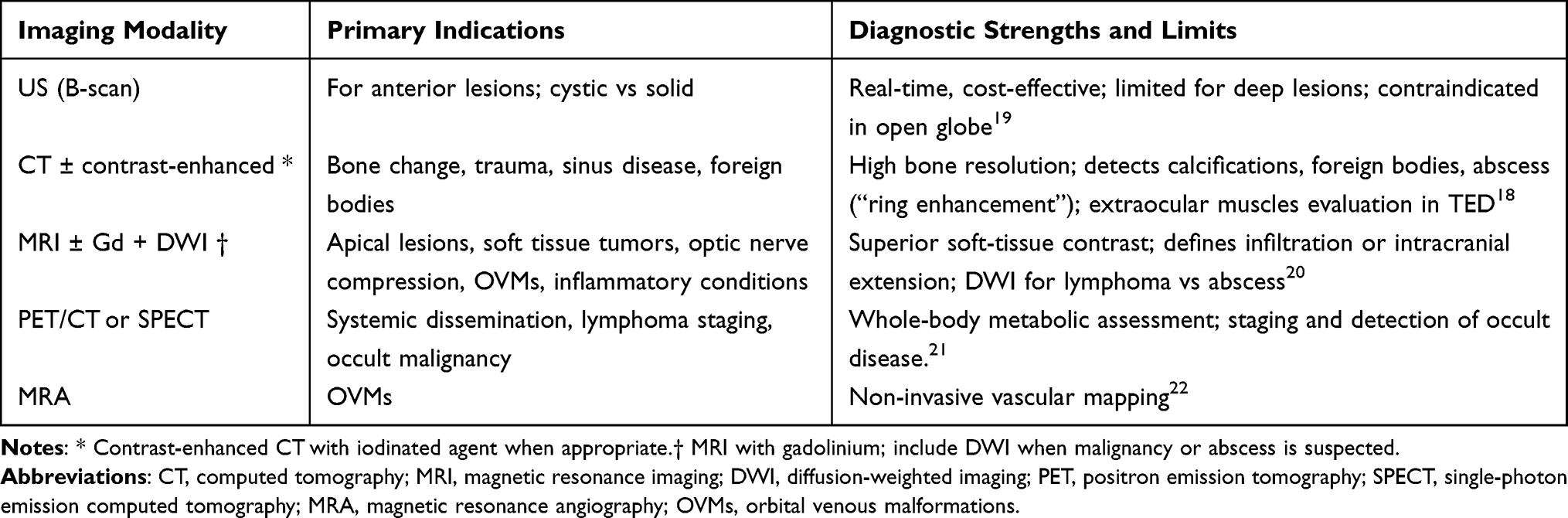 |
Table 4 Choose Modality by Clinical Question and Anatomic Target |
Definitive classification relies on histopathology with targeted immunohistochemistry (IHC), including proliferative indices (e.g., Ki-67). (Table 5).
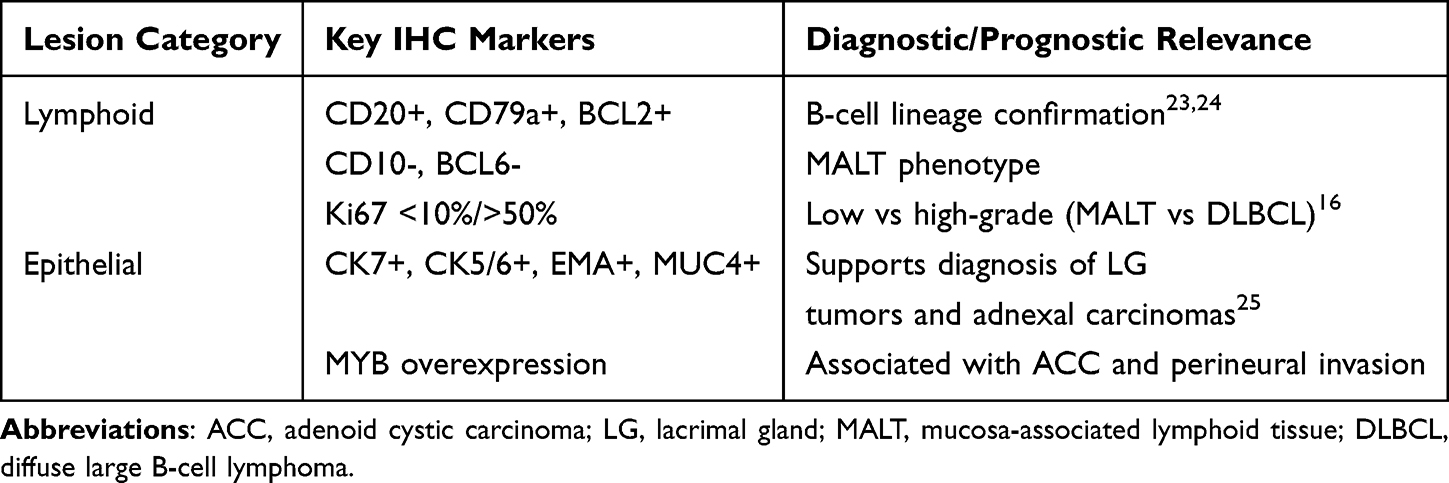 |
Table 5 Key IHC Markers Aid in the Classification of Orbital Lymphoid and Epithelial Tumors |
Despite technological advances, integrated analyses correlating laterality, compartmental anatomy, imaging characteristics, and immunophenotype in unilateral orbital disease remain limited with most existing diagnostic algorithms addressing individual modalities rather than a coordinated multidisciplinary workflow derived from real-world tertiary-center practice.This study presents a tertiary-center cohort of unilateral orbital lesions, aiming to (i) define clinicopathologic patterns that facilitate timely differential diagnosis, (ii) outline a didactic framework for clinical decision-making, and (iii) promote a multidisciplinary, evidence-based approach to orbital pathology.
Materials and Methods
Design and Setting
Retrospective descriptive case series at the Oculoplastic and Orbital Surgery Unit, Humanitas Research Hospital (Milan, Italy), a tertiary referral center for orbital disease.
Time Frame
January 2021–March 2025.
Eligibility
Inclusion: unilateral orbital lesion with diagnosis confirmed by excisional or incisional biopsy. Exclusion: contralateral orbital involvement at presentation or follow-up, or incomplete medical records.
Data Items
Demographics; laterality; symptom onset (acute < 1 mo, subacute 1–6 mo, insidious > 6 mo); pain; history of trauma/surgery, autoimmune or oncologic disease, prior radiotherapy; key signs (proptosis, palpable mass, ptosis, diplopia, visual changes); imaging (MRI/CT); procedure type; histology/IHC; treatment; outcomes. Supplementary Materials include additional clinical and histopathological images supporting the findings of this study. Additional clinical and histopathological images are available from the corresponding author upon reasonable request.
Imaging
CT for bony changes and calcifications; MRI (T1/T2, fat-suppressed, DWI/ADC; gadolinium when not contraindicated) for soft-tissue characterization and orbital apex assessment; MRA or PET/CT selectively for vascular mapping or systemic staging. High-risk lesions underwent radiologic surveillance with MRI at 3, 6, and 12 months, according to institutional practice.
Surgical Strategy
Excisional biopsy for anterior, well-circumscribed lesions; incisional biopsy for deep or infiltrative lesions; observation for high-risk cases with benign imaging profile, under structured follow-up.
Pathology
H&E plus targeted IHC panel (CD20/CD3, CK7/CK5/6/EMA/MUC4, S100/SOX10, D2-40/CD31, Ki-67). Frozen section used selectively intraoperatively.
Outcomes and Ethics
Primary outcome: final diagnosis; secondary: management pathway, complications, early recurrence. Descriptive statistics using Excel version 16.102 (25101223) applied. Study approved by the Humanitas Research Hospital Ethics Committee (No. 4967/2025) and conducted per the Declaration of Helsinki. Written consent obtained for publication. Tumor staging followed AJCC/UICC TNM (8th ed).
Results
Dermoid Cysts of the Orbit
Three male patients (mean age 26 years, range 21–29) presented with orbital dermoid cysts located at the frontozygomatic suture. One lesion was congenital and asymptomatic, whereas two manifested acute inflammation following cyst rupture. All underwent complete excision through anterior orbitotomy. No recurrence or postoperative complications were observed during follow-up. Demographic, radiologic, and histopathologic data are detailed in Table 6.
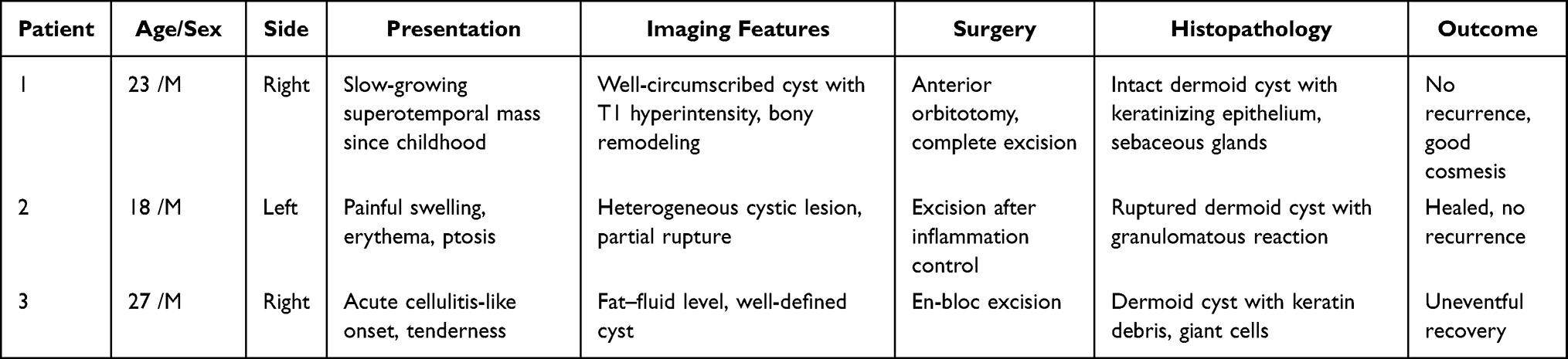 |
Table 6 Summary of Clinical, Radiologic, Surgical, and Histopathologic Findings in Three Patients with Orbital Dermoid Cysts |
Vascular Malformations of the Orbit
Six patients (4 women, 2 men; mean age 56 years, range 52–61) had unilateral extraconal vascular malformations, mainly in the superior or medial compartment. Lesions included three venous malformations (cavernous type), two mixed venous–lymphatic malformations, and one superficial venous lesion treated with image-guided sclerotherapy. Management included excision (n = 3), biopsy + observation (n = 2), sclerotherapy (n = 1).
All patients remained clinically stable with no recurrence or complications during a median follow-up of 18 months (range 6–30). A comprehensive summary is presented in Table 7.
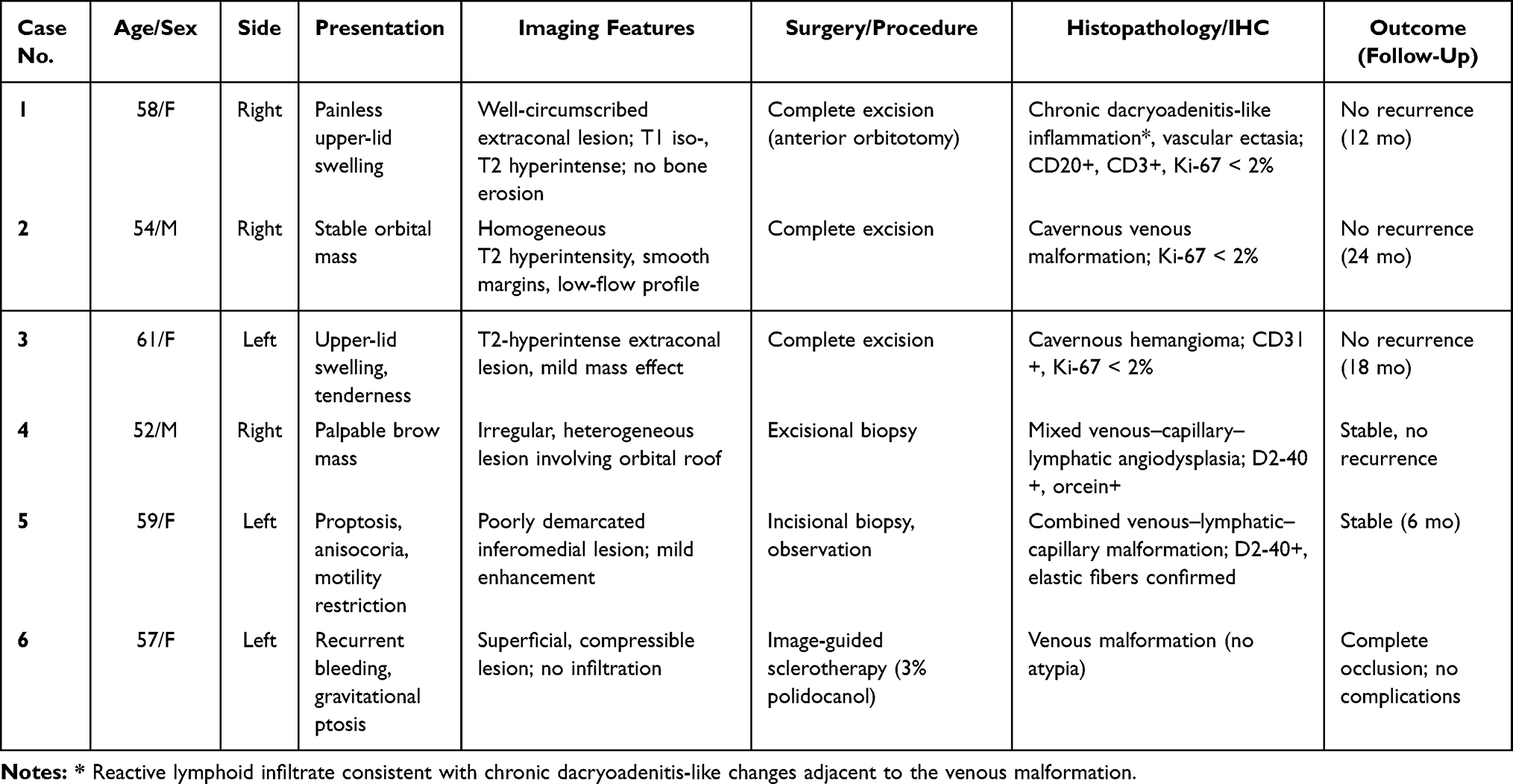 |
Table 7 Summary of Clinical, Radiologic, Surgical, and Histopathologic Findings in Three Patients with Orbital Vascular Malformations |
Solitary Orbital Neurofibroma
A 61-year-old woman presented with progressive upper-eyelid fullness and ptosis following previous orbital surgery. Examination revealed a firm, painless, superomedial mass without features of neurofibromatosis type 1. Complete removal via anterior orbitotomy was achieved while preserving levator and neurovascular structures. Histopathologic analysis confirmed a benign neurofibroma (SOX10/S-100+, Ki-67 < 1%). Recovery was uneventful; no recurrence occurred on follow-up.
Idiopathic Orbital Inflammation
Two patients (one woman aged 58 years, one man aged 71 years) were diagnosed with idiopathic orbital inflammation, one acute eosinophil-rich and one chronic fibrosing subtype, both involving the left orbit.
Acute IOI
The acute case presented with a five-year history of intermittent pain and swelling, initially treated as cellulitis with partial steroid response. The disease culminated in sudden visual decline (VA 0.3), complete ptosis, diplopia, conjunctival chemosis and episcleral caput medusae vessel dilation. MRI demonstrated diffuse T2-hyperintense inflammation of orbital fat and extraocular muscles, extending to the optic nerve sheath without bone erosion. Histopathology revealed eosinophil-rich infiltration and stromal edema without granulomas or vasculitis. Granulomatosis with polyangiitis, lymphoma, and IgG4-related disease were excluded. Intravenous hydrocortisone (300 mg/day), preferred over high-dose methylprednisolone pulse therapy in view of the patient’s comorbidity profile, resulted in complete visual and motility recovery within days.
Chronic IOI
The chronic case developed slowly progressive proptosis and diplopia over two years. Initial corticosteroid therapy was discontinued due to iatrogenic hyperglycemia. MRI showed a 23×15 mm T1/T2-hypointense inferomedial mass with restricted diffusion (ADC < 1.0 × 10−3 mm2/s) and mild bone remodelling. Histopathology demonstrated spindle-cell proliferation with lymphohistiocytic infiltrates (CD3⁺, CD20⁺, CD163⁺), Ki-67 < 5%, and MAP2K1 p.F53L mutation. Surgical debulking improved symptoms and achieved long-term stability at 24 months.
Orbital Meningioma
A 44-year-old woman presented with progressive, painless proptosis, anisocoria, RAPD, and complete motility restriction. Non-contrast CT revealed marked remodelling of the lateral orbital wall and sphenoid wing with mixed osteolytic–sclerotic pattern and an 8×27 × 24 mm extraconal mass compressing the optic nerve. Subtotal excision with bone decompression was performed via anterior orbitotomy. Histopathology confirmed a meningothelial meningioma (WHO grade I) with syncytial architecture, psammoma bodies, dense fibrosis, and immunopositivity for EMA, vimentin, and progesterone receptor (80%), Ki-67 < 1%. Postoperative recovery was uneventful, and both vision and motility remained stable at 18 months; no adjuvant radiotherapy was required.
Epithelial Tumors Involving the Orbit
Five patients (3 women, 2 men; median age 63 years, range 44–73) presented with malignant epithelial tumors extending into the orbit: adenoid cystic carcinoma (ACC) of the lacrimal gland (n = 1), basal/basosquamous carcinoma (BCC/BSC) of the eyelid (n = 2), primary mucinous carcinoma (MUC) of the eyelid (n = 1), and Merkel cell carcinoma (MCC) (n = 1). All lesions were right-sided. Routes of spread were direct or perineural in 4 of 5 cases. Table 8 summarizes tumor sites, imaging, treatment, staging, and early outcomes.
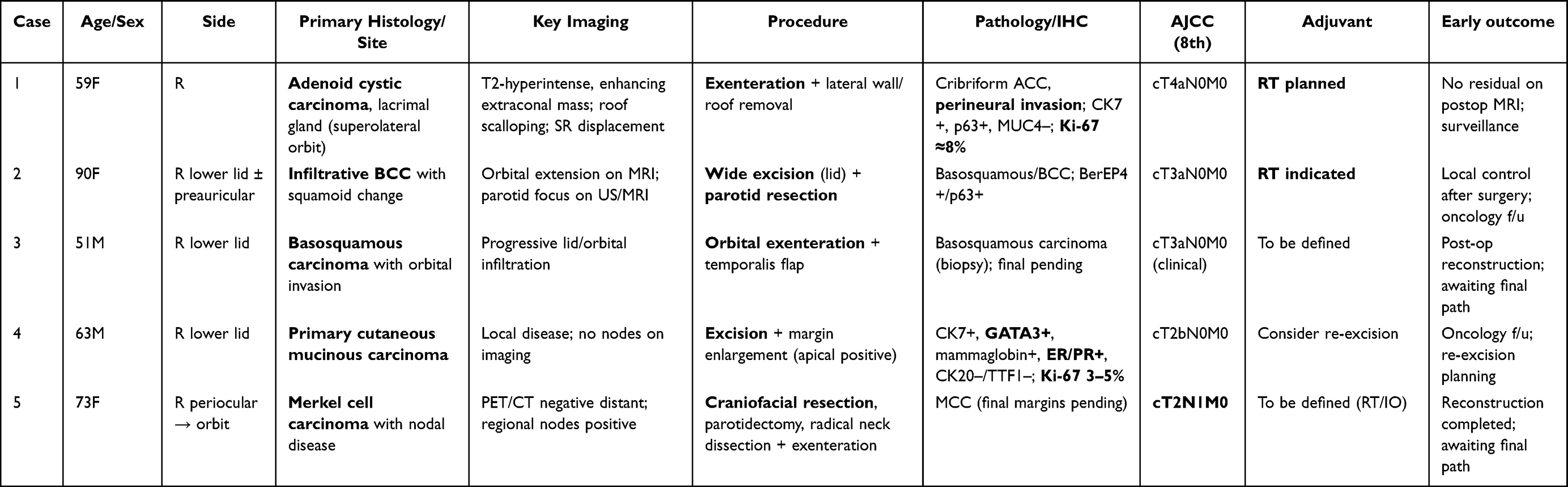 |
Table 8 Summary of Clinical, Radiologic, Surgical, and Histopathologic Findings in Patient with Malignant Epithelial Tumors |
Management included exenteration with or without craniofacial resection (n = 3; Cases 1, 3, 5), wide local excision with or without radiotherapy (n = 1; Case 4), and planned margin re-excision (n = 1). Histopathology confirmed ACC with perineural invasion, basosquamous/BCC variants (Case 2–3), mucinous carcinoma with CK7⁺/GATA3⁺/ER⁺/PR⁺ profile (Case 4), and MCC with regional nodal disease (Case 5). No distant metastases were detected at staging; local control is pending in the actively treated cases. Details of presentation, imaging, treatment, and staging are summarised in Table 8.
Discussion
Dermoid Cysts of the Orbit
Dermoid cysts represent the most common orbital tumors in children, accounting for up to 46% of pediatric orbital neoplasms and 3–9% of all orbital masses.26,27 Their typical location along suture lines, especially the frontozygomatic junction, reflects the embryologic sequestration of ectodermal rests during development.11
Step 1. Clinical and Radiologic Assessment
The present cases mirror the classic clinicopathologic patterns described in literature.11,26 The first pattern is a slow-growing, asymptomatic mass detected since childhood, typical of congenital lesions. The second corresponds to an acute, cellulitis-like presentation caused by rupture of the cyst wall and spillage of keratinous material, leading to chronic granulomatous inflammation. Published diagnostic pathways for pediatric orbital dermoid cysts are primarily driven by clinical presentation. In slow-growing, asymptomatic lesions located along typical suture lines, diagnosis relies mainly on clinical assessment, with CT or MRI selectively used for deep, atypical, or fixed masses to evaluate extent, bony remodeling, and possible intracranial extension. MRI is the primary imaging modality for evaluating orbital masses in children, with CT playing a complementary role for bone assessment.28 This selective use of cross-sectional imaging, aims to guide surgical planning rather than establish a histologic diagnosis, as elective complete excision remains the definitive treatment in uncomplicated cases.27 Recent evidence suggests that even non-midline periorbital dermoid cysts carry a 7% risk of intracranial extension, supporting preoperative imaging in atypical or deep lesions.29
In contrast, acute cellulitis-like presentations following cyst rupture follow a different pathway, analogous to orbital cellulitis, in which urgent cross-sectional imaging is recommended to differentiate inflammatory rupture from infection, exclude abscess formation, and determine the need for prompt surgical intervention.6,26
Cross-sectional imaging is pivotal for delineating lesion extent and guiding surgical planning: CT demonstrated sharply marginated, low-density masses with occasional calcifications and bony remodeling, whereas MRI demonstrated T1 hyperintensity, heterogeneous T2 signal, and occasional fat–fluid levels, reflecting lipid-rich cystic content.30 Figure 1 illustrates the diagnostic and management algorithm for congenital orbital dermoid cysts, integrating clinical presentation, imaging findings, and surgical strategy.
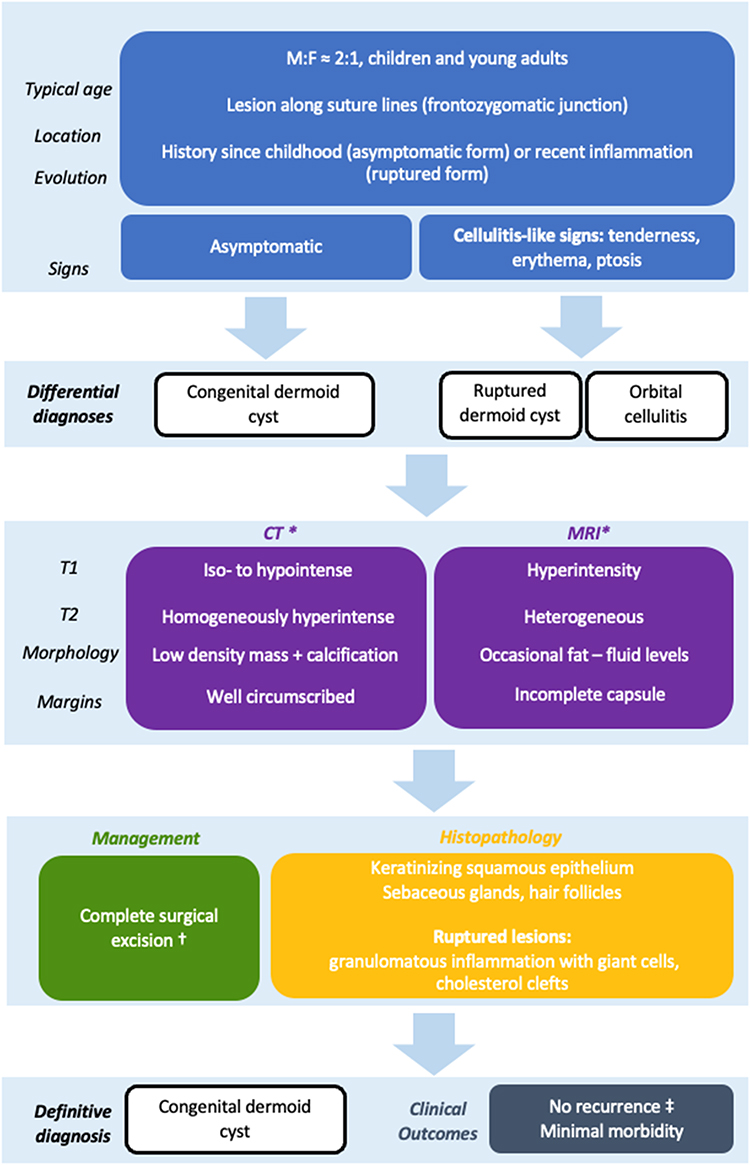 |
Figure 1 Diagnostic–therapeutic flowchart for congenital dermoid cysts. Notes: * Imaging with MRI or CT is indicated for deep, fixed, or atypically located lesions, or when there is suspicion for bony involvement or intracranial extension. † Superficial cysts are typically removed via a direct or eyelid crease incision, while deep or intraosseous lesions may require a lateral orbitotomy.‡ Clinical outcomes are excellent with complete excision, with minimal risk of visual sequelae or recurrence. |
Step 2. Management and Histopathology
All patients underwent surgical excision, as complete surgical excision remains standard to prevent rupture, chronic inflammation, and secondary deformity. Anterior orbitotomy under general anesthesia was performed in each case, with emphasis on intact removal to prevent keratin spillage and subsequent lipogranulomatous inflammation.26 In Case 3, intraoperative rupture occurred and was successfully managed with copious irrigation and meticulous clearance of residual debris. Histopathology confirmed dermoid cysts in all patients, showing keratinizing squamous epithelium with sebaceous glands and hair follicles. Ruptured lesions exhibited foreign-body granulomatous inflammation with multinucleated giant cells, cholesterol clefts, and keratin debris, whereas intact lesions contained laminated keratin within a well-formed epithelial lining.11 Postoperative recovery was uneventful in all cases, with no recurrence observed during follow-up and satisfactory functional and aesthetic outcomes achieved, without the need for adjunctive medical therapy.
Vascular Malformations of the Orbit
OVMs are congenital, low-flow anomalies encompassing venous, lymphatic, and mixed subtypes. Although benign, their overlap with neoplastic or inflammatory lesions often complicates diagnosis and can lead to unnecessary surgery.8,20,31 Figures 2a and Figure 2b illustrate the diagnostic–therapeutic workflow, emphasizing a shift toward multidisciplinary, function-preserving management.
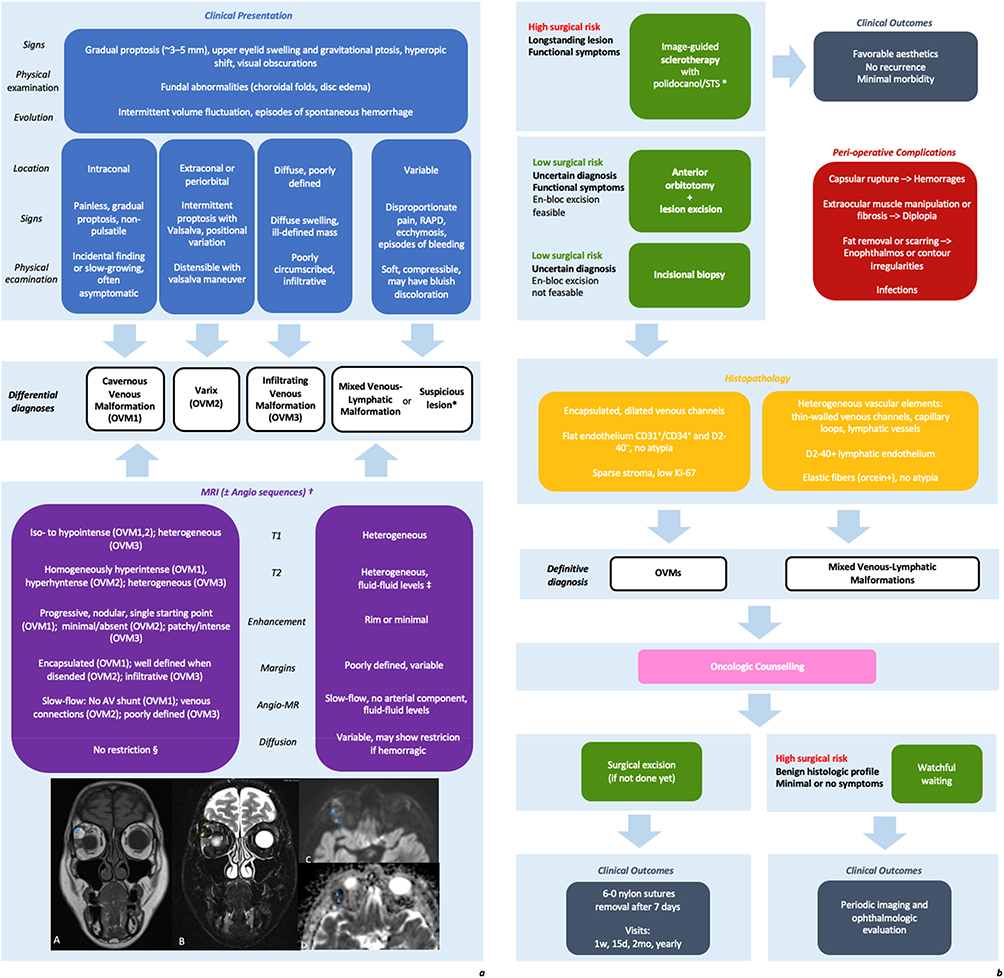 |
Figure 2 (a)Diagnostic flowchart for orbital venous malformations (A) Coronal T1-weighted TSE sequence shows a well-circumscribed, mildly hyperintense extraconal lesion displacing the medial rectus muscle. (B) Fat-suppressed T2-weighted Dixon image reveals homogeneous hyperintensity with suppression of surrounding fat. (C) Diffusion-weighted imaging (b800) shows no signal restriction. (D) Corresponding ADC map confirms preserved diffusivity, supporting a benign, low-flow vascular etiology. * Suspicious lesion indicates atypical clinical or MRI features not consistent with a typical low-flow venous malformation (e.g., rapid growth, disproportionate pain or neurologic signs such as RAPD, infiltrative margins, discordant diffusion restriction, or unusually aggressive enhancement), warranting escalated work-up and possible biopsy.† MRI (± Angio-MR) is recommended for lesion mapping and subtype characterization; Angio-MR is particularly useful when Valsalva-dependent distensibility or venous connections are suspected (typical of OVM2) and to exclude an arterial component.‡ Fluid–fluid levels with recurrent ecchymosis or bleeding favor a combined venous–lymphatic malformation, especially in heterogeneous lesions with variable location.§ DWI/ADC helps confirm low-flow behavior: OVM1–OVM2 typically show no restriction with preserved ADC (ratio ~1.6–1.8). Restricted diffusion should prompt caution for hemorrhage/thrombosis or non-vascular mimickers, consider orbital lymphoma when ADC <0.8 × 10−3 mm2/s. (b) Therapeutic flowchart for orbital venous malformations. |
A three-step diagnostic approach (clinical-radiologic assessment, histopathologic confirmation, and management) mirrors the International Society for the Study of Vascular Anomalies (ISSVA) classification framework, which stratifies vascular malformations into simple (venous, lymphatic, arteriovenous) and combined subtypes based on clinical, imaging, and genetic features.32,33 The ISSVA system emphasizes that accurate classification is essential for appropriate treatment selection, as different OVM subtypes (OVM1, OVM2, OVM3) exhibit distinct clinical behaviors and require tailored management strategies.22
Step 1. Clinical and Radiologic Assessment
OVMs usually present as painless, slowly progressive masses with positional change or compressibility, though manifestations depend on the dominant vascular component.22 In Cases 1–3, venous-dominant lesions caused gradual proptosis and eyelid swelling; Case 3 developed gravitational ptosis from a chronic medial canthal malformation. Figure 3 shows a representative case. Case 5 showed proptosis, diplopia, and anisocoria due to mixed angiodysplasia.
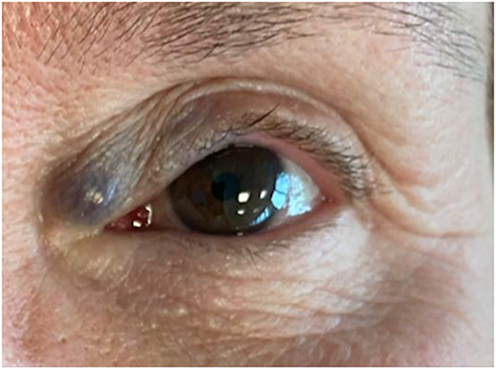 |
Figure 3 OVM at the medial canthus presenting as a longstanding bluish, compressible mass with gravitational ptosis. |
The ACR Appropriateness Criteria recommend MRI without and with IV contrast as first-line imaging for suspected orbital vascular lesions, with CT reserved for delineating calcifications, osseous involvement, or dynamic assessment with Valsalva maneuver.34 MRI patterns guide early differentiation: T1-isointensity and marked T2-hyperintensity typify venous malformations, while heterogeneous signal and irregular borders suggest mixed or lymphatic forms. Recent studies confirm that structural MRI at 3 Tesla can differentiate cavernous venous malformations (OVM1) from other orbital lesions with 93% accuracy using a signature combining T2 hyperintensity relative to cortex, chemical shift artifact, and single starting point of enhancement.35 Lack of diffusion restriction or arteriovenous shunting confirms a low-flow, non-proliferative profile over malignancy or inflammatory pseudotumor.20
Long-standing lesions may show fatty degeneration or orbital-wall remodeling rather than invasion, as seen in Case 2. In Case 2, mild enhancement near the superior rectus mimicked malignancy, highlighting how mass effect and motility restriction can resemble orbital tumors. This represents a recognized diagnostic pitfall: acute thrombosis in venous malformations can present with peripheral rim enhancement and T2 hypointense core, mimicking abscess or tumor, and requires careful clinical correlation.
Step 2. Histopathology
Diagnosis relies on thin-walled, non-proliferative vascular channels with flat endothelium and low Ki-67 (< 2%). Immunostains such as CD31, D2-40, and orcein confirm venous or lymphatic lineage.36 One excised lesion (Case 1) showed chronic dacryoadenitis-like inflammation and vascular ectasia, indicating reactive changes secondary to chronic venous congestion.
Step 3. Management
Management should be tailored within an interdisciplinary framework, favoring individualized surgical planning over radical excision.22,36 Therapeutically, the stepwise approach used in this series mirrors published recommendations.
(i.) Complete en-bloc excision remains the treatment of choice for symptomatic, encapsulated cavernous venous malformations, as demonstrated in Cases 1–3 in this series. Capsule preservation is essential to prevent postoperative inflammation secondary to intraoperative rupture.8 Colletti et al identified OVM1 as a distinct subtype amenable to transnasal endoscopic excision for medial or superomedial lesions, achieving excellent outcomes with minimal morbidity.22
(ii.) Incisional biopsy and observation are appropriate for mixed venous–lymphatic malformations (Cases 4–5), where the lesion’s indolent course and benign histology justify a conservative strategy once malignancy has been excluded. Regular imaging and patient counseling ensured compliance.37 However, recent evidence suggests that observation alone may not be optimal for all patients: more than 60% of venous malformations reportedly progress during adolescence, supporting consideration of earlier intervention even for asymptomatic lesions. For lymphatic malformations, spontaneous regression is rare.
(iii.) Image-guided sclerotherapy represents an effective, minimally invasive option for superficial venous malformations or patients with high surgical risk, such as monocular individuals (Case 6). Its safety profile in the periorbital region is well established. Systematic reviews report 54.9% complete cure rates for low-flow orbital vascular malformations, with 3.4% risk of emergent decompressive surgery and 2.7% risk of vision loss.38 Among sclerosants, the intralesional injection of polidocanol is preferred periorbitally due to its low inflammatory profile. Sclerotherapy is performed under fluoroscopic control using 3% polidocanol, diluted in normal saline solution, with real-time ophthalmologic monitoring of intraocular pressure and ocular motility, followed by post-procedural imaging confirmation.38 However, critical evidence challenges the long-term efficacy of sclerotherapy for distensible venous-dominant malformations: Cohen et al reported universal recurrence after sclerotherapy (mean 3.5 treatments), whereas embolization with excision achieved 100% symptom resolution with no recurrences over 3 years (p < 0.001).39 Alternative sclerosants such as pingyangmycin (bleomycin) have shown 94% marked-to-moderate improvement in low-flow OVMs with minimal adverse events.40
(iv.) Emerging medical therapies with sirolimus have shown promise for refractory pain, swelling, and coagulopathy associated with venous malformations, with 82.5% partial response rates in Phase 2 trials, representing an evolving treatment option for extensive or refractory lesions.41
Solitary Orbital Neurofibroma
Solitary orbital neurofibromas are rare benign peripheral nerve sheath tumors typically presenting as solitary, slow-growing masses, often without systemic manifestations of NF1 (Figure 4).
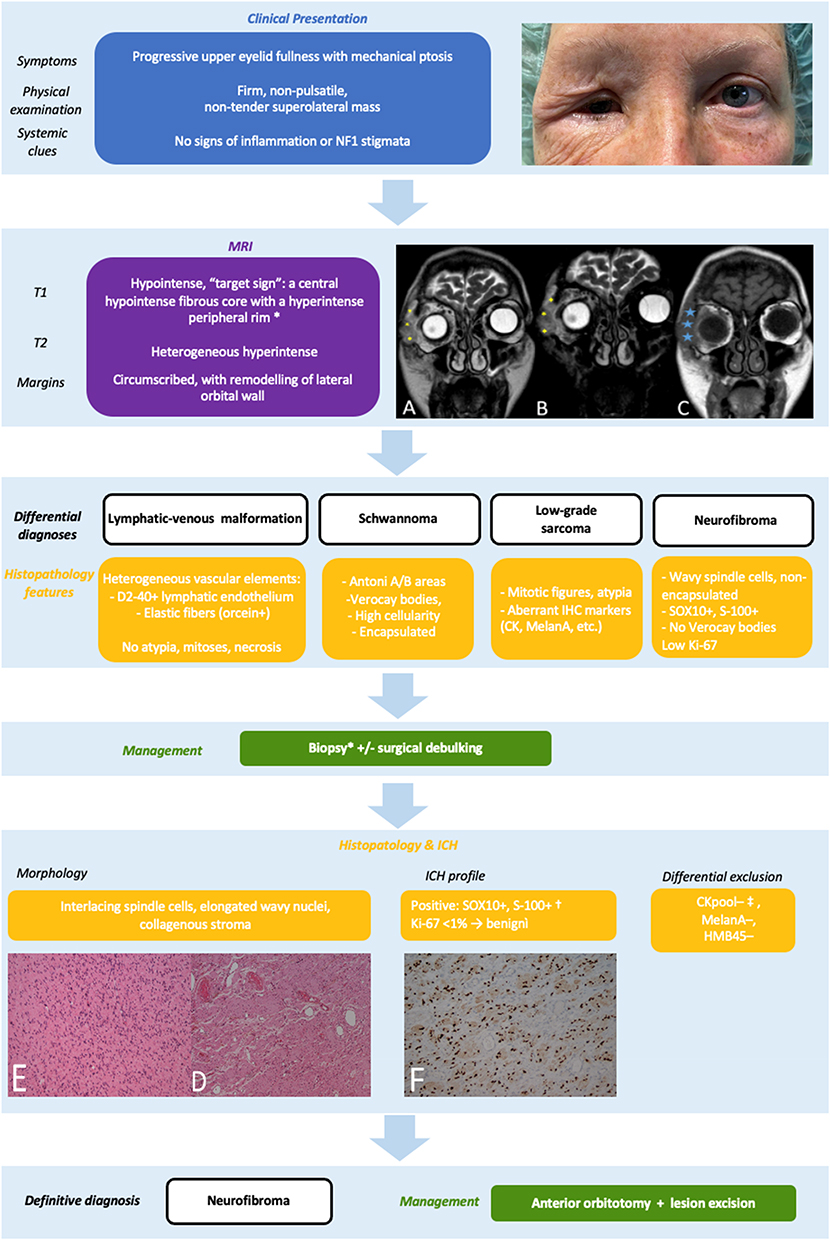 |
Figure 4 Diagnostic–therapeutic flowchart for orbital neurofibroma (A–C) MRI: well-circumscribed, solid extraconal lesion in the right superolateral orbit; lateral orbital wall invasion from subcutaneous tissues, T1-weighted images hypointensity (C, blue asterisks), T2 heterogeneous hyperintensity. (D) H&E low magnification: interlacing spindle cells in a collagenous stroma; (E) high- magnification: elongated wavy nuclei and pale cytoplasm without atypia, mitotic figures or necrosis; (F) IHC: diffuse SOX10+ nuclear staining†. † SOX10 and S-100 positivity confirm neural crest origin, supporting the diagnosis of neurofibroma. ‡ Absence of cytokeratins (CK AE1/AE3), MelanA, and HMB45 excludes epithelial and melanocytic mimickers. |
Step 1. Clinical and Radiologic Assessment
Clinically, they may mimic cavernous hemangioma, schwannoma, or low-grade mesenchymal tumors. Therefore, published pathways rely on MRI as the first major discriminating step rather than symptoms alone.33 Consistently with literature, MRI demonstrated a 2.3-cm T1-hypointense, T2-heterogeneous extraconal lesion encasing the lateral rectus and producing mild bony remodeling without erosion, consistent with a chronic, benign process.42
Step 2. Histopathology
A transcutaneous anterior orbitotomy via an eyelid crease incision provided optimal access to the anterior extraconal space while preserving function and cosmesis. Under magnification, the solid gray-yellow nodular mass (~2.3 cm) was excised with minimal disruption to the levator palpebrae superioris, superior oblique tendon, and neurovascular bundles, despite moderate adherence to surrounding tissues. Accurate histopathologic characterization is essential to differentiate neurofibroma from other spindle-cell orbital tumors. The lesion demonstrated interlacing spindle cells with diffuse SOX10 and S-100 positivity and low proliferative index.43
Step 3. Management
Complete excision via an anterior orbitotomy offers excellent exposure with minimal morbidity. Long-term surveillance is advised because of possible late recurrence, although prognosis remains favorable after total removal.
Idiopathic Orbital Inflammation
IOI, or orbital pseudotumor, represents a non-infectious, non-neoplastic inflammatory disorder of uncertain etiology that may mimic cellulitis, vasculitis, or lymphoma.3
IOI remains a diagnosis of exclusion and should be considered in patients with subacute orbital symptoms (e.g., proptosis, pain, chemosis, diplopia, lid edema) in the absence of infection, malignancy, or systemic disease.3 Published diagnostic pathways for IOI emphasize a subtype-driven sequence that closely mirrors the present workflow. The 2017 Orbital Society Consensus criteria distinguish myositic IOI, in which a short therapeutic trial of systemic corticosteroids may serve as a key diagnostic maneuver, from nonmyositic or infiltrative IOI, where tissue diagnosis is recommended before corticosteroid therapy to avoid obscuring lymphoma, IgG4-related ophthalmic disease, and other mimicking conditions.3,44
In this cohort, both acute and chronic IOI presentations are illustrated. Figures 5a and Figure 5b show the diagnostic and therapeutic workflow.
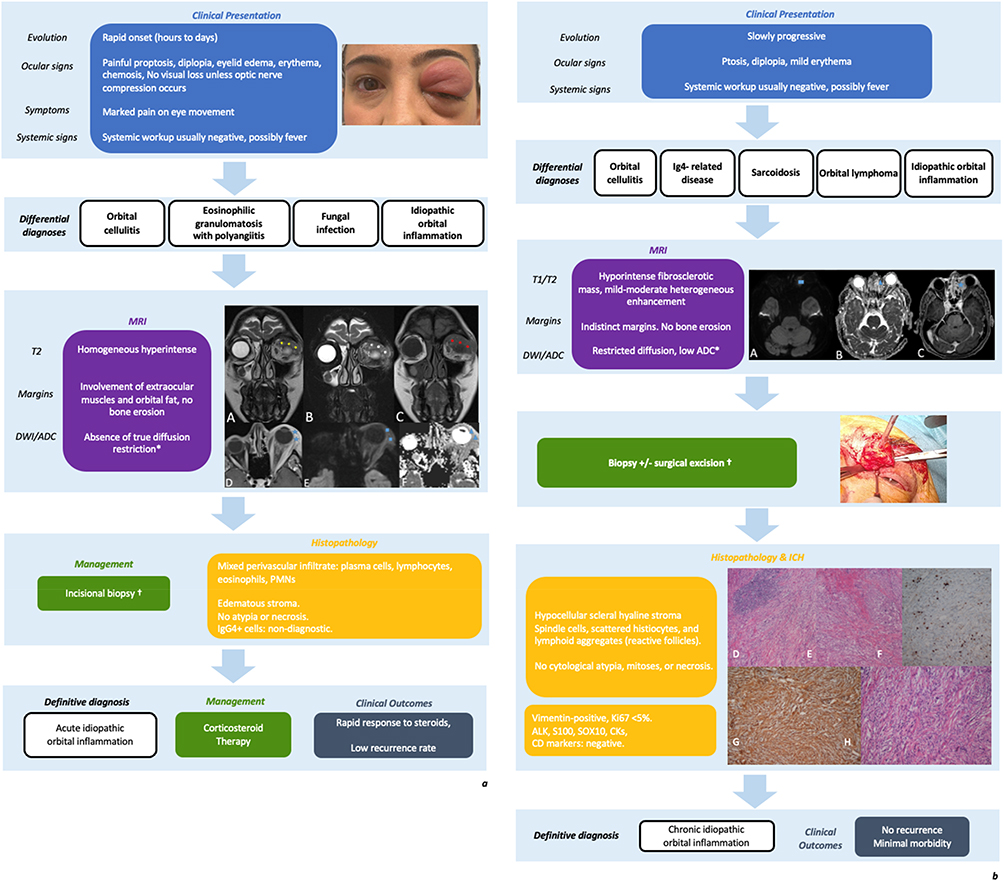 |
Figure 5 (a) Diagnostic–therapeutic flowchart for acute IOI.(A–F) Coronal MRI: T2-hyperintense inflammatory mass involving orbital fat and extraocular muscles, hypointense on T1 (C, red asterisk), without bone erosion.DWI: mild hyperintensity with preserved diffusivity on ADC mapping (E–F), consistent with benign inflammation.† Biopsy should precede corticosteroid therapy to prevent histologic distortion.(b) Diagnostic–therapeutic flowchart for chronic IOI. (A–C) Axial T1- and T2-weighted MRI: hypointense fibrosclerotic mass with indistinct margins from the medial rectus and restricted diffusion (low ADC).(D–E) H&E hypocellular hyalinized stroma with spindle-cell proliferation, histiocytic elements, and lymphoid aggregates.(F) Low Ki-67 (< 5%); (G) diffuse vimentin positivity.IHC excluded malignancy (negative ALK, actin ML, CD3, CD20, CD163, CK AE1/AE3, S100, SOX10, STAT6), supporting fibrosing IOI.*In chronic IOI, diffusion restriction reflects fibrosclerotic tissue and should be interpreted in conjunction with clinical course and histopathology.†Depending on lesion size, location, and clinical impact, either incisional or excisional biopsy may be performed. |
Step 1: Clinical and Radiologic Assessment
Within imaging-based pathways, contrast-enhanced MRI is considered the first-line modality, with diffusion-weighted imaging (DWI) serving as an adjunct to triage inflammatory disease versus lymphoproliferative disorders.45–47 The radiologic patterns observed in this series are consistent with published imaging signatures, with acute IOI typically demonstrating T2 hyperintensity and diffuse soft-tissue involvement, whereas chronic or fibrosing IOI may appear T2 hypointense with associated diffusion restriction.45 Absence of bone erosion or abscess formation helps exclude infection or neoplasm.46 In fulminant cases, biopsy should precede corticosteroid therapy to preserve histologic features.48
Step 2: Histopathology
Acute IOI (Case 1) showed eosinophil-rich infiltration without granulomas, suggesting immune dysregulation.49 Chronic IOI (Case 2) demonstrated fibrosing, spindle-cell proliferation with lymphohistiocytic infiltrates and MAP2K1 p.F53L mutation, consistent with low-grade fibroinflammatory behavior. Moreover, immunostains (CD3, CD20, CD163) in case 2 confirm polymorphic composition, excluding lymphoma and IgG4-related disease.3
Step 3: Management
A multidisciplinary approach involving Ophthalmologist, ENT, rheumatologist, and oncologist is essential. From a therapeutic standpoint, the stepwise management strategy adopted in this series reflects contemporary pathways that retain systemic corticosteroids as first-line therapy, with rapid symptomatic improvement often confirming diagnosis, while reserving immunomodulatory agents for refractory or relapsing disease.50 Chronic or relapsing cases may require surgical debulking, methotrexate, or rituximab. As a matter of fact, recent comparative studies and interventional trial data further support rituximab as an effective option in selected cases of refractory orbital inflammatory disease.51 In vision-threatening inflammation, orbital decompression can restore optic nerve function while histologic confirmation is awaited. Long-term multidisciplinary follow-up is recommended given the risk of relapse or fibrosing transformation.
Orbital Meningioma
Orbital meningiomas account for 1–2% of orbital tumors and may arise primarily from the optic nerve sheath or secondarily from sphenoidal or cavernous origins.14,52
Step 1: Clinical and Radiologic Assessment
Published studies emphasize a stepwise, imaging-driven approach in which MRI and CT are complementary: MRI for soft-tissue definition and optic nerve involvement, CT for hyperostosis and osteosclerotic bone remodeling, hallmark features that differentiate spheno-orbital meningiomas from fibrous dysplasia or metastatic disease.53 This approach is endorsed by the European Association of Neuro-Oncology (EANO) guidelines.54
Step 2: Histopathology
Across published pathways, WHO grading is the central decision point, directly determining prognosis and adjuvant therapy: Grade I lesions display minimal mitoses, strong progesterone receptor positivity, and low proliferative index, and are managed with surgery and surveillance.55 Grade II–III tumors require adjuvant radiotherapy or stereotactic radiosurgery.55,56
Step 3: Management
Published algorithms emphasize symptom-driven, function-preserving management, recognizing that complete resection is often limited by proximity to the optic nerve and cavernous sinus.56 Surgical decompression provided dual benefit: (i). histological confirmation, since grading is essential for therapy, WHO Grade I can be monitored after resection, whereas higher grades may require radiotherapy; and (ii). relief of compressive optic neuropathy, thereby preserving visual function.55,56
Long-term follow-up remains mandatory due to the risk of recurrence or intracranial extension.54,55 Figure 6 shows the diagnostic and therapeutic workflow.
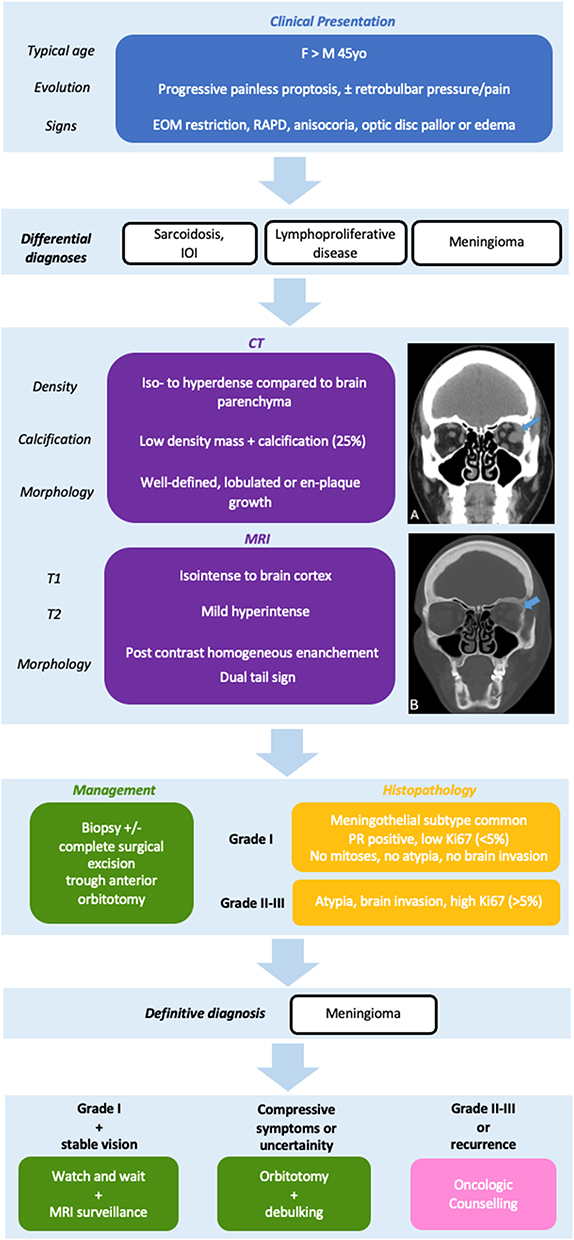 |
Figure 6 Diagnostic-therapeutic flowchart for orbital meningioma. (A) Non-contrast coronal CT: hyperdense extraconal mass adjacent to the lateral rectus muscle on the left side, with well-defined borders and no intraconal extension (arrow).(B) Bone window demonstrates frontal bone remodeling with irregular hyperostosis and an osteosclerotic pattern, highly suggestive of spheno-orbital meningioma (arrow). |
Epithelial Tumors Involving the Orbit
Epithelial malignancies may invade the orbit via direct extension or perineural spread, carrying high risks of local recurrence and functional loss. Clinical warnings signs include rapid growth, ulceration, pain, eyelid destruction, and globe displacement.57
The diagnostic and therapeutic workflow for malignant epithelial tumors is summarized in Figure 7, outlining red-flag clinical features, differential diagnosis, and tailored management strategies based on histopathologic subtype and immunophenotypic profile. A representative case of lacrimal gland adenoid cystic carcinoma (ACC) is illustrated in Figure 8.
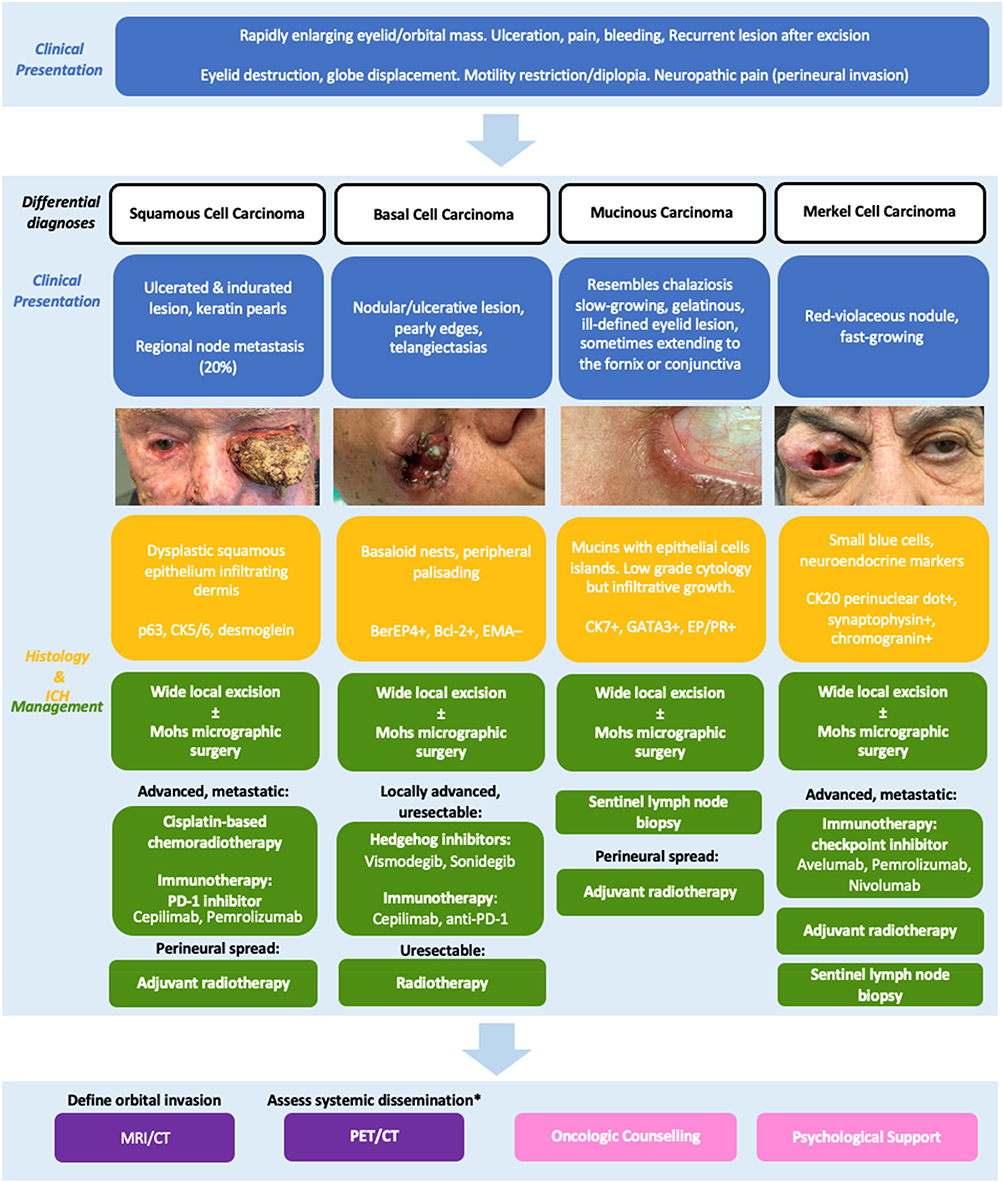 |
Figure 7 Diagnostic–therapeutic flowchart for malignant epithelial tumors involving the orbit. |
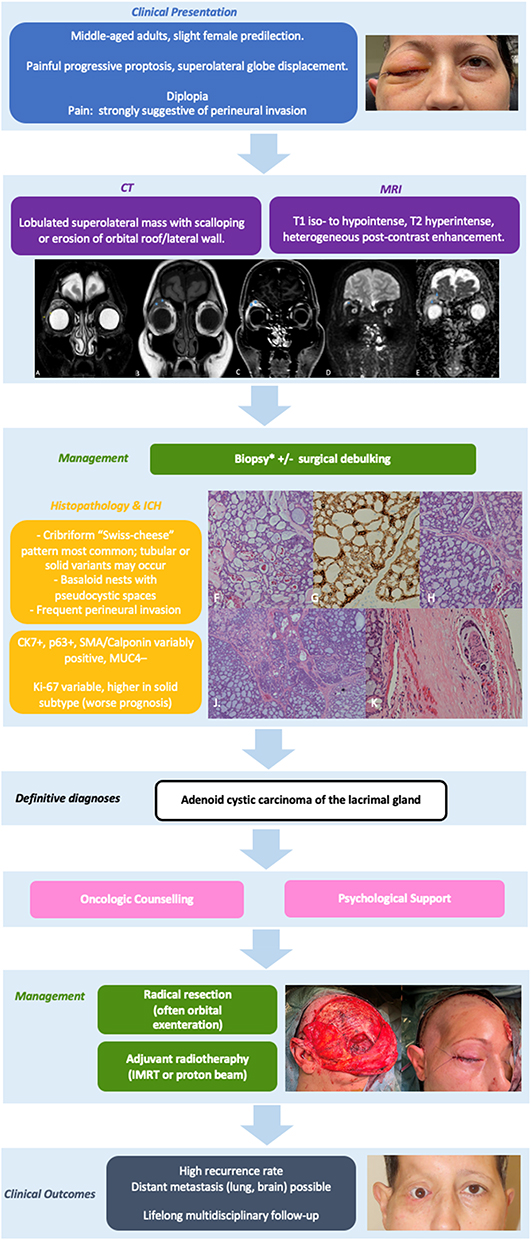 |
Figure 8 Diagnostic–therapeutic flowchart for ACC of the lacrimal gland.(A) Axial T2-weighted Dixon image: hyperintense extraconal lesion near the superior rectus with clear fat suppression.(B and C) Coronal T1 and post-contrast fat-suppressed sequences: hypointensity and strong enhancement.(D and E) DWI (b = 1000) and ADC: high diffusivity, consistent with slow-growing behavior.(F–K) Histopathology: cribriform “Swiss-cheese” architecture with pseudocystic spaces and basophilic material; perineural infiltration (H&E 4×–20×).IHC: CK7⁺/EMA⁺/MUC4⁺, Ki-67 ≈ 10%, confirming ACC. |
Step 1: Clinical and Radiologic Assessment
Imaging (CT for bone; contrast MRI for soft-tissue/perineural disease) defines extent. The ACR Appropriateness Criteria recommend MRI orbits with IV contrast as the optimal modality for suspected orbital malignancy, with CT reserved for bone involvement.34
Step 2: Histopathology
Histopathology with IHC confirms diagnosis, determines margin status and depth of invasion, and guides adjuvant therapy.58 In this setting, Mohs micrographic surgery (MMS) is the standard of care due to superior margin control and tissue preservation.59 Primary MUC shows mucin pools with epithelial islands and a CK7⁺/GATA3⁺/ER⁺/PR⁺ profile.60 For ACC, perineural invasion is a key prognostic factor, and basaloid/solid histologic subtype correlates with worse disease-specific survival.61
Staging followed American Joint Committee on Cancer (AJCC) 8th edition criteria, which standardize TNM classification for eyelid carcinoma, MCC, and ACC. Validation studies confirm that T category per AJCC 8th edition is predictive of nodal metastasis, distant metastasis, and disease-specific survival, with T2c or worse associated with higher risk.62 The criteria used in this study are summarized in Table 6.63 (Table 9)
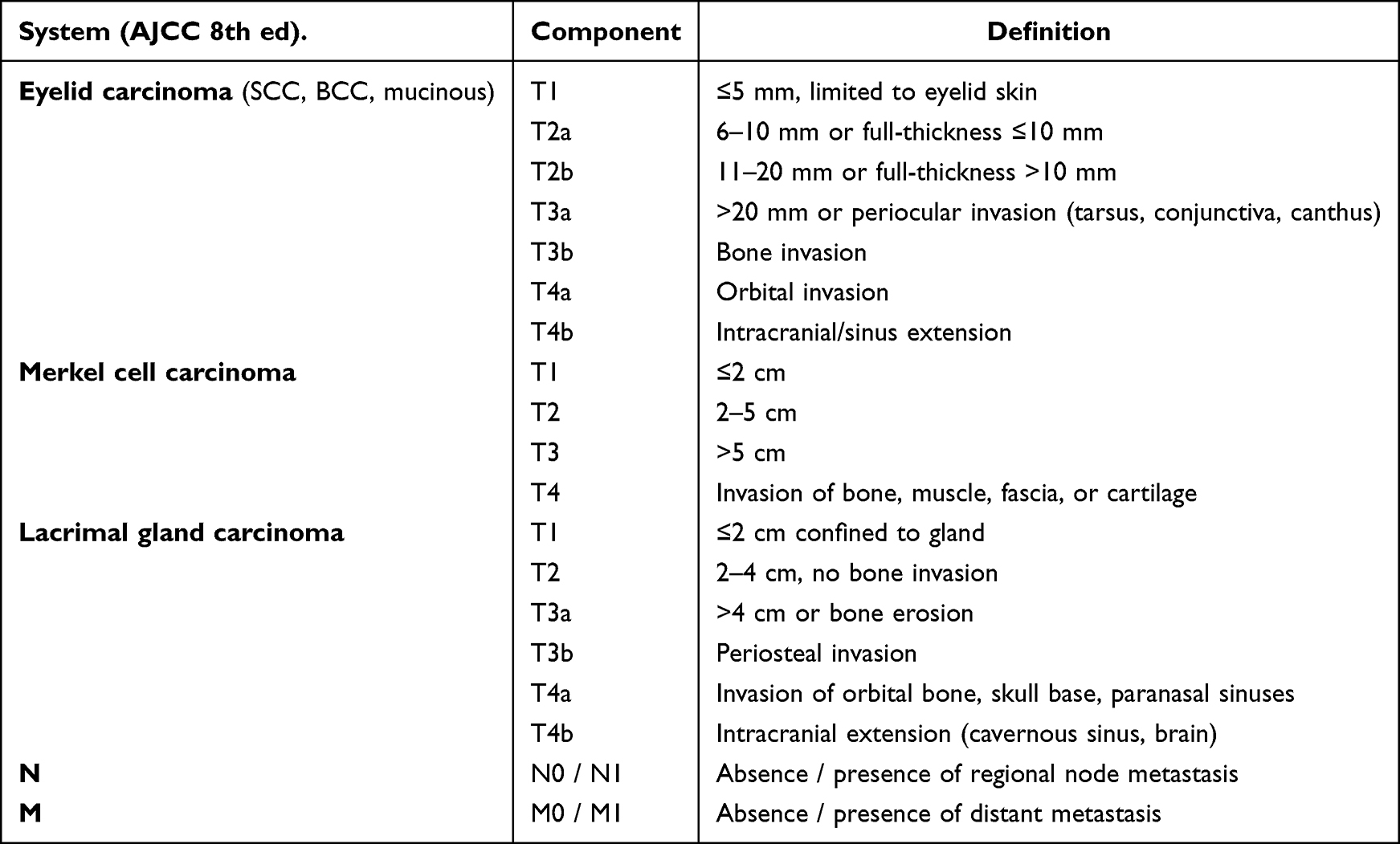 |
Table 9 Staging Criteria for Epithelial Orbital Tumors (AJCC 8th Edition) |
Step 3: Management
Management is Multidisciplinary
(i) ACC of the lacrimal gland: often requires exenteration + adjuvant RT due to perineural invasion (Figure 9); however, contemporary evidence supports multimodal treatment with neoadjuvant intra-arterial cytoreductive chemotherapy (IACC), surgery, and extended-field radiotherapy as superior for local tumor control and eye salvage (5-year survival 84% vs. 72%; HR 0.4).61
 |
Figure 9 Orbital exenteration specimen following radical orbital exenteration for LG ACC. The globe is en-bloc with surrounding periorbital soft tissues and adnexal structures, following oncologic resection principles. The specimen demonstrates intact removal with macroscopically clear margins to minimize the risk of perineural spread and local recurrence. |
(ii) BCC/BSC with orbital invasion: complete excision with margin control ± RT; hedgehog inhibitors (e.g., sonidegib), may enable organ preservation in selected BCC cases;64 cemiplimab is approved for locally advanced or metastatic SCC.65 Recent evidence demonstrates MMS is associated with improved outcomes compared to wide local excision for high-stage cSCC (local recurrence 9.6% vs. 19.8%; disease-specific death 7.1% vs. 17.5%).66
(iii) Primary MUC: wide local excision with margin control; sentinel node assessment can be considered.
(iv) MCC: aggressive resection with nodal management, adjuvant RT/systemic immunotherapy per staging.64,67–70 For periocular MCC, MMS or PDEMA is preferred for margin control.57
Overall, optimal treatment relies on complete excision with margin control and tailored adjuvant therapies guided by a multidisciplinary tumor board.58,71
Limitations
This study is limited by its retrospective design, small sample size, and single tertiary referral setting, which may have introduced a selection bias toward more complex cases and limits generalizability. The absence of a non-multidisciplinary control cohort restricts comparative outcome assessment, and patient-reported outcome measures were not systematically collected, precluding a comprehensive evaluation of functional and quality-of-life endpoints. Future prospective, multicenter studies with larger cohorts and validated outcome instruments are needed to confirm the diagnostic and therapeutic benefits of structured multidisciplinary pathways for unilateral orbital disease.
Conclusions
This clinicopathological series illustrates the diagnostic complexity of unilateral orbital lesions and the value of an integrated clinical, radiologic, and histopathologic approach. Rather than introducing novel diagnostic tools, the study offers a pragmatic synthesis of established methods into reproducible decision pathways applicable to real-world clinical practice.
Close collaboration among ophthalmologists, radiologists, pathologists, and oncologists enabled accurate lesion stratification, appropriate surgical planning, and tailored adjuvant management while prioritizing functional preservation.
Beyond individual findings, this work emphasizes the educational and practical relevance of a structured diagnostic framework. Although developed in a tertiary referral setting, the adaptability of the proposed workflow may support earlier diagnostic reasoning, timely referral, and avoidance of unnecessary interventions across different levels of care. Further prospective and multicenter validation will be essential to quantify its impact on diagnostic efficiency, clinical outcomes, and resource utilization.
Data Sharing Statement
De-identified data underlying the results reported in this article (clinical variables, imaging summaries, and histopathologic categorizations) are available from the corresponding author upon reasonable request for academic purposes.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Humanitas Research Hospital, Milan (protocol code 4967; project title “Neoformazioni orbitarie”; approval date 15 July 2025).Patient consent for publication was waived due to the retrospective design and full anonymization of data, as approved by the Ethics Committee.
Acknowledgments
The authors thank the multidisciplinary team at Humanitas Research Hospital for their support and collaboration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no financial or non-financial competing interests related to the content of this manuscript.
References
1. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions. Ophthalmology. 2004;111(5):997–24. doi:10.1016/j.ophtha.2003.01.002.
2. Demirci H, Shields CL, Shields JA, Honavar SG, Mercado GJ, Tovilla JC. Orbital tumors in the older adult population. Ophthalmology. 2002;109(2):243–248. doi:10.1016/S0161-6420(01)00932-0
3. Mombaerts I.Idiopathic Orbital Inflammation.Patel BCK, Singh AD.editors..Clinical Ophthalmic Oncology.Internet;Cham;Springer Nature Switzerland.2025.75–83.
4. Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43–67. doi:10.1530/EJE-21-0479
5. Piscopo R, Romano M, Maria AD, Vinciguerra R, Vinciguerra P. Ocular onset of paraneoplastic pemphigus presenting as hyperemic conjunctivitis and massive bilateral eyelid ulceration: a case report and literature review. Ocul Immunol Inflamm. 2018;26(2):265–268. doi:10.1080/09273948.2016.1203958
6. Tsirouki T, Dastiridou AI, Ibánez Flores N, et al. Orbital cellulitis. Surv Ophthalmol. 2018;63(4):534–553.
7. Sindoni A, Fama’ F, Vinciguerra P, et al. Orbital metastases from breast cancer: a single institution case series. J Surg Oncol. 2020;122(2):170–175. doi:10.1002/jso.25927
8. Rootman DB, Heran MKS, Rootman J, White VA, Luemsamran P, Yucel YH. Cavernous venous malformations of the orbit (so-called cavernous haemangioma): a comprehensive evaluation of their clinical, imaging and histologic nature. Br J Ophthalmol. 2014;98(7):880–888. doi:10.1136/bjophthalmol-2013-304460
9. Rossin EJ, Szypko C, Giese I, Hall N, Gardiner MF, Lorch A. Factors associated with increased risk of serious ocular injury in the setting of orbital fracture. JAMA Ophthalmol. 2021;139(1):77. doi:10.1001/jamaophthalmol.2020.5108
10. Di Maria A, Barone G, Gaeta A, et al. Persistent conjunctival chemosis after lower lid blepharoplasty: a comparison of different surgical techniques. J Clin Med. 2024;13(7):2093. doi:10.3390/jcm13072093
11. Sherman RP, Rootman J, Lapointe JS. Orbital dermoids: clinical presentation and management. Br J Ophthalmol. 1984;68(9):642–652. doi:10.1136/bjo.68.9.642
12. Sindoni A, Di Maria A, Fama’ F. Orbital metastases in infiltrating lobular carcinoma of the breast. J Surg Oncol. 2020;122(3):569. doi:10.1002/jso.26045
13. Prabhakaran VC. Orbital and Adnexal Sarcoidosis. Arch Ophthalmol. 2007;125(12):1657. doi:10.1001/archopht.125.12.1657
14. Yarabarla V, Mylarapu A, Han TJ, McGovern SL, Raza SM, Beckham TH. Intracranial meningiomas: an update of the 2021 World Health Organization classifications and review of management with a focus on radiation therapy. Front Oncol. 2023;13:1137849. doi:10.3389/fonc.2023.1137849
15. Sindoni A, Famà F, Vinciguerra P, Gioffrè-Florio M, Di Maria A. Orbital metastasis in a male patient after seven years from breast cancer diagnosis. Breast J. 2020;26(10):2060–2062. doi:10.1111/tbj.13937
16. Sjö LD. Ophthalmic lymphoma: epidemiology and pathogenesis. Acta Ophthalmol. 2009;87:1–20. doi:10.1111/j.1755-3768.2008.01478.x
17. Kirkova R, Dineva S, Stradiotto E, Tanev I, Di Maria A. The riddle of the double vision—a rare case of intracranial tumor: when imaging resolves the mystery. Diagnostics. 2024;14(9):932. doi:10.3390/diagnostics14090932
18. Tawfik HA, Abdelhalim A, Elkafrawy MH. Computed tomography of the orbit – a review and an update. Saudi J Ophthalmol. 2012;26(4):409–418. doi:10.1016/j.sjopt.2012.07.004
19. Bryden FM, Pyott AA, Bailey M, McGhee CNJ. Real time ultrasound in the assessment of intraocular foreign bodies. Eye. 1990;4(5):727–731. doi:10.1038/eye.1990.103
20. Sepahdari AR, Politi LS, Aakalu VK, Kim HJ, Razek AAKA. Diffusion-weighted imaging of orbital masses: multi-institutional data support a 2-adc threshold model to categorize lesions as benign, malignant, or indeterminate. Am J Neuroradiol. 2014;35(1):170–175. doi:10.3174/ajnr.A3619
21. Graue GF, Finger PT, Maher E, et al. Ocular adnexal lymphoma staging and treatment: American joint committee on cancer versus ann arbor. Eur J Ophthalmol. 2013;23(3):344–355.
22. Colletti G, Biglioli F, Poli T, et al. Vascular malformations of the orbit (lymphatic, venous, arteriovenous): diagnosis, management and results. J Cranio-Maxillofac Surg. 2019;47(5):726–740.
23. Borgia A, Manara S, Balzarotti M, Vinciguerra P, Di Maria A. Small lymphocytic lymphoma in true trilineage hematopoietic tissue within heterotopic ossification in an enucleated blind painful eye: a case report. J Med Case Rep. 2020;14(1):92. doi:10.1186/s13256-020-02430-9
24. Lowen MS, Saraiva VS, Martins MC, Burnier MN. Immunohistochemical profile of lymphoid lesions of the orbit. Can J Ophthalmol. 2005;40(5):634–639. doi:10.1016/S0008-4182(05)80060-2
25. Płachta I, Kleibert M, Czarnecka AM, Spałek M, Szumera-Ciećkiewicz A, Rutkowski P. Current diagnosis and treatment options for cutaneous adnexal neoplasms with apocrine and eccrine differentiation. Int J Mol Sci. 2021;22(10):5077. doi:10.3390/ijms22105077
26. Bajric J, Griepentrog GJ, Mohney BG. Pediatric periocular dermoid cysts: incidence, clinical characteristics, and surgical outcomes. Ophthalmic Epidemiol. 2019;26(2):117–120. doi:10.1080/09286586.2018.1525412
27. Shields JA, Shields CL. Orbital cysts of childhood—classification, clinical features, and management. Surv Ophthalmol. 2004;49(3):281–299. doi:10.1016/j.survophthal.2004.02.001
28. Joseph AK, Guerin JB, Eckel LJ, et al. Imaging findings of pediatric orbital masses and tumor mimics. Radiogr Rev Publ Radiol Soc N Am Inc. 2022;42(3):880–897.
29. Buncke MJ, Lilly GL, Hamilton BE, MacArthur CJ. When is pre-operative imaging required for craniofacial dermoid cysts/sinuses? A review. Int J Pediatr Otorhinolaryngol. 2022;155:111090. doi:10.1016/j.ijporl.2022.111090
30. Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006;239(3):650–664. doi:10.1148/radiol.2393050823
31. Legiehn GM, Heran MKS. Venous malformations: classification, development, diagnosis, and interventional radiologic management. Radiol Clin North Am. 2008;46(3):545–597. doi:10.1016/j.rcl.2008.02.008
32. Wassef M, Blei F, Adams D, et al. Vascular anomalies classification: recommendations from the international society for the study of vascular anomalies. Pediatrics. 2015;136(1):e203–214. doi:10.1542/peds.2014-3673
33. Tawfik HA, Dutton JJ. Orbital vascular anomalies: a nomenclatorial, etiological, and nosologic conundrum. Ophthal Plast Reconstr Surg. 2022;38(2):108–121. doi:10.1097/IOP.0000000000002029
34. Expert Panel on Neurological Imaging. Friedman ER, Juliano AF, Hagiwara M, et al. ACR Appropriateness Criteria® Vision Loss. J Am Coll Radiol JACR. 2025;22(11S):S738–65. doi:10.1016/j.jacr.2025.08.030.
35. Elbaze S, Duron L, Mambour N, et al. A signature of structural MRI features at 3 Tesla allows an accurate characterization of orbital cavernous venous malformation. Eur Radiol. 2023;33(3):2149–2159. doi:10.1007/s00330-022-09163-x
36. Li T, Jia R, Fan X. Classification and treatment of orbital venous malformations: an updated review. Front Med. 2019;13(5):547–555. doi:10.1007/s11684-018-0623-2
37. Benoiton LA, Chan K, Steiner F, FitzJohn T, Tan ST. Management of orbital and periorbital venous malformation. Front Surg. 2017;4:27. doi:10.3389/fsurg.2017.00027
38. De Maria L, De Sanctis P, Balakrishnan K, Tollefson M, Brinjikji W. Sclerotherapy for venous malformations of head and neck: systematic review and meta-analysis. Neurointervention. 2020;15(1):4–17. doi:10.5469/neuroint.2019.00213
39. Cohen LM, Goldberg RA, Rootman DB. Recurrence of distensible orbital venous-dominant venolymphatic malformations after sclerotherapy versus embolization with excision. Ophthal Plast Reconstr Surg. 2022;38(3):283–288. doi:10.1097/IOP.0000000000002085
40. Jia R, Xu S, Huang X, et al. Pingyangmycin as first-line treatment for low-flow orbital or periorbital venous malformations: evaluation of 33 consecutive patients. JAMA Ophthalmol. 2014;132(8):942–948. doi:10.1001/jamaophthalmol.2013.8229
41. Gallant SC, Chewning RH, Orbach DB, Trenor CC, Cunningham MJ. Contemporary management of vascular anomalies of the head and neck-part 1: vascular malformations: a review. JAMA Otolaryngol-- Head Neck Surg. 2021;147(2):197–206. doi:10.1001/jamaoto.2020.4353
42. Hassell DS, Bancroft LW, Kransdorf MJ, et al. Imaging appearance of diffuse neurofibroma. Am J Roentgenol. 2008;190(3):582–588.
43. Magro G, Broggi G, Angelico G, et al. Practical approach to histological diagnosis of peripheral nerve sheath tumors: an update. Diagnostics. 2022;12(6):1463. doi:10.3390/diagnostics12061463
44. Mombaerts I, Bilyk JR, Rose GE, et al. Consensus on diagnostic criteria of idiopathic orbital inflammation using a modified delphi approach. JAMA Ophthalmol. 2017;135(7):769–776. doi:10.1001/jamaophthalmol.2017.1581
45. Lee EJ, Jung SL, Kim BS, et al. MR imaging of orbital inflammatory pseudotumors with extraorbital extension. Korean J Radiol. 2005;6(2):82. doi:10.3348/kjr.2005.6.2.82
46. Ferreira TA, Saraiva P, Genders SW, Buchem MV, Luyten GPM, Beenakker JW. CT and MR imaging of orbital inflammation. Neuroradiology. 2018;60(12):1253–1266. doi:10.1007/s00234-018-2103-4
47. Aydin N, Saylisoy S, Celik O, Aslan AF, Odabas A. Segmentation of orbital and periorbital lesions detected in orbital magnetic resonance imaging by deep learning method. Pol J Radiol. 2022;87:e516–20. doi:10.5114/pjr.2022.119808
48. Mohammad AENA. Local steroid injection for management of different types of acute idiopathic orbital inflammation: an 8-year study. Ophthal Plast Reconstr Surg. 2013;29(4):286–289. doi:10.1097/IOP.0b013e318293750c
49. Noguchi H, Kephart GM, Campbell RJ, et al. Tissue eosinophilia and eosinophil degranulation in orbital pseudotumor. Ophthalmology. 1991;98(6):928–932. doi:10.1016/S0161-6420(91)32200-0
50. Al-Ghazzawi K, Neumann I, Knetsch M, et al. Treatment outcomes of patients with orbital inflammatory diseases: should steroids still be the first choice? J Clin Med. 2024;13(14):3998. doi:10.3390/jcm13143998
51. Suhler EB, Lim LL, Beardsley RM, et al. Rituximab therapy for refractory orbital inflammation: results of a phase 1/2, dose-ranging, randomized clinical trial. JAMA Ophthalmol. 2014;132(5):572–578. doi:10.1001/jamaophthalmol.2013.8179
52. Saeed P, Rootman J, Nugent RA, White VA, Mackenzie IR, Koornneef L. Optic nerve sheath meningiomas. Ophthalmology. 2003;110(10):2019–2030. doi:10.1016/S0161-6420(03)00787-5
53. Lyndon D, Lansley JA, Evanson J, Krishnan AS. Dural masses: meningiomas and their mimics. Insights Imaging. 2019;10(1):11. doi:10.1186/s13244-019-0697-7
54. Goldbrunner R, Minniti G, Preusser M, et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016;17(9):e383–391. doi:10.1016/S1470-2045(16)30321-7
55. Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-Oncol. 2021;23(8):1231–1251. doi:10.1093/neuonc/noab106
56. Colombo G, Ferreli F, Baram A, et al. Inferolateral transorbital endoscopic approach for spheno-orbital meningiomas. J Craniofac Surg. 2022;33(3):e260–5. doi:10.1097/SCS.0000000000008062
57. Merritt H, Sniegowski M, Esmaeli B. Merkel cell carcinoma of the eyelid and periocular region. Cancers. 2014;6(2):1128–1137. doi:10.3390/cancers6021128
58. Leibovitch I, Mcnab A, Sullivan T, Davis G, Selva D. Orbital invasion by periocular basal cell carcinoma. Ophthalmology. 2005;112(4):717–723. doi:10.1016/j.ophtha.2004.11.036
59. Periocular and ocular surface nonmelanoma skin cancer - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/37866412/.
60. Papalas JA. Primary mucinous carcinoma of the eyelid: a clinicopathologic and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128(9):1160. doi:10.1001/archophthalmol.2010.177
61. Tse DT, Benedetto PW, Tse BC, Feuer WJ. Neoadjuvant intra-arterial cytoreductive chemotherapy for lacrimal gland adenoid cystic carcinoma: a long-term follow-up study of a trimodal strategy. Am J Ophthalmol. 2022;240:239–251. doi:10.1016/j.ajo.2022.03.027
62. Sa HS, Rubin ML, Xu S, et al. Prognostic factors for local recurrence, metastasis and survival for sebaceous carcinoma of the eyelid: observations in 100 patients. Br J Ophthalmol. 2019;103(7):980–984. doi:10.1136/bjophthalmol-2018-312635
63. Klingenstein A, Samel C, Messmer EM, Garip-Kuebler A, Priglinger SG, Hintschich CR. Epidemiological characteristics and clinical course of eyelid squamous cell carcinoma patients from a large tertiary centre between 2009 and 2020. Br J Ophthalmol. 2022;106;(8):1057–62
64. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):2171–2179. doi:10.1056/NEJMoa1113713
65. Trotier DC, Huang L, van Landingham SW, Burr AR, Ma VT. Review of recent advances in managing periocular skin malignancies. Front Oncol. 2024;14:1275930. doi:10.3389/fonc.2024.1275930
66. Wang DM, Vestita M, Murad FG, et al. Mohs surgery vs wide local excision in primary high-stage cutaneous squamous cell carcinoma. JAMA Dermatol. 2025;161(5):508–514. doi:10.1001/jamadermatol.2024.6214
67. Stratigos AJ, Sekulic A, Peris K, et al. Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: an open-label, multi-centre, single-arm, phase 2 trial. Lancet Oncol. 2021;22(6):848–857.
68. Kaufman HL, Russell J, Hamid O, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016;17(10):1374–1385.
69. Giannaccare G, Bernabei F, Angi M, et al. Iatrogenic ocular surface diseases occurring during and/or after different treatments for ocular tumours. Cancers. 2021;13(8):1933. doi:10.3390/cancers13081933
70. Romeo MA, Taloni A, Borselli M, et al. Iatrogenic ocular surface complications after surgery for ocular and adnexal tumors. Cancers. 2025;17(9):1384. doi:10.3390/cancers17091384
71. Di Maria A, Barone G, Ferraro V, et al. Recurrence of basal cell carcinoma treated with surgical excision and histopathological analysis with frozen section technique with complete margin control (cmc-fs): a 15-year experience of a reference center. Cancers. 2023;15(15):3840. doi:10.3390/cancers15153840
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.