Back to Journals » Journal of Healthcare Leadership » Volume 17
Collaborative and Shared Leadership Dynamics in Healthcare Action Teams: A Systematic Literature Review
Authors Curșeu PL ![]() , van Rijswijk J
, van Rijswijk J ![]() , Schruijer SGL
, Schruijer SGL
Received 28 October 2025
Accepted for publication 25 December 2025
Published 31 December 2025 Volume 2025:17 Pages 877—899
DOI https://doi.org/10.2147/JHL.S520534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Petru Lucian Curșeu,1,2 Jan van Rijswijk,1 Sandra GL Schruijer3
1Department of Organization, Open Universiteit, Heerlen, the Netherlands; 2Department of Psychology, Babeş – Bolyai University Cluj-Napoca, Cluj-Napoca, Romania; 3Utrecht School of Governance, Utrecht University, Utrecht, the Netherlands
Correspondence: Petru Lucian Curșeu, Open Universiteit, Valkenburgerweg 177, Heerlen, 6419 AT, the Netherlands, Email [email protected]; [email protected]
Background: Healthcare Action Teams (HATs) operate under high-pressure, time-sensitive conditions where effective collaboration is critical for patient outcomes. While collaborative leadership is increasingly recognized as beneficial in such contexts, the literature remains fragmented, with inconsistent terminology and limited integration of findings.
Aim: This study systematically reviews how collaborative leadership is conceptualized, operationalized, and evaluated in HATs. It identifies different forms of collaborative leadership, the mechanisms that support or constrain its effectiveness, the organizational factors that influence its implementation, and the outcomes for team performance and patient care.
Methods: A systematic literature review is conducted based on PRISMA guidelines and using a comprehensive and expanded search query in Web of Science and EBSCOhost. More than 250 studies were identified in the initial screening, and 56 peer-reviewed articles, published through September 2025, that addressed collaborative leadership in HATs were ultimately selected and included in further analyses. Analysis was guided by four research questions and integrated based on functional leadership theory and models of social differentiation in teams.
Results: Two main forms of leadership were identified: vertical differentiation (authority shifts across hierarchical roles) and horizontal differentiation (distributed leadership among peers). Collaborative leadership enhances team adaptability, shared mental models, psychological safety, and communication. However, its effectiveness depends on factors such as organizational hierarchy, professional identity salience, task complexity, and team member interpersonal familiarity. A functional definition of collaborative leadership was proposed, emphasizing four leadership functions: activating resources, framing the task environment, mobilizing support, and synthesizing collaboration.
Conclusion: Collaborative leadership in HATs is a dynamic, context-sensitive process that enables adaptive coordination in complex clinical settings. When supported by appropriate organizational structures and team-level conditions, it enhances communication, trust, and patient safety. However, under rigid hierarchies or unclear role structures, its effectiveness may be reduced. This study offers a functional lens for understanding collaborative leadership in HATs and provides future research directions.
Keywords: collaborative leadership, shared leadership, healthcare, healthcare action teams
Introduction
Teamwork is essential in modern healthcare environments for delivering high-quality patient care. In particular, certain areas of healthcare, such as trauma response, emergency care, surgical interventions, and general inpatient care, rely on multidisciplinary teams that operate under significant time pressure and clinical uncertainty, which makes effective collaboration and communication critical for achieving positive patient outcomes.1 These multidisciplinary teams are often referred to as Healthcare Action Teams (HATs), and current literature identifies leadership within these teams as an important predictor of successful team performance.2,3 While leadership may take many forms, decentralized leadership, entailing the distribution (or sharing) of leadership functions among different individuals, is particularly well-suited to integrating diverse resources within the teams.4 Such collaborative forms of leadership in HATs foster the integration of diverse expertise and resources, enabling dynamic adaptation to shifting clinical demands while ensuring the swift and coordinated implementation of work protocols and medical procedures.
Despite the recognition of the positive impact of collaborative leadership (CL) in HATs, it remains unclear what this leadership approach entails, which forms of CL exist in HATs, under what conditions these forms are applicable, and how they are effectively realized in practice. The literature currently employs various terms to describe forms of CL, including distributed, shared, and collective leadership, resulting in conceptual fragmentation and limiting the comparison of empirical results. Earlier review and scoping attempts were unable to bring together the full body of research on this topic,2,5,6 as they either focus only on a particular aspect of CL or incorporate too few studies to allow meaningful integration. Moreover, scholarly interest in this topic has increased over the past decade,7,8 and substantial but fragmented knowledge has been developed about different CL structures and the conditions under which HATs experience positive team outcomes related to patient care. The lack of appropriate conceptualization, on the one hand, and the fragmentation of results, on the other, hinder not only theoretical advancement but also have far-reaching practical consequences. This limited understanding obstructs the implementation of CL models and associated training for HAT members, and since these teams mostly operate in situations where decisions directly affect patients’ lives, this also hinders efforts to further improve the quality of care delivered.
Our paper seeks to critically address the current understanding of CL in medical settings by conducting a systematic literature review of how CL is conceptualized and operationalized in the context of HATs (Rosenman et al, 2014). After an initial assessment of the selected papers, we formulate four key research questions that shape our analysis and synthesis:
RQ1: What forms of collaborative leadership exist in Healthcare Action Teams?
RQ2: Which team-level mechanisms and behavioral patterns predict effective collaborative leadership within Healthcare Action Teams?
RQ3: What organizational factors influence the successful implementation of collaborative leadership in Healthcare Action Teams?
RQ4: What are the reported effects of collaborative leadership on team members and patient care in Healthcare Action Teams?
By systematically analyzing existing empirical and theoretical literature, this review provides an integrated overview of CL in HATs. Our paper contributes to the literature by (1) clarifying the different forms of CL that occur in these teams and their predictive factors, (2) presenting the current state of research and identifying key gaps, and (3), based on the critical analysis of the findings, outlining a future research agenda to guide studies on leadership in HATs. In doing so, it advances the understanding of leadership behaviors in HATs and contributes not only to theoretical development but also to practical applications, as it offers actionable insights for designing leadership training, structuring team protocols, and shaping organizational policies that support adaptive, high-performing teams in time-critical healthcare environments.
Theoretical Framework
HATs can be defined as multidisciplinary groups that collaborate to deliver time-pressured, critical patient care under dynamic conditions.9 Recent definitions of HATs draw on two key perspectives presented in Edmondson10 and Klein, Ziegert, Knight and Yan11 that emphasize: (1) multidisciplinary as HATs are composed of members with various specialized skills, often from different medical professions; (2) task complexity as HATs are asked to perform in unpredictable, uncertain, and often urgent circumstances that create a high degree of interdependence among HAT members, (3) dynamism as task conditions are often changing and the HAT members have to improvise and coordinate effectively in order to respond to novel and expected task demands, and (4) dual action orientation as during brief performance events, HATs have to provide patient care and at the same time create learning and training opportunities for their less experienced members. These teams function as complex adaptive systems, characterized by emergent behaviors, non-linear interactions, and often diverse communication frameworks in high-uncertain environments.1,12 According to van Rijswijk, Curşeu and van Oortmerssen13 and based on Bunderson and Van der Vegt,14 the effectiveness of such multidisciplinary teams relies on two dimensions that reflect two forms of differentiation that always coexist. On the one hand, horizontal differentiation refers to the distribution of skills and knowledge within the team; on the other hand, vertical differentiation involves hierarchical differences arising from unequal distribution of cognitive resources or information-processing abilities within teams. The interplay between horizontal and vertical differentiation results in task synergetic or relational dissolution processes and, thereby, predicts the process gains and losses that determine team performance. When vertical differentiation is high, team hierarchy arises, hindering cognitive integration processes and limiting the learning opportunities available to the team members, and in line with the subject of this paper, thereby hindering distributed forms of leadership. Instead, more traditional, hierarchy-based forms of leadership take over, and teams do not fully utilize the cognitively diverse resources to promote learning and development of the team members, which is essential for team viability.
In contrast to traditional healthcare teams, HATs often have fluid membership that varies with staffing and expertise needs, and therefore, conventional models of team development grounded in stable team tenure are less applicable. Although HATs are seen as beneficial for patient outcomes, they do not always succeed in addressing the complex challenges of teamwork and leadership associated with these forms, and research has therefore focused on the factors that predict positive team outcomes, such as shared mental models, communication lines, and various leadership structures.15–17
Research indicates that various HATs employ different leadership models, from hierarchical management to more distributed approaches.2,18 While hierarchical leadership offers important advantages, including efficient management and clarity about accountability,6,19 the complexity of medical challenges and the diversity of specialisms involved often also require cross-disciplinary input for effective decision-making. Therefore, scholars have advocated for the adoption of more collaborative and shared leadership approaches that rely on collective influence and more situation-dependent role allocation.7,20 CL is the shared responsibility of setting direction, stimulating alignment, and building commitment among all involved to achieve a common purpose.21,22 Leadership in this form is not the responsibility of one person, but rather a dynamic and interactive process among multiple or all team members, leveraging the benefits of shared mental models and successful coordination to enhance decision quality and team effectiveness. The Complex Adaptive Systems theory (CAS)23 explains why these leadership models can produce significant patient-outcome benefits in HATs, as they strengthen adaptive capacity by supporting distributed decision-making, flexible coordination, and role negotiation. CAS conceptualizes organizations and groups as evolving networks of interrelated agents that adjust to shifting environmental conditions, focusing on adaptability and emergent outcomes over strict hierarchical control. Building on this, the Complexity Leadership Theory (CLT)24 views leadership as an entanglement of adaptive functions. In this view, CL fosters self-organization and creates room for multidisciplinary interactions, including sensemaking and sensegiving processes, that are essential for the integration of diverse expertise.25,26 These processes are particularly important in HATs, where uncertainty, dynamic team composition, and complex medical cases under time pressure require effective shared direction setting.2
Method
The literature review was conducted in September 2025, following the PRISMA reporting guidelines for systematic reviews.27,28 To develop the search strategy, we adapted and expanded the search query used by Janssens, Simon, Beckmann and Marshall2 in their review of shared leadership literature up to 2017. Our query is composed as follows:
(collaborative leader* OR shared leader* OR cooperative leader*) AND (“healthcare team*” OR “action team*” OR “rapid response team*” OR “emergency team*” OR “cardiac arrest” OR “trauma team*” OR “operating room team*” OR “surgical team*” OR “maternity team*” OR “obstetric team*” OR “anaesthesia team*” OR “anesthesia team*” OR “code team*” OR “intensive care team*” OR “clinical team*”).
We searched for studies in titles, abstracts, and keywords, and the preliminary inclusion criteria were limited to those published in English and subject to peer review. The databases that were searched are Web of Science and EBSCOhost (all journal databases selected: MEDLINE, PsycArticles, PsycINFO, LISTA, ERIC, GreenFILE, CINAHL, Psychology & Behavioral Sciences Collection, Business Source Complete, and Academic Search Premier). A PRISMA diagram of the search and selection process is visible in Figure 1.
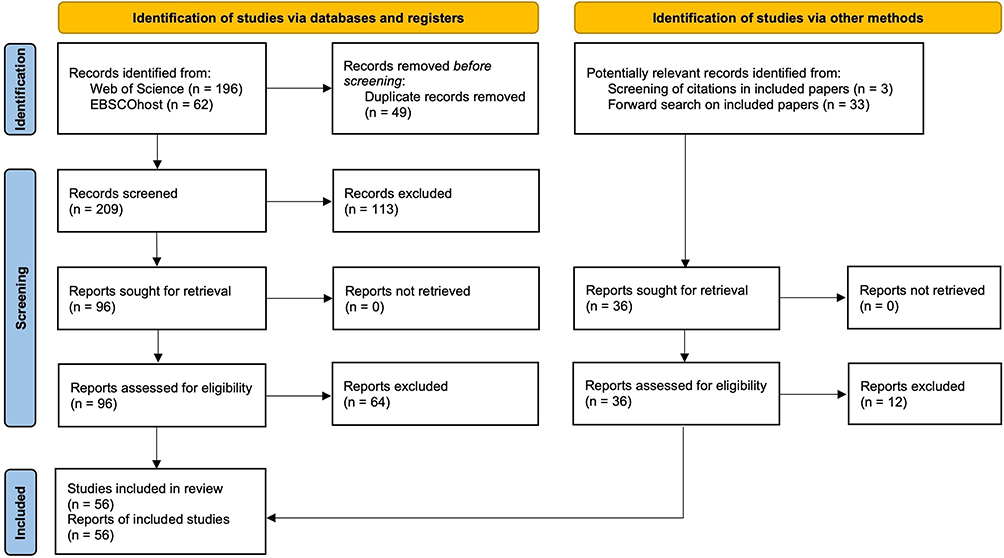 |
Figure 1 PRISMA diagram of the literature search process. Note: Based on the PRISMA 2020 Flow Diagram. From “The PRISMA 2020 statement: An updated guideline for reporting systematic reviews,” by Page et al.27 |
The search query yielded 209 unique records, from which 113 records were excluded in the initial screening step, as it was clear from reading the title and abstract that they did not fall within the scope of this study. As our study focuses on CL related to HATs, we excluded studies that do not meet these two criteria. Therefore, we used the definitions mentioned in the theoretical introduction of this paper, which means, for example, that we only included literature that describes HATs experiencing time-pressured conditions. In the next screening step, the resulting 96 papers were read in depth and re-screened to determine whether they fell within the scope and definitions used in this paper. This process results in 32 papers that are included in our sample. To expand our sample and reduce the risk of inadvertently overlooking relevant literature, we screened the citations of these articles and performed a backward and forward search, resulting in an additional 36 potentially relevant articles, of which 24 were added to the sample after a further selection process. Therefore, our final sample comprises 56 articles.
Results
Description of the Sample
The papers in our sample were published between 2005 and 2025, with the exception of the study by Lomas and Goodall, which was published in 1994. Figure 2 presents the annual distribution of these publications, indicating a growing interest in the topic over the years. Of the 56 papers, 34 were published in the last decade.
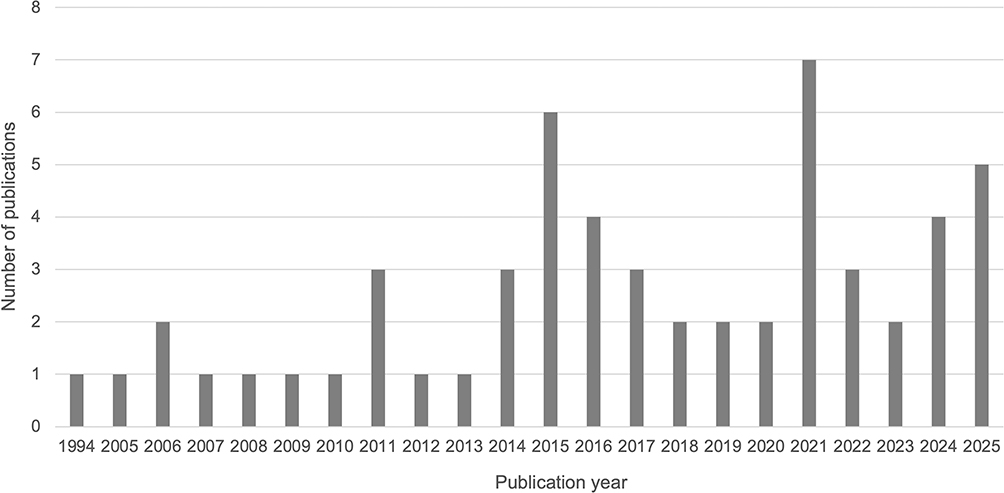 |
Figure 2 Annual distribution of the publications included in the sample. Note: Consistent with the timing of our literature review, the number of publications for the year 2025 is reported up to September. |
Most papers in the sample are published in healthcare-oriented journals. In total, the papers are spread across 46 different journals, suggesting that knowledge on this subject is widely disseminated. Only two journals, BMJ Leader and Journal of Interprofessional Care, have published three papers each on this topic. Table 1 provides a complete overview of the sample, including a summary of the key findings related to CL in HATs.
 |
Table 1 Overview of Included Studies |
The literature on CL in HATs is heterogeneous; therefore, in what follows, we summarize the key themes emerging from our analysis along the four research questions that guided the review. In the subsequent discussion, we attempt an integration of these results using insights from functional perspectives on CL71 and social differentiation in teams literature.13
Theme 1: Forms and Dynamics of Collaborative Leadership
The first research question focuses on identifying the forms of CL that are described in the literature about HATs. The literature uses different terms to refer to CL structures in HATs, ranging from shared, distributed, collaborative, and co-leadership. Overall, studies refer to CL in HATs as fluid, situational, and rotating work arrangements with the aim of initiating, guiding, and adjusting the goal-directed behavior of HATs. In line with the shared leadership model of van Knippenberg, Pearce and van Ginkel,72 the deployment of CL practices in HATs unfolds as a process of dynamic leadership transitions, in which leadership functions are dynamically delegated across team members depending on their expertise and the task requirements. In terms of forms of CL, we can distinguish between authority shifts and dynamic leadership role allocation, a distinction that reflects vertical and horizontal differentiation13 of leadership in HATs. CL as vertical differentiation reflects transitions of authority (vertical differentiation) during task accomplishment, as illustrated by shifting authority depending on the phase of the medical intervention between roles such as the attending surgeon, surgical fellow, and the admitting resident.11 Sarah Janssens presents a particular illustration of CL as vertical differentiation in her work on co-leadership in interprofessional teams in maternity emergencies, in which a clinician and a midwife share leading roles representing medical and midwifery professions.2,15,47 Such clinician-midwife dyads shifted leading roles either in a pre-planned manner or guided by the task requirements imposed by the nature of the emergency and the general composition of the emergency response team.47 CL as horizontal differentiation reflects emergent diffusion of leadership roles among different team members without involving a clear status differentiation between those fulfilling these functions and the rest of the team.3,52,68 Examples of horizontal CL are nurses that share different leadership functions,3 the leadership role constellations as described in Chreim and MacNaughton,17 the emergent distribution of leadership functions across various team members,20,58 leaders that encourage and empower members to participate in medical decisions68 and, the sharing of leading roles among nurses and residents in anesthesia teams.49 CL as vertical differentiation captures how authority migrates across medical personnel positioned at different hierarchical levels while maintaining formal rank awareness,11,18,63 while CL as horizontal differentiation describes how various leadership functions are enacted across peers or team members of comparable standing or hierarchical position.49,58
Theme 2: Team-Level Mechanisms
The second research question focuses on identifying the team-level mechanisms and behavioral patterns that predict effective CL within HATs. Several studies explored the mechanisms that explain the effects of CL on outcomes (team performance, patient safety, and well-being), and the results can be clustered in enablers of team performance (enhanced adaptability, shared mental models, increased cohesion, and psychological safety) and constraining mechanisms (diffused responsibility, role conflict, communication saturation) that reduce performance and patient safety. On the one hand, studies show that CL fosters the emergence of shared mental models, as team members are better able to develop a common understanding of goals roles and responsibilities, leading to improved coordination,16 the emergence of trust and psychological safety,19,37 the emergence of effective communication loops to share expertise and effectively use skills,33,45 as well as the emergence of cognitive integration and learning.7,25,30,46 On the other hand, some of the studies show that CL can blur accountability and generate role ambiguity and coordination overload,17,52 lead to conflicting mental models and goal misalignment among members or subgroups,18,31 activate professional identities that generate power imbalance and resistance.46,52,69 Overall, these two types of mechanisms activated by CL also align with the horizontal and vertical differentiation within HATs, as cognitive integration, psychological safety, and process gains are typical consequences of horizontal differentiation, while role ambiguity, process losses (social loafing, communication saturation), and conflict are typical consequences of vertical differentiation in teams.13
Theme 3: Organizational and Contextual Influences
The third research question focuses on what organizational factors influence the successful implementation of CL in HATs. Studies extensively show that successful CL implementation needs management endorsement and organizational support in the form of training and protected reflection time.37,38 In addition, professional identities often activate interpersonal boundaries and maintain hierarchical cultures that constrain the implementation of CL in HATs.31,69 Contextual influences are also dualistic in that some organizational features, such as institutionalized dyads47 and clearly defined rotating leadership protocols,7 act as structural enablers of CL, while some organizational features, such as formal authority and hierarchical cultural norms,31,54,69 training deficits,9 and macro systemic pressures, are factors that constrain the successful implementation of CL in HATs. CL often falters in HATs not because of individual or team-level constraints, but due to organizational and contextual misalignment that is generated by rigid hierarchies, risk-averse medical cultures, or disciplinary silos. Under such circumstances, CL reverts to positional and hierarchical control, and the potential benefits of collaboration remain unrealized.
Theme 4: Outcomes and Performance Effects of CL
The last research question focuses on the effects of CL on team members and patient care in HATs, and in Table 1, we cluster the studies in three categories depending on the general influence of CL on team outcomes. The vast majority of the studies included in our systematic literature review (N=36) reveal positive outcomes associated with CL on team processes as well as patient safety. CL arrangements enhance communication, situational awareness, and psychological safety, which in turn improve HATs’ effectiveness. The beneficial effects of CL are supported by clear role structures, the emergence of accurate shared mental models, and the emergence of mutual trust among different medical professionals. A second category of studies (N=6) emphasizes the detrimental effects of CL as a consequence of role ambiguity and overload. Especially under high task complexity, the ambiguous authority boundaries associated with CL lead to slower decision-making, while rigid professional hierarchies spur resistance and foster coordination failures leading to suboptimal team outcomes. A third category of studies reveals a context-dependent pattern for the effects of CL on team outcomes. This last category is particularly important, as it points out contingencies that shape the effectiveness of CL implementation in HATs. Taken together, these findings suggest that while CL can enhance the operational capacity of HATs, its effectiveness is contingent on organizational, contextual, and task-related variables as well as on the quality of interpersonal relations, the professional identities and boundaries, and the organizational climate. Table 2 presents an integrative overview of the most important moderating factors that qualify the outcomes associated with CL.
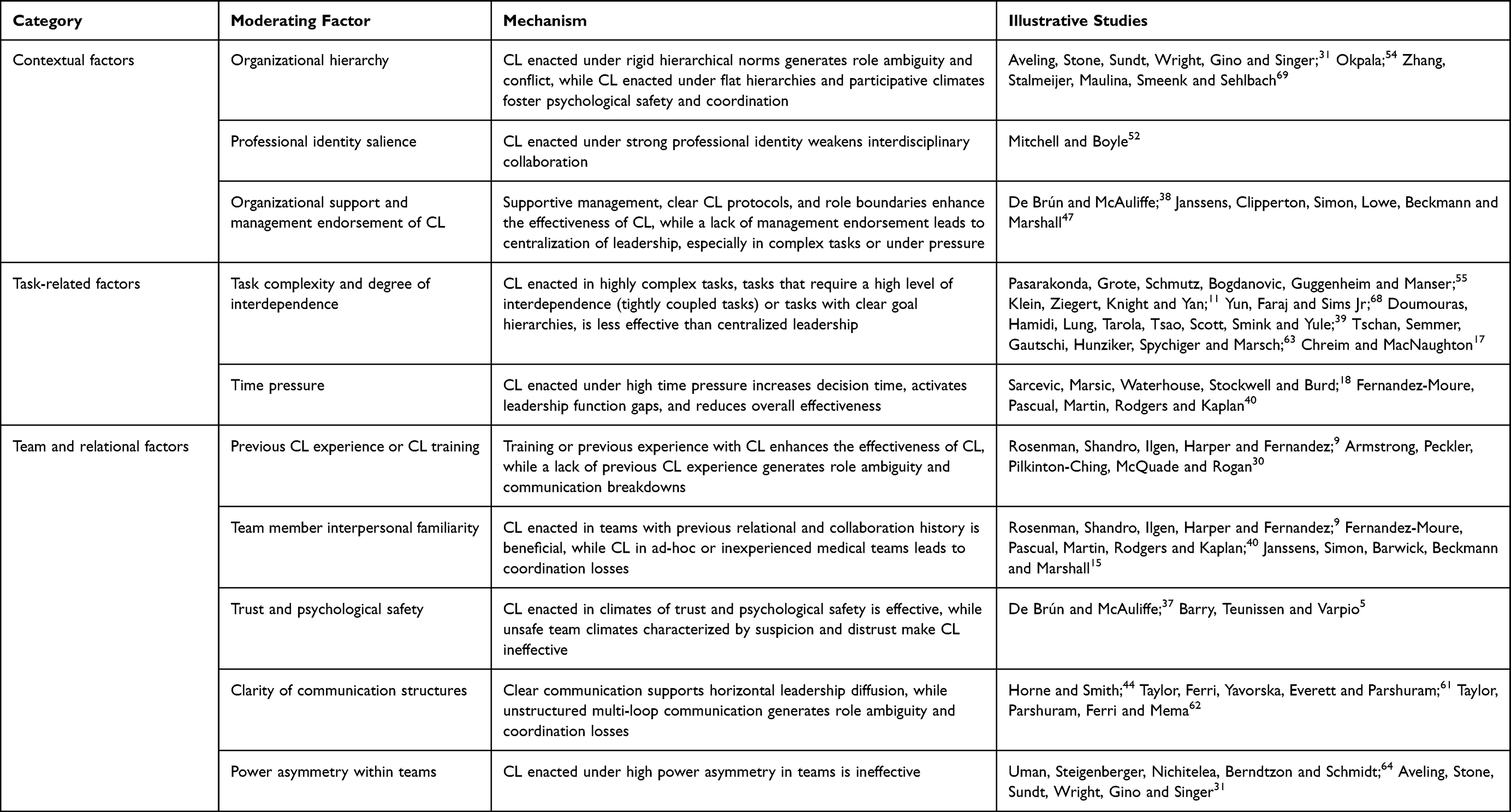 |
Table 2 An Overview of the Moderating Factors That Influence CL Effectiveness |
Discussion and Integration
Our analyses reveal three key problematic areas related to the literature on CL in HATs. First, although the terms collaborative and shared leadership are extensively used and broadly accepted, the idiosyncratic approaches make it difficult to draw generic conclusions on the theoretical grounding of CL in HATs. Second, although the formal definition of HATs include key elements of multidisciplinarity, task complexity, dynamism, and a dual task focus, our literature search not only revealed an inconsistent use of the term HAT, yet, more importantly, some strands of research on action teams that do fit the four definitional criteria, were not included, such as research on ambulance crews,73 basically because either the term “team” or “leadership” were not identified in our initial systematic search. Third, although most of the studies we included in the review discuss a variety of team outcomes, it is unclear how team effectiveness criteria were selected and used, as in some of the studies, emergent states, such as trust and psychological safety, or processes, such as coordination effectiveness, were (implicitly) used as indicators of team effectiveness. We build on established conceptualizations of team effectiveness as a multifaceted construct74 to argue that for HATs, effectiveness should include assessments of: (1) patient outcomes (symptom burden, relapse, patient well-being), (2) team members’ attitudes (satisfaction, commitment), and (3) team viability (team members’ capacity to perform effectively in the future, including the training of less experienced members). In what follows, we address these three critical points by building on theoretical models from team research and collaborative leadership to provide integrative insights aimed at opening future research venues.
In order to bring more theoretical clarity to CL research, we argue that, besides focusing on formal roles only, CL in HATs should be conceptualized as fluid transitions of leadership functions among professionals composing the HAT, either among members with the same status or involving different (professional) hierarchies. As illustrated in the integrative presentation of results, the conceptual fragmentation of the CL in HATs literature can be unified around the functional perspective on CL as presented in Curşeu and Schruijer.71 Integrating previous analyses of CL in interorganizational relations, Curşeu and Schruijer71 distinguish four key functions of CL, namely: activating resource assistance, framing the collaborative task environment, mobilizing stakeholder support, and synthesizing the collaborative process. These key CL functions are important for addressing the complexity and dynamism of tasks performed by HATs. Based on this functional approach, we adapted the definition of CL in HATs as a dynamic, situational, and functionally distributed process of shared influence through which members activate relevant task resources, frame collaborative processes, mobilize support, and collectively guide, coordinate, and align their actions towards patient care goals. As we argued in the previous section, CL in HATs has a dual conceptualization as authority shifts subsequent to varying task demands and situational characteristics and as a horizontal diffusion of leadership functions leading to an emergent transition of enacted leadership roles among peers. Both conceptualizations of CL can be formulated and assessed in the functional approach of CL.71
We also call for a more inclusive use of the term HATs to broaden its scope and include other settings that satisfy the definitional criteria presented here, yet where the term “ team” may not be deployed. Think of those groups consisting of members that work across organizational boundaries and where members may not be co-located or even working simultaneously (think of all parties that are involved in ambulance work, that may include healthcare organizations and the police). HATs are multidisciplinary; they perform complex tasks in dynamic environments and have a dual action focus on providing patient care and training opportunities for their members. In addition, HATs also have highly specialized role prescriptions and action protocols to guide the (inter)actions of their members.75 When also focusing on boundary-crossing interorganizational work in health care, one can widen the scope and thus learn more about CL.
As mentioned, a functional perspective on CL provides a clearer conceptual lens for analyzing how HATs perform under such complex circumstances. Shifting decision authority based on task demands can activate relevant resources that are required to make accurate diagnostic or medical intervention decisions, such as shifting decision discretion in various stages from emergency, anesthesia, to surgical staff.60 Similarly, radiographers can temporarily assume leadership authority during trauma imaging sequences, bringing relevant knowledge for accurate diagnosis, with physicians and nurses adopting supportive roles.7 CL transitions can therefore activate expertise and latent resources embedded in different professional groups at similar hierarchical levels as the dynamic task delegation during surgery or resuscitation.11,63 Moreover, in terms of framing the collaborative task environment, authority transfer in vertically differentiated teams can clarify the diagnostic and procedural requirements specific to each medical phase and accurately frame the evolving medical task environments. In terms of stakeholder support, vertical CL shifts can signal role boundaries and, based on shared recognition of competence, professional norms, and medical protocols, can mobilize trust and compliance that is necessary for coordinated action in HATs.5,37 When managed effectively, vertical leadership transitions can integrate expertise situated at higher hierarchical levels and promote systemic cohesion and functional integrity30,69 in line with the medical protocols and evolving task demands.
Horizontal CL, seen as a lateral diffusion and rotation of leadership functions among peers of comparable hierarchical standing, can activate diverse types of skills distributed across professional boundaries and enhance the pool of knowledge and expertise available to the team.3 Horizontal transitions also create an environment in which shared sensemaking can emerge, and where HAT members can engage in a collective negotiation of roles and objectives that are required when working on a collaborative task.33 Horizontal leadership transitions create valuable learning opportunities, therefore helping HATs to achieve their second focus, namely, to provide training and learning opportunities for their members. In light of these observations, we call for a more integrative approach to assess the effectiveness of HATs as a multifaceted construct that includes (1) patient outcomes, (2) team member attitudes, and (3) team viability as reflected by the opportunities to train the less experienced team members. Horizontal CL can boost member satisfaction and foster the learning and professional development of team members.
As illustrated in the studies that reported detrimental effects of CL or those that revealed mixed or ambiguous effects, a variety of organizational, task, and team contextual variables nuance the effects of CL for HAT outcomes. Drawing on prior work on the interplay of horizontal and vertical differentiation in teams,13,14 we argue that when both forms of differentiation co-exist in HATs, the positive effects of CL on member satisfaction and learning opportunities are attenuated. We propose to integrate the contingencies reported in the studies included in our review by differentiating those that are likely to enhance the vertical differentiation from those that are expected to reduce the vertical differentiation. Situations that enhance the vertical differentiation in HATs are expected to reduce the beneficial effects of CL on team effectiveness as a multidimensional construct (patient outcomes, team member attitudes, and team viability). Such situations include rigid organizational hierarchies and culture,31,54,69 high levels of professional identity salience and rigid professional boundaries,52 goal hierarchy associated with highly complex tasks,11,55,68 as well as a pre-existing power asymmetry within the team.31,64 Situations that are expected to reduce the vertical differentiation in HATs include: leadership training and exposure to CL best practices,9,30 organizational support and a strong management endorsement of CL,38,47 interpersonal familiarity of the members composing the HAT,15,57 clarity of communication structures,31,61,62,64 awareness of task interdependence and previous collaborative experience.39,63 All in all, it is our contention that CL in HATs is beneficial, especially for member satisfaction and team viability when the degree of vertical differentiation in HATs is low rather than high.
Theoretical Implications and Future Research Directions
Our review aimed to reconcile the conceptual fragmentation in the literature. It positions CL in HATs as a functionally distributed and dynamically co-evolving system that harmonizes procedural prescriptions and formal protocols with social influence processes in changing task environments to support team effectiveness. The latter is reflected by three key indicators, namely patient outcomes, team member satisfaction, and team viability. We subsequently propose to build on a structural, functional, and dynamic perspective on leadership in teams to make four important contributions to the literature.
We frame CL in HATs not as structural and static, but as a functional and dynamic system of social influence that adapts and changes in function of task demands and the needs of the HAT. In this perspective, CL reflects how the four key leadership functions (activating resources, framing the task environment, mobilizing support, and synthesizing the collaborative processes) are dynamically allocated across members depending on their expertise and professional background in relation to the task requirements. Such a functional and dynamic approach to leadership allows for a better understanding of leadership supportive behaviors required during transition processes (leadership behaviors that support planning and task organization) as well as during action processes (leadership behaviors that enable coordination and monitoring the progress towards goal accomplishment).9 In this perspective, CL is a core integration mechanism in HATs that allows them to adapt effectively to changing task demands. Future studies could adopt longitudinal and event-based designs to capture how these four key functions of CL shift over time, following different task completion stages in HATs. We also call for research that explores the functions of CL in different HAT setups, such as inter- versus intra-organizational, co-located versus virtual, or emergency versus non-emergency medical settings. Drawing on the call from van Knippenberg, Pearce and van Ginkel72 for temporal co-evolution models of leadership in teams, researchers could use experience-sampling methods or behavioral coding of medical teams interacting in real time to trace how vertical and horizontal CL patterns alternate in response to evolving clinical challenges. Moreover, building on the functional framework of CL and the scale validated in Curşeu and Schruijer,71 future research could adapt the instrument for the context of HATs and develop new observational measures for the key functions of CL in medical teams.
Second, based on the co-evolution of vertical and horizontal leadership in teams72 and the distinction between horizontal and vertical social differentiation in teams,13 we explain how vertical authority shifts and horizontal leadership role diffusion jointly impact team processes, emergent states, and ultimately performance. We argue that vertical CL transitions serve to activate resources needed to perform different phases of the medical tasks and frame the collaboration process by redistributing decision-making authority according to phase-specific demands. Horizontal CL serves to mobilize support and synthesize collaborative process functions by promoting trust, interprofessional learning, and reflexive communication practices that allow HATs to adapt dynamically to the varying task demands. Future research could explore in multilevel designs the contingencies (hierarchical norms, interpersonal familiarity, task complexity, time pressure, previous CL training, and experience) that impact the effectiveness of vertical and horizontal CL and test the non-linear and phase-contingent effects of CL on team outcomes.
Third, building on van Knippenberg, Pearce and van Ginkel,72 we position CL as a coevolutionary process unfolding in HATs. Our review suggests a context-dependent effect of CL, such that vertical authority shifts and horizontal diffusion of CL functions can alternate as a function of contextual and task influences. Synergic co-evolution is reflected by a functional alignment of vertical and horizontal CL in line with the task and contextual demands, while functional misalignment (unclear roles, unclear collaborative task framing) can reduce the effectiveness of vertical-horizontal integration, produce process losses, and ultimately reduce the effectiveness of HATs. Future experimental studies using simulations could further explore the interplay of vertical–horizontal forms of CL as they shape team dynamics and outcomes in various types of tasks, bringing causal tractability to the claims relating CL to medical team dynamics and outcomes.
Finally, our review integrates social differentiation with functional leadership approaches within a multilevel framework of CL effectiveness. We identify individual-level enablers (leadership competence and readiness), team-level mechanisms (communication structures, interpersonal familiarity, shared cognition), as well as organizational and contextual variables (hierarchical flexibility, managerial endorsement) that impact the effectiveness of CL in HATs. Future studies could use multilevel modeling to explore the cross-level interactions between these moderating factors and further clarify the relative importance of various contingencies that impact the effectiveness of CL.
Limitations
Besides its contributions, our systematic literature review also has limitations. First, in order to ensure a focus on high-quality empirical evidence, we have selected and analyzed peer-reviewed publications indexed in major databases, and we did not include studies published in languages other than English. This may have inadvertently excluded relevant literature. Second, although we have used a comprehensive and expanded search query, it remains possible that relevant studies addressing collaborative leadership aspects in HATs were not captured in the initial search because they used alternative terminology (such as crews, supervision, crisis management) or because they did not label leadership as a key investigated concept. Third, the literature summarized in our review is highly heterogeneous in terms of study designs, analytical approaches, and operationalizations of both CL and team effectiveness. Such methodological and conceptual heterogeneity limits the comparability of findings across studies and constrains the strength of cumulative inferences that can be drawn. Finally, a considerable proportion of the empirical evidence synthesized in our review is derived from simulation-based studies, retrospective analyses, or self-reports rather than systematic observations of collaborative leadership dynamics in naturalistic healthcare settings. In an attempt to provide actionable insights to practitioners, we used a functional approach to collaborative leadership to integrate these findings, yet the ecological validity and generalizability of our findings to clinical practice may be limited.
Practical Implications
Our functional lens on CL offers guidance for healthcare organizations to improve the effectiveness of HATs. We call for an integrative, multifaceted assessment of the effectiveness of HATs, including indicators related to patient outcomes (symptom burden, relapse, patient well-being), team members’ attitudes (satisfaction, commitment), as well as viability (capacity of performing effectively in the future, as also captured by training and learning opportunities offered to the team members). First, we propose to (re)design leadership training programs so as to reflect the dynamic and situational nature of CL. For example, simulation-based training that alternates leadership roles between nurses, residents, and attending physicians11,30,47 can foster adaptive delegation and prepare team members for vertical and horizontal leadership transitions. We suggest that such training explicitly targets the four leadership functions that we discussed in this review. Second, we advise that organizational protocols that are applicable to HATs, incorporate such dynamic CL structures. Maternity HATs that institutionalize clinician–midwife co-leadership47 illustrate how predefined dyads can reduce ambiguity and enhance coordination. Such dyad structures could also be applied in trauma or resuscitation teams, ensuring that leadership transitions are guided by task demands rather than rigid formal hierarchies. Third, management endorsement and structural support are essential. Time for team reflection, as for instance implemented in the Co-Lead intervention,38 enables teams to develop shared mental models and clarify role boundaries. This is particularly relevant in ad hoc HATs, where interpersonal familiarity is low and therefore coordination losses are more likely to occur. Fourth, communication protocols are to be adapted to support CL. Studies show that multi-loop communication without a clear structure61,62 undermines horizontal CL. Implementing structured briefing formats and assigning event managers to coordinate communication can mitigate these risks and enhance clarity during critical interventions. Finally, an effective CL adoption depends on reducing task-inappropriate vertical differentiation. This can be achieved by flattening hierarchical norms, promoting interprofessional respect, and aligning leadership roles with expertise rather than rank. In sum, HATs should move beyond static and traditional leadership models in order to adopt flexible, functionally distributed leadership structures tailored to the dynamic realities of HATs.
Conclusions
This review integrates fragmented empirical evidence on CL in HATs and conceptualizes it as a dynamic, functionally distributed system of social influence that supports adaptive coordination in high-pressure clinical settings. We build on the functional approach to CL71 to argue that CL fulfills four interrelated functions: activating resources, framing the task environment, mobilizing support, and synthesizing collaboration. We also use insights on horizontal–vertical differentiation13,72 to distinguish between vertical CL (authority shifts across hierarchies and professional boundaries) and horizontal CL (leadership diffusion among peers), whose balance shapes medical team adaptability. CL enhances the quality of intrateam communication, trust, and psychological safety when hierarchies are flexible, professional boundaries are permeable, and a shared understanding is present, yet it can be detrimental to team performance under rigid hierarchical structures, role ambiguity, and high task complexity. Overall, CL emerges as a context-sensitive integrative capability in HATs with the potential to impact adaptation as well as learning and effectiveness, with important consequences for the quality of medical outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnson JD. Framing communication in health care action teams. Int J Healthc Manage. 2019;12(1):68–74. doi:10.1080/20479700.2017.1398386
2. Janssens S, Simon R, Beckmann M, Marshall S. Shared leadership in healthcare action teams: a systematic review. J Patient Safety. 2021;17(8):e1441–e1451. doi:10.1097/pts.0000000000000503
3. Abdelwahab Ibrahim El-Sayed A, Shaheen RS, Farghaly Abdelaliem SM. Collaborative leadership and productive work performance: the mediating role of nurses’ innovative behavior. Int Nurs Rev. 2024;71(4):868–878. doi:10.1111/inr.12934
4. Wang D, Waldman DA, Zhang Z. A meta-analysis of shared leadership and team effectiveness. J Appl Psychol. 2014;99(2):181–198. doi:10.1037/a0034531
5. Barry ES, Teunissen P, Varpio L. Followership in interprofessional healthcare teams: a state-of-the-art narrative review. BMJ Leader. 2024;8(2):127–133. doi:10.1136/leader-2023-000773
6. Courtenay M, Nancarrow S, Dawson D. Interprofessional teamwork in the trauma setting: a scoping review. Human Res Health. 2013;11(1):57. doi:10.1186/1478-4491-11-57
7. Bäckström M, Engström Å, Lundvall LL, Leijon-Sundqvist K, Jonsson K. Unspoken synergy: team interdependence with radiographers in trauma alerts: an interview and observational study of trauma teams. Radiography. 2025;31(5):103097. doi:10.1016/j.radi.2025.103097
8. Janssens S, Simon R, Barwick S, Clipperton S, Beckmann M, Marshall S. Midwifery leadership in maternity emergencies: a video analysis. J Interprof Care. 2025;39(4):567–573. doi:10.1080/13561820.2019.1675611
9. Rosenman ED, Shandro JR, Ilgen JS, Harper AL, Fernandez R. Leadership training in health care action teams: a systematic review. Acad Med. 2014;89(9):1295–1306. doi:10.1097/acm.0000000000000413
10. Edmondson AC. Speaking up in the operating room: how team leaders promote learning in interdisciplinary action teams. J Manage Studies. 2003;40(6):1419–1452. doi:10.1111/1467-6486.00386
11. Klein KJ, Ziegert JC, Knight AP, Yan X. Dynamic delegation: shared, hierarchical, and deindividualized leadership in extreme action teams. Adm Sci Q. 2006;51(4):590–621. doi:10.2189/asqu.51.4.590
12. Plsek PE, Greenhalgh T. Complexity science: the challenge of complexity in health care. BMJ. 2001;323(7313):625–628. doi:10.1136/bmj.323.7313.625
13. van Rijswijk J, Curşeu PL, van Oortmerssen LA. Cognitive and neurodiversity in groups: a systemic and integrative review. Small Group Res. 2024;55(1):44–88. doi:10.1177/10464964231213564
14. Bunderson JS, Van der Vegt GS. Diversity and inequality in management teams: a review and integration of research on vertical and horizontal member differences. Annual Rev Organ Psychol Organ Behav. 2018;5(47):47–73. doi:10.1146/annurev-orgpsych-032117-104500
15. Janssens S, Simon R, Barwick S, Beckmann M, Marshall S. Leadership sharing in maternity emergency teams: a retrospective cohort study in simulation. BMJ Simul Technol Enhanced Learn. 2020;6(3):135–139. doi:10.1136/bmjstel-2018-000409
16. Aufegger L, Shariq O, Bicknell C, Ashrafian H, Darzi A. Can shared leadership enhance clinical team management? A systematic review. Leadersh Health Serv. 2019;32(2):309–335. doi:10.1108/lhs-06-2018-0033
17. Chreim S, MacNaughton K. Distributed leadership in health care teams: constellation role distribution and leadership practices. Health Care Manag Rev. 2016;41(3). doi:10.1097/HMR.0000000000000073
18. Sarcevic A, Marsic I, Waterhouse LJ, Stockwell DC, Burd RS. Leadership structures in emergency care settings: a study of two trauma centers. Int J Med Inform. 2011;80(4):227–238. doi:10.1016/j.ijmedinf.2011.01.004
19. Sims S, Hewitt G, Harris R. Evidence of a shared purpose, critical reflection, innovation and leadership in interprofessional healthcare teams: a realist synthesis. J Interprof Care. 2015;29(3):209–215. doi:10.3109/13561820.2014.941459
20. Kida R, Fujitani K, Matsushita H. Impact of collaborative leadership, workplace social capital, and interprofessional collaboration practice on patient safety climate. J Healthcare Qual. 2024;46(5):268–275. doi:10.1097/jhq.0000000000000443
21. Drath WH, McCauley CD, Palus CJ, Van Velsor E, O’Connor PMG, McGuire JB. Direction, alignment, commitment: toward a more integrative ontology of leadership. Leadersh Q. 2008;19(6):635–653. doi:10.1016/j.leaqua.2008.09.003
22. Browning HW, Torain DJ, Patterson TE. Collaborative healthcare leadership: a six-part model for adapting and thriving during a time of transformative change; 2011.
23. Lansing JS. Complex Adaptive Systems. Annu Rev Anthropol. 2003;32:183–204. doi:10.1146/annurev.anthro.32.061002.093440
24. Uhl-Bien M, Marion R, McKelvey B. Complexity leadership theory: shifting leadership from the industrial age to the knowledge era. Leadersh Q. 2007;18(4):298–318. doi:10.1016/j.leaqua.2007.04.002
25. Faraj S, Xiao Y. Coordination in fast-response organizations. Manage Sci. 2006;52(8):1155–1169. doi:10.1287/mnsc.1060.0526
26. Kramer MW. Sensemaking. In: The International Encyclopedia of Organizational Communication. 2016:1–10.
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88. doi:10.1016/j.ijsu.2021.105906
28. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34. doi:10.1016/j.jclinepi.2009.06.006
29. Amacher SA, Schumacher C, Legeret C, et al. Influence of gender on the performance of cardiopulmonary rescue teams: a randomized, prospective simulator study. Crit Care Med. 2017;45(7):1184–1191. doi:10.1097/CCM.0000000000002375
30. Armstrong P, Peckler B, Pilkinton-Ching J, McQuade D, Rogan A. Effect of simulation training on nurse leadership in a shared leadership model for cardiopulmonary resuscitation in the emergency department. Emerg Med Australasia. 2021;33(2):255–261. doi:10.1111/1742-6723.13605
31. Aveling E-L, Stone J, Sundt T, Wright C, Gino F, Singer S. Factors influencing team behaviors in surgery: a qualitative study to inform teamwork interventions. Ann Thorac Surg. 2018;106(1):115–120. doi:10.1016/j.athoracsur.2017.12.045
32. Bouchez T, Cagnon C, Hamouche G, Majdoub M, Charlet J, Schuers M. Interprofessional clinical decision-making process in health: a scoping review. J Adv Nurs. 2024;80(3):884–907. doi:10.1111/jan.15865
33. Brandstorp H, Kirkengen AL, Sterud B, Haugland B, Halvorsen PA. Leadership practice as interaction in primary care emergency team training. Action Res. 2015;13(1):84–101. doi:10.1177/1476750314566660
34. Brewster DJ, Butt WW, Gordon LJ, Sarkar MA, Begley JL, Rees CE. Leadership during airway management in the intensive care unit: a video-reflexive ethnography study. Front Med. 2023;10. doi:10.3389/fmed.2023.1043041.
35. Cassidy DJ, Jogerst K, Coe T, et al. Simulation versus reality: what can interprofessional simulation teach us about team dynamics in the trauma bay? Global Surg Educ. 2022;1(1):56. doi:10.1007/s44186-022-00063-8
36. Clements A, Curtis K, Horvat L, Shaban RZ. The effect of a nurse team leader on communication and leadership in major trauma resuscitations. Int Emerg Nurs. 2015;23(1):3–7. doi:10.1016/j.ienj.2014.04.004
37. De Brún A, McAuliffe E. Identifying the context, mechanisms and outcomes underlying collective leadership in teams: building a realist programme theory. BMC Health Serv Res. 2020;20(1):261. doi:10.1186/s12913-020-05129-1
38. De Brún A, McAuliffe E. “When there’s collective leadership, there’s the power to make changes”: a realist evaluation of a collective leadership intervention (Co-Lead) in healthcare teams. J Leadership Organ Stud. 2023;30(2):155–172. doi:10.1177/15480518221144895
39. Doumouras AG, Hamidi M, Lung K, et al. Non-technical skills of surgeons and anaesthetists in simulated operating theatre crises. Br J Surg. 2017;104(8):1028–1036. doi:10.1002/bjs.10526
40. Fernandez-Moure J, Pascual JL, Martin ND, Rodgers H, Kaplan LJ. Emergency response teams in and outside of medicine—Structurally crafted to be worlds apart. J Trauma Acute Care Surg. 2019;86(1):134–140. doi:10.1097/ta.0000000000002073
41. Geyer R, Kilgore J, Chow S, Grant C, Gibson A, Rice M. Core team members’ impact on outcomes and process improvement in the initial resuscitation of trauma patients. J Trauma Nurs. 2016;23(2). doi:10.1097/JTN.0000000000000191
42. Gosman GG, Baldisseri MR, Stein KL, et al. Introduction of an obstetric-specific medical emergency team for obstetric crises: implementation and experience. Am J Clin Exp Obstet Gynecol. 2008;198(4). doi:10.1016/j.ajog.2007.06.072
43. Guerra S, Lambe K, Manolova G, Sadler E, Sheehan KJ. Multidisciplinary team healthcare professionals’ perceptions of current and optimal acute rehabilitation, a Hip fracture example A UK qualitative interview study informed by the theoretical domains framework. PLoS One. 2022;17(11). doi:10.1371/journal.pone.0277986
44. Horne S, Smith J. Preparation of the trauma response in a UK emergency department. Trauma. 2015;17(4):250–257. doi:10.1177/1460408615572364
45. Jacobsson M, Hargestam M, Hultin M, Brulin C. Flexible knowledge repertoires: communication by leaders in trauma teams. Scand J Trauma Resusc Emerg Med. 2012;20(1):44. doi:10.1186/1757-7241-20-44
46. James S, Subedi P, Indrasena BSH, Aylott J. Review DebrIeF: a collaborative distributed leadership approach to “hot debrief” after cardiac arrest in the emergency department: a quality improvement project. Leadersh Health Serv. 2022;35(3):390–408. doi:10.1108/lhs-06-2021-0050
47. Janssens S, Clipperton S, Simon R, Lowe B, Beckmann M, Marshall S. Clinicians’ attitudes towards a co-leadership structure for maternity emergency teams: an interview study. J Interprof Care. 2025;39(4):636–644. doi:10.1080/13561820.2022.2070607
48. Kress T, Tasota FJ, Broge-Connor M, Jackson J. Preparing nurses to respond to in-house emergencies as a team. Nursing2016. 2016;46(10):15–19. doi:10.1097/01.Nurse.0000490223.07427.38
49. Künzle B, Zala-Mezö E, Wacker J, Kolbe M, Spahn DR, Grote G. Leadership in anaesthesia teams: the most effective leadership is shared. Qual Saf Health Care. 2010;19(6):e46–e46. doi:10.1136/qshc.2008.030262
50. Leary M. In-hospital cardiac arrest. Nurs Crit Care. 2015;10(1):34–40. doi:10.1097/01.Ccn.0000457311.26630.38
51. Lomas GA, Goodall O. Trauma teams vs non-trauma teams. Accident Emerg Nurs. 1994;2(4):205–210. doi:10.1016/0965-2302(94)90024-8
52. Mitchell R, Boyle B. Too many cooks in the kitchen? The contingent curvilinear effect of shared leadership on multidisciplinary healthcare team innovation. Human Re Manag J. 2021;31(1):358–374. doi:10.1111/1748-8583.12309
53. Muller-Juge V, Cullati S, Blondon KS, et al. Interprofessional collaboration between residents and nurses in general internal medicine: a qualitative study on behaviours enhancing teamwork quality. PLoS One. 2014;9(4). doi:10.1371/journal.pone.0096160
54. Okpala P. Addressing power dynamics in interprofessional health care teams. Int J Healthc Manage. 2021;14(4):1326–1332. doi:10.1080/20479700.2020.1758894
55. Pasarakonda S, Grote G, Schmutz JB, Bogdanovic J, Guggenheim M, Manser T. A strategic core role perspective on team coordination: benefits of centralized leadership for managing task complexity in the operating room. Human Factors. 2021;63(5):910–925. doi:10.1177/0018720820906041
56. Reyes DL, Bisbey T, Day D, Salas E. Translating 6 key insights from research on leadership and management in times of crisis. BMJ Leader. 2021. doi:10.1136/leader-2020-000349
57. Rosen MA, DiazGranados D, Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychologist. 2018;73(4):433–450. doi:10.1037/amp0000298
58. Sadideen H, Weldon S-M, Saadeddin M, Loon M, Kneebone R. A video analysis of intra- and interprofessional leadership behaviors within “the burns suite”: identifying key leadership models. J Surg Educ. 2016;73(1):31–39. doi:10.1016/j.jsurg.2015.09.011
59. Streiff S, Tschan F, Hunziker S, et al. Leadership in medical emergencies depends on gender and personality. Simul Healthcare. 2011;6(2). doi:10.1097/SIH.0B013E318209382B
60. Tai NRM, Russell R. Right turn resuscitation: frequently asked questions. J Royal Army Med Corps. 2011;157(Suppl 3):S310. doi:10.1136/jramc-157-03s-10
61. Taylor KL, Ferri S, Yavorska T, Everett T, Parshuram C. A description of communication patterns during CPR in ICU. Resuscitation. 2014;85(10):1342–1347. doi:10.1016/j.resuscitation.2014.06.027
62. Taylor KL, Parshuram CS, Ferri S, Mema B. A description of the “event manager” role in resuscitations: a qualitative study of interviews and focus groups of resuscitation participants. J Crit Care. 2017;39:254–258. doi:10.1016/j.jcrc.2016.12.015
63. Tschan F, Semmer NK, Gautschi D, Hunziker P, Spychiger M, Marsch SU. Leading to recovery: group performance and coordinative activities in medical emergency driven groups. Human Perform. 2006;19(3):277–304. doi:10.1207/s15327043hup1903_5
64. Uman T, Steigenberger N, Nichitelea D, Berndtzon M, Schmidt M. A configurational approach to the relationship between ethnic diversity, leadership, and performance in health care teams. Health Care Manag Rev. 2025;50(4):285–295. doi:10.1097/hmr.0000000000000451
65. Varpio L, Teunissen P. Leadership in interprofessional healthcare teams: empowering knotworking with followership. Med Teach. 2021;43(1):32–37. doi:10.1080/0142159X.2020.1791318
66. Wallin C-J, Meurling L, Hedman L, Hedegård J, Felländer-Tsai L. Target-focused medical emergency team training using a human patient simulator: effects on behaviour and attitude. Medical Education. 2007;41(2):173–180. doi:10.1111/j.1365-2929.2006.02670.x
67. Wurster LA, Coffey C, Haley K, Covert J. The role of the trauma nurse leader in a pediatric trauma center. J Trauma Nurs. 2009;16(3). doi:10.1097/JTN.0B013E3181B9E0CA
68. Yun S, Faraj S, Sims HP Jr. Contingent leadership and effectiveness of trauma resuscitation teams. J Appl Psychol. 2005;90(6):1288. doi:10.1037/0021-9010.90.6.1288
69. Zhang G, Stalmeijer RE, Maulina F, Smeenk FWJM, Sehlbach C. Interprofessional collaboration in primary care for patients with chronic illness: a scoping review mapping leadership and followership. BMJ Leader. 2025;9(2):131–139. doi:10.1136/leader-2024-001102
70. Zhuravsky L. Crisis leadership in an acute clinical setting: Christchurch hospital, New Zealand ICU experience following the February 2011 earthquake. Prehospital Disaster Med. 2015;30(2):131–136. doi:10.1017/S1049023X15000059
71. Curşeu PL, Schruijer SGL. Leading without position power: preliminary validation of the multiparty collaborative leadership scale (MCLS). Int J Conflict Manag. 2024;35(2):411–426. doi:10.1108/IJCMA-01-2023-0014
72. van Knippenberg D, Pearce CL, van Ginkel WP. Shared leadership – vertical leadership dynamics in teams. Organ Psychol Rev. 2025;15(1):44–67. doi:10.1177/20413866241292341
73. Wilson C, Janes G, Lawton R, Benn J. Types and effects of feedback for emergency ambulance staff: a systematic mixed studies review and meta-analysis. BMJ Qual Saf. 2023;32(10):573. doi:10.1136/bmjqs-2022-015634
74. Hackman JR. The design of work teams. In: Lorsch J, editor. Handbook of Organizational Behavior. Prentice-Hall; 1987:315–342.
75. Sundstrom E, De Meuse KP, Futrell D. Work teams: applications and effectiveness. Am Psychologist. 1990;45(2):120–133. doi:10.1037/0003-066X.45.2.120
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.