Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Cognitive reserve and Aβ1-42 in mild cognitive impairment (Argentina-Alzheimer’s Disease Neuroimaging Initiative)
Authors Harris P, Fernandez Suarez M, Surace E, Chrem Méndez P, Martín M, Clarens MF, Tapajóz F, Russo MJ, Campos J, Guinjoan S, Sevlever G ![]() , Allegri R
, Allegri R
Received 10 March 2015
Accepted for publication 8 June 2015
Published 7 October 2015 Volume 2015:11 Pages 2599—2604
DOI https://doi.org/10.2147/NDT.S84292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Paula Harris,1,2 Marcos Fernandez Suarez,1 Ezequiel I Surace,1,2 Patricio Chrem Méndez,1 María Eugenia Martín,1 María Florencia Clarens,1 Fernanda Tapajóz,1,2 Maria Julieta Russo,1 Jorge Campos,1 Salvador M Guinjoan,1,2 Gustavo Sevlever,1 Ricardo F Allegri1,2
1Instituto de Investigaciones Neurológicas, 2Consejo Nacional de Investigaciones Científicas y Técnicas, Buenos Aires, Argentina
Background: The purpose of this study was to investigate the relationship between cognitive reserve and concentration of Aβ1-42 in the cerebrospinal fluid (CSF) of patients with mild cognitive impairment, those with Alzheimer’s disease, and in control subjects.
Methods: Thirty-three participants from the Argentina-Alzheimer’s Disease Neuroimaging Initiative database completed a cognitive battery, the Cognitive Reserve Questionnaire (CRQ), and an Argentinian accentuation reading test (TAP-BA) as a measure of premorbid intelligence, and underwent lumbar puncture for CSF biomarker quantification.
Results: The CRQ significantly correlated with TAP-BA, education, and Aβ1-42. When considering Aβ1-42 levels, significant differences were found in CRQ scores; higher levels of CSF Aβ1-42 were associated with higher CRQ scores.
Conclusion: Reduced Aβ1-42 in CSF is considered as evidence of amyloid deposition in the brain. Previous results suggest that individuals with higher education, higher occupational attainment, and participation in leisure activities (cognitive reserve) have a reduced risk of developing Alzheimer’s disease. Our results support the notion that enhanced neural activity has a protective role in mild cognitive impairment, as evidenced by higher CSF Aβ1-42 levels in individuals with more cognitive reserve.
Keywords: amyloid, biomarkers, cerebrospinal fluid, Alzheimer’s disease
Introduction
Alzheimer’s disease (AD) is a neurodegenerative disorder characterized by progressive functional and cognitive decline.1 Increasing evidence suggests that the pathological substrate of AD may begin years to decades before the clinical diagnosis, with an initial asymptomatic stage followed by a phase of mild cognitive impairment (MCI).
MCI is a nosological entity useful for identifying adults at risk of developing AD or other dementia syndromes. It is defined by objective evidence of cognitive impairment, subjective memory complaints, and preserved global cognition and activities of daily living.2,3
Although rates of conversion from MCI to AD range from 5% to 23%, many individuals diagnosed with MCI remain stable or progress to a non-AD dementia.4
Hallmark lesions of sporadic AD comprise intraneuronal inclusions of abnormally phosphorylated tau protein and extracellular deposits of amyloid-beta peptide, especially the 42 amino acid isoform (Aβ1-42).
Cerebrospinal fluid (CSF) biomarkers, ie, Aβ1-42, phosphorylated tau181, and total tau, are altered in AD patients compared with controls: decreased Aβ1-42 reflects deposition of amyloid-beta in plaques while high total tau levels reflect active axonal and neuronal damage.5–7
In other types of dementia, as well as in a subgroup of patients with MCI, less specific changes in these biomarker concentrations have been reported.8–10 Likewise, correlations between cognitive status and amyloid burden at autopsy have not been found. This fact raises the question about a possible relationship between cognitive status, amyloid burden, and disease progression.
On the other hand, many studies indicate that a set of life experiences, such as educational and occupational attainment and leisure activities, is associated with reduced risk of developing dementia and with a slower rate of memory decline during normal aging. Several prospective studies reported that up to 25% of older subjects who were cognitively normal in life met full pathological criteria for AD at autopsy.11,12 The cognitive reserve (CR) construct has been proposed to account for the discrepancy between the degree of brain pathology and its clinical manifestation. Therefore, individuals with high CR may tolerate substantial pathology before showing cognitive loss, whereas those with low CR may decline earlier. The CR paradigm postulates that individual differences in cognitive achievement, and/or neural networks underlying task performance, allow some people to cope better than others with brain damage; according to the CR hypothesis, persons with higher CR can sustain cognitive function in the presence of more brain pathology than subjects with lower CR.13
Stimulating environments, a component of CR measured in humans by variables such as engagement in leisure activities and occupational attainment, promote neurogenesis in animals, and upregulate brain-derived neurotrophic factor, which fosters neural plasticity.14 There is evidence suggesting that environmental enrichment might act directly to prevent or slow the accumulation of AD pathology.15 Therefore, as cognitive stimulation regulates factors that increase neuronal plasticity, a complete account of CR should integrate the interactions between genetics, environmental influences on brain reserve, pathology, and the ability to actively compensate for the effects of pathology.
Roe et al have investigated the relationship between CR, AD biomarkers, and the risk of cognitive impairment, and found that Aβ1-42 combined with education and normalized whole brain-volume better predicts progression across follow-up.16 The purpose of this study was to investigate the relationship between CR and Aβ1-42 concentrations.
Patients and methods
Patients
Thirty-three Caucasian participants from the Argentina Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (eight cognitively normal, 23 with amnesic MCI, two with AD; mean age 68.3±8.4 years, education 13.6±3.8 years and Mini Mental State Examination [MMSE] score 27.7±3.1) recruited at the Neurological Institute of Investigation between February and December 2013 were included for this investigation after giving their informed consent. The subjects were included only if they agreed to undergo a lumbar puncture. Approval for the study was obtained from the ethics committee of the Neurological Institute of Investigation.
The diagnosis of MCI was established according to Petersen criteria, while the diagnosis of AD was done according to the recommendations from the National Institute on Aging.3,17
Inclusion criteria were: age 55–90 years; written informed consent obtained prior to the study; a Geriatric Depression Scale score ≤4; and education equivalent to ≥6 grade. Exclusion criteria included: medical history of psychiatric or any other neurological disease that could interfere with completion of assessments; consumption of psychoactive drugs; severe sensory or comprehension deficit; and not consenting to lumbar puncture for CSF biomarkers.
Materials
During assessment, subjects completed the ADNI neuropsychological battery, an Argentinian accentuation reading test (TAP-BA) that assesses the accentuation of 50 infrequent, irregularly stressed Spanish words as a measure of premorbid intelligence, and the Cognitive Reserve Questionnaire (CRQ) devised by Rami et al to estimate CR.18,19 They all underwent lumbar puncture to study CSF levels of total tau, phosphorylated tau181, and Aβ1-42. The research was conducted in accordance with the Declaration of Helsinki (1975).
CSF was collected by lumbar puncture at the L3/L4 or L4/L5 level during the morning. The first 20 drops were discarded and the remaining CSF (approximately 4–5 mL) was collected and aliquoted in polypropylene tubes. These tubes were stored at −80°C until analysis. Quantification of Aβ1-42, total tau, and phosphorylated tau181 was performed using commercially available enzyme-linked immunosorbent assay kits (Innogenetics, Ghent, Belgium) according to the manufacturer’s instructions. Briefly, 25 μL or 75 μL of CSF samples were used for measurement of Aβ1-42 and total tau or phosphorylated tau181, respectively. Samples were incubated in the corresponding capture antibody-coated polypropylene plate with specific biotinylated monoclonal detector antibodies. After washing, the antigen-antibody complexes were detected by peroxidase-labeled streptavidin followed by addition of tetramethyl benzidine as the peroxidase substrate. Absorbance at 450 nm and 620 nm (used as reference wavelengths) was measured using a Benchmark Plus microplate spectrophotometer (Bio-Rad, Hercules, CA, USA). Standard curve interpolation of the data and subsequent analysis were performed using GraphPad Prism 5 software. Receiver operating characteristic analysis using a cohort of cognitively normal controls and AD patients showed that the cut-off point of 532.5 pg/mL best discriminated these two populations (sensitivity 100%, specificity 87.5%). MCI subjects were divided in two groups according to Aβ1-42 level (median 560 pg/mL; cut-off 532.5 pg/mL).
The ADNI is a large, multicenter, longitudinal neuroimaging study launched in 2004 by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, the US Food and Drug Administration, private pharmaceutical companies, and nonprofit organizations. ADNI includes adult subjects aged 55–90 years who meet entry criteria for a clinical diagnosis of amnestic MCI, probable AD, or normal cognition. Participants receive baseline and periodic physical and neurological examinations and standardized neuropsychological assessments, and provide biological samples (blood, urine, and in a subset, CSF) throughout the study. Imaging (magnetic resonance imaging and for a subset, F-fluorodeoxyglucose positron emission tomography [PET] and Pittsburgh compound B PET) is performed at baseline and at regular intervals thereafter (http://www.adni-info.org/).
The ADNI neuropsychological battery comprises the Spanish versions of: MMSE;20 Logical Memory;21 Clinical Dementia Rating;22 The Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog);23 Rey Auditory Verbal Learning Test (RAVLT);24 Montreal Cognitive Assessment (MoCA);25 Clock Drawing Test;26 Category fluency-animals;27 Trail Making Test A and B;28 and Boston Naming Test.29 Some of the tests selected for ADNI are:
- The MMSE, a 30-point questionnaire that is widely used to screen for cognitive impairment (10 points for spatial and temporal orientation; 6 points for memory retention and recall; 5 points for attention and calculation; 8 points for language; and 1 point for visual construction).
- The Boston Naming Test, a confrontation naming test that measures word retrieval using a set of pictures (30 items in the ADNI version).
- Story A from the WMS-III Logical Memory (subtest of the Wechsler Memory Scale) is an immediate and delay measure of episodic memory.
- The RAVLT, a list-learning paradigm in which the patient, after hearing a list of 15 nouns (list A) is asked to recall as many words from the list as possible (five repetitions of free-recall). An “interference” list (list B) is presented in the same manner, after the interference trial, the participant is immediately asked to recall the words from list A. After a 20-minute delay, the participant is asked to again recall the words from list A, followed by a recognition phase (50 words).
- The ADAS-Cog, a brief standardized test battery that assesses learning and memory, language production, language comprehension, constructional praxis, ideational praxis, and orientation. Following the objective testing, subjective clinical ratings of language ability and the ability to remember test instructions are performed by the examiner.
- The Clinical Dementia Rating, a global measure of dementia, which is usually completed by a clinician by means of an interview with the patient and the caregiver (covered areas are memory, orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care).
- Category fluency (animals), a widely used measure of semantic memory in which the subject is asked to name different exemplars from a given semantic category. The number of correct unique exemplars named is scored.
- The MoCA, designed as a rapid screening instrument for mild cognitive dysfunction, assesses attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation. The total possible score is 30 points; a score of 26 or above is considered normal.
- Trail Making Test, a test of processing speed and executive function. Although both Parts A and B depend on visual-motor and perceptual scanning skills, Part B also requires cognitive flexibility in shifting from number to letter sets under time pressure.
The CRQ included:
- Education: (0–10)
- Patient years of education (0–5)
- Patient’s parents educational level (0–2)
- Patient training courses (0–3)
- Working activity: (0–4)
- Leisure activity: (0–8)
- Musical training (0–2)
- Reading (0–4)
- Intellectual activities (0–2)
- Languages (multilingualism): (0–3)
- Only mother tongue (first language; 0)
- Mother tongue plus a low fluency second language (1)
- Bilingualism (2)
- Multilingualism (3)
The total score is 25. The authors divided scores into quartiles to determine the level of CR (first quartile ≤6; second quartile 7–9; third quartile 9–14; fourth quartile ≥15).
Data analysis
Analyses were performed using Statistical Package for the Social Sciences version 17.0 software. Association between variables (CSF biomarkers, CR, accentuation test, and neuropsychological battery) was estimated using Spearman’s correlation coefficient. An independent-samples t-test was used for comparing groups according to AB1-42 or CR levels. Linear regression was performed to estimate the association between CRQ score and CSF Aβ1-42.
Results
There were no significant differences between the groups (control, MCI, AD) regarding sex, education, CRQ, or TAP-BA. The CRQ had a positive correlation with TAP-BA (rs=0.54; P≤0.005), education (rs=0.69; P≤0.001), and Aβ1-42 (rs=0.42; P<0.05; Figure 1). Inverse correlations were found between CRQ and Trail Making Test A (rs=−0.54; P≤0.01) and Trail Making Test B (rs=−0.75; P≤0.001). Aβ1-42 significantly correlated with total tau (rs=−0.53; P≤0.005), Alzheimer’s profile (rs=0.79; P≤0.001) category fluency (animals; rs=0.45; P≤0.05), and RAVLT. Differences remained significant after correction for age. Significant correlations were found too between total tau and cognitive measures (category fluency and RAVLT). Sixteen subjects presented a positive Alzheimer’s profile (12 MCI, three controls, one AD). After dividing the MCI patients according to Aβ1-42 levels (cut-off 532.5 pg/mL), significant differences were found within subgroups in CRQ scores (P<0.05; Table 1), showing that higher levels of CSF Aβ1-42, were associated with higher CRQ scores.
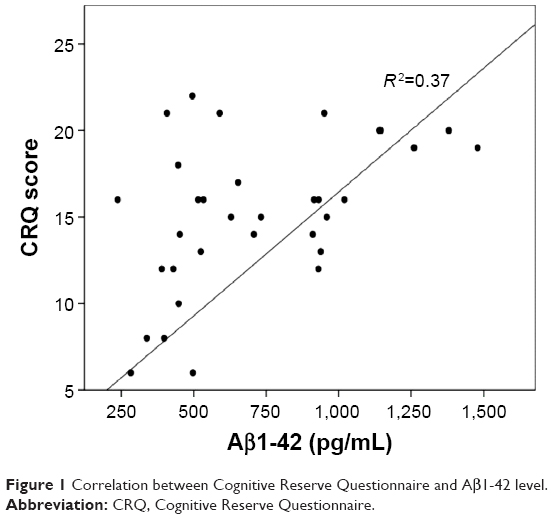 | Figure 1 Correlation between Cognitive Reserve Questionnaire and Aβ1-42 level. |
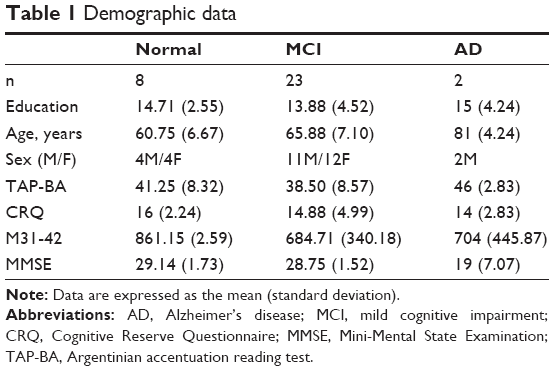 | Table 1 Demographic data |
Significant differences were also found after classifying subjects according to their CR level (low, <15; high, ≥15); only four patients with high CR had CSF Aβ1-42 lower than the cut-off (Table 2). No other measure differed significantly across groups. No significant differences between MCI groups were found regarding age, education, and MMSE score (Table 2).
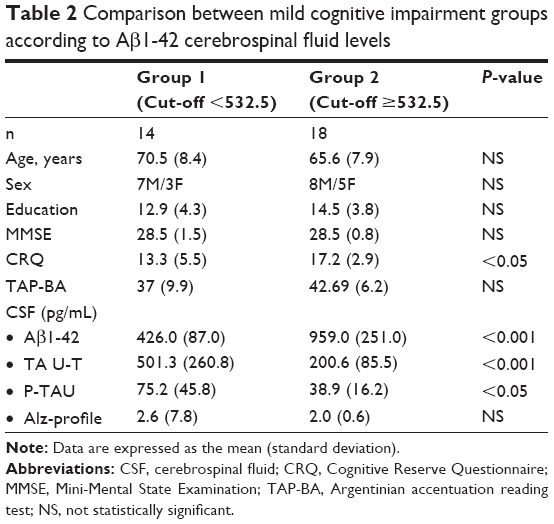 | Table 2 Comparison between mild cognitive impairment groups according to Aβ1-42 cerebrospinal fluid levels |
Discussion
Pathological hallmarks of AD include synaptic and neuronal degeneration and the presence of extracellular deposits of amyloid-beta in the cerebral cortex. With the advent of CSF biomarkers, such as tau and amyloid-beta (Aβ1-42), measuring in vivo levels of peptides in CSF has been helpful for the diagnosis of AD.30 Some studies have reported that these markers could reflect brain pathology and could be used as surrogates for AD lesions.
Based on the CR theory, highly educated subjects would have more marked abnormalities in the CSF than those with a shorter education because of the compensatory effect over brain damage. Moreover, the CR hypothesis predicts that, at the same level of cognitive impairment, the underlying pathology will be more advanced in individuals with higher CR.
According to Stern et al AD patients with higher education exhibited a stronger brain pathology, including reduced temporoparietal PET with fluorodeoxyglucose or single photon emission computed tomography measurements, when compared with patients with AD with low educational attainment at similar levels of dementia severity.31
The aim of the current investigation was to investigate the relationship between CR and concentrations of Aβ1-42 in patients from our ADNI cohort. Several studies found an inverse correlation between Aβ1-42 and CR, suggesting that subjects with high CR have greater biomarker abnormalities than subjects with low CR. Similarly, Rolstad et al observed that, at the same level of clinical severity, patients converting to dementia with high CR had lower Aβ1-42 than converters with a medium and low CR (measured by educational level).32
On the other hand, recent studies proposed that amyloid-beta secretion might be affected by neural activity and that enhanced lifestyle practices are associated with reduced amyloid-beta deposition (based on Pittsburgh compound B PET and CSF Aβ1-42).33–35
Jagust and Mormino observed that brain activity regulates amyloid-beta secretion and deposition.11 They hypothesize that CR may play different roles during pre-amyloid and post-amyloid plaque stages: once Aβ1-42 deposition begins, CR allows high CR individuals to cope better with neuronal dysfunction than in individuals with low CR. However, in pre-amyloid plaque stages, CR could act to diminish Aβ1-42 production through better neural efficiency.
Our study revealed a significant direct relationship between CSF Aβ1-42 level and CRQ score. These results are consistent with the observation that participation in cognitively stimulating activities is associated with less accumulation of amyloid-beta.
Liang et al examined associations between exercise engagement and biomarker levels in older adults without clinical symptoms of AD, and observed that individuals with elevated Pittsburgh compound B PET, CSF tau or phosphorylated tau181, or decreased CSF Aβ1-42 consistently exercised less.36
The notion that cognitive activity influences the development of AD pathology is supported by recent findings that cognitively normal older individuals with greater lifelong participation in complex mental activities showed less hippocampal atrophy, another biomarker of AD pathology. These authors reported a direct association between cognitive activity and [11C] Pittsburgh compound B uptake, suggesting that lifestyle factors found in individuals with high cognitive engagement may prevent or slow deposition of Aβ1-42-amyloid.35
Bennet et al using crude counts of AD pathology from the maximally involved area from four 6 μm sections stained with modified Bielschowsky silver stains, reported that education modified the relationship between senile plaques – but not neurofibrillary tangles – and level of cognition.37 Thus, focusing on amyloid-beta as the measure of primary AD pathology is based on previous studies showing that education (cognitive reserve) reduced the impact of amyloid-beta pathology but not tau pathology on cognitive performance.
This preliminary result supports the hypothesis of the protective role of enhanced lifelong neural activity on amyloid deposition and the utility of biomarkers, specifically Aβ1-42, as substitutes for pathology in relation to CR. To our knowledge, this preliminary study is the first Argentinian investigation reporting this association. A prospective analysis of cognitive decline in a larger cohort would be important in order to determine the frequency of conversion from MCI to dementia. The limitations of this paper include the small size of the sample due to the inclusion criterion requiring that patients from the ADNI protocol consent to a lumbar puncture.
Disclosure
The authors report no conflicts of interest in this work.
References
Khachaturian ZS. Diagnosis of Alzheimer’s disease. Arch Neurol. 1985;42:1097–1105. | ||
Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256:183–194. | ||
Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol. 2005;62:1160–1163. | ||
Mitchell AJ, Shiri-Feshki M. Rate of progression of mild cognitive impairment to dementia-meta-analysis of 41 robust inception cohort studies. Acta Psychiatr Scand. 2009;119:252–265. | ||
Strozyk D, Blennow K, White LR, Launer LJ. CSF Abeta 42 levels correlate with amyloid-neuropathology in a population-based autopsy study. Neurology. 2003;60:652–656. | ||
Tapiola T, Alafuzoff I, Herukka SK, et al. Cerebrospinal fluid (beta) amyloid 42 and tau proteins as biomarkers of Alzheimer-type pathologic changes in the brain. Arch Neurol. 2009;66:382–389. | ||
Blennow K. Cerebrospinal fluid protein biomarkers for Alzheimer’s disease. NeuroRx. 2004;1:213–225. | ||
Blennow K. CSF biomarkers for mild cognitive impairment. J Intern Med. 2004;256:224–234. | ||
De Jong D, Kremer BP, Olde Rikkert MG, Verbeek MM. Current state and future directions of neurochemical biomarkers for Alzheimer’s disease. Clin Chem Lab Med. 2007;45:1421–1434. | ||
Visser PJ, Verhey F, Knol DL, et al. Prevalence and prognostic value of CSF markers of Alzheimer’s disease pathology in patients with subjective cognitive impairment or mild cognitive impairment in the DESCRIPA study: a prospective cohort study. Lancet Neurol. 2009;8:619–627. | ||
Jagust WJ, Mormino EC. Lifespan brain activity, B-amyloid, and Alzheimer’s disease. Trends Cogn Sci. 2011;15:520–526. | ||
Knopman DS, Parisi JE, Salviati A, et al. Neuropathology of cognitively normal elderly. J Neuropathol Exp Neurol. 2003;62:1087–1095. | ||
Stern Y. Cognitive reserve. Neuropsychologia. 2009;47:2015–2028. | ||
Brown J, Cooper-Kuhn CM, Kemperman G, Van Praag H, Winkler J, Gage FH. Enriched environment and physical activity stimulate hippocampal but not olfactory bulb neurogenesis. Eur J Neurosci. 2003;17:2042–2046. | ||
Lazarov O, Robinson J, Tang YP, et al. Environmental enrichment reduces Abeta levels and amyloid deposition in transgenic mice. Cell. 2005;120:701–713. | ||
Roe CM, Fagan AM, Williams MM, et al. Improving CSF biomarker accuracy in predicting prevalent and incident Alzheimer disease. Neurology. 2011;76:501–510. | ||
McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging and the Alzheimer’s Association Workgroup. Alzheimers Dement. 2011;7:263–269. | ||
Burin D, Jorge RE, Arizaga RA, Paulsen JS. Estimation of premorbid intelligence: the Word Accentuation Test-Buenos Aires version. J Clin Exp Neuropsychol. 2000;22:677–685. | ||
Rami L, Valls-Pedret C, Bartres-Faz D, et al. Cuestionario de reserva cognitiva: valores obtenidos en población anciana sana y con enfermedad de Alzheimer [Cognitive reserve questionnaire. Scores obtained in a healthy elderly population and in one with Alzheimer’s disease]. Rev Neurol. 2011;52:195–201. Spanish. | ||
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198. | ||
Wechsler D. Wechsler Memory Scale Revised. San Antonio, TX, USA: Psychological Corporation; 1987. | ||
Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43:2412–2414. | ||
Rosen W, Mohs R, Davis K. A new rating scale for Alzheimer’s disease. Am J Psychiatry. 1984;141:1356–1364. | ||
Rey A. [L‘Examen Clinique en Psychologie]. Paris, France: Presses Universitaires de France; 1964. French. | ||
Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695–699. | ||
Goodglass H, Kaplan E. The Assessment of Aphasia and Related Disorders. 2nd ed, Philadelphia, PA, USA: Lea & Febiger; 1983. | ||
Morris JC, Heyman A, Mohs RC, et al. The consortium to establish a registry for Alzheimer’s disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology. 1989;39:1159–1165. | ||
Reitan RM. Validity of the Trail-Making Test as an indication of organic brain damage. Percept Mot Skills. 1958;271–276. | ||
Kaplan E, Goodglass H, Weintraub S. Boston Naming Test. Philadelphia, PA, USA: Lea & Febiger; 1983. | ||
Blennow K, Zetterberg H. Cerebrospinal fluid biomarkers for Alzheimer’s disease. J Alzheimers Dis. 2009;18:413–417. | ||
Stern Y, Alexander GE, Prohovnik I, Mayeux R. Inverse relationship between education and parietotemporal perfusion deficit in Alzheimer’s disease. Ann Neurol. 1992;32:371–375. | ||
Rolstad S, Nordlund A, Eckerström C, Gustavsson MH, Zetterberg H, Wallin A. Cognitive reserve in relation to abeta42 in patients converting from MCI to dementia – a follow-up report. Dement Geriatr Cogn Disord. 2009;28:110–115. | ||
Kamenetz F, Tomita T, Hsieh H, et al. APP processing and synaptic function. Neuron. 2003;37:925–937. | ||
Cirrito JR, Yamada KA, Finn MB, et al. Synaptic activity regulates interstitial fluid amyloid-beta levels in vivo. Neuron. 2005;48:913–922. | ||
Landau SM, Marks SM, Mormino EM, et al. Association of lifetime cognitive engagement and low B-amyloid deposition. Arch Neurol. 2012;69:623–629. | ||
Liang KY, Mintun MA, Fagan AM, et al. Exercise and Alzheimer’s disease biomarkers in cognitively normal older adults. Ann Neurol. 2010;68:311–318. | ||
Bennett DA, Schneider JA, Wilson RS, et al. Education modifies the association of amyloid but not tangles with cognitive function. Neurology. 2005;65:953–955. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.