Back to Journals » Clinical Interventions in Aging » Volume 20
Cognitive Function Profiles and Associated Factors in Older Adults Living with Type 2 Diabetes: A Latent Profile Analysis
Authors Ye B, Pan M, Lei X, Wen Y, Zhang Q
Received 11 July 2025
Accepted for publication 26 November 2025
Published 10 December 2025 Volume 2025:20 Pages 2493—2503
DOI https://doi.org/10.2147/CIA.S553115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Beilei Ye,1,2 Mengxia Pan,1,2 Xiaoju Lei,2 Ying Wen,2 Qiong Zhang2
1Geriatric Medicine Center, Department of Geriatric Medicine, Zhejiang Provincial People’s Hospital(Affiliated People’s Hospital), Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Nursing, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Qiong Zhang, Department of Nursing, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Objective: This study aims to explore the latent profile characteristics of cognitive function in older adults living with diabetes and analyze the influencing factors, providing theoretical evidence for early intervention.
Methods: A cross-sectional study design was used to select older adults living with diabetes hospitalized at a tertiary hospital as the study population. Cognitive function was assessed using the Mini-Mental State Examination (MMSE). Demographic characteristics, disease-related data (such as duration of diabetes, BMI, and HbA1c levels), and lifestyle factors (such as sleep quality, physical activity, and social support) were collected. Latent profile analysis (LPA) was employed to classify cognitive function, and ordered multinomial logistic regression was performed to analyze the influencing factors of each cognitive profile.
Results: A total of 564 patients were included. Latent profile analysis of cognitive impairment identified three categories: complete cognitive impairment (12.82%), partial cognitive impairment (54.74%), and at-risk cognitive impairment (32.44%). Logistic regression analysis revealed that gender, education level, duration of diabetes, HbA1c, diverse intellectual activities, and nutrition were independent factors influencing cognitive impairment (P< 0.05).
Conclusion: Cognitive impairment in older adults living with diabetes exhibits distinct profile characteristics and is influenced by multiple factors. Interventions should focus on improving blood glucose control, promoting diverse intellectual activities, and enhancing social support to delay the decline in cognitive function.
Keywords: older adults, diabetes, cognitive impairment, influencing factors
Introduction
With the acceleration of population aging, the prevalence of diabetes among the older adults has significantly increased.1 A systematic review and meta-analysis reported that up to 45% of patients with type 2 diabetes exhibit cognitive impairment,2 which can adversely affect their daily functioning and treatment adherence, further complicating disease management and increasing the risk of early mortality, leading to a higher risk of early mortality. The onset of cognitive impairment results from a combination of multiple factors. Studies have shown that physiological mechanisms such as hyperglycemia, elevated inflammation, vascular damage, and insulin resistance in older adults living with diabetes may directly impair cognitive function3,4 Furthermore, individual psychosocial factors (such as lack of social support and depression) and lifestyle behaviors (such as irregular sleep patterns and lack of physical activity) are also closely associated with cognitive impairment.5,6 However, there is still insufficient research on the diversity of cognitive function in living with diabetes, and studies focusing on different cognitive profile groups are inadequate.
Despite previous studies identifying various risk factors for cognitive impairment in older adults with diabetes, most research has primarily focused on overall prevalence rates or examined linear associations with single factors. Limited attention has been given to the heterogeneity of cognitive performance within this population, and evidence regarding the coexistence of distinct cognitive subtypes is still lacking. This gap partially restricts the development and implementation of targeted, precision interventions.
Latent Profile Analysis (LPA) is a person-centered statistical approach that classifies individuals based on patterns of observed indicators.7 Unlike traditional methods that rely on overall cognitive scores (eg, MMSE total score), LPA can utilize domain-specific MMSE scores to identify distinct cognitive function profiles, thereby providing a more nuanced understanding of heterogeneity and potentially revealing subgroups with different prognostic risks.
Accordingly, this study aimed to explore the latent profile characteristics of cognitive function in older adults with diabetes using LPA and to analyze associated factors. The findings are intended to provide theoretical evidence for developing personalized intervention strategies. By identifying and comparing distinct cognitive profiles, this study may enhance the understanding of cognitive impairment in this population, inform early screening and intervention in clinical practice, and ultimately improve quality of life while reducing the societal and familial burden of disease.
Methods
Participants
A convenience sampling method was used to select older adults (age ≥60 years) living with type 2 diabetes hospitalized at a tertiary hospital in Zhejiang Province from December 2023 to November 2024. The inclusion criteria were as follows: (1) age ≥ 60 years; (2) diagnosis of type 2 diabetes according to the 1999 World Health Organization (WHO) criteria;4 (3) stable chronic condition,defined as no acute exacerbation of diabetes or other major chronic diseases (eg, hypertension, cardiovascular disease) in the past month; (4) informed consent. The exclusion criteria were: (1) patients diagnosed with dementia or psychiatric disorders; (2) patients with severe visual or auditory impairments; (3) patients unable to complete the survey due to severe illness.
Sample Size Estimation
The sample size was estimated using the formula for cross-sectional studies: N =Z2α/2×P (1−P) /δ2, whereα=0.05, Zα/2=1.96, P is the prevalence rate and δ is the allowable margin of error. According to a literature review, the prevalence of cognitive impairment in older adults living with diabetes is approximately 45%,2 with δ= 0.06. The required sample size was calculated to be 264 participants. Assuming a 90% effective response rate, the required sample size was adjusted to N = 294.
In this study, 571 patients were initially recruited; after applying inclusion and exclusion criteria (n = 3) and accounting for withdrawal of informed consent (n = 4), a total of 564 eligible participants were ultimately included. The final sample size exceeded the minimum requirement, ensuring adequate statistical power and transparency of the sampling process.
Instrument Design
The assessment tool consisted of 6 sections as follows:
Section 1: Socio-Demographic and Diabetes-Related Information
A self-designed, validated Chinese-language general information questionnaire was designed based on a literature review of diabetes and cognitive frailty, as well as expert opinions and group discussions. The questionnaire primarily covered the following aspects: (1) Demographic and sociological information: gender, age, education level, marital status, occupation, living arrangements, and personal monthly income; (2) Health behaviors and lifestyle: including regular physical exercise and engagement in diverse intellectual activities.
Section 2 Mini Mental State Examination (MMSE)
Developed by Folstein et al8 in 1975, the Mini-Mental State Examination (MMSE) is a widely used and influential tool for assessing and screening cognitive function both domestically and internationally. It includes five dimensions: orientation, memory, attention and calculation, recall ability, and language ability, with a total score of 30 points. The scoring criteria are as follows: normal cognition: 24 points and above; mild cognitive impairment: 18–23 points; moderate to severe cognitive impairment: 17 points and below.9
Section 3 Mini Nutritional Assessment Short-Form (MNA-SF)
Developed by Rubenstein et al10 as a simplified version of the Mini Nutritional Assessment (MNA), the scale consists of 6 items with a total score of 14 points. A score of 0–7 points indicates malnutrition, 8–11 points indicates a risk of malnutrition, and 12–14 points indicates normal nutritional status. The scale has a Cronbach’s α coefficient of 0.711 and is one of the primary nutritional screening tools for older adults patients.
Section 4 Athens Insomnia Scale (AIS)
Developed by American scholar Soldatos et al,11 this scale is used to assess sleep quality over the past month. The scale consists of 8 items, with each item scored from 0 to 3, yielding a maximum score of 24 points. A higher score indicates poorer sleep quality. A score of <4 points indicates no sleep disturbance, 4–6 points suggests suspected insomnia, and >6 points indicates insomnia. The scale has a Cronbach’s α coefficient of 0.884 and is internationally recognized as a standard tool for assessing sleep quality.
Section 5 5-Item Geriatric Depression Scale (GDS-5)
Developed by Hoyl et al12 as a simplified version of the GDS-15, this scale is an effective tool for screening depression in older adults individuals. The scale consists of 5 items, each scored from 0 to 1, with a maximum score of 5 points. A higher score indicates greater severity of depression. A score of ≥2 points indicates the presence of depression. The sensitivity of this scale for screening depression is 94%, with a specificity of 81%, and it shows significant consistency with clinical depression diagnoses.
Section 6 Social Support Rating Scale (SSRS)
Developed by Chinese scholar Xiao Shuiyuan,13 this scale consists of 10 items across 3 dimensions, with a score range of 12–66 points. A higher score indicates better social support. A total score ≤22 points indicates low social support, 23–44 points indicates moderate social support, and ≥45 points indicates high social support. The scale has a Cronbach’s α coefficient of 0.92 and is widely used in the Chinese medical community.
Statistical Analysis
Statistical data analysis was performed using SPSS 25.0 software. Normally distributed continuous variables are presented as mean ± standard deviation (x ± s), while categorical variables are expressed as frequencies and percentages (%). Group comparisons were conducted using the chi-square (χ2) test. Multivariate analysis was performed using ordered multinomial logistic regression. A significance level of P < 0.05 was set. Data descriptive statistics and analysis were conducted using SPSS 25.0 software.
Latent profile analysis (LPA) was performed using Mplus 8.0 software, based on the five domain scores of the Mini-Mental State Examination (MMSE) (orientation, memory, attention/calculation, language, visuospatial ability), rather than the total score. All domain scores were standardized prior to analysis. Missing data were handled using Full Information Maximum Likelihood (FIML) to utilize all available information,14 and local independence was assessed by examining within-class correlations to ensure that, conditional on the latent class, the MMSE domain scores were independent.
The number of categories in the model was gradually increased from the initial model until the model fit was optimized. Model fit indices included Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), Adjusted Bayesian Information Criterion (a BIC), entropy, Lo-Mendell-Rubin Test (LMRT), and Bootstrap-based likelihood ratio tests. When the changes in AIC, BIC, and a BIC were small, entropy > 0.8 (with values ranging from 0 to 1, where entropy > 0.8 indicates a classification accuracy of 90%), and the LMRT showed significant differences (P < 0.05), it indicated that the k-profile model was superior to the k-1 profile model. A P value of < 0.05 was considered statistically significant. Besides, MMSE cutoffs were used without education adjustment, consistent with prior studies,9 while education was analyzed as an independent factor. The Brant test indicated no violation of the proportional odds assumption (χ2=8.13, df=6, p=0.23), supporting the use of the ordered logistic regression model.
Ethical Consideration
The study was approved by the Zhejiang Provincial People’s Hospital’s Research Ethics Committee (ZJPPHEC20221(079)). Written informed consent was obtained from all participants in the study. Before completing the survey, the participants were informed that their participation in this study would not pose any harm and that all the provided information would be kept confidential.
Result
Demographics and Clinical Characteristics of Participants
A total of 564 patients were included in this study, of whom 289 were male (51.2%) and 275 were female (48.8%). The age distribution was as follows: 237 patients (42.0%) were aged 60–69 years, 242 patients (42.9%) were aged 70–79 years, and 85 patients (15.1%) were aged 80 years or older. Most participants were younger-old (60–79 years), with a smaller proportion of the oldest-old (≥80 years). Detailed demographic information is shown in Table 2.
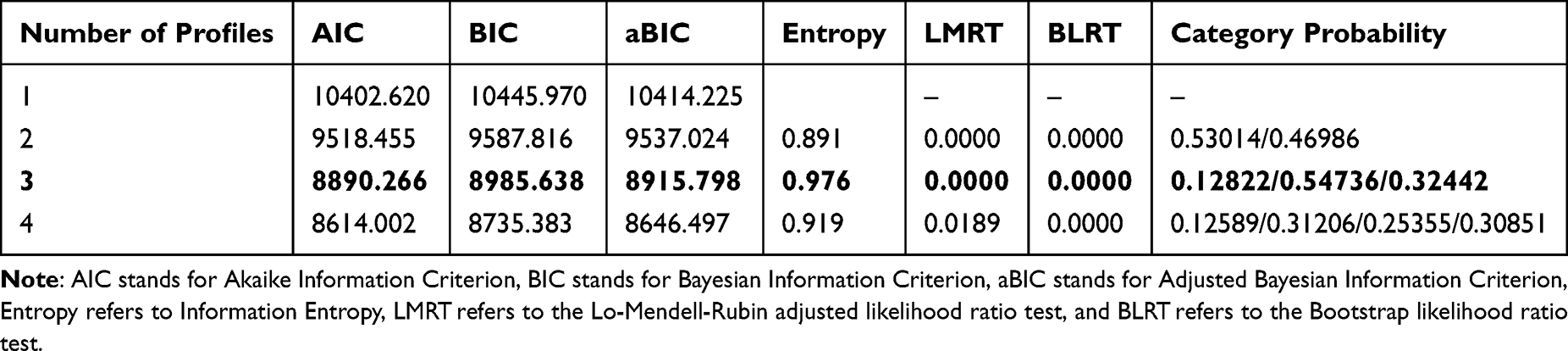 |
Table 1 Fit Indices of Latent Profile Analysis for Cognitive Impairment in Older Adults Living with Diabetes |
Results of Latent Profile Analysis of Cognitive Impairment in Older Adults Living with Diabetes
In this study, four latent profiles were fitted, and the third model was identified as the best model. The values of the fit indices are shown in Table 1. As the number of model categories increased, AIC, BIC, and aBIC gradually decreased. When the number of categories was set to 3, AIC, BIC, and aBIC were relatively small, the Entropy value was maximized, and both LMRT and BLRT values were statistically significant (P < 0.05), indicating the best model fit. Although the fourth model had the smallest AIC, BIC, and aBIC values, its Entropy was also smaller. Considering all factors, the third model was determined to be the most optimal.
Figure 1 shows the scores on the five dimensions of the Mini-Mental State Examination (MMSE) in older adults living with diabetes. Category 1 exhibited low scores across all dimensions, with significant cognitive impairment, and was thus labeled as “Complete Cognitive Impairment,” accounting for 12.82% of the total sample. Category 2 had relatively higher average scores, indicating mild cognitive impairment or a potential risk of cognitive decline, and was therefore labeled as “At-risk Cognitive Impairment,” representing 54.74% of the total sample. Category 3 patients exhibited intermediate deficits, especially in memory and attention, corresponding to “Partial Cognitive Impairment” (32.44%).
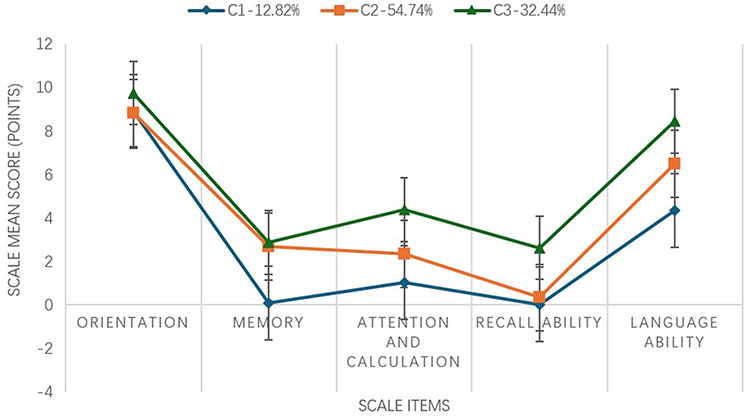 |
Figure 1 Three Latent Profiles of Cognitive Impairment in older adults living with diabetes. Note: C1 - Complete Cognitive Impairment Group (n = 73, 12.82%), C2 - Partial Cognitive Impairment Group (n = 309, 54.74%), C3 - At-risk cognitive impairment Group (n = 182, 32.44%), Error bars represent standard errors (±SE). |
Univariate Analysis of Cognitive Impairment in Older Adults Living with Diabetes
The univariate analysis results show that the following variables, including age, occupation type, living arrangements, personal monthly income, BMI, marital status, smoking and drinking habits, fasting blood glucose, number of comorbid chronic diseases, regular physical activity, and depression, did not show significant statistical differences (P > 0.05). This suggests that these common demographic and lifestyle characteristics may not be the primary drivers of cognitive impairment heterogeneity in this cohort.
However, the following factors, including gender, education level, duration of diabetes, HbA1c, intellectual activities, nutrition status, social support, and sleep condition, showed significant statistical differences between the groups (P < 0.05), as shown in Table 2. Specifically, women, individuals with lower education, longer diabetes duration, poorer glycemic control, malnutrition, insufficient cognitive activities, and inadequate sleep were more frequently represented in the cognitively impaired groups. These findings highlight modifiable clinical and lifestyle factors that could be targeted in interventions.
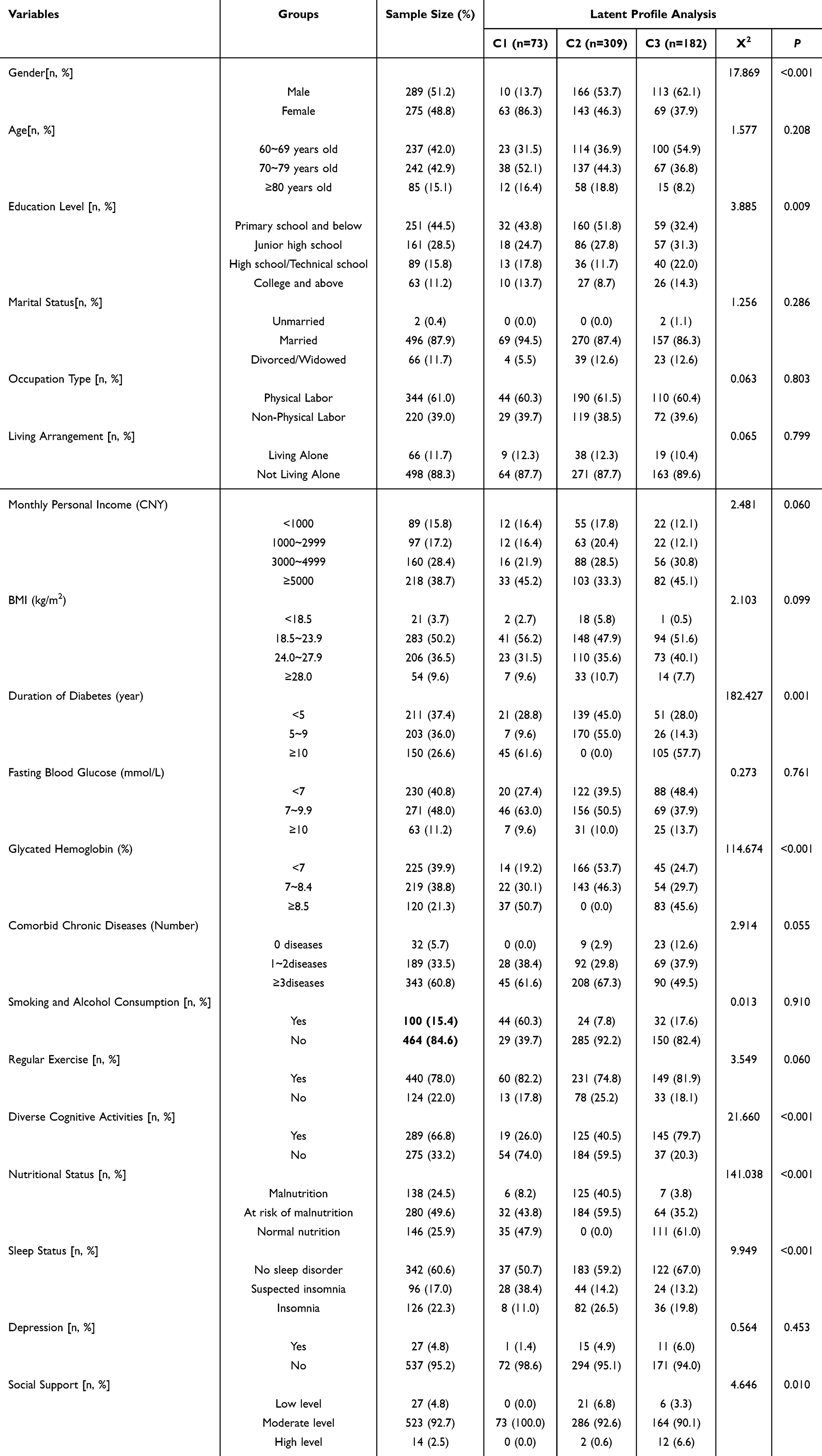 |
Table 2 Univariate Analysis of Demographic Data and Cognitive Impairment Profiles (n=564) |
Multivariate Analysis of Cognitive Impairment in Older Adults Living with Diabetes
Ordered multinomial logistic regression was used for multivariate analysis, with the three cognitive impairment categories in older adults living with diabetes as the dependent variable, and the “ at-risk cognitive impairment Group” category as the reference group. Variables with statistically significant results from the univariate analysis were assigned as independent variables, with the assignment method detailed in Table 3.
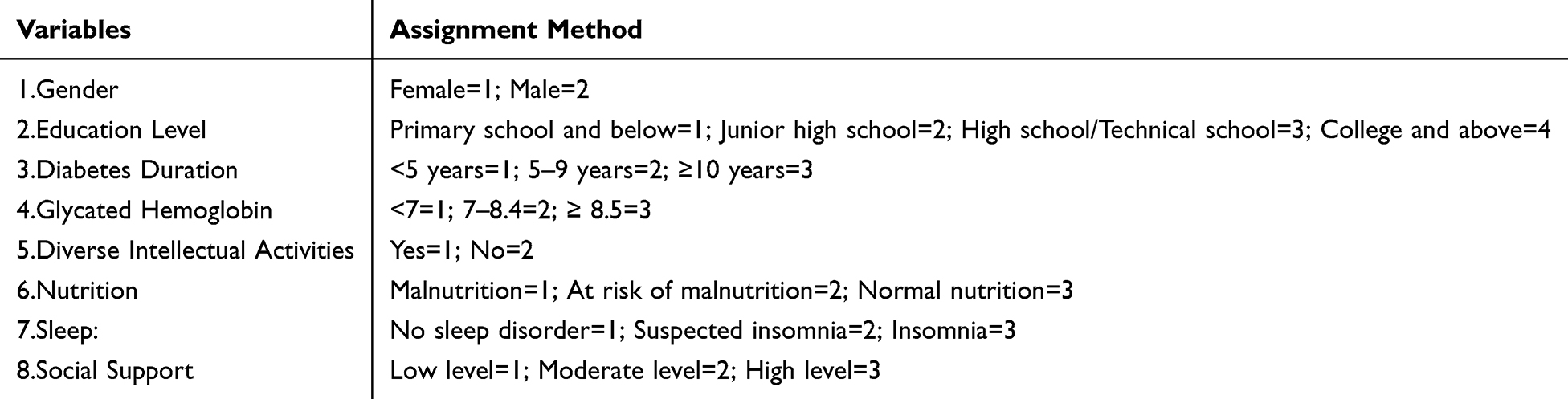 |
Table 3 Method of Assigning Independent Variables |
The results of this study indicate that gender, education level, diabetes duration, HbA1c, diversified intellectual activities, and nutritional status are independent influencing factors for cognitive impairment in older adults living with diabetes (P < 0.05), as shown in Table 4.
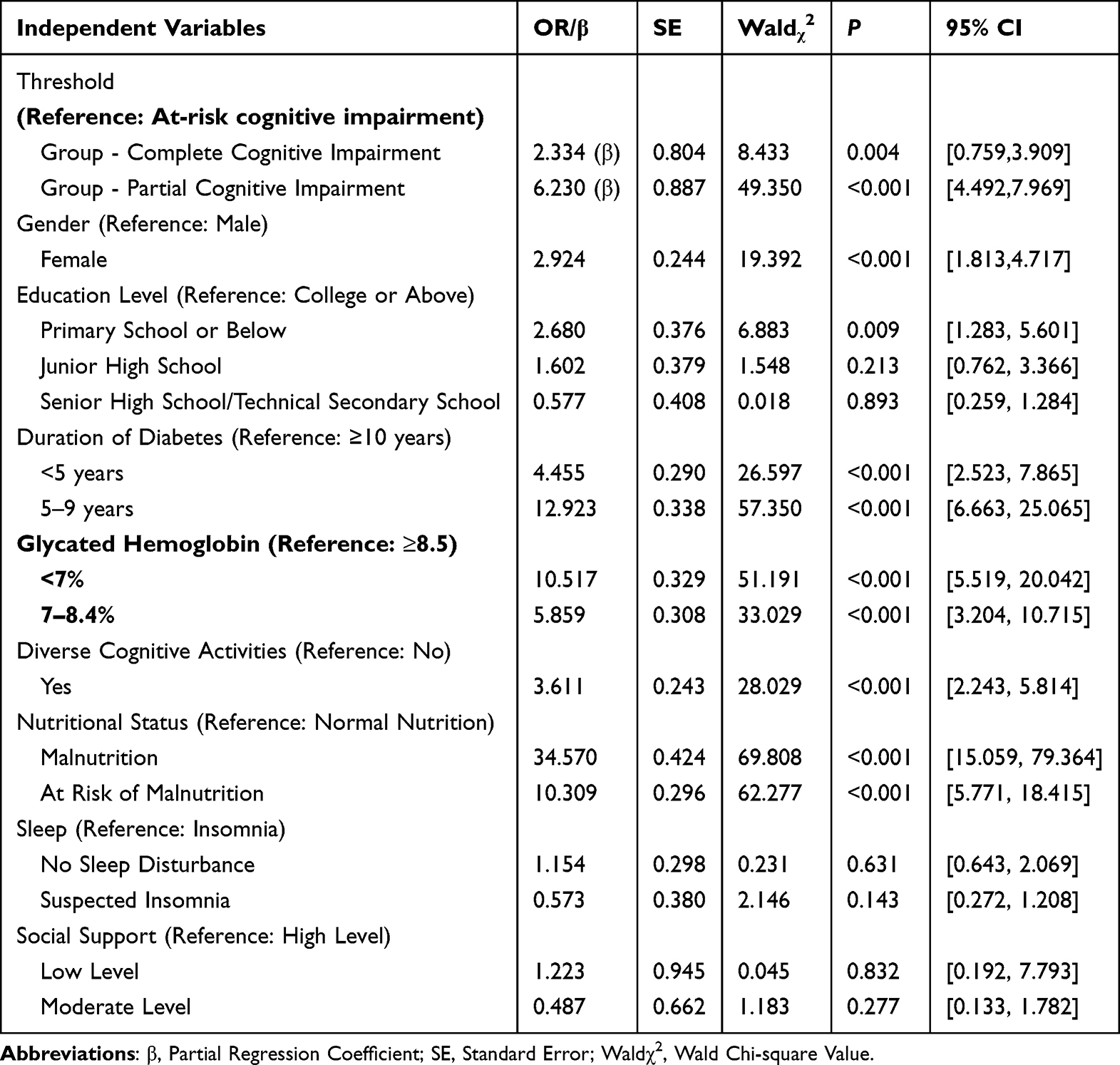 |
Table 4 Logistic Regression Analysis of the Factors Influencing Cognitive Frailty in Older Adults Living with Diabetes |
Discussion
Cognitive Impairment Stratification and Overall Trends in Older Adults Diabetes Patients
In recent years, the association between diabetes and cognitive impairment has been increasingly recognized. The present study adds to this evidence by identifying three distinct cognitive profiles among older adults with type 2 diabetes through latent profile analysis: complete impairment, partial impairment, and an at-risk impairment. This classification underscores the heterogeneity of cognitive decline in this population and highlights the importance of tailored intervention strategies. Beyond overall prevalence, we further examined demographic, clinical, and lifestyle factors associated with cognitive status, providing insights into potential targets for early prevention and management. These findings underscore the importance of early identification and intervention, which is consistent with the findings of Militaru et al (2024), who used the MMSE to show that type 2 diabetes combined with atrial fibrillation significantly increased the risk of cognitive decline, emphasizing the interaction between metabolic and cardiovascular comorbidities in accelerating cognitive deterioration.15
Gender and Education Level are Key Factors in Cognitive Impairment Among Older Adults Living with Diabetes
This study found that gender and education level are important factors influencing cognitive impairment in older adults living with diabetes. Analysis revealed that female patients have a significantly higher risk of cognitive impairment than males, which may be related to various physiological and social factors. On one hand, the sharp decline in estrogen levels after menopause may negatively impact the central nervous system, accelerating neurodegenerative changes, a mechanism also observed in neurodegenerative diseases like Alzheimer’s disease.16 On the other hand, women typically take on more caregiving roles in family and society, which may lead to increased psychological stress, further affecting cognitive function. Patients with lower education levels (elementary school or below) have a significantly higher risk of cognitive impairment. This aligns with the cognitive reserve theory, which suggests that individuals with higher cognitive reserve (eg, those with longer education) are better able to cope with cognitive decline through more flexible and efficient neural networks, while those with lower education may lack this adaptability.17
Further analysis of cognitive impairment stratification showed that gender and education level also play crucial roles in the graded transition of cognitive impairment. In the transition from risk-type to partial and complete cognitive impairment, the risk for female patients may accumulate, suggesting that this group should be a focus for early intervention. Meanwhile, patients with lower education levels show a higher risk across different cognitive stages, emphasizing the need for education and cognitive training before cognitive function becomes severely impaired to enhance cognitive reserve.
Diabetes Duration and Blood Glucose Control Significantly Impact Cognitive Impairment in Older Adults Living with Diabetes
Diabetes duration, blood glucose control, and nutritional status are significant factors influencing cognitive impairment in older adults living with diabetes. The risk of cognitive impairment increases with longer diabetes duration. Patients with a duration of less than 5 years have a significantly lower risk, while those with a 5–9 year duration show a notable increase in risk. This trend suggests that prolonged high blood glucose levels may exacerbate oxidative stress and chronic inflammation, leading to microvascular changes and neuronal damage, which in turn contribute to cognitive decline.18
Blood glucose control is also an independent factor influencing cognitive function. Studies show that patients with an HbA1c level below 7% have a lower risk of cognitive impairment, while those with an HbA1c between 7%-8.4% exhibit a significantly higher risk. This suggests that poor long-term blood glucose control is associated with more severe cognitive impairment. Previous research has also demonstrated that higher HbA1c levels are significantly correlated with brain volume reduction and impaired executive function in older adults living with diabetes.19 Therefore, blood glucose management in diabetes patients should focus not only on minimizing short-term fluctuations but also on long-term stability to reduce the cumulative cognitive damage caused by chronic hyperglycemia.
In addition to the unidirectional effect of diabetes on cognitive decline, previous studies have highlighted a bidirectional relationship between the two conditions. On one hand, diabetes increases the risk of cognitive impairment through mechanisms such as insulin resistance, chronic hyperglycemia, vascular injury, and neuroinflammation.20 On the other hand, cognitive impairment may exacerbate diabetes progression by reducing patients’ ability to adhere to treatment regimens, monitor blood glucose, and maintain a healthy lifestyle.21 In particular, impaired executive function and memory deficits can result in poor medication compliance, irregular diet, and higher risk of hypoglycemia, which in turn further deteriorate glycemic control. This vicious cycle underscores the importance of simultaneously addressing both metabolic and cognitive health in elderly diabetes patients, suggesting that comprehensive management strategies should include regular cognitive screening and early interventions to break this cycle.
The Impact of Intellectual Activities, Depression, and Nutrition on Cognitive Impairment in Older Adults Living with Diabetes
This study found that the frequency of intellectual activity participation and nutritional status are important protective factors for cognitive impairment in older adults living with diabetes. Patients who frequently engaged in intellectual activities had a significantly lower risk of cognitive impairment compared to those with lower participation frequencies. Diverse intellectual activities, such as reading, playing chess, writing, or socializing, not only promote neuroplasticity but also help delay cognitive decline by activating cognitive networks and increasing cognitive reserve.22 Particularly in older age, engaging in cognitively stimulating activities is considered one of the most effective strategies for reducing the risk of dementia.
Good nutritional status plays a crucial protective role in cognitive function. Malnourished patients face a significantly higher risk of cognitive impairment, highlighting the importance of nutrition in maintaining brain health. In particular, deficiencies in specific micronutrients (such as vitamin B12, vitamin D, and polyunsaturated fatty acids) may accelerate neuronal degeneration and cognitive decline.23 Studies have shown that deficiencies in vitamin B12 and folic acid are closely associated with cognitive impairment, while unsaturated fatty acids have anti-inflammatory and neuroprotective effects that help improve cognitive status23,24 Therefore, in the comprehensive management of living with diabetes, dietary intervention should be a key measure. Personalized nutrition guidance and dietary supplementation can optimize patient health and further reduce the risk of cognitive impairment.
In addition, this study used the Geriatric Depression Scale (GDS) to assess depressive symptoms. However, unlike some previous studies reporting a frequent co-occurrence of cognitive decline and depression,25 depression was not significant in our univariate analysis and was therefore not included in the latent profile stratification model. This discrepancy may be related to differences in sample size, patient population, cultural background, or the sensitivity of assessment tools. Nevertheless, previous research has suggested that depression may indirectly contribute to cognitive decline through mechanisms such as increased arterial stiffness and diastolic dysfunction, which warrants further investigation in larger-scale studies.25
Limitations
This study has several limitations. First, the cross-sectional design limits the ability to infer causal relationships, and the findings should be interpreted as associations only. Second, the study was conducted in a single tertiary hospital, which may restrict the generalizability of the findings to broader populations of older adults with diabetes. Third, although the MMSE is widely used, it is a screening tool with limited sensitivity for detecting subtle cognitive changes. Fourth, psychosocial and lifestyle factors were assessed via self-report, which may introduce recall or social desirability bias.
Furthermore, although we collected the number of diabetes-related comorbidities, we did not analyze the potential impact of specific comorbidities, including dyslipidemia, on cognitive outcomes. This represents an important limitation of the study. In addition, while we collected data on diabetes duration and fasting blood glucose levels, detailed information on the frequency of hypoglycemic events was not recorded. Although such information could be obtained from medical records, due to time and resource constraints, this variable was not included in the present analysis. Given the wide variety and scattered distribution of comorbidities, only the overall number of comorbid conditions was presented in the Results section, without examining individual comorbidities in detail.
Future multi-center, longitudinal, and interventional studies are warranted to validate, expand, and refine these findings, and to further investigate the effects of specific comorbidities on cognitive function in older adults with diabetes.
Conclusion
This study used Latent Profile Analysis (LPA) to explore the latent categorical characteristics of cognitive function in older adults living with diabetes. The patients were categorized into three groups: complete cognitive impairment, partial cognitive impairment, and at-risk cognitive impairment, which enhances understanding of the heterogeneity of cognitive dysfunction in older adults living with diabetes. Additionally, the study identified factors associated with cognitive impairment, such as gender, education level, diabetes duration, HbA1c levels, diversified cognitive activities, and nutritional status. By comparing different cognitive function categories, the study revealed which factors impact specific categories, providing preliminary evidence to inform risk stratification and potential management approaches for older adults living with diabetes. Future research should validate these associations through longitudinal and interventional studies before firm recommendations for clinical interventions can be made.
Trial Registration
This study was a cross-sectional observational study and therefore was not registered in a clinical trial registry, as it did not involve any health-related interventions or prospective assignment of participants to different treatment groups.
Use of the Chinese MMSE
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR (Invoice IN-00524826). The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due [The work of this manuscript is a part of a research project which is currently not finished.] but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Zhejiang Provincial People’s Hospital’s Research Ethics Committee (ZJPPHEC20221(079)). All participants provided written informed consent prior to enrollment. All methods were performed in accordance with the Declaration of Helsinki.
Funding
This research was funded by the Zhejiang Provincial Medical and Health Science and Technology Plan (2022KY586).
Disclosure
All authors declare no competing interests.
References
1. Hashemi R, Rabizadeh S, Yadegar A, et al. High prevalence of comorbidities in older adult patients with type 2 diabetes: a cross-sectional survey. BMC Geriatr. 2024;24(4):873. doi:10.1186/s12877-024-05483-3
2. You Y, Liu Z, Chen Y, et al. The prevalence of mild cognitive impairment in type 2 diabetes mellitus patients: a systematic review and meta-analysis. Acta Diabetol. 2021;58(6):671–685. doi:10.1007/s00592-020-01648-9
3. Hänninen T, Hallikainen M, Tuomainen S, et al. Prevalence of mild cognitive impairment: a population-based study in elderly subjects. Acta Neurol Scand. 2002;106(3):148–154 doi:10.1034/j.1600-0404.2002.01225.x.
4. Strachan MW, Reynolds RM, Marioni RE, et al. Cognitive function, dementia and type 2 diabetes mellitus in the elderly. Nat Rev Endocrinol. 2011;7(2):108–114 doi:10.1038/nrendo.2010.228.
5. Li J, Li X, Liu J, et al. Relationships between clinical symptoms, cognitive functioning, and TMS-evoked potential features in patients with major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2025 136;111184 doi:10.1016/j.pnpbp.2024.111184.
6. Komalasari R, Mpofu E, Chang HCR, et al. Higher dynamic balance performance was associated with cognitive function among U.S. community-dwelling low-income older adults. SAGE Open Nurs. 2024;10:23779608241296629 doi:10.1177/23779608241296629.
7. Guo L, Zhang M, Namassevayam G, et al. Identification of sleep quality clusters among stroke patients: a multi-center latent profile analysis study. Sleep Med. 2023;112:203–208 doi:10.1016/j.sleep.2023.10.019.
8. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198 doi:10.1016/0022-3956(75)90026-6.
9. Tombaugh TN, J N. McIntyre The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–935 doi:10.1111/j.1532-5415.1992.tb01992.x.
10. Rubenstein LZ, Harker JO, Salvà A, et al. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–72. doi:10.1093/gerona/56.6.M366
11. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. 2000;48(6):555–560. doi:10.1016/S0022-3999(00)00095-7
12. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the geriatric depression scale. J Am Geriatr Soc. 1999;47(7):873–878. doi:10.1111/j.1532-5415.1999.tb03848.x
13. Xiao SY. Social support rating scale. Chin Mental Health J. 1993;42–46.
14. Lim AJ, W M. Cheung Evaluating FIML and multiple imputation in joint ordinal-continuous measurements models with missing data. Behav Res Methods. 2022;54(3):1063–1077. doi:10.3758/s13428-021-01582-w
15. Militaru M, Lighezan DF, Tudoran C, et al. Connections between cognitive impairment and atrial fibrillation in patients with diabetes mellitus type 2. Biomedicines. 2024;12(3). doi:10.3390/biomedicines12030672
16. Iulita MF, Bejanin A, Vilaplana E, et al. Association of biological sex with clinical outcomes and biomarkers of Alzheimer’s disease in adults with Down syndrome. Brain Commun. 2023;5(2):fcad074. doi:10.1093/braincomms/fcad074
17. Yoneda T, Lewis NA, Knight JE, et al. The importance of engaging in physical activity in older adulthood for transitions between cognitive status categories and death: a coordinated analysis of 14 longitudinal studies. J Gerontol a Biol Sci Med Sci. 2021;76(9):1661–1667. doi:10.1093/gerona/glaa268
18. Tang X, Wang Y, Simó R, et al. The association between diabetes duration and domain-specific cognitive impairment: a population-based study. J Alzheimers Dis. 2023;91(4):1435–1446. doi:10.3233/JAD-220972
19. Yu JH, Kim REY, Park SY, et al. Association of long-term hyperglycaemia and insulin resistance with brain atrophy and cognitive decline: a longitudinal cohort study. Diabetes Obes Metab. 2023;25(4):1091–1100. doi:10.1111/dom.14958
20. Biessels GJ, Despa F. Cognitive decline and dementia in diabetes mellitus: mechanisms and clinical implications. Nat Rev Endocrinol. 2018;14(10):591–604. doi:10.1038/s41574-018-0048-7
21. Wang M, Guan X, Yan J, et al. Perceptions and responses to cognitive decline in people with diabetes: a systematic review of qualitative studies. Front Public Health. 2023;11:1076030. doi:10.3389/fpubh.2023.1076030
22. Ye KX, Sun L, Wang L, et al. The role of lifestyle factors in cognitive health and dementia in oldest-old: a systematic review. Neurosci Biobehav Rev. 2023;152:105286. doi:10.1016/j.neubiorev.2023.105286
23. Zhang C, Luo J, Yuan C, et al. Vitamin B12, B6, or folate and cognitive function in community-dwelling older adults: a systematic review and meta-analysis. J Alzheimers Dis. 2020;77(2):781–794 doi:10.3233/JAD-200534.
24. van Soest APM, van de Rest O, Witkamp RF, et al. Positive effects of folic acid supplementation on cognitive aging are dependent on ω-3 fatty acid status: a post hoc analysis of the FACIT trial. Am J Clin Nutr. 2021;113(4):801–809. doi:10.1093/ajcn/nqaa373
25. Tudoran M, Tudoran C, Ciocarlie T, et al. Aspects of diastolic dysfunction in patients with new and recurrent depression. PLoS One. 2020;15(1):e0228449. doi:10.1371/journal.pone.0228449
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.