Back to Journals » Psychology Research and Behavior Management » Volume 15
Cognitive Behavioral and Cognitive Remediation Strategies for Managing Co-Occurring Anorexia Nervosa and Elevated Autism Spectrum Traits
Authors Saure E ![]() , Ålgars M, Laasonen M, Raevuori A
, Ålgars M, Laasonen M, Raevuori A
Received 21 February 2022
Accepted for publication 13 April 2022
Published 20 April 2022 Volume 2022:15 Pages 1005—1016
DOI https://doi.org/10.2147/PRBM.S246056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Emma Saure,1,2 Monica Ålgars,1,3,4 Marja Laasonen,5 Anu Raevuori6,7
1Department of Psychology and Logopedics, Faculty of Medicine, University of Helsinki, Helsinki, Finland; 2BABA Center and Department of Clinical Neurophysiology, Children’s Hospital, Helsinki, Finland; 3Department of Psychiatry, Helsinki University Hospital, Helsinki, Finland; 4Department of Psychology, Åbo Akademi University, Turku, Finland; 5Logopedics, School of Humanities, Philosophical Faculty, University of Eastern Finland, Joensuu, Finland; 6Department Psychiatry, Division of Adolescent Psychiatry, Helsinki University Hospital, Helsinki, Finland; 7Clinicum, Department of Public Health, University of Helsinki, Helsinki, Finland
Correspondence: Emma Saure, Department of Psychology and Logopedics, Faculty of Medicine, University of Helsinki, P.O. Box 21, Helsinki, FI-00014, Finland, Tel +358443035828, Email [email protected]
Abstract: Anorexia nervosa (AN) is a potentially severe eating disorder whose core characteristics include energy intake restriction leading to low body weight. Autism spectrum disorder (ASD) is a developmental disorder characterized by deficits in social interaction and communication as well as repetitive, stereotyped behavior and interests. Both high ASD traits and diagnosed ASD are overrepresented among individuals with AN, and AN and ASD appear to share certain neurocognitive features. These features are associated with the severity of eating disorder symptoms and prolongation of AN. Thus, individuals with AN and high ASD traits or ASD may benefit less from traditional treatment when compared to those with low ASD traits. No previous reviews have summarized what is known about treatment adaptations for individuals with AN and high ASD traits or ASD. The purpose of this narrative review was to investigate the feasibility of cognitive remediation therapy (CRT), cognitive remediation and emotional skill training (CREST), and cognitive behavioral therapy (CBT), and give an overview of treatment modifications for individuals with AN and co-occurring ASD or high ASD traits. We found nine studies that fulfilled our inclusion criteria. The combined results suggest that individuals with AN and high ASD traits or ASD benefit less from CRT, CREST, and CBT than those with AN and low ASD traits. However, CRT and CREST administered in individual format may be associated with improved cognitive flexibility, motivation for change, and decreased alexithymia among adults with AN and high ASD traits or ASD. Individuals with comorbid AN and ASD themselves highlight the importance of treatment adaptations that take the characteristics of ASD into account. In the future, controlled studies of the treatment strategies for individuals with AN and ASD/high ASD traits are needed in order to improve the outcome of individuals with this challenging comorbidity.
Keywords: anorexia nervosa, feeding and eating disorders, autism spectrum disorder, treatment, cognitive remediation, cognitive behavioral therapy
Introduction
Anorexia nervosa (AN) is an eating disorder whose core characteristics include restriction of energy intake leading to low body weight, intense fear of gaining weight, or persistent behavior that interferes with weight gain and a disturbance in the way in which one’s body weight/shape is experienced.1 Autism spectrum disorder (ASD) is a developmental disorder characterized by deficits in social interaction and communication as well as repetitive, stereotyped behavior and interests.1 Elevated ASD traits are overrepresented among individuals with AN.2–7 Many studies report that elevated ASD traits occur both before and after acute AN3,8–11 and thus these traits are unlikely to occur only because of consequences of starvation or other acute illness-related process. Furthermore, a subgroup of individuals with AN fulfills the diagnostic criteria of ASD.2–7 Studies that have actively screened for ASD among individuals with current AN have reported its prevalence to be between 10% and 30% in female patients with AN.3–5,12 In registry-based studies, the prevalence of ASD among females with AN has been reported to be between 1.3% and 2.5%, while the corresponding prevalence of ASD among the control females has been reported to be 0.6%.8,9 In these studies, individuals with AN also have a highly elevated risk of receiving a later diagnosis of ASD, and the risk is higher for male than for female individuals.13,14
AN and ASD appear to share certain neurocognitive features, that is, difficulties in social cognition, cognitive inflexibility, weak central coherence, and atypical sensory processing.15–19 Difficulties in social cognition include challenges in emotion recognition, poor theory of mind, low empathy, and difficulties in interpersonal relationships.8,18,20,21 Individuals with AN and ASD have been described having developed disturbed eating behavior as a response to social challenges.22,23 Cognitive flexibility refers to the ability to shift between tasks and adapt to changing rules and situations. Challenges in cognitive flexibility may result in the rigid behavior typical to AN and ASD and contribute to the development of rigid eating pattern including the urge to count and monitor calories and weight.17,22,23 Weak central coherence, in turn, refers to increased attention to detail and challenges in global integration and processing information in its context.24 This may be involved in attentional bias towards food and body.25 Sensory processing atypicality may manifest as sensory sensitivity and sensory avoidance, for example, sensitivity for some food textures or tastes, which may underlie some eating disturbances.16 These ASD-related neurocognitive features have been reported to be associated with the severity of eating disorder symptoms among acutely ill individuals with AN.9,16 These traits are also suggested to contribute to the development and prolongation of AN.23,26–28 Some studies have not found an association between ASD traits and treatment outcome of AN,29,30 but several other studies report that treatment outcome is poorer among individuals with AN and ASD or elevated ASD traits when compared to those with low ASD traits.7,31–33 It has been suggested that neurocognitive features of ASD may contribute to the lack of treatment response to traditional treatments among individuals with co-occurring AN and ASD or high ASD traits.22,23 To summarize, ASD-related neurocognitive characteristics may predispose to disordered eating behavior, and AN in individuals with high ASD traits or ASD is likely to differ from AN in individuals with low ASD traits. Individuals with this comorbidity also appear to benefit less from the current treatment methods for AN, when compared to individuals with AN and low ASD traits. Recent studies have indeed highlighted the need for developing tailored treatments for individuals with AN and ASD or high ASD traits.
Cognitive remediation therapy (CRT) is a treatment method that could benefit individuals with AN and co-occurring ASD. CRT includes training in neurocognitive skills, for example, cognitive flexibility and central coherence, which, among other things, facilitates functioning in daily life.34–36 CRT can also include training of emotional skills (cognitive remediation and emotional skill training, CREST), targeted at social and emotional difficulties.37 Besides CRT and CREST, it has been suggested that also cognitive behavioral therapy (CBT) could be modified in ways that take high ASD traits into account. The underlying assumption in CBT is that one can learn to identify and alter dysfunctional thinking, emotional responses, and behaviors.38 Enhanced forms of CBT (CBT -E), targeting biased body image and over evaluation of shape and weight and their control, is commonly used in the treatment of AN.39 However, among individuals with AN and ASD, the ASD traits such as the effect of sensory sensitivity on disordered eating might be beneficial to consider one of the treatment target of CBT.16 Further, other adaptations in treatment target and settings that take into account the effects of ASD traits, would also be beneficial for individuals with AN and ASD. However, no previous reviews have summarized literature regarding treatment adaptations for individuals with AN and co-occurring ASD. The purpose of this narrative review was to investigate the feasibility of CRT, CREST, and CBT and give an overview of treatment modifications for individuals with AN and co-occurring ASD. CBT, CREST, and CBT were selected for this review, because CBT is one of the most commonly used treatments for both AN and ASD and their psychiatric co-morbidities and, as outlined above, CRT and CREST target some of the central common features of AN and ASD.40,41
Methodology
In order to include all relevant studies in this narrative review, a systematic search was conducted. To be included in the review, the studies were required to 1) be published in English and in a peer-reviewed journal, and 2) be original research articles that included participants with diagnosed AN and diagnosed ASD or high ASD traits, and 3) to investigate treatment in some of the following areas: CRT, CREST, CBT, or treatment adaptations. High ASD traits were defined as ASD traits above the cut-off for high ASD traits/ASD in the questionnaire or observation-based measurement method. We set no limitations for study designs. Case studies and qualitative studies were also included as only a few quantitative studies focusing on treatment for co-occurring AN and ASD or high ASD traits emerged in searches. A systematic search in the Ovid Medline, Ovid PsycINFO, and the PubMed databases was conducted using the following terms: “eating disorders” or “feeding and eating disorders” or “anorexia nervosa” and “autism spectrum disorder” and “treatment” or “cognitive behavioral therapy” or “cognitive remediation” or “therapy”. All searches were conducted on January 19th, 2022. The literature search resulted in 575 articles. After the removal of duplicates, 374 articles were screened for title and abstract. A total of 331 articles were excluded, and the remaining 43 articles were screened based on full text, leading to the exclusion of another 34 articles. The final sample consisted of 9 articles. Two authors (E.S. and M.Å.) independently screened the resulting articles for their appropriateness for inclusion. See Figure 1 for the Flow chart.
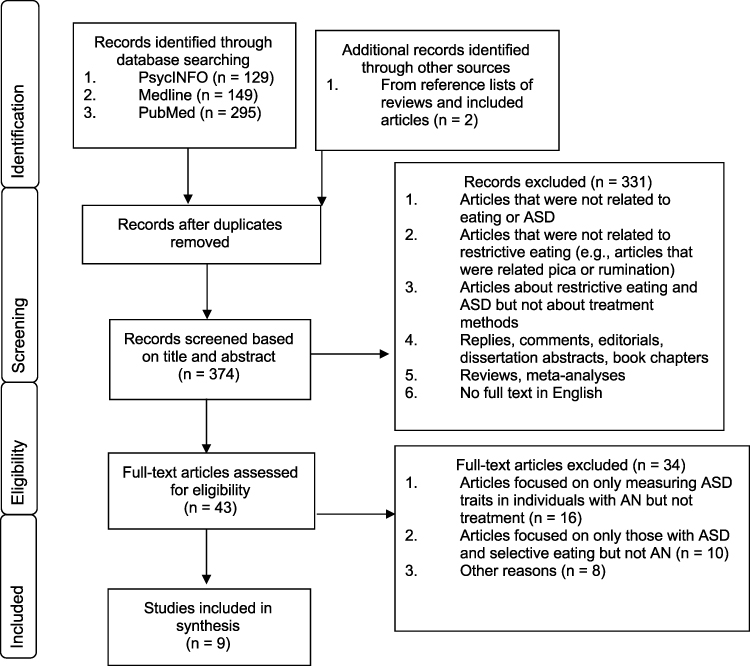 |
Figure 1 Study selection process. |
Results
Four of the articles focused on CRT, including one case study. One study focused on CREST. We found one qualitative study in which participants’ experiences of CBT were included as one interview theme. In addition, we found four studies that investigated treatment adaptations. Of these, one was a case study focusing on a family-based intervention, one focused on sensory issues, and two studies used qualitative interviews and focused on treatment adaptations. See Table 1 for a summary of the included studies.
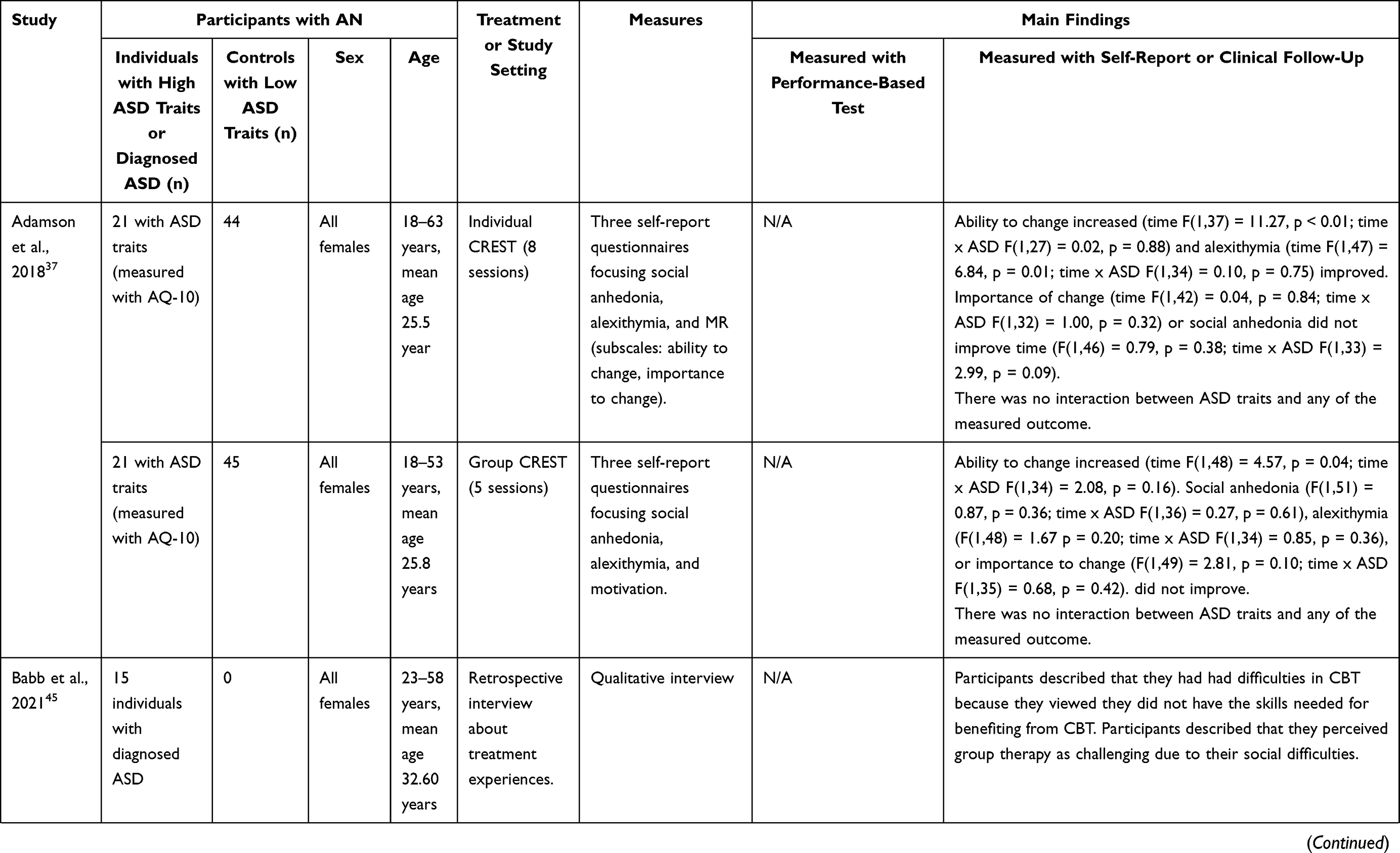 | 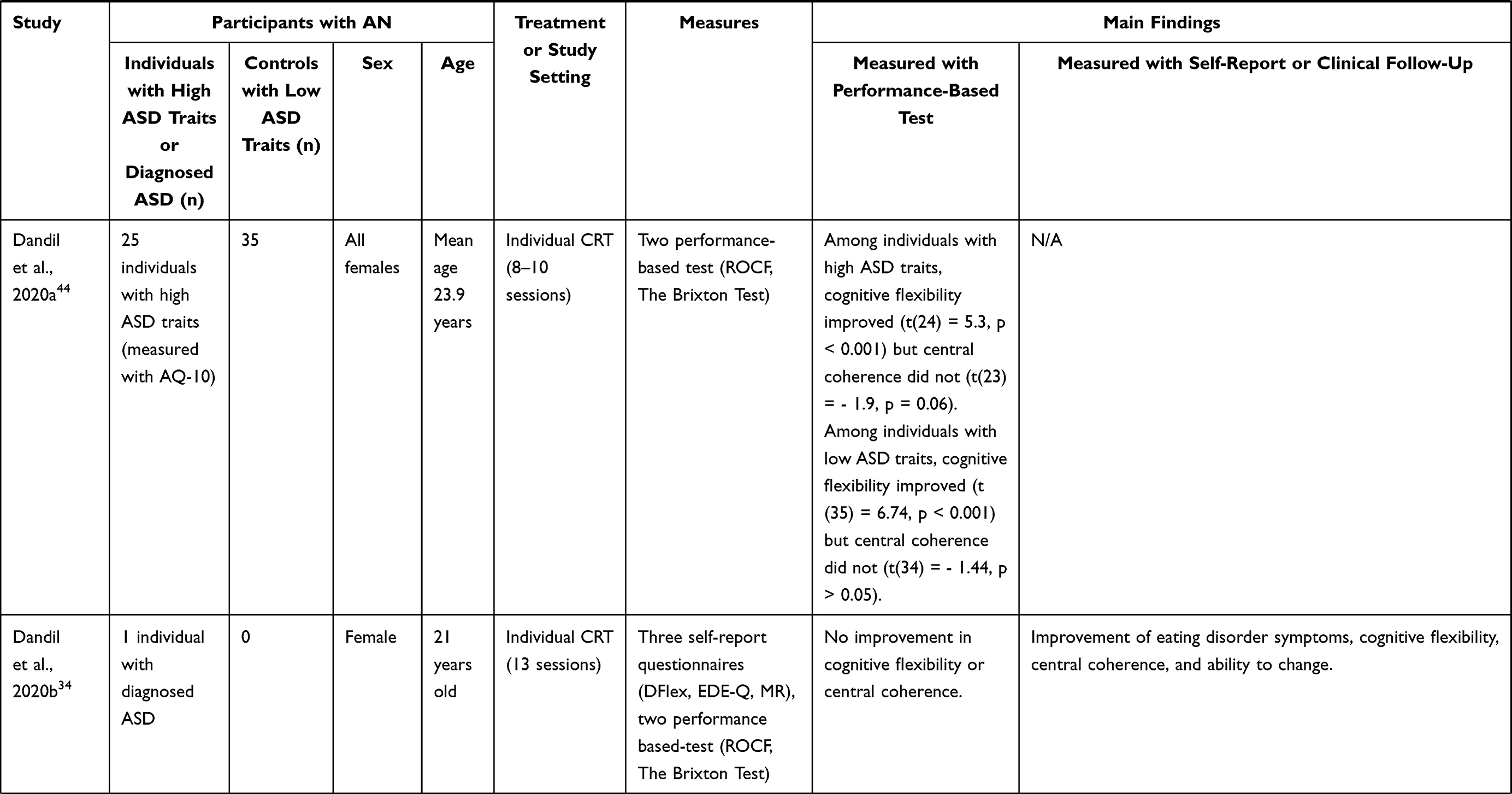 | 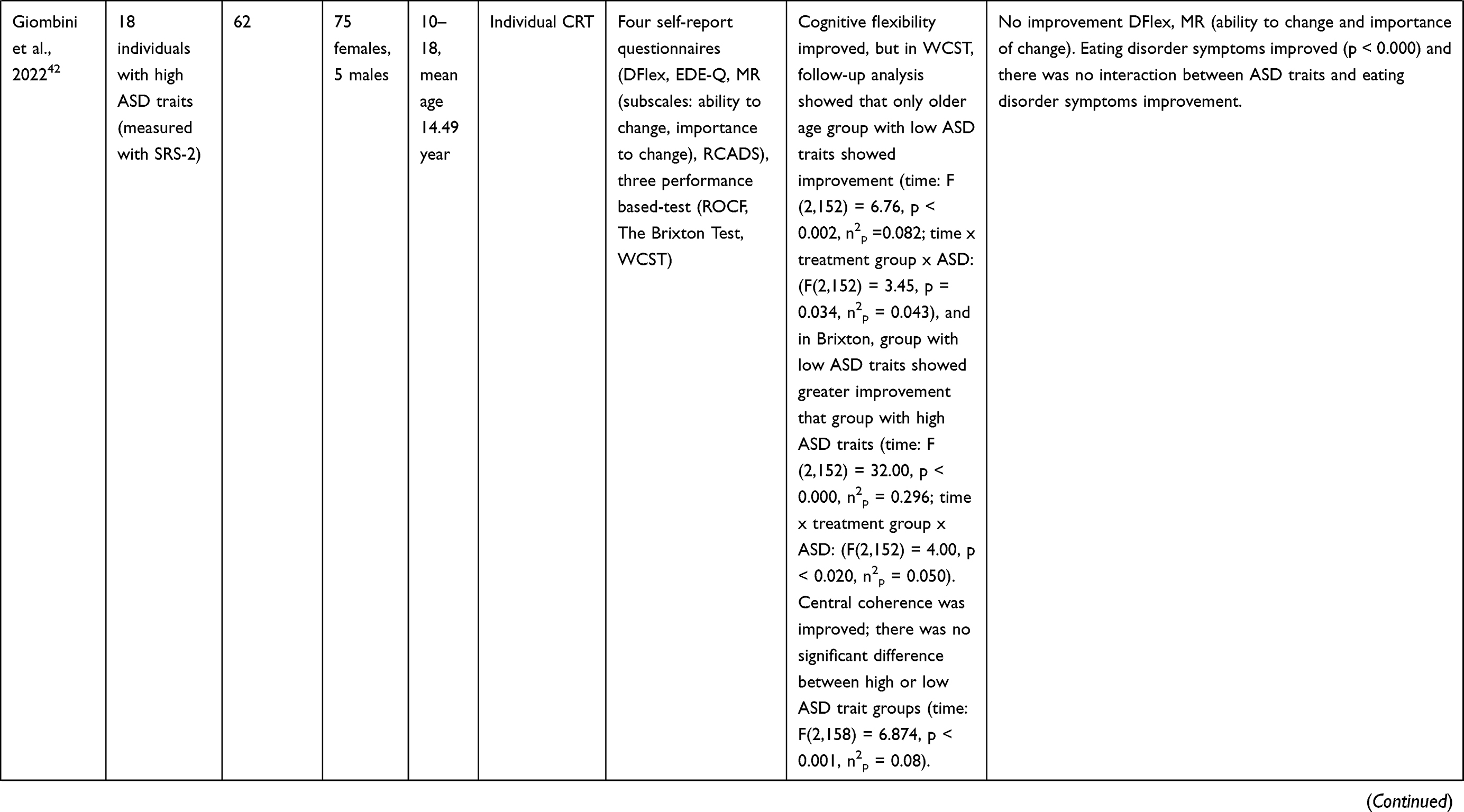 | 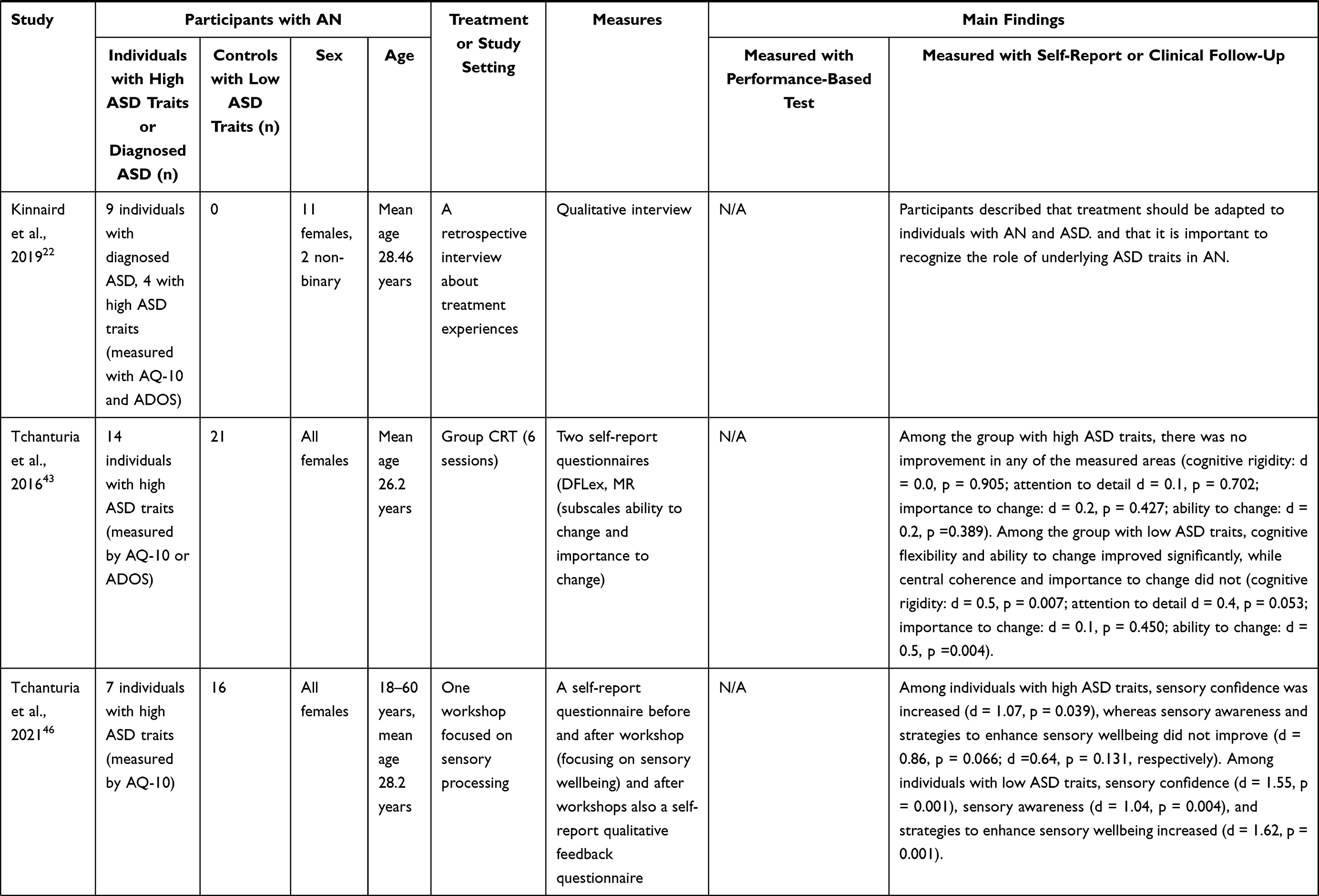 |
Table 1 Characteristics and Main Results of the Included Studies |
CRT, CREST, and CBT
Two of the four studies34,37,42,43 investigated individual CRT and one investigated group CRT among individuals with AN and high ASD traits. One was a case study that described CRT in females with AN and diagnosed ASD.44 All four studies focused on CRT for cognitive flexibility and central coherence. One study found no improvement after group CRT among adults with high ASD traits whereas among those with low ASD traits cognitive flexibility improved.43 Other study found improvement in cognitive flexibility in performance-based tests after individual CRT among adolescent participants with high and low ASD traits, but the improvement was more subtle among individuals with high ASD traits when compared to those with low ASD traits (Wisconsin card sorting task: combined results of both group including individuals with low and high ASD traits).42 Further, one study found improvement in cognitive flexibility measured with a performance-based test after individual CRT among adults with high and low ASD traits.44 One of the studies with adolescent participants who received individual CRT found improvement in central coherence both among those with high and low ASD traits,42 whereas other studies found no improvement in central coherence.43,44 Further, in the case study with adult women with AN and ASD, self-reported cognitive flexibility and central coherence were improved after CRT, but in the performance-based test, no improvement was observed.34
We found one study which investigated CREST.37 The study included two groups of adult participants; one group received individual CREST, while the another group received group CREST.37 The authors reported that CREST in both individual and group formats was associated with participants’ increased self-reported motivation for change, and that this improvement was seen among both those with high and low ASD traits. Further, individual CREST, but not group CREST, was associated with decreased alexithymia among both individuals with high and low ASD traits.
We found no studies that applied CBT for individuals with AN and high ASD traits or ASD. However, one qualitative study included individuals with AN and diagnosed ASD, who were interviewed concerning their experiences in treatment that included CBT.45 Participants described experiencing difficulties in CBT because they felt that they lacked some basic skills, such as ability to generalize and transfer learned things to real-life situations, necessary for benefitting from this treatment. Furthermore, they had experienced group situations challenging due to their experienced social challenges.
To conclude, individuals with AN and high ASD traits or ASD may benefit less from CRT, CREST, and CBT than those with AN and low ASD traits. However, this very limited body of evidence suggests that CRT and CREST administered in individual format may be associated with improved cognitive flexibility, central coherence, and motivation for change, and decreased alexithymia among adults with AN and high ASD traits or ASD.
Treatment Adaptations
We found two studies that applied treatment adaptations for individuals with AN and high ASD traits or ASD. In one study, women with AN and low or high ASD traits participated in a workshop focusing on sensory processing.46 The workshop included psychoeducation about sensory processing and group discussion about sensory experiences. Further, participants made their own sensory item, for example, scented hand cream. The authors reported that confidence in managing sensory wellbeing was increased among both groups, that is, in those with high and low ASD traits. However, among those with low ASD traits, sensory wellbeing, and sensory awareness also increased, suggesting that those with low ASD traits benefited more from the workshop. Another study was a case study including individuals with AN and high ASD traits who underwent Maudsley anorexia nervosa treatment for adults (MANTRA), with treatment adaptations targeted specifically for ASD-related difficulties.47 In this study, inflexibility, social difficulties, and social isolation were considered as important underlying factors for anorexia nervosa, and treatment was targeted specifically for these. As a result, assessed only with a qualitative clinical follow-up, flexibility was reported to increase and some improvement in social difficulties was also noted.
Two qualitative studies examined how individuals with AN with high ASD traits or diagnosed ASD experienced treatment.22,45 In both studies, participants described the experience of being misunderstood in treatment due to their ASD-related traits and behavior. They reported, for example, that they were considered resistant, uncooperative, and difficult because of their slow progress, social difficulties, or inability to eat certain foods due to their of atypical sensory processing. Further, they described that their social challenges made it difficult for them to engage in treatment and create a satisfying relationship with health-care professionals. They suggested adaptations to the treatment of AN in order to take ASD traits into account. These were suggested to include adaptations to the communication style and treatment environment, offering more flexible and individualized approaches, considering the possibility that ASD traits may underlie AN symptoms; and increasing the awareness of the specific manifestation of AN among those with ASD.22,45 To conclude, studies suggest that individuals with AN and high ASD traits or ASD appear to benefit less from CRT, CREST, and CBT compared to those with low ASD traits. In addition, individuals with comorbid AN and ASD themselves highlight the importance of treatment adaptations that take the ASD traits underlying AN into account.
Discussion
The purpose of this narrative review was to evaluate how individuals with AN and ASD or high ASD traits respond to CRT, CREST, or CBT, and to investigate what kinds of treatment modifications might be beneficial for them. The combined results suggest that individual CRT and CREST may improve cognitive flexibility, central coherence, and motivation in individuals with AN and ASD traits, but the improvement was more subtle than among those with AN and low ASD traits. Individuals with AN and ASD also report that they encounter difficulties in treatment related to their ASD traits, and that they wish for more flexible and individualized treatment approaches, as well as a greater understanding of ASD traits underlining their AN symptoms. Our findings suggest that adaptations to the treatments appear to benefit individuals with AN and ASD or high ASD traits. However, given the small number of studies, these results should be considered with caution.
Social difficulties are widespread and generalized among those with AN and ASD.15 In individuals with AN and co-occurring ASD, social difficulties may underlie eating disorder behaviors and cause struggling both in treatment settings and in peer relationships. Group situations may be difficult for these individuals, and therefore, as the results of the previous study suggest, CREST in its individual form may be effective and enable flexible approaches for each individual’s specific difficulties.37,45 On the other hand, these individuals may also benefit from practicing social interaction, such as structured group conversations.45 As a part of their treatment, individuals with AN and ASD may also benefit from additional support to engage in age-appropriate peer relationships, because their social network may be limited, and, making new friends may be difficult for them.48 Further, when working with families, it is worth keeping in mind a relatively high heritability of ASD,49 which tend to manifest as difficulties in social communication and interaction among biological relatives, such as parents.47 In family-based treatment settings, the whole family may thus require extra support.47,48
In the context of cognitive inflexibility, there is some evidence that individual CRT may improve cognitive rigidity among individuals with AN and high ASD traits or co-occurring ASD.44 Among individuals with AN and ASD traits or ASD, cognitive rigidity usually precedes AN, but during acute AN, it may be emphasized even further.17,19 Cognitive inflexibility has also been shown to be associated with acute eating disorder symptoms.9 Individuals with AN and ASD describe that their rigidity and inflexibility have contributed to development of rigid routines around eating and also made it difficult to change eating habits during treatment.22 Cognitive inflexibility could therefore be an important factor contributing for poorer treatment outcomes among individuals with AN and ASD or high ASD traits. These findings suggest that cognitive inflexibility would be an important treatment target, and since individual CRT seems to improve cognitive inflexibility, it could be a promising addition to other treatments.
We found only one study focusing on sensory processing.46 In this study, participants received psychoeducation and discussed their experiences of sensory processing in workshops, which they experienced beneficial, but no planned modifications to their treatment were made. Among individuals with ASD, selective eating based on sensory processing atypicality is very common even in the absence of a co-occurring clinical eating disorder.50 Therefore, it is likely that in individuals with both AN and ASD, selective eating has occurred to some degree even before the onset of a clinical eating disorder. Among individuals with both AN and ASD, it may therefore be essential to clarify what kind of food they ate before the onset of AN, because it is likely that they have always avoided certain textures or tastes.48 It has also been suggested that foods offered in the treatment would be bland, mild, and of soft texture; and that predictability of the served food would be valued by not varying menus that much, and providing photographs of foods beforehand.51 Modifications of served food for those with ASD and prominent sensory processing atypicalities may be of importance, because without such modifications these individuals may not be able to engage in treatment. However, after the individual has achieved some degree of weight restoration and is committed to treatment, it is also important to widen the accepted food repertoire.48 In the context of ASD, numerous strategies have been developed to treat selective eating and some of these treatment strategies may also be beneficial for individuals with AN and ASD. In addition, it is likely that among those with ASD, some overlap exists between AN and avoidant/restrictive food intake disorder (ARFID), in which atypical sensory processing is one of the main factors underlying the eating disturbance. Thus, CBT that has been developed for ARFID and includes particular treatment strategies for eating disturbances based on sensory avoidance may also be beneficial for some individuals with AN and ASD.52,53 See Table 2 for a summary of treatment adaptations.
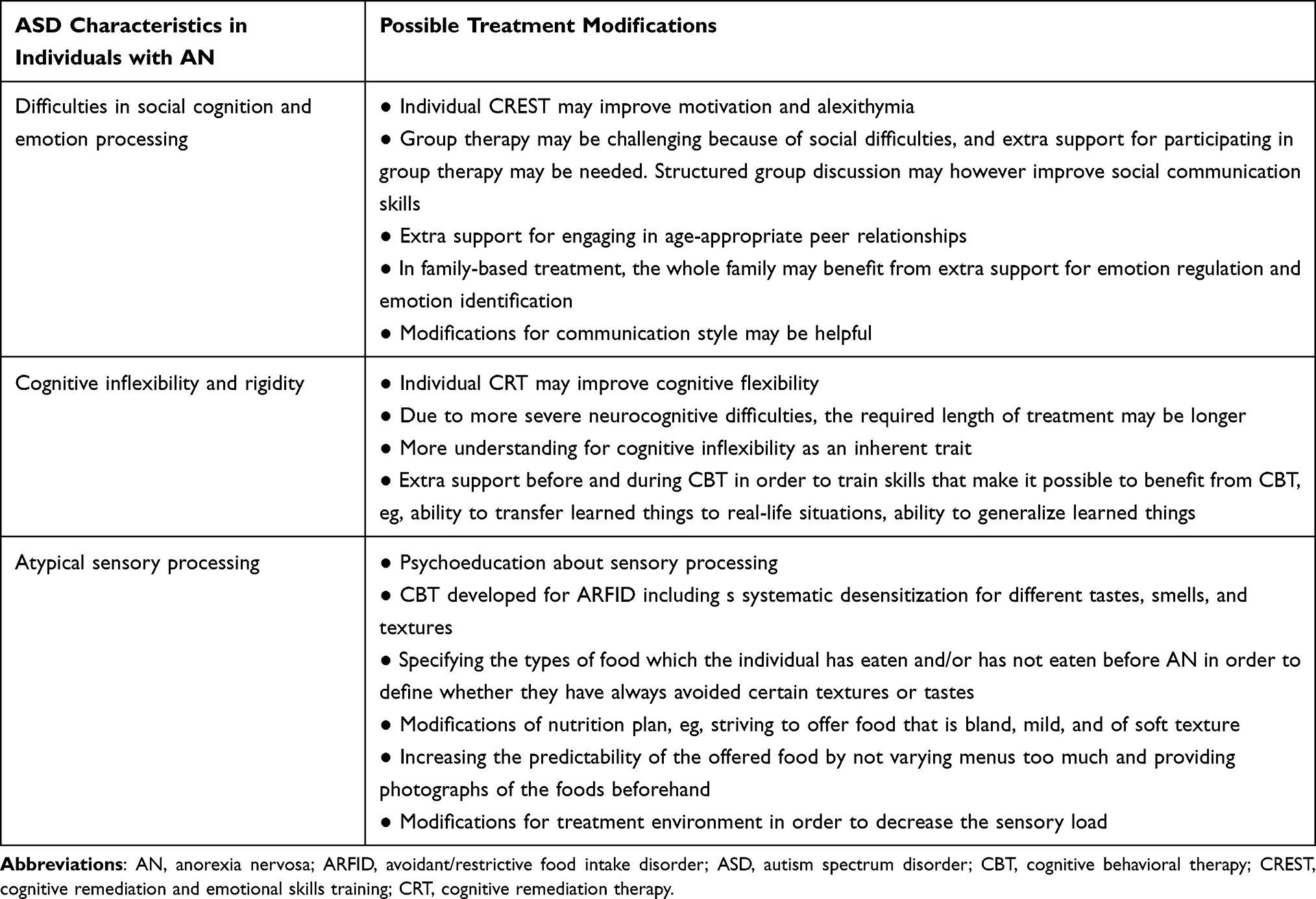 |
Table 2 Treatment Adaptations for Individuals with Anorexia Nervosa and Autism Spectrum |
Limitations
The main limitations of this review include overall low number of studies and relatively small samples, high heterogeneity of study designs, and low number (five) of controlled studies. The outcomes of treatment were measured with different methods across studies and therefore the results of the studies may not be directly comparable. Also, in five of the studies, the treatment outcome was assessed only with self-report measures. Further, most of the participants in the studies did not have a formal ASD diagnosis but only high ASD traits measured with self-report, most often by the Autism Quotient −10 (AQ-10). Participants were mostly women. Because it has been shown that sex and gender differences affect the presentation of ASD,54 the results may not be generalizable to males or non-binary individuals.
Conclusions
The limited body of evidence covered in this review suggests that individually provided forms of CRT and CREST appear to be associated with improved social skills, cognitive flexibility, and central coherence in individuals with AN and ASD or ASD traits. Among these individuals, atypical sensory processing should be considered in feeding and nutritional treatment and provide appropriate modifications. In the future, large controlled studies of the treatment strategies for individuals with AN and ASD/high ASD traits are needed in order to improve the outcome of individuals with this challenging comorbidity.
Disclosure
Professor Anu Raevuori reports equity ownership in Meru Health Inc., outside the submitted work. The authors have no other conflicts of interest to declare in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM.
2. Fuglset TS. Set-shifting, central coherence and decision-making in individuals recovered from anorexia nervosa: a systematic review. J Eat Disord. 2019;7(22):14. doi:10.1186/s40337-019-0251-5
3. Wentz E, Lacey JH, Waller G, Rastam M, Turk J, Gillberg C. Childhood onset neuropsychiatric disorders in adult eating disorder patients. A pilot study. Eur Child Adolesc Psychiatry. 2005;14(8):431–437. doi:10.1007/s00787-005-0494-3
4. Huke V, Turk J, Saeidi S, Kent A, Morgan JF. Autism spectrum disorders in eating disorder populations: a systematic review. Eur Eat Disord Rev. 2013;21(5):345–351. doi:10.1002/erv.2244
5. Vagni D, Moscone D, Travaglione S, Cotugno A. Using the Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R) disentangle the heterogeneity of autistic traits in an Italian eating disorder population. Res Autism Spectr Disord. 2016;32:143–155. doi:10.1016/j.rasd.2016.10.002
6. Renwick B, Musiat P, Lose A, et al. Neuro- and social-cognitive clustering highlights distinct profiles in adults with anorexia nervosa. Int J Eat Disord. 2015;48(1):26–34. doi:10.1002/eat.22366
7. Rastam M, Gillberg C, Wentz E. Outcome of teenage-onset anorexia nervosa in a Swedish community-based sample. Eur Child Adolesc Psychiatry. 2003;12 Suppl 1(9212296):I78–190. doi:10.1007/s00787-003-1111-y
8. Krug I, Penelo E, Fernandez-Aranda F, et al. Low social interactions in eating disorder patients in childhood and adulthood: a multi-centre European case control study. J Health Psychol. 2013;18(1):26–37. doi:10.1177/1359105311435946
9. Roberts ME, Tchanturia K, Treasure JL. Exploring the neurocognitive signature of poor set-shifting in anorexia and bulimia nervosa. J Psychiatr Res. 2010;44(14):964–970. doi:10.1016/j.jpsychires.2010.03.001
10. Solmi F, Bentivegna F, Bould H, et al. Trajectories of autistic social traits in childhood and adolescence and disordered eating behaviours at age 14 years: a UK general population cohort study. J Child Psychol Psychiatry. 2021;62(1):75–85. doi:10.1111/jcpp.13255
11. Dinkler L, Rydberg Dobrescu S, Rastam M, et al. Visual scanning during emotion recognition in long-term recovered anorexia nervosa: an eye-tracking study. Int J Eat Disord. 2019;52(6):691–700. doi:10.1002/eat.23066
12. Boltri M, Sapuppo W. Anorexia nervosa and autism spectrum disorder: a systematic review. Psychiatry Res. 2021;306:114271. doi:10.1016/j.psychres.2021.114271
13. Koch SV, Larsen JT, Mouridsen SE, et al. Autism spectrum disorder in individuals with anorexia nervosa and in their first- and second-degree relatives: Danish nationwide register-based cohort-study. Br J Psychiatry J Ment Sci. 2015;206(5):401–407. doi:10.1192/bjp.bp.114.153221
14. Dinkler L, Taylor MJ, Rastam M, et al. Anorexia nervosa and autism: a prospective twin cohort study. J Child Psychol Psychiatry. 2020;62:316–326. doi:10.1111/jcpp.13265
15. Kinnaird E, Tchanturia K. Looking beneath the surface: distinguishing between common features in autism and anorexia nervosa. J Behav Cogn Ther. 2021;31(1):3–13. doi:10.1016/j.jbct.2020.09.001
16. Brand-Gothelf A, Parush S, Eitan Y, Admoni S, Gur E, Stein D. Sensory modulation disorder symptoms in anorexia nervosa and bulimia nervosa: a pilot study. Int J Eat Disord. 2016;49(1):59–68. doi:10.1002/eat.22460
17. Westwood H, Stahl D, Mandy W, Tchanturia K. The set-shifting profiles of anorexia nervosa and autism spectrum disorder using the Wisconsin Card Sorting Test: a systematic review and meta-analysis. Psychol Med. 2016;46(9):1809–1827. doi:10.1017/S0033291716000581
18. Oldershaw A, Hambrook D, Stahl D, Tchanturia K, Treasure J, Schmidt U. The socio-emotional processing stream in Anorexia Nervosa. Neurosci Biobehav Rev. 2011;35(3):970–988. doi:10.1016/j.neubiorev.2010.11.001
19. Saure E, Laasonen M, Raevuori A. Anorexia nervosa and comorbid autism spectrum disorders. Curr Opin Psychiatry. 2021;34(6):569–575. doi:10.1097/YCO.0000000000000742
20. Bora E, Köse S. Meta-analysis of theory of mind in anorexia nervosa and bulimia nervosa: a specific impairment of cognitive perspective taking in anorexia nervosa?: toM IN ED. Int J Eat Disord. 2016;49(8):739–740. doi:10.1002/eat.22572
21. Kerr-Gaffney J, Harrison A, Tchanturia K. Autism spectrum disorder traits are associated with empathic abilities in adults with anorexia nervosa. J Affect Disord. 2020;266(h3v, 7906073):273–281. doi:10.1016/j.jad.2020.01.169
22. Kinnaird E, Norton C, Stewart C, Tchanturia K. Same behaviours, different reasons: what do patients with co-occurring anorexia and autism want from treatment? Int Rev Psychiatry Abingdon Engl. 2019;31(4):308–317. doi:10.1080/09540261.2018.1531831
23. Brede J, Babb C, Jones C, et al. “For me, the anorexia is just a symptom, and the cause is the autism”: investigating restrictive eating disorders in autistic women. J Autism Dev Disord. 2020;50(12):4280–4296. doi:10.1007/s10803-020-04479-3
24. Happé FGE, Booth RDL. The power of the positive: revisiting weak coherence in autism spectrum disorders. Q J Exp Psychol. 2008;61(1):50–63. doi:10.1080/17470210701508731
25. Stott N, Fox JRE, Williams MO. Attentional bias in eating disorders: a meta‐review. Int J Eat Disord. 2021;54(8):1377–1399. doi:10.1002/eat.23560
26. King JA, Korb FM, Vettermann R, Ritschel F, Egner T, Ehrlich S. Cognitive overcontrol as a trait marker in anorexia nervosa? Aberrant task- and response-set switching in remitted patients. J Abnorm Psychol. 2019;128(8):806–812. doi:10.1037/abn0000476
27. Saure E, Laasonen M, Lepistö‐Paisley T, Mikkola K, Ålgars M, Raevuori A. Characteristics of autism spectrum disorders are associated with longer duration of anorexia nervosa: a systematic review and meta‐analysis. Int J Eat Disord. 2020;53(7):1056–1079. doi:10.1002/eat.23259
28. Cardi V, Mallorqui-Bague N, Albano G, Monteleone AM, Fernandez-Aranda F, Treasure J. Social difficulties as risk and maintaining factors in anorexia nervosa: a mixed-method investigation. Front Psychiatry. 2018;26(9):12. doi:10.3389/fpsyt.2018.00012
29. Stewart CS, McEwen FS, Konstantellou A, Eisler I, Simic M. Impact of asd traits on treatment outcomes of eating disorders in girls: the impact of ASD traits on treatment outcomes of eating disorders in young people. Eur Eat Disord Rev. 2017;25(2):123–128. doi:10.1002/erv.2497
30. Pruccoli J, Rosa S, Cesaroni CA, Malaspina E, Parmeggiani A. Association among autistic traits, treatment intensity and outcomes in adolescents with anorexia nervosa: preliminary results. J Clin Med. 2021;10(16):3605. doi:10.3390/jcm10163605
31. Nazar BP, Peynenburg V, Rhind C, et al. An examination of the clinical outcomes of adolescents and young adults with broad autism spectrum traits and autism spectrum disorder and anorexia nervosa: a multi centre study. Int J Eat Disord. 2018;51(2):174–179. doi:10.1002/eat.22823
32. Nielsen S, Dobrescu SR, Dinkler L, et al. Effects of autism on 30-year outcome of anorexia nervosa. J Eat Disord. 2022;10(1):4. doi:10.1186/s40337-021-00518-1
33. Huke V, Turk J, Saeidi S, Kent A, Morgan JF. The clinical implications of high levels of autism spectrum disorder features in anorexia nervosa: a pilot study. Eur Eat Disord Rev. 2014;22(2):116–121. doi:10.1002/erv.2269
34. Dandil Y, Baillie C, Tchanturia K. Cognitive remediation therapy as a feasible treatment for a young person with anorexia nervosa and autism spectrum disorder comorbidity: a Case Study. Clin Case Stud. 2020;19(2):115–132. doi:10.1177/1534650119890425
35. Plemeniti Tololeski B, Suhodolčan Grabner A, Kumperscak HG. Adolescents with autism spectrum disorder and anorexia nervosa comorbidity: common features and treatment possibilities with cognitive remediation therapy and oxytocin. Front Psychiatry. 2021;3(12):686030. doi:10.3389/fpsyt.2021.686030
36. Lindvall Dahlgren C, Rø Ø. A systematic review of cognitive remediation therapy for anorexia nervosa - development, current state and implications for future research and clinical practice. J Eat Disord. 2014;2(1):26. doi:10.1186/s40337-014-0026-y
37. Adamson J, Leppanen J, Murin M, Tchanturia K. Effectiveness of emotional skills training for patients with anorexia nervosa with autistic symptoms in group and individual format. Eur Eat Disord Rev J Eat Disord Assoc. 2018;26(4):367–375. doi:10.1002/erv.2594
38. Galsworthy-Francis L, Allan S. Cognitive behavioural therapy for anorexia nervosa: a systematic review. Clin Psychol Rev. 2014;34(1):54–72. doi:10.1016/j.cpr.2013.11.001
39. Fairburn C. Cognitive Behavior Therapy and Eating Disorders. Guilford Press; 2008.
40. Spain D, Sin J, Chalder T, Murphy D, Happé F. Cognitive behaviour therapy for adults with autism spectrum disorders and psychiatric co-morbidity: a review. Res Autism Spectr Disord. 2015;9:151–162. doi:10.1016/j.rasd.2014.10.019
41. Muratore AF, Attia E. Current therapeutic approaches to anorexia nervosa: state of the art. Clin Ther. 2021;43(1):10. doi:10.1016/j.clinthera.2020.11.006
42. Giombini L, Nesbitt S, Kusosa R, et al. Neuropsychological and clinical findings of cognitive remediation therapy feasibility randomised controlled trial in young people with anorexia nervosa. Eur Eat Disord Rev. 2022;30(1):50–60. doi:10.1002/erv.2874
43. Tchanturia K, Larsson E, Adamson J. How anorexia nervosa patients with high and low autistic traits respond to group cognitive remediation therapy. BMC Psychiatry. 2016;16(1):334. doi:10.1186/s12888-016-1044-x
44. Dandil Y, Smith K, Adamson J, Tchanturia K. Individual cognitive remediation therapy benefits for patients with anorexia nervosa and high autistic features. Eur Eat Disord Rev. 2020;28(1):87–91. doi:10.1002/erv.2707
45. Babb C, Brede J, Jones CRG, et al. “It’s not that they don’t want to access the support … it’s the impact of the autism”: the experience of eating disorder services from the perspective of autistic women, parents and healthcare professionals. Autism. 2021;25(5):1409–1421. doi:10.1177/1362361321991257
46. Tchanturia K, Baillie C, Biggs C, et al. Sensory wellbeing workshops for inpatient and day-care patients with anorexia nervosa. Neuropsychiatrie. 2021. doi:10.1007/s40211-021-00392-y
47. Treasure J, Schmidt U, Kan C. An illustration of collaborative care with a focus on the role of fathers in Maudsley Anorexia Nervosa Treatment for Adults (MANTRA). J Clin Psychol. 2019;75(8):1403–1414. doi:10.1002/jclp.22789
48. Loomes R, Bryant-Waugh R. Widening the reach of family-based interventions for Anorexia Nervosa: autism-adaptations for children and adolescents. J Eat Disord. 2021;9(1):157. doi:10.1186/s40337-021-00511-8
49. Thapar A, Rutter M. Genetic advances in autism. J Autism Dev Disord. 2021;51(12):4321. doi:10.1007/s10803-020-04685-z
50. Cermak SA, Curtin C, Bandini LG. Food selectivity and sensory sensitivity in children with autism spectrum disorders. J Am Diet Assoc. 2010;110(2):238–246. doi:10.1016/j.jada.2009.10.032
51. Tchanturia K, Smith K, Glennon D, Burhouse A. Towards an improved understanding of the anorexia nervosa and autism spectrum comorbidity: PEACE pathway implementation. Front Psychiatry. 2020;Jul(11):640. doi:10.3389/fpsyt.2020.00640
52. Thomas JJ, Wons OB, Eddy KT. Cognitive–behavioral treatment of avoidant/restrictive food intake disorder. Curr Opin Psychiatry. 2018;31(6):425–430. doi:10.1097/YCO.0000000000000454
53. Thomas J, Eddy K. Cognitive-Behavioral Therapy for Avoidant/Restrictive Food Intake Disorder. United Kingdom: Cambridge University Press; 2019.
54. Tubío-Fungueiriño M, Cruz S, Sampaio A, Carracedo A, Fernández-Prieto M. Social camouflaging in females with autism spectrum disorder: a systematic review. J Autism Dev Disord. 2021;51(7):2190–2199. doi:10.1007/s10803-020-04695-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.